Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Healthcare Utilization and Costs After Appropriate or Inappropriate Implantable Defibrillator Shocks: A Retrospective Real-World Data Study in Japan
Authors Noda T, Matsumoto T, Tanaka Y ![]() , Goto T
, Goto T
Received 19 November 2025
Accepted for publication 6 February 2026
Published 31 March 2026 Volume 2026:18 577970
DOI https://doi.org/10.2147/CEOR.S577970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Takashi Noda,1 Tomoko Matsumoto,2 Yuji Tanaka,2 Tadahiro Goto3,4
1Cardiovascular Center, Kindai University Hospital, Sakai, Osaka, Japan; 2Healthcare Economics and Government Affairs, Medtronic Japan Co., Ltd., Minato-ku, Tokyo, Japan; 3Department of TXP Research, TXP Medical Co. Ltd., Chiyoda-ku, Tokyo, Japan; 4Department of Health Data Science, Yokohama City University, Yokohama, Kanagawa, Japan
Correspondence: Yuji Tanaka, Healthcare Economics and Government Affairs, Medtronic Japan Co., Ltd., Minato-ku, Tokyo, Japan, Tel +8180-7097-2442, Email [email protected]
Background: Implantable cardioverter-defibrillators (ICDs) and cardiac resynchronization therapy with defibrillators (CRT-Ds) effectively prevent sudden cardiac death. However, there is a lack of detailed data on healthcare utilization and healthcare cost following ICD/CRT-D shock events in Japan. This study aimed to examine real-world data (RWD) stored in an emergency department system to clarify healthcare utilization and healthcare costs associated with ICD/CRT-D shocks in Japan.
Methods and Results: This retrospective study analyzed RWD from four tertiary hospitals between January 2022 to June 2024. Among 1,807 ICD/CRT-D implanted adult patients, 84 patients (4.6%) who visited the hospital at least once following an ICD/CRT-D shock event were identified. Of these, a total of 146 ICD/CRT-D shock events were observed, with 33 patients (39.3%) experiencing multiple episodes. Of these, 122 (83.6%) were appropriate and 24 (16.4%) were inappropriate. Hospitalization was required in 55 (37.7%) cases. Appropriate shocks were associated with longer hospital stays (24.6 ± 29.3 vs. 12.5 ± 4.2 days) and higher costs (1,123,531 ± 2,195,483 JPY vs. 67,091 ± 131,282 JPY) than inappropriate shocks.
Conclusion: In this multicenter retrospective study using real-world data in Japan, we investigated the healthcare utilization and costs associated with ICD/CRT-D shock events. Our findings provide valuable insight into post-shock care in daily practice and highlight the need for optimized management strategies to improve care delivery and resource use in the Japanese clinical setting.
Keywords: implantable cardioverter-defibrillator, healthcare cost, retrospective real-world data analysis
Graphical Abstract:

Introduction
Implantable cardioverter-defibrillators (ICDs) and cardiac resynchronization therapy devices with defibrillators (CRT-Ds) are widely used for patients who have experienced lethal ventricular arrhythmias, such as ventricular tachycardia and ventricular fibrillation, or who have low left ventricular function with structural heart disease. In addition, these devices have been shown to improve survival in populations at high risk for sudden cardiac death,1,2 while ICD/CRT-D shocks including appropriate and inappropriate, are associated with impaired quality of life3,4 as well as increased mortality.5–7
Although data on healthcare utilization (HCU) and related expenditure for shock events are available from other regions,8,9 their applicability to the Japanese healthcare context remains limited. Furthermore, clinical data from Japan regarding potential differences between inappropriate and appropriate shocks in terms of treatment type and intensity are scarce. This study therefore aimed to examine real-world data (RWD) collected during routine clinical care and stored in an emergency department (ED) system to clarify healthcare utilization and medical costs associated with ICD/CRT-D shocks in Japan. This analysis was conducted across four tertiary hospitals representing geographic regions in Japan. The use of a nationally standardized healthcare reimbursement system may enhance the generalizability of the findings to routine clinical practice.
Methods
Study Design and Data Sources
This was a retrospective observational study utilizing data from tertiary hospitals in Japan. To efficiently extract data associated with ICD/CRT-D shocks, four hospitals, representing different areas of Japan, were selected for data analysis. These hospitals have implemented the NEXT Stage emergency room (NSER) patient information and management software (TXP Medical Co. Ltd., Tokyo, Japan), received a large number of ICD/CRT-D patients, demonstrated high levels of emergency medical activity, and had substantial experience in ICD/CRT-D implantations. The NSER structures emergency department data and links these records with Diagnosis Procedure Combination (DPC) data stored in TXP Medical’s data warehouse. Details of the NSER system have been described previously.10,11 DPC is a Japanese fixed-payment reimbursement system that standardizes hospital payments based on diagnosis and procedures.12 In addition, DPC data and medical chart data from the selected hospitals were extracted to identify patient characteristics, device type, shock type, comorbidity, medical procedures and healthcare costs. Contracts were executed between TXP Medical and each participating hospital. With the hospital’s authorization and in collaboration with the site principal investigator, TXP Medical personnel performed analyses on patient-level data within the hospital’s secure environment; no patient-level data were permitted to leave the hospital. Only aggregated (non-identifiable) results from the within-hospital analyses were transferred from each hospital to TXP Medical. TXP Medical then conducted additional analyses on the aggregate data received from each hospital and provided those results to Medtronic Japan. The study protocol was reviewed and approved by TXP Medical’s Ethics Committee, which confirmed the appropriateness of the data handling and ethical considerations. As the study did not involve any clinical intervention and no patient-level data were transferred outside the hospitals, approval from individual institutional review boards was deemed unnecessary. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Inclusion Criteria and Identification
This study included patients aged 18 years or older who underwent ICD/CRT-D implantation and had at least one visit following an ICD/CRT-D shock event between January 1, 2022 and June 30, 2024, as the inclusion criteria.
