")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Healthcare-Seeking Delays in Acute Ischemic Stroke Patients: The Influence of Gender, Immigrant Status, and Educational Background
Authors Jiang Y , Xiong Y, Chi Y, Lin F, Zhao Q, Li Y
Received 30 October 2023
Accepted for publication 16 January 2024
Published 18 January 2024 Volume 2024:17 Pages 191—204
DOI https://doi.org/10.2147/RMHP.S445001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Youli Jiang, Yao Xiong, Yue Chi, Fu Lin, Qingshi Zhao, Yanfeng Li
Department of Neurology, People’s Hospital of Longhua, Shenzhen, 518109, People’s Republic of China
Correspondence: Qingshi Zhao; Yanfeng Li, Email [email protected]; [email protected]
Purpose: Timely medical attention is crucial for patients with Acute Ischemic Stroke (AIS), as delays can significantly impact therapeutic outcomes. These delays are influenced by a combination of socio-cultural, educational, and clinical factors.
Patients and Methods: An in-depth analysis was conducted to assess the prevalence and median duration of healthcare-seeking delays in AIS patients. The study specifically investigated the independent impacts of sociocultural and clinical determinants on these delays, with a focus on immigrant status, gender disparities, and educational levels. Multivariate regression analysis was employed to identify these independent effects while controlling for potential confounding factors.
Results: Among 1419 AIS patients, 82.52% (n = 1171) experienced delays exceeding 2 hours from symptom onset of symptoms to hospital arrival. The median delay was 12.3 hours. Immigrant populations encountering longer delays compared to native groups. Younger males (< 45 years) and elderly females were more prone to delay in healthcare-seeking. Identified independent risk factors for delay included male gender (OR = 1.65 [95% CI:1.14− 2.48]), self-acknowledged diabetes (OR = 2.50 [95% CI:1.21– 5.17]), small vessel (OR = 2.07 [95% CI:1.27– 3.36]), and wake stroke (OR = 7.04 [95% CI:3.69– 13.44]). Educational background (high school and above), GCS score with 3– 8 points (OR = 0.52 [95% CI:0.09– 0.69]), understanding stroke-related knowledge (OR = 0.26 [95% CI:0.09– 0.44]), conscious disturbance (OR = 0.25 [95% CI:0.10– 0.62]) and limb weakness (OR=0.21[95% CI:0.21– 0.49]) are protective factors for timely treatment.
Conclusion: Immigrant populations experienced longer delays from symptom onset to hospital arrival. The crucial roles of education and knowledge about stroke underscore the need for enhanced health literacy campaigns and public awareness, with a targeted focus on younger males and elderly females.
Keywords: healthcare-seeking behavior, immigrant population, educational disparity, pre-hospital delay, AIS
Introduction
Stroke is the second leading cause of death globally, and its incidence is rapidly increasing, especially in developing countries such as China, which accounts for more than one-fifth of the world’s population.1 Among the diverse stroke subtypes, acute ischemic stroke (AIS) is the most common, accounting for the majority of stroke cases globally and in China. Its significant morbidity and mortality rates emphasize the pressing need for timely intervention and management.2 Intravenous thrombolysis has shown profound efficacy in averting fatalities and minimizing irreversible brain damage when administered promptly post-disease onset. However, any delay in treating AIS, even a brief one, magnifies the risk of complications and can be life-threatening.3 Despite the known benefits of timely thrombolysis, only 7.3% of AIS patients receive the treatment within the crucial <4.5-hour window,4 underscoring the importance of expediting hospital arrival and minimizing healthcare-seeking delay.
The Chinese Stroke Prevention Program Committee (CSPPC) sets a benchmark for healthcare delay in AIS patients at 3 hours: this includes up to 2 hours from symptom onset to emergency room arrival and an additional hour from reaching the emergency room to initiating treatment (in-hospital delay).5 Existing research highlights a global concern regarding healthcare-seeking delays, with AIS patients often postponing medical consultations.6 Specifically, 54% of stroke patients do not seek immediate medical attention post symptom onset, with the average duration ranging between 38 minutes to 4 hours before they consult a doctor.7 Such delays are also prevalent in China, often exceeding those observed in both developed countries and some developing nations. For instance, the median healthcare delay in China’s Northeast and Western regions is approximately 15 hours, compared to 7.9 hours in South Korea.8 However, in Shenzhen, a city with a significant immigrant population and located in the rapidly growing Guangdong-Hong Kong-Macao Greater Bay Area, there’s a a notable gap in research reporting healthcare-seeking delay among patients in Shenzhen.
