")
Back to Journals » International Journal of General Medicine » Volume 16
Health Related Quality of Life and Associated Factors Among Adult Patients with Rheumatic Heart Disease Patients in Ethiopia
Authors Nasir M , Taddesse K, Ahmed M , Argaw Z, Gebretensaye TG , Markos S
Received 12 May 2023
Accepted for publication 3 August 2023
Published 9 August 2023 Volume 2023:16 Pages 3403—3412
DOI https://doi.org/10.2147/IJGM.S419118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Mohammed Nasir,1 Konno Taddesse,2 Muluken Ahmed,3 Zeleke Argaw,2 Tigistu Gebreyonnis Gebretensaye,2 Sura Markos4
1Pediatrics Department, Hawassa University, Hawassa, Ethiopia; 2Nursing Department, Addis Ababa University, Addis Ababa, Ethiopia; 3Pediatrics Department, Arba Minch University, Arba Minch, Ethiopia; 4Internal Medicine Department, Hawassa University, Hawassa, Ethiopia
Correspondence: Mohammed Nasir, Pediatrics Department, Hawassa University, Hawassa, Ethiopia, Tel +251911739081, Email [email protected]
Background: Quality of life (QOL) is defined as “individuals” perceptions of their position in life. Rheumatic heart disease (RHD) is a consequence of severe, single, or recurrent bouts of acute rheumatic fever. To improve overall patient outcomes, there is currently a greater emphasis on assessing the QOL of these patients. The purpose of this study is to assess the QOL of adult RHD patients who had followed up at St Peter and Tikur Anbessa Hospital, Ethiopia.
Methods: An institutional-based cross-sectional study done at St Peter and Tikur Anbessa Hospital, Ethiopia from March 1−June 30/2021 in adult RHD patients. The sample size was 297. Socio-demographic and clinical data were collected using a structured questionnaire. The Amharic version of Short form-36 (SF-36) was used to assess the QOL. A logistic regression model was used to identify associated factors.
Results: The study included 297 patients. The majority are female (71%), and half of them are aged between 18− 30 years of age. Of the patiends, 81.1% had no comorbidity, and 15.8% had interventions. RHD affects all domains and summary scores of short form 36 QOL parameters compared to normative values. Age, marital status, place of residence, presence of comorbidity, number of medications, and whether an intervention was done are associated with the QOL of these patients.
Conclusion: RHD patients had poor QOL assessed by SF-36. It affects all domains and summary score of short form 36 QOL parameters. Old age, divorce, living in rural areas, associated comorbid conditions, and no intervention done are associated with poor QOL. Identification and treating comorbid conditions and intervention may improve QOL.
Keywords: quality of life, rheumatic heart disease, health-related quality of life, Ethiopia, QOL, RHD
Background
Rheumatic heart disease (RHD) is a consequence of severe single or recurrent bouts of acute rheumatic fever and is primarily characterized by stenosis and regurgitation of the mitral valve. It continues to be a problem for public health in both the developing world and underprivileged areas of the developed world. According to current estimates, it currently affects 33.4 million individuals globally. This condition also resulted in 305,000 deaths in 2015, and it causes more than one million premature deaths annually.1, 2
RHD has a wide range of complications, including heart failure, stroke, and infective endocarditis.3,4 These morbidities also affect patients’ quality of life (QOD), in addition to the health consequence of this disease.4 Additionally, the death rate for RHD is still high. However, the mortality rate for RHD is declining generally, albeit unevenly.3, 5 This is seen by the 47.8% decrease in age-standardized global mortality from RHD.5 In the past in the field of cardiology outcome measures mainly concentrated on the magnitude of mortality and morbidity.6 Regarding RHD, the improvement in patient medical and surgical management contributed a lot to the decrease in mortality in this chronic disease.1 Therefore, to improve overall patient outcomes, there is currently a greater emphasis on assessing the lived experience of patients (QOD) with RHD.7, 8
QOD is defined by the WHO as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.”
It is multi-dimensional and includes one’s level of independence, level of independence, mental and physical health, as well as social ties and one’s own beliefs and their interconnections.7 Health-related QOD is specifically focused on health aspects while also considering other aspects of overall QOD.7
This study evaluated the QOD of patients with RHD who had follow-ups at Tikur Anbessa Hospital and St. Peter Specialized Hospital, Ethiopia using a general assessment of health status self-administered questionnaire called the short form 36. We used this form because there is no specific tool to assess the QOD in patients with RHD and this tool was used by others for assessing RHD QOL with good results. It is also easy and contains many domains for assessing health-related QOD for chronic illness. To our knowledge, there are only a few numbers of studies that evaluate the QOD and associated factors in patients with adult RHD.
