Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Healthcare Resource Use and Burden Associated with Influenza Transmission Among Household Members with a Primary Infection: Commercial Claims Data Analysis
Authors Wallick C, Abbass IM ![]() , Sheinson D, Moawad D
, Sheinson D, Moawad D
Received 1 January 2021
Accepted for publication 13 April 2021
Published 30 April 2021 Volume 2021:13 Pages 335—342
DOI https://doi.org/10.2147/CEOR.S298992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Christopher Wallick, Ibrahim M Abbass, Daniel Sheinson, Dalia Moawad
Genentech, Inc, South San Francisco, CA, USA
Correspondence: Christopher Wallick
Genentech, Inc., South San Francisco, CA, USA
Tel +1 650-797-3006
Fax +1 650-225-4630
Email [email protected]
Purpose: To assess the burden of influenza transmission and care-seeking patterns over 3 influenza seasons among commercially insured households with a primary influenza infection.
Patients and Methods: This retrospective cohort study used commercial claims data from the US MarketScan® Commercial and Medicare Supplemental databases for the 2014, 2015, and 2016 influenza seasons. Patients with a billed diagnosis of influenza and with coverage for at least 1 household member under the same health plan policy were included. A secondary diagnosed case was defined as a diagnosis of influenza in a second household member occurring within 14 days of the index case in a household.
Results: Among 1,224,808 households with ≥ 2 members and a primary case of influenza, a secondary case of influenza was reported in 119,883 households (9.8%). A secondary diagnosed case of influenza occurred within 4 days of the primary diagnosis in 93,883 (78.3%) of those households. Both primary and secondary diagnosed influenza cases occurred most often among children (∼ 60%). Household size was positively correlated to both the risk of a second case (6.4% of households with 2 or 3 members versus 12.6% of households with ≥ 4 members, P < 0.001) and the time to diagnosis of a second case (Spearman rank correlation coefficient = 0.09; P < 0.001).
Conclusion: Claims data for 3 influenza seasons (2014, 2015, 2016) showed that intrahousehold transmission of influenza occurs in approximately 10% of households with a primary case and poses a higher burden on larger households. Intrahousehold transmission of influenza represents a large healthcare resource use burden, with an unmet need for interventions that limit transmission.
Keywords: claims, household, influenza, retrospective, observational, children
Introduction
Seasonal influenza is associated with a high disease and economic burden. The Centers for Disease Control and Prevention (CDC) estimates that influenza has resulted in 9.3 to 45 million illnesses, 140,000 to 960,000 hospitalizations, and 12,000 to 79,000 deaths annually in the US since 2010.1 An estimated 5% to 20% of patients in the US are infected with influenza each year;2 however, recent publications have estimated that only 2% of commercially insured patients have an influenza-related visit, including a billed diagnosis code of influenza, each year.3 Across 8 influenza seasons from 2001/2002 through 2008/2009, projected annual numbers of influenza-related healthcare encounters ranged from 11.3 to 25.6 million and healthcare costs ranged from $2.0 to $5.8 billion; the average cost across all seasons was $3.5 billion.4
Healthy adults can transmit influenza virus from 24 hours before symptom onset and for up to 5 to 7 days after symptoms develop; children can remain infectious even longer, sometimes for more than 7 days.5 The typical incubation period for influenza is 1 to 4 days, with an average of 2 days; thus the virus may be transmitted before the appearance of symptoms and also during the symptomatic phase. Infected but asymptomatic individuals can also transmit the virus.5,6 Household transmission studies suggest that the risk of infection from household contact can be as high as 38%, with a 2- to 4-day median interval between symptom onset in the index cases and the secondary case.7,8
Information on influenza transmission is important for informing decisions about control strategies. Since up to 30% of influenza virus transmission occurs among household members,9,10 studies of household transmission are of particular interest. The household provides a strategic setting for examining influenza transmission in a confined area. Understanding influenza transmission and care seeking among households can help quantify influenza burden and determine the effectiveness of control measures such as antiviral prophylaxis or treatment. In this study, real-world claims data were used to understand the care-seeking burden for a second case of influenza among households and the impact of household size on household influenza burden. A diagnosis code of influenza in a second member of the household was used as a proxy for intrahousehold transmission.
