Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Healthcare Teams: Terminology, Confusion, and Ramifications
Authors Martin AK ![]() , Green TL
, Green TL ![]() , McCarthy AL
, McCarthy AL ![]() , Sowa PM
, Sowa PM ![]() , Laakso EL
, Laakso EL ![]()
Received 6 December 2021
Accepted for publication 11 March 2022
Published 8 April 2022 Volume 2022:15 Pages 765—772
DOI https://doi.org/10.2147/JMDH.S342197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Aleysha K Martin,1 Theresa L Green,2 Alexandra L McCarthy,3 P Marcin Sowa,4 E-Liisa Laakso5,6
1Faculty of Medicine, Mater Research Institute – The University of Queensland, Brisbane, QLD, Australia; 2School of Nursing, Midwifery and Social Work, The University of Queensland – MNHHS Surgical Treatment and Rehabilitation Service, Brisbane, QLD, Australia; 3School of Nursing, Midwifery and Social Work, Mater Research Institute – The University of Queensland, Brisbane, QLD, Australia; 4Centre for the Business and Economics of Health, The University of Queensland, Brisbane, QLD, Australia; 5Allied Health, Mater Research Institute – The University of Queensland, Brisbane, QLD, Australia; 6Menzies Health Institute Queensland, Gold Coast, Australia
Correspondence: Aleysha K Martin, Faculty of Medicine, Mater Research Institute – The University of Queensland, Level 2 Aubigny Place, Raymond Terrace, South Brisbane, QLD, 4101, Australia, Tel +61 457 993 248 ; +61 7 3163 2550, Email [email protected]
Abstract: One strategy to meet increasing consumer demand for healthcare services in the pandemic era has been to reorganize the healthcare workforce. This can be achieved by reorganizing healthcare teams, which are associated with improved workforce productivity and better patient outcomes. However, healthcare teams are described using numerous terminologies and labels, which has led to conceptual confusion for researchers and research users. In this paper, we explore the disparate nature of healthcare team terminology, ramifications of conceptual confusion, and we propose standardized terminology with synthesized definitions focused on characteristics of clinically based healthcare teams including unidisciplinary, multidisciplinary, interprofessional, and transdisciplinary teams.
Keywords: teamwork, unidisciplinary, multidisciplinary, interprofessional, transdisciplinary
Introduction
Many types of healthcare teams are described in the literature. Healthcare teams comprise professionals from various disciplines who enter a collaborative relationship with the patient to deliver coordinated, high-value, and patient-centered healthcare.1,2 Team-based care is well researched and associated with numerous benefits including improved patient outcomes and satisfaction, efficient use of staff time, improved staff satisfaction, and decreased monetary expenditure.3–7 At a time where healthcare services are increasingly in demand and the healthcare workforce is under pressure from current and expected pandemics, team-based care is more important than ever.3,8 As healthcare workers are experiencing increased staff absences due to infection rates, redeployment, and burnout,9,10 healthcare teams need to reflect on team processes, team member roles and scopes of practice, and adapt to new demands. However, healthcare team definitions are ambiguous, terminology is used interchangeably, and this has ramifications for healthcare teams and researchers.1,4,5,7,11,12 The disparate nature of terminology in this field was observed by the authors when conducting a scoping review on transdisciplinary teams, and one recommendation for research was to review healthcare team terminologies.13 Standardized definitions related to interprofessional education, learning, and practice were recently published in the Proposed Lexicon for the Interprofessional Field.14 In this perspectives paper, we aim to explore ramifications of conceptual confusion, extend on the aforementioned Lexicon and, based on our knowledge of the literature and our clinical experience, we propose standard terminology and characteristics of clinically based healthcare teams. By doing so, we aim to provide greater clarity when a healthcare team seeks to modify its structure and purpose.
What are the Ramifications of Conceptual Confusion?
The conceptual confusion surrounding healthcare team terminology is due to inconsistent definitions, misuse of terms, and interchangeable use of similar terms such as multidisciplinary and multiagency, or transdisciplinary, transprofessional and supra-disciplinary. In the literature the term “multidisciplinary” is often used interchangeably with “interdisciplinary”,7 and “transdisciplinary” is often mislabeled as “interdisciplinary”.12 In clinical settings, “multidisciplinary” is frequently used instead of “interprofessional”.14 For example, a definition provided by the Department of Health on “multidisciplinary case conferences” describes characteristics that are more aligned with an interprofessional team, such as communication that occurs between a minimum of three care providers and the patient to ensure care needs are met.15 It is important to explore the impact interchangeable terminology and inconsistent definitions might have for those tasked with knowledge generation (researchers) and knowledge translation (healthcare professionals).
