Back to Journals » Journal of Pain Research » Volume 12
Healthcare Costs And Resource Utilization In Chronic Pain Patients Treated With Extended-Release Formulations Of Tapentadol, Oxycodone, Or Morphine Stratified By Type Of Pain: A Retrospective Claims Analysis, 2012–2016
Authors Zah V ![]() , Brookfield RB
, Brookfield RB ![]() , Imro M
, Imro M ![]() , Tatovic S, Pelivanovic J, Vukicevic D
, Tatovic S, Pelivanovic J, Vukicevic D ![]()
Received 10 July 2019
Accepted for publication 19 October 2019
Published 8 November 2019 Volume 2019:12 Pages 3037—3048
DOI https://doi.org/10.2147/JPR.S222617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Überall
Vladimir Zah,1 Rowe B Brookfield,2 Martina Imro,1 Simona Tatovic,1 Jovana Pelivanovic,1 Djurdja Vukicevic1
1Health Economics and Outcomes Research Department, ZRx Outcomes Research Inc, Mississauga, Ontario, Canada; 2Field Medical Affairs, Depomed, Inc, Newark, CA, USA
Correspondence: Vladimir Zah
Health Economics and Outcomes Research Department, ZRx Outcomes Research Inc., 3373 Cawthra Road, Mississauga, Ontario, Canada
Tel/fax +14169534427
Email [email protected]
Purpose: Chronic pain treatment imposes a substantial economic burden on US society. Treatment costs may vary across subgroups of patients with different types of pain. The aim of our study was to compare healthcare costs (HC) and resource utilization in musculoskeletal (MP), neuropathic (NP), and cancer pain (CaP) patients treated with long-acting opioids (LAO), using real-world evidence.
Patients and methods: We compared total HC and resource utilization in subgroups of chronic pain patients (MP, NP or CaP) treated with three LAO alternatives: morphine-sulfate extended-release (MsER), oxycodone ER (OxnER) and tapentadol ER (TapER). Retrospective claims data were analyzed in the IBM Truven Health MarketScan® Commercial Claims Database (October 2012 through March 2016). All patients were continuously health plan enrolled for at least 12 months before the index date (first LAO prescription date) and during the LAO-treatment period. The cohorts were propensity-score matched.
Results: A total of 2824 TapER-treated patients were matched to 16,716 OxnER-treated patients, while 2827 TapER patients were matched to 16,817 MsER patients. The average monthly total HC were lower in the TapER than in the OxnER cohort ($2510 vs. $3720, p<0.001), reflecting significantly lower outpatient, inpatient and emergency department visit rates in the TapER cohort. Similarly, the TapER cohort exhibited a lower average monthly total HC ($2520 vs. $2900, p<0.05) than MsER cohort, with significantly fewer inpatient and outpatient visits in the TapER cohort. TapER demonstrated significantly lower total HC than OxnER in patients with NP and MP, and similar to OxnER in CaP patients. TapER costs were similar to MsER costs in all pain-type subpopulations.
Conclusion: Based on real-world evidence, the TapER treatment for chronic pain was associated with significantly lower HC compared with MsER or OxnER. When categorized by type of pain, TapER remained a less costly strategy in comparison with OxnER for MP and NP.
Keywords: long-acting opioids, real-world evidence, administrative database, cost analysis, subgroup analysis
Plain Language Summary
Given the huge economic burden of chronic pain treatment in the USA, this study aimed to evaluate healthcare costs and resource utilization among patients with chronic pain treated with different types of long-acting opioids.
We conducted a retrospective claims analysis to compare three treatment alternatives: morphine-sulfate extended-release (MsER), oxycodone ER (OxnER) and tapentadol ER (TapER) in subgroups of patients with musculoskeletal, neuropathic, and cancer-related pain.
The results of this study demonstrated a lower economic burden associated with the long-term tapentadol compared with either long-term oxycodone or morphine treatment among adherent chronic pain patients. When categorized by type of pain, tapentadol was less costly in subgroups of patients with musculoskeletal and neuropathic pain. In patients with cancer-related pain, the costs of TapER and OxnER were comparable. Total healthcare costs of TapER treatment were similar to MsER costs across all categories of pain.
Our findings can be used as an aid to clinical and healthcare policy decision-making related to chronic pain treatment, as they provide significant evidence on the comparative economic burden of commonly prescribed treatment alternatives in the real world setting.
Introduction
Chronic pain represents a complex condition defined as pain persisting beyond the period of tissue healing time, which is assumed to be three months.1 Clinical expert guidelines for treatment of chronic pain recommend a wide spectrum of options depending on symptom severity.2 Opioids are used to treat the chronic pain that responds poorly to other pain medications. The selection of opioid treatment should be guided by a set of factors, including individual patient characteristics, dosing schedule, costs of treatment, need for rescue therapy and frequency of adverse events.3 Long-acting opioids (LAO) are reserved for treatment of moderate to severe pain that requires around-the-clock analgesia.4,5 Furthermore, a twice-daily dosing schedule of these extended-release (ER) formulations is convenient for patients, potentially leading to better treatment adherence.6 Adherence to the opioid treatment is also an important criterion in clinical decision-making since it maximizes the patient benefits and minimizes the economic burden.7,8
Chronic pain management imposes a significant economic impact on the US health care system. More than 100 million US adults suffer from chronic pain conditions.9 The annual cost of pain management is estimated to be in the $560 ─ 635 billion range and exceeds the cost of heart disease, cancer and diabetes.9,10 One of the factors that affects total costs of chronic pain treatment is the underlying etiology of the condition. The LAO doses and healthcare service utilization rates are substantially higher in patients with cancer-related pain compared with those with non-malignant pain causes.11–13 Thus, it is not only important to realize the average cost and resource use per chronic pain patient, but having a better understanding of these outcomes based on the etiology of chronic pain will provide additional information for decision-makers. Studies assessing the economic impact of opioid treatments are commonly performed in subpopulations of non-cancer patients, failing to present a broader scope and to provide more general practical implications.14,15 On the other hand, non-cancer pain conditions may be further stratified according to the pain etiology. The most common non-cancer pain causes are neuropathic and musculoskeletal conditions.16,17 Since they require different patterns of management and treatment, the heterogeneity of healthcare resource consumption and costs may persist even in the non-cancer pain population. Furthermore, the LAO drug prescription costs may vary greatly depending on the patent protection ie, generic vs branded drugs.18 The cost difference is further influenced by the differences in healthcare service utilization and additional medications for breakthrough pain. No studies were previously published comparing healthcare costs and resource utilization of different LAO treatments in subpopulations of chronic pain patients.
