Back to Journals » Clinical Epidemiology » Volume 17
Healthcare Use Patterns for High Volume Musculoskeletal Shoulder Disorders: A Longitudinal Cohort from the US Military Health System
Authors George SZ ![]() , Morton-Oswald S, Lee HJ, Horn ME
, Morton-Oswald S, Lee HJ, Horn ME ![]() , Bhavsar NA, Rhon DI
, Bhavsar NA, Rhon DI
Received 23 July 2025
Accepted for publication 25 November 2025
Published 10 December 2025 Volume 2025:17 Pages 1049—1060
DOI https://doi.org/10.2147/CLEP.S555681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor H Sorensen
Steven Z George,1 Sarah Morton-Oswald,2 Hui-Jie Lee,2 Maggie E Horn,3 Nrupen A Bhavsar,4 Daniel I Rhon5
1Departments of Orthopaedic Surgery and Population Health Sciences, Duke Clinical Research Institute, Duke University, Durham, NC, USA; 2Department of Biostatistics and Bioinformatics, Duke University School of Medicine, Durham, NC, USA; 3Departments of Orthopaedic Surgery and Population Health Sciences, Duke University, Durham, NC, USA; 4Departments of Surgery and Biostatistics and Bioinformatics, Duke University School of Medicine, Durham, NC, USA; 5Department of Physical Medicine and Rehabilitation, F. Edward Hébert School of Medicine, Uniformed Services University, Bethesda, MD, USA
Correspondence: Steven Z George, Email [email protected]
Background: Shoulder injuries are a prevalent form of musculoskeletal disorders and common reason to seek healthcare. Health system level care utilization patterns for shoulder disorders are unknown. Accordingly, we described the frequency and timing of diagnostic imaging and treatment for a new episode of shoulder pain and determine usage variations across common diagnostic subgroups, military, and private sector care clinics.
Methods: A retrospective cohort of US Military Health System beneficiaries (n = 456,241) classified into 1) non-specific shoulder diagnosis only, 2) rotator cuff/sub-acromial pain, 3) acromioclavicular (AC joint) dysfunction, 4) shoulder instability/dislocation, 5) hypomobility/adhesive capsulitis, 6) osteoarthrosis, and 7) multiple diagnoses. Outcomes were healthcare use encounters within the first three months of the index visit classified into diagnostic imaging, pharmacological, and non-pharmacological treatments.
Results: The mean age of the cohort was 41 years old (SD 13). A majority of the cohort never received diagnostic imaging (76.7%). Advanced imaging was common for the multiple diagnoses group (53.6% of all advanced imaging). NSAIDS was the most common pharmacological treatment with 10.4% receiving at least one prescription, and physical therapy was the most common nonpharmacologic treatment received by 31% of the cohort. There was lower physical therapy and active treatment use and higher MRI or X-ray use for the same diagnostic group when care was initiated in a civilian clinic. Patients with rotator cuff disorders, multiple shoulder diagnoses, and hypomobility disorders were likely to have received at least one steroid joint injection if care was initiated in civilian compared to military clinics (28.1% vs 16%; 41.2% vs 32%; and 18.6% vs 13.3%, respectively).
Conclusion: Care patterns for high volume shoulder injuries were largely congruent across military and civilian clinics. However, for specific diagnostic groups, use of imaging, steroid injections and physical therapy varied notably between military and civilian clinics.
Keywords: shoulder condition, health care utilization, shoulder disorder, care patterns
Introduction
Shoulder conditions and disorders are commonly experienced musculoskeletal pain conditions and have a prevalence (20.9%) comparable to back (26.9%) and neck pain (20.6%).1 For example, in a 15-year population-based study in the Netherlands, only 47% of the cohort were free of chronic arm, neck, or shoulder pain throughout the observation period.1 The 53% experiencing these conditions were further described as having either development (18.3%), persistence (8.5%), recovery (7.5%), or variable (18.7%) disease courses.2 Moreover, the healthcare burden is high for those with shoulder injuries, including up to 58% of those with chronic arm, neck, and shoulder pain from the aforementioned Netherlands cohort study.3
Health system level care utilization patterns for shoulder conditions and disorders have not previously been well described; a stark contrast to other commonly occurring musculoskeletal conditions like low back pain.4,5 Furthermore, available literature for characterizing shoulder conditions has included cross-sectional analysis which does not allow for an understanding of healthcare utilization and care trajectories over time.6 This knowledge gap has potentially important ramifications for data-driven recommendations improving care for this highly prevalent musculoskeletal condition. Also, in many instances, shoulder conditions are grouped broadly as “musculoskeletal pain” for population-based studies, including being clustered with neck and arm pain as in the aforementioned cohort study in the Netherlands, as well as other studies.7,8 Most large-scale healthcare resource utilization (HCRU) studies have focused on other areas of musculoskeletal pain, leaving shoulder conditions and disorders as under-studied. Furthermore, the lack of shoulder-specific data on HCRU limits the development of value-based models that have been established in similarly prevalent conditions.