Patients with ICD/CRT-D implantation were identified in the DPC dataset using International Classification of Disease, 10th Revision (ICD-10) code Z95.0 (Presence of cardiac pacemaker) and classification ID 20098634 (Presence of implantable cardiac defibrillator) and in NSER by documented the past medical history and/or diagnosis. From the ICD/CRT-D implanted patients, those aged 18 years or older at the time of hospital visit following ICD/CRT-D shock were selected. The DPC dataset does not include codes related to ICD/CRT-D shock, so patients with evidence of at least one visit after an ICD/CRT-D shock event (not related to an external defibrillator or follow-up visit) were identified from the medical chart. Medical charts were reviewed by a trained data analyst (SW) from TXP Medical, who is a certified clinical laboratory technologist, under the supervision of an emergency physician and a critical care physician. Prior to data extraction, predefined judgment criteria were shared with the reviewer. During the review process, cases requiring complex clinical judgment were discussed with the supervising physicians, and the extracted data were revised as necessary. The supervising physicians ensured the medical validity of the assessments, including the appropriateness of shock classification. If the same patient visited the hospital multiple times, each visit was counted as a separate shock event. We also captured the number of ICD/CRT-D shock events per patient as well as the shock type and type of hospital visit for each shock.
Data Collection
All shock events were classified as either appropriate or inappropriate by medical chart review. Appropriate shocks were defined as those delivered for true ventricular tachyarrhythmias (ventricular tachycardia/ventricular fibrillation), whereas inappropriate shocks were defined as those delivered for any other type of detected rhythm, including atrial fibrillation, supraventricular tachycardia, T-wave oversensing, or noise, according to criteria described in the previous study by Turakhia et al.8 If the medical chart review included terms such as “inappropriate”, “malfunction”, or “erroneous shock”, the shock was classified as an inappropriate shock.
The primary outcomes were 1) ICD/CRT-D shock-related HCU and 2) expenditures resulting from the HCU. Shock-related HCU and patient characteristics were captured at the time of the post-shock hospital visit. The data were extracted by patient and/or shock event. Patient characteristics consisted of age, sex, admission route after shock, type of cardiac device implanted, presence of comorbidities, and current medications. HCU included hospital visits (outpatient or inpatient) and medical procedures (electrocardiography, X-rays, cardiac catheterization, echocardiography, emergency room visit, electrophysiology study and ablation, stress test, lead or device revision, percutaneous coronary intervention, circulatory support, heart/pericardium operations including surgery and cardioversion) by shock type and visit type. Clinical outcomes included length of hospital stay, and any recorded complications. The healthcare costs were estimated using the DPC EF data. These costs represent the sum of both the bundled payment (comprehensive fee) and fee-for-service components of the DPC payment system.12 Detailed information on the items, data sources, and code used in this study is provided in Supplemental Tables 1–4.
Statistical Analysis
Continuous variables are presented as means ± standard deviations, while categorical variables are expressed as counts and percentages. We did not conduct any statistical significance tests between appropriate and inappropriate shock events due to the lack of access to individual patient-level data and because we had access only to the aggregated data. To provide additional insights into healthcare costs and length of hospital stay, since percentile information (eg, median and interquartile range [IQR]) was not available in the aggregate data from each hospital, these values were estimated under the assumption that the data followed a gamma distribution. The estimated median and IQR were calculated using the inverse cumulative distribution function in Microsoft Excel for Microsoft 365 (Microsoft Corporation, Redmond, WA, USA). All other statistical analyses were conducted using R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Selection and Clinical Characteristics
From the DPC dataset, 1,807 individuals aged 18 years or older who underwent ICD or CRT-D implantation either during or prior to the study inclusion period were extracted. After the medical chart review, 84 patients who presented at least once after experiencing an ICD/CRT-D shock event were identified. Among them, 33 patients had multiple shock episodes, resulting in a total of 146 shock events (Figure 1). Full baseline characteristics at the hospital visit are presented in Table 1. The mean age of patients experiencing shock events was 65 ± 14 years, and the majority were male (86.9%). Among the 84 patients, the majority visited cardiology outpatient clinics following their ICD/CRT-D shock events, while a substantial number also presented to EDs. A few patients were seen in other outpatient departments. The most common comorbidities in the included patients were ventricular arrhythmias, followed by heart failure, atrial arrhythmias, hypertension, and ischemic heart disease including prior myocardial infarction. Regarding pharmacological treatment, 63.1% were prescribed beta-blockers, over 40% received antithrombotic or anticoagulant therapy, and 41.7% were on diuretics.
