Back to Journals » Clinical Epidemiology » Volume 14
Healthcare Use in the Five Years Before a First Infertility Diagnosis: A Danish Register-Based Case–Control Study in the CROSS-TRACKS Cohort
Authors Ebdrup NH ![]() , Riis AH, Ramlau-Hansen CH
, Riis AH, Ramlau-Hansen CH ![]() , Bay B, Lyngsø J, Rytter D
, Bay B, Lyngsø J, Rytter D ![]() , Jørgensen MJ, Knudsen UB
, Jørgensen MJ, Knudsen UB
Received 28 January 2022
Accepted for publication 25 April 2022
Published 11 May 2022 Volume 2022:14 Pages 677—688
DOI https://doi.org/10.2147/CLEP.S360292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Ninna Hinchely Ebdrup,1– 3 Anders Hammerich Riis,4,5 Cecilia Høst Ramlau-Hansen,2 Bjørn Bay,1,6 Julie Lyngsø,7 Dorte Rytter,2 Marianne Johansson Jørgensen,4 Ulla Breth Knudsen1,3
1Department of Obstetrics and Gynecology, Fertility Clinic, Horsens Regional Hospital, Horsens, Denmark; 2Department of Public Health, Aarhus University, Aarhus, Denmark; 3Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 4Department of Research, Regional Hospital Horsens, Horsens, Denmark; 5Enversion A/S, Aarhus, Denmark; 6Maigaard Fertility Clinic, Aarhus, Denmark; 7Department of Obstetrics and Gynecology, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Ninna Hinchely Ebdrup, Department of Obstetrics and Gynecology, Fertility Clinic, Horsens Regional Hospital, Sundvej 30, Horsens, 8700, Denmark, Tel +45 28 47 21 11, Email [email protected]
Purpose: Infertility may affect somatic and mental health later in life. Nevertheless, health status before diagnosed infertility is sparsely studied in women. We aimed to describe healthcare use in primary and secondary care before a first infertility diagnosis and compare use between cases and controls.
Materials and Methods: The case–control study was based on register data and used incidence density sampling. From the CROSS-TRACKS Cohort, we included women residing in the Horsens area in Denmark in 2012– 2018 (n = 54,175). Eligible women were aged 18– 40 years, nulliparous, and living in heterosexual relationships. Cases were women with a first infertility diagnosis in the Danish National Patient Registry (index date). Five controls were matched on age, birth year, and calendar time. Through linkage to Danish national health registries, we identified general practitioner (GP) attendance, paraclinical examinations, hospital contacts, diagnoses, and redeemed prescriptions. Healthcare use from one year to five years before index date was compared with conditional logistic regression.
Results: We identified 711 cases and 3555 controls. At one year before index date, cases consulted their GP (odds ratio (OR) = 5.2, 95% confidence interval (CI): 3.2, 8.3) and visited hospital (OR = 1.2, 95% CI: 1.0, 1.4) and redeemed prescriptions (OR = 2.3 95% CI: 1.9, 2.7) more often compared to controls. Cases more often had blood and hemoglobin tests performed, redeemed more drugs related to genitourinary and hormonal diseases, and were more often diagnosed with endocrine and genitourinary diseases in the year before a first infertility diagnosis compared to controls. Cases and controls had comparable healthcare use from five years to one year before a first infertility diagnosis.
Conclusion: Cases and controls had similar healthcare use from five years to one year before a first infertility diagnosis. However, cases had a higher healthcare use in the year preceding a first infertility diagnosis compared to controls.
Keywords: behavior, health status, incidence density, fertility, preconception health, medically assisted reproduction
Introduction
One in ten women in Denmark are diagnosed as infertile or have fewer children than desired, and 10.5% of children are born after medically assisted reproduction in Denmark.1 The growing number of people needing medical assistance to become parents has led to increased interest in the health of this specific population.2–4
The reasons for pursuing fertility treatment is related to combined (25–40%) or isolated factors in the female (20–35%) or male (20–30%) and 10–15% suffer unexplained infertility.2 Reduced fecundity can be due to increasing age of family formation, known or unknown underlying diseases in the woman or man, or single women or women in same-sex partnerships desiring motherhood (who can of course also suffer biological infertility).2,5 It has been suggested that infertility can have systemic effects that may be associated with chronic morbidity or adverse events later in life.5–7 Diseases like endometriosis, polycystic ovary syndrome (PCOS), and uterine fibroids have been associated with increased risk of endocrine disorders, metabolic syndromes, and cardiovascular disease in nulliparous women.7–11 Additionally, infertility has been associated with impaired mental health.12,13
Health care use is a proxy of health status. Describing the healthcare use among women in need of fertility treatment is important to gain insight in their general health status. Women’s health prior to a diagnosis of infertility remains sparsely studied, but lower fecundity has been found in women with chronic diseases.10,11,14 Moreover, some medical drugs have been suspected to interfere with the hypothalamic-pituitary-gonadal axis and thus impair fecundity.15 The general health status of women in need of fertility treatment is of great importance since optimal mental and physical health increases the chance of having the long awaited child.16 Help-seeking for infertility is selective in many respects and may be based on social, cultural characteristics or health of the women. The medical registries made us able to identify women with an infertility diagnosis and thereby to study women referred to a fertility clinic.
The aim of the present study was to describe the use of primary and secondary care across different types of services, redeemed prescriptions, and diagnoses in women prior to a first infertility diagnosis and to compare these estimates with those obtained for their matched controls.
Materials and Methods
We conducted a nested case–control study in the CROSS-TRACKS Cohort17 with incidence density sampling design. We linked health information across national registries available in the CROSS-TRACKS Cohort by using the unique personal identification number assigned to all Danish citizens at birth or after immigration.18,19 We assessed the use of primary and secondary care before a first infertility diagnosis in women of fertile age and compared their use with the use among the matched controls for the study period from 1 September 2012 to 31 December 2018.
Study Population and Outcome
Information on the participants, including civil status, and register data on their healthcare use was available from the population-based open CROSS-TRACKS Cohort, which has been described in detail elsewhere.17 In the CROSS-TRACKS Cohort, individuals were included on their 18th birthday or when moving into the catchment area of Horsens Regional Hospital (Horsens, Odder, Skanderborg and Hedensted municipalities). Individuals were followed from the date of inclusion until the end of the study period or date of death. Individuals moving away from these municipalities were followed after the date of moving until the end of the study period or date of death. We included information for the five years prior to each individual’s date of inclusion.
