Back to Journals » Risk Management and Healthcare Policy » Volume 14
Health Technology Assessment in High, Middle, and Low-income Countries: New Systematic and Interdisciplinary Approach For Sound Informed-policy Making: Research Protocole
Authors Alkhaldi M, Al Basuoni A, Matos M, Tanner M, Ahmed S
Received 24 March 2021
Accepted for publication 26 May 2021
Published 28 June 2021 Volume 2021:14 Pages 2757—2770
DOI https://doi.org/10.2147/RMHP.S310215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mohammed Alkhaldi,1– 4 Aisha Al Basuoni,5 Márcia Matos,1 Marcel Tanner,2,3 Sara Ahmed1
1School of Physical and Occupational Therapy, Faculty of Medicine, McGill University, Montreal, Canada; 2Department of Public Health, University of Basel, Basel, Switzerland; 3The Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, Basel, Switzerland; 4Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine; 5Projects Unit, Gaza Community Mental Health Programme, Gaza, Palestine
Correspondence: Mohammed Alkhaldi Email [email protected]
Abstract: Technological innovation has a significant role in improving health systems (HSs) and achieving universal health coverage (UHC). The World Health Organization (WHO) has declared resolutions on Health Technology Assessment (HTA) and other global organizations emphasized on HTA systems to achieve the Sustainable Development Goals (SDGs). HTA is a modern multidisciplinary decision-making framework linking knowledge and policymaking by assessing the medical, social, economic, organizational, and ethical effects, and/or impacts within health and social systems. The research significance lies in the growing need for HTA at these moments than ever as it is seen as an essential development approach to tackle the current global challenges and pandemics, particularly in developing countries. The research aims to comprehensively evaluate and understand HTA systems concerning the level of knowledge about HTA, current HTA structure, practices, application, capacity, gaps, and solutions. The project starts in January 2021 and ends in January 2022 and will be carried out in seven countries: Canada, Switzerland, Brazil, Lebanon, Jordan, Palestine, and Tanzania. A mixed-methods, quantitative and qualitative, along with a literature review will be applied. In each country, ten HTA-associated institutions will complete an adapted electronic survey, developed by the WHO, and ten key-informants selected purposively from the government, academia, NGOs, and private sectors to participate in ten individual in-depth interviews. One government representative from each country will participate in one expanded inter-country workshop. Excel, IBM Statistical Package for the Social Sciences (SPSS), and MAXQDA software programs will be used for data management and analysis. The research will form cutting-edge evidence not only for the seven countries, but also for the global, regional, and national endeavors with regards to opening a room for HTA best application and optimization. It will reveal lessons learned, determine gaps, and build a well-enabled and institutionalized HTA for better UHC, health systems, and multi-sectoral development.
Keywords: HTA systems, health systems, health policy and decision-making, HMLICs
Background
Technological innovation has a significant role in improving healthcare delivery and universal health coverage, where the World Health Organization (WHO) and other global health organizations emphasize supporting regional and national Health Technology Assessment (HTA) systems. A growing interest in HTA and its eventual institutionalization in low and middle-income countries (LMICs) is driven in part by WHO’s recommendation for it to be a critical component to achieving UHC.1 Integrating HTA within a country’s health innovation system would help in the smooth convergence of technology, innovation and policy for addressing systemic gaps.2 HTA is immensely increasing not only in developed countries but also in developing countries. It reduces resource waste, inefficiencies, and inappropriate investments in Health Systems (HSs). As being a tool for a strategy of evidence-based decision-making, HTA can help address issues relating to both affordability and equity when allocating resources.3 HTA is a multidisciplinary decision-making process that uses information about the medical, social, economic, organizational, and ethical issues related to the use of growing health technologies and interventions such as information and communication technology, E-Health, electronic health records, medical devices, diagnostic devices, clinical interventions, medicines, vaccines, and practice management solutions. HTA involves a rigorous review of new technologies, not just in terms of their added clinical utility but also often with an eye toward cost-effectiveness. Assessing the effectiveness and optimal utilization of these interventions within the health and social systems using sound methodological evaluation, assessments, and analyses like HTA is indispensable before being introduced into practice.4–6 As it is a framework that bridges research and policymaking, this evaluation provides evidence to decision-makers and ensures the value of money and resources7,8 by evaluating properties, effects, and/or impacts.9 HTA may be seen as a development strategic question that needs to be addressed institutionally, nationally, regionally, and globally. Specifically in countries with limited HTA institutionalization, formalizing a system for HTA will reinforce the efforts for achieving UHC and promote good value for money while ensuring the provision of suitable healthcare services for the population.10 And recently, the first HTA on a COVID-19 innovative health technology (from India) shows the value of HTA in providing evidence on efficiency, equity and quality of SARS-CoV-2 testing policy.2 Implementing HTA is particularly important to improve health surveillance, HS management, health education, and clinical decision-making, and to support behavioral changes related to public-health priorities and long-term diseases management.