Factors influencing pre-hospital healthcare delay in stroke patients include not only sociodemographic attributes, such as education, family income and health insurance status,9,10 but also clinical aspects like the nature of initial symptoms, history of underlying illnesses, and timing of symptom onset.11,12 Systematic reviews further identify key determinants such as emergency medical service activation, ambulance usage, and regional strategies to mitigate geographical distances to Stroke Units.13 Additionally, factors like atypical or milder symptoms, socioeconomic status, and advanced age are associated with longer onset-to-needle times.14,15 These insights highlight the complexity of delays, influenced by a combination of individual, clinical, and regional factors, alongside broader sociocultural contexts. Given the significant impact of gender, education, and immigrant status, as indicated in the title, our study endeavors to explore these aspects in the context of medical delays. We anticipate that the outcomes will shed light on these three pivotal factors, providing empirical insights vital for designing targeted interventions and shaping future strategic planning.
Materials and Methods
Study Design and Participants
In our retrospective analysis, we centered our focus on Shenzhen, a pivotal city within the Hong Kong-Macao-Guangdong Greater Bay Area, renowned for its meteoric economic growth. As of the 2022 census, Shenzhen boasts a population of approximately 17.68 million, with over 12 million being migrants.16 This unique demographic composition not only makes Shenzhen a representative microcosm of the Greater Bay Area but also mirrors the demographic dynamics of other major Chinese cities. The foundation of our research was built on data obtained from the Shenzhen Stroke Follow-up System Platform (SSFS) covering the period from December 2021 to August 2023. The SSFS is a comprehensive database meticulously tracking the progress of AIS patients from symptom onset through to post-discharge evaluations. The platform is managed by a dedicated team of professionals, ensuring the accuracy and reliability of the collected data.
Inclusion and Exclusion Criteria
Inclusion Criteria: 1) Patients who have been included in the follow-up platform from December 2021 onwards; 2) Patients diagnosed with AIS, confirmed through diagnostic tools including but not limited to CTA and MRI; 3) Individuals who can provide verifiable identity data to ensure authenticity of patient data; 4) Patients who are aged 18 years and above. Exclusion Criteria: 1) Cases that do not conform to the AIS diagnostic criteria or are diagnosed with conditions other than AIS; 2) Entries with duplicate patient IDs, which could arise due to system glitches, human error, or other factors leading to multiple data entry; 3) Data sets that are incomplete, ambiguous, or do not provide comprehensive information required for the study.
Definition of Healthcare Seeking Delay
Conforming to the benchmarks established by the Stroke Prevention Planning Committee of China, each crucial phase from the onset of stroke symptoms to calling for help, from making the call to arriving at the hospital, and from being admitted to the initiation of treatment should ideally not exceed 1 hour.5 Drawing from these standards, our research defines “healthcare seeking delay” as the duration that extends beyond 2 hours from when symptoms first manifest to the moment a patient is admitted to the hospital.
Variables
Informed by an comprehensive literature review and insights from the neurology expert panel, we meticulously compile an exhaustive list of potential risk factors that could influence healthcare-seeking delay in AIS patients. These factors encompass: gender, age, ethnicity, residency status, living situation, health insurance status, educational background, and lifestyle habits (smoking, drinking); patient health awareness including understanding of stroke-related knowledge, acknowledgement of personal health conditions such as hypertension (HBP) and diabetes mellitus (DM), engaging in self-medication prior to hospitalization; and clinical details encompassing the mode of transportation to the hospital, modified Rankin Scale (mRS) score prior to symptom onset, National Institutes of Health Stroke Scale (NIHSS) score, Glasgow Coma Scale (GCS) score, in-hospital mRS score, electrocardiogram results, Trial of Org 10,172 in Acute Stroke Treatment (TOAST) classification, presence of medical conditions (valvular heart disease, coronary artery disease, etc.), initial symptoms (dizziness, conscious disturbance, weakness, etc.).
Statistical Analysis
We statistically analyzed the data using Python 3.9. Healthcare seeking delay durations were depicted using median values. Continuous variables were represented as either median (interquartile range [IQR]) or mean ± standard deviation (SD). Based on the outcomes of a normality assessment, T-tests or Mann–Whitney U-tests were applied for continuous variable comparisons. Box plots visually captured delay durations, highlighting data variability and potential outliers. Correlation analysis was conducted on significant univariate analysis variables, excluding highly collinear ones, and the results were visually represented using Network Visualization. A stepwise forward logistic regression identified factors influencing healthcare-seeking delay, with odds ratios estimating the effect size of significant variables.
Results
Basic Characteristics
From the initial data of 1461 stroke patients obtained from the stroke follow-up platform, 26 were diagnosed with non-AIS diseases, and 16 had incomplete identification details. The final cohort comprised 1419 AIS patients, with a significant 82.52% (1171 patients) experienced healthcare-seeking delays (Figure 1).