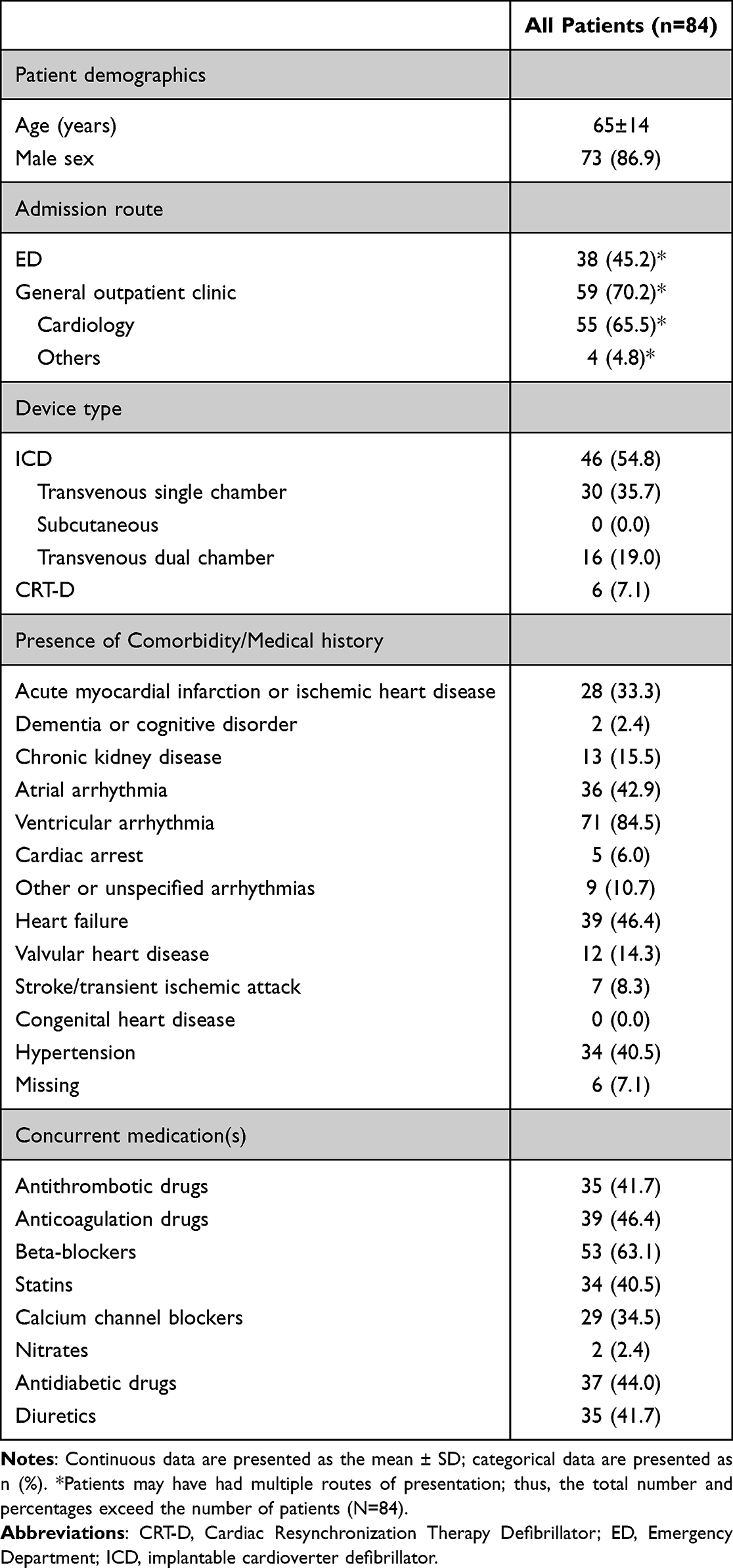 |
Table 1 Patient Characteristics of 84 Patients at the Hospital Visit After ICD/CRT-D Shock Event |
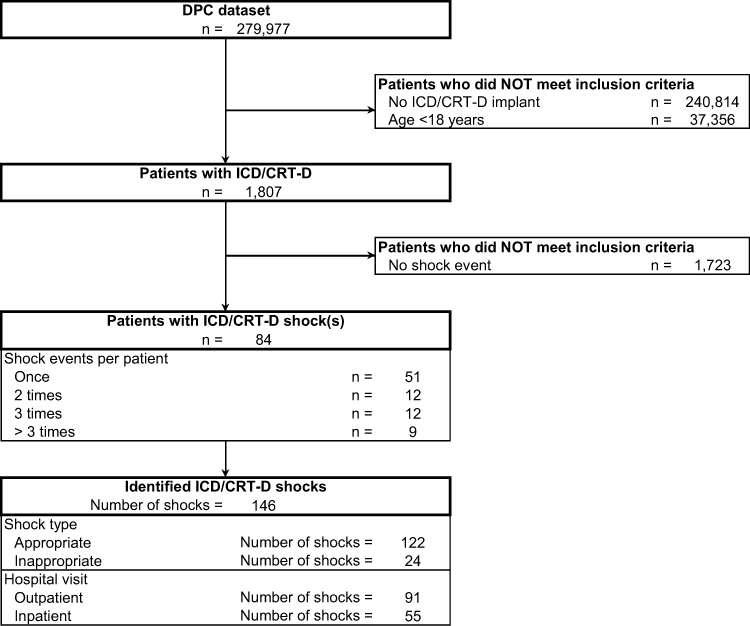 |
Figure 1 Patient flowchart. Abbreviations: CRT-D, Cardiac Resynchronization Therapy Defibrillator; DPC, Diagnosis Procedure Combination; ICD, implantable cardioverter defibrillator. Note: The names of each flow step are shown bold for clarity. |
Outcomes After Medical Consultation
Of the total 146 shock events, 122 events were classified as appropriate shock therapy, while 24 events were deemed inappropriate. In terms of care setting, 58.2% of shock events occurred in an outpatient setting and 41.8% of events required hospitalization. In contrast, 83.3% of inappropriate shock events were managed in an outpatient setting and deemed suitable for non-hospitalization (Table 2). None of these patients required intensive care unit admission.
