")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Health-Related Quality-of-Life and Associated Factors Among Children and Adolescents with Type 1 Diabetes Mellitus: A Cross-Sectional Study
Authors Bekele BT , Demie TG , Worku F
Received 28 February 2022
Accepted for publication 14 June 2022
Published 22 June 2022 Volume 2022:13 Pages 243—256
DOI https://doi.org/10.2147/PHMT.S364454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Roosy Aulakh
Bisrat Tamene Bekele,1 Takele Gezahegn Demie,2 Frehiwot Worku2
1Clinical Governance and Quality Improvement Directorate, Zewditu Memorial Hospital, Addis Ababa, Ethiopia; 2School of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Bisrat Tamene Bekele, Clinical Governance and Quality Improvement Directorate, Zewditu Memorial Hospital, P.O. Box 316, Addis Ababa, Ethiopia, Tel +251912444904, Email [email protected]
Background: Type 1 diabetes mellitus (T1DM) is one of the most common chronic diseases during childhood and adolescence. It threatens the health and endangers life with consequences for the physical and emotional development of the child and adolescent. Our study aimed at determining the health-related quality-of-life (HRQoL) and factors affecting it in children and adolescents with T1DM.
Methods: A hospital-based cross-sectional study was conducted among 379 randomly selected children and adolescents, 5– 18 years of age, with T1DM on follow-up at endocrine clinics from 25 August to 25 September 2021. PedsQLTM 4.0 generic core scales were used to collect the data. Paired sample t-test was used to compare children’s and adolescents’ self-reports and caregiver’s reports. Bivariable and multivariable linear regression is used to explore to identify significant predictor factors of HRQoL.
Results: Total mean score of HRQoL was 88.42± 10.82 as reported by the children and adolescents and 82.17± 12.65 reported by their primary caregivers. According to self-reports, age (β=− 0.197, p=0.028), mothers’ educational status (β=0.242, p< 0.001), fathers’ educational status (β=0.259, p< 0.001), fathers’ occupation (β=0.170, p=0.038), frequency of insulin administration (β=− 0.132, p=0.007), diabetes duration (β=− 0.101, p=0.050), and frequency of monitoring of blood glucose (β=0.165, p=0.006) were statistically significant predictors of HRQoL, explaining 21.6% of the variability of total HRQoL scores of children and adolescents (R2=0.216, F(21,357)=5.968, p< 0.001).
Conclusion: Children and adolescents with T1DM in Ethiopia have relatively good HRQoL. Increased age, longer diabetes duration, and insulin administrations of three times per day were associated with decreased HRQoL scores. Educated parents, having an employed father, and frequent blood glucose monitoring were associated with higher HRQoL scores.
Keywords: adolescents, quality-of-life, children, type-I diabetic mellitus, PedsQL, Addis Ababa, Ethiopia
Introduction
Type I Diabetes Mellitus (T1DM) is one of the most common chronic diseases during childhood and adolescence, which is caused by an autoimmune reaction where the body’s defense system attacks the cells that produce insulin. As a result, the body produces very little or no insulin. According to the American Diabetic Association, T1DM is diagnosed if the child or adolescent has a fasting blood glucose level ≥126 mg/dL (7.0 mmol/L), or 2-hour plasma glucose level ≥200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test (OGTT), or having HbA1C ≥6.5% (48 mmol/mol), or the presence of random blood glucose ≥200 mg/dL (11.1 mmol/L) in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis.1
There are an estimated 600,900 children under 15 years of age living with T1DM worldwide, affecting an estimated 108,300 children under 15 years annually worldwide, with this figure increasing to nearly 149,500 under 20 years and an overall annual increase of around 3%. In Ethiopia, the estimated prevalence of T1DM among children and adolescents of 0–19 years old is 2.4 per 100,000 per year according to International Diabetes Federation (IDF) 2021 report.2
Living with T1DM presents numerous daily challenges associated with disease management to children and adolescents and includes such challenges as serious life style alterations with intensive therapeutic exogenous insulin regimes, need for dietary restrictions, regular exercise, and frequent monitoring of biochemical markers.3
Health-related quality-of-life (HRQoL) of children and adolescents with T1DM consists of the physical, social, school, and emotional functioning of the patients. It is known to affect and be affected by and factors like child’s age, child’s sex, family income, duration of illness, level of knowledge of the illness, presence or absence of biochemical disease control, and lifestyle of children and adolescents. It goes beyond direct measures of population health, life expectancy, and cause of death, and focuses on the impact health status has on quality-of-life.4 Evidence shows that HRQoL has been reported to be lower among T1DM children and adolescents compared to their counterparts without diabetes.5 Adolescents in particular are known to have unique needs based on the significant developmental changes that occur during this transitional period of life.5–7
Type-I diabetes mellitus care has focused on obtaining a target glycemic level in order to avoid the disease’s complications. However, in today’s medicine, health is more than just the absence of clinical characteristics or disease markers; it encompasses all domains of health and emphasizes the necessity of treating all aspects of a patient’s health.3,8 As a result, prior studies have recommended that children and adolescents with diabetes have their HRQoL measured on a regular basis.9–11
Assessment of HRQoL needs to be incorporated with the medical management of diabetes mellitus for children and adolescents. Health-related quality-of-life implicates valuable information about disease progress and impact of treatment on children and adolescents with T1DM. Although the number of children’s with T1DM in Ethiopia is high and increasing in incidence,12 apart from the medical treatment on the glycemic control and prevention of the chronic complications, the generic HRQoL has been neglected and there are limited studies in our country. A study that included 229 children from Addis Ababa showed a mean score of HRQoL of 78.8±15.6 as reported by children and 61±7.9 reported by parents. In the study children of age 5–7 were not included, a small sample size was used, and one of the largest hospitals providing diabetic care for the children and adolescents was not involved.9 Therefore, this study assessed HRQoL and its associated factors among children and adolescents with T1DM from the age of 5 up to 18 years old on follow-up at Pediatrics Endocrine clinics of four specialized teaching hospitals in Addis Ababa, Ethiopia. The results of this study will identify the level and factors affecting of HRQoL and provide information for healthcare providers and policymakers.