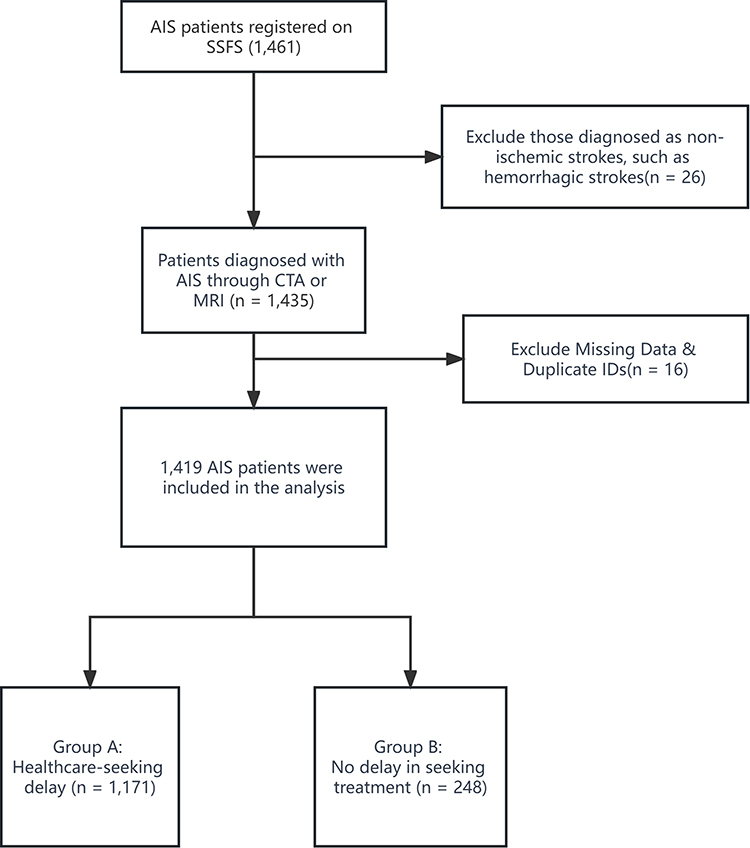 |
Figure 1 Flowchart. |
The median delay in seeking healthcare was 12.3 hours. The average age of patients in the delayed group was 58.14 years, slightly higher than the 56.48 years in the timely treatment group. Male patients constituted 72.76% in the delayed group versus 69.76% in the non-delayed group. A majority (95%) were of Han ethnicity. Among lifestyle factors, 77.37% of the delayed group consumed alcohol, and 69.60% were smokers. Detailed sociodemographic and clinical attributes are provided in Table 1.
 |
Table 1 Baseline Characteristics and Delay Analysis of AIS Patients (n = 1419) |
Univariate Analysis of Healthcare-Seeking Delay
In the univariate analysis of healthcare-seeking delays, significant differences were observed between between groups in terms of treatment delay rates. Utilizing the chi-square test and T-test, variables that demonstrated substantial discrepancies included: education (p=0.012), awareness of stroke-related knowledge (p≤0.001), self-admission (p≤0.001), arrival by ambulance (p≤0.001), method of transportation to the hospital (p≤0.001), self-acknowledged DM (p=0.003), atrial fibrillation (AF) (p≤0.001), HBP (p=0.033), DM (p=0.031), coronary artery disease (p=0.012), valvular heart disease (p=0.006), TOAST classification (p≤0.001), among others. Comprehensive insights on these distinctions are presented in Table 1.
Distribution of Delayed Healthcare-Seeking Time
In our analysis exploring the relationship between healthcare-seeking delays and various factors, we identified a number of critical variables significantly associated with longer delay durations. Patients with different immigrant statuses and modes of hospital admission (self-admitted versus otherwise) showed significant variations in delay times. Additionally, the presence of dysarthria symptoms and varying in NIHSS score categories distinctly contributed to these differences. A comprehensive portrayal of these distinctions is presented in Figure 2.
 |
Figure 2 Boxplot comparison of the time of healthcare seeking delay across different clinical variables. |
Network Visualization
In our correlation analysis, illustrated in Figure 3, several variable pairs were identified with Pearson’s correlation coefficients exceeding 0.5. Notably, a strong correlation was observed between self-admission and the method of transportation to the hospital, as well as among different age categories, with coefficients exceeding 0.7. These findings indicate potential multicollinearity, which could impact the validity of our analysis. To address this concern and enhance the robustness of our multivariate analysis, we specifically focused on “transportation to the hospital” and “age” as our principal variables of interest. This strategic approach was adopted to minimize the effects of confounding factors and to more accurately determine the impact of these key variables on healthcare-seeking delays among AIS patients.
