")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Healthcare Simulation: A Key to the Future of Medical Education – A Review
Received 13 December 2021
Accepted for publication 25 March 2022
Published 5 April 2022 Volume 2022:13 Pages 301—308
DOI https://doi.org/10.2147/AMEP.S353777
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Omair Ayaz,1 Faisal Wasim Ismail2
1Aga Khan University Medical College, Karachi, Sindh, Pakistan; 2Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan
Correspondence: Faisal Wasim Ismail, Aga Khan University, National Stadium Road, Karachi, Sindh, 74800, Pakistan, Tel +92 21 34864607, Email [email protected]
Aim: Simulation originates from its application in the military and aviation. It is implemented at various levels of healthcare education and certification today. However, its use remains unevenly distributed across the globe due to misconception regarding its cost and complexity and to lack of evidence for its consistency and validity. Implementation may also be hindered by an array of factors unique to the locale and its norms. Resource-poor settings may benefit from diverting external funds for short-term simulation projects towards collaboration with local experts and local material sourcing to reduce the overall cost and achieve long-term benefits. The recent shift of focus towards patient safety and calls for reduction in training duration have burdened educators with providing adequate quantity and quality of clinical exposure to students and residents in a short time. Furthermore, the COVID-19 pandemic has severely hindered clinical education to curb the spread of illness. Simulation may be beneficial in these circumstances and improve learner confidence. We undertook a literature search on MEDLINE using MeSH terms to obtain relevant information on simulation-based medical education and how to best apply it. Integration of simulation into curricula is an essential step of its implementation. With allocations for deliberate practice and mastery learning under supervision of qualified facilitators, this technology is becoming essential in medical education.
Purpose: To review the adaptation, spectrum of use, importance, and resource challenges of simulation in medical education and how best to implement it according to learning theories and best practice guides.
Conclusion: Simulation offers students and residents with adequate opportunities to practice their clinical skills in a risk-free environment. Unprecedented global catastrophes provide opportunities to explore simulation as a viable training tool. Future research should focus on sustainability of simulation-based medical education in LMICs.
Keywords: simulation training, medical education, continuing education
Introduction
Simulation is defined as “the imitative representation of the functioning of one system or process by means of the functioning of another”.1 It is an activity that mimics natural phenomena without the added risk of sustaining expected consequences. The degree to which a simulation resembles reality is termed fidelity.2 Modern day simulation is used by a wide spectrum of generalist and specialist occupations for the purpose of training and certification.3 However, simulation finds its historical and utilitarian roots in the fields of military and aviation.3
Military application of simulation has long been observed in the form of war games.4 Although the cost of purchasing and maintaining sophisticated simulators in the military has grown, their advantages far outweigh their liability.5 Edward Link introduced simulation into aviation with his “Blue box” flight trainer.6 Within 50 years, simulators were formally incorporated into civil aviation to be used to certify and license pilots.3 One of many notable contributions to flight simulation is the National Aeronautics and Space Administration’s (NASA) Cockpit Resource Management principles.3 These have been adopted in healthcare to benefit intensive care, anesthesia and surgical residents today.3
Up until the 20th century, traditional apprenticeship was standard for clinical education.7 It is still used as a primary delivery vehicle in some parts of the developing world.7 Although simulation has long been established in medicine by means of anatomical models and preserved cadaveric tissue, Bradley defined three movements that paved the way for its modernization: the resuscitation movement, introduction of anesthetic simulators, and medical education reform.7 Laerdal’s Resusci-Anne, Gaba’s CASE 1.2, and Good and Gravenstein’s GAS serve as predecessors to the modern human-patient simulator.8 Medical simulators have continued to evolve rapidly in the past few decades.8
Simulation has been adopted by medical educators throughout most of the developed world.9 Although its advantages are comparable between resource contrasted settings, developing countries still struggle to employ it into mainstream use.10 This stems from misconceptions regarding its availability, range and cost, and ambiguity related to its consistency and validity.11 Because of the SARS-CoV-2 pandemic, patient interaction has been limited for students and residents to prevent spread of the disease.12 This has created a unique opportunity to help galvanize momentum towards simulation in low- to middle-income countries (LMICs).13
The aim of this literature review is to provide relevant and comprehensive information regarding the utility of simulation in medical education and use knowledge theories to determine how to best implement it in under and postgraduate medical education. We undertook a literature search on MEDLINE using MeSH terms: undergraduate medical education, postgraduate medical education, review, guidelines and simulation. Only articles in written in English were selected for further review, and preference was given to research published within the last 10 years.