Materials And Methods
Aim
The aim of this study was to explore healthcare utilization and total healthcare costs in adherent LAO-treated chronic pain patients, stratified into three groups based on the pain type – musculoskeletal pain (MP), neuropathic pain (NP) and cancer-related pain (CaP).
Data Sources
This was a retrospective claims database analysis conducted in the Truven Health Analytics MarketScan® Commercial Claims and Encounters Databases using data from October 2012 through March 2016 (Figure 1).
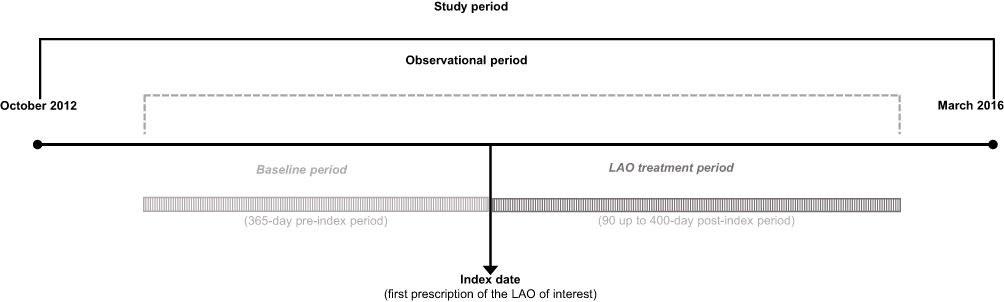 |
Figure 1 Study design. Abbreviation: LAO, long-acting opioid. |
The database contains eligibility, pharmacy claims and medical claims data for several million individuals and their dependents covered by the largest commercial health insurance plans in the US The databases are fully de-identified, and are thus in compliance with the rules established by the Health Insurance Portability and Accountability Act (HIPAA) Privacy Regulations.
Study Population
The study population was composed of patients who were 18–64 years old, diagnosed with any type of chronic pain and treated with LAOs: tapentadol extended release (TapER), oxycodone ER (OxnER) and morphine ER (MsER) between October 2012 and March 2016. The only product included in the TapER cohort was Nucynta®ER, while the OxnER and MsER cohorts consisted of all patients prescribed either generic or branded medications launched by 2016. Patients were assigned to one of the three mutually exclusive cohorts based on the initially prescribed treatment. Treatment crossover was not allowed. The index date was set as the date of the first LAO prescription. In order to meet eligibility criteria, patients were required to be prescribed with the initial LAO treatment for at least 90 and up to 400 days; to be continuously insured throughout the 12-month pre-index period and 90- to 400-day treatment period; and to be adherent to the LAO treatment (Figure 2). The proportion of days covered (PDC) was used as a measure of the record-based patient adherence to LAO treatment. The PDC was estimated as a proportion of days covered with LAO prescriptions within the treatment duration. The treatment duration was calculated as an interval from the first LAO claim to the end of the last LAO prescription fill during the observational period. The adherent treatment was defined as a PDC greater than 80%.
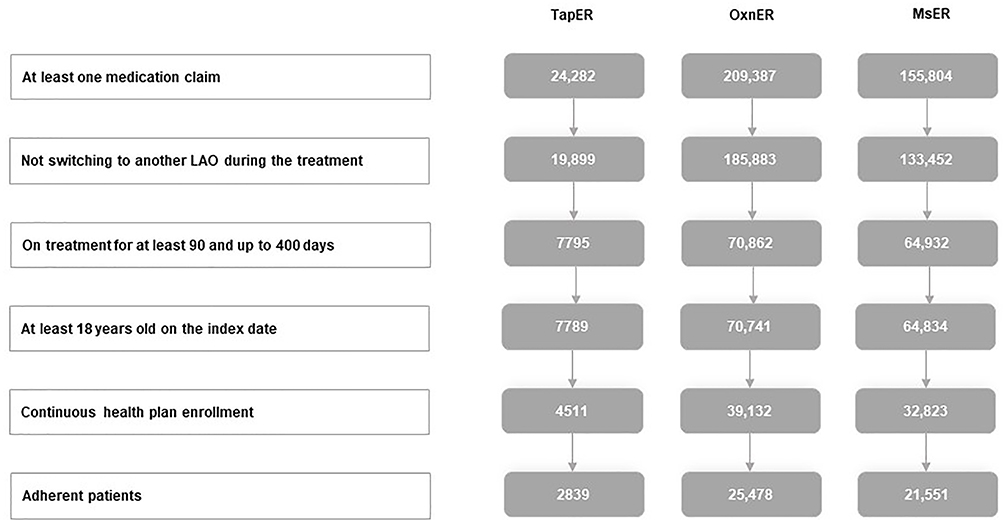 |
Figure 2 Patient attrition. Abbreviations: LAO, long-acting opioid; MsER, morphine sulfate extended release; OxnER, oxycodone extended release; TapER, tapentadol extended release. |
Demographics And Clinical Characteristics
Demographic and clinical characteristics of patients were assessed to describe the initial study sample. Demographic characteristics (age, gender, and geographic region of residence) were observed on the index date, while clinical characteristics (comorbidities included in Charlson comorbidity index (CCI)) were assessed during the pre-index baseline period. Diagnoses of different chronic pain types (NP, MP, CaP) were identified using the International Classification of Diseases, 9th and 10th Revision, Clinical Modification (ICD-9/10-CM) medical claims, during the pre-index and the LAO treatment period. A small number of patients were diagnosed with unspecific chronic pain conditions, such as chronic pain syndrome and unspecified abdominal pain, thus categorized into a separate subgroup. CCI was evaluated using ICD-9/10-CM medical claims recorded during the pre-index period, with respective weights assigned for each specific comorbidity. Details regarding the CCI evaluation process using administrative claims analysis were described elsewhere.19
Healthcare Cost And Resource Utilization
Healthcare costs and resource use were calculated during the treatment period, from the index date to the expiration of the last LAO fill. Because of the variable treatment duration, the results were presented as average monthly costs and resource utilization rates. Healthcare costs were composed of pharmacy and medical costs (outpatient, inpatient and emergency department (ED) costs). The pharmacy costs were comprised of LAO prescription costs and costs of concomitant medications. Healthcare resource utilization was observed through the rates of inpatient, outpatient and ED visits and the length of hospital stay. Total healthcare costs and resource utilization were compared among the treatment cohorts in chronic pain patients. The analyses were repeated in subpopulations of patients with specific type of pain: MP, NP, or CaP.