Similar to other body regions, several different diagnostic categories of shoulder conditions exist, ranging from acute injuries to severe degenerative disease requiring surgery. Moreover, prognosis and care trajectories can vary substantially across shoulder conditions. Therefore, when examining healthcare utilization patterns at the population level, conditions should be evaluated separately. From a policy and planning perspective, knowledge of how healthcare use varies across different diagnostic categories is a necessary first step to understanding which care patterns have the highest impact on the health system. The knowledge of healthcare use across different shoulder diagnostic categories is important because it informs whether ongoing management is potentially aligned with best practice recommendations. Investigation of alignment with best practice recommendations for shoulder conditions and disorders is largely missing from existing literature but is important to know given its high prevalence. One analysis investigating the timing and ordering of manual therapy and opioid prescription for shoulder pain within the military health system provided insights related to the economic burden of these care pathways.9 Another analysis of the same health system, this time for knee disorders, demonstrated cost savings to the organization when stepped care pathways are followed.10 However, such examples are rarely reported in the literature. Filling this information gap will also allow future assessment of whether shoulder care (in this and other health systems) aligns with best practice recommendations for diagnostic imaging use,11–13 and pharmacologic and nonpharmacologic treatments.12,14,15
This analysis used routinely collected health data to 1) describe the frequency and timing of diagnostic imaging (x-rays and advanced imaging services) and treatment use (non-pharmacologic and pharmacologic) for a new episode of shoulder pain and 2) identify how usage varied across high-volume shoulder conditions in different settings (military clinics versus private sector care). High volume conditions represent those most commonly seen within the health system. This analysis adds to the existing literature by HCRU among patients within different shoulder diagnostic categories, thereby enabling future efforts to better understand what constitutes value-based care for this highly prevalent musculoskeletal condition.
Methods
Study Overview
This was a retrospective cohort study of United States Military Health System (MHS) beneficiaries seeking care for a shoulder disorder. The MHS is a single-payer government health system and one of the largest health systems in the US, with over 50 hospitals and over 400 clinics. We used de-identified data from the MHS Data Repository (MDR) from January 2013 to July 2019; specifically, the Comprehensive Ambulatory/Professional Encounter Records (CAPER), the Non-Institutional TRICARE Encounter Data (TED-NI), the Ancillary Laboratory and Radiology data (Ancillary), the Pharmacy Detail Transaction Service data (PDTS), the Defense Enrollment Eligibility Reporting System (DEERS), the Institutional TRICARE Encounter Data (TED-I), and the Standard Inpatient Data Records (SIDR). CAPER and SIDR include data from the outpatient and inpatient electronic medical records used in military clinics. TED-NI and TED-I include claims data from outpatient and inpatient visits in the private sector. The ancillary file includes imaging procedures that take place in military clinics, and PDTS includes all prescription data from outpatient encounters. The index date was defined as the date the individual had their first encounter that recorded a shoulder disorder diagnosis or procedure (Supplemental Table 1). Both sources that feed to the MDR, from military or private sector care clinics, are based on procedure (Current Procedural Terminology – CPT) and diagnosis (International Statistical Classification of Diseases and Related Health Problems (ICD) codes, allowing for a standardized comparison).16
Ethics Approval
This project received ethics approval from the Institutional Review Board at US Army Medical Center of Excellence, San Antonio, TX (#25-00019n, PI: Dan Rhon). The Institutional Review Board at Duke University reviewed this project and declared it as exempt because statistical analyses were performed on de-identified data (Pro00109909, PI: Steven George).
Eligibility Criteria
Individuals had an index date between July 2013, and March 2019. To be eligible, all cases were required to have a minimum six-month lead-in period (ie, no care seeking for shoulder disorder) and a three-month follow-up period to ensure this was a new episode of shoulder pain and to allow for a three-month analysis window of initial care utilization.
Patients were excluded if they were older than 65 years old, or less than 18 years old on the index date except those on active duty as emancipated minors, or their index visit was in an inpatient setting. Patients were further excluded if, during the surveillance period, they had a diagnosis or procedure indicating trauma, open dislocation, shoulder/humerus fractures, or upper extremity amputation. Diagnosis codes for the exclusion criteria can be found in Supplemental Table 1.
Exposures
Using encounters within three months of the index visits, the primary diagnostic shoulder group exposures were classified as: 1) non-specific shoulder diagnosis only, 2) rotator cuff/sub-acromial pain, 3) acromioclavicular (AC joint) dysfunction, 4) shoulder instability/dislocation, 5) hypomobility/adhesive capsulitis, 6) osteoarthrosis (OA), and 7) multiple diagnoses (Supplemental Table 1). Individuals with more than one specific diagnosis were placed in the multiple diagnoses category. The secondary exposure was the location of the index visit, which could be either military clinics or private sector (civilian clinics) care.
Outcomes
The study outcomes were HCRU within the first three months from the index visit and were broadly classified into three main groups: diagnostic imaging, pharmacological, and non-pharmacological treatments (codes in Supplemental Table 2). Diagnostic imaging procedures included radiographs, magnetic resonance imaging (MRI), magnetic resonance arthrogram (MRA), and computed tomography (CT) scans. Imaging that included MRI, MRA, or CT was further categorized as advanced imaging. Patients who received both radiographs and advanced imaging were further categorized based on the order of imaging (radiograph prior to advanced imaging or vice versa). Pharmacological treatments included prescriptions for NSAIDs, opioids, benzodiazepines, muscle relaxers, analgesics, and steroid joint injections, based on American Hospital Formulary Service therapeutic class codes in the PDTS file. Non-pharmacological treatments included receipt of acupuncture, physical therapy, and then more specifically whether patients received supervised therapeutic exercise, passive modalities (eg, ultrasound, electrical stimulation, heat/cold therapy), or manual therapy. These outcomes were defined as binary indicators of utilization and as continuous variables (ie, number of procedures, prescriptions, and treatment visits per patient).
