Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Health Educational Methods for Improving Self-Efficacy Among Patients with Coronary Heart Disease: A Scoping Review
Authors Sugiharto F ![]() , Haroen H, Alya FP
, Haroen H, Alya FP ![]() , Jamlaay R, Mai F, Abdillah H, Yusanti I, Assidiqy B, Nuraeni A
, Jamlaay R, Mai F, Abdillah H, Yusanti I, Assidiqy B, Nuraeni A ![]()
Received 27 December 2023
Accepted for publication 14 February 2024
Published 22 February 2024 Volume 2024:17 Pages 779—792
DOI https://doi.org/10.2147/JMDH.S455431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Firman Sugiharto,1,* Hartiah Haroen,2,* Fania Putri Alya,1,* Ruth Jamlaay,1,* Freda Mai,1,* Hadi Abdillah,1,* Irma Yusanti,1,* Birry Assidiqy,1,* Aan Nuraeni3,*
1Master Study Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Community Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Emergency and Critical Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Firman Sugiharto, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6282218235600, Fax +6202287793411, Email [email protected]
Background: Coronary heart disease (CHD) is the leading cause of death and disability worldwide, with higher prevalence in low and middle-income countries. Self-efficacy (SE) is an essential element that affects a patients ability to manage their care, and low SE levels in patients with CHD can lead to poor health outcomes and quality of life. Planning suitable methods to improve SE in CHD patients is essential.
Purpose: This review explores health education methods to improve SE in patients with CHD.
Methods: Scoping review is reported based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR). A literature search was conducted using relevant keywords from six primary databases, such as CINAHL Plus with Full Text and Academic Search Complete, PubMed, ScienceDirect, Scopus, Taylor and Francis, and one search engine, Google Scholar. The inclusion criteria were full-text articles in English that were accessible, research articles with experimental designs. The quality of evidence was assessed using the Joanna Briggs Institute critical appraisal checklist, and data synthesis was used thematically with an explorative, descriptive approach.
Results: Fifteen articles were found and included in the review. There are two types of interventions such as traditional and digital-based health education. The media used in traditional health education are booklets, pamphlets, posters, and workbooks. In addition, digital-based health education generally uses websites, social platforms, mobile applications, video players and sound clips.
Conclusion: This review found that traditional health education and digital-based interventions improve SE, knowledge, self-esteem and health literacy levels, in CHD patients. Health professionals, including nurses, may used both methods in improving self efficacy in CHD patients.
Keywords: coronary heart disease, digital intervention, health education, self-efficacy
Introduction
Coronary heart disease (CHD) is still a significant health problem with high morbidity and mortality rates globally.1 The higher prevalence of CHD occurs in low- and middle-income countries, with estimates accounting for up to 82% of total global deaths.2 In 2020, the death rate due to CHD reached 112.37 per 100.000, with the highest death rates occurring in North Africa and the Middle East, Eastern Europe and Central Asia.3 This death rate is estimated to continue to increase to 24.2 million people in 2030. Meanwhile, deaths in Indonesia due to CHD in 2019 reached 245,343 out of a total of 651,481 deaths each year.4
The increase in mortality and morbidity rates in CHD patients is consistent with the lack of self-care and compliance in participating cardiac rehabilitation.5,6 Previous reviews reported that CHD patients have low participation rates in cardiac rehabilitation (≤50%).7 Similarly, several previous studies also indicated that the level of self-care in CHD patients tends to be low,8–10 and it impacts the hospital stay and patient’s quality of life.6,11 Moreover, previous reviews also reported that there was a relationship between the level of self-care and QoL in patients with CHD and poor self-care can directly impact QoL in CHD patients.12 Therefore, paying attention to factors that can influence CHD patients’ self-care and rehabilitation compliance is essential.
Self-efficacy (SE) is essential to a patient’s self-care ability.13 SE is defined as an individual’s belief in the ability to carry out the steps necessary to achieve the desired results.14 In the context of CHD, SE means patient’s belief in the ability to manage the signs and symptoms of cardiovascular disease.15 A low level of SE in CHD patients will result in a lack of self-acceptance, poor health conditions, and the emergence of depressive symptoms.16 In addition, it is argued that low SE also have a negative effect on self-care, especially in terms of physical activity.6,17 In contrast, patients with higher SE tend to have better psychological well-being, a higher quality of life, and more compliance with cardiac rehabilitation and self-care programs.18–20 Therefore, it is argued that CHD patients are encourage to have high SE in order to improve their ability to manage and maintain their self-care througout the trajectory of disease.21
Several factors may influence SE in CHD patients. The factors include demographic characteristics, such as age, gender, body mass index (BMI), income level, and education level.22–24 Previous reviews reported that the level of knowledge about heart disease and awareness were the main predictors of SE in CHD patients.13 Knowledge about the disease contributes to appropriate understanding of the condition and also increases the level of adherence to a healthy lifestyle that can prevent CHD. Therefore, it is argued, when a patient has sufficient knowledge about CHD, the level of SE in CHD prevention efforts will also be higher.25
Knowledge is the main predictor of low SE in CHD patients. Patient education is the main thing that needs to be paid attention to by health professionals.13 Nevertheless, increasing knowledge of CHD patients requires appropriate strategies to convey essential information to reach the goal of health education. Several previous studies concluded that education using booklets, peer education, electronic-based education with social media platforms, and workbooks significantly increase knowledge about CHD and SE in CHD patients.26–29 These interventions have been proven to improve CHD patients’ understanding about what should they do to manage their disease in daily basis.30
Based on the results of the literature search, there are no literature studies that summarize and analyze educational methods to improve SE in the CHD population. Previous reviews discussing strategies to improve SE in patients with chronic diseases did not focus on patients with CHD.31 In addition, other reviews only discuss the effectiveness of internet-delivered self-management support in CHD patients.32 So, this study is the first scoping review which identify the health education methods in improving SE in patients with CHD. By comprehensively exploring and analyzing various educational strategies, this scoping review aims to provide information to health professionals and policymakers to promote a deeper understanding of effective methods to improve SE among patients with CHD. This insight is critical in developing targeted and impactful health education initiatives, which can ultimately contribute to improved patient outcomes.