We restricted the source population from CROSS-TRACKS to women at risk of infertility and named it the Horsens Fertility Cohort (HFC) (Supplemental Figure 1). The source population was restricted to nulliparous women aged 18–40 years and living in heterosexual partnerships (married or cohabiting) at the time of the index date. Marital status was obtained from the Danish Civil Registration System (CRS),19 and a cohabitant heterosexual partnership was defined as men and women with shared address and less than 15 years of age difference at the time of the index date. The definition of cohabitant partnerships was made in accordance with the similar variable (efalle) defined by Statistics Denmark.20 Nulliparity was defined as women without a birth diagnosis identified in the Danish National Patient Registry (NPR) as a main, secondary, or supplementary ICD-10 diagnosis (DO6-DO8) or home birth (RGAE04, ZLC04, ZLJ02) prior to the index date.21
The outcome of interest was a first infertility diagnosis registered at a public fertility clinic.22 During the study period, public medically assisted reproduction treatment was free of charge (tax financed) for three-six inseminations and three in vitro treatments for women aged up to 41 years having their first child. Treatment required a consultation with the woman’s general practitioner (GP), who assessed if the woman would benefit from referral to fertility treatment. Hereafter, referred women were invited to the fertility clinic in secondary care. In the study period, the time period was approximately three months from referral to first fertility consultation, where the infertility diagnosis was registered. Cases were defined as women with a first infertility diagnosis identified in the NPR in the study period.22 The NPR holds nationwide information on inpatient and outpatient hospital contacts and primary and secondary diagnoses related to each contact. In the study period, the International Classification of Diseases, 10th version (ICD-10) was used.23 In the CROSS-TRACK Cohort, the NPR data were available from 1 September 2002.17 First, we included cases on the basis of the primary infertility diagnosis (DN97 spectrum diagnoses). Second, we also identified cases as women with a secondary infertility diagnosis if the women had a relevant primary diagnosis of reproductive diseases (endometriosis, PCOS, or ovarian insufficiency) related to the same fertility contact. Third, we also identified cases as women with a relevant contact code to fertility treatment and a secondary infertility diagnosis (DN97 spectrum diagnoses) related to the same fertility contact. Women receiving treatment due to single motherhood or same-sex partnership were excluded.
By incidence density sampling, we sampled five controls for each case at the index date, matched on age, birth year, and calendar time. At the date of the first infertility diagnosis (index date), controls needed to be residents in the HFC source population and at risk of being diagnosed with infertility. The incidence sampling design allowed controls to enter the study as cases later on, and controls could be sampled again without replacement.24
Healthcare Use Prior to an Infertility Diagnosis
Healthcare use was defined as GP attendance, paraclinical examinations in general practice, redemptions of prescriptions, hospitalizations, and related diagnoses in the one year (12 months) before the index date and in the five- to one-year period preceding the last 12 months leading up to the index date.
Primary Healthcare
From the Danish National Health Service Register (DNHSR), we identified number of contacts and paraclinical examinations at the GP.25,26 We identified daytime face-to-face consultations as well as email, telephone, and on-call doctor contacts (hereinafter referred to as “all GP contacts”). The DNHSR is based on reimbursement, which ensured a high degree of coverage, but it does not provide detailed information about the reason for the contact. However, paraclinical examinations are documented in the register, and we extracted information on blood tests, hemoglobin tests, spirometry tests, electrocardiograms, urine tests, rapid strep tests and C-reactive protein tests.27
Redeemed Prescriptions
From the Danish National Database of Reimbursed Prescriptions (DNDRP), we identified the date of drug redemption and categorized the drug types into the 14 pharmacological groups in the Anatomical Therapeutic Chemical classification (ATC) system.28 Since 2004, the DNDRP has included all reimbursable prescriptions redeemed at Danish pharmacies.
Secondary Healthcare
From the Danish National Patient Registry (NPR), we identified all somatic and psychiatric hospital contacts (inpatient admissions, outpatient visits, and emergency visits), admission dates, and the associated diagnoses.21 We identified the main diagnosis registered for the contact in the NPR and classified it in accordance with the 21 chapters in the ICD-10 classification system.21,23 Chapter 16 (conditions in the perinatal period) was irrelevant to the study aim and was excluded. The NPR does not contain information from non-refundable contacts with private psychologists, which account for a minor subset of contacts.17
The electronic health record (EHR) in the Central Denmark Region records the healthcare information listed above, and these data are delivered to the NPR. Further, these data include results of clinical tests and other healthcare-related registrations which are linked with date and time.17
Covariates
Socioeconomic covariates were identified in the Danish Register for Evaluation of Marginalization (DREAM).29 DREAM holds weekly recordings of social security benefits and any other transfer incomes with full population coverage, regardless of labour market affiliation. We categorized the study population into three groups of transfer payments: no transfer payment (ie not receiving social security benefits), labour-market-related benefits, and health-related benefits.30,31 As a proxy of ethnicity, we identified citizenship, which is also available in DREAM.
Information on date of birth, gender, vital status, civil status, migration, municipality, and residential address originates from the CRS.17,19
Statistical Analysis
Using conditional logistic regression, we estimated odds ratios (ORs) and 95% confidence intervals (CIs) to compare healthcare use between cases and controls. We identified covariates related to health care a priori. The model adjusted for the matching variables of age, birth year, and calendar time, and we adjusted further for income and citizenship.
We described the frequency of “any” contacts at the GP, “any” redeemed prescription, and “any” hospital contacts (count and type) in cases and compared these estimates with the frequency among controls. Moreover, we categorized the GP contacts into tertiles on the basis of number of contacts made by the controls, which reflected the healthcare use in the source population. Further, we a priori defined three categories of number of redeemed prescriptions (0, 1–3, and ≥4) and of secondary sector contacts (0, 1–3 and ≥4).
All primary and secondary care contacts were first analyzed for the one year preceding infertility diagnosis, second for the five- to one-year period preceding infertility diagnosis, and third (in a sub-analysis) for the overall five-year period preceding an infertility diagnosis.
In secondary analyses, we estimated ORs and 95% CIs: first for having at least one paraclinical examination in each of the identified tests, second for having at least one redeemed prescription of a drug in each specific ATC group, and third for having at least one main diagnosis in each specific ICD-10 chapter.
Case and control sampling was done on a SQL server, and analyses were performed with Stata, version 15.0 (StataCorpLP, College Station, TX, USA).