In research, we suggest that healthcare teams have been labelled according to the author’s understanding of the evidence and definitions, local use of terminology, and ultimately, the author’s subjective choice. Labelling healthcare teams in this idiosyncratic way has compromised effectiveness of search strategies and identification of evidence.4 The result is that researchers must dedicate a significant amount of time to search databases and construct complex search strategies that still might miss relevant or key papers. Conceptual confusion is also a barrier to the translation of knowledge into clinical practice. Healthcare professionals who are unable to decipher exactly what type of healthcare team is the most valuable for their local setting might not initiate change, resulting in missed opportunities for improving workforce organization.
There are also consequences for partnerships between researchers and healthcare professionals. Such partnerships, often referred to as research co-production, allow researchers and research users to collaborate throughout the research and health service improvement processes to identify consumer needs, develop research questions, design interventions, and interpret findings.16 Research co-production in the field of team-based care becomes challenging when researchers and healthcare professionals understand and use terminology inconsistently. In research co-production, we suggest the inconsistent use of terminology could lead to misunderstandings between stakeholders, reluctance to collaborate, disagreements, and unsuccessful clinical research, translation, and implementation. We contend that the first step to addressing the conceptual confusion is synthesized and standardized definitions of healthcare teams.
Which Healthcare Team is Which?