Materials and Methods
Design
The design used in this study was a scoping review. A scoping review is a flexible methodological technique for exploring new, rapidly developing topics.33 This design has a more comprehensive conceptual scope to explain relevant research results. The scoping review framework consists of 5 core stages: identifying review questions, identifying relevant literature, selecting eligible studies or literature, extracting and mapping data, compiling, summarizing and reporting the results.33 The PRISMA Extension for Scoping Reviews (PRISMA-ScR) was used in this literature review to find types of health education methods that effectively improve SE in patients with CHD. This review has followed the PRISMA-ScR checklist guidelines (Supplementary Table 1).
Eligibility Criteria
The articles were selected for this review by six reviewers based on the PRISMA Extension for Scoping Review (PRISMA-ScR) (see Figure 1).34 Research questions and eligibility criteria for research articles using the PCC approach (Population, Concept, and Context).
 |
Figure 1 PRISMA flow diagram. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.34. |
P (Population): Patients with CHD
C (Concept): Health Educational Methods
C (Context): Self Efficacy
In this review, full-text articles that were inaccessible, not in English, and secondary research were excluded. The inclusion criteria in this review are published in English and articles with an experimental design (Randomized controlled trial and Quasi-Experimental). In addition, this review has no criteria for limiting publication years because it looks at various types of methods related to the topic so that the search for studies is comprehensive. Then, the determination of SE criteria in this review includes general SE, cardiac SE, and cardiac exercise SE which are the outcomes in each study analyzed.
Data Collection and Analysis
Search Strategy
Searching of articles was carried out systematically using five primary databases: CINAHL Plus with Full Text and Academic Search Complete, PubMed, ScienceDirect, Scopus, and Taylor and Francis, and Google Scholar search engine. The author uses the Boolean operators “AND” and “OR” to trim or expand the search results for various tenses. The keywords used were “coronary heart disease OR coronary artery disease OR myocardial infarction OR cardiovascular disease OR Heart Disease AND Education Methods OR Teaching Methods OR Health Education AND Self Efficacy OR Cardiac Self Efficacy OR General Self-efficacy”. Each term verified by MeSH (Medical Subject Headings), synonyms are used to retrieve all possible relevant articles (Supplementary Table 2).
Study Selection and Quality Appraisal
Three authors (F.S., F.P.A., and R.J) independently selected studies that met eligibility criteria. The authors checked for duplication in the initial selection process using the Mendeley reference manager. Then, the author checked the title, abstract, and full text for relevance to the research topic and establish inclusion and exclusion criteria. All articles that met the criteria were examined and further evaluated for quality using the Joanna Briggs Institute (JBI) critical assessment checklist by four authors (F.M, H.A, I.Y, and B.A).35 The critical assessment consists of 13 questions for randomized control trial design articles and nine for quasi-experimental designs. Each question consists offours response choices: Yes, No, Not Applicable, and Unclear. The answer “Yes” was given a score of 1, and other answers were given a score of 0. After the assessment, the authors eliminated all studies with a JBI score less than 75% and the final determination of included articles was carried out by two other researchers considered as experts in nursing (H.H and A.N). Any differences between the evaluators were discussed to obtain a firm agreement. All authors had no differences of opinion regarding the appropriateness of this research.
Data Extraction and Analysis
In this review, data extraction from the studies is analyzed using tables that describe in detail all the results related to the topic discussed. The information presented in the extraction table relates to the characteristics of the research, including: country, outcome, design, sample, intervention (educational methods and setting) and research results. All studies included were experimental primary research with RCT and quasi-experimental designs. Therefore, data analysis was carried out thematically using an exploratory descriptive approach. The data analysis process begins with identifying and presenting the obtained data in table form based on the articles reviewed. After obtaining the data, all authors analyzed and explained each finding based on educational methods that can improve SE in CHD patients. Finally, the authors double-checked the included studies to ensure and minimize errors in the data extraction process.