 |
Figure 3 Network visualization of variables with Pearson correlation coefficients exceeding 0.5 and 0.7 thresholds. |
Multivariate Analysis of Healthcare-Seeking Delay
In the multivariate analysis, several factors significantly influenced healthcare-seeking delays. Education was found to be a critical determinant, with patients having a high school education or higher being less likely to experience delays compared to those with junior high school education or lower, as indicated by an odds ratio (OR=0.65 [95% CI:0.44–0.97]). This effect was more pronounced for individuals with a bachelor’s degree or higher (OR=0.32 [95% CI:0.20–0.51]). The type of stroke also impacted delay durations with of undetermined etiology presented fewer delays than Large-artery atherosclerosis strokes (OR=0.65 [95% CI:0.43–0.99]). Some symptoms decrease the likelihood of delay (OR=0.25 [95% CI:0.10–0.62]) and limb weakness (OR=0.21 [95% CI: 0.21–0.49]), were associated with a reduced likelihood of delay. Patients with a GCS score between 3–8 sought treatment more promptly than those scoring between 13–15 (OR=0.52 [95% CI:0.09–0.69]). Gender differences were notable, with males experiencing a 1.65 times greater risk of delay than females. Specific conditions such as wake-up strokes (OR=7.04 [95% CI: 3.69–13.44]) and small-vessel occlusion strokes (OR=2.07 [95% CI:1.28–3.36]). These findings are detailed in Table 2.
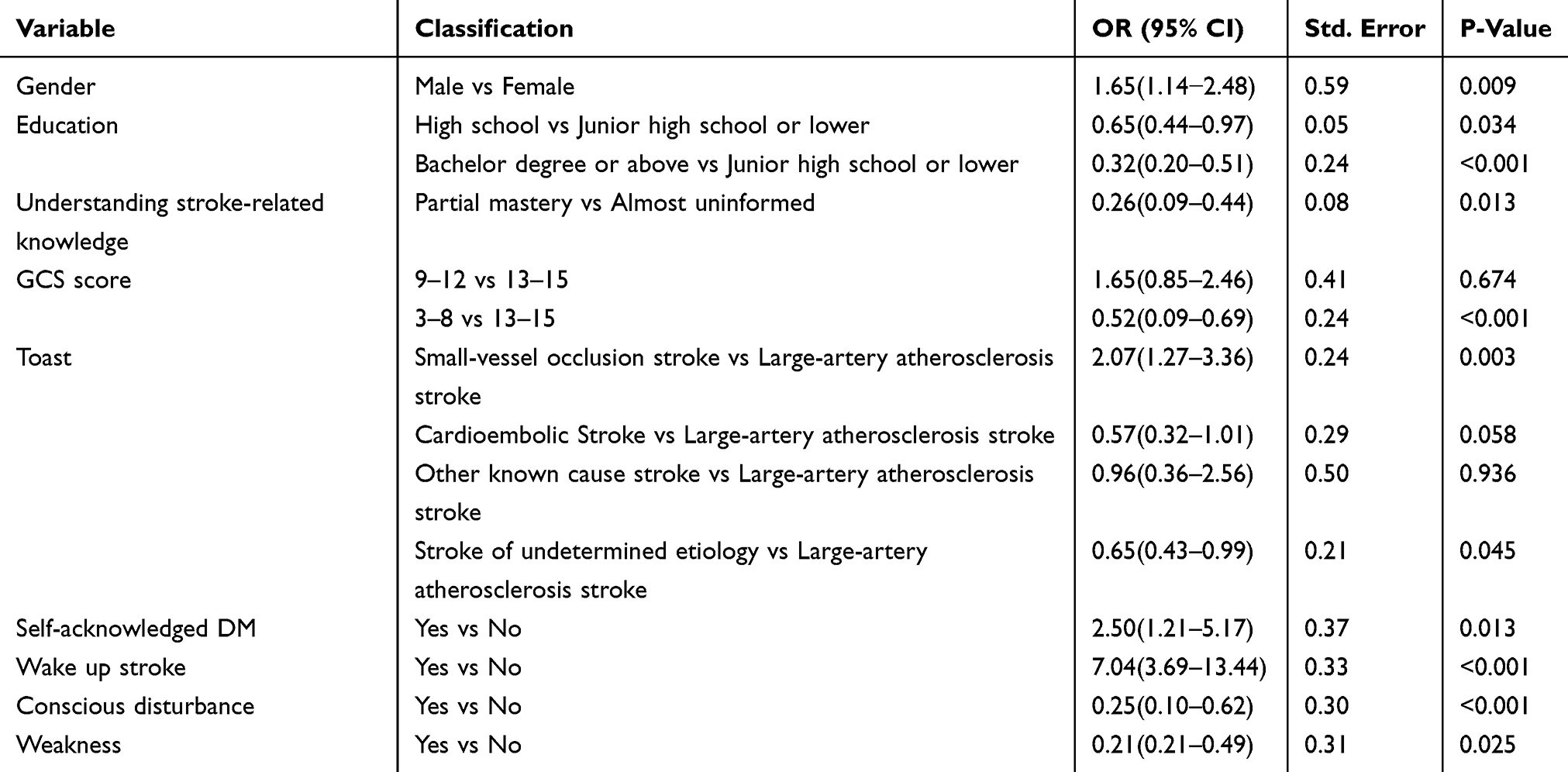 |
Table 2 Factors Influencing Treatment Delay in AIS Patients: Results from Binary Stepwise Logistic Regression Analysis.(n = 1419) |
Subgroup Analysis
In a subgroup analysis focusing on gender-based disparities in healthcare-seeking delays, notable trends emerged. Among all patients who experiencing the delays, younger males under 45 years constituted a significant proportion, at 33.57%, a marked contrast to their female counterparts of the same age group, who accounted for only 12.23%. A profound divergence was also observed in terms of educational background. A hefty 57.68% of females experiencing the delay had an education up to junior high school or lower, compared to just 28.17% of males. On the flip side, in the segment holding a bachelor’s degree or higher, females appeared less prone to the delay, with a count of only 16 cases. Another pivotal observation pertained to DM prevalence; 29.47% of the delayed female cohort had DM, surpassing the 19.37% prevalence found in the delayed male cohort. These detailed insights and disparities are further elaborated in Table 3.