Patients and Methods
Study Design
This was a retrospective analysis of US commercial claims data from the 2014, 2015, and 2016 influenza seasons (04/01/2014–05/30/2017). Data were extracted from the MarketScan® Commercial Claims and Encounters Database and the MarketScan® Medicare Supplemental and Coordination of Benefits Database (IBM Watson Health, Cambridge, MA). The databases include employees, dependents, and retirees with employer-sponsored commercial and Medicare insurance. The claims files capture inpatient and outpatient care, use of facilities and services, pharmacy, and payment information.
The study sample included patients with a billed diagnosis of influenza who also had coverage for at least 1 household member under the same health plan policy. The diagnostic codes used to identify influenza patients were ICD-9: 487.xx or 488.xx or ICD-10: J09.xx, J10.xx, or J11.xx. A secondary diagnosed case was defined as a diagnosis of influenza in a second household member occurring within 14 days of the index case in a household potentially including a visit on the same day (or even a concurrent visit billed for each patient); for these cases one patient was randomly designated primary and the other secondary. Patients were required to have continuous health plan coverage during each influenza episode.
The study used de-identified publicly available data and was exempt from Institutional Review Board review. The research was compliant with the Health Insurance Portability and Accountability Act.
Outcomes and Statistical Analyses
The outcomes evaluated were the number of additional household members who sought care for influenza (secondary diagnosed case), the time elapsed between the index (primary case) and second case of influenza, impact of household size on secondary cases, and duration between influenza-related office visits. In addition, the characteristics of households and individual household members who sought care for influenza were determined. The association of household size with number of days between primary and secondary diagnosed cases was assessed using the Spearman rank correlation coefficient, with a t-test used to determine statistical significance. Impact of household size (2 or 3 vs ≥4) on proportion of households with a secondary diagnosed case was analyzed with Fisher’s exact test.
Results
Study Population
Overall, 1,224,808 households with ≥2 members were identified with a primary diagnosis of influenza during the 2014, 2015, and 2016 seasons (Figure 1). Among households with ≥2 members and at least one influenza diagnosis, a second member sought care for influenza within 14 days of the initial influenza episode in 119,883 households (9.8%). A total of 15,759 (1.3%) of households of ≥2 members had multiple secondary diagnosed cases of influenza.
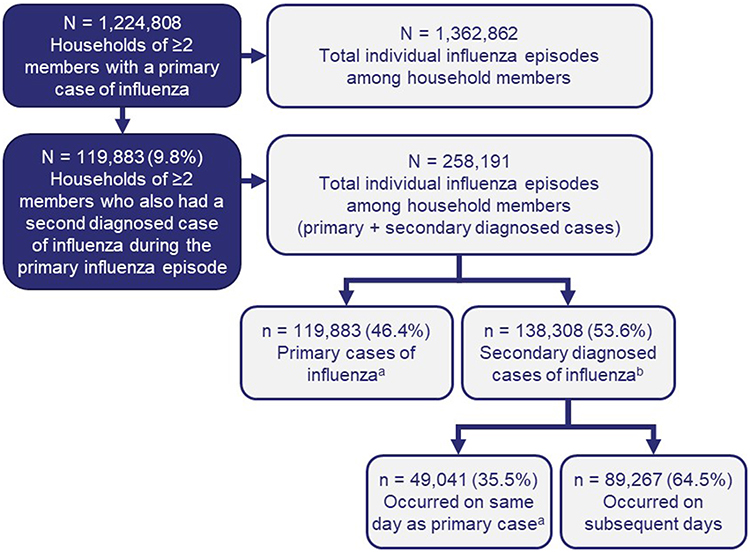 |
Figure 1 Households of 2 or more members with a primary and a secondary diagnosed case of influenza during the 2014, 2015, and 2016 seasons. aWhen multiple cases within a household occurred on the same day, one was randomly assigned as primary. bSome households had multiple secondary diagnosed influenza cases. |
Demographics of Included Households
The median household size was 4 members. The distribution of households by household size was as follows: 2 members, 21%; 3 members, 24%; 4 members, 33%; 5 members, 15%; and 6+ members, 7%. Among 138,308 secondary diagnosed cases of influenza, 35.5% (n = 49,041) sought care on the same day as the primary case and 64.5% (n = 89,267) sought care on subsequent days (≤14 days) following the primary case of influenza in the family (Figure 1). There were no differences in demographic characteristics (age, sex, health plan type, and region) between household members that were the primary or a secondary diagnosed case of influenza (Table 1). The highest proportion of either primary or secondary diagnosed cases was recorded among children (62.0%), followed by employees (20.7%) and spouses (17.3%).