Numerous terminologies are used to label healthcare teams. The terms observed most frequently include unidisciplinary, uniprofessional, intradisciplinary, intraprofessional, multidisciplinary, multiagency, interdisciplinary, interprofessional, interprofessional collaboration, cross-disciplinary, transdisciplinary, transprofessional, and supra-disciplinary (Table 1).1,2,6,7,11,12,17–26 These terms are used interchangeably and defined inconsistently throughout the literature. Notably, the suffixes “discipline” and “profession” are also used interchangeably despite distinct definitions where “discipline” refers to a body of scientific knowledge, and “profession” is defined as an occupation in which qualified professionals are committed to a shared vision.1
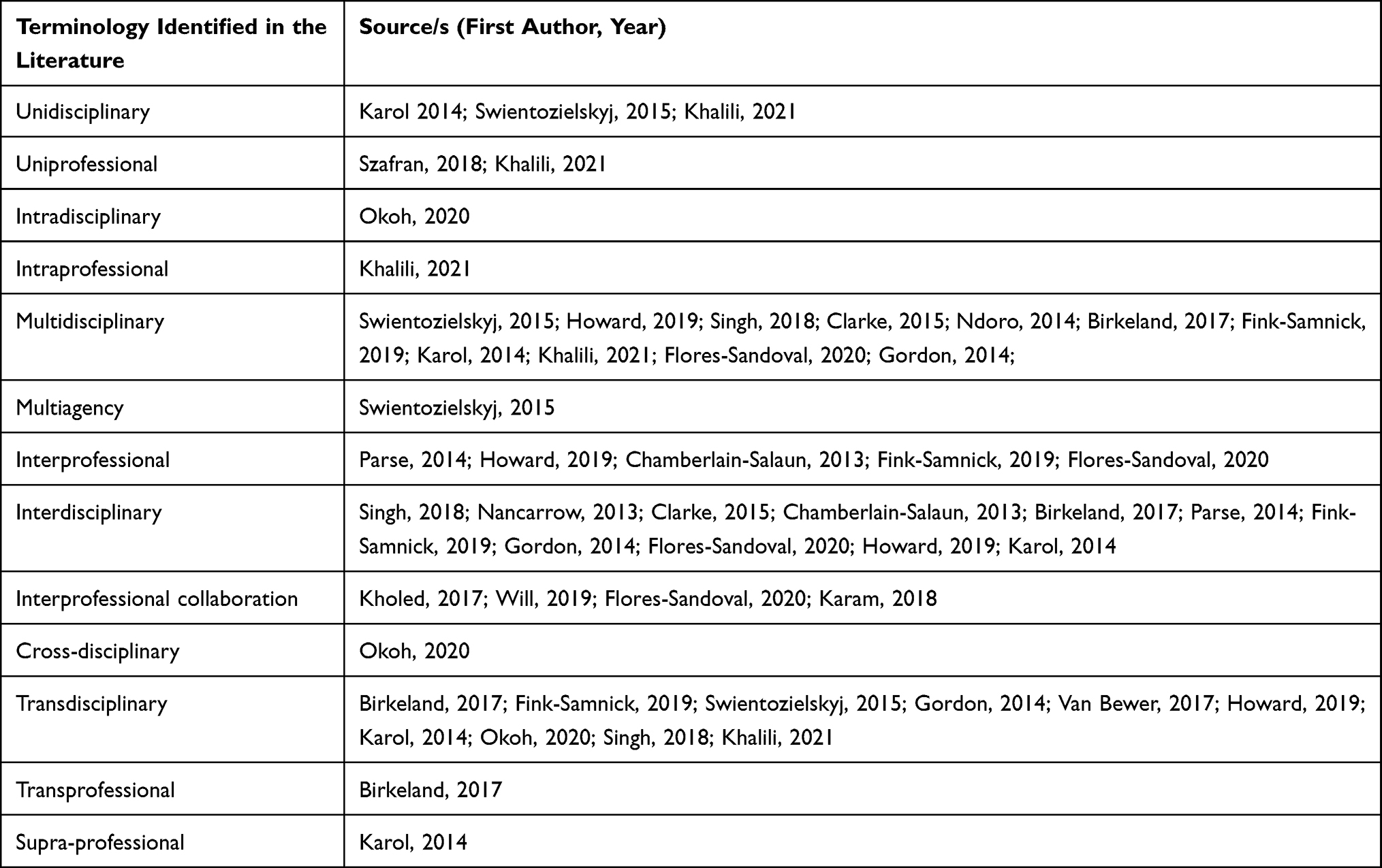 |
Table 1 Summary of Terminology and Sources |
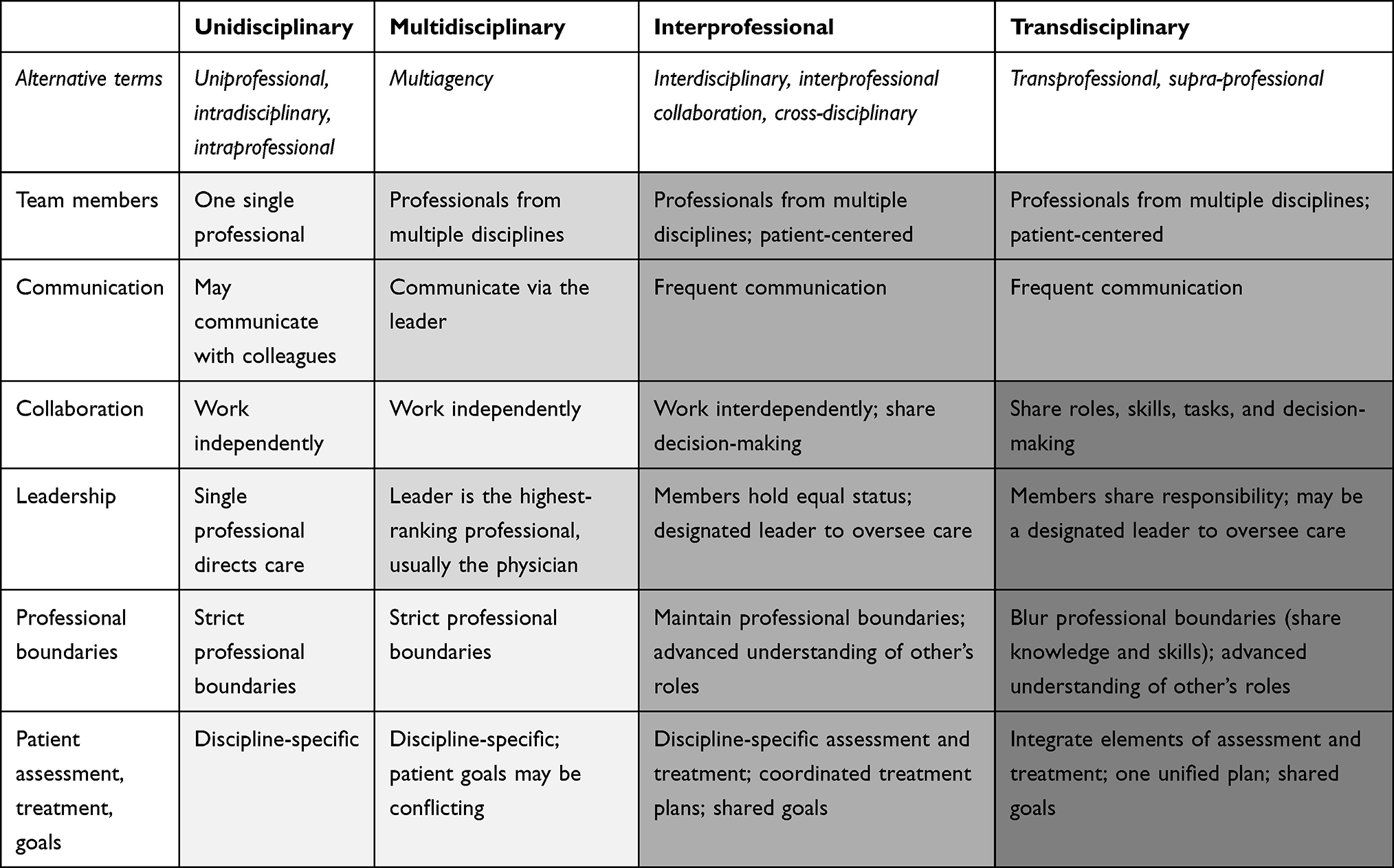 |
Table 2 Key Characteristics of Healthcare Teams |
The terms unidisciplinary and uniprofessional are used interchangeably and are generally defined as a single discipline provider of their services within a defined scope of practice.12,14,17,27 One author extends on this definition and suggests that unidisciplinary care might also involve consultation with other professionals on an already established plan.17 The latter characteristic aligns with intradisciplinary or intraprofessional teams, which involve professionals interacting within their own discipline.14,25
Multidisciplinary teams (MDTs), also referred to as multiagency teams,17 are described as having varying levels of communication. Many authors agree that MDTs frequently communicate via the physician (or the highest ranking professional), meaning that formal team meetings are not required, and other team members work in parallel or sequentially and therefore may not communicate between themselves at all.6,7,12,14,20 Conversely, some authors suggest that all MDT members collaborate, share information and skills, and develop shared patient-centered goals.19,21,22 The latter description aligns more closely with interdisciplinary teams and interprofessional teams. The composition of MDTs is described more consistently in the literature as a team of professionals from multiple disciplines, who bring a unique discipline perspective but function independently from one another.1,6,12,17,18,20,22 Many authors suggest that patient assessment, goals, and treatment are discipline-specific which, due to differing discipline perspectives represented within the team, could lead to contradictory expectations of clinician-directed goals and treatments.6,7,18