In the intervention categorization, the author divides interventions into two categories: Traditional and Digital-Based Health Education. Traditional-based intervention is a method of providing intervention that is carried out using conventional methods, including face-to-face counselling, group intervention, workbooks or printed materials, and direct counselling by professional health workers.31 In addition, digital-based intervention delivers interventions involving digital technology, such as software, mobile applications, or online platforms that include web-based interventions, mobile-based interventions, digital health games, and specially designed social media platforms.36
Results
Study Selection
An initial literature search from several databases and one search engine obtained 1950 research articles. Next, the authors filtered research based on title, abstract, and inclusion criteria, resulting 1829 articles remained. Next, the author filtered 1829 articles based on predetermined inclusion criteria and the remaining 97 articles. Then, of these 97 articles, the full texts were read. The author excluded 82 articles because the population and sample did not match (n=43), they were not published in English (n=5), and the study outcome did not match the main aim of this review (n =35) and the remaining 15 research articles. Then, the authors assessed the quality of the articles using the JBI critical appraisal tool. The results of the JBI that the majority of research was of good quality (>75%) (see Table 1). As a result, the authors included 15 studies in this review. Figure 1 illustrates the number of studies retrieved using the PRISMA flow chart diagram.
 |
Table 1 JBI Critical Appraisal Results |
Study Characteristics
There are 8 RCT and 7 quasi-experimental studies in CHD populations. Almost all of the articles are from countries on the Asian continent, including Thailand (n=3), Hong Kong (n=3), Iran (n=6), Egypt (n=4), Indonesia (n=3), China (n=3), and Brazil (n=1) (see Table 2). All participants (n=1961, IG=979; CG=982) in the articles analyzed in this review were patients with CHD, most of whom had primary to secondary school education levels. Then, JBI results in RCT studies, most research did not explain aspects of treatment delivery without knowing the treatment assignment, and outcomes assessors were blind to treatment assignment. In contrast, in quasi-experimental studies, most of the study did not carry out follow-ups.
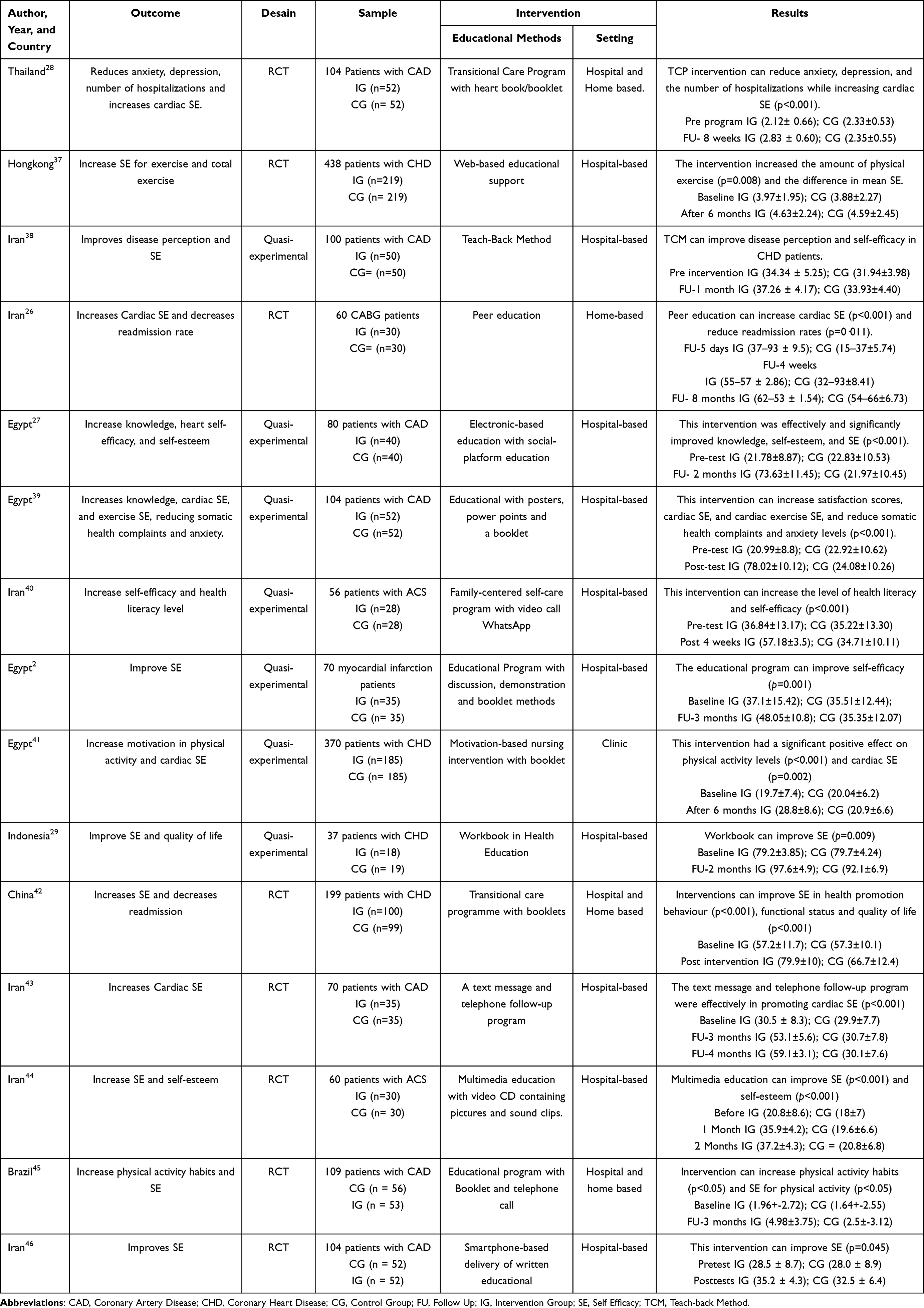 |
Table 2 Characteristics of Study |
Health Education Methods
It is found that 15 educational methods were carried out in hospitals, clinics, and patients’ homes. Table 3 shows that the most frequently used media is booklets,2,28,39,41,42 and intervention frequency in 1–6 sessions. However, four studies did not mention the frequency of intervention delivery.27,29,39,45 Then, only three studies used simulation or practice methods.2,27,42 In this review, the authors categorize the 15 intervention methods into two categories: traditional health education and digital-based health education (see Table 3).