Data Analysis
For Aim 1, the HCRU in the first three months of shoulder care across the diagnostic shoulder groups was summarized as the number of unique people who received that care at least once. In addition, descriptive statistics, including the mean and standard deviation, summarized the number of times the care was received per patient. Chi-square and Wilcoxon rank sum tests were used to test the difference in treatment receipt between diagnosis categories without adjusting for multiple testing. However, given the large sample size of this study, a small non-clinically important difference can be claimed as statistically significant with a p-value <0.05.17 Therefore, the focus on clinical relevance was prioritized, and inferential statistical testing was not performed.
For Aim 2, we descriptively compared the same HCRU outcomes between cases that occurred initially in military clinics versus private sector clinics for each shoulder disorder category. All statistical analyses were completed using SAS 9.4 software (SAS Institute, Cary, NC, USA).
Results
The initial data abstraction from MDR identified 1,488,821 unique persons with care for an initial episode of shoulder pain from January 2013 to July 2019 in MDR. After exclusions for age, prior shoulder care, trauma-related incidents, and minimum eligibility periods, the research team was provided with a file representing 663,573 unique individuals. Manual validation of the data removed additional cases based on age, presence of shoulder trauma, and beneficiary eligibility windows not met. This led to 456,241 individuals meeting eligibility for inclusion in the final cohort (Table 1). The two most common reasons an individual was excluded during manual validation were not having the index visit in