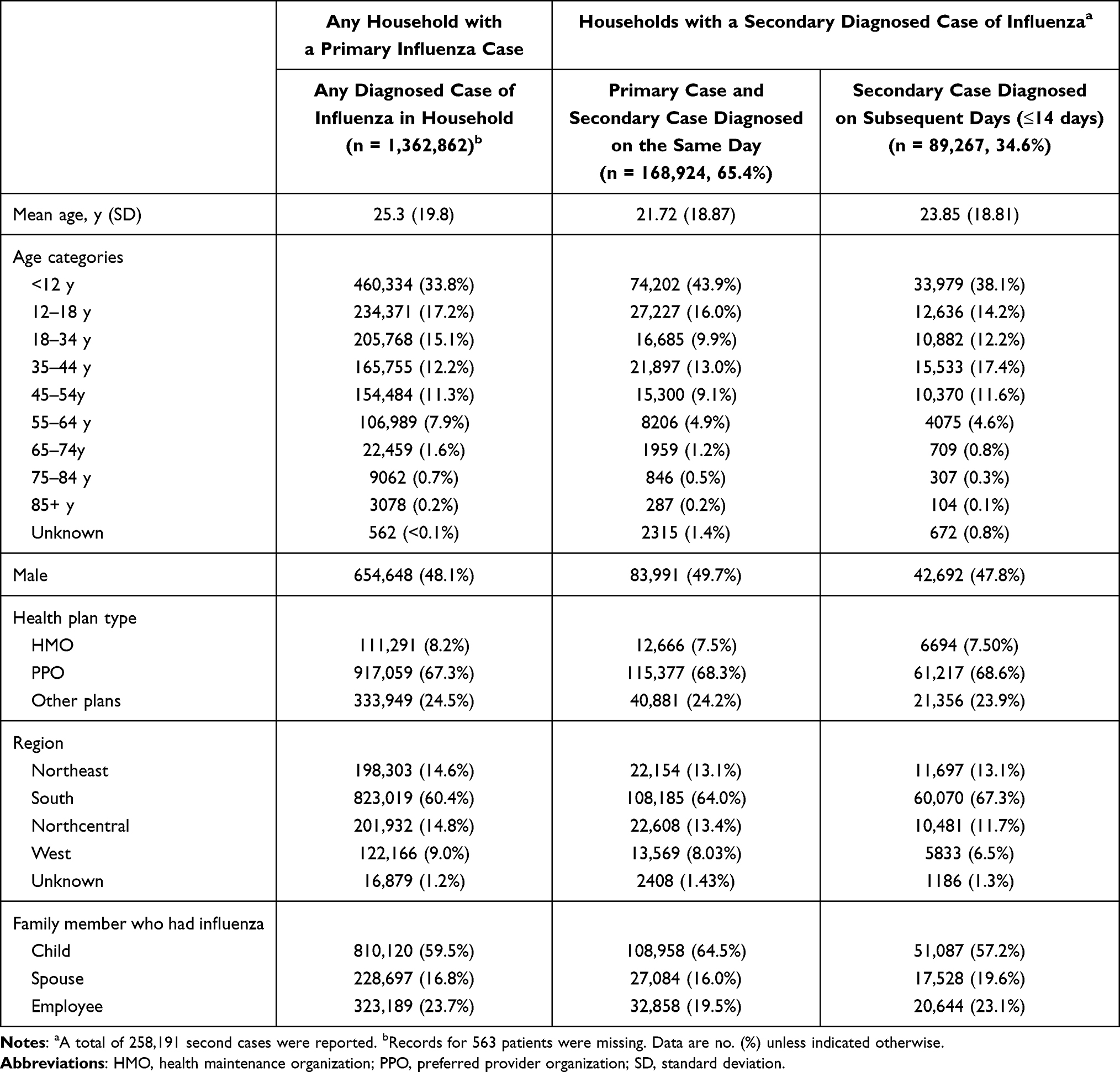 |
Table 1 Demographics of Household Members with a Diagnosed Case of Influenza (Household of ≥2 Members) |
Characteristics of Secondary Diagnosed Cases
Among households with a secondary diagnosed case of influenza, the secondary case occurred within 4 days of the primary case in 93,883 households (78.3%) and within 7 days of the primary case in 108,551 households (90.5%) (Figure 2). It is notable that one-third of secondary diagnosed cases occurred on the same day as the primary diagnosis.