Research Significance and Rational
Globally, HTA receives great attention and is seen as a development approach. WHO has declared resolutions to adopt HTA as an essential approach to tackle global challenges, improve HSs and achieve the Sustainable Development Goals (SDGs).11 The rationale behind conducting this research is that, in developed countries, HTA is rapidly growing, for example, Canada and Switzerland, are two leading countries in this field despite some challenges in their HTA systems independence, methodology, translation, and application.12,13 As the less-resourced developing countries are in more need of HTA, there are considerable unrecognized gaps in HTA understanding, practice, and utilization. Regionally, Figure 1 reveals that 52% of the Middle East countries are performing and utilizing HTA or HTA-like activities, which means that 48% are still not performing HTA-like activities. Furthermore, using HTA in the decision-making process was viewed as the biggest obstacle.14,15 Healthcare interventions and technologies in the Middle East region, with all its components, innovation, regulation, assessment, and management, remain a major challenge.16 Therefore, Brazil, Lebanon, Palestine, and Tanzania are essentially in need of HTA to manage the scarcity and misallocation of the resource on one hand, and to tackle many challenges that represent a large proportion of the burden of disease on another hand.8,9,17–19
 |
Figure 1 Eastern Mediterranean Region spending on research compared with the share of global wealth. |
The importance of this research stems from insufficient knowledge and literature about the HTA in the region and specifically in the three countries, Brazil, Lebanon, Palestine, and Tanzania. The research will advance the existing evidence on the subject and will generate optimal knowledge translation strategies for useful HTA frameworks and models, which is the focus of this research. While in developed countries such as Canada and Switzerland, HTA at the local and provincial levels needs to be assessed for further improvement and importantly transferring the successful adapted models and experience to our developing countries. Therefore, the approach of evaluating HTA from various settings and contexts is useful where it will develop reliable evidence, insights, and comparisons to be added to the current knowledge advancement and for innovating further global and regional best practices of HTA. The ideation of this research emerged from the Principal Investigator’s (PI) Ph.D. project, which dealt with analyzing the whole health research system in Palestine targeting three sectors: academic, government, and local and international organizations. Both topics, Health Research System (HRS) and HTA, are organically linked to each other, which both urged for planning and implementing health interventions and making decisions based on research and evidence. The key recommended policy advice was implementing health policy and systems research (HPSR) and using innovative and evidence-based approaches and instruments to support the evidence-informed decision-making in the health sector in Palestine.20 Figure 2 illustrates that Evidence-informed policy-making for health should be driven by six essential pillars, and HTA is one of them that is required to be assessed and strengthened.6,8,15
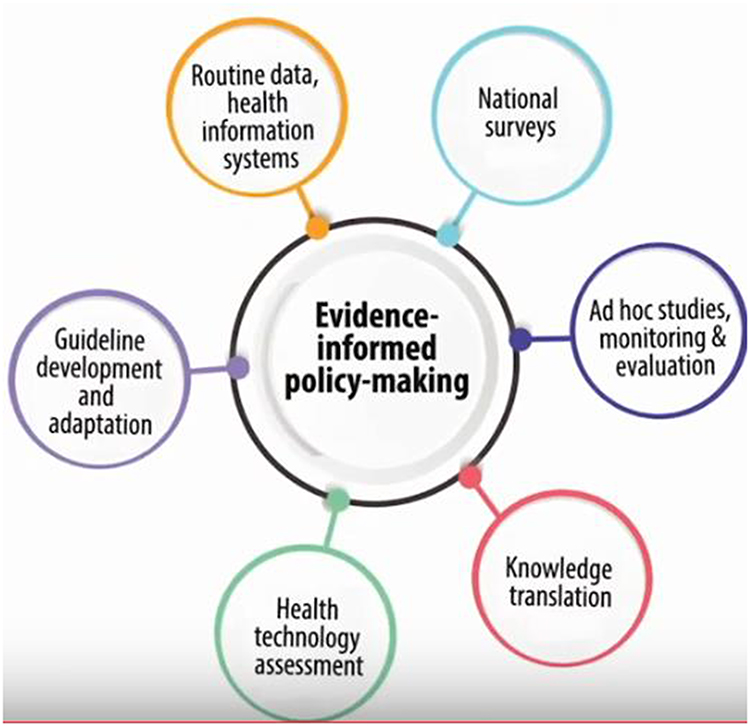 |
Figure 2 Six key pillars of the Evidence-informed policy-making for health. |
Additionally, HTA is addressing such an interdisciplinary approach that incorporates various sectors and disciplines to collaborate together to employ technology, science, and health research to strengthen our HSs and to solve our communities’ problems is an optimal goal and crucial demand.4 In this context, investigating HTA systems in the seven selected countries may also open a new horizon for fostering SDGs achievement in these countries with a focus on the three developing countries (Brazil, Lebanon, Jordan, Palestine, and Tanzania).
Research Theoretical Framework
Figure 3 shows the framework of the proposed pillars of the research that will be investigated. It embraces five essential components; HTA conceptualization, implementation, capacity, gaps, and strengthening strategies, as they are clearly covered in the objectives section.
 |
Figure 3 The analysis framework of the HTA system. |
Research Aim and Objectives
Given the World Bank income classification, the selected countries were classified as follows: Canada and Switzerland as high-income countries, Brazil and Lebanon as upper-middle-income countries, Jordan and Palestine as lower-middle-income countries, and Tanzania as a low-income country (see Table S1). The overall aim of this research is to comprehensively understand the HTA systems and evaluate the current technologies of the HSs using HTA in these seven countries through the following specific objectives:
- Assess the understanding level among stakeholders on HTA concept, importance, and practices;
- Explore the HTA applicability, capacities, and utilization in health decision and policy-making process;
- Evaluate the extent to which and how current health technologies and interventions are examined using HTA;
- Identify gaps and propose feasible solutions such as a framework to support best practices for HTA and knowledge translation strategies in national and regional arenas.
Research Question(s) and/or Hypothesis (Es)
The research is expected to answer the following questions:
- Is the concept, functions, and practices of HTA understood by HTA stakeholders in selected countries? The research assumed that there is a varying and inadequate level of conceptualization and knowledge about HTA and that this hinders its strengthening in the health sectors.
- Is the implementation of health technologies and interventions managed and applied appropriately, evaluated systematically, and actively used in the decision-making and planning process? And are HTA systems in the five settings, mainly in developing countries, are capacitated and resourced enough? The hypothesis is that technologies and interventions are unsystematically or might be inappropriately applied and evaluated as HTA is non-institutionalized and used in health decision-making, especially in LMICs.
- Are HTA stewardship capacity and financial and human resources are varied and exist but misapplied and misallocated, largely in developing countries.
- Are there differences between the seven contexts in terms of the current HTA practices and interventions, HTA knowledge level, application, capacity, and barriers? There is an assumption that there are significant differences and countries may share the same and different practices and interventions related to HTA aspects.
- Are there differences between the seven contexts in terms of challenges and barriers? There is an assumption that there are significant differences and countries may share the same challenges and barriers related to HTA aspects.