an outpatient setting (n = 22,046) and having evidence of fracture or trauma (n = 106,772). The summary of this cohort by diagnostic group is presented in Table 2 and by index clinic type (Supplemental Table 3). The size of the diagnostic groups ranged from non-specific shoulder pain as the largest (n = 305,764, 67%) to rotator cuff injury (n = 84,698, 18.6%) to AC joint disorders as the smallest (n = 4,013, <0.1%).
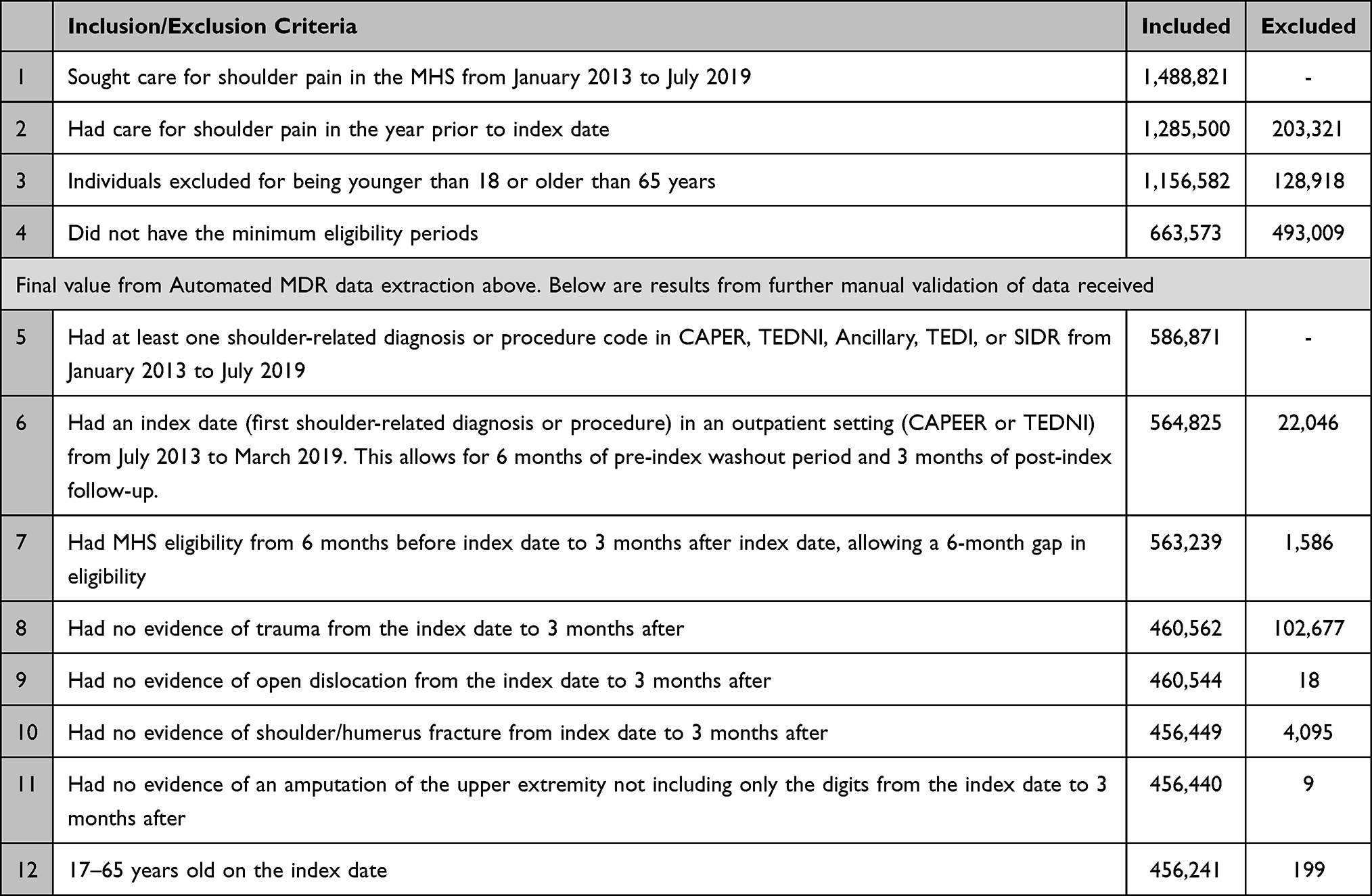 |
Table 1 Summary of Individuals Included and Excluded from Analysis |
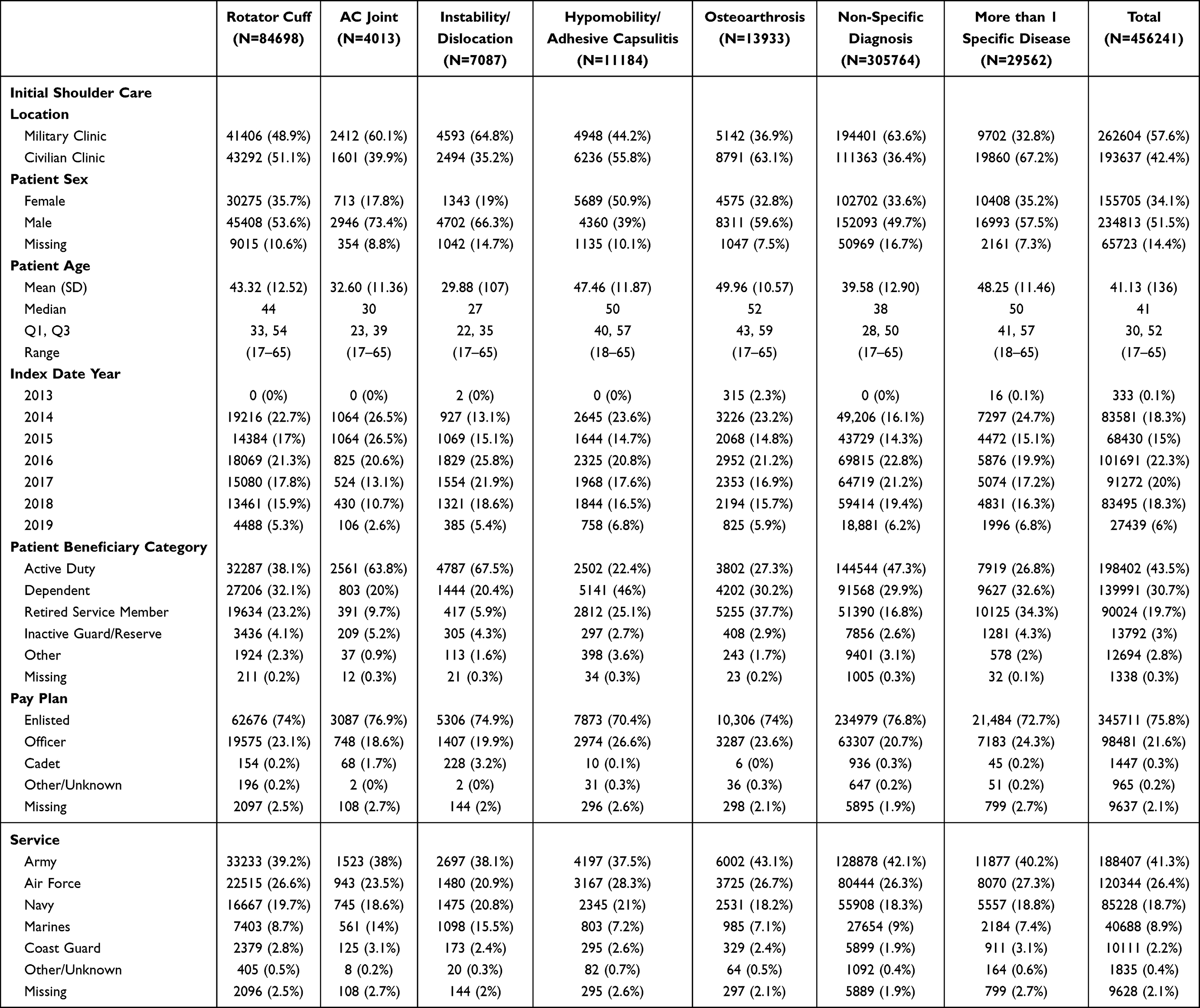 |
Table 2 Demographic Characteristics by Diagnostic Groups |
Table 2 was stratified by the diagnostic groups and the characteristics summarized include the data source of the patient’s index date, age, index year, sex, beneficiary category, pay plan, and service branch (the latter two variables represent the status of the sponsor). Sex was missing for 14.4% of the total patients. All diagnostic groups showed a higher percentage of male patients (between 49.7% and 73.4%) except for the Hypomobility/Adhesive Capsulitis disease group which had 50.9% female patients and only 39% male. Patients with hypomobility/adhesive capsulitis, OA, and multiple diagnoses had a higher mean age (47, 50, and 48, respectively), whereas patients with AC Joint and instability/dislocation had a lower mean age (33 and 30, respectively). The AC Joint and Instability/Dislocation disease groups had the highest percentage of active duty patients (63.8% and 67.5%, respectively), compared to the others which ranged from 22.4% to 47.3%. Across all diagnostic groups, patients were mainly enlisted members (ranging from 70.4% to 76.9%; compared to officers) within the Army (37.5–43.1%; compared to the other service branches).