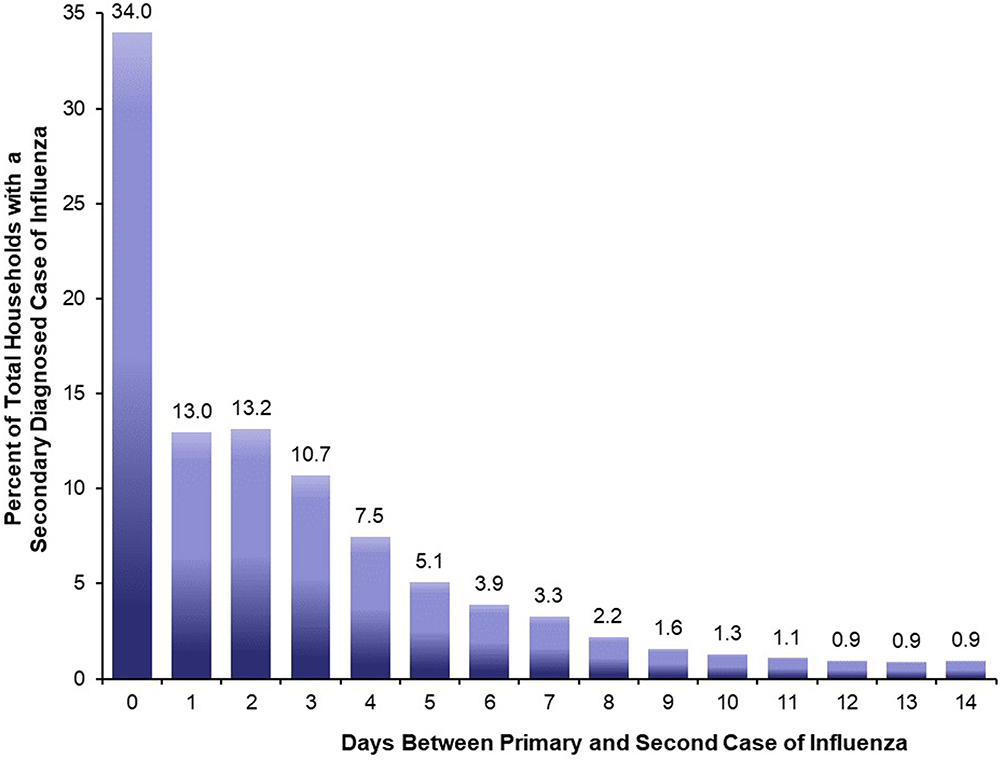 |
Figure 2 Number of days until the next influenza diagnosis in the same household. The total number of households with a secondary diagnosed case of influenza was 119,883. |
Larger household size was associated with both increased risk of having a secondary diagnosed case and the length of time to diagnosis of the secondary case. The number of members in a household was positively associated with having a secondary diagnosed case of influenza in the 14-day period after a primary infection (Figure 3A). In households with 2 or 3 members (n = 554,649), the frequency of a secondary diagnosed case of influenza was 6.43% (n = 35,637), whereas in households with >4 members (n = 670,159), the frequency of a secondary diagnosed case increased to 12.57% (n = 84,246). The days to diagnosis of influenza in another household member correlated positively with larger household size (Spearman rank correlation coefficient = 0.09; P < 0.001) (Figure 3B).