Methods and Materials
Institution based cross-sectional study design was employed in Tikur Anbessa Specialized Hospital and St. Peter Specialized Hospital, Ethiopia between March 1–June 30, 2021. These Hospitals are found in Addis Ababa, capital city of Ethiopia. They have outpatient and inpatient service for cardiac patients. These two hospitals together give outpatient and inpatient services for more than 1157 patients with RHDs. The sample size was calculated from all RHD adult patients, aged over 18 years, attending follow up in selected hospitals based on the assumption of single population proportion formula, with the assumption of 50% prevalence since there was no similar study found during literature search in the area and 95% CI and 0.5 margin of error. As the study population is below 10,000, correction formula was applied and additional 10% participants were included to compensate for non-responders. Accordingly, a total of 297 RHD patients were involved in the study.
Tikur Anbessa Specialized Hospital cardiac clinic had 970 patients on follow up, and is the source population. St. Peter Specialized Hospital cardiac had 187 RHD patients on follow up. These will be the general source population in the study period. 236 from Tikur Anbessa Specialized Hospital and 61 from St. Peter Specialized Hospital were proportionally assigned to get total of 237 sample size. Participants were proportionally allocated based on the total patient flow in the two hospitals. Before starting data collection, a sampling frame list of the study population was prepared from the appointment list for the study period. Then, study subjects were selected by systematic random sampling technique from the study population and k value was 3.
Instrument
A questionnaire consisted of three parts which was divided as socio-demographic characteristics assessment part, clinical check list part and SF-36 questionnaire. Under socio-demographic part, there were seven questions. The clinical checklist had six questions. The English version of Short Form 36 (SF 36) measuring tool which contains 36 questions was translated to Amharic according to the guidelines set by the developers.
The SF-36 is a 36-item scale, which measures eight domains of health status: physical functioning (ten items); physical role limitations (four items); bodily pain (two items); general health perceptions (five items); energy/vitality (four items); social functioning (two items); emotional role limitations (three items) and mental health (five items) The two summary scores namely Physical Component Summary (PCS) and Mental Component Summary (MCS) summarizes the result of the eight domains into two cumulative aspects of QoL. A scoring algorithm was used to convert the raw scores into the eight dimensions listed above. The scores were transformed to range from zero where the respondent has the worst possible health to 100 where the respondent is in the best possible health. It yields an eight-scale profile of scores as well as physical and mental health summary measures. SF-36’s strong focus on health and evidence of responsiveness make it particularly useful.9 It was filled by filled by nurses under supervision of principal investigator and supervisors.
Quality Assurance
The quality of data was assured before, during and after data collection. Accordingly, before data collection, training was given to the data collectors. During data collection the principal investigator and supervisors ensured completeness and consistence of the questionnaires administered each day. Missed variables were completed by reviewing the chart. After data collection, the collected information was rechecked for its completeness and consistence by the principal investigator before transferring to computer software. Non-overlapping unique code was given for each individually answered questionnaires and the coded data was entered and cleaned in epi data version 4.6.0.2.
Data Analysis
Each item of SF-36 was scored on a linear scale which was obtained by summation of the corresponding items. The linear score was transformed into on a 0–100 Z-scores as per the recommendation of SF-36 algorithm. Aggregate component scores, PCS and MCS, were then calculated by rotating the corresponding Z-scores orthogonally. Frequencies, percentages, means and standard deviations were used for demographic variables and the mean scores of the study variables were described. Bivariate analysis was done by using binary logistic regression to identify factors associated with the lower quartile of summary scores. Variables with P-value less than 0.2 were included for multiple logistic regressions. Odd ratio was used to assess strength of association between the factors and summary scores. To check for significance level, 95% CI that did not cross 1 and a statistical significance at P value of <0.05 is considered. SPSS version 27 was used for data analysis.
The following Terms and Operational Definitions are used:
RHD patient is a patient following at adult cardiac clinic in TASH and St. Peter specialized hospital with as main diagnosis is put as RHD in his/ her chart.
HRQoL/ QoL is Patient’s perception and rating of his/ her own health in regard to all eight domains of SF 36 in the past four weeks.