Statistical Analyses
Descriptive statistics were used to compare baseline demographics, clinical characteristics, healthcare resource utilization and costs for the eligible study sample. Due to significant differences in baseline characteristics (Table 1), chronic pain patients treated with TapER were propensity score matched to the OxnER patients and, separately, to the MsER patients, both in the ratio 1:6, using the nearest-neighbor matching algorithm. The maximum allowed caliper distance between the matched patients was 0.001. Propensity scores were calculated using the logistic regression model with the predictor variables presented in Table 2. Predictor and outcome variables were compared across the cohorts using the analysis of variance (ANOVA) and independent t-test for continuous variables or Chi-square test of independence for categorical variables. All statistical analyses were performed using the software package IBM SPSS Statistics version 23.0 for Windows. The threshold for statistical significance was 0.05.
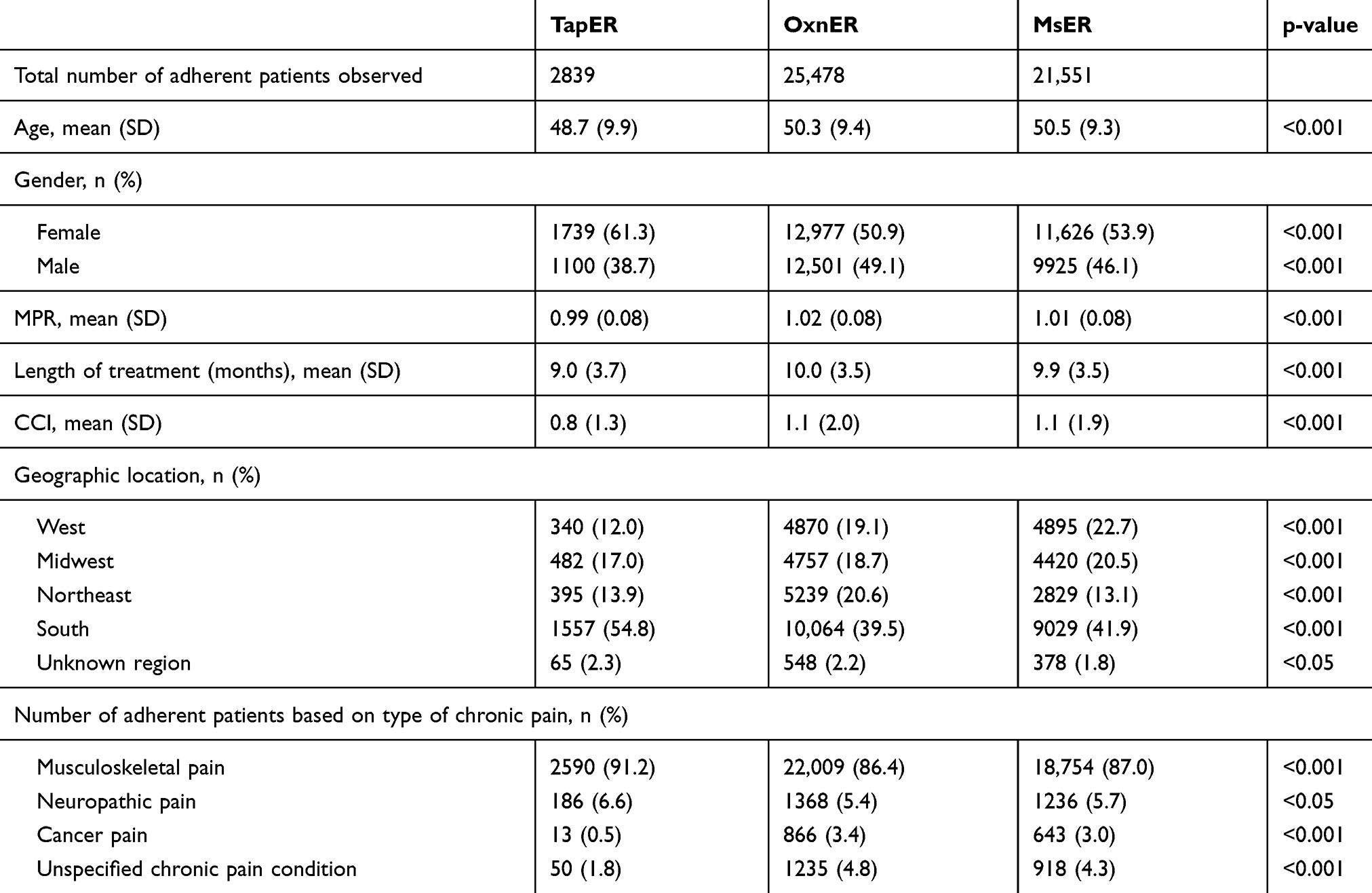 |
Table 1 Baseline Characteristics Of TapER, OxnER, And MsER Patients (Pre-matching) |
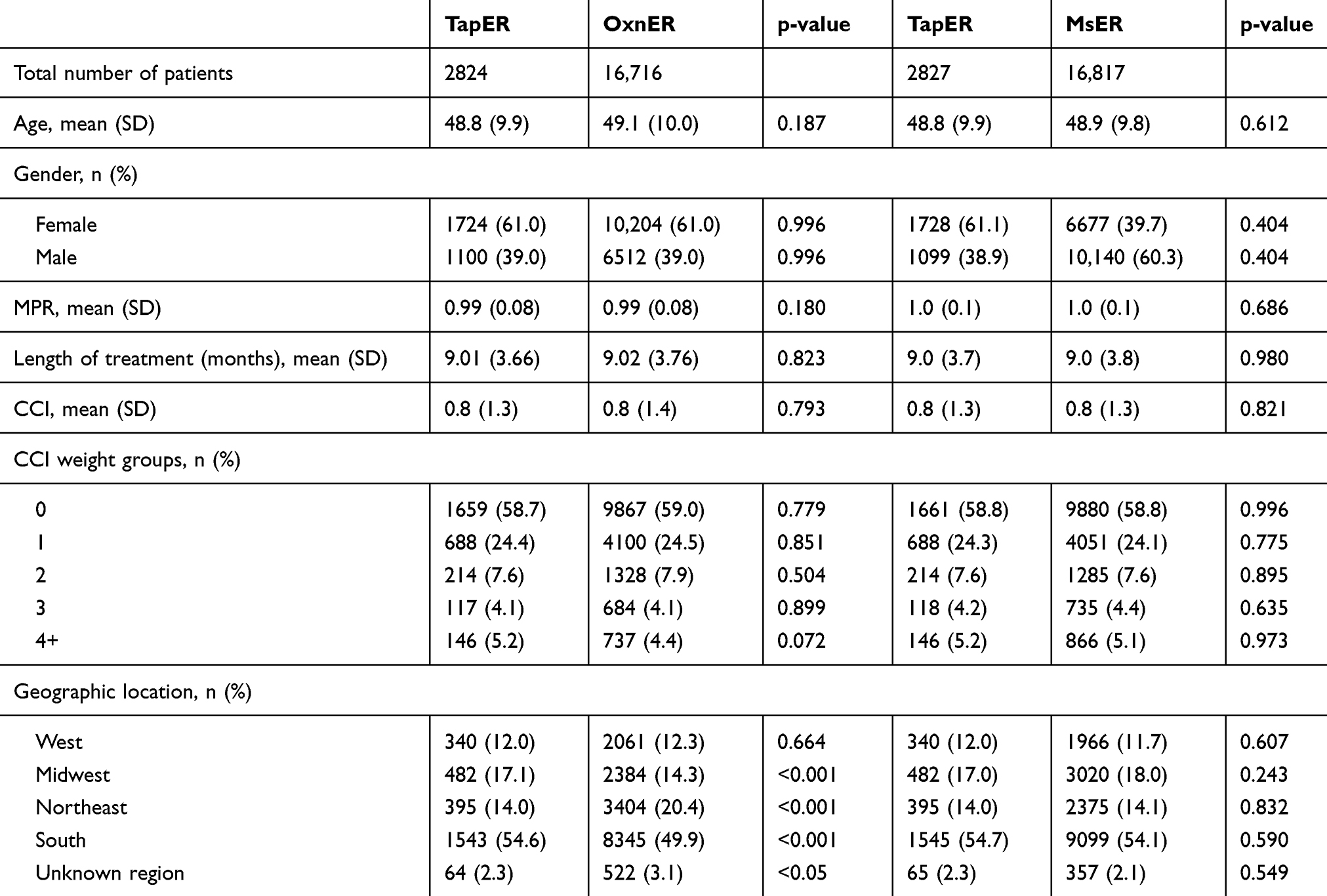 |
Table 2 Baseline Characteristics Of TapER Vs OxnER And TapER Vs MsER Patients After Matching |
Results
Characteristics Of The Study Sample
We identified a total of 49,868 patients eligible for a subsequent matching process. A total of 2824 TapER-treated patients were successfully matched to 16,716 OxnER-treated patients, while 2827 TapER patients were successfully matched to 16,817 MsER patients. Table 1 captures patients’ characteristics prior to propensity-score matching across the LAO cohorts. After the matching, key covariates did not differ significantly across the cohorts (p-values given in Table 2). The mean age of patients was approximately 50 years and comparable across the three cohorts, with a majority of female patients (roughly 60%). The average duration of all three treatments was approximately 9 months. The average CCI score was similar among the cohorts, suggesting the coexisting conditions were well-balanced.
Healthcare Costs And Resource Utilization In Chronic Pain Patients