Materials and Methods
Study Design, Setting, and Period
A hospital-based cross-sectional study was conducted from August 25, 2021 to September 25, 2021 to assess the HRQoL and its associated factors among children and adolescents withT1DM on follow-up at four pediatric endocrine clinics of specialized teaching hospitals in Addis Ababa, Ethiopia. Addis Ababa is the capital city of Ethiopia and located 2,355 meters above sea level. Based on the population projection of the Central Statistical Agency of Ethiopia in 2021, Addis Ababa has a total population of 3,774,000, of whom 1,782,000 are male.13 Among the teaching hospitals, five of them, namely St. Paul’s Hospital Millennium Medical College (SPHMMC), Tikur Anbessa Specialized Hospital (TASH), Tirunesh Beijing Hospital (TBH), Yekatit 12 Medical College (Y12MC), and Zewditu Memorial Hospital (ZMH) are providing services for pediatric endocrinology and have Pediatrics Endocrine outpatient clinics. Of these, four of the hospitals were chosen purposefully for this study, and TBH was used for the pretest study.
Participants, Sample Size, and Sampling
The source population was all caregivers and children and adolescents with T1DM visiting the selected hospitals’ outpatient pediatrics endocrine clinics. Selected children and adolescents with T1DM and their caregivers who came to the outpatient departments during the study period were the study population. Children and adolescents who had known comorbid chronic medical illnesses in addition to T1DM, seriously ill T1DM patients who were unable to respond to the questionnaire, and those who refused to participate were excluded from this study.
The sample size was calculated using a single population proportion formula by considering the following assumptions: the prevalence of a low level of health-related quality-of-life among children and adolescents with T1DM score was 42.8% for emotional functioning from a similar previous study conducted at a governmental hospital in Addis Ababa Ethiopia,9 with a 5% marginal error and at 95% confidence level. Then, the final sample size calculated by adding 10% for the non-response rate was 414. The sample size was proportionally allocated to the hospitals based on the total number of children and adolescents on follow-up, and a simple random sampling technique was used to select participants (caregivers with children and adolescents with T1DM) visiting the selected hospitals’ outpatient pediatrics endocrine clinics using a lottery method technique.
Study Variables
The dependent variable is the mean score of the HRQoL of children and adolescents with T1DM. The independent variables in this study were divided into two categories. They were a) Sociodemographic – this category included variables such as age, gender, marital status of primary caregivers, average family monthly income, primary caregiver’s employment status, educational status of the child and adolescent, educational status of primary caregiver, family setting; and b) Clinical and nutritional related factors – this category included variables such as the diabetes duration, age at diagnosis, HbA1c level, blood sugar control and monitoring frequency, Insulin administration frequency, physical activity, nutritional status of child and adolescent, family history of diabetes, and number of admissions over past 6 months.
Operational Definitions
Pediatric Quality-of-Life inventory (PedsQLTM):14 The Pediatric Quality-of-Life Inventory (PedsQL) is a brief measure of health-related quality-of-life in children and adolescents. Parents (the Proxy Report) as well as children and young people (the Self-Report) can complete the measure.
Health-related Quality-of-Life (HRQoL):14 Health-related Quality-of-Life (HRQoL) refers to the physical, school, emotional, psychosocial, and social domains of health that are influenced by a person’s experiences, beliefs, expectations, and perceptions.
Recent HbA1c:9 A HbA1c test that was done within the past 3 months.
Children:14 Pediatric age groups from 5–12 years old.
Adolescents:14 Pediatric age groups from 13–18 years old.
Primary caregiver: In this study, the primary caregiver is defined as an individual who provides the majority of care or guardianship (has the greatest responsibility for the daily care and rearing) of a child and/or adolescent.
Physical activity:15 Daily 60 minutes or more of moderate-to-vigorous intensity physical activity.
Glycemic control:16 Well-controlled FBS levels are: 90–180 mg/dL for age group5–12 and 90–130 mg/dL for age group 13–18 years: Poor glycemic control is: <90 or >180 mg/dL for age group8–12 and <90 or >130 mg/dL for age group 13–18 years.
Co-morbidity: The occurrence of any chronic health condition among children and adolescents with T1DM in addition to the DM.