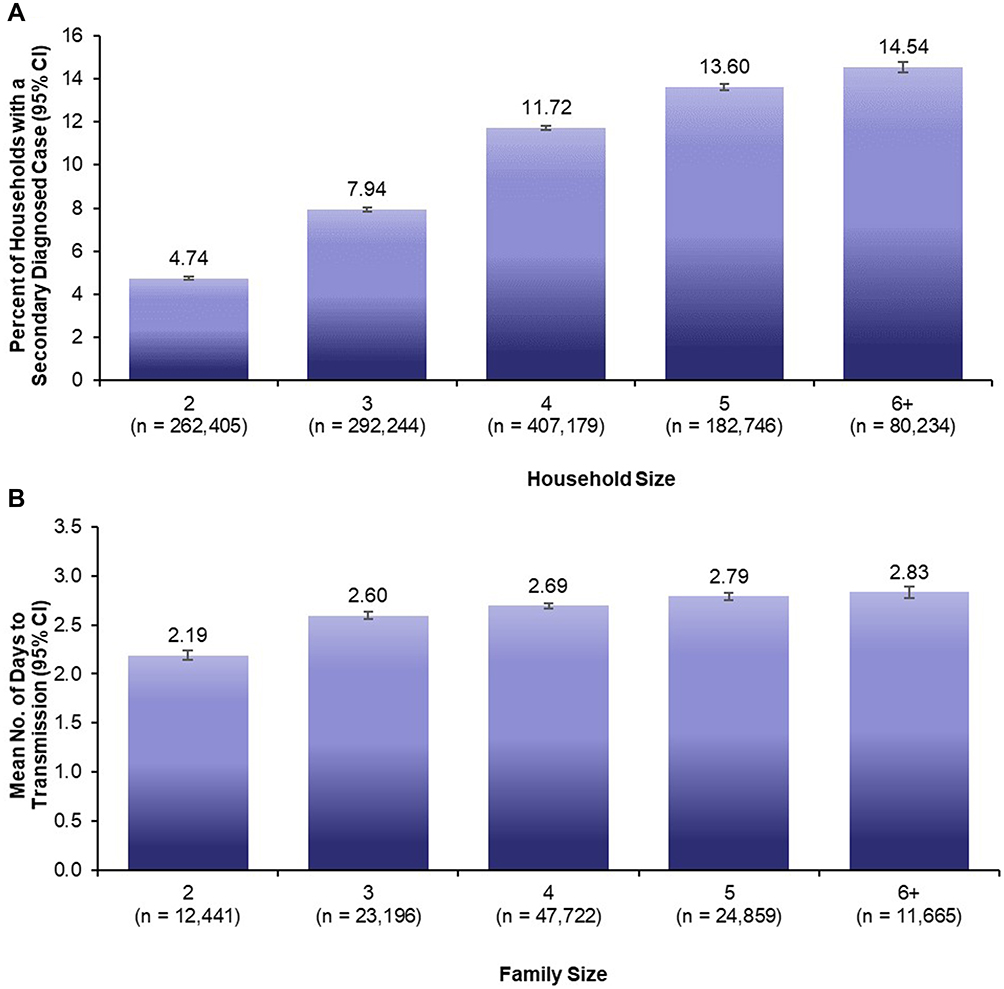 |
Figure 3 Relationship between household size and (A) secondary diagnosed case of influenza and (B) days until the next influenza diagnosis among members of the same household. Household size in (A) is the number of households of ≥2 members that had a primary case of influenza. Household size in (B) is the number of households of ≥2 members that had a secondary diagnosed case of influenza. |
Discussion
Influenza has a large impact on the health care system, including payers, employers and above all patients. Understanding the transmissibility of influenza infection and associated burden, particularly within the most vulnerable settings for transmission, is crucial to understanding the epidemiology of influenza and for designing effective control measures. Although the current study did not have data on COVID-19 available for analysis, findings regarding household transmission of influenza may be useful in informing underlying principles of respiratory virus transmission in the household setting. The present claims database study used the most recently available data for the 2014, 2015, and 2016 influenza seasons and included more than 1.2 million multimember households with a primary diagnosed case of influenza. Using a diagnostic claim for a second influenza episode among household members as a proxy for intrahousehold transmission, this analysis showed that approximately 10% of households with a primary diagnosed case of influenza had a second household member seek care for influenza. Both primary and secondary diagnosed cases were reported primarily in children, with approximately 80% of secondary cases occurring within 4 days of a primary diagnosis. Larger households experienced both a higher number of secondary diagnosed cases and a longer time until a secondary visit for influenza.