- Will the strengthening framework or roadmap fit the seven contexts and other similar countries and lead to achievable results? It is assumed that the framework may vary from one environment to another with the belief that this framework will make the advancement of practices, strategies, and interventions possible if HTA is appropriately acknowledged, embraced and applied.
Methodology
Study Design
The research is a cross-sectional study and will apply mixed methods; quantitative and qualitative methods along with a literature review to address these three dimensions: 1) the conceptual dimension of HTA concepts, functions and usage, 2) the technical and functional dimension in terms of HTA applicability and capacity, and 3) gaps and solutions identification for HTA institutionalization and strengthening.
Study Setting/Data Sources
The uniqueness that the research will be conducted in seven different countries selected based on the World Bank income classification; Canada, Switzerland, Brazil, Jordan, Lebanon, Palestine, and Tanzania to figure out differences, similarities, gaps, successes, and lessons learned among these settings. In each country, ten institutional surveys, ten in-depth interviews (IDIs), and one expanded inter-country focus group discussion (FGD) workshop will be conducted with health experts, policymakers, academicians, and managers selected purposively from the 1st, 2nd, and 3rd levels of the HS structure and its departments. Thus, intensive consultations to sort out comprehensive lists of institutions and participants based on pre-defined criteria and conditions will be approached. The participants from the seven settings will be mainly invited from these top levels of the government sector (Ministry of Health and relevant departments and ministries), academic, and private and non-governmental organizations. Different sampling strategies will be used to maximize representation and knowledge saturation and reduce bias. IDIs and FGD are selected as the best supplementary method along with the survey to meet the aims of this study. Both are useful methodologies to obtain information on perspectives and experiences of a homogenous group of people related to a common topic as well as a heterogeneous group descending from different contexts, disciplines, sectors, and leadership classes. This will facilitate discussions and produce a variety of ideas in a short time among participants. Data from literature review, as a secondary source, will be used such as published and unpublished national, regional, and international reports, briefs, articles, studies, facilities’ records, and bulletins to complement the primary data. Pilot studies for the quantitative and qualitative tools are expected to be tested in the field in May 2021 and its findings will be consulted with peers.
Study Population and Inclusion and Exclusion Criteria
This research has two categories of populations. The first is a group of all health institutions, whether governmental, academic, private, or non-governmental institutions, that operate in the health sector in each country and meet the following inclusion criteria: each institution has to be officially recognized, active at least one year since its establishment, has mission and task in HTA stewardship, production, and funding; has any previous or current programs, projects or interventions that directly or indirectly related to HTA; or participates/ed in one or more of HTA activities. The second population is the entire group of people who are working in different departments, units, and centers in these HTA-associated institutions in seven countries. Those individuals who are responsible for and working in the field of HTA could be either health experts, academicians, policymakers, managers, or professionals. They have to be officially holding positions in HTA at three different levels of the HS at both local and national administrative systems of the country: 1st policy level, 2nd managerial level, and 3rd technical and operational level. The institutions and their departments that have no direct or indirect role in HTA and do not meet the inclusion criteria will be excluded. This certainly applies to individuals as well. To explore and identify the lists of HTA-associated institutions and individuals, two methods will be conducted 1) a rapid review of grey and published literature, and 2) an extensive consultation with a pre-defined collaborator in each country. These methods will give information that leads to preparing two types of lists for each country, a) a list of existing local and national participating institutions, up to ten institutions or perhaps less, depending on the availability of HTA institutions in the country; b) a list of individuals that includes ten personnel who are working in or running these institutions. The sample size of individuals and strategies of sampling will be explained in the next sub-section.
Sampling Method
For the institutions, a simple purposive sampling will be used to select all major HTA-associated institutions, up to ten and at least five institutions from each country, from the list established in a prior based on country collaborator’s consultations supported by a quick systematic literature review. For the individuals, a mixed sampling method will be approached to build a final list of ten key informants and participants from each country based on the country’s collaborator consultations and literature review. To reach a large representation of all sectors, institutions, and three policy, managerial, and technical levels in each country, probability and non-probability sampling methods using various sampling strategies will be used as follows: simple sampling, critical case, snowballing, convenience, and self-identified sampling. In each country of the seventh countries targeted in this study, the ten participants involved in HTA in the ten institutions will be recruited as follows: two local and national decision and policy-makers, one independent expert, one academician, one private representative, one NGO representative, two managerial participants, and two technical participants. Those ten participants will be invited for individual IDIs. In another word, ten IDIs in each country and seventy IDIs in total will be conducted in all targeted seven countries. Lastly, using the same sampling methods, the country collaborator will be asked to nominate one highly-represented participant from the HTA from each country field to participate in one expanded FGD that gathers seven participants representing the seven participating countries.
Sample Size (Sample Size Assumptions/Estimate)
The sample size of the participating HTA-associated institutions from different sectors, government, academic, private, and NGOs is likely to be ten or less in each country, it should be up to ten and not less than five institutions. The number of institutions depends on the availability or the existence of institutions already functioning in the HTA or indirectly involved in the field. The estimated total number of individuals in each country will be ten participants for IDIs and one highly represented participant to be invited for FGD. Overall, seventy-seven participants from all seven countries will be directly participating in the two main activities: IDIs (70) and FGD (7).
Data Collection (Data Collection Methods and Tools)
This research will use four data collection tools as follows:
- The literature review by conducting a systematic review based on the seven pre-defined themes, understanding HTA, use and application, implementation, goverance, capacity, and gaps and solutions, to extract relevant data from published and unpublished local, regional, and international relevant resources such as institutions’ websites, articles and magazines, scientific repositories and databases, and knowledge platforms about the institutions’ work and HTA components or themes under investigation.