The Spectrum of Healthcare Simulation (HS) in Medical Education
Gaba described 11 dimensions of the application of simulation in medical education.14 Dimension 8 categorizes simulation technology based on complexity.14 The five components of that dimension are role playing, standardized patients (SP), part-task trainers, the computer patient, and the electronic patient/virtual reality (VR).14 SPs are trained individuals who can provide a concise medical history and portray relevant physical findings for their scenario.8 They are popularly employed by medical educators throughout the globe because no technology is needed for the set-up.8 SPs can also effectively simulate a vast array of medical and ethical scenarios.8 Their validity and reliability in clinical skills assessment has led to the incorporation of SPs in examinations for licensure in Canada and the United States.11,15–17
Part-task trainers comprise a representation of only a component of the human body.7 These are frequented by subspecialties that recognize the benefit of deliberate practice to obtain mastery in technical, procedural, or psychomotor skills.7 High-fidelity simulators can exhibit multiple clinical scenarios, and they are interactive and reactive.18 Advanced part-task trainers with haptic feedback (ie, creating an experience of touch by applying force, vibration or movement in response to user operation) are being increasingly accepted in interventional and surgical training specialties such as ophthalmology and orthopedics.11 Table 1 summarises the progress of medical simulators over time.
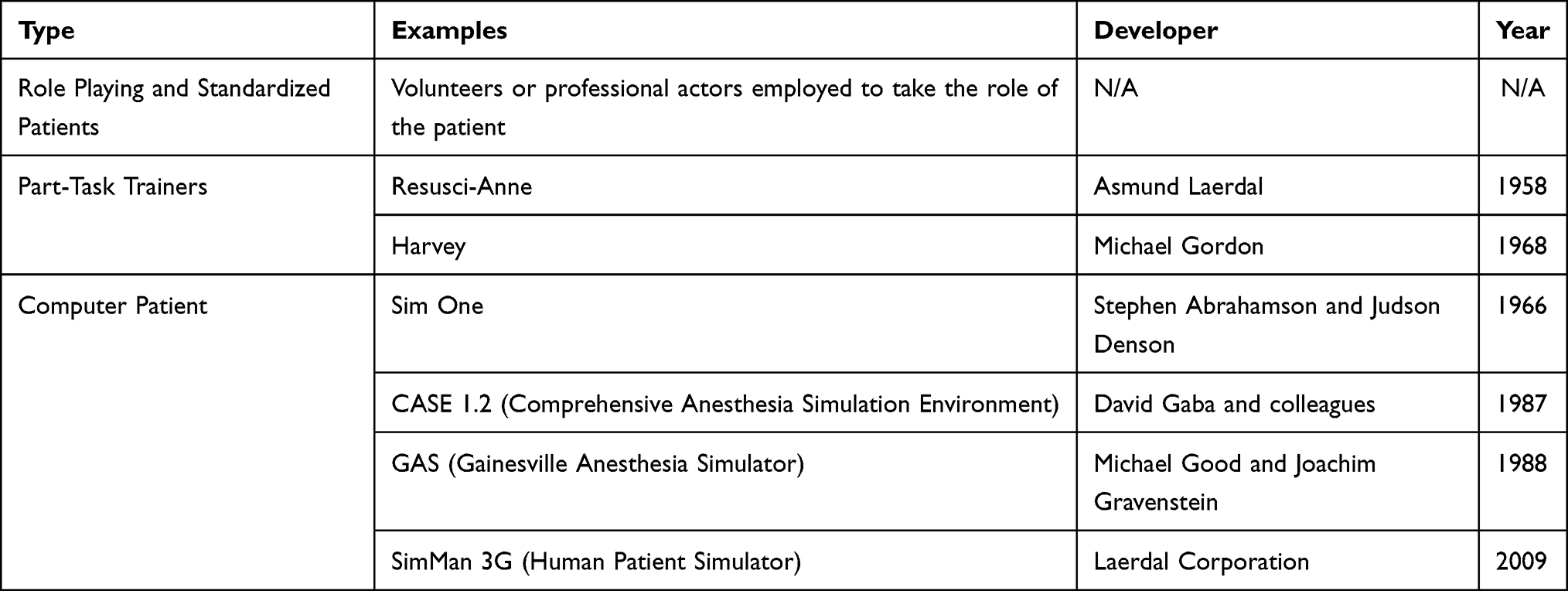 |
Table 1 The Progress of Medical Simulators |
Initial resistance to the implementation of simulation stemmed from the financial burden of training staff and maintenance of expensive technology.19 Development of simulation centers is bridging the tricky gap between educator needs and access to equipment.11 Despite the recent contributions to the gamut of simulation fidelity and cost-reduction, issues regarding its consistency and validity are the primary reason for the delay in global application.11 However, evidence for the transition of the medical training enterprise towards simulation has gathered volume in the past 2 decades.20 This is, in part, due to the growing emphasis on patient safety rather than bedside teaching.20
The Imperative to Incorporate HS in Medical Education
Medical education is intensive and extensive.21 Medical professionals are expected to be proficient and effective.21 With a rapidly changing pattern of healthcare delivery, medical students and residents face an added challenge to keep up to date with the most recent standards of care.22,23 Calls to reduce the duration of professional training and time constraints throughout the education process have the adverse effect of limiting exposure of students and residents to an adequate quality and quantity of clinical exposure.24,25
This is where simulation may flourish. It can provide all learners with an acceptable variety and number of clinical scenarios. Furthermore, exposing all participants to the same scenarios and uncommon clinical cases might allow a more standard approach to clinical curricula.2 This might also be useful downstream in potentially confronting the inadequacy and lack of preparedness felt by medical students and novice physicians in recent years.26–31
It is important to correct the perception of simulation as a universally expensive commodity. Low-fidelity simulators like SPs and part-task trainers are readily available, inexpensive, and easily implemented.8 This can ease incorporation into continued education and recertification programs without substantial impact on financial resources.2
Most medical care is now delivered by teams, and simulation is integral in improving patient safety by means of Crisis Resource Management and team training techniques.14,32 Real team training has the advantage over improvised team training because it allows for better observational learning, verbal persuasion, and heightened physiological responses borne out of member familiarity.33,34 Moreover, testing team simulation in-situ yields far more constructive results than conducting the exercise at a simulation center.33