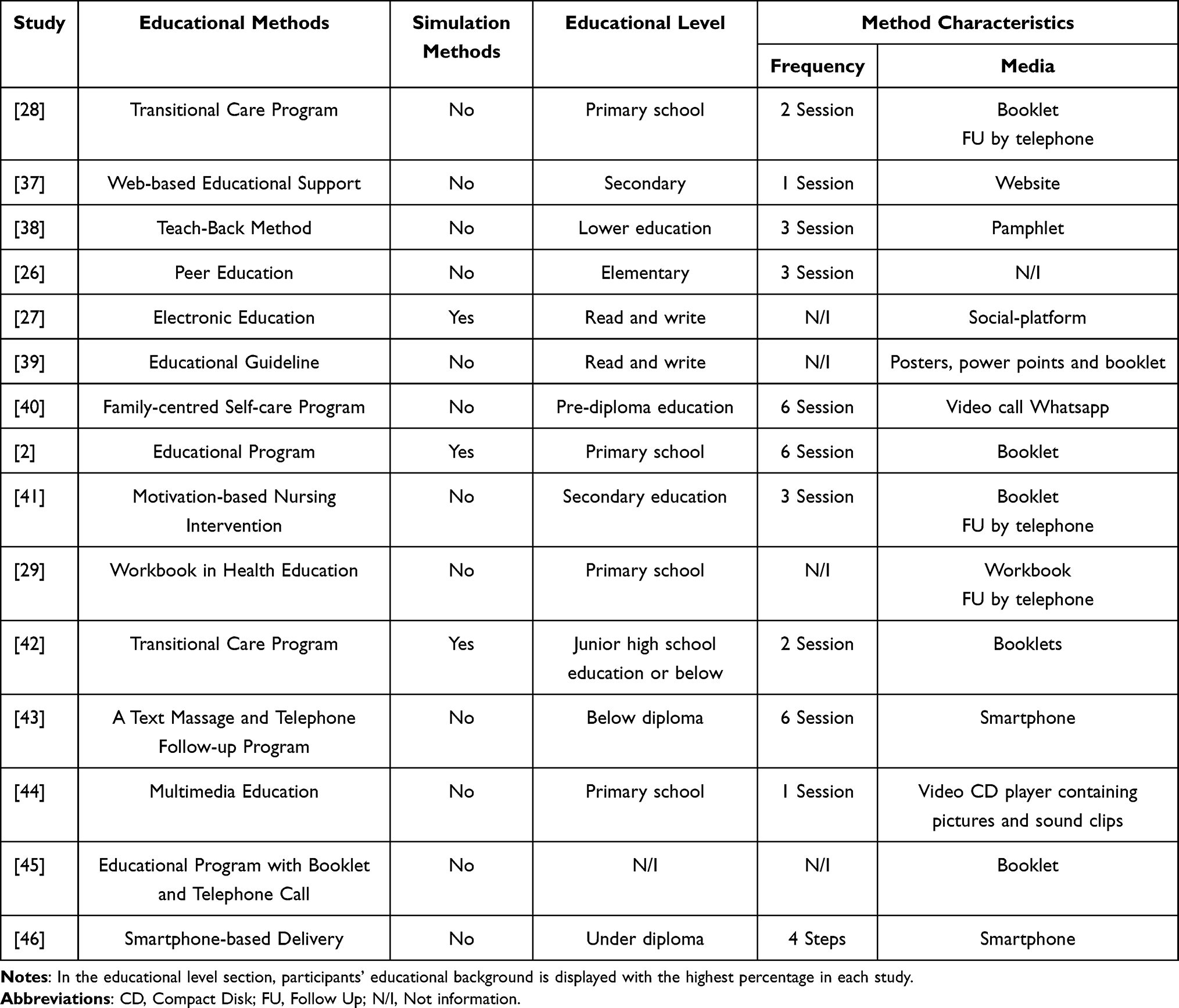 |
Table 3 Characteristics of Educational Methods |
Traditional Health Education
In this review, most media used were booklets with various educational content. The transitional care program intervention emphasizes providing information regarding the initial management of heart symptoms, lifestyle modification, and the use of medication packaged in a heart book/booklet.28 This intervention was led by a cardiovascular specialist nurse and was carried out during 2 phases, namely during discharge planning and after discharge from the hospital. Health education was provided for approximately 20 minutes before discharge, and follow-up was carried out by telephone 48 hours after discharge from the hospital. Next, the second phase is followed up once a week for six weeks, which lasts around 10 to 20 minutes. This phase carries out follow-up which includes four main elements: monitoring, education and counselling, psychological support, and coordination with the health team if necessary.28
Transitional care program interventions are also carried out by P. Zhang et al. This intervention, which is also led by nurses, consists of 2 phases, namely pre-discharge (around one week before the patient goes home) and post-discharge (7 months).42 In the pre-discharge phase, patients are given health education, with the media used was handout booklets that contain content information including healthy eating patterns, exercising regularly, managing stress, building positive relationships, and being responsible for health. In the post-discharge phase, patients attend educational session and home visits once a week for the first month and group activities once or twice weekly.42
Another intervention is an educational program with discussion, demonstration and booklet methods.2 This educational program consists of 6 sessions, which include theory and practice. In the theory part, patients are given a booklet designed according to CHD patients’ learning needs, covering four sessions. Apart from that, the practical part consists of 2 sessions, which contain steps in carrying out self-care and SE.2
Motivation-based nursing intervention can significantly increase SE in CHD patients. The intervention consisted of 3 sessions conducted in the heart clinic and a follow-up by telephone one week after hospital discharge.41 The researchers provided 40 minutes of face-to-face education on characteristics, signs and symptoms, risk factors, CHD management and medication adherence. Apart from that, patients are also taught how to do physical exercise at home. Then, a brief telephone follow-up is conducted to help patients gain greater motivation to engage in exercise, adhere to a healthy diet, and improve their problem-solving abilities.41
Pitta et al and Ebraheim and Khorais also conduct research on health education programs using booklets.39,45 In Pitta et al, the booklet contains information regarding guidance on nutrition, risk factor management, smoking cessation, psychosocial support, and the importance of physical activity, followed up to motivate individuals to fulfil the recommended physical activity and lifestyle changes.45 Meanwhile, in Ebraheim and Khorais, educational media is not only booklet but also poster and PowerPoint point, which include information related to CHD, steps to overcome complications, nutritional management, and steps to increase the level of knowledge, self-efficacy, health complaints, and anxiety levels.39
Another traditional health education method is the tech-back method using pamphlet. This method was carried out individually in three sessions over three days.38 The first training session was conducted at the patient’s bedside one day after hospitalization and after the patient was stable and each session was approximately 30 to 45 minutes. Next, a final session was held at the patient’s home, where the patient was asked to recalltaught CHD concept or topic in his or her own words. If the patient does not understand the material provided, the learning material was repeated to them.38
Besides booklets, PowerPoint presentations, and pamphlets, intervention using workbooks also increases SE in CHD patients.29 The workbook was designed based on an assessment of the learning needs of CHD patients, which includes cardiovascular anatomy and physiology and management of CHD symptoms, such as CHD patient activities in the hospital and at home, controlling lifestyle risks, fulfilling sexual needs, stress management with drugs, and CPR. The workbook contains CHD management implementation records which are filled in by the patient every day.29