Ethical Approval
No ethical approval was required for this type of study according to Danish law. The project complies with the Danish Act on Processing of Personal Data. Approval was handled by Aarhus University as Data Controller (No 2016-051-000001, project No 1374). Access to CROSS-TRACKS data was granted by the CROSS-TRACKS steering committee.
Results
Of all women of fertile age in the Horsens area, 54,174 were identified as the source population. After exclusion of women with same-sex partnerships and singles (28.8% of women with incident infertility diagnosis in the study period), 711 eligible women were included as cases and matched 1:5 with 3555 controls. Table 1 presents the matching variables and covariates for cases and controls. Cases were aged 30.9 (4.6 SD) years at the first infertility diagnosis.
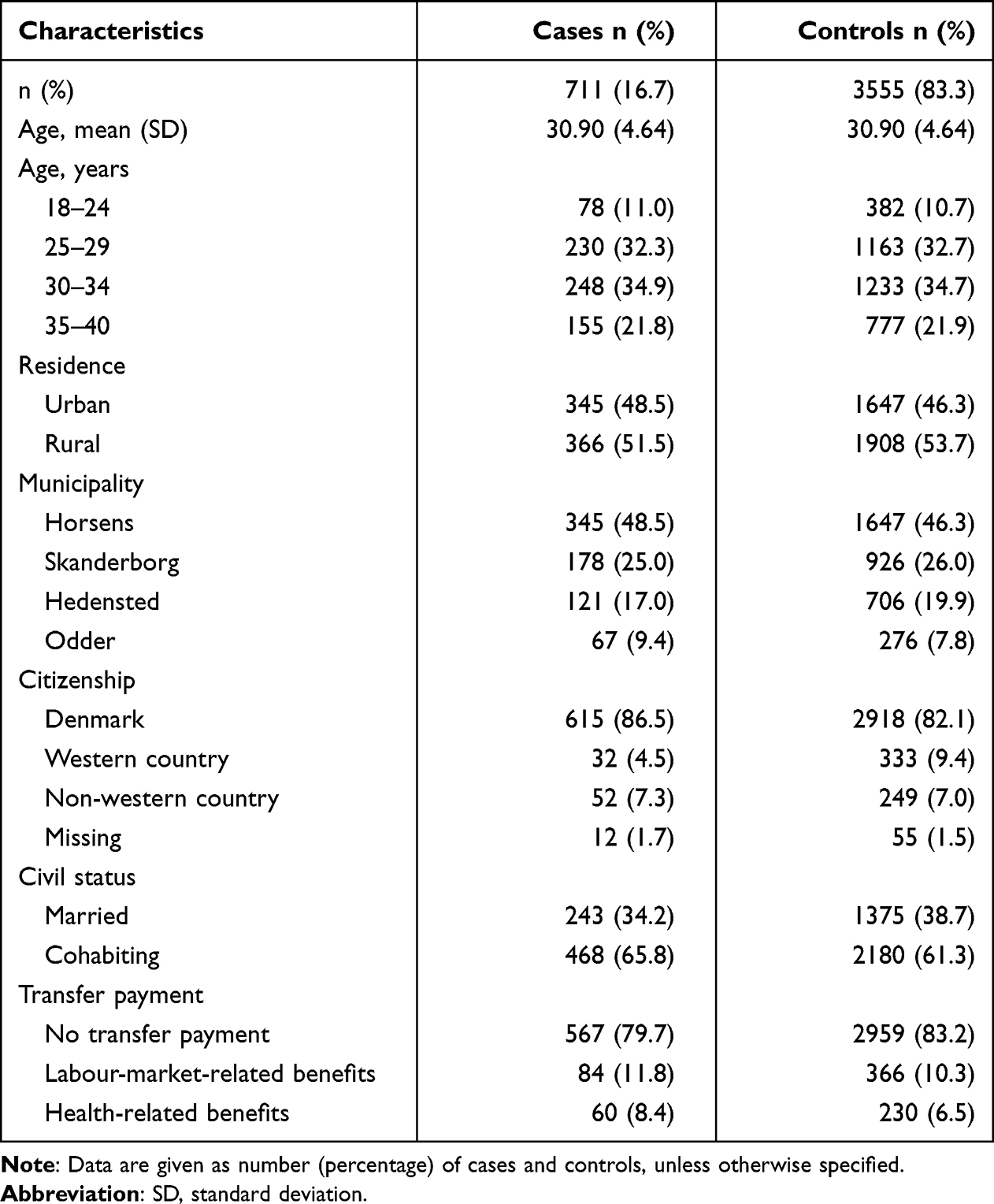 |
Table 1 Characteristics of Cases at Date of First Infertility Diagnosis (Index Date) and Matched Controls, from the CROSS-TRACKS Cohort Including Women Residing in the Horsens Area in Denmark from 1 September 2012 to 31 December 2018 |
In the year before the index date, cases were more likely to have had any contact in both primary (OR = 5.2, 95% CI: 3.2, 8.3) and secondary care (OR = 1.2, 95% CI: 1.0, 1.4) compared to controls after adjustment for age, birth year and calendar time and socioeconomic factors. Additionally, cases had more contacts to the GP (66% of cases had ≥4 face-to-face contacts compared with 44% of controls, and 52% of cases had ≥12 all GP contacts compared with 34% of controls). Cases also redeemed more prescriptions than controls (OR = 2.3 95% CI: 1.9, 2.7), with 38% of cases redeeming ≥4 prescriptions compared to 21% of controls. Moreover, cases had more inpatient and outpatient hospital visits with the exemption of emergency referrals compared to controls (Table 2).