It is also important to address the misconception that simulation is meant only to improve psychomotor skills. Studies show that simulation improves participant affective interpersonal communication and yields more empathic and adept professionals entering the workforce.35–37
The utility of simulation is in allowing participants to revisit clinical scenarios and practice skills individually and collectively as a team until competence is achieved. A new model of medical education is thus required that has patient safety at its core, avoids the flaws of a purely apprenticeship training model, and provides unlimited opportunities to practice and perfect skills in a risk-free environment.
The Challenge for Low- to Middle-Income Countries (LMICs)
HS has already become the gold standard for medical education in a vast majority of the developed world.9 The benefits of simulation-based medical education (SBME) are comparable between resource poor and resource abundant settings.10 However, the need for these benefits is far more pronounced in developing countries due to inadequate access of care.10 Using SBME to train entry-level providers, educate community workers, and bridge the gaps of understanding between healthcare providers and local populations who mistrust modern medicine may enhance the overall impact of HS.10 It may also lower the rate of preventable adverse events that are already underreported in LMICs.38
A recent literature review done by Martinerie et al showed that most studies investigating SMBE in LMICs were conducted in collaboration with international organizations.9 Indeed, most quality improvement projects launched in LMICs are reliant on external funding.38 Unit cost and operator expertise remain notable areas of concern regarding SBME implementation in resource poor settings.9 This is worsened by inadequate cost reporting in SBME research.39 Nevertheless, the availability of modern low-cost simulators could promote self-reliance in LMICs.9 This is important as it will prevent unnecessary disruptions in the continuity of SBME due to bureaucratic tribulations.40
Simulation may also be conducted online or virtually where the use of the internet or computer programs can help eliminate costs related to purchasing expensive equipment for on-site training.41–43 A study by Okrainec et al demonstrated effective use of laparoscopic telesimulation in Botswana where resident training took place through SkypeTM.42 In another study, Adhikari et al used immersive virtual reality to conduct a sepsis game for pre-registered nurses.43 Virtual reality provides three-dimensional environment that closely resembles real life.43 The experience may be enhanced with haptics that provide real-time force feedback.44 They reported a significant improvement in self-confidence and reduction in anxiety faced by the participants.43 In addition to cost reduction, these courses can be taught over several weeks using a more dispersed strategy as opposed to short intensive modules.42 However, there are limitations to these initiatives such as availability of technology, a stable internet connection, and digital literacy and confidence of users.42,43
Another challenge for LMICs is the adaptability of SBME.40 SBME is only effective if the simulations mimic realistic and relevant scenarios that account for resource limitations and disease distribution in the target setting.40 If the simulation involves rare scenarios or clinical management that is not in common practice, the overall impact of the educational activity is lost.40 Additionally, vital learner feedback during the process may be hindered by hierarchy in training structures, social and cultural norms, gender implications or language barriers.40 Since each LMIC faces different challenges, dedicated time from experts and educators is required to define clear learning objectives, establish effective delivery of feedback and evaluate the type of SBME modality to use.40
LMICs may also benefit from collaboration of local experts, institutions and manufacturers to develop and implement SBME.40 A recent study by Gheza et al has shown that overall cost of expensive medical equipment can be effectively controlled using locally sourced materials and readily available devices while yielding comparable outcomes to patented products.45 These efforts not only improve accessibility but also help increase market share for the products.46
Sound Educational Andragogy