Poor QOD is RHD patients with mean summary scores below 50.
Good QOL is RHD patients with mean summary scores above 50.
Ethical Consideration
Before data collection, ethical clearance was obtained from the Institutional Research Ethics review board (IRB) of Addis Ababa University, College of medicine and health sciences (IRB/1007/2021). Letter of the permission was obtained from respective bodies. Participation in the study was voluntary and the purpose of the study was explained to participants before conducting an interview. Written consent was obtained from study participants by attaching a statement of consent to each questionnaire. However, the identification of the participants was not recorded anywhere on the questionnaire, and confidentiality was assured by analyzing the data in aggregate. To protect the study participants and data collectors from the pandemic personal protective equipment was provided during the interview for the study participants and data collectors.
Results
Socio-Demographic Characteristics
A total of 297 patients participated in this study with a response rate of 100%. Females comprised close to three quarters of the sex category (71%). Half of the study populations were in the age group of 18 to 30, accounting for 49.8%. Mean age of the study population was 34.51± 12.96 SD years, and ranged between 18 and 81 years. Married participants accounted for 46.5% while singles comprised 44.1%. Majority of study population were urban dwellers (79.5%). Participants who have diploma and above comprise 30.3%, and 16.5% were illiterates. About 55% of the participants were employed (Table 1).
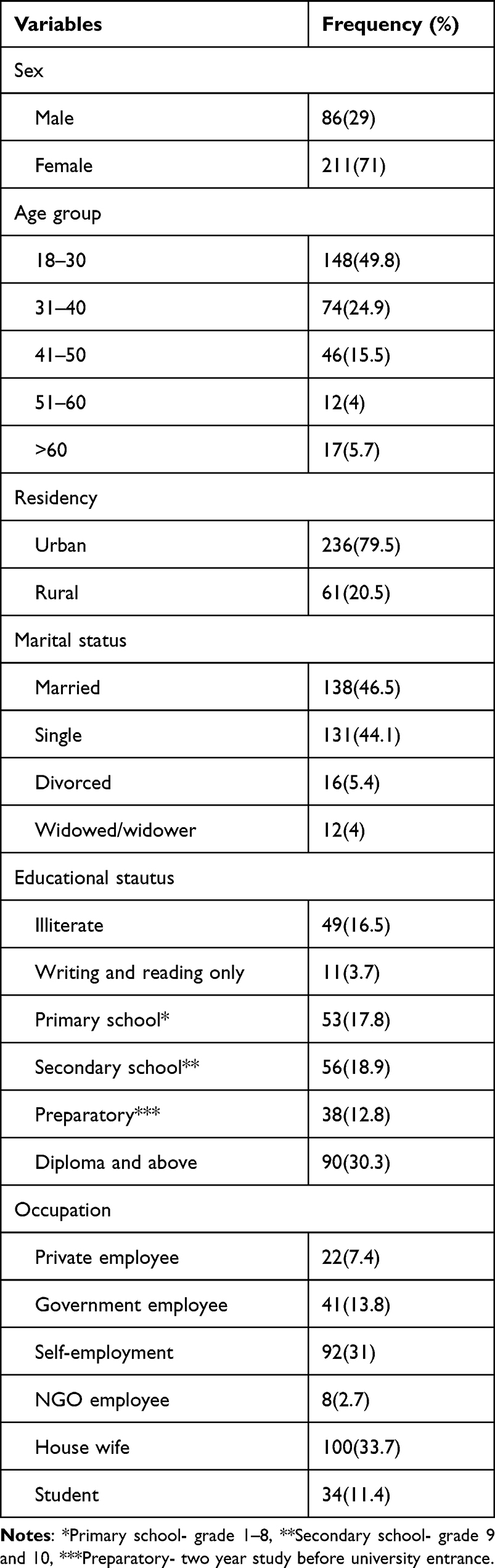 |
Table 1 Socio-Demographic Characteristics of RHD Patients in Selected Government Hospitals, Addis Ababa, Ethiopia, 2021 (n = 297) |
Clinical Characteristics
Study participants have been following in cardiac clinic from 3 months to 33 years with mean duration of 88 months. Majority of participants (81.1%) had no additional clinical conditions that require medical attention. Out of the 56 participants who had other comorbidities; 23 of them (41.1%) had hypertension either alone or together with another chronic illness/es. The second most frequently identified comorbidity was diabetes. Twelve of the 56 patients (21.43%) with one or more comorbidities had Diabetes. Participants were taking from one (2%) up to eight medications to either prevent or manage of RHD or treat the co morbidities at the time of study period. Mean number of medications were 2.89 and median number of medications was 3. Only 47 participants had undergone a surgical intervention (15.8%) (Table 2).