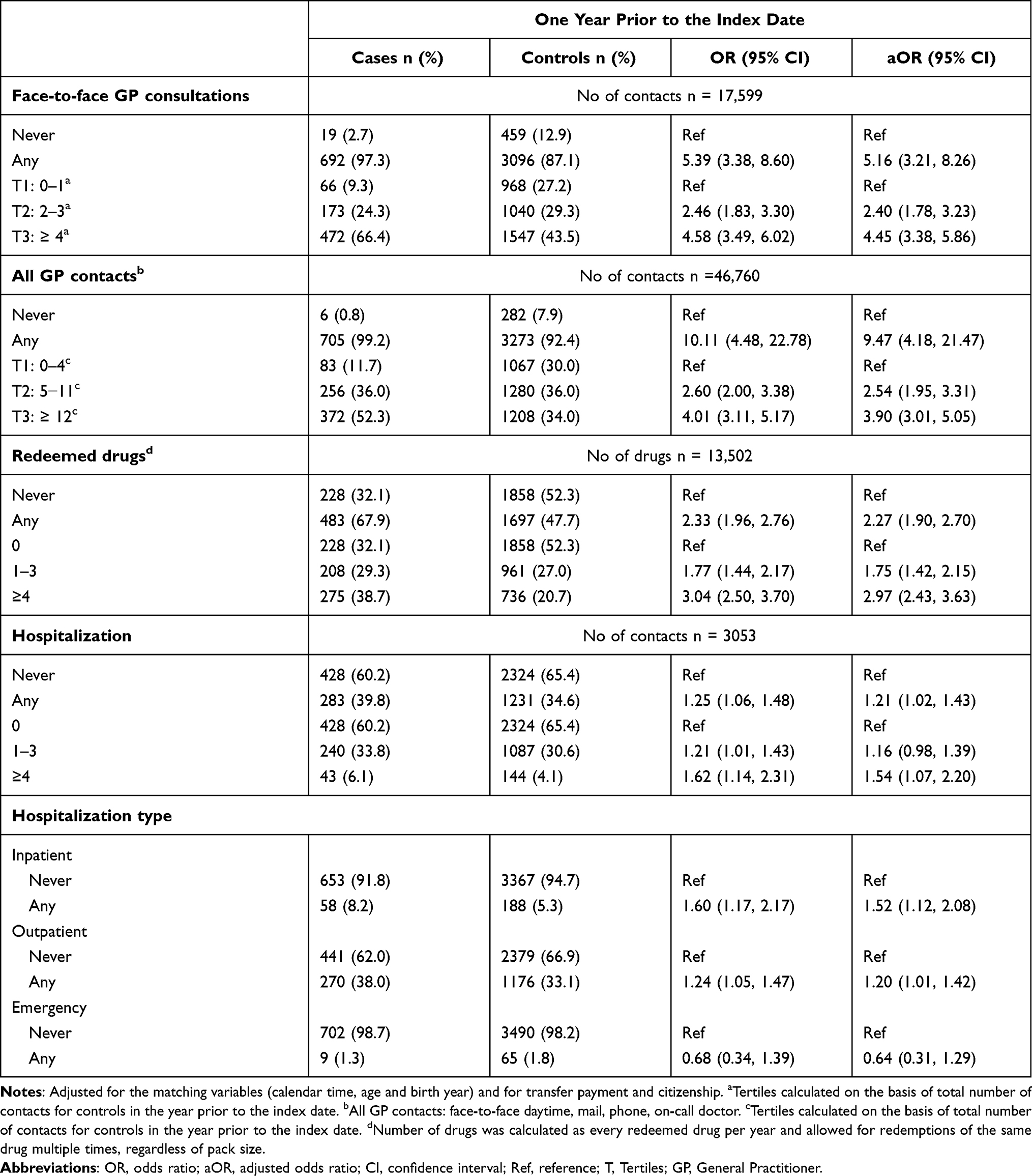 |
Table 2 Use of Primary and Secondary Healthcare for Cases and Controls in the Year Prior to the Date of First Infertility Diagnosis (Index Date) |
In the analyses performed on specific paraclinical examinations at the GP (Figure 1), cases more often had blood (OR = 3. 4, 95% CI: 2.9, 4.1) and hemoglobin tests (OR = 1.4, 95% CI: 1.1, 1.7) performed in the year preceding the index date. For redeemed prescriptions (Figure 2) in the year preceding the index date, cases were more likely to have redeemed prescriptions for drugs in ATC groups G, ie genito-urinary system, (OR = 7.2, 95% CI: 5.6, 9.1) or H, ie systemic hormones, (OR = 1.8, 95% CI: 1.3, 2.4), and controls more often redeemed prescribed drugs in ATC groups C, ie cardiovascular system, (OR = 0.5, 95% CI: 0.3, 0.9), or N, ie nervous system, (OR = 0.7, 95% CI: 0.5, 0.9). For diagnoses (Figure 3) in the year preceding the index date, cases had more often received diagnoses from ICD-10 chapters IV, ie endocrine and metabolic systems, [DE00−DE90] (OR = 3.2, 95% CI: 2.1, 4.8) or XIV, ie genitourinary system, [DN00−DN99] (OR = 2.5, 95% CI: 1.8, 3.5) compared to controls.
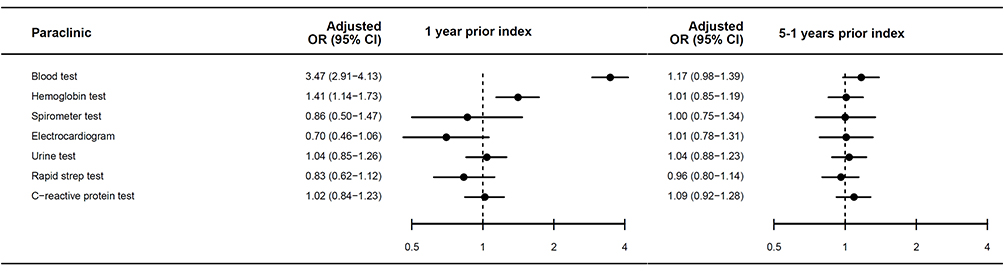 |
Figure 1 Paraclinical examinations performed at the general practitioner in the one year and five- to one- year period prior to the date of first infertility diagnosis (index date). Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; Ref, reference. Note: Adjusted for transfer payment and citizenship. |
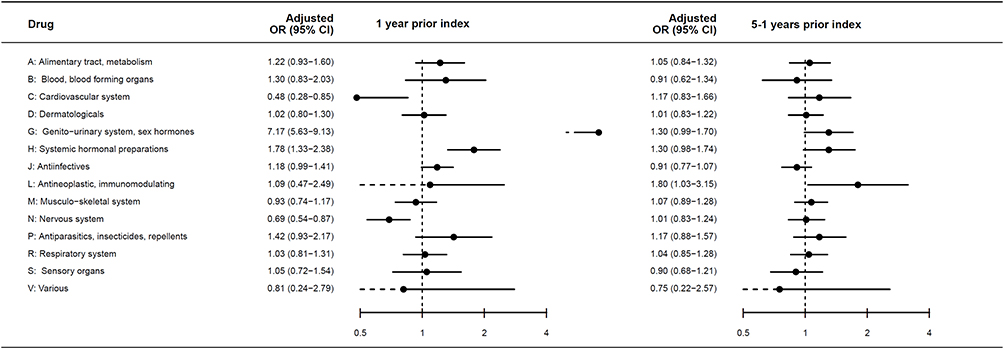 |
Figure 2 Redeemed prescriptions for drugs in specific ATC groups in the one year and five- to one-year period prior to the date of first infertility diagnosis (index date). Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; Ref, reference. Note: Adjusted for transfer payment and citizenship. |