Data Collection Methods and Procedures
A standardized structured questionnaire was used by adopting from the PedsQLTM 4.0 generic core scales and anthropometry measurements of the children and adolescents were taken.14 The questionnaire was obtained from eprovide.mapi-trust.org with permission (Special terms No. 34,085 dated April 6, 2021). The questionnaire was designed to obtain information on the socio-demographic characteristics, health-related characteristics, and psychosocial condition of the study participants. Validated and reliable Amharic version with Cronbach’s alpha coefficient for the total GCS (α child self-report=0.96; α parent proxy report=0.95) of PedsQLTM 4.0 were used.17
PedsQLTM 4.0 generic core scales contain questionnaires to be filled in by the children and adolescents (Self-report) and primary caregivers (Parent report) for those aged 5–18 years, which contains 23 items comprising of four dimensions (Physical functioning (8 items), emotional functioning (5 items), social functioning (5 items), and school functioning (5 items)). The Physical Health Summary Score (8 items) is the same as the Physical Functioning Subscale. To create the Psychosocial Health Summary Score (15 items), the mean is computed as the sum of the items divided by the number of items answered in the Emotional, Social, and School Functioning Subscales. The items for each of the forms are essentially identical, differing in developmentally appropriate language, or first or third-person tense. The instructions ask how much of a problem each item has been during the past 1 month. A 5-point response scale is utilized across child self-report for ages 8–18 and parent proxy-report (0=never a problem; 1=almost never a problem; 2=sometimes a problem; 3=often a problem; 4=almost always a problem). To further increase the ease of use for the young child self-report (ages 5–7), the response scale is reworded and simplified to a 3-point scale (0=not at all a problem; 2=sometimes a problem; 4=a lot of a problem), with each response choice anchored to a happy to sad faces scale. Items are reverse scored and linearly transformed to a 0–100 scale (0=100, 1=75, 2=50, 3=25, 4=0), so that higher scores indicate better HRQoL. Scale scores are computed as the sum of the items divided by the number of items answered. If more than 50% of the items in the scale are missing, the scale score is not computed (33).
The questionnaires were interviewer-administered and the interview and anthropometric measurements were conducted by two trained Nurses who hold bachelor degrees and two General Practitioners, and was supervised by the principal investigator. The data collectors completed the personal questionnaires by one-to-one interviews with the children/adolescent with type 1 diabetes and their parents in the hospitals. Completing the questionnaires took approximately 15–20 minute. The principal investigator checked the completeness and consistency of the collected data daily. Individual records with incomplete data were excluded from the analysis.