Supplemental Table 3 reports patient characteristics based on the location of the initial shoulder care (military or private sector clinic). Patients with missing sex were all initially seen in military clinics. Patients whose initial care occurred in the military clinics had a lower mean age compared to patients with initial care occurring in private sector clinics (38 vs 46, respectively). As expected, a higher percentage of active-duty service members were seen in military versus private sector clinics (63% vs 17%), compared to fewer dependent (18.3% vs 47.5%) and retired service members (13.4% vs 28.3%).
Diagnostic Imaging (Aim 1)
A majority of the cohort never received diagnostic imaging (76.7% overall), but there was variability in imaging use among diagnostic groups (Supplemental Table 4). For example, 61.4% of patients with OA and 73.5% with multiple diagnoses had at least one imaging procedure. Radiographs were the most common imaging (18.3% overall), except for the multiple diagnoses group receiving equal radiographs and MRIs (53.6% and 53.0% respectively). Advanced imaging was most common for the multiple diagnoses group (53.6%), followed by OA (22.8%), rotator cuff (17.4%), and instability/dislocation disorders (12.4%). When examining the order of imaging services among patients who used imaging services, 34.4% of the patients with multiple diagnoses had a radiograph first, 27.1% had only a radiograph, 27% had only advanced imaging, and 11.1% had advanced imaging prior to a radiograph. Of the patients who used imaging services, the percentage of patients with advanced imaging first was the highest in the multiple diagnoses group (11.1%), followed by the rotator cuff group (5.5%) and Hypomobility/Adhesive Capsulitis disease group (3.5%). Advanced imaging prior to radiograph occurred for only <3% of those in all other diagnostic groups.
Pharmacologic and Nonpharmacologic Treatments (Aim 1)
Supplemental Table 4 summarizes pharmacologic and nonpharmacologic treatments by the shoulder diagnosis groups. NSAIDs were the most common pharmacological treatment across the entire cohort, with 10.4% receiving at least one prescription. Within the diagnostic groups, almost 13% or higher received an NSAID prescription in hypomobility/adhesive capsulitis, OA, and multiple diagnoses groups. This was closely followed by steroid injections with 10.2% overall, and within the diagnostic groups, >20% for rotator cuff, OA, and multiple diagnoses groups. Opioid prescriptions were filled by 8.4% of the patients overall, but within the diagnostic groups >10% in hypomobility/adhesive capsulitis, OA, and multiple diagnoses groups. Benzodiazepine prescriptions were the least common, with only 3.6% of the cohort receiving this medication. Among those who had at least one prescription of NSAIDS or opioid, the mean numbers of NSAIDS or opioid prescriptions were around 5 or 3 for all diagnostic groups, respectively. Among those who had at least one steroid joint injection, the mean number was 1 across all diagnostic groups.
Physical therapy was received by 31% of the cohort. Specific elements included therapeutic exercise (32.2% having at least one occurrence), followed by manual therapy (19.7%), and passive treatments (13.7%). Those who received therapeutic exercise or physical therapy had a mean number of around 5 sessions, with the diagnostic groups of Hypomobility/Adhesive capsulitis and multiple diagnosis groups having the most sessions. Acupuncture was used for 0.4% of the cohort, thus limiting the ability to explore variation across different diagnostic groups.
Differences in Military and Civilian Care Settings (Aim 2)
Supplemental Table 5 compares HCRU between patients initially seen in civilian and military clinics. Figure 1 illustrates the percentages of patients utilizing at least one pharmacological treatment by diagnostic groups and location of the initial shoulder care encounter (military or private sector clinic). Receipt of pharmacological treatments was relatively similar between clinic types within the same disease group, except for a few instances. NSAIDs were filled about 3% more often for private sector shoulder care compared to military clinics for patients with rotator cuff disorders, AC joint, instability/dislocation, and non-specific diagnosis. The percentages of patients using opioids were higher by 1–2% when care was initiated in a private sector clinic compared to a military clinic for all diagnostic groups except for Hypomobility/Adhesive capsulitis and OA. Patients with rotator cuff disorders, Hypomobility/Adhesive capsulitis, and multiple diagnoses were more likely to have received at least one steroid joint injection if shoulder care was initiated in the private sector compared to military clinics (28.1% vs 16%; 18.6% vs 13.3%; and 41.2% vs 32.0%, respectively).