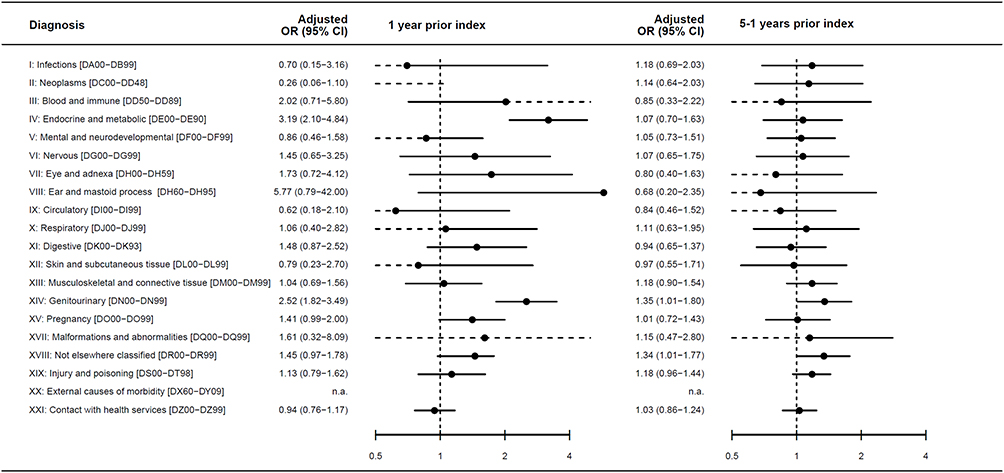 |
Figure 3 Main diagnosis of hospital contacts divided into ICD-10 chapters for the one year and five- to one-year period prior to the date of first infertility diagnosis (index date). Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; Ref, reference. Note: Adjusted for transfer payment and citizenship. ICD-10 chapter XVI (conditions in the perinatal period) was excluded due to irrelevance and missing diagnoses in accordance with the aim of the study. |
In the five- to one-period prior to the index date, the contact pattern was similar between cases and controls (Table 3). Additionally, no difference was seen for paraclinical examinations at the GP between cases and controls (Figure 1). Prescriptions of drugs in ATC group L, ie antineoplastic and immunomodulating agents, (OR = 1.8, 95% CI: 1.0, 3.2) was more often redeemed by cases in the five- to one-year period preceding the index date (Figure 2). Diagnoses from chapters XIV, ie genitourinary syndromes, [DN00−DN99] (OR = 1.4, 95% CI: 1.0, 1.8) or XVIII, ie not elsewhere classified, [DR00−DR99] (OR = 1.3, 95% CI: 1.0, 1.8) were more frequent among cases than controls (Figure 3).
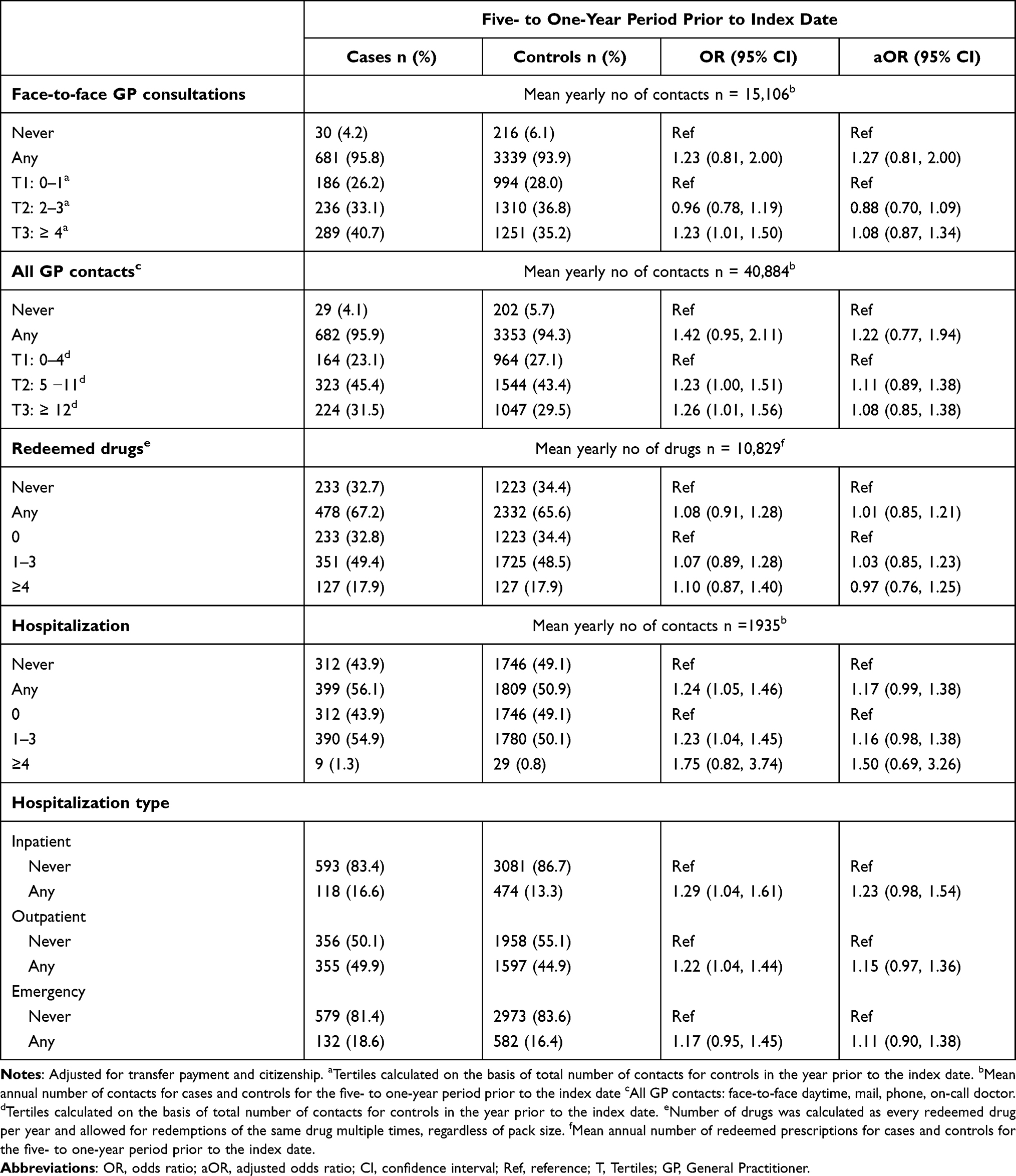 |
Table 3 Use of Primary and Secondary Healthcare for Cases and Controls in the Five- to One-Year Period Prior to the Date of First Infertility Diagnosis (Index Date) |
The results for the overall five-year period are presented in Supplemental Table 1 and reflect combined estimates for the analyses made for the one-year and the five- to one-year periods.