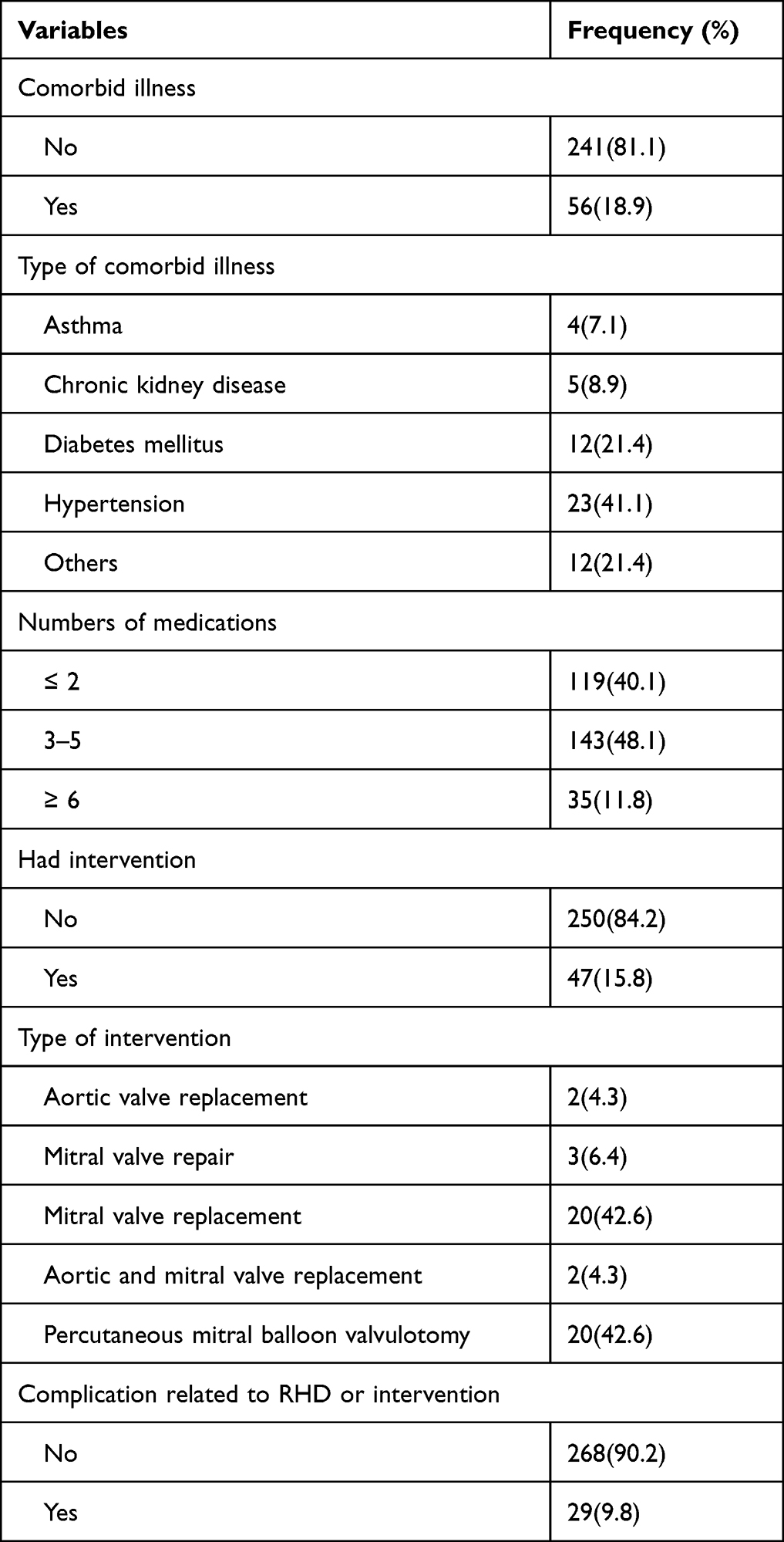 |
Table 2 Clinical Characteristics of RHD Patients in Selected Government Hospitals, Addis Ababa, Ethiopia, 2021 (n = 297) |
Health Related Quality of Life, SF-36
The domains Role Physical and Role Emotional scored in the lower end with mean value below 60. Respondents scored on the higher end for the social functioning (70.33 ± 31.67) and vitality (70.6±31.7). Except for only one domain, vitality (0.665), the Cronbach’s alpha reliability tests were well beyond 0.7 (Table 3). The two summary scores were below 50 with PCS and MCS of 43.85 and 45.91 respectively taking the cut point value of summary scores for poor HRQoL at 50.