The peer education intervention consisting of 3 sessions carried out in the hospital increases SE in CHD patients.26 A peer is a patient who has undergone CABG and has been trained by experts regarding the benefits of peer education, controlling dyspnea, fatigue, chest pain, body weight, eating patterns, regular activity levels and social interactions. Then, the peer educates the patient before and after undergoing CABG, each session lasting for 60 minutes. This intervention significantly increases cardiac SE.26
Digital-Based Health Education
Several methods are used in digital-based interventions to improve SE in CHD patients. Web-based educational support is provided to patients, which includes information about CHD, its risk factors, and suggestions for lifestyle modifications.37 This website is given to patients to take home after a 20-minute health education session previously conducted in hospital by a trained nurse.37 Participants are advised to do brisk walking for at least 30 minutes over a distance of around 2.5–3 km (around 5–6 laps of a running track/soccer field in HK) every five times weekly.
Electronic-based education with social platforms has also proven effective in increasing SE in CHD patients.27 The social platform used is the WhatsApp application in which health education is provided, including the definition of CAD, its aetiology, diet, appropriate use of heart medication, stress management strategies, and physical activity. In addition, information regarding steps to overcome complications and increase patient self-efficacy is also provided using a video CD containing images and sound clips every day.27
Ghaemmaghami et al also used the WhatsApp application, where this intervention is based on a family centered-self-care program.40 SE training emphasises the influential role of the individual and other family members in 6 sessions lasting 45 to 60 minutes. This intervention was carried out via direct WhatsApp video calls.40
Multimedia education with CDs containing pictures and sound clips is given to patients as guidance during home treatment.44 They were also given a reminder checklist, including diet adherence, physical activity, heart medication, smoking cessation, and stress management. They were asked to rate their compliance by marking the weekly checklist items for eight consecutive weeks. Weekly telephone contacts were made to remind participants to use the educational program.44
Another digital-based intervention is a text message and telephone follow-up program.43 This intervention was carried out via text messages and telephone for three months. Six text messages with a maximum of 160 words were sent to patients weekly, and 72 text messages were sent within three months. In addition, telephone calls were also made twice a week in the first month and once a week in the following months. The duration of the call was 15 minutes, and a total of 16 calls were made to discuss cardiac SE assessment.43
The last digital intervention in education to improve SE is smartphone-based.46 This educational method was delivered using the smartphone (SPBD) and the control group used printed delivery (pamphlets) method. The patient is then connected to an electronic web page containing educational materials via smartphone. This page features educational content on three main topics: disease and treatment approaches, diagnostic and therapeutic methods, and treatment. Patients can access relevant educational materials by selecting each material. The educational method using the smartphone is reported to be more effective in increasing self-efficacy in the treatment process.46
Discussion
This study is the first scoping review that discusses health education methods to improve SE in CHD patients. This scoping review shows that many health education methods can improve SE, especially in the CHD population. All participants in this study were CHD patients, and almost all of the study was conducted in Asia. Based on the research results, the author found 15 interventions, which were then categorized into two methods, namely traditional and digital-based health education.