Interdisciplinary teams (IDTs) and interprofessional teams (IPTs) are considered as an extension to MDTs.1 While the terminology of IDT and IPT is often used interchangeably,23,28 Parse stated that IDTs align the resources of two or more disciplines to establish combined educational courses or projects, whereas IPTs involve professionals who combine their unique disciplinary knowledge to provide healthcare services.24
Interprofessional collaboration (IPC) is another frequently used term. Some authors use IPC synonymously with IPTs and team-based care,1,2 while others acknowledge IPC as the outcome of IPTs.26 IPC is also frequently described as having the same composition and characteristics of IDTs and IPTs, where health professionals from multiple disciplines work with patients, communicate regularly, and share goals and decision-making to deliver high-quality patient care.1–3,26
When comparing definitions, cross-disciplinary teams (CDTs) could be considered a fourth interchangeable term. CDTs are defined as teams of professionals who collaborate and have an advanced understanding of other members’ roles but maintain discipline boundaries.25 This definition matches some of the characteristics associated with IDTs and IPTs, which are frequently described to include members with different professional perspectives who work in a patient-centered, interdependent, and collaborative manner to share knowledge and decision-making, develop shared plans, and achieve common goals.6,7,12,18,20–22,28 Importantly, patient-centered care occurs when healthcare professional/s partner with the patient (or their representative) and integrate patient preferences, needs, experiences, and goals into every phase of care.29 At the extreme end of patient centered care, a patient (or their representative) could be considered as an equal team member.