- Seventy electronic institutional surveys on HTA are expected to be administered to all participating institutions of the seventh countries. The survey will be designed using McGill’s REDCap cloud-based clinical software application. The final adapted questionnaire that was developed by the WHO is supplemented with this proposal (Supplement 1. An official invitation describing the research objectives and activities will be sent to the head of each institution to get approval. One electronic survey will be sent to every institution among ten or fewer institutions selected from each country. In each country, every institution will have an internal working team that will be formed from the managerial and technical staff. A team leader from the institution will be internally nominated to lead this team to be a contact person. The team will be instructed virtually on the process of survey completion and then giving them one month, expected in April or May 2021, to complete and send this survey online. The survey covers six essential parts (themes) of the HTA:
- Understanding and Perceptions of HTA Application
- The use and application of HTA in the health-sector decision-making process
- Implementation Processes of HTA
- Stewardship capacity (governance and management)
- Resources supporting HTA processes.
- Interests and impediments to strengthening the capacity.
- Ten IDIs with key informants from all sectors, government, academia, private, and NGO, that are involved in HTA will be conducted in each country. In Sampling Method, types, classes, numbers, and selection strategies of the ten were explained. To gain a holistic and diverse understanding, ten participants from each country will be demonstrating the perspectives on HTA from three levels of the country HS, policy, managerial, and technical. The interviews will be conducted via a web audio-video conferencing platform (Zoom communications Inc., 2020) and each interview will last between 45–60 minutes. This complementary qualitative tool, Supplement 2 will dig deeper into further wide-ranging and similar HTA themes covered in the quantitative survey. These semi-structured interviews will be run based on a written guide that will be emailed along with the invitation, consent form, and short description on the study to the participants before conducting the IDI. To avoid bias, similar sampling strategies will be used and one research team led by the PI and assisted by a local collaborator will carry out the interviews using one English language. The local collaborator will assist in translation if the participant is unable to communicate in English. The research team will apply the same strategy about data management, translation, transcription, and quality check and validity feedback. An additional quality and validity check will be applied among the countries in general and within the country in terms of sectors and leadership levels.
- One expanded inter-country FGD that consists of seven participants from all seven targeted countries. From each country, one policymaker who represents the MOH, or Public Health department, or the HTA agency will be invited to the FGD. Before the FGD, documents that comprise a description of the research, the consent form, and the FGD meeting guide will be emailed to the participants. An online tool (Doodle) will be used to find a common time across all participants from the seven countries for the FGD and for the IDIs alike. The FGD will be held via a web video-conferencing platform (Zoom Video Communications Inc., 2020). The FGD will last 60 minutes to focus on five key questions or themes: the current importance of HTA, evaluation of the current policies, capacities, and practices of HTA systems, needs and priorities, and limitations and solutions. The PI will moderate the FGD accompanied by two assistants, the first as an observer and the second as a note-taker. This also will be applied in the IDIs. An electronic package of documents consists of an invitation, FGDs questions guide, and workshop agenda and instructions will be sent to all seven participants before the FGD. At the end of each IDI and FGD, verbal summaries will be provided to participants to ensure the clarity and accuracy of the content. After a while, participants of IDI and FGD will receive a synthesis of results to comment on to ensure trustworthiness and validity. Using Zoom for the IDIs and FGD has a key advantage because of its ability to securely record and store meetings without recourse to third-party software. This particular feature is essential in research where the protection of highly sensitive data is required. Other essential security features include user-specific authentication, real-time encryption of meetings, and the ability to backup recordings to secured McGill servers or local drives.
The above-mentioned four tools are designed to address main three dimensions that derived from the study objectives: 1) the conceptual dimension of HTA concepts, functions and usage, 2) the technical and functional dimension in terms of HTA applicability and capacity, and 3) gaps and solutions identification for HTA institutionalization and strengthening. To make this feasible, a specific plan with a defined timeline, instructions, preparation, roles, names, and expected deliverables will be constructed to guide the collection data measures. This will be managed and guided by the PI in close collaboration with the co-investigators and the country’s collaborators. The adapted survey and IDIs questions were subjected to a rigorous review and consultation process done by ten eminent experts, scholars, and professors from leading institutions around the world from the USA, Canada, UK, Tunisia, Australia, Switzerland, Palestine, and South Africa. All feedback and comments from them were appropriately incorporated.
Data Management Plan
Specific criteria for the literature review, such as identifying sources, relevant materials, and aspects (themes) to focus on, will be defined to conduct a meaningful systematic review. Data from the literature review will be managed, organized, and categorized using an Excel program. All data from the survey, IDI, and FGD, will be stored on secure McGill servers and only accessible by authorized members of the research team. If participants withdraw and ask for data to be removed, their data will be discarded and not included in the final data set. Quantitative data from the online survey will be collected automatically using the RedCap cloud of McGill University, stored in a secured server, and then imported to the IBM Statistical Package for the Social Sciences (SPSS) for data management and analysis. IDIs and FGD qualitative data will be audio-recorded and then simultaneously translated and transcribed in English into MS word sheets by the PI assisted by trained co-investigators. Transcripts will then be revised for precision, checking, and cleaning for accuracy and quality. Transcripts will be imported to the software program, MAXQDA 12 (VERBI GmbH, Berlin) for qualitative data management and analysis. Descriptive and inferential quantitative analysis and thematic qualitative analysis will be conducted using the abovementioned software programs. The methodological approach of this research was built based on similar reliable international studies.19,21–23
Data Analysis
Descriptive statistics will be used to summarize the characteristics and the information to survey for all institutions. Data extracted from the literature will be descriptive using the Excel software program to support findings from other tools. Data from the survey will be analyzed to produce different descriptive statistics using the SPSS software program. Descriptive statistics for institutional details and other sixth domains of the surveys will be conducted. These are the following quantitative analyses that will be used: percentages, frequency distribution, categories, means, standard deviation, and comparative metrics among countries or institutions. For the qualitative data, different steps will be approached as follows: First, short debriefings, notes, and summaries will be organized and discussed with the moderator, assistants, and reviewers after each IDI and FGD. All recorded qualitative data will be translated into English language if required and transcribed verbatim by the research assistants and immersed themselves in the data by repeatedly reading and listening to the recordings to become familiar with the content and document initial meanings arising. Second, the PI will perform a double check by selecting randomly a group of transcripts to ensure texts quality and accuracy. Third, two coders and co-investigators will conduct data coding. The PI along with two independent reviewers will verify the final or main codes that reflecting the explicit objectives of the study. All transcripts will be imported to the MAXQDA and categorized into two data groups: IDIs and FGD. The two coders will read line by line to create codes to look for concepts/ideas in the text by dragging the transcripts texts and linking each quote, line, or passage to the relevant code. In this research, these codes will be in a predetermined coding system derived from the research objectives. Two independent reviewers will verify the codes, themes, and check the associations between them to resolve any discrepancies contributing to the consistency of the findings. Fourth, codes rating will be performed to identify meaningful patterns, themes, and categories using four types of analysis as follows: content, framework, thematic, and ground theory. This deductive analysis approach will be used to test the pre-constructed hypotheses described in Research Question(s) and/or Hypothesis (Es). Different features that will promote the trustworthiness, credibility, and reflexivity of this research are: 1) triangulation of data sources and methods, 2) peer debriefing, review, and consultation coupled with the PI critical check for reliability, consistency, and consensus purposes; 3) the shared summary of the IDI and FGD with participants for feedback and coding reviewers check.