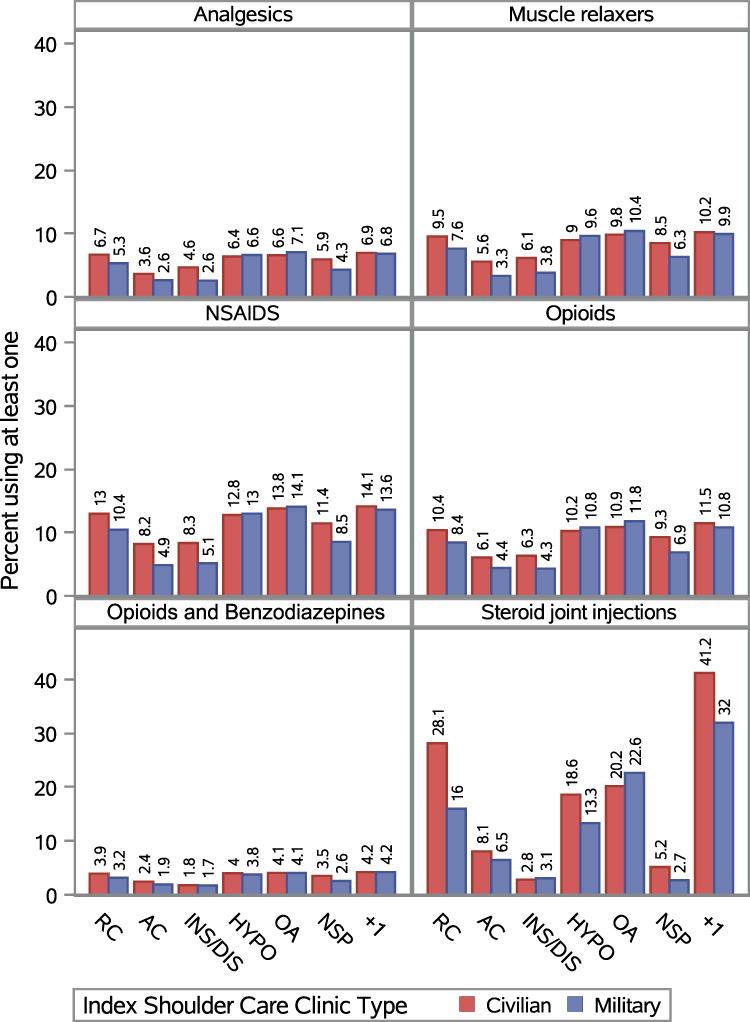 |
Figure 1 Use of pharmacologic treatments for shoulder disorders in civilian and military settings. The pharmacologic treatments were not mutually exclusive and multiple medications could have been prescribed for a single individual. |
Across all diagnostic groups, care initiated in a military clinic was more likely to consist of at least one session of a non-pharmacological treatment compared to care initiated in a private sector clinic (Figure 2). However, manual therapy was similar across both settings for Hypomobility/Adhesive capsulitis and multiple diagnoses groups. On the other hand, if care was initiated in a private sector clinic, patients were more likely to have received an advanced imaging or X-ray than if care was initiated in a military clinic (Figure 3).
 |
Figure 2 Use of non-pharmacologic treatments for shoulder disorders in civilian and military settings. The non-pharmacologic treatments were not mutually exclusive, for example, the active exercise, passive treatment, and manual therapy likely occurred within the context of a physical therapy visit. |
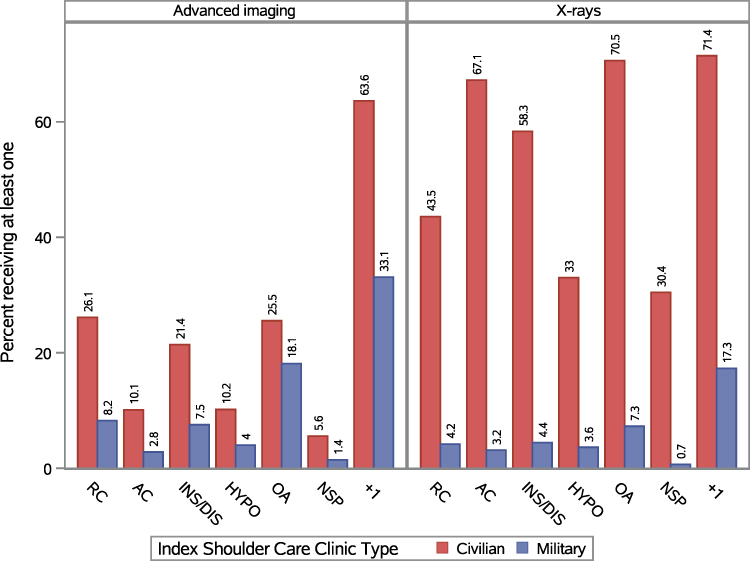 |
Figure 3 Diagnostic imaging for shoulder disorders in civilian and military settings. Diagnostic imaging categories were not mutually exclusive and multiple tests could have been received for a single individual. |
Discussion
Shoulder conditions are highly prevalent in both military and civilian populations and are a common reason to seek healthcare. This comparative analysis of shoulder diagnostic groups provided novel data on HCRU patterns that, to the best of our knowledge, had not been previously described at the health system level. For example, shoulder disorders have the highest rates of diagnostic imaging compared to competing musculoskeletal conditions, like back, knee, or neck pain;18 yet guidance for imaging decision-making is often left to expert opinion for the shoulder.19 These findings provide patients, clinicians, and policy-makers the ability to identify overall prescription rates among commonly used modalities for the management of shoulder disorders. These data may be critical to establishing benchmarks and HCRU metrics that inform the development of value-based care pathways in this population.
In this cohort, there were relatively low rates of diagnostic imaging (almost 77% of the cohort received none) and low prescription rates for opioids and steroid injections (each ≤10%). Furthermore, the variability observed in the HCRU largely coincided with what would be considered clinically appropriate for a given diagnostic group. For example, the multiple diagnoses group had the highest rates for advanced diagnostic imaging, steroid injections, and physical therapy. Relative to the other diagnostic groups, these higher rates appear justified given the multiple diagnoses group likely represents individuals with more complex cases.