The total healthcare costs of LAO treatment were lower in the chronic pain patients treated with TapER than in those treated with OxnER ($2510 vs $3720 per patient per month (PPPM), p<0.001) (Table 3). When observing the cost categories (Table 3), the outpatient, inpatient and ED costs were lower in TapER- than in OxnER-treated patients ($1030 vs $1570 PPPM for outpatient, $500 vs $1090 PPPM for inpatient, $100 vs $140 PPPM for ED costs; p<0.001, for all).
 |
Table 3 Average Monthly Healthcare Costs In Matched TapER Vs OxnER And TapER Vs MsER Patients |
When comparing TapER vs MsER, outpatient costs ($1030 vs $1330 PPPM, p<0.001), inpatient costs ($500 vs $860 PPPM, p<0.001), ED costs ($100 vs $150 PPPM, p<0.05), and total healthcare costs ($2520 vs $2900 PPPM, p<0.05) were lower in the TapER cohort. In contrast, the MsER pharmacy costs were lower than those of TapER, as presented in Table 3.
Similar trends were observed within the healthcare resource utilization patterns. The patients treated with TapER had a lower average number of hospitalizations and length of hospital stay, as well as lower rates of ED and outpatient visits than those treated with OxnER (Table 4). Compared with MsER, TapER-treated patients had a significantly lower mean number of hospitalizations (0.02 vs 0.04 PPPM, p<0.001), a shorter mean length of hospital stay (0.09 vs 0.19 days PPPM, p<0.001), a lower number of ED visits (0.07 vs 0.10 PPPM, p<0.001) and a lower number of LAO prescriptions (1.01 vs 1.03 PPPM, p<0.001) (Table 4).
 |
Table 4 Average Monthly Healthcare Resource Utilization In Matched TapER Vs OxnER And TapER Vs MsER Patients |
Healthcare Costs Categorized By Type Of Pain
The average total healthcare costs were significantly lower in NP and MP patients treated with TapER than in those treated with OxnER ($3490 vs $4640 PPPM, p<0.05 for NP; $2400 vs $3260 PPPM, p<0.001 for MP), while there was no difference between the compared strategies in patients with CaP ($13,580 vs $17,150 PPPM; p=0.415) (Table 5, Figure 3). Similar results were obtained when analyzing outpatient costs ($1180 vs $1730 PPPM, p<0.05 for NP; $1000 vs $1270 PPPM, p<0.001 for MP), inpatient costs ($710 vs $1510 PPPM, p<0.05 for NP, $460 vs $980 PPPM, p<0.001 for MP) and ED costs ($150 vs $190, p= 0.270 for NP; $90 vs $130, p<0.001 for MP). In patients with CaP, the only difference was denoted when comparing costs of concomitant medications that were lower in the TapER-treated patients ($410 vs $1640 PPPM, p<0.001) (Table 5).