Coordination, Monitoring and Quality Control Plan
McGill University in Canada is the host institution of this project and this will be an important element in supporting the project implementation in all aspects, scientifically, technically, and logistically. Three essential coordination and quality assurance will be followed to make the fieldwork successful and feasible:
- Strong collaboration is already established with partners and collaborators from the Middle East countries such as Philadelphia University in Jordan, the American University of Beirut in Lebanon, MENA health policy forum in the regional and Palestine offices, Ifakara Health Institute (IHI) in Tanzania. In Europe, an established network with the Swiss Tropical and Public Health Institute in Switzerland could be the potential collaborating institution. Having an existing collaboration with academic collaborators in Brazil who are affiliated with institutions such as Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde (CONITEC) could also a catalyst to perform the data collection properly. This broad well-established network will support this research intervention and fieldwork in particular for three purposes: 1) providing useful scientific and technical consultations, 2) facilitating all country fieldwork, and 3) assisting in knowledge translational activities. Having such inter-country, regional, and international networks and outstanding research and advisory teams, this research project will be a reality and it will exactly meet the stated goals.
- Solid fieldwork consists of specific activities, timeline, responsible persons, roles, and expected outcomes and indicators for the four tools will be established before the implementation of a project to measure the work progress, achievement, and deliverables. In addition to the research team led by the PI, one well-trained and specialized research assistant from each country will be recruited in addition to co-investigators support. One training and coaching session will be conducted to train assistants and co-investigators on the whole process of the project and providing them specific technical techniques and skills.
- Data collection process, starting from search strategies and building tools, will be strictly governed by a mixed scientific team from all partners and settings in a collaboration with the PI and co-investigators. This is to collaborate in building robust strategies and tools, ensuring appropriate data collection, guarantying good data management and protection, and then designing appropriate and standardized data analysis approaches based on clear indicators and conditions developed from consultations and scientific evidence.
Ethical Considerations
This research deals with experts, policymakers, and managers, and administrative approval is essential will be taken from the health authorities from each country to access the institutions to implement the activities. In this research, there is no human subjects’ experimentation or trials to obtain ethical approvals. However, three kinds of ethical approvals from countries were obtained in 2020 and 2021, particularly from the national Helsinki ethics committee in Palestine (number PHRC/HC/732/20), the institutional review board of Philadelphia University in Jordan, and the approval from McGill ethics institutional board in Canada ((Info-Ed File Number: 21-04-009. /IRB Number: A04-E13-21A). Further approvals from other implementing and collaborating institutions may be requested. An official letter on the research along with a project summary and documents will be submitted to the administrations of the participating institutions in the seven countries to receive their administrative approval. The PI and team members will initially contact potential participants to provide them with a copy of the research information sheet to get their individual consent form. The expected limitations of obtaining the ethical, administrative, and individual approvals can be time-consuming. This can be managed earlier before the stage of implementation through receiving support from the host university, partners and collaborators, and effective communications.
Discussion
HTA is an effective tool to support priority setting and generate evidence for decision making especially en route to achieving UHC.24 HTA has been hypothesized to play a significant role in improving healthcare delivery and UHC through developing reliable evidence, insights, and comparisons to be added to the current knowledge advancement and for innovating further global and regional best practices of HTA.
With a noticeable rise of technologies being developed to address the COVID-19 situation, the role of HTA in addressing medical, ethical, economic, and social implications of a policy decision becomes even more important, however, while the use of HTA to inform policy decisions is well established in the high- income and upper-middle-income countries, its use and application in HSs has been limited in LMICs.2 HTA has been increasingly considered to support health policy decisions in the MENA region.25
The deteriorating scarce resources in most LMICs, cannot ensure that everyone obtains health services at an affordable price. Therefore, priority-setting processes are necessary to maximize the HS’s ability to work towards UHC due to limited healthcare resources and insufficient health revenue to satisfy increasing and competing demands.24 This study will provide a comprehensive understanding of the HTA systems in different income levels of the countries. While there are notable LMIC exceptions of introducing and institutionalizing HTA, others may be constrained by limited technical and administrative capacity, scarcity of data, time and governance structures to carry out HTA.1 This study will evaluate the current technologies of the HSs, identify gaps and propose feasible solutions to support best practices for HTA and knowledge translation strategies at the national and regional arenas. Eventually, recognizing the efficient use of resources is a crucial factor for ensuring the sustainability of HSs and achieving UHC.10
To our knowledge, this will be the first research on HTA conducting in seven different countries selected based on the World Bank income classification; Canada, Switzerland, Brazil, Jordan, Lebanon, Palestine, and Tanzania, and it is a unique attempt in terms of research scope and inclusive approach. It is expected to produce a thorough evidence-based framework highlighting the differences, similarities, gaps, successes, and lessons learned among these settings. The research will encourage the state’s officials to make serious decisions for strengthening HTA at national, regional, and global levels to strengthen the resilience and capacity of HSs in developing countries specifically in emergency settings to respond effectively during pandemics.