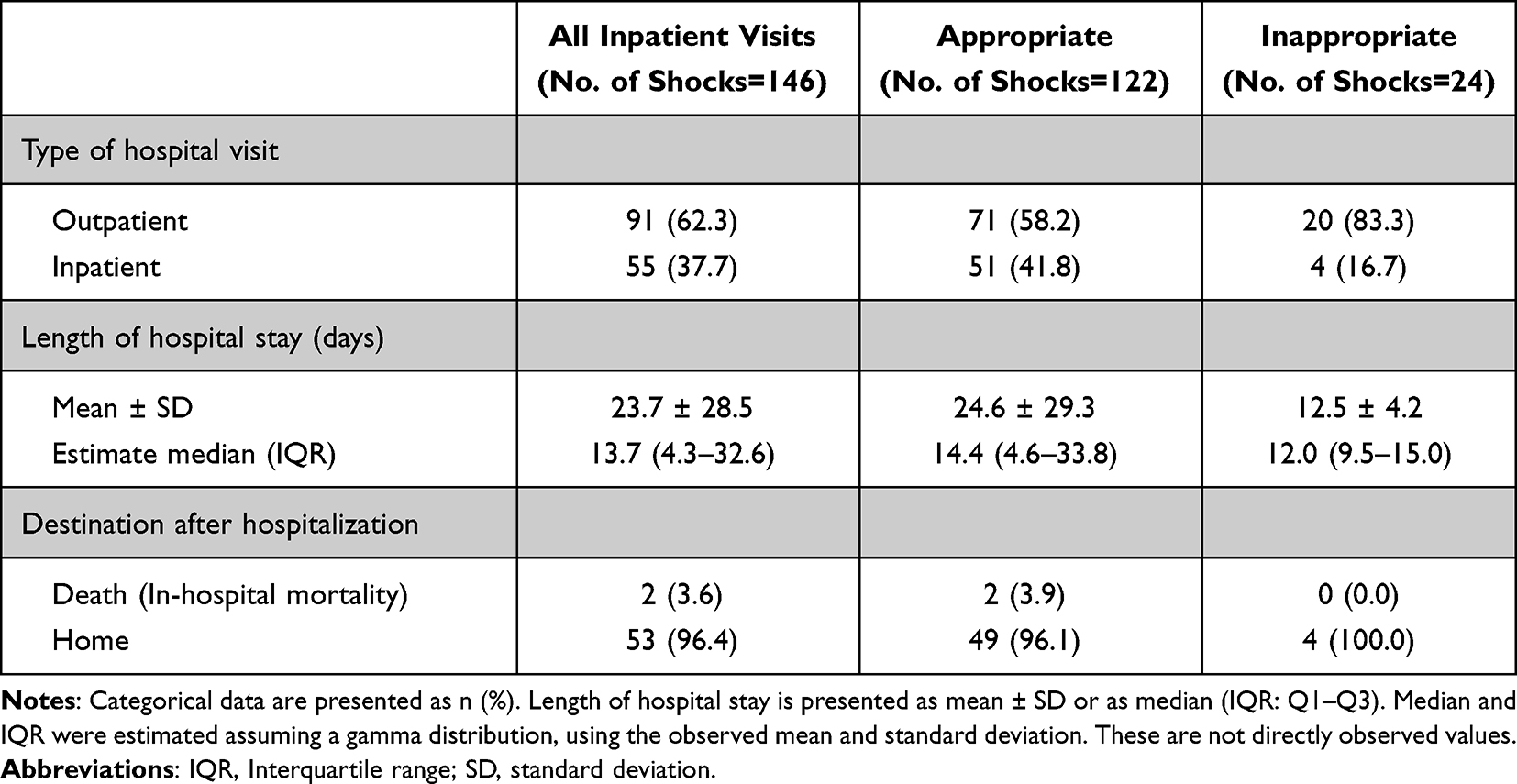 |
Table 2 Comparison of Hospitalization Characteristics for Appropriate and Inappropriate Shock Events |
In hospitalized patients with appropriate shock events, all patients underwent an ECG and chest X-ray (Figure 2). Echocardiography was performed in 72.7% of hospitalized patients and 83.1% of non-hospitalized patients in appropriate shocks events. However, among patients who were not hospitalized following inappropriate shock events, the rate of echocardiography was low at 20.0%. Patients with appropriate events often underwent further medical procedures, including emergency room visits, cardiac catheterization, and electrophysiology study and ablation. Circulatory support was provided in one case during lead or device replacement, which was presumed to be intra-aortic balloon pumping. Among patients who were not hospitalized, ECG and chest X-rays were routinely performed, followed by echocardiography. However, no additional medical procedures were performed beyond these standard evaluations in non-hospitalized patients, regardless of event appropriateness.