Discussion
Main Findings and Previous Research
Overall, women with a first infertility diagnosis had an increased number of contacts in primary and secondary care in the year prior to the index date. Cases more often redeemed prescribed drugs and were diagnosed with diseases that are known to contribute to infertility. For the five- to one-year period, there was similarity in the use of healthcare when comparing cases and controls.
We only identified few previous studies of healthcare use prior to recognized infertility. In accordance with our findings, a Danish cohort study of 42,897 women in assisted reproductive technology (ART) treatment from 1994 to 2009 found overall similar healthcare use in secondary care for women in ART treatment compared to the general population. The results showed a higher percentage of women in ART treatment with urinary and reproductive comorbidity compared to untreated women for the two- to seven-year period prior to receiving ART treatment.32
For the one year prior to a first infertility diagnosis, we found more GP visits for cases compared to controls. This could partly reflect initial diagnosing and the need for a GP consultation to be referred for fertility treatment. Controls were more likely to have redeemed prescribed drugs to treat cardiovascular and nervous system diseases compared to controls; this could indicate that controls are more likely to suffer from severe diseases, which could make engagement in family formation and fertility treatment less likely.33
In the five- to one-year period before a first infertility diagnosis, there was generally no difference in healthcare use between cases and controls. However, some specific ATC groups and diagnoses that can be associated with infertility were more frequently seen in cases compared to controls. Hence, cases redeemed more antineoplastic and immunomodulatory drugs compared to controls. Women with inflammatory bowel disease and recurrent pregnancy loss are treated with drugs belonging to this ATC group.34,35 Furthermore, we found that cases were more likely to have a diagnosis in the genitourinary spectrum and in the group of diagnoses involving diffuse symptoms, such as abdominal pain. This was, however, not statistically significant. These contacts could include women with conditions such as endometriosis, which is a chronic disorder with onset in the reproductive age and with varied pain symptoms, which often postpones the correct diagnosis.36 Comorbidity affecting female reproductive health is evidently associated with infertility because endocrine dysfunction (such as hyperthyroidism, hypothyroidism, diabetes and polycystic ovary syndrome (PCOS)) is associated with ovulatory dysfunction.15 These endocrine disorders might not be diagnosed prior to infertility in a younger population and may thus not be identified in our study. In addition, the use of hormone contraceptives can hide reproductive disorders, such as endometriosis and PCOS, up until discontinuation. Thereafter, infertility will lead to diagnosis of the underlying reproductive disease.
Strengths and Limitations
While individual diseases or comorbidities have been explored in relation to female fecundity, this study is, to the best of our knowledge, the first to describe healthcare use across primary and secondary care in women with a first infertility diagnosis and to compare it with controls. Hence, this study included both mild, severe, and chronic conditions treated in general practice as well as in hospital settings.
We gathered individual level primary and secondary care data into a complete resource from validated national registers based on a tax-funded healthcare system.18 By linkage through the unique personal identification number (CPR number), we could follow women in time, even when participants moved into or away from the municipalities in the HFC. Thus, dropout was of no concern. We sampled cases and controls from the open CROSS-TRACKS Cohort providing full follow-up of all inhabitants, which limited the risk of selection bias. The selection of controls was considered representative of the source population.
Misclassification of infertility diagnoses poses a risk of selection bias. In previous studies, fertility treatment has been found to be associated with healthy user effects due to self-selection of healthier women into fertility treatment.32 Hence, the healthcare use of the included cases might not be representative of all infertile women as some do not seek treatment and some conceive spontaneously.
In addition, women who had received fertility treatment (most likely intrauterine inseminations) at a private clinic were not registered in the NPR and therefore not included as cases. A minor proportion of potential cases might have been misclassified as controls. However, in the study area we do not expect many nulliparous women to be in self-paid private fertility treatment to the short distance to the public clinic and the fact that public fertility treatment was free of charge during the study period and the waiting time to receive treatment relatively short.
We linked information on cases and controls from the same registries. Potential differences in the coding or clinical practices in primary or secondary care was not expected to be associated with healthcare use. Potential misclassification would most likely have resulted in non-differential misclassification biasing estimates towards the null. We do not expect this potential bias to be of great concern, as we took into consideration differences over time and location by matching cases and controls by calendar time, and the source population resided in the same region of Denmark.
Some controls were expected to be pregnant during the study period and thereby to have more GP contacts as the GP is responsible for antenatal routine visits in Denmark. This would have overestimated the healthcare use for these controls and biased the estimates towards the null.
For the analyses of drug redemptions, the data from the DNDRP do not include non-refundable drugs, such as oral contraceptives, benzodiazepines, over-the-counter drugs, and medicine dispensed during hospitalization.28 It was estimated that 97% of drugs were sold in the primary health sector in 2010.28 We expected that a prescription from a medical doctor reflected a symptom or disease with limited risk of misclassification between ATC groups.
We studied healthcare use as a proxy of health status.37 The threshold for consulting a healthcare professional as well as symptom recognition and doctor–patient relations are associated with individual differences in health behavior, which is also influenced by cultural and social factors.38–40 Thus, apart from somatic and mental health, healthcare use was also expected to reflect health behavior. For some individuals, the health behavior might be associated with frequent healthcare use, whereas others might avoid healthcare use.40 We included income and citizenship in the analyses as socioeconomic factors are recognized as proxies of factors related to health behavior.38 If cases were more prone to consult their GP than controls, this might explain some of the increased contacts in primary care. Unfortunately, the DNHSR does not provide information on the cause of each GP contact, which could have helped disentangle the interplay between infertility, morbidity, and health behavior.