In this study, a second diagnosed case of influenza occurred in 10% of households with ≥2 members, which is broadly consistent with the estimated 7% to 8% probability of transmission from an infected individual to another household member obtained from household cohort studies.9,11 Our study likely underestimates this rate because secondarily infected patients may not seek care, especially if no intervention is offered, and thus would not be available in our data analysis. Published estimates of the intrahousehold secondary influenza infection risk range from 1% to 38%;7,8 this heterogeneity arises from differences in diagnostic methods for case ascertainment, host factors, and viral infectivity.
A secondary diagnosed case of influenza occurred within 2 days of the primary case in 60% of households and within 4 days of the primary diagnosis in 78% of households, suggesting rapid transmission among household members. In models of experimental infection and in naturally acquired infection, viral shedding was detected within 1 day after inoculation, with a shedding duration of almost 5 days.12,13 Approximately 10% of secondary diagnosed cases in this study occurred 7 to 14 days after the primary diagnosis, but because of the longer interval between the 2 diagnoses, the possibility that these infections were acquired from the community cannot be discounted.
Both primary and secondary diagnosed cases in this study were reported predominantly in children, a finding that supports the major role of children in the dissemination of influenza in households.14–16 Children may be less likely than adults to have protective anti-influenza antibodies but are at greater risk of transmitting due to poor hygiene and higher and more prolonged viral shedding.17 Data on preseason antibody levels were not available for this study, but it has been shown that even after correcting for preseason hemagglutination inhibition titers, the risk of household infection remains higher in children than in adults.9
The risk of a secondary diagnosed case of influenza increased significantly as the household size increased. Although our study design differed from the design in previous studies, this finding concurs with results from some previous studies showing that household size and number of children were risk factors for household transmission;11,18 other studies however suggest that the risk of secondary transmission diminishes with increasing household size.16,19 Larger household size was also associated with a longer interval between the presentation of primary and secondary diagnosed cases, hypothetically leading to a longer total duration of illness burden for the household; this could potentially lead to a longer duration of absenteeism from work and increased loss of productivity.
Interventions that limit transmission may help alleviate the burden on households and the healthcare system. Early treatment of index cases with an antiviral agent may reduce the risk of infection in their household contacts,20,21 and additionally, post-exposure antiviral prophylactic treatment of household contacts may provide some degree of protection.22–24
There are several limitations to our study methodology, including the method used to identify influenza patients. Identifying patients using a billed diagnosis for influenza provides the date a patient first interacted with the healthcare system, not necessarily the date of infection or symptom onset. While this can inform some aspects of influenza transmission, particularly from a healthcare resource utilization perspective, it is likely to be less accurate from a virological perspective. Additionally, many influenza patients, for various reasons, do not seek medical care and thus would not be included in our analysis, leading to an under-representation of the true burden of household transmission. There may also be reduced incentive to seek care for a second case of influenza within the household after one member was diagnosed, especially if no treatment was given. Additionally, our methods had inherent selection bias, favoring index cases that had severe enough symptoms to seek medical assistance from their healthcare provider. Many cases, especially those that are asymptomatic and subclinical, are less likely to be detected in claims database studies, but evidence of viral shedding in these individuals suggests their potential to transmit the virus to close contacts.6 Thus it is possible that households with asymptomatic cases were not enrolled or that an asymptomatic case preceded the assumed index diagnosis. Similarly, vaccination status was not available in the data set and previous studies suggested that vaccination claims are likely to be underreported and thus vaccination could not be included in the analysis.25,26 Additionally, because we used a 14-day period after primary infection for identifying secondary cases, there is a possibility that some community-transmitted infections were classified as secondary cases. The database may not be representative of the US population since it reflects individuals enrolled in commercial healthcare plans and some supplemental Medicare plans; in addition, the geographic distribution was skewed toward cases from the South. Since laboratory testing status was not available, diagnosis of both primary and secondary cases of influenza could be based on clinical symptoms, leaving a possibility that cases with other viral illnesses could have been misidentified as influenza.