Data Processing and Analysis
Using the Kobo toolbox, the collected data were exported to SPSS version 25 for further analysis. The data were cleaned and checked for outliers and inconsistencies ahead of the statistical analysis. Descriptive analysis was performed to describe the number and percentage of sociodemographic characteristics of categorical variables. The data were summarized in means, medians, standard deviations, tables, and charts. Paired sample t-test was used to compare children, adolescents self-report, and caregiver’s report. Bivariable and multivariable linear regression is used to explore the real difference in mean scores and to identify the significant predictor factor of quality-of-life of children and adolescents. A p-value of ≤0.05 was considered to declare a statistically significant association between independent variables and quality-of-life. Tables, figures, charts, and texts are used for data presentation.
Results
Socio-Demographic Characteristics
A total of 379 participants were included in the study (giving a 91.5% response rate). The mean age of the children and adolescents was 11.65 years ±3.56 SD. The mean age of the children was 8.98±2.42 years, and that of the adolescents was 14.89±1.33 years. Two hundred and fourteen (56.5%) children and adolescents were girls. About 69.1% of children and adolescents live with both parents (mothers and fathers). The median monthly income of the primary caregivers is 4,500 Ethiopian birr with an IQR between 2,000–8,000. Regarding educational status of parents, 43 (12.3%) of the children’s mothers, 19 (6.8%) of the children’s fathers, and four other primary caregivers had no formal education. On average there were around 2.37 children who are less than or equal to 18 years old in the children and adolescent’s household (Table 1).
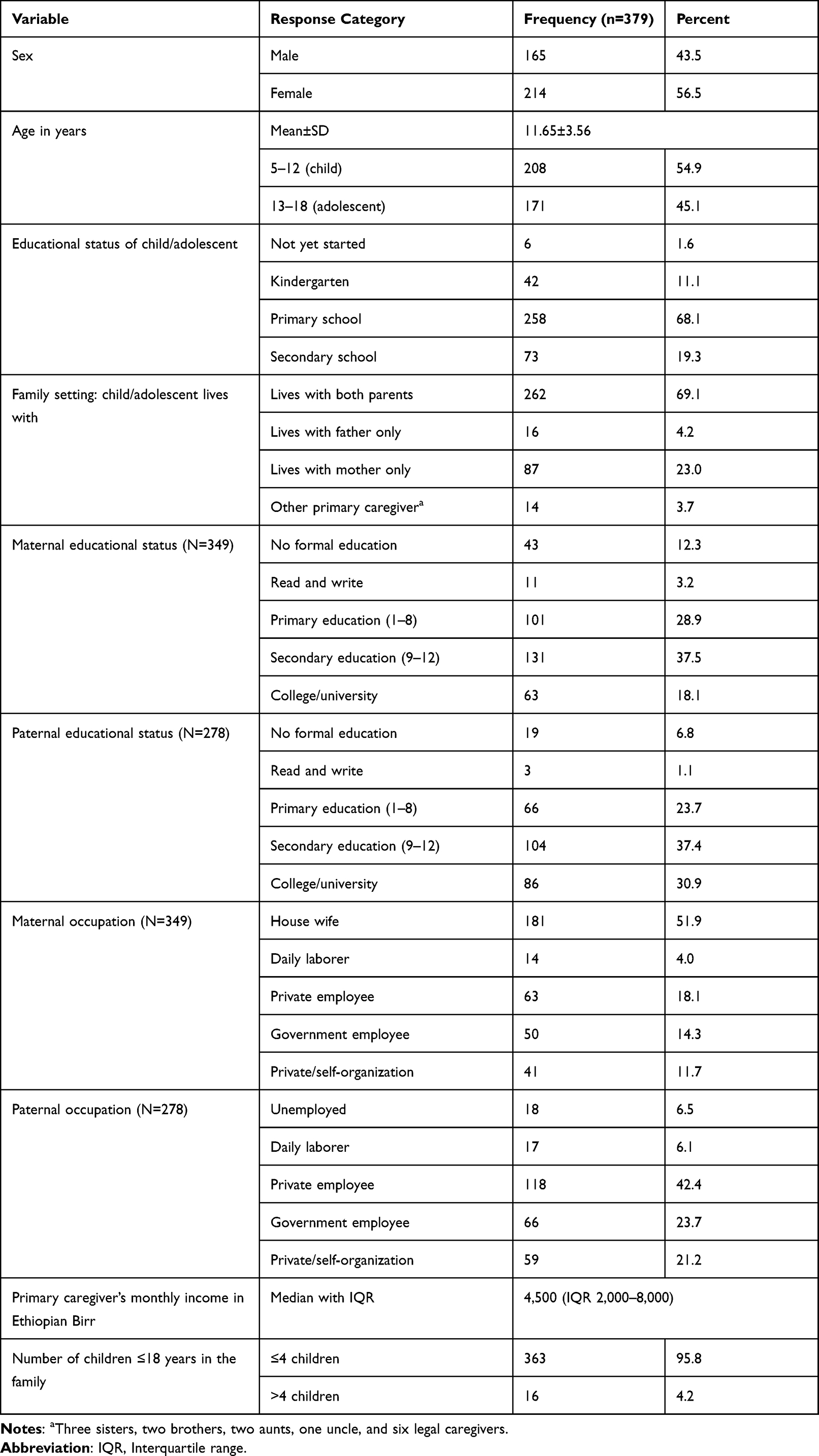 |
Table 1 Sociodemographic Characteristics of Children and Adolescents with Type 1 Diabetes Mellitus on Follow-Up at Selected Specialized Hospitals in Addis Ababa, September 2021 |
Clinical Characteristics of Children and Adolescents
The mean age at onset of diabetes for participants was 7.36 years with a SD of ±4.16 years. The mean diabetes duration among participants were 4.34 years with a SD of ±3.47, with 112 (29.6%) having had it for more than 5 years and 26 (6.9%) for less than a year. All of children and adolescents were only insulin users. The average HbA1c level was 10.12±2.04. They had 179.76±78.45 mean level of fasting blood sugar (FBS) level with the minimum being 36 and maximum of above 600. About 108 (28.5%) children and adolescents had a history of admission at health facilities in the last 6 months and 86 (22.7%) children and adolescents had a family history of diabetes (Table 2).