Bioscience, sociocultural, and learning theories have been used to design frameworks that are core to HS education strategies.47 Kolb’s learning cycle is the most prominent among these theories and has been commonly used as a conceptual framework for simulation programs involving team training.48 Kolb emphasizes that transformation of experience is essential in creation of knowledge.49 His theory consists of four parts: concrete experience, reflective observation, abstract conceptualization, and active experimentation.49 Participants undergo concrete experience as they complete the simulation scenario.49 This is followed by debriefing where they reflect upon the experience and draw generalizations and conclusions from their observations to form abstract concepts.49 These concepts are then actively used to influence actions in repeat simulations.49 Active experimentation is an important but neglected step in the simulator learning process in most programs.33 This is partly due to time and resource constraints.33
Knowles’ adult learning principles of prior experience and response to problem-centered learning as opposed to content-centered learning, and Dewey’s theory of reflective thought argue that learners exhibit increased internal motivation to reflect on their performance when faced with difficult and relevant scenarios.49–51 Debriefing in a group of participants where critique is offered under the observation of trained facilitators creates an environment for individuals to reflect on their own conceptual framework (innate beliefs that guide their thinking and actions).33 According to Schön, this kind of reflection is more beneficial than reflecting-in-action during the simulation or reflecting-on-action after the simulation, which individuals usually do on their own and without peer input.52
The convergence of the behavioral, constructivist, and social cognitive learning theories makes a strong case for HS to be incorporated into medical education curricula in both developed and developing countries.53
COVID-19 and the Case for Simulation
The SARS-CoV-2 pandemic has negatively impacted the education of undergraduate and postgraduate trainees globally.12 In response to isolation and preventative requirements issued by governments worldwide, there has been a unanimous shift towards technology-based education. Medical teaching employs a two-pronged approach: learning and practice.54 Learning has been effectively delivered using online platforms during the pandemic, however the transition to a virtual setup presents its own problems.54 These include time management, lack of infrastructure and resources, poor communication, negative attitudes and student engagement.54 The opportunity for students to practice their clinical skills remains an area of concern.54,55 While the gradual transition to telemedicine and the use of prerecorded clinical encounters have been helpful, they do not provide a viable substitute for physical examinations and direct observation of skills for feedback.55 This is particularly pronounced with surgical/procedural training due to rationing of personal protective equipment and limiting of non-essential staff in operating rooms.55 With access to patients being limited, elective surgical procedures being cancelled or reduced, and a limited number of students and residents allowed to engage in care to maintain standard operating procedures, it has become evident that simulation can fill a very important niche during this unprecedented time.13 It will allow students and residents adequate exposure, time, and opportunity to learn and hone their skills.13 This may be the best time for institutions to adopt HS as a medical education strategy and prepare for future contingencies.13
The COVID-19 pandemic has also disproportionately affected vulnerable medical students such as those from developing countries and those with financially disadvantaged backgrounds.56 Although the use of technology has been effective in these developing circumstances, students in LMICs may not have access to appropriate equipment and a stable internet connection to run them.56 It is in part because of these issues that online learning is met with a poor response in the developing world.56 This makes it more important to dispel the misconception of simulation as an expensive commodity and promote the use of local manufacturing and low-cost simulation.