 |
Table 3 Reliability, Central Tendency, and Variability of Scales in This Study |
Associated Factors for Low HRQOL of RHD Patients
After adjusting cofounder, age, living area, marital status, comorbidity, number of medications and presence of intervention were associated with summary score of HRQAL. Age greater than 60 was 1.7 more likely to lie in the lower centile than age 30. Compared to living in urban areas living in rural areas was 68% less likely to be in the lower centile than living in urban areas.
Divorced status associated with 2.8 times more likely to be the lower centile than married status. The presence of comorbid condition and 2–5 medications the patient was taking associated with 2.8 and 1.5 times more likely to be in the lower centile than patients with no comorbidity and patients taking only one medication respectively. Compared with patients who do not undergo surgery, those who undergo surgical intervention 57% less likely to lie in the lower centile (Table 4).
 |
Table 4 Factors Associated with HRQoL in Relation with SF-36 Lower Centile of Summary Scores in Patients with RHD in Selected Government Hospitals, Addis Ababa, Ethiopia, 2021 (n = 297) |
Discussion
In this study, adult RHD patients older than 18 years were evaluated for QOL using SF-36 and compared with the normative values of the general population. Additionally we assessed associated factors of lower quartile for the two summery scored.
Our study revealed females occupied large proportion of cases. A 71% of RHD patients were female, which is similar to studies conducted in Malaysia, India, and Uganda (74.5%, 71.4% and 63.5 respectively).9–11 RHD is one of the autoimmune diseases from immune reaction to streptococcal antigens, and since studies have shown that girls are more likely than males to develop autoimmune diseases, this may be the reason for the study’s female dominance.
The mean age was 34.51 which is comparable to sub Himalayan region (37 yrs) but lower than Myanamar (44 yrs) studies.12,13 This may be accounted for by the epidemiology of rheumatic fever’s first episode and recurrence, which primarily occur soon before adolescence and and adulthood, respectively. Few had comorbid illness and hypertension was the most common comorbidity among RHD patients in this study. Only 15% patients had intervention which is the main stay of cure for most them.
The result showed that the two summary’ mean scores fell below the normative values for the general population. Furthermore, the average scores of all domains and summary scores were lower than the score for the general population.14 The physical and general health subscales were lower than the emotional and social ones, which is similar to research done in Egypt15 (Figure 1).
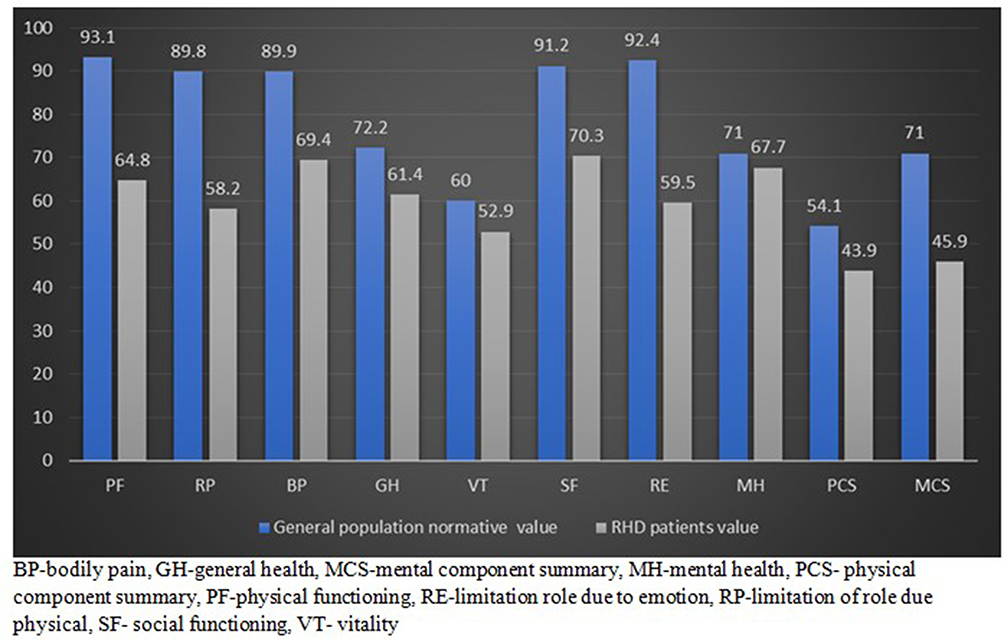 |
Figure 1 Comparison of general population normative value with this study. |
The QOL of people with RHD is influenced by a number of factors. The odds of falling of physical and mental summary scores increases by 1.2 in age group above 60 compared to age less than 30. Similarly, researches from Egypt and India showed that older patients were more severely affected by the condition.16, 17 The high comorbidity rate, economic dependence, and increased prevalence of dementia due to aging in elderly patients could all be contributing factors.