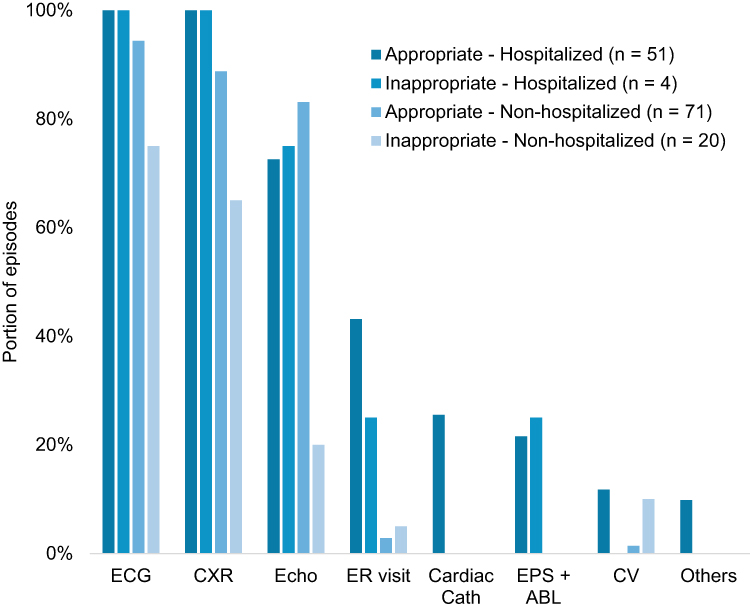 |
Figure 2 Procedures after hospital visit among 146 shock events. Abbreviations: ECG, Electrocardiogram; CXR, Chest X-ray; Echo, Echocardiography; ER visit, Emergency Room Visit; Cardiac Cath, Cardiac Catheterization; EPS + ABL, Electrophysiology Study and Ablation; CV, Cardioversion. |
Healthcare Costs
The average total hospital cost for all shock events was 949,870 ± 2,013,210 JPY (Table 3). When categorized by shock event appropriateness, the cost was 1,123,531 ± 2,195,483 JPY for appropriate shock events and 67,091 ± 131,282 JPY for inappropriate shock events. Healthcare costs were higher in appropriate events than in inappropriate ones, likely reflecting the greater need for medical interventions in such cases. Shock events managed in an outpatient setting had substantially lower healthcare costs than those managed with hospitalization and with less disparity between the type of shock event (20,268 ± 13,647 JPY for appropriate and 33,394 ± 29,498 JPY for inappropriate). The procedure associated with the highest individual cost was lead or device revision (Supplemental Table 5).
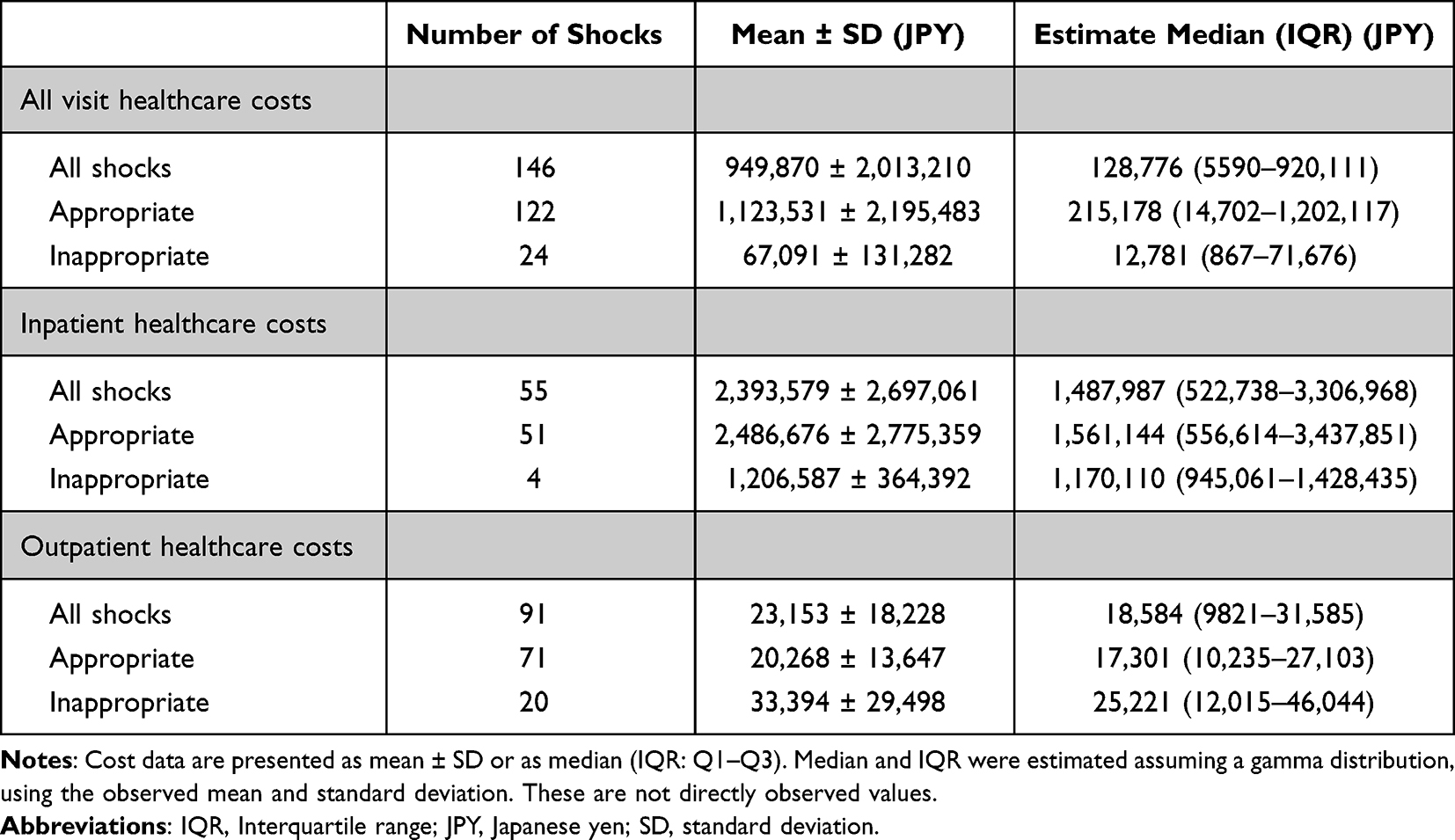 |
Table 3 Healthcare Costs Related to ICD/CRT-D Shock Events |
Length of Hospital Stay and Complications
The average length of hospital stay for all shock events was 23.7 ± 28.5 days. When categorized by shock event appropriateness, the length was 24.6 ±29.3 days for appropriate shock events and 12.5 ± 4.2 days for inappropriate shock events. Appropriate shock events were associated with longer hospital stays compared to inappropriate events. Among hospitalized patients with appropriate events, two deaths were recorded (Table 2).