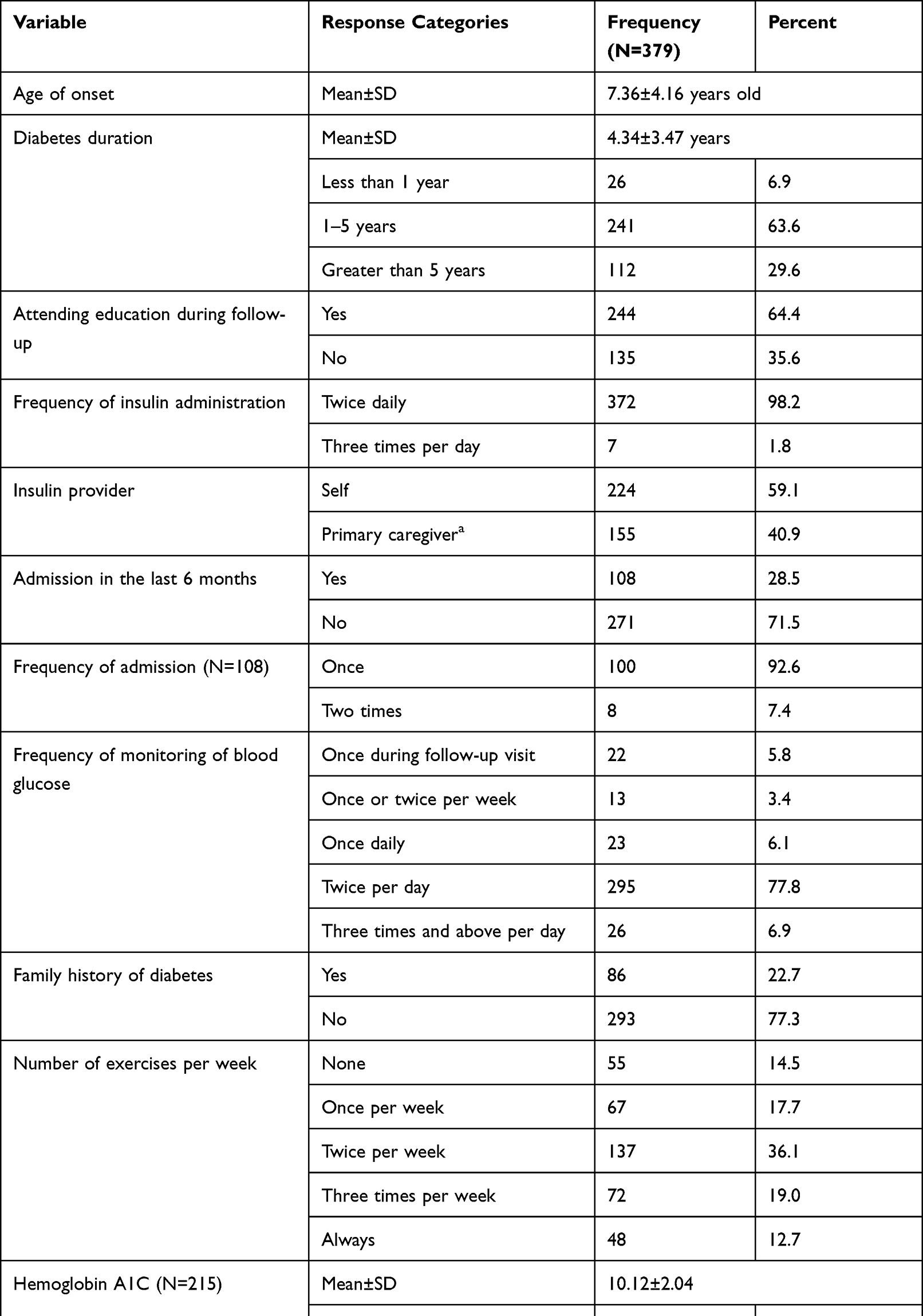 |
Table 2 Clinical Characteristics of Children and Adolescents with Type 1 Diabetes Mellitus on Follow-Up at Selected Public Hospitals in Addis Ababa, September 2021 |
Nutritional Status of Children and Adolescents
The mean weight and height of children and adolescents were 37.44 kg with a SD of ±12.17 and 140.59±16.71 cm, respectively. Average body mass index (BMI) of the study participants was 18.45±2.90 kg/m2. Using the WHO anthropometric measurement tool, 353 (93.1%) children and adolescents had normal BMI for age. Thirteen (3.45%) of the patients were found to have wasting.
Total Score and Comparison of Pediatric Health-Related Quality-of-Life (HRQoL)
Total mean scores on the PedsQL™ 4.0 were found to be 90.11±9.88 for 5–12 year olds and 86.36±11.47 for the 13–18 year olds, as reported by the children and adolescents themselves, and the total mean scores were 85.31±10.91 for children and 78.34±13.57 for adolescents as reported by primary caregivers. Both children and adolescents’ self-report and parent proxy reports for school and emotional functioning were coinciding with each other. There were relatively low scores when compared to other sub-scale scores. The paired sample t-test compares children and adolescents’ self-reports and parent proxy report of PedsQL™ 4.0 Generic Core Scales scores of children and adolescents. There was a statistically significant difference in self-reports and parent proxy reports of PedsQL™ 4.0 Generic Core scales scoring in all sub-scales but social functioning (Table 3).
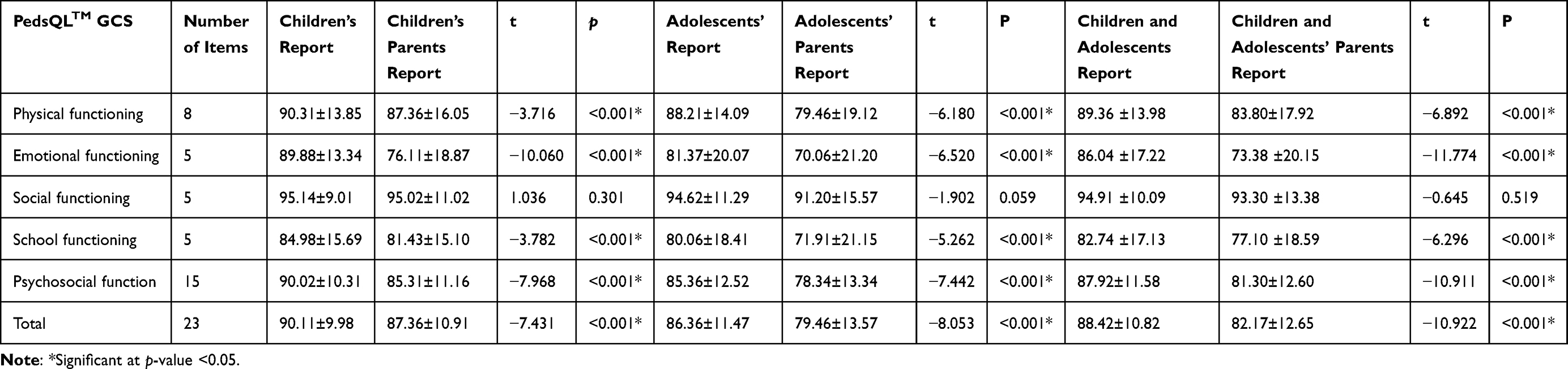 |
Table 3 Comparison of Children and Adolescents’ Self-Reports and Parent Proxy Reports of Quality-of-Life Among Children and Adolescents with Type 1 Diabetes Mellitus on Follow-Up at Selected Public Hospitals in Addis Ababa, Ethiopia, September 2021 |
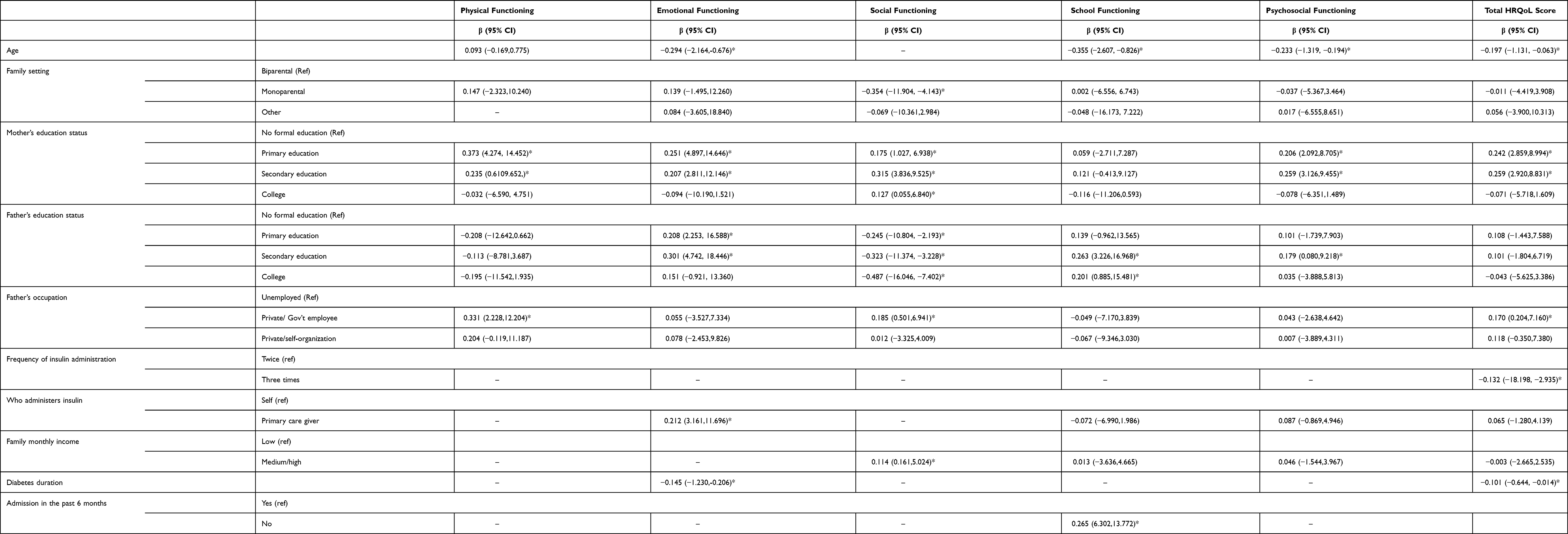 |
Table 4 Summary of Multiple Linear Regression on HRQoL with Socio-Demographic and Clinical Characteristics Among Children and Adolescents with Type I Diabetes Mellitus on Follow-Up at Selected Public Hospital, Addis Ababa, Ethiopia, September 2021 |
Factors Associated with Health-Related Quality-of-Life