The GP was found to be a central healthcare professional in the year prior to a first infertility diagnosis. Cases needed to have at least one extra visit at their GP compared to controls, in accordance with the Danish guidelines on referral by the GP to fertility treatment. Overall, this was not likely to fully explain the results. Cases more often had more than four face-to-face contacts and more than 12 “all cause GP contacts” (including face-to-face, mail and telephone consultations) compared to controls. These findings could reflect a higher degree of morbidity in women with a first infertility diagnosis compared to controls. Apart from assessing if the woman needs referral to fertility treatment, the GP may also optimize her health prior to fertility treatment. Optimal health is likely to increase the treatment success rate as somatic and mental resources increase the chances of initiation and continuation of fertility treatment.16,41 Experiencing infertility is associated with both mental and physical stress, and the GP might also be a central resource in addressing some of these concerns.42,43 This might partly explain the higher number of GP consultations in cases compared to controls in the year preceding the infertility diagnosis. This hypothesis could not be investigated further, as the DNHSR did not provide information on the specific aim of the GP contact. It was therefore not possible to disentangle the fertility referral consultations and related tests from other health conditions. However, the use of secondary care and diagnoses spectrum indicated that cases did not suffer pronounced different and severe comorbidity compared to controls. Bias by individual differences in health behavior was of less concern for the secondary care results because the patient needed referral to secondary care from their GP. Therefore, the different healthcare use between cases and controls might reflect morbidity with mild severity of diseases, which are possible to treat in primary care, and/or differences in health behavior between cases and controls. It would be a fruitful area for further work to disentangle the fertility referral consultations and related tests from other health conditions in primary care.
We studied a representative sample of nulliparous women in heterosexual relationships who resided in a specific geographical area. Still, the cohort represented both rural and urban areas and contacts to both regional hospitals and university hospitals. Therefore, we expect the results to be generalizable to a national context or similar healthcare sectors, although not for the subset of women excluded due to same-sex partnerships, singles, or women >40 years.
Conclusion
Cases had more GP contacts in the year prior to the first infertility diagnosis compared to controls. This corresponds well with the fact that cases need referral from their GP to fertility treatment. However, differences in health behavior or morbidity might also explain why cases consulted their GP more often than controls. Healthcare use during the one- to five-year period prior to a first infertility diagnosis did not differentiate significantly between the two groups. In conclusion, women in need of fertility treatment did not have a high degree of comorbidity before getting the first infertility diagnosis, but they consulted their GP more often than controls.
Acknowledgments
We are thankful to the CROSS-TRACKS steering committee for initiating the project and providing access to the cohort. The funders and the CROSS-TRACKS steering committee had no influence on data collection, analyses, or results presented.
Funding
The study was supported by grants from Horsens Regional Hospital, the Health Research Foundation of the Central Denmark Region, Aarhus University, Aase and Ejnar Danielsen’s Foundation, Merck and Ferring.
Disclosure
Mr Bjørn Bay reports personal fees/lecture fee from MSD outside the submitted work. The authors report no conflicts of interest in relation to this work.
References
1. Danish Fertility Association. Annual report 2019. Danish. Available from: https://fertilitetsselskab.dk/wp-content/uploads/2020/10/dfs2019-til-hjemmesiden.pdf.
2. European Society of Human Reproduction and Embryology. ART fact sheet 2020 data 2016–2020. Available from: file:///C:/Users/au631982/Downloads/ESHRE_ARTFactSheet_2022.pdf.
3. Murugappan G, Li S, Lathi RB, Baker VL, Luke B, Eisenberg ML. Increased risk of severe maternal morbidity among infertile women: analysis of US claims data. Am J Obstet Gynecol. 2020;223:
4. Duffy JMN, Adamson GD, Benson E, et al. Top 10 priorities for future infertility research: an international consensus development study. Fertil Steril. 2021;115:180–190. doi:10.1016/j.fertnstert.2020.11.014
5. Vander Borght M, Wyns C. Fertility and infertility: definition and epidemiology. Clin Biochem. 2018;62:2–10. doi:10.1016/j.clinbiochem.2018.03.012
6. Cedars MI, Taymans SE, DePaolo LV, Warner L, Moss SB, Eisenberg ML. The sixth vital sign: what reproduction tells us about overall health. Proceedings from a NICHD/CDC workshop. Hum Reprod Open. 2017;2017:hox008. doi:10.1093/hropen/hox008
7. Christensen MW, Kesmodel US, Christensen K, Kirkegaard K, Ingerslev HJ. Early ovarian ageing: is a low number of oocytes harvested in young women associated with an earlier and increased risk of age-related diseases? Hum Reprod. 2020;35:2375–2390.
8. Senapati S. Infertility: a marker of future health risk in women? Fertil Steril. 2018;110:783–789. doi:10.1016/j.fertnstert.2018.08.058
9. Vassard D, Schmidt L, Glazer CH, Lyng Forman J, Kamper-Jorgensen M, Pinborg A. Assisted reproductive technology treatment and risk of ovarian cancer-a nationwide population-based cohort study. Hum Reprod. 2019;34:2290–2296. doi:10.1093/humrep/dez165
10. Murugappan G, Li S, Lathi RB, Baker VL, Eisenberg ML. Increased risk of incident chronic medical conditions in infertile women: analysis of US claims data. Am J Obstet Gynecol. 2019;220(473):e471–473. doi:10.1016/j.ajog.2019.01.214
11. Hanson B, Johnstone E, Dorais J, Silver B, Peterson CM, Hotaling J. Female infertility, infertility-associated diagnoses, and comorbidities: a review. J Assist Reprod Genet. 2017;34(2):167–177. doi:10.1007/s10815-016-0836-8
12. Klemetti R, Raitanen J, Sihvo S, Saarni S, Koponen P. Infertility, mental disorders and well-being–a nationwide survey. Acta Obstet Gynecol Scand. 2010;89:677–682. doi:10.3109/00016341003623746
13. Pedro J, Vassard D, Malling GMH, Hougaard C, Schmidt L, Martins MV. Infertility-related stress and the risk of antidepressants prescription in women: a 10-year register study. Hum Reprod. 2019;34:1505–1513. doi:10.1093/humrep/dez110
14. Rostad B, Schmidt L, Sundby J, Schei B. Infertility experience and health differentials - a population-based comparative study on infertile and non-infertile women (the HUNT Study). Acta Obstet Gynecol Scand. 2014;93:757–764. doi:10.1111/aogs.12404