There were some HCRU patterns, however, that indicated an opportunity for improvement. The limited use of acupuncture as a non-pharmacologic treatment was one notable finding, given that the treatment modality has been used to improve short-term shoulder outcomes.20 Another interesting finding is that large differences in military and civilian clinics were noted in the use of imaging, steroid injections, and physical therapy for specific diagnostic subgroups. These differences provide circumstantial evidence that system-level factors may facilitate care decisions.11,21 For example, in civilian clinics, higher reimbursement could lead to greater use of diagnostic imaging and steroid injections, while copayments could be a barrier to the use of physical therapy.
The strengths of this analysis include a large sample size of both military and civilian care recipients, likely one of the largest existing samples for shoulder disorders. This analysis also used data collected from a closed single-payer healthcare system, increasing the likelihood it represents a true reflection of actual care received. Comparisons to the existing literature are challenging because our approach investigated HCRU patterns along with increased granularity in shoulder diagnostic groups. A study by Joo et al6 described healthcare use for three different shoulder diagnostic groups (ie, adhesive capsulitis, rotator cuff syndrome, and shoulder impingement syndrome) from National Health Insurance (Korea) claims data. However, their focus was on describing the location, provider type, and cost of service making difficult direct comparisons with our cohort. Another study from Leggit et al22 assessed shoulder disorders across this same health system in fiscal year 2014. They reported 55,643 individuals that met study inclusion, with 75.3% undergoing radiological assessment and 91% being prescribed pain medications.22 However, case assessment was limited to only ICD-9 codes, and they did not investigate patterns based on diagnostic groups or differentiate between care in military versus civilian clinics. When considering these results within the context of a theoretical framework for orthopedic hospitals, our data were best aligned with one domain (provision of sustainable medical care services), while less informative for other domains (organizational management, economic, environmental, and social).23
There are some limitations to consider. First, our sample included cases from the years 2013–2019 which may not represent current practices. We intentionally chose the time frame to exclude years overlapping with the COVID pandemic because of the disruption in ambulatory care. More recent years were not yet available for analysis. Second, we used a washout period to avoid prior care seeking; but there remains a possibility these findings do not represent their true initial index shoulder visit for all patients. Another important limitation to consider when interpreting these findings is that over-the-counter medications and healthcare visits outside of civilian/military clinics may not be captured. No costs for care in the MHS versus the likely need to fund additional care out of pocket makes over the counter medication use less likely. However, due to this limitation, we cannot directly comment on any rates or differences in rates for over-the-counter medication use. Finally, medication prescriptions could not be directly linked to a diagnosis, so the shoulder disorder could not validated as the primary reason for the order.
Conclusion
This study describes the use of care for different shoulder diagnostic groups and adds to the existing literature by comprehensively describing patterns within a large health system; one of the first studies to describe care at this level of detail for this highly prevalent musculoskeletal condition. Collectively, care patterns were congruent across military and civilian clinics with notable exceptions being much higher imaging rates and steroid injection use in civilian clinics and higher physical therapy use in military clinics. These findings suggest that policies in the MHS may facilitate clinical practices that are more likely to be consistent with existing practice guidelines, especially with regard to use of imaging, steroid injection, and physical therapy. However, future research is needed in this area to determine what are the definitive or primary drivers for the care variability observed in this cohort study.
Data Sharing Statement
Data from the MDR are available publicly after execution of a Data Sharing Agreement with the US Defense Health Agency (DHA). Applications can be found at health.mil. Data that were cultivated and included in these analyses can be provided upon reasonable request from Dan Rhon ([email protected]) or Hui-Jie Lee ([email protected]), upon meeting requirements under the DHA Data Sharing Agreement.
Acknowledgment
The view(s) expressed herein are those of the author(s) and do not necessarily reflect the official policy or position of the Defense Health Agency, the Department of Defense, the Uniformed Services University, nor any agencies under the US Government.
Funding
This research was supported by the Uniformed Services University, Department of Physical Medicine & Rehabilitation, Musculoskeletal Injury Rehabilitation Research for Operational Readiness (MIRROR) program (HU00011920011).