Traditional health education has been widely carried out and proven effective in increasing patient knowledge and SE in the CHD population.2,26,28,29,38,39,41,42,45 Based on the review results, this traditional method can provide various programs or interventions such as teach-back methods, peer education, specially designed educational programs, and transitional care programs. This method can be used when patients are still being treated in the hospital, during transitions of care, and even independently/assisted in the patient’s home or home-based interventions.28
Some of these traditional methods can not only increase knowledge and SE. Previous studies reported that the teach back method using pamphlets can also improve disease perception in CAD patients.38 This method also improves disease perception among patient with hypertension s, nutritional knowledge, and diet compliance.47 Similarly, other research also reports that traditional methods with peer education can reduce readmission rates.26 Then, educational programs designed explicitly by researchers using posters, power points and booklets can also reduce somatic health complaints and anxiety levels in CAD patients,39 and improve health promotion behaviour, functional status and quality of life.42 Therefore, this traditional method can be an option or alternative for health professionals to improve health outcomes, especially in the patient population with CHD.
This review shows that booklets are the media most widely used in this traditional method.2,28,38,39,41,42,45 The use of booklets/leaflets can provide clarity of information with a structured and practical layout.45 In addition, this media is relatively easy to produce and be accepted by individuals or society to reach a wider audience. The advantage of booklets/leaflets is their portability, as patients can carry the information and refer back to the relevant material when necessary.28 However, although booklets or leaflets can be an effective medium in many cases, booklets also have several disadvantages that need to be considered, such as limited information presented, and individuals with reading barriers will find it difficult. The possibility of damage and the risk of not being read by the patient is very high, so it needs to be designed as attractively as possible to be used sustainably.48
Interventions to increase SE in CHD patients can also be implemented using digital technology.27,37,40,43,44,46 This review found that, digital-based intervention refers to providing health education that involves digital technology, such as mobile applications and online platforms, including websites, digital health games, and specially designed social media.36 The findings of this review show that education based on websites, social platforms, WhatsApp video calls, use of smartphones, and use of multimedia such as videos and sound clips have proven effective in increasing SE in CHD patients.27,37,40,43,44,46 In addition, digital-based health education can also improve other outcomes in CHD patients such as knowledge, health literacy, self-esteem, and others.
In this review, digital-based health education is not only effective in increasing SE. Previous studies reported that technology intervention programs can improve patient knowledge and self-esteem.27,44 A study in Iran also reported that the intervention of a family-centred self-care program with WhatsApp video calls significantly increased health literacy and cardiac SE.40 This can help patients feel more confident and able to take the necessary steps to improve their heart health.40 Therefore, the many benefits obtained indicate that technology can effectively deliver health programs, especially in the context of long-distance services.
Several benefits can be obtained when carrying out digital-based health education. The use of mobile technology in developing countries has increased patient awareness regarding their current healthcare services.49,50 The technology also provides opportunities to increase access to health promotion interventions. The techological-based health education has advantages such as, accessibility that can be acessed anytime and anywhere, and the ability to communicate and send information in various ways.51 Therefore, health professionals, including nurses, can consider this digital-based intervention, which is considered effective in improving several health-related outcomes, especially in patients with CHD.
Various factors can influence the health education process using traditional and digital methods.52 In this review, most of the participants in each study had a primary and secondary school educational background, which is likely to be a factor that can influence the level of SE.2,26–29,37–39,41,42,44 Other factors, such as limited access to information, the relationship between patients and health professionals, self-regulation, and environmental factors, can also influence patient education.52 Factors influencing the digital-based health promotion method are technological support and the accessibility of the digital devices used. Adequate technological support and device accessibility are essential to ensure that patients can easily use a digital-based education platform.27
In general, traditional health education methods in this review are based on media use. Although several studies have utilized telephone or call features for the patient follow-up process, this review still includes traditional methods. This is because the follow-up process mostly only aims to remind patients. However, using applications such as WhatsApp in traditional methods does not eliminate the possibility of impacting the results obtained. Therefore, this review still fully recommends both methods, which can be applied in healthcare areas and hospitals.
Strengths and Limitations
There are several limitations to this review. First, the articles in this review were mostly conducted in Asian countries, so the results may be not relevant for countries outside the Asian countries. In fact, this review has carried out a systematic search strategy from five main databases and one search engine with no restrictions on the year of article publication. Second, the characteristics of the participants have heterogeneous educational backgrounds, so this is likely to influence the results of existing research. However, the entire sample in this review was CHD patients totalling 1961 participants (IG=979; CG=982) to minimize bias in the results of this study. Third, the research sample is relatively small, so researchers recommend that future research be able to increase participants and reach a wider range of research settings and places. Therefore, this may increase the generalizability of the findings in this review.