Conclusions
This real-world study used commercial claims data for the 2014, 2015, and 2016 influenza seasons and showed that approximately 10% of households with a primary influenza diagnosis had a second member seek care for influenza. Almost 80% of secondary diagnoses occurred within 4 days of the primary diagnosis. Children accounted for the majority of both primary and secondary diagnosed cases. Both the risk of having a second household case and the overall duration of illness within a household increased as the household size increased. Influenza transmission within households poses a large burden on the healthcare system, suggesting a need for treatment options that limit transmission.
Data Sharing Statement
The data that support the findings of this study are available from IBM MarketScan Research Databases, but these data are not publicly available. All relevant data are provided within the manuscript.
Acknowledgments
Medical writing services were provided Meher M. Dustoor, PhD, of Global Outcomes Group, and medical editing services were provided by Esther Tazartes, MS, of Global Outcomes Group; these services were funded by Genentech, Inc. This paper was presented at “IDWeek: Advancing Science, Improving Care” on October 6, 2018, in San Francisco, California, as a poster presentation with interim findings. The poster’s abstract was published in Open Forum Infect Dis. 2018;5(Suppl 1):S749. https://academic.oup.com/ofid/search-results?page=1&q=Wallick&fl_SiteID=5338&SearchSourceType=1&allJournals=1-.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The study was sponsored and funded by Genentech, Inc., South San Francisco, CA.
Disclosure
All authors are full-time employees of Genentech, Inc. and hold Genentech stock.
References
1. Centers for Disease Control and Prevention. Disease burden of influenza; 2020. Available from: https://www.cdc.gov/flu/about/disease/burden.htm.
2. Sullivan KM, Monto AS, Longini IM
3. Wallick C, Wu N, To TM, Keebler D, Moawad D. Antiviral use is associated with a decrease in the rate of influenza-related complications and healthcare resource utilization.
4. Yan S, Weycker D, Sokolowski S. US healthcare costs attributable to type A and type B influenza. Hum Vaccin Immunother. 2017;13(9):2041–2047. doi:10.1080/21645515.2017.1345400
5. Centers for Disease Control and Prevention. How flu spreads; 2018. Available from: https://www.cdc.gov/flu/about/disease/spread.htm.
6. Ip DK, Lau LL, Leung NH, et al. Viral shedding and transmission potential of asymptomatic and paucisymptomatic influenza virus infections in the community. Clin Infect Dis. 2017;64(6):736–742. doi:10.1093/cid/ciw841
7. Tsang TK, Lau LLH, Cauchemez S, Cowling BJ. Household transmission of influenza virus. Trends Microbiol. 2016;24(2):123–133. doi:10.1016/j.tim.2015.10.012
8. Lau LL, Nishiura H, Kelly H, Ip DK, Leung GM, Cowling BJ. Household transmission of 2009 pandemic influenza A (H1N1): a systematic review and meta-analysis. Epidemiology. 2012;23(4):531–542. doi:10.1097/EDE.0b013e31825588b8
9. Cauchemez S, Ferguson NM, Fox A, et al. Determinants of influenza transmission in South East Asia: insights from a household cohort study in Vietnam. PLoS Pathog. 2014;10(8):e1004310. doi:10.1371/journal.ppat.1004310
10. Chao DL, Halloran ME, Obenchain VJ, Longini IM
11. Hirotsu N, Wada K, Oshitani H, Cowling BJ. Risk factors of household transmission of pandemic (H1N1) 2009 among patients treated with antivirals: a prospective study at a primary clinic in Japan. PLoS One. 2012;7(2):e31519. doi:10.1371/journal.pone.0031519
12. Carrat F, Vergu E, Ferguson NM, et al. Time lines of infection and disease in human influenza: a review of volunteer challenge studies. Am J Epidemiol. 2008;167(7):775–785. doi:10.1093/aje/kwm375
13. Cowling BJ, Chan KH, Fang VJ, et al. Comparative epidemiology of pandemic and seasonal influenza A in households. N Engl J Med. 2010;362(23):2175–2184. doi:10.1056/NEJMoa0911530
14. Viboud C, Boelle PY, Cauchemez S, et al. Risk factors of influenza transmission in households. Br J Gen Pract. 2004;54(506):684–689.