For IDTs and IPTs, many authors also highlight the importance of frequent communication, formal meetings, and equality of members (including the patient or their representative).1,6,7,18,20,22,23 Descriptions regarding leadership and discipline boundaries vary between sources. While one author described shared leadership among members,23 other authors suggest IDTs and IPTs require a designated leader (who can be from any profession).7,20 In terms of discipline boundaries, some authors posit that while members have a shared understanding and acceptance of overlap inherent in their disciplines, they maintain discipline-specific roles, skills, and competencies.12,20 Yet other authors either do not acknowledge overlap in discipline boundaries,7 or have stated that IDTs and IPTs are based on discipline overlap, shared skills, and blurred roles.18,21 Blurred roles and discipline boundaries appear to be a characteristic that is more strongly associated with transdisciplinary teams.
Transdisciplinary teams (TDTs), synonymous with transprofessional or supra-disciplinary teams,12,22 are consistently described as skill-sharing or multi-skilling models where professionals from multiple disciplines blur and transcend traditional professional boundaries by exchanging knowledge and skills, blending perspectives, sharing decision-making, and integrating elements of assessment, treatment, and goal setting.6,7,11,12,17,18,22,25 Blurred professional boundaries means that team roles are re-designed, cross-training is required, and one health professional can take on the traditional role of another health professional by agreement.12,14,17,20 TDTs describe a streamlined approach to healthcare delivery, rather than replacement of professionals and their expertise. Commonly cited characteristics of TDTs include fluid role boundaries, mutual learning, communication, collaboration, trust, patient-centered care (where the patient or representative can be considered an equal member), integrated care, shared responsibility for care, and in-depth understanding of and respect for each member’s knowledge and expertise.6,7,11,12,18 However, agreement within the literature regarding training and leadership in TDTs is not as unified with few authors indicating that training staff across numerous skills is essential for TDTs,12,20 and that a leader should be appointed to oversee team discussion and care.7,25
Standardized Terminology and Definitions
Recently, a group of authors have published standardized definitions in a Proposed Lexicon for the Interprofessional Field.14 The definitions are focused on interprofessional practice and education, rather than healthcare teams working in clinical settings. Another author recommends that healthcare teams should be described every time, as a consensus on standardized definitions has not been established.28 While we acknowledge that there will be multiple opinions regarding preferred terms and defining characteristics, it is timely that standardized terms and definitions for healthcare teams are proposed for broader discussion (Table 2). Based on our knowledge of the literature and lived experience with clinical teams, the authors propose definitions for unidisciplinary, multidisciplinary, interprofessional, and transdisciplinary teams. We also recognize that healthcare teams are dynamic and propose a new term, hybrid teams. We have provided a case example that demonstrates the application of each type of healthcare team in the same clinical environment, in this instance the Emergency Department (Table 3).