 |
Table 3 Subgroup Analysis of Delayed Seeking Healthcare Among Male and Female AIS Patients.(n=1171) |
Discussion
Our findings indicate a median healthcare-seeking delay of 12.3 hours for AIS patients. For comparison, a decade-long analysis in mainland China reported a median onset-to-door duration nearing 24 hours.17 In Shanghai, the median delay is recorded at 8 hours,18 while Taiwan reports a time of 5 hours.19 Although the delay observed in our study is shorter than the broader trend seen in mainland China, it remains protracted when juxtaposed with regions renowned for their advanced healthcare infrastructures.
Our study highlights a notable healthcare-seeking delay among AIS within the immigrant population, a topic that has received limited attention in contemporary AIS research. Various challenges likely contribute to this delay, including language barriers, cultural differences, lack of health insurance, and unfamiliarity with the local healthcare systems. Supporting our observations, prior research has indicated that immigrants are less likely to undergo thrombolysis compared to native citizens.20 These findings emphasize the need for cities and regions with large immigrant populations to enhance healthcare accessibility.There is a pressing need to intensify health education efforts, focusing on the early symptoms of stroke, and advocate for inclusive and prompt healthcare access for every member of the community.
Our findings reveal that, while the median healthcare-seeking delay for males is comparable to that of females, a significant difference emerged in the risk of delay between genders. Specifically, males were found to have a 1.67 times greater risk of experiencing a delay compared to females, diverging from patterns observed in other countries. For instance, a study in Texas involving 1134 American patients found that males of Mexican origin exhibited a slightly lower risk of delay, a trend not consistently seen across other racial or ethnic groups.21 This variation highlights the complex interplay of geographical, cultural, and socio-economic factors in shaping healthcare-seeking behavior.22
An intriguing aspect of our analysis pertains to the role of gender in healthcare-seeking delays. Although our univariate analysis did not identify significant differences between males and females, the multivariate analysis revealed a different picture. This transition can likely be attributed to the complex interplay of multiple factors, which becomes discernible in a multivariate setting where variables are controlled.Particularly noteworthy was our approach to screen out variable pairs with correlation coefficients greater than 0.7. This step helped eliminate potential interactions and confounding factors, thereby unveiling the true relationship between gender and the delay in seeking medical treatment.This finding emphasizes the intricate nature of healthcare behaviors, illustrating how certain effects may remain hidden in univariate analyses but are revealed in a multivariate context.
Delving into the relationship between gender and healthcare-seeking delays, our subgroup analyses revealed distinct trends. Among females, a significant proportion of those who delayed seeking health-care were aged over 45, suggesting that middle-aged and older women might downplay symptoms or wait for spontaneous recovery, possibly due to entrenched beliefs.23 Conversely, younger males showed a more pronounced tendency for the delay than their female counterparts of the same age bracket. This could be attributed to a combination of overconfidence in health, reduced ailment sensitivity to ailments, and the weight of societal and familial responsibilities at this life stage, potentially deterring timely medical attention.24 From an educational standpoint, males with higher education levels exhibited more significant delays in seeking healthcare compared to females with analogous educational backgrounds. This difference could from the heightened occupational pressures and responsibilities these males face, compelling them to persevere at work despite early symptom onset rather than promptly seeking medical aid.25 Furthermore, a notable portion of females who delayed treatment resorted to self-medication. These insights underscore the pressing need for strategic educational and intervention measures.26 To address these disparities, comprehensive, multi-faceted approach is essential. We advocate for strengthened public health initiatives, focusing on targeted awareness campaigns. A special emphasis should be placed on high-risk groups, such as older female, younger male, and the highly-educated males. Collaborative efforts between medical establishments and public health entities are crucial to promote these initiatives, emphasizing the critical importance of early stroke symptom recognition and the need for immediate medical intervention.