The most frequently observed complications were cases of heart failure (14.5%), followed by infection- or sepsis-related issues (9.1%), which were categorized under “others”. In one appropriate event, emergency cardiovascular surgery was performed, which corresponded to lead or device revision (Supplemental Table 6).
Discussion
In this retrospective analysis of RWD collected from routine clinical practice and stored in the ED system, several key findings emerged. First, a subset of patients who had undergone ICD or CRT-D implantation experienced shock events that led to hospital visits, with some requiring hospitalization. Second, multiple shock episodes were observed among these patients, and a considerable proportion resulted in inpatient care. Lastly, hospital stays and associated costs varied widely, with appropriate ICD shocks generally linked to higher resource utilization.
Healthcare Costs After ICD Shock Events
The occurrence of ICD shocks, whether appropriate or inappropriate, is associated with increased healthcare costs as patients seek treatment, which may include hospital admissions for shock-related complications, the need for detailed check-ups, and potentially additional procedures such as emergency room visits, cardiac catheterization, and electrophysiology study and ablation, all of which increase healthcare resource use. Furthermore, patients who experience multiple ICD shocks often face serious complications, which can lead to higher healthcare resource consumption, including longer inpatient stays and more intensive management.
Several prior studies from Western countries have examined healthcare utilization following ICD shock events. A previous US study, examining ICD shock events using RWD from linked commercial and Medicare supplemental claims databases found both appropriate and inappropriate shocks initiated a cascade of healthcare utilization that frequently included invasive procedures, many with uncertain effects on patient outcomes.8 The investigators also showed that among all shock episodes, 46% had shock-related health care utilization and 14% were hospitalized. In contrast to our study, cardiac catheterization was performed in 75.7% of these patients including half of patients with inappropriate ICD shocks. The US study also showed that the costs for patients with appropriate ICD shocks were similar to those for patients with inappropriate ICD shocks ($5,592 ± $13,831 vs $4,470 ± $5,283, respectively). In contrast, our results found that healthcare costs were higher for patients with appropriate ICD shocks. A previous UK study reported that 89% of all shock episodes in patients with ICDs were associated with additional health care utilization and 37% of them required an inpatient stay.9 The total costs of patients with appropriate ICD shocks were higher than those for patients with inappropriate ICD shocks (£199,454 vs £53,098, respectively) although the mean length of hospital stay was shorter than that of our patients (3.6 ± 4.7 days vs 23.7 ± 28.5 days, respectively). These differences may partly reflect variations in healthcare systems, hospitalization practices, and reimbursement structures across countries.
Beyond direct medical costs, ICD/CRT-D shocks may also impose substantial indirect societal burdens. From a broader societal perspective, prolonged hospital stays may also result in substantial productivity losses, representing an important but often underexplored component of the overall economic burden associated with ICD/CRT-D shocks and warrant further investigation of indirect costs. Psychological distress following ICD implantation and ICD shocks may limit social participation or necessitate job changes or workplace reassignment, leading to indirect productivity losses for both patients and employers.13,14 These indirect costs are frequently overlooked and highlight the need for a more comprehensive evaluation of the socioeconomic impact of ICD/CRT-D shocks. Under the Japanese DPC system, per-diem bundled reimbursement is structured on the assumption that medical resource utilization decreases over the course of hospitalization; accordingly, the daily reimbursement rate tends to decline as the length of stay increases.15 As a result, hospital revenue generally decreases with prolonged hospitalization, potentially acting as a disincentive for extended hospital stays. Although additional fee-for-service components may still apply in severe or resource-intensive cases.
While appropriate shocks cannot be avoided, efforts to reduce the frequency of ICD shocks through anti-tachycardia pacing (ATP) as well as optimized device programming including high-rate cutoff or long duration of detection are important. One sub-analysis of the PROVIDE (Programming Implantable Cardioverter Defibrillators in Patients With Primary Prevention Indication) study by Sanders et al showed that patients with ICDs/CRT-Ds for primary prevention who received ATP therapy had lower healthcare costs mainly due to avoiding hospitalization compared with those who received shock therapy.16 The mean total cost per patient-year was $1,817 for patients with no therapy (no ATP and no shock therapy), $1,405 for those with ATP therapy only, and $4,278 for those with shock therapy. From both clinical and economic perspectives, these findings, together with evidence from prior studies, support the consideration of anti-tachycardia pacing in eligible patients as a potential approach to reduce ICD shocks and associated healthcare utilization. Careful arrhythmia management represents a strategy to minimize healthcare costs in the long term.