Implementation of HS in Medical Education
Incorporation of HS as a teaching strategy in undergraduate and postgraduate medical education curricula requires a stepwise approach.57,58 The first step is the assembly of human capital.59 Simulation, as a teaching method, requires properly trained facilitators.59 Improperly executed simulation can lead to unaccomplished objectives, poor to no learning, and disengaged or even psychologically impacted participants.2,60–63 It is extremely important for medical institutions to recognize this and provide their faculty with adequate training in the operation of healthcare simulators before planning for induction and implementation of simulation as an education strategy. Adherence to best practices during the pre-brief, the simulation itself, and the debrief (including skill sign-off) is essential in the long-term success of a simulation program.64
The next step is integration of simulation into the standard curriculum of a teaching program.57 This can be done via amalgamation of this modality into an existing curriculum or through development of new curricula.57 The process is carried out by a collaboration of the program director, content expert, and simulation expert in four phases: planning, implementation, evaluation, and revision.57 Curricular integration has the advantage of using simulators to achieve learning objectives instead of ad hoc use that only adds to the course load, without achieving palpable benefit.57
Once part of the curriculum, there should be provisions for deliberate practice.57 Coined by Ericsson in 2004, deliberate practice is the repetition of psychomotor or cognitive skills to achieve defined goals in a controlled setting.65 It is designed to provide feedback for error correction in subsequent practice until the participant displays competence and advances onto the next skill.65 Deliberate practice is a more powerful predictor of superior expert performance than clinical aptitude.66 It is also particularly useful in training for rarely performed procedures.65 Simulation is versatile in the ability to not only expand on psychomotor skills but also assist in refining trainee confidence and self-sufficiency.35–37,67
Deliberate practice is crucial in mastery learning.57 The objective of mastery learning is to achieve performance on a level higher than basic competence.57 Residents take different times to achieve mastery as they have dissimilar strengths and weaknesses.57 Each participant must meet a set standard to progress through educational units of increasing difficulty.57 Once mastery is achieved for a skill, range of difficulty and clinical variation in simulation training is increased in the case mix.57 Both need to be adjusted according to the needs of the training program.57
True learning occurs when participants are given time to achieve goals at a pace that is complementary to their learning capability. Desired outcomes can be accomplished by integrating simulation into curricula with the support of trained facilitators.
Conclusion
It is imperative that HS is adopted in undergraduate and postgraduate medical education globally. The evidence for its efficacy in adult learning is overwhelming, yet its use remains variable and opportunistic. Medical education needs to produce proficient and poised doctors for the future. Therefore, students and residents need to be provided with opportunities to practice and perfect their skills before real patient encounters. Future research priorities should focus on sustainability of simulation in LMICs and prioritize adequate and informative cost reporting. Foreign funds invested in limited and short-term simulation initiatives in developing countries should be redirected in collaboration with local experts towards more attainable and long-term projects. Unprecedented times when global healthcare is operating under extreme pressure (eg, during the COVID-19 pandemic) where patient interaction is limited provide unique opportunities to explore these areas. Strategic and integrated use of simulation is the way forward.
Funding
The authors have received no funding for this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Simulation [website on the Internet]. Merriam-Webster.com dictionary; 2021. Available from: https://www.merriam-webster.com/dictionary/simulation.
2. Fritz PZ, Gray T, Flanagan B. Review of mannequin-based high-fidelity simulation in emergency medicine. Emerg Med Australas. 2008;20(1):1–9. doi:10.1111/j.1742-6723.2007.01022.x
3. Aebersold M. The history of simulation and its impact on the future. AACN Adv Crit Care. 2016;27(1):56–61. doi:10.4037/aacnacc2016436
4. Perla PP. The Art of Wargaming: A Guide for Professionals and Hobbyists. Annapolis (MD): Naval Institute Press; 1990.
5. Strachnan IW. Technology leaps all around propel advances in simulators [website on the Internet]. National Defense Magazine; 2000. Available from: https://www.nationaldefensemagazine.org/articles/2000/10/31/2000november-technology-leaps-all-around-propel-advances-in-simulators.
6. Flight Simulator [website on the Internet]. The editors of Encyclopaedia Britannica. Encyclopedia Britannica; 2021. Available from: https://www.britannica.com/technology/flight-simulator.