Our study highlights a strong correlation between educational attainment and healthcare-seeking behavior in AIS patients. Specifically, individuals with only a junior high school education or lower were found to have a higher propensity for delaying healthcare-seeking. In contrast, having a high school or university education appeared to serve as protective factors, reducing the likelihood of such delays. This observation resonates with prior research indicating that individuals with merely elementary education experience a 1.41 times higher risk of treatment delay when juxtaposed with the higher-educated counterparts.27 The reasons behind this educational disparity in healthcare-seeking delay are multifaceted. Primarily, higher educational levels typically are often associated with enhanced health literacy. Individuals with more education can often more swiftly recognize preliminary stroke symptoms, assign greater priority to their health, and consequently, are more inclined to promptly seek medical intervention.28 This proactive health-seeking behavior is not solely a byproduct of enhanced health knowledge and cognizance. These individuals frequently benefit from robust social networks and community scaffolds, facilitating more immediate access to guidance and assistance when health anomalies arise.29 Furthermore, their heightened familiarity with healthcare ecosystems and the inherent ease of navigating medical services could be instrumental in reducing delays. In essence, this data accentuates the pivotal role of health education in curbing healthcare-seeking delay.30
Our findings highlight the crucial role of knowledge about stroke in influencing the speed at which patients seek medical intervention. This knowledge encompasses a comprehensive understanding of the primary symptoms, risk factors, and preventive measures associated with stroke. Crucially, this understanding is not merely academic, it deeply informs patients’ everyday decisions and health behaviors. Our observations are in line with previous research, supporting a widely recognized consensus on the crucial role of education about stroke in fostering prompt medical intervention.31,32 This knowledge not only enables patients to recognize symptoms at an early stage but also cultivates a proactive approach towards seeking medical assistance.33 In light of these insights, it is clear that expanding the reach and depth of stroke-related education is a pressing need. This calls for a collaborative effort, encouraging both the general public and healthcare professionals to work together in promoting more effective stroke management and outcomes.
In line with previous studies,34–38 our research highlights the significant impact of initial symptoms and specific clinical factors on the delay AIS patients experience in reaching a hospital. For example, a lower GCS score, indicating a substantial neurological deficit, typically prompts patients or their caregivers to seek medical help more proactively. Symptoms such as altered consciousness and limb weakness are often perceived as alarming, leading to quicker decisions to seek medical intervention.34,35 In contrast, patients with small vessel disease, like Pure Sensory Stroke may not exhibit the same level of urgency. Despite an increased risk of treatment delay, these patients often present with milder symptoms, leading to an underestimation of the severity of their condition.36 This is corroborated by clinical studies showing that Pure Sensory Stroke generally has a favorable prognosis, with about 41.5% of patients being symptom-free at hospital discharge.39 Such a deceptive sense of security may contribute to delays in seeking medical consultation among patients with small vessel diseases, highlighting the need for increased awareness and education about the potential severity of these strokes. Similarly, patients aware of their Diabetes Mellitus status frequently mistook stroke symptoms for DM-induced complications, adding to their healthcare-seeking delays.39 Further complicating the scenario, those awakening to stroke symptoms faced inherent uncertainties about symptom onset, leading to hesitations in seeking immediate care.38 Collectively, these insights emphasize the intricate interplay of clinical manifestations, symptom recognition, and patient behavior, underscoring the need for targeted public health initiatives that prioritize early symptom detection and immediate medical intervention.
The retrospective nature of this study and challenges related to data traceability have limited our ability to include several relevant variables. Critical factors such as the availability of telecommunication devices, essential for timely emergency response, and the implementation of prehospital stroke protocols, which significantly affect the efficiency of emergency care, were not within the scope of our examination. Additionally, the analysis of posterior circulation stroke cases was impeded by a substantial amount of missing data, necessitating their exclusion from the study. Moreover, the limited representation of the ultra-elderly population (aged over 85 years) in our dataset restricts the depth of our understanding regarding their healthcare-seeking delays.40 Despite these limitations, exploring the unique risk factors and experiences of the ultra-elderly remains a crucial area of research. Advancing studies in this field is vital for enhancing stroke care and intervention strategies across different age groups, thereby contributing to a more comprehensive understanding of stroke management.
Conclusion
Delays in seeking health-care for AIS are influenced by a multifaceted interplay of sociodemographic and clinical factors. Healthcare-seeking delays within the immigrant population highlight the necessity of addressing systemic barriers to health-care. The significant influence of education and knowledge about stroke highlights the essential role of enhanced health literacy and targeted public awareness campaigns. These interventions are especially important for specific groups such as younger males, older females, and males with higher educational levels. Ultimately, a holistic and collaborative approach, integrating public health initiatives and systemic reforms, is essential for timely medical interventions and improved stroke outcomes.