15. Taylor HP, Sell L. Speroff’s Clinical Gynecologic Endocrinology and Infertility.
16. Crawford NM, Hoff HS, Mersereau JE. Infertile women who screen positive for depression are less likely to initiate fertility treatments. Hum Reprod. 2017;32:582–587. doi:10.1093/humrep/dew351
17. Riis AH, Kristensen PK, Petersen MG, Ebdrup NH, Lauritsen SM, Jorgensen MJ. Cohort profile: CROSS-TRACKS: a population-based open cohort across healthcare sectors in Denmark. BMJ Open. 2020;10:e039996. doi:10.1136/bmjopen-2020-039996
18. Erlangsen A, Fedyszyn I. Danish nationwide registers for public health and health-related research. Scand J Public Health. 2015;43:333–339. doi:10.1177/1403494815575193
19. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39:22–25. doi:10.1177/1403494810387965
20. Statistics Denmark. Times. Efalle (variable). Danish. Available from: https://www.dst.dk/da/Statistik/dokumentation/Times/forskningsservice/efalle.
21. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
22. Gnoth C, Godehardt E, Frank-Herrmann P, Friol K, Tigges J, Freundl G. Definition and prevalence of subfertility and infertility. Hum Reprod. 2005;20:1144–1147. doi:10.1093/humrep/deh870
23. World Health Organization. Tenth revision of the international classification of diseases and related health problems (ICD-10). Geneva: World Health Organization; 1992. Available from: https://icd.who.int/browse10/2019/en.
24. Heide-Jorgensen U, Adelborg K, Kahlert J, Sorensen HT, Pedersen L. Sampling strategies for selecting general population comparison cohorts. Clin Epidemiol. 2018;10:1325–1337. doi:10.2147/CLEP.S164456
25. Olivarius NF, Hollnagel H, Krasnik A, Pedersen PA, Thorsen H. The Danish national health service register. A tool for primary health care research. Dan Med Bull. 1997;44:449–453.
26. Andersen JS, Olivarius Nde F, Krasnik A. The Danish national health service register. Scand J Public Health. 2011;39:34–37. doi:10.1177/1403494810394718
27. Kjaersgaard MI, Vedsted P, Parner ET, et al. Algorithm linking patients and general practices in Denmark using the Danish national health service register. Clin Epidemiol. 2016;8:273–283. doi:10.2147/CLEP.S108307
28. Johannesdottir SA, Horvath-Puho E, Ehrenstein V, Schmidt S, Pedersen L, Sorensen HT. Existing data sources for clinical epidemiology: the Danish national database of reimbursed prescriptions. Clin Epidemiol. 2012;4:303–313. doi:10.2147/CLEP.S37587
29. Hjollund NH, Larsen FB, Andersen JH. Register-based follow-up of social benefits and other transfer payments: accuracy and degree of completeness in a Danish interdepartmental administrative database compared with a population-based survey. Scand J Public Health. 2007;35:497–502. doi:10.1080/14034940701271882
30. Stapelfeldt CM, Jensen C, Andersen NT, Fleten N, Nielsen CV. Validation of sick leave measures: self-reported sick leave and sickness benefit data from a Danish national register compared to multiple workplace-registered sick leave spells in a Danish municipality. BMC Public Health. 2012;12(1):661. doi:10.1186/1471-2458-12-661
31. Fonager K, Lundbye-Christensen S, Andreasen JJ, et al. Work status and return to the workforce after coronary artery bypass grafting and/or heart valve surgery: a one-year-follow up study. Rehabil Res Pract. 2014;2014:631842. doi:10.1155/2014/631842
32. Vassard D, Schmidt L, Pinborg A, et al. Mortality in women treated with assisted reproductive technology-addressing the healthy patient effect. Am J Epidemiol. 2018;187:1889–1895. doi:10.1093/aje/kwy085
33. Leonard EA, Marshall RJ. Cardiovascular disease in women. Prim Care. 2018;45:131–141. doi:10.1016/j.pop.2017.10.004
34. Druvefors E, Landerholm K, Hammar U, Myrelid P, Andersson RE. Impaired fertility in women with inflammatory bowel disease: a national cohort study from Sweden. J Crohns Colitis. 2021;15(3):383–390. doi:10.1093/ecco-jcc/jjaa191
35. Eshre Guideline Group on RPL. ESHRE guideline: recurrent pregnancy loss. Hum Reprod Open. 2018;2018:hoy004. doi:10.1093/hropen/hoy004
36. Alderman MH 3rd, Yoder N, Taylor HS. The systemic effects of endometriosis. Semin Reprod Med. 2017;35:263–270. doi:10.1055/s-0037-1603582
37. Jorgensen JT, Andersen JS, Tjonneland A, Andersen ZJ. Determinants of frequent attendance in Danish general practice: a cohort-based cross-sectional study. BMC Fam Pract. 2016;17:9. doi:10.1186/s12875-016-0412-4
38. Schuz B. Socio-economic status and theories of health behaviour: time to upgrade a control variable. Br J Health Psychol. 2017;22:1–7. doi:10.1111/bjhp.12205
39. Andersen RS, Vedsted P, Olesen F, Bro F, Sondergaard J. Does the organizational structure of health care systems influence care-seeking decisions? A qualitative analysis of Danish cancer patients’ reflections on care-seeking. Scand J Prim Health Care. 2011;29:144–149. doi:10.3109/02813432.2011.585799
40. Seibaek L, Petersen LK, Blaakaer J, Hounsgaard L. Symptom interpretation and health care seeking in ovarian cancer. BMC Womens Health. 2011;11:31. doi:10.1186/1472-6874-11-31
41. Pedro J, Sobral MP, Mesquita-Guimaraes J, Leal C, Costa ME, Martins MV. Couples’ discontinuation of fertility treatments: a longitudinal study on demographic, biomedical, and psychosocial risk factors. J Assist Reprod Genet. 2017;34:217–224. doi:10.1007/s10815-016-0844-8
42. Schmidt L. Infertility and assisted reproduction in Denmark. Epidemiology and psychosocial consequences. Dan Med Bull. 2006;53:390–417.
43. Kjaer T, Albieri V, Jensen A, Kjaer SK, Johansen C, Dalton SO. Divorce or end of cohabitation among Danish women evaluated for fertility problems. Acta Obstet Gynecol Scand. 2014;93:269–276. doi:10.1111/aogs.12317
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.