In our study, living in a rural area increases the odds of being in the lower centile by 68%. Area doubles the odds, that one’s physical and mental summary scores fall into the lower centile compared to living in rural areas.
Education and employment status of the patients in our study had no relation with HRQoL similar to Ethiopian and Indian studies. However, unlike these studies, our study found there is a relationship between marital status and HRQL. Those who are divorced have lower health related QOL compared to married one.17, 18
In contrast to other Ethiopian study, in our study, the patient’s HRQoL was affected by the presence of comorbidity and the number of medications they were taking.18 This could be explained by additional burden of comorbidities and number of medications on the patient health. The other that determine QOL is whether intervention was done or not. The odds of physical and mental summary scores to lie in the lower centile decreases after intervention done. Studies conducted in Fiji Island, and Nepal backed up this finding.19, 20 This could be explained by the fact that patients generally recover significantly following surgery, and that their symptoms and drug load also decrease.
Limitation of Study
The main limitation of this study was its cross sectional nature of the study. There may be difficulty of recall issue. The other limitation luck of instrument available to assess health-related QOL of RHD. In other setting they use SF-36 to assess HRQOL of RHD patients with good result. So we used this tool. It would have been better to assess effect of intervention on QOL before and after intervention on same type of patients. Other limitation was there may translation issue because SF-36 tool is written in English. The last point is we have not assessed New york heart association functional classification which also decrease QOL.
Conclusion
RHD patients had poor QOL assessed by SF-36. It affects all domains and summary score. Old age, divorced, living in rural area, associated comorbid conditions and no intervention done are associated with poor QOL. Identification and treating comorbid conditions and intervention may improve QOL.
Abbreviations
ARF, Acute Rheumatic Fever; BP, Bodily pain; CDC, Center for Disease Control; CRHD, Chronic Rheumatic Heart Disease; GH, General Health; HF, Heart Failure; HRQOL, Health-Related Quality of Life; MCS, Mental component summary; MH, Mental Health; NGO, Nongovernmental organization; PF, Physical Function; PCA, Principal component analysis; PCS, physical component summary; QOL, Quality of Life; RE, Limitation in role due to emotions; RHD, Rheumatic Heart Disease; RP, Limitations in role due to physical health; SF-36, Short Form-36; SF, Social Function; Std/SD, Standard deviation; TASH, Tikur Anbessa Specialized Hospital; VT, Vitality.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent and Ethical Clearance
The study complied with the Declaration of Helsinki. A letter of ethical clearance was obtained from Addis Ababa University, College of Health Sciences, Institutional Review Board (protocol number = 06/21SNM). Written informed consent was obtained from each patient to participate in the interview and to extract data from their medical charts. Privacy and confidentiality were ensured during patient interview and medical chart review.
Acknowledgment
We would like to acknowledge the participants and data collectors for providing us consent to share his history and collecting data respectively. We also want to mention our gratitude to Addis Ababa University for giving us ethical clearance. This paper is based on the thesis of Konno Taddesse. It has been published on the institutional website: http://etd.aau.edu.et/handle/123456789/28826
Disclosure
The authors declare that there is no conflicts of interest in this work.
References
1. Leal MT, Passos LS, Guarçoni FV, et al. Rheumatic heart disease in the modern era: recent developments and current challenges. Rev Soc Bras Med Trop. 2019;52. doi:10.1590/0037-8682-0041-2019
2. World Health Organization. Rheumatic fever and rheumatic heart disease. report by the director general. seventy-first world health assembly. Geneva, Switzerland: World Health Organization. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_25-en.pdf.201.