The research design will engage health experts, managers, and policymakers from the seven settings from both gender and structural levels of the HS in each country including levels of the government sector (Ministry of Health and relevant departments and ministries), academic, and private, and NGOs. The mixed participants from the policy, management, and technical levels will lead to better professional representation, inclusive different mindsets, and discipline to effective HTA implementation.
Findings from this research will inform health service planners and policymakers to strengthen the practice of HTA during decision-making, resource allocation, protection and prevention, detection and diagnostics, and therapeutics. Thus, its implementation is expected to improve health surveillance, HS management, health education, and clinical decision-making, and to support behavioral changes related to public-health priorities and long-term disease management.
The research may face some constraints used to exist in LMICs such as the limited capacity, data, time and priority setting governance structures to carry out HTA. The scarcity of literature on HTA in LMICs may pose a constraint but to address this, we will broaden our search scope by including published and unpublished resources that reflect the landscape of HTA. Limitations related to obtaining ethical, administrative, and individual approvals, which can be time-consuming. This will be managed earlier before the stage of project implementation through receiving support from the partners and systematic communications and using the WHO ethical and administrative official approvals to be submitted along with the project documents. The spread of COVID-19 pandemic and infection risks might limit the movement and face-to-face interviews. This can be mitigated by using virtual remote communication. In addition, some potential challenges of the preoccupation of HS actors from the front line management in LMICs. This can be managed by engaging the 1st, 2nd, and 3rd levels of the HS structure in each country in the assessment.
In terms of HTA implementation research, coordination and quality control is a key to success. We are aware that time constraints and workload of each stage may vary, but we are confident that intense communication during the HTA tools application, monitoring and continuous discussions could improve participants’ contribution to this study. Zero potential biases will be guaranteed due to the various HTA scientific data collection tools (surveys, IDIs, and FGDs), and the contribution of the 1st, 2nd, and 3rd levels of the HS structure in each of the seventh countries.
Implications
This research yields tremendous direct and indirect benefits where its outputs target various beneficiaries, groups, and stakeholders at the local, regional, and global levels in the short or long term on the field of HTA that will lead to better healthcare priority setting.The research project has two kinds of beneficiaries that will be benefiting from the outcomes of the implementation of the project; direct and indirect beneficiaries. Direct will be: 1) policymakers, decision-makers, health planners, health officials, thinkers, experts, and strategists exist in the national HS in each county, 2) heads, managers, and directors of various public health departments, such as planning, public health and epidemiology, primary healthcare, hospital, health economic, health information, and pharmaceuticals and supplies, 3) directors and representatives of non-state actors and organizations such as private sector, non-governmental organizations, national institutions, and community-based organizations, 4) scientific community and researchers for further research attempts. The main benefit for this group, number four, is assisting the first three beneficiaries in the existing strategies and plans and providing the best practices and feasible solutions. While beneficiaries who will be indirectly benefiting are the population and people (healthcare consumers) in the seven countries in particular and other many countries sharing the same context and classification of the countries targeted in this research. This indirect benefit could be tangible in the long-term by enjoying a sufficient level of healthcare accessibility, coverage, equity, affordability, and quality if the HTA best practices are appropriately applied and institutionalized.
There are significant contributions and outcomes expected to be accomplished from this research as follows:
- An online global knowledge exchange forum will be hosted that will include groups of countries’ representatives, policymakers, collaborators, partners, experts, scientists, and students to discuss and review results and develop an action plan for the working group.
- Advance an innovative triangulated analytic framework to be applied in different contexts and a comparative analysis of the seven different settings, including Canada and Switzerland, will be introduced to enrich the national and international knowledge libraries and to complement the gap in light of literature limitations.
- As the HTA is dependent on several country-specific factors such as the proportion of public investment in health, political support, access to good quality health information and technology infrastructure. With the rising cost of healthcare, HTA can be a useful tool to inform decision-making about UHC and promote an equitable, efficient, and high-quality HS.10
- The research findings, reinforced by the Canadian and Swiss HTA models, can be a benchmark for the countries for better strategies and tools for HTA systems.
- Further specific assessments are needed to investigate HTA management and methodology in the developed countries like Canada and Switzerland despite the plenty of literature.11,12,19,23 In contrast in developing countries, as deep contextual assessments are still needed, for instance, HTA was not examined in Palestine and insufficiently investigated in Brazil, Lebanon, and Tanzania.
- Knowledge production and translation: four papers will be published in prestigious journals, a book on HTA will be designed for research and education purposes, 5 dissemination workshops will be held, HTA Webinars and learning platform will be established, and policy briefs will be produced. In these expected papers, the results will be presented and structured based on the pre-defined themes. Every paper may address one or two themes. This means that results generated from the three methods will be combined and presented in a complementary approach in each paper. All papers combined will portray the comprehensive landscape of the HTA systems in the seven countries. The expected papers will jointly be co-authored by the set of authors engaged in this research as follows:
- Paper 1: AlKhaldi M, Al Basuoni A, Amorim M, Tanner M, Ahmed S. Assessment of the level of knowledge and understanding on HTA among state and non-state stakeholders in high, middle, and low-income countries. Health Policy and Systems Research (HPSR, BMC).
- Paper 2: AlKhaldi M, Al Basuoni A, Amorim M, Tanner M, Ahmed S. A landscape analysis of HTA applicability, capacities, and utilization in health decision and policy-making process in high, middle, and low-income countries: evidence synthesis. The International Journal of Health Policy and Management (IJHPM).
- Paper 3: AlKhaldi M, Al Basuoni A, Amorim M, Tanner M, Ahmed S. Mapping of HTA in regards to bold question: how current health technologies and interventions are examined using HTA in selected countries?: a mixed-methods analysis. Health Policy and Technology (HPT).