15. Wardell R, Prem K, Cowling BJ, Cook AR. The role of symptomatic presentation in influenza A transmission risk. Epidemiol Infect. 2017;145(4):723–727. doi:10.1017/S0950268816002740
16. Cauchemez S, Donnelly CA, Reed C, et al. Household transmission of 2009 pandemic influenza A (H1N1) virus in the United States. N Engl J Med. 2009;361(27):2619–2627. doi:10.1056/NEJMoa0905498
17. Cowling BJ, Chan KH, Peiris JS, Riley S, Leung GM. Viral shedding, clinical history and transmission of influenza. Hong Kong Med J. 2013;19(Suppl 4):19–23.
18. France AM, Jackson M, Schrag S, et al. Household transmission of 2009 influenza A (H1N1) virus after a school-based outbreak in New York City, April-May 2009. J Infect Dis. 2010;201(7):984–992. doi:10.1086/651145
19. Thai PQ, Mai le Q, Welkers MR, et al. Pandemic H1N1 virus transmission and shedding dynamics in index case households of a prospective Vietnamese cohort. J Infect. 2014;68(6):581–590. doi:10.1016/j.jinf.2014.01.008
20. Fry AM, Goswami D, Nahar K, et al. Effects of oseltamivir treatment of index patients with influenza on secondary household illness in an urban setting in Bangladesh: secondary analysis of a randomised, placebo-controlled trial. Lancet Infect Dis. 2015;15(6):654–662. doi:10.1016/S1473-3099(15)70041-1
21. Ng S, Cowling BJ, Fang VJ, et al. Effects of oseltamivir treatment on duration of clinical illness and viral shedding and household transmission of influenza virus. Clin Infect Dis. 2010;50(5):707–714. doi:10.1086/650458
22. Ikematsu H, Hayden FG, Kawaguchi K, et al. Baloxavir marboxil for prophylaxis against influenza in household contacts. N Engl J Med. 2020;383(4):309–320. doi:10.1056/NEJMoa1915341
23. Pebody RG, Harris R, Kafatos G, et al. Use of antiviral drugs to reduce household transmission of pandemic (H1N1) 2009, United Kingdom. Emerg Infect Dis. 1993;83(12):990–999. doi:10.3201/eid/1706.101161
24. Kashiwagi S, Watanabe A, Ikematsu H, et al. Laninamivir octanoate for post-exposure prophylaxis of influenza in household contacts: a randomized double blind placebo controlled trial. J Infect Chemother. 2013;19(4):740–749. doi:10.1007/s10156-013-0622-9
25. Lochner KA, Wynne MA, Wheatcroft GH, Worrall CM, Kelman JA. Medicare claims versus beneficiary self-report for influenza vaccination surveillance. Am J Prev Med. 2015;48(4):384–391. doi:10.1016/j.amepre.2014.10.016
26. Schwartz KL, Jembere N, Campitelli MA, Buchan SA, Chung H, Kwong JC. Using physician billing claims from the Ontario Health Insurance plan to determine individual influenza vaccination status: an updated validation study. CMAJ Open. 2016;4(3):E463–E470. doi:10.9778/cmajo.20160009
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.