7. Bradley P. The history of simulation in medical education and possible future directions. Med Educ. 2006;40(3):254–262. doi:10.1111/j.1365-2929.2006.02394.x
8. Cooper JB, Taqueti VR. A brief history of the development of mannequin simulators for clinical education and training. Postgrad Med J. 2008;84(997):563–570. doi:10.1136/qshc.2004.009886
9. Martinerie L, Rasoaherinomenjanahary F, Ronot M, et al. Health care simulation in developing countries and low-resource situations. J Contin Educ Health Prof. 2018;38(3):205–212. doi:10.1097/CEH.0000000000000211
10. Andreatta P. Healthcare simulation in resource-limited regions and global health applications. Simul Healthc. 2017;12(3):135–138. doi:10.1097/SIH.0000000000000220
11. Rosen KR. The history of medical simulation. J Crit Care. 2008;23(2):157–166. doi:10.1016/j.jcrc.2007.12.004
12. Dedeilia A, Sotiropoulos M, Hanrahan J, Janga D, Dedeilias P, Sideris M. Medical and surgical education challenges and innovations in the COVID-19 era: a systematic review. In Vivo. 2020;34(Suppl 3):1603–1611. doi:10.21873/invivo.11950
13. Tabatabai S. COVID-19 impact and virtual medical education. J Adv Med Educ Prof. 2020;8(3):140–143. doi:10.30476/jamp.2020.86070.1213
14. Gaba DM. The future vision of simulation in health care. Qual Safe Health Care. 2004;13(Suppl 1):i2–i10. doi:10.1136/qshc.2004.009878
15. Barrows HS. An overview of the uses of standardized patients for teaching and evaluating clinical skills. AAMC. Acad Med. 1993;68(6):443–451. doi:10.1097/00001888-199306000-00002
16. van der Vleuten CP, Swanson DB. Assessment of clinical skills with standardized patients: state of the art. Teach Learn Med. 1990;2(2):58–76. doi:10.1080/10401339009539432
17. Wallace P. Following the threads of an innovation: the history of standardized patients in medical education. Caduceus. 1997;13(2):5–28.
18. Gordon MS, Forker AD, Gessner I, et al. Teaching bedside cardiologic examination skills using “Harvey”, the cardiology patient simulator. Med Clin. 1980;64(2):305–313.
19. Iserson KV. Ethics of virtual reality in medical education and licensure. Camb Q Healthc Ethics. 2018;27(2):326–332. doi:10.1017/S0963180117000652
20. Okuda Y, Bryson EO, DeMaria S, et al. The utility of simulation in medical education: what is the evidence? Mt Sinai J Med. 2009;76(4):330–343. doi:10.1002/msj.20127
21. Anderson MB, Cohen JJ, Hallock JA, Kassebaum DG, Turnbull J, Whitcomb ME. Learning objectives for medical student education — guidelines for medical schools: report I of the medical school objectives project. J Assoc Am Med Coll. 1999;74(1):13–18. doi:10.1097/00001888-199901000-00010
22. Williams S, Dale J, Glucksman E, Wellesley A. Senior house officers’ work related stressors, psychological distress, and confidence in performing clinical tasks in accident and emergency: a questionnaire study. BMJ. 1997;314(7082):713–718. doi:10.1136/bmj.314.7082.713
23. McManus IC, Richards P, Winder BC. Clinical experience of UK medical students. Lancet. 1998;351(9105):802–803. doi:10.1016/S0140-6736(05)78929-7
24. Chikwe J, de Souza AC, Pepper JR. No time to train the surgeons. BMJ. 2004;328(7437):418–419. doi:10.1136/bmj.328.7437.418
25. Talbot M. Good wine may need to mature: a critique of accelerated higher specialist training. Evidence from cognitive neuroscience. Med Educ. 2004;38(4):399–408. doi:10.1046/j.1365-2923.2004.01778.x
26. Cartwright MS, Reynolds PS, Rodriguez ZM, Breyer WA, Cruz JM. Lumbar puncture experience among medical school graduates: the need for formal procedural skills training. Med Educ. 2005;39(4):437. doi:10.1111/j.1365-2929.2005.02118.x
27. Feher M, Harris-St. John K, Lant A. Blood pressure measurement by junior hospital doctors–a gap in medical education? Health Trends. 1992;24(2):59–61.