Ethics Statement
This study was conducted in compliance with the ethical standards of the 1964 Helsinki Declaration and its subsequent amendments. Given the retrospective nature of our research and the use of anonymized data, the Institutional Review Board of Shenzhen Longhua People’s Hospital granted us an exemption from a full review. Prior to extracting data from the Shenzhen Stroke Follow-up System Platform (SSFS), we secured all necessary permissions and ensured the complete anonymization of the data, making it impossible to trace back to individual participants. Due to the fully anonymized nature of the data used in this study, informed consent from participants was not obtained. This requirement was waived by the Institutional Review Board of Shenzhen Longhua People’s Hospital, as the complete anonymization of the data guarantees the privacy protection of the participants.
Acknowledgments
We express our heartfelt gratitude to YX for his invaluable contribution to patient follow-up. Special thanks to YC and FL for their meticulous editorial support throughout the preparation of this paper. Our sincere appreciation goes to QZ and YL for their consistent guidance and assistance in this study.
Funding
This study was funded by the High Level Project of Medicine in Longhua, ShenZhen under grant number HLPM201907020102 and construction funds of key medical disciplines in Longhua District, Shenzhen under grant number MKD202007090208.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
2. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
3. Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929–1935. doi:10.1016/S0140-6736(14)60584-5
4. Rabinstein AA. Update on Treatment of Acute Ischemic Stroke. Continuum. 2020;26(2):268–286. doi:10.1212/CON.0000000000000840
5. Chao B, Yan F, Hua Y, et al. Stroke prevention and control system in China: CSPPC-Stroke Program. Int J Stroke. 2021;16(3):265–272. doi:10.1177/1747493020913557
6. Evans MRB, White P, Cowley P, Werring DJ. Revolution in acute ischaemic stroke care: a practical guide to mechanical thrombectomy. Practical Neurol. 2017;17(4):252–265. doi:10.1136/practneurol-2017-001685
7. Teuschl Y, Brainin M. Stroke education: discrepancies among factors influencing prehospital delay and stroke knowledge. Int J Stroke. 2010;5(3):187–208. doi:10.1111/j.1747-4949.2010.00428.x
8. Kim YS, Park S, Bae H, et al. Stroke awareness decreases prehospital delay after acute ischemic stroke in Korea. BMC Neurol. 2011;11:2. doi:10.1186/1471-2377-11-2
9. John M, Palmer P, Faile E, Broce M. Factors causing patients to delay seeking treatment after suffering a stroke. West Virginia Med J. 2005;101(1):12–15.
10. Gao Z, Liu Q, Yang L, Zhu X. Identification of high-risk factors for prehospital delay for patients with stroke using the risk matrix methods. Front Public Health. 2022;10:858926. doi:10.3389/fpubh.2022.858926
11. Zhou Y, Yang T, Gong Y, et al. Pre-hospital Delay after Acute Ischemic Stroke in Central Urban China: prevalence and Risk Factors. Mol Neurobiol. 2017;54(4):3007–3016. doi:10.1007/s12035-016-9750-4
12. Nepal G, Yadav JK, Basnet B, Shrestha TM, Kharel G, Ojha R. Status of prehospital delay and intravenous thrombolysis in the management of acute ischemic stroke in Nepal. BMC Neurol. 2019;19(1):155. doi:10.1186/s12883-019-1378-3
13. Botelho A, Rios J, Fidalgo AP, Ferreira E, Nzwalo H. Organizational Factors Determining Access to Reperfusion Therapies in Ischemic Stroke-Systematic Literature Review. J Med. 2022;19.
14. Sharobeam A, Jones B, Walton-Sonda D, Lueck CJ. Factors delaying intravenous thrombolytic therapy in acute ischaemic stroke: a systematic review of the literature. J Neurol. 2021;268(8):2723–2734. doi:10.1007/s00415-020-09803-6
15. Sobral S, Taveira I, Seixas R, et al. Late Hospital Arrival for Thrombolysis after Stroke in Southern Portugal: who Is at Risk? J Stroke Cerebrovascular Dis. 2019;28(4):900–905. doi:10.1016/j.jstrokecerebrovasdis.2018.12.009
16. Shenzhen Municipality Bureau Of Statistics, Survey Office of the National Bureau of Statistics in Shenzhen. Shenzhen Statistical Yearbook 2022. Beijing: China statistics press; 2022.