Candidate variables for multiple linear regression analysis in the total of HRQoL were identified by simple linear regression at a p-value ≤0.05. In multivariable linear regression analysis, age, children and adolescents’ with T1DM mothers’ and fathers’ educational status, and fathers’ occupation were sociodemographic factors that affect HRQoL (Table 4). From clinical factors, the frequency of insulin administration, diabetes duration and frequency of monitoring of blood glucose were independent influencing factors for HRQoL scoring of children and adolescents. These variables explain approximately a quarter of the variability of total HRQoL scores of children and adolescents (R2=0.216, F(21,357)=5.968, p<0.001).
For every 1-year increase in the age of a child or an adolescent, the score of HRQoL was decreased by 0.197 (β=−0.197, p=0.028). Children and adolescents with T1DM whose mothers attended primary education and secondary education have 0.242-times and 0.259-times higher scores in the total HRQoL compared to those who cannot read and write or had no formal education, respectively (β=0.242, p<0.001, and β=0.259, p<0.001). Children and adolescents with T1DM whose fathers were an employee of an organization have a HRQoL mean score of a 0.170-times higher score than those who had no occupation or were daily laborers (β=0.170, p=0.038). Children and adolescents who took insulin injections three times per day have a total HRQoL mean score 0.132-times less than those who take it twice per day (β=−0.132, p=0.007). Also, patients who monitor their blood glucose level 1–2 times a week have a 0.165-times higher score of total HRQoL than those who get their blood glucose monitored only during hospital follow-up visits (β=0.165, p=0.006). For every 1-year increase in diabetes duration, patient’s HRQoL decreases by 0.101 (β=−0.101, p=0.050).
Discussion
Health-related quality-of-life is important in many aspects for diabetes patients and healthcare providers. This study evaluated the level of quality-of-life among children and adolescents with T1DM on follow-up at public endocrine clinics and determinant factors for their level of quality-of-life. The results of this study revealed that there were lower mean scores in sub-domains of emotional and school function of HRQoL with a similar pattern in both self-reports and parent proxy reports of HRQoL of children and adolescents but they had better scores in social functionin of the HRQoL sub-domain. These findings are similar to the findings of the studies done in Addis Ababa and Turkey.10,18 The reason for lower scores of the emotional functioning in the current study might be lower as age increases the very nature of adolescence, resulting in more worry about children and adolescent’s disease condition. The better scores in a social functioning sub-domain might be the fact that, in Ethiopian culture, every individual is wholehearted about patients and support children and adolescents rather than isolating.