Conclusions
This review found two health education methods, traditional and digital-based, equally effective for increasing SE in patient populations with CHD. The media most widely used to facilitate the implementation of traditional health education is booklets, while digital-based ones mostly use mobile applications.
This review can provide an overview for health professionals in planning health education strategies appropriate to the work conditions and environments. In addition, health professionals including nurses can consider both methods in providing health education carried out both inside and outside health services. Then, because most of the research on this method was carried out on the Asian continent, the author recommends that future research be carried out in countries in Europe, America or other continents to increase the generalization of the findings in this review.
Acknowledgments
All authors thank to Universitas Padjadjaran, Bandung, West Java, Indonesia, who has facilitated the database for us in this study.
Disclosure
The authors report no conflicts of interest in this research.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi:10.1161/CIR.0000000000000757
2. Yelvita FS. Effect of an educational program on self- efficacy for patients with myocardial infraction. J Nurs Sci. 2022;3(1):1.
3. American Heart Association. 2023 heart disease and stroke statistics update fact sheet; 2023. Available from: https://professional.heart.org/en/science-news/heart-disease-and-stroke-statistics-2023-update.
4. Ministry of Health Republic of Indonesia. Prevent heart disease by implementing CERDIK and PATUH behavior. Sehat Negeriku; 2023. Available from: https://sehatnegeriku.kemkes.go.id/baca/rilis-media/20230925/4943963/cegah-penyakit-jantung-dengan-menerapkan-perilaku-cerdik-dan-patuh/.
5. Fang J, Wang JW, Li J, Li H, Shao C. The correlates of social capital and adherence to healthy lifestyle in patients with coronary heart disease. Patient Prefer Adherence. 2017;11:1701–1707. doi:10.2147/PPA.S140787
6. Ahn S, Song R, Choi SW. Effects of self-care health behaviors on quality of life mediated by cardiovascular risk factors among individuals with coronary artery disease: a structural equation modeling approach. Asian Nurs Res. 2016;10(2):158–163. doi:10.1016/j.anr.2016.03.004
7. Sugiharto F, Nuraeni A, Trisyani Y, Melati Putri A, Aghnia Armansyah N. Barriers to participation in cardiac rehabilitation among patients with coronary heart disease after reperfusion therapy: a scoping review. Vasc Health Risk Manag. 2023;19:557–570. doi:10.2147/VHRM.S425505
8. Sidaria S, Huriani E, Nasution SD. Self Care dan Kualitas Hidup Pasien Penyakit Jantung Koroner (Self care and quality of life for coronary heart disease patients). Jik J Ilmu Kesehat. 2023;7(1):41.
9. Zhang S, Wang Z, Lin X, et al. Kinesiophobia and self-management behaviour related to physical activity in Chinese patients with coronary heart disease: the mediating role of self-efficacy. Nurs Open. 2023;10(1):105–114. doi:10.1002/nop2.1283
10. Maruta M, Moriyama S, Mizuguchi Y, et al. Evaluation of the determinant factors and clinical implications of self-care agency among patients with acute myocardial infarction. Clin Nurs Res. 2021;30(2):207–214. doi:10.1177/1054773820933450
11. Sugiharto F, Trisyani Y, Nuraeni A, Mirwanti R, Melati Putri A, Aghnia Armansyah N. Factors associated with increased length of stay in post primary percutaneous coronary intervention patients: a scoping review. Vasc Health Risk Manag. 2023;19:329–340. doi:10.2147/VHRM.S413899
12. Harsono H. The relationship between self care and quality of life among coronary heart disease patient after receiving percutaneous coronary intervention: a systematic review. In:
13. Sugiharto F, Nuraeni A, Trisyani Y, Putri A, Armansyah N, Zamroni A. A scoping review of predictors associated with self-efficacy among patients with coronary heart disease. Vasc Health Risk Manag. 2023;19:719–731. doi:10.2147/VHRM.S435288
14. Nuraeni A, Sugiharto F, Anna A, et al. Self-efficacy in self-care and its related factors among patients with coronary heart disease in Indonesia: a rasch analysis. Vasc Health Risk Manag. 2023;19:583–593. doi:10.2147/VHRM.S427488
15. Wahyuni A, Setyowati S. Concept analysis of self efficacy among coronary heart disease patients undergoing percutaneous coronary intervention. J Aisyah J Ilmu Kesehat. 2022;7(4):1051–1058.
16. Wantiyah RFRP, Hakam M. The correlation between religiosity and self-efficacy in patients with coronary artery disease. Belitung Nurs J. 2020;6(5):172–176. doi:10.33546/bnj.1134
17. Woodgate J, Brawley LR. Self-efficacy for exercise in cardiac rehabilitation: review and recommendations. J Health Psychol. 2008;13(3):366–387. doi:10.1177/1359105307088141
18. Al-Sutari M, Ahmad M. Predictors of adherence to self-care behaviors among patients with coronary heart disease. Nurs Pract Today. 2022;9(2):145–157.