28. Maguire GP, Rutter DR. History-taking for medical students. Lancet. 1976;308(7985):556–558. doi:10.1016/S0140-6736(76)91804-3
29. Ramani S, Ring BN, Lowe R, Hunter D. A pilot study assessing knowledge of clinical signs and physical examination skills in incoming medicine residents. J Grad Med Educ. 2010;2(2):232–235. doi:10.4300/JGME-D-09-00107.1
30. Mann KV. Theoretical perspectives in medical education: past experience and future possibilities. Med Educ. 2011;45(1):60–68. doi:10.1111/j.1365-2923.2010.03757.x
31. Jilg S, Möltner A, Berberat P, Fischer MR, Breckwoldt J. How do supervising clinicians of a university hospital and associated teaching hospitals rate the relevance of the key competencies within the CanMEDS roles framework in respect to teaching in clinical clerkships? GMS Z Med Ausbild. 2015;32(3):Doc33. doi:10.3205/zma000975
32. Kohn LT, Corrigan J, Donaldson MS. To Err is Human: Building a Safer Health System. Washington (DC): National Academy Press; 2009.
33. Stocker M, Burmester M, Allen M. Optimisation of simulated team training through the application of learning theories: a debate for a conceptual framework. BMC Med Educ. 2014;14(1):69. doi:10.1186/1472-6920-14-69
34. Bandura A. Social Foundations of Thought and Action: Social Cognitive Theory.
35. Bry K, Bry M, Hentz E, et al. Communication skills training enhances nurses’ ability to respond with empathy to parents’ emotions in a neonatal intensive care unit. Acta Paediatr. 2016;105(4):397–406. doi:10.1111/apa.13295
36. Blackmore A, Kasfiki EV, Purva M. Simulation-based education to improve communication skills: a systematic review and identification of current best practice. BMJ Simul Technol Enhanc Learn. 2017;4(4):159–164. doi:10.1136/bmjstel-2017-000220
37. MacLean S, Kelly M, Geddes F, Della P. Use of simulated patients to develop communication skills in nursing education: an integrative review. Nurse Educ Today. 2017;48:90–98. doi:10.1016/j.nedt.2016.09.018
38. Puri L, Das J, Pai M, et al. Enhancing quality of medical care in low income and middle income countries through simulation-based initiatives: recommendations of the Simnovate Global Health Domain Group. BMJ Simul Technol Enhanc Learn. 2017;3:S15–S22. doi:10.1136/bmjstel-2016-000180
39. Zendejas B, Wang AT, Brydges R, Hamstra SJ, Cook DA. Cost: the missing outcome in simulation-based medical education research: a systematic review. Surgery. 2013;153:160–176. doi:10.1016/j.surg.2012.06.025
40. Yin Mar OO, Nataraja RM. The application of simulation-based medical education in low- and middle-income countries; the Myanmar experience. Semin Pediatr Surg. 2020;29(2):150910. doi:10.1016/j.sempedsurg.2020.150910
41. Bediang G, Bagayoko CO, Raetzo MA, Geissbuhler A. Relevance and usability of a computerized patient simulator for continuous medical education of isolated care professionals in sub-saharan Africa. Stud Health Technol Inform. 2011;169:666–670.
42. Okrainec A, Henao O, Azzie G. Telesimulation: an effective method for teaching the fundamentals of laparoscopic surgery in resource-restricted countries. Surg Endosc. 2010;24(2):417–422. doi:10.1007/s00464-009-0572-6
43. Adhikari R, Kydonaki C, Lawrie J, et al. A mixed-methods feasibility study to assess the acceptability and applicability of immersive virtual reality sepsis game as an adjunct to nursing education. Nurse Educ Today. 2021;103:104944. doi:10.1016/j.nedt.2021.104944
44. Rangarajan K, Davis H, Pucher PH. Systematic review of virtual haptics in surgical simulation: a valid educational tool? J Surg Educ. 2020;77(2):337–347. doi:10.1016/j.jsurg.2019.09.006
45. Gheza F, Oginni FO, Crivellaro S, Masrur MA, Adisa AO. Affordable laparoscopic camera system (ALCS) designed for low- and middle-income countries: a feasibility study. World J Surg. 2018;42(11):3501–3507. doi:10.1007/s00268-018-4657-z
46. Zimmermann M, Adamson B, Lam-Hine T, Rennie T, Stergachis A. Assessment tool for establishing local pharmaceutical manufacturing in low- and middle-income countries. Int J Pharm Pract. 2018;26(4):364–368. doi:10.1111/ijpp.12455
47. Hodges BD, Kuper A. Theory and practice in the design and conduct of graduate medical education. Acad Med. 2012;87(1):25–33. doi:10.1097/ACM.0b013e318238e069
48. Yardley S, Teunissen PW, Dornan T. Experiential learning: AMEE guide no. 63. Med Teach. 2012;34(2):e102–15. doi:10.3109/0142159X.2012.650741
49. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development.