- Paper 3: AlKhaldi M, Al Basuoni A, Amorim M, Tanner M, Ahmed S. Pitfalls and strengthening strategies of HTA systems in high, middle, and low-income countries. The International Journal of Technology Assessment in Health Care (IJTAHC), Cambridge University Press.
About contribution to the relevant scholarly literature, there is an abundance of literature covering the subject of HTA in developed countries. In contrast, the literature on HTA in LMICs still needs further deep contextual assessments to reflect a clearer landscape of HTA. Most of these countries have an utmost necessity for HTA in their HSs owing to the scarcity of resources and the specificity of challenges. For instance, HTA did not examine in Palestine, and at the same time, it is insufficiently investigated at the country and regional levels of Lebanon and Tanzania. Therefore, this research seeks to fill this relatively wide knowledge gap through updating and advancing novel knowledge and evidence to inform both communities, scientific and decision making, in selected countries. This evidence can assist scientists to build supplementary knowledge and can encourage the state’s officials to make serious decisions for strengthening HTA at national and regional levels. This will be a cross-cutting research that provides evidence within rarely investigated studies in the Middle East region, that will further strengthen with the academic collaborations to generate replicable findings, address challenges, and offer solutions for better applications of HTA which will be reflected in strengthening the HSs as a whole. Also, the research will utilize and modify internationally modified tools, and will mix both qualitative and quantitative methodologies in data collection. Moreover, the construction of the research in comparing the different settings in different countries will provide and build a robust enhanced evidence-based decision-making and useful knowledge for other HSs and its outcomes in similar countries and communities.
Recalling the WHO health innovation working group alignment of the health innovation with the dimensions of UHC, then improving the performance of the HS will be an overarching goal of health innovation.
It is time for adopting new useful and interdisciplinary approaches such as HTA to strengthen the resilience and capacity of HSs in developing countries to respond effectively to pressing health challenges, including the current and future pandemics.
Conclusion
This research will generate optimal knowledge translation strategies for useful HTA frameworks and models benefiting mainly the low and least developed settings through adopting HTA as an essential approach to improve HSs and tackle existing challenges, particularly in developing countries as they share most of the health burdens in our regions and worldwide.
The research will form cutting-edge evidence and reference not only for the seven countries, but also for the global, regional, and national endeavors with regards to opening a room for HTA best application and optimization based on the produced knowledge from this research. It will reveal lessons learned, determine gaps, and set an applicable strengthening framework for HTA. This framework will eventually aid the decision and policymakers in these countries, and other similar countries and international organizations to build a well-enabled and institutionalized HTA for better UHC, HSs, and multi-sectoral development.
Data Sharing Statement
As mentioned earlier, the confidentiality of participants’ perceptions and data will be anonymously classified and appropriately stored in a secured server of McGill University with protected accessibility. These data are stored in a highly secured system with a secured entry, under the control of the PI (MK) and the supervisor (SA), and only they have the right of accessibility to review and use these data through a secured institutional system. Confidentiality and anonymity will be also applied when coded and analyzed data are published.
Acknowledgments
This research received technical support and scientific advice from professors and experts from various international institutions. We show special gratitude to the following professors and experts who reviewed the protocol and put their useful scientific inputs and made additional enrichment insights. The experts are as follows: Prof. Kaspar Wyss, Director of Swiss Centre for International Health in Switzerland; Prof. Yehia Abed, Al-Quds University, Palestine; Dr. Hamza Abdeljawad, Al-Quds University, Palestine; and Dr. Abdulsalam Khayyat, An-Najah National University, Palestine. Exceptional gratitude to the ten global experts, scholars, and professors who contributed in commenting on tools that led to good improvement. Experts and professors as follows: Dr. Irene Anne Jillson, Georgetown University-USA; Kirsty Kaiser, COHRED-South Africa; Dr. Mouna Jameleddine Chtioui, Chair of the ISPOR MENA HTA-Tunisia; Dr. Wesam Mansour, Liverpool School of Tropical Medicine (LSTM)-UK; Prof. Renato Mattli, Zurich University of Applied Sciences-Switzerland; Prof. Kaspar Wyss, Swiss TPH-Switzerland; Dr. Anke Holtorf, Health Outcomes Strategies-Switzerland; Dr. Loai Albarqouni, Bond University-Australia; Dr. Hamza Abdeljawad, Al-Quds University-Palestine; and Dr. Tatiana Villacres, McMaster University-Canada. Special thank and appreciation to the following country collaborators who provided all necessary support and collaboration: Dr. Ken Bond, Institute of Health Economics-Canada, Dr. Aline Silva, HTAi-Brazil, Dr. Ola El Zein, AUB-Lebanon, Dr.Fadwa Al Halaiqa, Philadephia University-Jordan, Prof. Matthias Schwenkglenks, University of Basel-Switzerland, Dr. Mwifadhi Mrisho and Dr. Abdallah Mkopi, Ifakara Health Institute-Tanzania, and Dr. Rana Khatib, MENA Health Policy Forum-Palestine.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
The research received various generous funding to cover the monthly stipend of the PI for one year. It is supported financially by the Lindsay Foundation Grant at CIUSSS Centre-Sud-de-l’Ile-de-Montréal in the amount of CAD 35,000 per annum. The project also received two small grants; ($ 6000) from a USA-based center, Palestinian American Research Center (PARC), through a one-year Research Fellowship. These three funding will be declared in the four manuscripts that will be produced from the project. The research team seeking to attract funding to finance other important technical and logistical needs in seven countries.Disclosure
Prof. Dr. Marcel Tanner reports personal fees from University Hospital Basel Board, Fondation Botnar Board, Gebert-Rüf Foundation Board and R. Geigy Foundation, Board, outside the submitted work. The authors declare that they have no other competing interests.