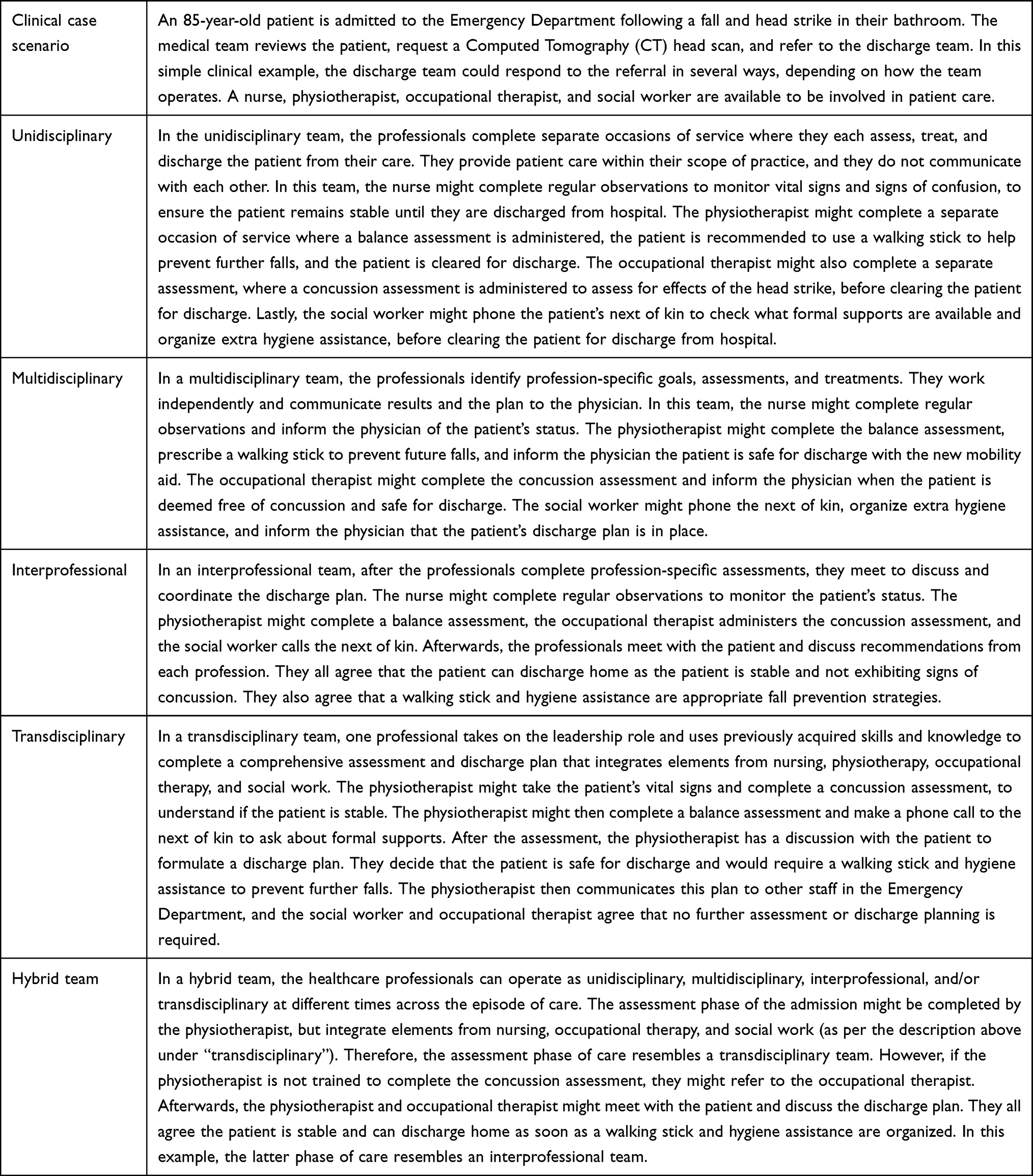 |
Table 3 Clinical Examples of Healthcare Teams |
Unidisciplinary
As the term observed most frequently in our literature search, unidisciplinary is the preferred option and encompasses alternative terms including uniprofessional, intradisciplinary, and intraprofessional. Unidisciplinary care occurs when a single professional provides healthcare only within their scope of practice. While the single professional is responsible for all aspects of patient care, consultation with other professionals might occur.
Multidisciplinary
Multidisciplinary teams comprise professionals from multiple disciplines who work independently and complete discipline-specific assessments and treatments to achieve discipline-specific and clinician-directed patient goals (that might or might not complement the work of other professionals). Each member contributes their unique discipline perspective, and all communication occurs through the highest-ranking member (usually the physician) who directs patient care. The alternate term, multiagency, should be referred to only when different healthcare professionals from different organizations come together to provide care.
Interprofessional
While the term interdisciplinary appears frequently in the literature, we suggest that interprofessional is the preferred contemporary term. Alternative terms include interprofessional collaboration and cross-disciplinary. Interprofessional teams are gaining traction alongside the trend towards interprofessional education in the education sector. Interprofessional teams consist of professionals from multiple disciplines who hold equal status (which can include the patient or their representative) and work in an interdependent, patient-centered manner. In these teams, a leader oversees care and the health professionals complete discipline-specific assessments and treatments. Members have an advanced understanding of each other’s roles and expertise, communicate frequently, share decision-making, and collaborate to establish coordinated plans and patient treatment goals. Interprofessional collaboration should be referred to as the output of interprofessional teams.
Transdisciplinary
As the term observed most frequently in literature, transdisciplinary is the preferred option, and encompasses alternative terms including transprofessional and supra-professional. Transdisciplinary teams require professionals from multiple disciplines to work beyond traditional professional boundaries (ie, complete tasks that might usually be completed by another professional), redesign roles, blend perspectives, exchange knowledge and skills, and integrate elements of assessment and treatment into one unified and patient-centered plan. In these teams, professionals hold equal status (which can include the patient or their representative), understand and respect other member’s roles, communicate frequently, trust other members, and engage in mutual learning and/or formal training. While members share responsibility, there may also be a designated leader to oversee patient care.
Hybrid Teams
The four definitions for unidisciplinary, multidisciplinary, interprofessional, and transdisciplinary teams are not intended to limit healthcare teams or provide rigid boundaries. Instead, we propose the term “hybrid teams” to describe teams that are dynamic and take on characteristics of different types of healthcare teams at different phases of healthcare provision (or at any one time).