50. Knowles MS, Nadler L, Nadler Z. Andragogy in Action: Applying Modern Principles of Adult Learning. San Francisco (CA): Jossey-Bass; 1985.
51. Miettinen R. The concept of experiential learning and John Dewey’s theory of reflective thought and action. Int J Lifelong Educ. 2000;19(1):54–72. doi:10.1080/026013700293458
52. Schön DA. Educating the Reflective Practitioner: Toward a New Design for Teaching and Learning in the Professions.
53. McGaghie WC, Harris IB. Learning theory foundations of simulation-based mastery learning. Simul Healthc. 2018;13(3SSuppl 1):S15–20. doi:10.1097/SIH.0000000000000279
54. Nimavat N, Singh S, Fichadiya N, et al. Online medical education in India–different challenges and probable solutions in the age of COVID-19. Adv Med Educ Pract. 2021;12:237–243. doi:10.2147/AMEP.S295728
55. Dedeilia A, Sotiropoulos MG, Hanrahan JG, Janga D, Dedeilias P, Sideris M. Medical and surgical education challenges and innovations in the COVID-19 era: a systematic review. In Vivo. 2020;34(3 Suppl):1603–1611.
56. Sharma D, Bhaskar S. Addressing the COVID-19 burden on medical education and training: the role of telemedicine and tele-education during and beyond the pandemic. Front Public Health. 2020;8:589669. doi:10.3389/fpubh.2020.589669
57. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE guide no. 82. Med Teach. 2013;35(10):e1511–e1530. doi:10.3109/0142159X.2013.818632
58. INACSL Committee. INACSL standards of best practice: SimulationSM Simulation design. Clin Simul Nurs. 2016;12(S):5–12. doi:10.1016/j.ecns.2016.09.005
59. INACSL Standards Committee. INACSL standards of best practice: SimulationSM: operations. Clin Simul Nurs. 2017;13(12):681–687. doi:10.1016/j.ecns.2017.10.005
60. Anderson LW, Krathwohl DR, editors. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives. Boston (MA): Allyn & Bacon; 2001.
61. Kolbe M, Grande B, Spahn DR. Briefing and debriefing during simulation-based training and beyond: content, structure, attitude and setting. Best Pract Res Clin Anaesthesiol. 2015;29(1):87–96. doi:10.1016/j.bpa.2015.01.002
62. Rudolph JW, Raemer DB, Simon R. Establishing a safe container for learning in simulation. Simul Healthc. 2014;9(6):339–349. doi:10.1097/SIH.0000000000000047
63. Der Sahakian G, Alinier G, Savoldelli G, Oriot D, Jaffrelot M, Lecomte F. Setting conditions for productive debriefing. Simul Gaming. 2015;46(2):197–208. doi:10.1177/1046878115576105
64. INACSL Standards Committee. INACSL standards of best practice: simulationSM debriefing. Clin Simul Nurs. 2016;12(S):21–25. doi:10.1016/j.ecns.2016.09.008
65. Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(Suppl 10):S70–81. doi:10.1097/00001888-200410001-00022
66. Ericsson KA. The influence of experience and deliberate practice on the development of superior expert performance. In: Ericsson KA, Hoffman RR, Kozbelt A, Williams AM, editors. The Cambridge Handbook of Expertise and Expert Performance. Cambridge (UK): Cambridge University Press; 2006:683–704.
67. Silberman NJ, Litwin B, Panzarella KJ, Fernandez-Fernandez A. High fidelity human simulation improves physical therapist student self-efficacy for acute care clinical practice. J Phys Ther Educ. 2016;30(1):14–24. doi:10.1097/00001416-201630010-00003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.