Disclosure
Steven George reports grants from DoD/Geneva Foundation, during the conduct of the study; received honoraria and travel for the Editor in Chief role from APTA, received royalties from an online pain education course from Rehab Essentials, Inc, outside the submitted work. Sarah Morton-Oswald reports grants from Geneva Foundation, during the conduct of the study. Dr Nrupen Bhavsar reports grants from DoD/Geneva, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Picavet HSJ, Schouten JSAG. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003;102(1–2):167–178. doi:10.1016/s0304-3959(02)00372-x
2. van Hulst R, van Oostrom SH, Ostelo RWJG, Verschuren WMM, Picavet HS. Long-term patterns of chronic complaints of the arms, neck, and shoulders and their determinants--the Doetinchem Cohort Study. Pain. 2016;157(5):1114–1121. doi:10.1097/j.pain.0000000000000488
3. Huisstede BMA, Wijnhoven HA, Bierma-Zeinstra SM, Koes BW, Verhaar JA, Picavet S. Prevalence and characteristics of complaints of the arm, neck, and/or shoulder (CANS) in the open population. Clin J Pain. 2008;24(3):253–259. doi:10.1097/AJP.0b013e318160a8b4
4. Hopkins RE, Campbell G, Degenhardt L, et al. Use of pharmacological and nonpharmacological treatments for chronic noncancer pain among people using opioids: a longitudinal cohort study: a longitudinal cohort study. Pain. 2022;163(6):1049–1059. doi:10.1097/j.pain.0000000000002484
5. Kim LH, Vail D, Azad TD, et al. Expenditures and health care utilization among adults with newly diagnosed low back and lower extremity pain. JAMA Network Open. 2019;2(5):e193676. doi:10.1001/jamanetworkopen.2019.3676
6. Joo H, Lee YJ, Shin JS, et al. Medical service use and usual care of common shoulder disorders in Korea: a cross-sectional study using the health insurance review and assessment service National Patient Sample. BMJ Open. 2017;7(7):e015848. doi:10.1136/bmjopen-2017-015848
7. Roldán-Ruiz A, Bailón-Cerezo J, Falla D, Torres-Lacomba M. The prevalence of cervical contribution in patients reporting shoulder pain. An observational study. Musculoskelet Sci Pract. 2024;73(103158):103158. doi:10.1016/j.msksp.2024.103158
8. Tang L, Zhang YH, Du SH, Wang XQ. Prevalence and related factors for neck pain in military personnel: a systematic review. EFORT Open Rev. 2024;9(8):806–816. doi:10.1530/EOR-23-0150
9. Rhon DI, Greenlee TA, Fritz JM. The influence of a guideline-concordant stepped care approach on downstream health care utilization in patients with spine and shoulder pain. Pain Med. 2019;20(3):476–485. doi:10.1093/pm/pny212
10. Garcia AN, Cook CE, Rhon DI. Adherence to stepped care for management of musculoskeletal knee pain leads to lower health care utilization, costs, and recurrence. Am J Med. 2021;134(3):351–360.e1. doi:10.1016/j.amjmed.2020.08.006
11. Bradley MP, Tung G, Green A. Overutilization of shoulder magnetic resonance imaging as a diagnostic screening tool in patients with chronic shoulder pain. J Shoulder Elbow Surg. 2005;14(3):233–237. doi:10.1016/j.jse.2004.08.002
12. Lowry V, Lavigne P, Zidarov D, Matifat E, Cormier AA, Desmeules F. A systematic review of clinical practice guidelines on the diagnosis and management of various shoulder disorders. Arch Phys Med Rehabil. 2024;105(2):411–426. doi:10.1016/j.apmr.2023.09.022
13. Karel YHJM, Verkerk K, Endenburg S, Metselaar S, Verhagen AP. Effect of routine diagnostic imaging for patients with musculoskeletal disorders: a meta-analysis. Eur J Intern Med. 2015;26(8):585–595. doi:10.1016/j.ejim.2015.06.018
14. Kerns RD, Philip EJ, Lee AW, Rosenberger PH. Implementation of the veterans health administration national pain management strategy. Transl Behav Med. 2011;1(4):635–643. doi:10.1007/s13142-011-0094-3
15. Rosenberg JM, Bilka BM, Wilson SM, Spevak C. Opioid therapy for chronic pain: overview of the 2017 US Department of Veterans Affairs and US Department of Defense Clinical Practice Guideline. Pain Med. 2018;19(5):928–941. doi:10.1093/pm/pnx203
16. Rhon DI, Clewley D, Young JL, Sissel CD, Cook CE. Leveraging healthcare utilization to explore outcomes from musculoskeletal disorders: methodology for defining relevant variables from a health services data repository. BMC Med Inform Decis Mak. 2018;18(1):10. doi:10.1186/s12911-018-0588-8
17. Ranganathan P, Pramesh CS, Buyse M. Common pitfalls in statistical analysis: clinical versus statistical significance. Perspect Clin Res. 2015;6(3):169–170. doi:10.4103/2229-3485.159943
18. Haas R, Gorelik A, O’Connor DA, Pearce C, Mazza D, Buchbinder R. Patterns of imaging requests by general practitioners for people with musculoskeletal complaints: an analysis from a primary care database. Arthritis Care Res. 2025;77(3):402–411. doi:10.1002/acr.25189
19. Expert Panel on Musculoskeletal Imaging; Amini B, Beckmann NM, et al. ACR appropriateness criteria® shoulder pain-traumatic. J Am Coll Radiol. 2018;15(5S):S171–S188. doi:10.1016/j.jacr.2018.03.013
20. Zhang HN, Chen JG, Wang XY, et al. Efficacy comparison between acupuncture and other modalities in the treatment of rotator cuff diseases: meta-analysis of randomized controlled trials. Am J Transl Res. 2024;16(2):599–616. doi:10.62347/NCRJ1270
21. George SZ, Lentz TA, Goertz CM. Back and neck pain: in support of routine delivery of non-pharmacologic treatments as a way to improve individual and population health. Transl Res. 2021;234:129–140. doi:10.1016/j.trsl.2021.04.006
22. Leggit JC, Wu H, Janvrin M, Korona-Bailey J, Koehlmoos TP, Schneider EB. Non-operative shoulder dysfunction in the United States military. Mil Med. 2023;188(5–6):e1003–e1009. doi:10.1093/milmed/usab468
23. Moldovan F, Moldovan L. Fair healthcare practices in orthopedics assessed with a new framework. Healthcare. 2023;11(20):2753. doi:10.3390/healthcare11202753
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.