Total HRQoL self-reports of children and adolescents and parent proxy reports were found to be significantly different. Parent proxy reports of children and adolescents HRQoL were lower than self-reports of children and adolescents. This was similar with findings of previous studies in Addis Ababa, Kuwait, and Greece.10,19,20 The explanation for the differences in the mean score might be the perception of primary caregivers, which is more than their children and adolescents. Also, since more responsibility on the overall health of children and adolescents with T1DM falls on the primary caregivers they are more likely to respond lesser score on the impact towards quality-of-life of the children and adolescents.
The study found that the mean score of HRQoL was higher among children than adolescents, as reported by a study conducted in Turkey.18 This may be due to the fact that most of the children were taken care of by their primary caregivers more than adolescents. In addition, adolescents tend to worry more than children, which resulted in lower HRQoL scores.
It was found that the number of children and adolescents in a household has a significant difference in HRQoL. Respondents living with lower than four children and adolescents had better HRQoL compared to those living with four or more children and adolescents. This finding is also aligned with a study conducted in Addis Ababa and Turkey.10,18
This study has found that mother’s educational status has a statistically significant association with all subdomains and total HRQoL, which is consistent with studies done in Egypt,5 but is in contrast to a study conducted in Greece14 where the mother’s educational level was not associated with the HRQoL of children and adolescents.19 This might be explained by the fact that most mothers in Ethiopia are housewives and have responsibility of taking care of their children and adolescents. Fathers’ educational status was also significantly associated with school, psychosocial, and total HRQoL.
In this study, age was associated with emotional functioning, school functioning, psychosocial functioning, and total HRQoL of children and adolescents. As age increases, HRQoL decreases. This finding is consistent with studies done in Egypt, Greece, and Saudi Arabia5,19,21 but it is inconsistent with studies conducted in Kuwait and Turkey,18,20 in which age was positively associated with HRQoL. This might be explained related to the discrepancies with primary caregiver’s supports for young age and older age children and adolescents. The fact that family supports and the needs of children for support were different was related to the developmental stages of children. The developmental and physiological changes in the children and adolescents also might explain the discrepancies among the findings.
A study done in Egypt5 showed consistent findings regarding the fathers’ occupation being significantly associated with physical functioning, social functioning, and total HRQoL of children and adolescents with T1DM. Children and adolescents whose fathers were employed and working had better HRQoL scores than those whose fathers had no job or were daily laborers. This finding indicates that employment with a good income from fathers might have resulted in better care and HRQoL outcome. Thus, securing jobs for fathers does positively affect the HRQoL of children and adolescents with T1DM.
Moreover, the HRQoL of children and adolescents is significantly associated with diabetes duration and frequency of monitoring of blood glucose. Longer diabetes duration and those who measure their blood glucose level less frequently have a lower score of HRQoL than those who frequently monitor their blood glucose.
The study was conducted in such a way that it involved most public hospitals with pediatrics endocrine service in order to maximize representative of the study. The QoL of children and adolescents with T1DM were assessed using generic instrument (PedsQL™ 4.0 Generic Core Scales) to increase detection of quality-of-life in different dimensions. Both the sub-domains and the summary measures were reported which will help to avoid the information loss that could have occurred in reporting only the summary measures. In addition, a random sampling technique was used to select the sample for the study through a direct face-to-face interview. However, this study does have some inherent limitations. First, the study design makes it difficult to determine the direction of causality and the absence of control groups in assessing generic core scales (HRQoL) for comparison. Besides, other QoL determining factors like behavioral risks (coping, depression, or other psychiatric states) and health service related are not included in this study. This study sampled children and adolescents with T1DM from endocrine clinics, thus the findings might not be generalized to all children and adolescents with T1DM in the community. Age classification of the study is not according to World Health Organization standard, which resulted in missing age 19 year old adolescents in the study.
Conclusions
In conclusion, although social functioning of the children and adolescents was high, emotional and school functioning were somewhat low. There was a negative relationship between age, diabetes duration, insulin administration of three times per day, and HRQoL, and a positive relationship between mothers’ and fathers’ educational status, fathers’ occupation, monitoring blood glucose at least one to two times per week and the QoL of the children and adolescents. An evaluation of the QoL after a diagnosis of diabetes can be used to detect early and to combat problems, which children and adolescents may encounter. In addition, assessing children with diabetes for detecting any problems that could affect their HRQoL should be included in diabetes management protocols.
Abbreviations
FBS, fasting blood sugar; HgA1c, hemoglobin A1C; HRQoL, health-related quality-of-life; PedsQLTM, pediatric quality-of-life inventory; SPHMMC, St. Paul’s Hospital Millennium Medical College; T1DM, type 1 diabetes mellitus; TASH, Tikur Anbessa Specialized Hospital; WHO, World Health Organization; Y12MC, Yekatit 12 Medical College; ZMH, Zewditu Memorial Hospital.
Data Sharing Statement
All data generated or analyzed during this study are available from the corresponding author on reasonable request.
Ethical Considerations and Informed Consent
Ethical clearance and approval were obtained from the Institutional Research Review Boards of St. Paul’s Hospital Millennium Medical College (PM23/294), Tikur Anbessa Specialized Hospital (ህጻ/ህት/262/13), Yekatit 12 Hospital Medical College (14/12), and from Addis Ababa public health research and emergency management directorate (A/A/5962/227). Permission to carry out the study was given by TASH, SPHMMC, Y12MC, and ZMH Hospital administrations. After a detailed explanation of the study purpose, written informed consent was obtained from caregivers and assent from participating children and adolescents. Confidentiality and privacy of the participant have been maintained throughout the process of data collection. The data were kept confidential and used for the intended purpose only. Participation in the study was on a voluntary basis. This study was conducted with a serious consideration of the coronavirus pandemic. So that, in order to minimize the risk of infection transition during the face-to-face interview, the interview was conducted in a ventilated area with keeping enough distance between the interviewer and interviewees, and also facemasks were worn by all participants as well the data collectors. This study was conducted as per the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge the study participants, data collectors, and administrative bodies of SPHMMC, TASH, TBH, Y12HMC, and ZMH for their permission.