Firstly, a hybrid team could move fluidly between the definitions, to suit local circumstances and different phases of healthcare delivery. For example, an acute stroke team might operate as a transdisciplinary team during the assessment phase, where a single clinician is available to assess neurological changes. Then during the rehabilitation phase, this healthcare team could transition to an interprofessional team, where multiple members collaborate with the patient to set a common goal (eg, return to oil painting) and commence discipline-specific treatments to meet this goal. Secondly, a hybrid team could blend characteristics of two or more definitions. For example, staff responding to a cardiopulmonary arrest code on a medical ward could communicate like a multidisciplinary team (communication occurs through the highest ranked staff member), while collaborating and sharing roles like a transdisciplinary team (any nurse, doctor, or allied health professional could be responsible for chest compressions, maintaining the patient airway, or operating the automated external defibrator).
Next Steps
Standardized terminology and definitions are the first step to addressing conceptual confusion in the field of healthcare teams. The standardized terminology and definitions proposed in this paper aim to establish common ground on which stakeholders (such as researchers and healthcare professionals) can understand one another, communicate effectively, successfully engage in research co-production and health service innovation, and contribute to knowledge generation and clinical translation. Ultimately, this should build the evidence base and support clinical implementation of healthcare teams across healthcare settings. To achieve these aims, the proposed terminology, definitions, and characteristics need to be adopted by all stakeholders. Such redesign could become more exigent as health worker numbers are affected by the current and expected pandemics. While disseminating the proposed standardized definitions is the first step, further work in this field is required. We suggest that the next steps are to 1) methodically review the healthcare team literature to build consensus, and 2) identify strategies that will support uptake of the standardized terms and definitions. Both suggestions are imperative to improve the research co-production, clinical implementation, and reporting of healthcare teams.
Abbreviations
MDT, multidisciplinary team; IDT, interdisciplinary team; IPT, interprofessional team; IPC, interprofessional collaboration; CDT, cross-disciplinary team; TDT, transdisciplinary team.
Acknowledgments
The first author received financial support for this work by the National Health and Medical Research Council (NHMRC) Postgraduate Scholarship, and The University of Queensland (UQ) Research Training Stipend. The authors wish to recognize the Mater Foundation for its generous support through the Betty McGrath Health Services Research Seeding Grant. Liza-Jane McBride provided guidance, support, and advice from a healthcare policy perspective for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flores-Sandoval C, Sibbald S, Ryan BL, Orange JB. Healthcare teams and patient-related terminology: a review of concepts and uses. Scand J Caring Sci. 2021;35(1):55–66. doi:10.1111/scs.12843
2. Will KK, Johnson ML, Lamb G. Team-based care and patient satisfaction in the hospital setting: a systematic review. J Patient Cent Res Rev. 2019;6(2):158–171. doi:10.17294/2330-0698.1695
3. Karam M, Brault I, Van Durme T, Macq J. Comparing interprofessional and interorganizational collaboration in healthcare: a systematic review of the qualitative research. Int J Nurs Stud. 2018;79:70–83. doi:10.1016/j.ijnurstu.2017.11.002
4. Sangaleti C, Schveitzer MC, Peduzzi M, Zoboli E, Soares CB. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review. JBI Database Syst Rev Implement Rep. 2017;15(11):2723–2788. doi:10.11124/JBISRIR-2016-003016
5. Reeves S, Pelone F, Harrison R, Goldman J, Zwarenstein M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6:6. doi:10.1002/14651858.CD000072.pub3
6. Fink-Samnick E. Leveraging interprofessional team-based care toward case management excellence: part 1, history, fundamentals, evidence. Prof Case Manag. 2019;24(3):130–141. doi:10.1097/NCM.0000000000000360
7. Howard I, Potts A. Interprofessional care for neuromuscular disease. Curr Treat Options Neurol. 2019;21(8):35. doi:10.1007/s11940-019-0576-z
8. Nelson S, Turnbull J, Bainbridge L, et al. Optimizing scopes of practice: new models of care for a new health care system; 2014. Available from: https://cahs-acss.ca/optimizing-scopes-of-practice-new-models-of-care-for-a-new-health-care-system/.