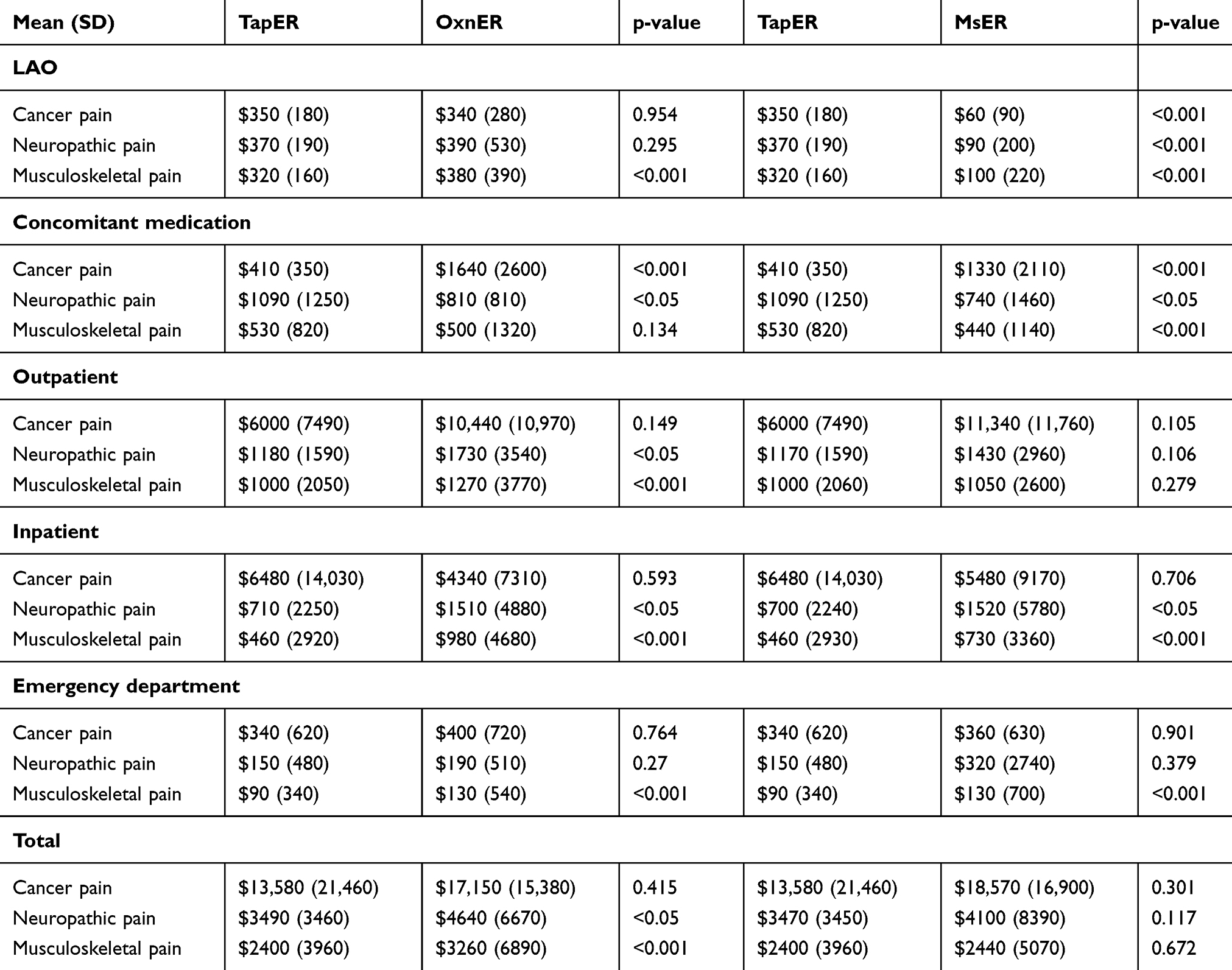 |
Table 5 Average Monthly Healthcare Costs Categorized By The Type Of Pain In Matched TapER Vs OxnER And TapER Vs MsER Patients |
Compared with MsER-treated patients, TapER-treated patients with NP and MP had significantly lower inpatient costs ($700 vs $1520, p<0.05 and $460 vs $730, p<0.001). Pharmacy costs were higher in the TapER cohort for all types of pain (Table 5). There was no significant difference in the total healthcare costs between the TapER- and MsER-treated patients regardless of the pain type (Figure 3).
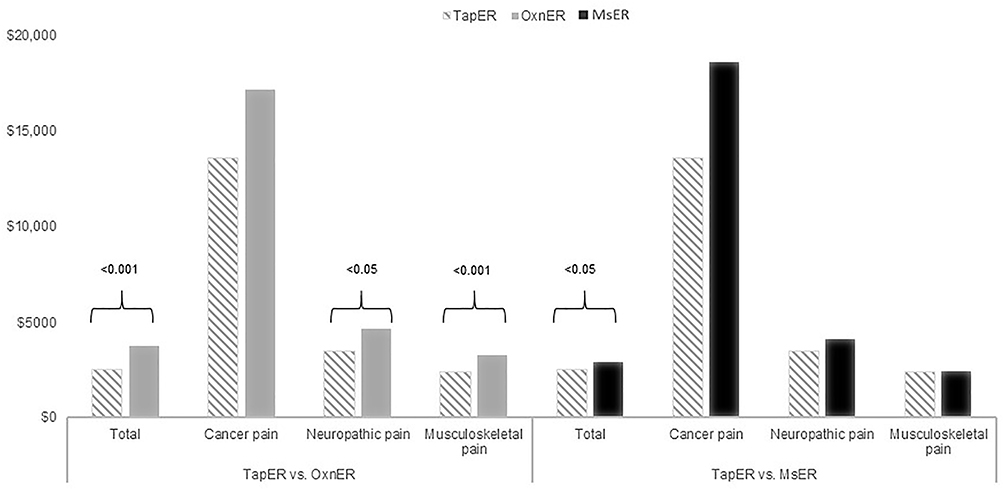 |
Figure 3 Average monthly costs per type of pain. Abbreviations: MsER, morphine sulfate extended-release; OxnER, oxycodone extended release; TapER, tapentadol extended release. |
Healthcare Resource Utilization Categorized By Type Of Pain
Healthcare resource utilization was higher in patients treated with OxnER than in those treated with TapER. Hospitalization rates, length of stay and ED visits were lower in NP and MP TapER-treated than OxnER-treated patients (Table 6). In the subpopulation of patients with CaP, healthcare utilization was generally similar in TapER- and OxnER-treated patients (Table 6).