Clinical Impact of Shock Events in Patients with ICD/CRT-D
The role of ICDs is to avoid sudden cardiac death,17 by constantly detecting and terminating any life-threatening arrhythmias such as ventricular tachycardia or ventricular fibrillation by ATP or shock therapy. However, the use of these lifesaving technologies is not without risks. Indeed, ICD shocks can be painful and psychologically distressing for patients.3 The previous studies have noted that 80% of ICD patients reported that their main concern was “an unexpected ICD shock”, while a similar percentage answered that they “felt safer with an ICD”. In a sub-analysis of the PainFree SST clinical trial4 which examined the acute and long-term impact of ICD shocks on device-measured physical activity and patient-reported outcomes, an ICD shock has both immediate and long-term adverse effects on global and disease-specific quality of life measurements. About 90 days after an ICD shock, patient physical activity gradually increased and returned to pre-shock levels. Given the associations between reduced quality of life and subsequent adverse cardiac events, it seems reasonable to say that patients with an ICD who experience shock and a prolonged decline in physical activity and quality of life attributed to the ICD shock may have an increased risk of hospitalization, morbidity, and mortality.4,18 In terms of psychological effects, in one recent meta-analysis, ICD patients who experienced shocks had significantly higher odds of having anxiety (odds ratio [OR] 3.92; 95% confidence interval [CI] 1.67–9.19) or depression (OR 1.86; 95% CI 1.34–2.59) compared to those patients who did not experience shocks.13 In another study conducted in the US, approximately 20% of the ICD patients experiencing shocks were diagnosed with post-traumatic stress disorder.19
Several studies have also shown that patients who receive appropriate shocks have a worse prognosis compared to those without shocks although appropriate ICD shocks are life-saving interventions for lethal ventricular arrhythmias.5,6 The sub-analysis of the SCD-HeFT study revealed that an appropriate ICD shock was associated with a significant increase in the subsequent risk of death from all causes compared with no appropriate shock (hazard ratio [HR] 5.68; 95% CI 3.97–8.12; P < 0.001) and the most common cause of death among patients who received any ICD shock was progressive heart failure.5 Moreover, multiple appropriate ICD shocks can be associated with a further increase in all-cause mortality. As for Japanese patients, Tenma et al have also reported that the amount of shock energy was significantly associated with all-cause death (adjusted HR 126 per 100 joule increase; P < 0.01), especially in the patients with low left ventricular ejection fraction.6 Indeed, appropriate shocks may indicate advanced heart disease and progression of heart failure as well as electrical instability leading to a worse prognosis. Therefore, an appropriate shock is not only a therapeutic event but also a marker of increased mortality risk and poor long-term outcomes.
ATP is an effective therapy provided by ICDs to terminate certain types of ventricular tachyarrhythmias, avoiding both painful shocks and reductions in activity levels.4 In addition, several clinical studies have demonstrated that ATP can safely and effectively terminate monomorphic ventricular tachycardia, thereby significantly reducing the number of ICD shocks and improving mortality rates as well as patient quality of life.7,20 A sub-analysis of the MADIT-RIT7 study has shown that appropriate ICD shocks were independently associated with an increased mortality risk (HR 6.32; 95% CI 3.13–12.75; p<0.001) whereas appropriate ATP was not related to an adverse outcome (HR 1.02; 95% CI 0.36–2.88; P=0.98). Therefore, minimizing ICD shocks through effective ATP programming and arrhythmia management strategies may be considered crucial in improving the long-term prognosis in ICD recipients and reducing healthcare utilization and costs. Optimal programming and patient-centered follow-up are essential to minimize unnecessary shocks and maximize therapeutic benefit. Future studies, including cost-utility analyses incorporating quality-of-life data, may help further clarify the broader economic implications of optimized device programming strategies such as ATP.
Limitations
This study had several limitations. First, this was a descriptive study based on secondary real-world data and was not designed to evaluate causal relationships or treatment effects. As with other secondary data analyses, this study evaluates HCU and healthcare costs based on routinely collected RWD from clinical settings. The data were retrospectively collected, and not all variables were available for every patient, leading to potential data missingness. While not all missing rates will be reported, the outcome data were complete for all patients, which enhances the reliability of the study findings. Second, due to the small sample size and the use of aggregated data, formal sensitivity analyses and adjustment for unmeasured confounding were not feasible. Therefore, the results should be interpreted as descriptive estimates rather than evidence of causal associations. Third, the RWD used in this study were obtained from four hospitals over a 2.5-year period, which may limit the generalizability of the findings to the broader patient population in Japan. Fourth, once patients were transferred to hospitals not covered by the TXP Medical RWD system, they could not be followed across institutions, and data linkage to external sources was not feasible. Fifth, baseline information based on prior medical history may be insufficient if the patient was not previously seen at the same hospital, as it often depends on patient interviews and may not be based on verified diagnoses. Sixth, it is difficult to capture deaths that occurred outside the hospitals covered by TXP Medical. Since most mortality data are collected during hospitalization, mortality may be underestimated. Seventh, in the patient identification process, some patients without actual shock events may have inadvertently been included. However, the thorough clinician-assisted review of patient medical chart undertaken as part of this study would have improved the likelihood of excluding these patients. Finally, given the descriptive nature of this study and the limited sample size, no causal inference can be made, and the findings should be interpreted as descriptive rather than inferential. Future studies using patient-level data with larger sample sizes and comparative designs are warranted to further explore potential causal relationships.
Conclusion
In this multicenter retrospective study using routinely collected RWD from Japanese emergency care and outpatient settings, we characterized the healthcare utilization and associated healthcare costs following ICD/CRT-D shock events. Our findings reveal the substantial medical resource demands and variability in care based on shock type and setting, providing important insights into current clinical practices in Japan. These results may inform future strategies for optimizing ICD/CRT-D management and resource allocation in real-world clinical environments.
Data Sharing Statement
The data generated in this study will not be shared.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of TXP Medical (Approval No. TXPREC-026).
Acknowledgments
We would like to thank Shiruku Watanabe (TXP Medical) for their valuable contributions to the electronic medical chart review.
Funding
This study was conceived and funded by Medtronic Japan.