References
1. Nemzoff C, Ruiz F, Chalkidou K, et al. Adaptive health technology assessment to facilitate priority setting in low-and middle-income countries. BMJ Global Health. 2021;6(4):e004549. doi:10.1136/bmjgh-2020-004549
2. Mukherjee K. Integrating technology, innovation and policy: COVID-19 and HTA. Health Policy Technol. 2021;10(1):16–20. doi:10.1016/j.hlpt.2021.01.003
3. MacQuilkan K, Baker P, Downey L, et al. Strengthening health technology assessment systems in the global south: a comparative analysis of the HTA journeys of China, India and South Africa. Glob Health Action. 2018;11(1):1527556. PMID: 30326795; PMCID: PMC6197020. doi:10.1080/16549716.2018.1527556
4. Banta D. The development of health technology assessment. Health Policy. 2003;63(2):121–132. PMID: 12543525. doi:10.1016/s0168-8510(02)00059-3
5. Ritrovato M, Faggiano FC, Tedesco G, Derrico P. Decision-oriented health technology assessment: one step forward in supporting the decision-making process in hospitals. Value Health. 2015;18:505–511. doi:10.1016/j.jval.2015.02.002
6. WHO, EMRO, Regional Committee For Theme/RC66/R.5. Sixty-sixth Session Agenda item 3(d) developing national institutional capacity for evidence-informed policy-making for health; October, 2019. Available from: https://applications.emro.who.int/docs/RC66-R5-eng.pdf?ua=1.
7. WHO, Regional Office for South-East Asia. SEA/RC66/R4 - Health intervention and technology assessment in support of universal health coverage; 2013. Available from: https://apps.who.int/iris/bitstream/handle/10665/128271/SEA-RC-66-R4-UHC.pdf?sequence=1&isAllowed=y.
8. WHO, EMRO, 2014. Pre-RC61 session on “Health Technology Assessment (HTA)”: a tool for evidence-informed decision making in health; May 14, 2021. Available from: http://www.emro.who.int/pdf/about-who/rc61/health-technology-assessment.pdf?ua=1.
9. Garrido M, Kristensen F, Nielsen C, Busse R For the WHO, the European Observatory on Health Systems and Policies. ISBN 978 92 890 4293 2: UK; 2008.
10. Sharma M, Teerawattananon Y, Dabak SV, et al. A landscape analysis of health technology assessment capacity in the Association of South-East Asian Nations region. Health Res Policy Syst. 2021;19(1):1–13. doi:10.1186/s12961-020-00647-0
11. Dankó D. Health technology assessment in middle-income countries: recommendations for a balanced assessment system. J Mark Access Health Policy. 2014;2:23181. doi:10.3402/jmahp.v2.23181
12. Brügger U, Horisberger B, Ruckstuhl A, Plessow R, Eichler K, Gratwohl A. Health technology assessment in Switzerland: a descriptive analysis of “Coverage with Evidence Development” decisions from 1996 to 2013. BMJ Open. 2015;5(3):e007021. doi:10.1136/bmjopen-2014-00702
13. Menon D, Stafinski T. Health technology assessment in Canada: 20 years strong? Value Health. 2009;12(Suppl 2):S14–9. PMID: 19523180. doi:10.1111/j.1524-4733.2009.00554.x
14. World Health Organization. 2015 Global survey on health technology assessment by National Authorities. Main findings; 2015. Available from: https://www.who.int/health-technology-assessment/MD_HTA_oct2015_final_web2.pdf.
15. WHO, EMRO. Health technology assessment (HTA): a tool for evidence-informed decision making in health.
16. The Middle East North Africa Health Policy Forum, Health Technology Assessment (HTA) for Universal Health Coverage. A report of the First Regional Conference on Health Technology Assessment Conference organized by the MENA HPF. Cairo, Egypt; 2019. Avilable from: https://syndicateofhospitals.org.lb/Content/uploads/SyndicateMagazinePdfs/3695_4-11.pdf.
17. Oortwijn W, Mathijssen J, Banta D. The role of health technology assessment on pharmaceutical reimbursement in selected middle-income countries. Health Policy. 2010;95:174–184. doi:10.1016/j.healthpol.2009.12.008
18. World Health Organization. Sixty-seventh World Health Assembly: programme of meetings. Geneva: Palais des Nations; May 19–24, 2014. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_JOUR4-en.pdf.
19. World Health Organization. Global Survey on Biomedical Engineering Professionals in Health Technology Assessment. Springer; 2017:595–598.
20. AlKhaldi M. Palestinian Health Research System: moving Forward [Doctoral Thesis]. Basel: University of Basel, Faculty of Science; 2018. Available from: https://edoc.unibas.ch/64963/1/PhD%20thesis%2C%20PHRS%2C%2027.5.18.%202%20.pdf.
21. Lessa F, Ferraz MB. Health technology assessment: the process in Brazil. Rev Panam Salud Publica. 2017;41:e25. PMID: 28614463; PMCID: PMC6660842. doi:10.26633/RPSP.2017.25
22. Oortwijn W, Broos P, Vondeling H, Banta D, Todorova L. Mapping of health technology assessment in selected countries. Int J Technol Assess Health Care. 2013;29:424–434. doi:10.1017/S0266462313000469
23. Tantivess S, Chalkidou K, Tritasavit N, Teerawattananon Y. Health technology assessment capacity development in low- and middle-income countries: experiences from the international units of HITAP and NICE. F1000Research. 2017;6:2119. doi:10.12688/f1000research.13180.1
24. Uzochukwu BSC, Okeke C, O’Brien N, et al. Health technology assessment and priority setting for universal health coverage: a qualitative study of stakeholders’ capacity, needs, policy areas of demand and perspectives in Nigeria. Global Health. 2020;16:58. doi:10.1186/s12992-020-00583-2
25. Fasseeh A, Karam R, Jameleddine M, et al. Implementation of health technology assessment in the Middle East and North Africa: comparison between the current and preferred status. Front Pharmacol. 2020;11:15. doi:10.3389/fphar.2020.00015
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.