Author Contributions
All authors made a significant contribution to the study in the conception, study design, execution, acquisition of data, analysis, and interpretation; were involved in drafting, substantially revising, and critically reviewing the article; and have agreed on the journal to which the article will be submitted. All authors reviewed and agreed on the revised versions of the article before submission and agreed to take responsibility and be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care. 2020;43(Supplement 1):S14–31. doi:10.2337/dc20-S002
2. International Diabetes Federation. IDF Diabetes Atlas, 10th edn [Internet]. Brussels, Belgium; [cited January 10, 2022]. Available from: https://www.diabetesatlas.org.
3. Steyn NP, Mchiza ZJR, Kengne AP. Future challenges for pediatric diabetes management in developing countries: lessons from Africa. Expert Rev Endocrinol Metab. 2015;10(1):75–86. doi:10.1586/17446651.2015.968552
4. Varni JW, Seid M, Kurtin PS. PedsQLTM 4.0: reliability and validity of the pediatric quality of life inventoryTM version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–812. doi:10.1097/00005650-200108000-00006
5. Gadallah MA, Ismail T, Aty N. Health related quality of life among children with Type I diabetes, Assiut city, Egypt. J Nurs Educ Pr. 2017;7(10):73–82.
6. Melab SM. Quality of life in children with diabetes at Kenyatta National Hospital; 2014.
7. de Souza ACCB, Felício JS, Koury CC, et al. Health-related quality of life in people with type 1 diabetes mellitus: data from the Brazilian Type 1 Diabetes Study Group. Health Qual Life Outcomes. 2015;13(1):1–9. doi:10.1186/s12955-014-0204-2
8. Definition WHO. diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. Geneva World Health Organ; 2006:3.
9. Naughton MJ, Ruggiero AM, Lawrence JM, et al. Health-related quality of life of children and adolescents with type 1 or type 2 diabetes mellitus: SEARCH for diabetes in youth study. Arch Pediatr Adolesc Med. 2008;162(7):649–657. doi:10.1001/archpedi.162.7.649
10. Girma D, Murugan R, Wondossen K, Yeshiwas S, Wale A, Tilahun S. Health-related quality of life and its associated factors in children and adolescents with type1 diabetes, Addis Ababa, Ethiopia. Glob Pediatr Health. 2021;8:2333794X211030879. doi:10.1177/2333794X211030879
11. Lontchi-Yimagou E, Mapa-Tassou C, Dehayem MY, et al. The effect of free diabetes care on metabolic control and on health-related quality of life among youths with type 1 diabetes in Cameroon. BMJ Open Diabetes Res Care. 2017;5(1):e000397. doi:10.1136/bmjdrc-2017-000397
12. Ogle GD, James S, Dabelea D, et al. Global estimates of incidence of type 1 diabetes in children and adolescents: results from the International Diabetes Federation Atlas. Diabetes Res Clin Pract. 2021;183:109083. doi:10.1016/j.diabres.2021.109083
13. Population Projection Towns as of July 2021 [Internet]. Addis Ababa, Ethiopia: Central Statistical Agency. Available from: https://www.statsethiopia.gov.et/population-projection/.
14. Varni J. Pediatric quality of life inventoryTM PedsQLTM. Lyon Fr Mapi Res Trust; 2010.
15. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
16. American Diabetes Association: Standards of Care for Diabetes. Brief summary of screening and diagnosis of type 2 diabetes and its complications. Diabetes Care. 2013;36:S11–61. doi:10.2337/dc13-S011
17. Girma D, Abita Z, Wale A, Tilahun S. Reliability and Validity of Ethiopian Amharic Version of the PedsQLTM 4.0 generic core scales and PedsQLTM 3.0 diabetes module. Adolesc Health Med Ther. 2021;12:77. doi:10.2147/AHMT.S312323
18. Özyazıcıoğlu N, Avdal EÜ, Sağlam H. A determination of the quality of life of children and adolescents with type 1 diabetes and their parents. Int J Nurs Sci. 2017;4(2):94–98. doi:10.1016/j.ijnss.2017.01.008
19. Emmanouilidou E, Galli-Tsinopoulou A, Karavatos A, Nousia-Arvanitakis S. Quality of life of children and adolescents with diabetes of Northern Greek origin. Hippokratia. 2008;12(3):168.
20. Abdul-Rasoul M, AlOtaibi F, Abdulla A, Rahme Z, AlShawaf F. Quality of life of children and adolescents with type 1 diabetes in Kuwait. Med Princ Pract. 2013;22(4):379–384. doi:10.1159/000347052
21. AlBuhairan F, Nasim M, Al Otaibi A, Shaheen NA, Al Jaser S, Al Alwan I. Health related quality of life and family impact of type 1 diabetes among adolescents in Saudi Arabia. Diabetes Res Clin Pract. 2016;114:173–179. doi:10.1016/j.diabres.2016.01.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.