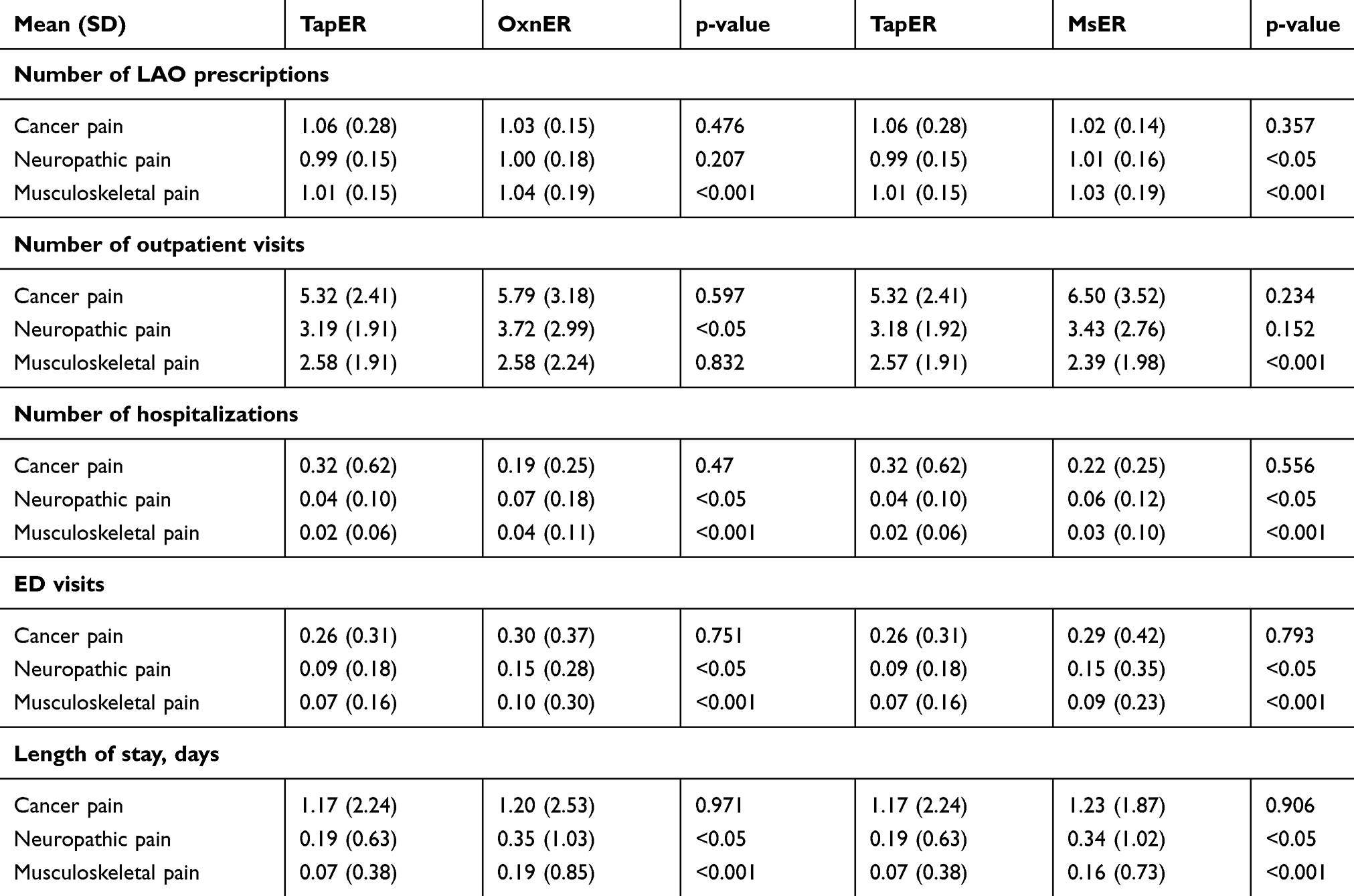 |
Table 6 Average Monthly Healthcare Resource Utilization Categorized By The Type Of Pain In Matched TapER Vs OxnER And TapER Vs MsER Patients |
For the subpopulation of CaP patients, healthcare resource utilization rates were also similar in the TapER compared to the MsER cohort. However, in NP and MP patients, hospitalization rates, length of hospital stay, number of ED visits and LAO consumption were significantly lower in TapER- compared with MsER-treated patients (Table 6).
Discussion
This retrospective study assessed the total healthcare costs of commercially insured chronic pain patients treated with different LAO treatments from a US healthcare payer’s perspective, based on real-world data. The study demonstrates a lower economic burden associated with the long-term tapentadol treatment compared with either long-term oxycodone or morphine treatment among adherent chronic pain patients. The estimated monthly total healthcare cost was approximately 30% higher among patients treated with OxnER than among those treated with TapER. Furthermore, the cost was approximately 15% higher for patients treated with MsER than for those treated with TapER, even though the MsER prescription cost was considerably lower ($100 vs $320 PPPM, respectively). The lower inpatient and outpatient cost components in the TapER cohort appear to be the main drivers of observed differences. Accordingly, the healthcare services utilization of TapER-treated patients was lower in both comparisons. TapER treatment is associated with less frequent outpatient visits and hospital admissions, a shorter duration of hospital stay, and less recurrent ED visits than both OxnER and MsER treatments. We aimed to estimate differences in the total healthcare costs of patients with distinct pain types treated with different LAO types, due to different management requirements for each LAO-treated condition. A majority of patients was diagnosed with MP, suggesting this was the most frequent chronic pain condition the LAOs are prescribed for. TapER appears to be a less costly treatment alternative compared with OxnER for MP and NP, while the treatments were comparable in the subpopulation of patients with CaP. Although the total healthcare costs of TapER-treated patients with chronic pain were significantly lower than costs of MsER-treated patients, the costs were similar when observing the subpopulations of patients with MP, NP, and CaP. This can be explained by the heterogeneity of patients with chronic pain, emphasizing the significance of etiology-specific analysis approach.
The healthcare service utilization was two to five times higher in patients with CaP compared with those with MP and NP. Consequently, the CaP treatment was associated with up to six-time higher costs than the therapy of MP and NP, which was expected due to the high cost of cancer treatment itself.
The cost of opioid treatment was reported in several real-world evidence studies. A retrospective claims analysis by Leider et al explored differences in annual total healthcare costs of the chronic opioid users compared with the matched non-opioid users. The study reported chronic pain opioid adherent users incurred annual total healthcare costs of $23,160.20 Despite the unequal follow up period, their results are in accordance with our results. Another retrospective study compared different patterns of LAO and short-acting opioid (SAO) treatment for the management of chronic pain in terms of healthcare costs. The study identified a single LAO treatment as the least costly alternative compared with SAO, a combination of LAO and SAO, and switching between SAO and LAO during the treatment. The estimated total healthcare cost for mono-LAO treatment was $4933, while the costs for mono-SAO and SAO-LAO combination were substantially higher.14 Direct comparison of the obtained results was challenging, as the authors reported the annual total healthcare cost within a heterogeneous group of LAO treatments disregarding patient adherence to analgesic treatment, while we assessed total healthcare cost per month among the chronic pain patients adherent to a specific LAO treatment.