3. Watkins DA, Beaton AZ, Carapetis JR, et al. Rheumatic heart disease worldwide: JACC scientific expert panel. J Am Coll Cardiol. 2018;72(12):1397–1416. doi:10.1016/j.jacc.2018.06.063
4. Marijon E, Mirabel M, Celermajer DS, Jouven X. Rheumatic heart disease. Lancet. 2012;379(9819):953–964. doi:10.1016/S0140-6736(11)61171-9
5. Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N Engl J Med. 2017;377(8):713–722. doi:10.1056/NEJMoa1603693
6. Wennberg JA. Perspective: AHCPR and the strategy for health care reform. Health Aff. 1992;11(4):67–71. doi:10.1377/hlthaff.11.4.67
7. Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers. 2016;2(1):1–24.
8. Marino BS, Shera D, Wernovsky G, et al. The development of the pediatric cardiac quality of life inventory: a quality of life measure for children and adolescents with heart disease. Qual Life Res. 2008;17:613–626. doi:10.1007/s11136-008-9323-8
9. Negi PC, Kandoria A, Asotra S, et al. Gender differences in the epidemiology of Rheumatic Fever/Rheumatic heart disease (RF/RHD) patient population of hill state of northern India; 9 years prospective hospital based, HP-RHD registry. Indian Heart J. 2020;72(6):552–556. doi:10.1016/j.ihj.2020.09.011
10. Liang-Choo H, Rajaram N. A review of acute rheumatic fever and rheumatic heart disease research in Malaysia. Med J Malaysia. 2016;71:79–86.
11. Okello E, Longenecker CT, Beaton A, Kamya MR, Lwabi P. Rheumatic heart disease in Uganda: predictors of morbidity and mortality one year after presentation. BMC Cardiovasc Disord. 2017;17:1. doi:10.1186/s12872-016-0451-8
12. Dhar M, Kaeley N, Bhatt N, Ahmad S. Profile of newly diagnosed adult patients with rheumatic heart disease in sub-Himalayan region–a 5-year analysis. J Family Med Prim Care. 2019;8(9):2933. doi:10.4103/jfmpc.jfmpc_363_19
13. Myint NP, Aung NM, Win MS, et al. The clinical characteristics of adults with rheumatic heart disease in Yangon, Myanmar: an observational study. PLoS One. 2018;13(2):e0192880. doi:10.1371/journal.pone.0192880
14. Kebede D, Alem A, Shibre T, Negash A, Deyassa N, Beyero T. Health related quality of life (SF-36) survey in Butajira, rural Ethiopia: normative data and evaluation of reliability and validity. Ethiop Med J. 2004;42(4):289–297.
15. Arafa MA, Zaher SR, El-Dowaty AA, Moneeb DE. Quality of life among parents of children with heart disease. Health Qual Life Outcomes. 2008;6(1):1–7. doi:10.1186/1477-7525-6-91
16. Monib D, Wahdan I, Hasab A, Zaher S. Health related quality of life of rheumatic heart disease patients in Alexandria: an intervention approach. J High Inst Public Health. 2013;43(2):112–120. doi:10.21608/jhiph.2013.19997
17. Dixit J, Jyani G, Prinja S, Sharma Y. Health related quality of life among rheumatic fever and rheumatic heart disease patients in India. PLoS One. 2021;16(10):e0259340. doi:10.1371/journal.pone.0259340
18. Tadele H, Ahmed H, Mintesnot H, Gedlu E, Guteta S, Yadeta D. Subjective wellbeing among rheumatic heart disease patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia: Observational Cross-Sectional Study. BMC Health Serv Res. 2021;21:1. doi:10.1186/s12913-021-07378-0
19. Joshi D, Shrestha A, Gurung M, et al. Spectrum of quality of life after valve surgery in patients with rheumatic heart disease. Nepal Heart J. 2021;18(1):53–56. doi:10.3126/njh.v18i1.36786
20. Mangnall LJ, Sibbritt DW, Fry M, Windus M, Gallagher RD. Health-related quality of life of patients after mechanical valve replacement surgery for rheumatic heart disease in a developing country. Heart Asia. 2014;6(1):172–178. doi:10.1136/heartasia-2014-010562
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.