Disclosure
TN have received compensation for advisory services for this study from Medtronic Japan, and other payments including honoraria, for lectures which were not directly associated with this study from Medtronic Japan. TM and YT are employees of Medtronic Japan. TG is an employee of TXP Medical, a company commissioned by Medtronic Japan. The authors have no other conflicts of interest to disclose for this work.
References
1. Bardy GH, Lee KL, Mark DB, et al; Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–11. doi:10.1056/NEJMoa043399
2. Iwasaki YK, Noda T, Akao M, et al; Japanese Circulation Society and Japanese Heart Rhythm Society Joint Working Group. JCS/JHRS 2024 guideline focused update on management of cardiac arrhythmias. J Arrhythm. 2025;41(3):e70033. doi:10.1002/joa3.70033
3. Januszkiewicz Ł, Barra S, Providencia R, et al. Long-term quality of life and acceptance of implantable cardioverter-defibrillator therapy: results of the European Heart Rhythm Association survey. Europace. 2022;24(5):860–867. doi:10.1093/europace/euac011
4. Sears SF, Rosman L, Sasaki S, et al. Defibrillator shocks and their effect on objective and subjective patient outcomes: results of the PainFree SST clinical trial. Heart Rhythm. 2018;15(5):734–740. doi:10.1016/j.hrthm.2017.12.026
5. Poole JE, Johnson GW, Hellkamp AS, et al. Prognostic importance of defibrillator shocks in patients with heart failure. N Engl J Med. 2008;359(10):1009–1017. doi:10.1056/NEJMoa071098
6. Tenma T, Yokoshiki H, Mitsuyama H, et al. Relation between total shock energy and mortality in patients with implantable cardioverter-defibrillator. Int J Cardiol. 2018;259:94–99. doi:10.1016/j.ijcard.2018.02.063
7. Ruwald AC, Schuger C, Moss AJ, et al. Mortality reduction in relation to implantable cardioverter defibrillator programming in the Multicenter Automatic Defibrillator Implantation Trial-Reduce Inappropriate Therapy (MADIT-RIT). Circ Arrhythm Electrophysiol. 2014;7(5):785–792. doi:10.1161/CIRCEP.114.001623
8. Turakhia MP, Zweibel S, Swain AL, et al. Healthcare utilization and expenditures associated with appropriate and inappropriate implantable defibrillator shocks. Circ Cardiovasc Qual Outcomes. 2017;10(2):e002210. doi:10.1161/CIRCOUTCOMES.115.002210
9. Llewellyn J, Barker E, Bowe C, et al. Assessing the cost and resource use impact of implantable cardiac defibrillator shocks in the UK CareLink Population. Clinicoecon Outcomes Res. 2023;15:425–432. doi:10.2147/CEOR.S403712
10. Kondo Y, Chiba T, Osawa M, et al. Medical cost analysis of implantable cardioverter defibrillators for primary prevention among cardiac arrest patients. Circ J. 2025;90:118–125. doi:10.1253/circj.CJ-25-0195
11. Goto T, Hara K, Hashimoto K, et al. Validation of chief complaints, medical history, medications, and physician diagnoses structured with an integrated emergency department information system in Japan: the Next Stage ER system. Acute Med Surg. 2020;7(1):e554. doi:10.1002/ams2.554
12. Nakagawa Y, Takemura T, Yoshihara H, et al. A new accounting system for financial balance based on personnel cost after the introduction of a DPC/DRG system. J Med Syst. 2011;35(2):251–264. doi:10.1007/s10916-009-9361-y
13. Ghezzi ES, Sharman RLS, Selvanayagam JB, et al. Burden of mood symptoms and disorders in implantable cardioverter defibrillator patients: a systematic review and meta-analysis of 39 954 patients. Europace. 2023;25(6):euad130. doi:10.1093/europace/euad130
14. Yamagishi Y, Watabe T, Nakahara D, et al. Characteristics of anxiety about returning to work after implantable cardioverter defibrillator implantation in Japan. J Cardiol. 2026;87(1):102–107. doi:10.1016/j.jjcc.2025.05.019
15. Hayashida K, Murakami G, Matsuda S, et al. History and profile of Diagnosis Procedure Combination (DPC): development of a real data collection system for acute inpatient care in Japan. J Epidemiol. 2021;31(1):1–11. PMID: 33012777; PMCID: PMC7738645. doi:10.2188/jea.JE20200288
16. Sanders P, Connolly AT, Nabutovsky Y, et al. Increased hospitalizations and overall healthcare utilization in patients receiving implantable cardioverter-defibrillator shocks compared with antitachycardia pacing. JACC Clin Electrophysiol. 2018;4(2):243–253. doi:10.1016/j.jacep.2017.09.004
17. Moss AJ, Zareba W, Hall WJ, et al; Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346(12):877–883. doi:10.1056/NEJMoa013474
18. Kramer DB, Mitchell SL, Monteiro J, et al. Patient activity and survival following implantable cardioverter-defibrillator implantation: The ALTITUDE Activity Study. J Am Heart Assoc. 2015;4(5):e001775. doi:10.1161/JAHA.115.001775
19. Sears SF, Harrell R, Sorrell A, et al. Addressing PTSD in implantable cardioverter defibrillator patients: state-of-the-art management of ICD shock and PTSD. Curr Cardiol Rep. 2023;25(9):1029–1039. doi:10.1007/s11886-023-01924-4
20. Strickberger SA, Canby R, Cooper J, et al. Association of antitachycardia pacing or shocks with survival in 69,000 patients with an implantable defibrillator. J Cardiovasc Electrophysiol. 2017;28(4):416–422. doi:10.1111/jce.13170
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.