As studies comparing the economic burden of different LAOs are lacking, our study contributes to the existing literature by adding real-world evidence about total healthcare costs associated with different opioid treatment types. Furthermore, the importance of this study is that it focuses on the subgroups of chronic pain patients with homogenous prognoses.
As reported in previous studies, TapER treatment offered significant clinical advantages over OxnER treatment for chronic pain patients.21–23 Results of a meta-analysis of randomized controlled trials demonstrated a lower incidence of adverse events and a lower risk of treatment discontinuation in TapER-treated compared with OxnER-treated patients.22 Rates of serious adverse events were compared among commonly prescribed opioid analgesics of varying potency in The Researched Abuse, Diversion and Addiction-Related Surveillance (RADARS®) System from 2012 through 2016.23 Results showed that the rates of serious adverse events were highest on hydromorphone (8.02 (7.42–8.65) per 100 kg of drug dispensed in MME), the lowest on tapentadol (0.27 (0.22–0.34) per 100 kg of drug dispensed), while the rate of serious adverse events on oxycodone was 1.74 (1.70–1.78) per 100 kg of drug dispensed.23 In addition to the list of clinical advantages TapER offers over OxnER, another post-marketing study confirmed an improved safety profile of TapER through its lower abuse liability. Butler et al reported that abuse was significantly less frequent in patients treated with TapER than in OxnER-treated individuals assessed for substance abuse problems (p<0.001). A retrospective cohort study evaluated the abuse liability of tapentadol compared with tramadol, hydrocodone, morphine, oxycodone, hydromorphone, and oxymorphone based on the Researched Abuse, Diversion and Addiction-Related Surveillance system RADARS® System data. The abuse and diversion rates among tapentadol users were significantly lower than in all other opioid cohorts when examined on the population level. The study results imply the low public health burden of tapentadol in comparison with other opioids.24 The reduced abuse prevalence of tapentadol compared with oxycodone among IR formulations was also observed.25–27
Furthermore, a cost-effectiveness analysis concluded that TapER provides convenient pain relief for a substantially higher number of patients, with a lower rate of common opioid-related adverse events, at a marginally higher direct payer’s total health care cost compared with OxnER.21 Our study observed a lower healthcare resource utilization associated with TapER treatment, which may be in line with the statements of an improved safety profile of TapER compared with OxnER. Several cost-effectiveness studies reported TapER as a dominant strategy in comparison with OxnER for MP treatment22 and as a first-line treatment of severe, chronic non-malignant pain28,29 and second-line treatment in the UK settings.29 A cost-effectiveness model analyzed from a perspective of a health care payer in Spain demonstrated that TapER is a cost-effective treatment strategy when compared with MsER, with an incremental cost-effectiveness ratio of €2656 per quality- adjusted life-year gained.28 A budget impact analysis recommended replacing 10% of oxycodone controlled-release formulary share with TapER as an optimal strategy for a reduction of the US healthcare budget spending, due to lower expenditures for managing opioid-related adverse events.30
There are multiple gaps in evidence-based knowledge of pain management.31 Most importantly, there is a lack of evidence to support an optimal practice in opioid prescribing. For this reason, it is important to weigh benefits, harms, and costs of commonly prescribed LAO treatment alternatives using real-world evidence. Although the retrospective claims analysis provides numerous advantages over other types of research methods, it has several limitations. Selection bias in retrospective claims analyses may occur because of the ICD-9/10-CM coding inconsistencies. The database used in the present study also did not include over-the-counter medications claims and their costs. Another potential limitation of this study represent a common restraint of propensity score matching - although the study groups were matched based on the relevant covariates identified through the regression analysis, there is always a possibility of unidentified covariates that may influence study outcomes. Factors that could have influenced healthcare costs and were not observed in the study were LAO doses and pain severity, with higher doses and stronger pain possibly resulting in higher healthcare costs. As the study was analyzed from the US healthcare payer perspective, we did not examine indirect costs of the opioid therapy, which could be a subject of future research.
Conclusion
The findings of the current study provide important evidence on comparative economic burden across commonly prescribed LAO treatment alternatives. Based on real-world evidence, the TapER treatment for chronic pain resulted in significantly lower costs compared with both MsER and OxnER. When categorized by type of pain, TapER remained a less costly strategy in comparison with OxnER for MP and NP, while the economic burden of the compared treatments was similar in the CaP patients.
The results of this study can aid to clinical and healthcare policy decision-making related to chronic pain. Establishing benefits, harms and long-term cost-effectiveness of LAO treatment alternatives in the US healthcare setting is suggested to be of high importance.
Abbreviations
CaP, cancer pain; CCI, charlson comorbidity index; ED, emergency department; ER, extended-release; HC, healthcare costs; HIPAA, Health Insurance Portability and Accountability Act; ICD-9/10-CM, International Classification of Diseases, 9th and 10th Revision, Clinical Modification; LAO, long-acting opioids; MP, musculoskeletal; MPR, Medication Possession Ratio; MsER, morphine-sulfate extended-release; NP, neuropathic; OxnER, oxycodone extended release; PDC, proportion of days covered; PPPM, per patient per month; RADARS®, The Researched Abuse, Diversion and Addiction-Related Surveillance; SAO, short-acting opioid; TapER, tapentadol extended release.
Acknowledgments
We thank Michael DeGeorge, PharmD and Steven D. Passik, Ph.D. (Collegium Pharmaceutical, Inc.) for comments on the manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
RB was an employee of Depomed, Inc. at the time of this research. VZ, MI, ST, JP, and DV are employees of ZRx Outcomes Research Inc. At the time of the research, Depomed, Inc. had the license for the commercialization of tapentadol in the U.S. VZ, MI, ST, JP, and DV declare financial support from Depomed, Inc. and Collegium Pharmaceutical, Inc. for the research. The authors report no other conflicts of interest in this work.
References
1. Classification of Chronic Pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of pain, subcommittee on taxonomy. Pain Suppl. 1986;3(S1).
2. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–49. doi:10.15585/mmwr.rr6501e1
3. Fine PG, Mahajan G, McPherson ML. Long-acting opioids and short-acting opioids: appropriate use in chronic pain management. Pain Med. 2009;10 Suppl 2:S79–S88. doi:10.1111/j.1526-4637.2009.00666.x
4. Nicholson B. Benefits of extended-release opioid analgesic formulations in the treatment of chronic pain. Pain Pract. 2009;9(1):71–81. doi:10.1111/ppr.2009.9.issue-1
5. Gudin JA. Assessment of extended-release opioid analgesics for the treatment of chronic pain. J Pain Palliat Care Pharmacother. 2013;27(1):49–61. doi:10.3109/15360288.2012.757575
6. Graziottin A, Gardner-Nix J, Stumpf M, Berliner MN. Opioids: how to improve compliance and adherence. Pain Pract. 2011;11(6):574–581. doi:10.1111/ppr.2011.11.issue-6
7. Manchikanti L, Atluri S, Trescot AM, Giordano J. Monitoring opioid adherence in chronic pain patients: tools, techniques, and utility. Pain Physician. 2008;11(2 Suppl):S155–S180.
8. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35–44. doi:10.2147/RMHP.S19801
9. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
10. Institute of Medicine (US) Committee on Advancing Pain Research C, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington (DC): National Academies Press (US); 2011.
11. Davis MP, Glare PA, Hardy J, Quigley C. Opioids in Cancer Pain. Oxford University Press; 2009.
12. Sondergaard J, Christensen HN, Ibsen R, Jarbol DE, Kjellberg J. Healthcare resource use and costs of opioid-induced constipation among non-cancer and cancer patients on opioid therapy: a nationwide register-based cohort study in Denmark. Scand J Pain. 2017;15:83–90. doi:10.1016/j.sjpain.2017.01.006
13. Gustavsson A, Bjorkman J, Ljungcrantz C, et al. Socio-economic burden of patients with a diagnosis related to chronic pain–register data of 840,000 Swedish patients. Eur J Pain. 2012;16(2):289–299. doi:10.1016/j.ejpain.2011.07.006
14. Landsman-Blumberg PB, Katz N, Gajria K, et al. Health care resource use and cost differences by opioid therapy type among chronic noncancer pain patients. J Pain Res. 2017;10:1713–1722. doi:10.2147/JPR
15. Kern DM, Zhou S, Chavoshi S, et al. Treatment patterns, healthcare utilization, and costs of chronic opioid treatment for non-cancer pain in the United States. Am J Manag Care. 2015;21(3):e222–e234.
16. Dworkin RH. An overview of neuropathic pain: syndromes, symptoms, signs, and several mechanisms. Clin J Pain. 2002;18(6):343–349. doi:10.1097/00002508-200211000-00001
17. Staats PS, Silverman SM. Controlled Substance Management in Chronic Pain: A Balanced Approach. Switzerland: Springer; 2016.
18. Office Of The Assistant Secretary For Planning And Evaluation (ASPE). Expanding the use of generic drugs; 2010. Available from: https://aspe.hhs.gov/basic-report/expanding-use-generic-drugs.
19. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
20. Leider HL, Dhaliwal J, Davis EJ, Kulakodlu M, Buikema AR. Healthcare costs and nonadherence among chronic opioid users. Am J Manag Care. 2011;17(1):32–40.
21. Neil N, Merchant S, Provenzano D, Ogden K, Mody SH. Clinical simulation model of long-acting opioids for treatment of chronic non-cancer pain in the United States. J Med Econ. 2013;16(2):307–317. doi:10.3111/13696998.2012.756401
22. Coluzzi F, Ruggeri M. Clinical and economic evaluation of tapentadol extended release and oxycodone/naloxone extended release in comparison with controlled release oxycodone in musculoskeletal pain. Curr Med Res Opin. 2014;30(6):1139–1151. doi:10.1185/03007995.2014.894501
23. Murphy DL, Lebin JA, Severtson SG, Olsen HA, Dasgupta N, Dart RC. Comparative rates of mortality and serious adverse effects among commonly prescribed opioid analgesics. Drug Saf. 2018;41(8):787–795. doi:10.1007/s40264-018-0660-4
24. Vosburg SK, Severtson SG, Dart RC, et al. Assessment of tapentadol API abuse liability with the researched abuse, diversion and addiction-related surveillance system. J Pain. 2018;19(4):439–453. doi:10.1016/j.jpain.2017.11.007
25. Butler SF, McNaughton EC, Black RA. Tapentadol abuse potential: a postmarketing evaluation using a sample of individuals evaluated for substance abuse treatment. Pain Med. 2015;16(1):119–130. doi:10.1111/pme.12524
26. Cepeda MS, Fife D, Vo L, Mastrogiovanni G, Yuan Y. Comparison of opioid doctor shopping for tapentadol and oxycodone: a cohort study. J Pain. 2013;14(2):158–164. doi:10.1016/j.jpain.2012.10.012
27. Dart RC, Cicero TJ, Surratt HL, Rosenblum A, Bartelson BB, Adams EH. Assessment of the abuse of tapentadol immediate release: the first 24 months. J Opioid Manag. 2012;8(6):395–402. doi:10.5055/jom.2012.0139
28. Obradovic M, Ikenberg R, Hertel N, Antonanzas F, Galvez R, Liedgens H. Cost-effectiveness of tapentadol in severe chronic pain in Spain: a cost analysis of data from RCTs. Clin Ther. 2012;34(4):926–943. doi:10.1016/j.clinthera.2012.02.011
29. Ikenberg R, Hertel N, Moore RA, et al. Cost-effectiveness of tapentadol prolonged release compared with oxycodone controlled release in the UK in patients with severe non-malignant chronic pain who failed 1st line treatment with morphine. J Med Econ. 2012;15(4):724–736. doi:10.3111/13696998.2012.670174
30. Merchant S, Noe LL, Howe A, et al. Budget impact analysis of tapentadol extended release for the treatment of moderate to severe chronic noncancer pain. Clin Ther. 2013;35(5):659–672. doi:10.1016/j.clinthera.2013.03.016
31. Chou R, Ballantyne JC, Fanciullo GJ, Fine PG, Miaskowski C. Research gaps on use of opioids for chronic noncancer pain: findings from a review of the evidence for an American Pain Society and American Academy of Pain Medicine clinical practice guideline. J Pain. 2009;10(2):147–159. doi:10.1016/j.jpain.2008.10.007
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.