9. Jackson D, Bradbury-Jones C, Baptiste D, et al. Life in the pandemic: some reflections on nursing in the context of COVID-19. J Clin Nurs. 2020;29(13–14):2041–2043. doi:10.1111/jocn.15257
10. Sarabia-Cobo C, Pérez V, de Lorena P, et al. Experiences of geriatric nurses in nursing home settings across four countries in the face of the COVID-19 pandemic. J Adv Nurs. 2021;77(2):869–878. doi:10.1111/jan.14626
11. Van Bewer V. Transdisciplinarity in health care: a concept analysis. Nurs Forum. 2017;52(4):339–347. doi:10.1111/nuf.12200
12. Karol RL. Team models in neurorehabilitation: structure, function, and culture change. NeuroRehabilitation. 2014;34(4):655–669. doi:10.3233/NRE-141080
13. Martin AK, McCarthy AL, Green TL, Sowa PM, Laakso EL. Allied health transdisciplinary models of care in hospital settings: a scoping review. J Interprof Care. 2022;1–13. doi:10.1080/13561820.2022.2038552
14. Khalili H, Gilbert J, Lising D, MacMillan KM, Xyrichis A. Proposed lexicon for the interprofessional field; 2021. Available from: https://interprofessionalresearch.global/.
15. The Department of Health. Multidisciplinary case conferences. [Internet]; 2013. Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/mbsprimarycare-caseconf-factsheet.htm.
16. Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research? Health Res Policy Sys. 2019;17(1):33. doi:10.1186/s12961-019-0432-3
17. Swientozielskyj S, Nwosu A, Cooper A, et al. MDT development - working toward an effective multidisciplinary/multiagency team; 2015. Available from: https://www.england.nhs.uk/wp-content/uploads/2015/01/mdt-dev-guid-flat-fin.pdf.
18. Gordon RM, Corcoran JR, Bartley-Daniele P, Sklenar D, Sutton PR, Cartwright F. A transdisciplinary team approach to pain management in inpatient health care settings. Pain Manag Nurs. 2014;15(1):426–435. doi:10.1016/j.pmn.2013.01.004
19. Ndoro S. Effective multidisciplinary working: the key to high-quality care. Br J Nurs. 2014;23(13):724–727. doi:10.12968/bjon.2014.23.13.724
20. Singh R, Küçükdeveci AA, Grabljevec K, Gray A. The role of interdisciplinary teams in physical and rehabilitation medicine. J Rehabil Med. 2018;50(8):673–678. doi:10.2340/16501977-2364
21. Clarke DJ, Forster A. Improving post-stroke recovery: the role of the multidisciplinary health care team. J Multidiscip Healthc. 2015;8:433–442. doi:10.2147/JMDH.S68764
22. Birkeland A, Tuntland H, Forland O, Jakobsen FF, Langeland E. Interdisciplinary collaboration in reablement – a qualitative study. J Multidiscip Healthc. 2017;10:195–203. doi:10.2147/JMDH.S133417
23. Nancarrow S, Booth A, Ariss S, Smith T, Enderby R, Roots A. Ten principles of good interdisciplinary team work. Hum Resour Health. 2013;11(1):19. doi:10.1186/1478-4491-11-19
24. Parse RR. Interdisciplinary and interprofessional: What are the differences? Nurs Sci Q. 2014;28(1):5–6. doi:10.1177/0894318414558624
25. Okoh AE, Akinrolie O, Bell-Gam HI, Adandom I, Ibekaku MC, Kalu ME. Nigerian healthcare workers’ perception of transdisciplinary approach to older adults’ care: a qualitative case study. Int J Care Coord. 2020;23(2–3):92–106. doi:10.1177/2053434520954362
26. Kholed SNS, Hassan NM, Ma’on SN, Hamid NZA. Teamwork and collaboration in healthcare: elements of inter-professional teamwork. Adv Sci Lett. 2017;23(11):10834–10837. doi:10.1166/asl.2017.10164
27. Szafran O, Torti JMI, Kennett SL, Bell NR. Family physicians’ perspectives on interprofessional teamwork: findings from a qualitative study. J Interprof Care. 2018;32(2):169–177. doi:10.1080/13561820.2017.1395828
28. Chamberlain-Salaun J, Mills J, Usher K. Terminology used to describe health care teams: an integrative review of the literature. J Multidiscip Healthc. 2013;6:65–74. doi:10.2147/JMDH.S40676
29. Bokhour BG, Fix GM, Mueller NM, et al. How can healthcare organizations implement patient-centered care? Examining a large-scale cultural transformation. BMC Health Serv Res. 2018;18(1):168. doi:10.1186/s12913-018-2949-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.