17. Yuan J, Lu ZK, Xiong X, et al. Age and geographic disparities in acute ischaemic stroke prehospital delays in China: a cross-sectional study using national stroke registry data. Lancet Regional Health. 2023;33:100693. doi:10.1016/j.lanwpc.2023.100693
18. Fang J, Yan W, Jiang G, Li W, Cheng Q. Time interval between stroke onset and hospital arrival in acute ischemic stroke patients in Shanghai, China. Clin Neurol Neurosurg. 2011;113(2):85–88. doi:10.1016/j.clineuro.2010.09.004
19. Chang K, Tseng M, Tan T. Prehospital delay after acute stroke in Kaohsiung, Taiwan. Stroke. 2004;35(3):700–704. doi:10.1161/01.STR.0000117236.90827.17
20. Mkoma GF, Norredam M, Iversen HK, Andersen G, Johnsen SP. Use of reperfusion therapy and time delay in patients with ischaemic stroke by immigration status: a register-based cohort study in Denmark. Eur J Neurol. 2022;29(7):1952–1962. doi:10.1111/ene.15303
21. Smith MA, Lisabeth LD, Bonikowski F, Morgenstern LB. The role of ethnicity, sex, and language on delay to hospital arrival for acute ischemic stroke. Stroke. 2010;41(5):905–909. doi:10.1161/STROKEAHA.110.578112
22. Vargas Bustamante A, Fang H, Rizzo JA, Ortega AN. Understanding observed and unobserved health care access and utilization disparities among US Latino adults. Med Care Res. 2009;66(5):561–577. doi:10.1177/1077558709338487
23. Lecouturier J, Rodgers H, Murtagh MJ, White M, Ford GA, Thomson RG. Systematic review of mass media interventions designed to improve public recognition of stroke symptoms, emergency response and early treatment. BMC Public Health. 2010;10:784. doi:10.1186/1471-2458-10-784
24. O’Brien R, Hunt K, Hart G. ‘It’s caveman stuff, but that is to a certain extent how guys still operate’: men’s accounts of masculinity and help seeking. Soc Sci Med. 2005;61(3):503–516. doi:10.1016/j.socscimed.2004.12.008
25. Wang J, Schmitz N, Dewa C, Stansfeld S. Changes in perceived job strain and the risk of major depression: results from a population-based longitudinal study. Am J Epidemiol. 2009;169(9):1085–1091. doi:10.1093/aje/kwp037
26. Westergaard ML, Glümer C, Hansen EH, Jensen RH. Medication overuse, healthy lifestyle behaviour and stress in chronic headache: results from a population-based representative survey. Cephalalgia. 2016;36(1):15–28. doi:10.1177/0333102415578430
27. Gu S, Dai Z, Shen H, et al. Delayed Stroke Treatment during COVID-19 Pandemic in China. Cerebrovascular Dis. 2021;50(6):715–721. doi:10.1159/000517075
28. Mirowsky J, Ross CE. Education, Health, and the Default American Lifestyle. J Health Social Behav. 2015;56(3):297–306. doi:10.1177/0022146515594814
29. Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Social Behav. 2010;51 Suppl:S28–S40. doi:10.1177/0022146510383498
30. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Internal Med. 2011;155(2):97–107. doi:10.7326/0003-4819-155-2-201107190-00005
31. Sakamoto Y, Yokota C, Miyashita F, et al. Effects of stroke education using an animated cartoon and a manga on elementary school children. J Stroke Cerebrovascular Dis. 2014;23(7):1877–1881. doi:10.1016/j.jstrokecerebrovasdis.2014.02.015
32. Grech P, Grech R. The role of health promotion theories in Stroke Awareness and Education. Appl Nursing Res. 2021;58:151415. doi:10.1016/j.apnr.2021.151415
33. Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical Attention Seeking After Transient Ischemic Attack and Minor Stroke Before and After the UK Face, Arm, Speech, Time (FAST) Public Education Campaign: results From the Oxford Vascular Study. JAMA Neurol. 2018;75(10):1225–1233. doi:10.1001/jamaneurol.2018.1603
34. Smith EE, Dreyer P, Prvu-Bettger J, et al. Stroke center designation can be achieved by small hospitals: the Massachusetts experience. Critical Pathways Cardiol. 2008;7(3):173–177. doi:10.1097/HPC.0b013e318184e2bc
35. Petty GW, Brown RD, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Ischemic stroke subtypes: a population-based study of functional outcome, survival, and recurrence. Stroke. 2000;31(5):1062–1068. doi:10.1161/01.str.31.5.1062
36. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991;337(8756):1521–1526. doi:10.1016/0140-6736(91)93206-o
37. Desalu OO, Wahab KW, Fawale B, et al. A review of stroke admissions at a tertiary hospital in rural Southwestern Nigeria. Ann Af Med. 2011;10(2):80–85. doi:10.4103/1596-3519.82061
38. Mackey J, Kleindorfer D, Sucharew H, et al. Population-based study of wake-up strokes. Neurology. 2011;76(19):1662–1667. doi:10.1212/WNL.0b013e318219fb30
39. Arboix A, García-Plata C, García-Eroles L, et al. Clinical study of 99 patients with pure sensory stroke. J Neurol. 2005;252(2):156–162. doi:10.1007/s00415-005-0622-5
40. Arboix A, Miguel M, Císcar E, García-Eroles L, Massons J, Balcells M. Cardiovascular risk factors in patients aged 85 or older with ischemic stroke. Clin Neurol Neurosurg. 2006;108(7):638–643. doi:10.1016/j.clineuro.2005.10.010
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.