19. Fahmi I, Suryaman A, Ganefianty A. The relationship of psychological well-being with a cardiac diet self efficacy in acute coronary syndrome patients. J Pendidik Keperawatan Indones. 2022;8(2):119–126. doi:10.17509/jpki.v8i2.51066
20. Almeida JAB, Florêncio RB, Lemos DA, Leite JC, Monteiro KS, Peroni Gualdi L. Self-efficacy instruments for individuals with coronary artery disease: a systematic review protocol. BMJ Open. 2022;12(7):1–4. doi:10.1136/bmjopen-2022-062794
21. Sol BGM, van der Graaf Y, van Petersen R, Visseren FLJ. The effect of self-efficacy on cardiovascular lifestyle. Eur J Cardiovasc Nurs. 2011;10(3):180–186. doi:10.1016/j.ejcnurse.2010.06.005
22. Chair SY, Wong KB, Tang JYM, Wang Q, Cheng HY. Social support as a predictor of diet and exercise self-efficacy in patients with coronary artery disease. Contemp Nurse. 2015;51(2–3):188–199. doi:10.1080/10376178.2016.1171726
23. Shrestha R, Rawal L, Bajracharya R, Ghimire A. Predictors of cardiac self-efficacy among patients diagnosed with coronary artery disease in tertiary hospitals in Nepal. J Public Health Res. 2020;9(4):1787. doi:10.4081/jphr.2020.1787
24. Kang Y, Yang I. Cardiac self-efficacy and its predictors in patients with coronary artery diseases. J Clin Nurs. 2013;22(17–18):2465–2473. doi:10.1111/jocn.12142
25. Suarningsih NKA, Saputra IK. Effectiveness of education using ha-man module on self-efficacy of adults in preventing coronary heart disease. Bali Med J. 2021;8(3):294–299.
26. Varaei S, Shamsizadeh M, Cheraghi MA, Talebi M, Dehghani A, Abbasi A. Effects of a peer education on cardiac self-efficacy and readmissions in patients undergoing coronary artery bypass graft surgery: a randomized-controlled trial. Nurs Crit Care. 2017;22(1):19–28. doi:10.1111/nicc.12118
27. Ebrahim El Tahry S, Anwar Aly A, Mohammed EM, Mohammed Ibrahim Ibrahim N. Effect of social-platform educational instructions on self-efficacy and self esteem of patients with coronary artery diseases. Egypt J Health Care. 2022;13(1):1888–1906. doi:10.21608/ejhc.2022.249391
28. Yuroong A, Asdornwised U, Pinyopasakul W, Wongkornrat W, Chansatitporn N. The effectiveness of the transitional care program among people awaiting coronary artery bypass graft surgery: a randomized control trial. J Nurs Scholarsh. 2021;53(5):585–594. doi:10.1111/jnu.12673
29. Nuraeni A, Mirwanti R, Anna A. Effect of a workbook in health education on self-efficacy and quality of life of patients with coronary heart disease. Belitung Nurs J. 2019;5(6):218–224. doi:10.33546/bnj.801
30. Chen AMH, Yehle KS, Plake KS, et al. The role of health literacy, depression, disease knowledge, and self-efficacy in self-care among adults with heart failure: an updated model. Heart Lung. 2020;49(6):702–708. doi:10.1016/j.hrtlng.2020.08.004
31. Farley H. Promoting self-efficacy in patients with chronic disease beyond traditional education: a literature review. Nurs Open. 2020;7(1):30–41. doi:10.1002/nop2.382
32. Palacios J, Lee GA, Duaso M, et al. Internet-delivered self-management support for improving coronary heart disease and self-managementyrelated outcomes a systematic review. J Cardiovasc Nurs. 2017;32(4):E9–E23. doi:10.1097/JCN.0000000000000392
33. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. doi:10.1002/2327-6924.12380
34. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
35. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. Joanna Briggs Institute; 2022 Available from: https://jbi.global/critical-appraisal-tools.
36. McCall M, Spencer E, Owen H, Roberts N, Heneghan C. Characteristics and efficacy of digital health education: an overview of systematic reviews. Health Educ J. 2018;77(5):497–514. doi:10.1177/0017896918762013
37. Wong EML, Leung DYP, Chair SY, Sit JWH. Effects of a web-based educational support intervention on total exercise and cardiovascular risk markers in adults with coronary heart disease. Worldviews Evidence-Based Nurs. 2020;17(4):283–292. doi:10.1111/wvn.12456
38. Saadatian M, Yoosefian N, Kerman Saravi F, Yaghoubinia F. The effect of the teach-back method on illness perception and self-efficacy in patients with coronary artery disease. Med Surg Nurs J. 2022;11(1):1–9.
39. Ebraheim MN, Khorais AM. Effect of educational guidelines on cardiac self efficacy, health complaints and anxiety level among patients with coronary artery disease. Egypt J Health Care. 2016;7(4):406–431. doi:10.21608/ejhc.2016.104841
40. Ghaemmaghami A, Moeini M, Keshvari M. The effect of the family‑centered self‑care program on the health literacy level and self‑efficacy of patients with acute coronary syndrome during discharge from hospital. Iran J Nurs Midwifery Res. 2023;28(5). doi:10.4103/ijnmr.ijnmr_356_21
41. Elzyen E, Abd Elsalam E, Ibrahim E, Amer H. Effect of motivation based nursing intervention on physical activity and cardiac self-efficacy among patients with coronary heart diseases. Menoufia Nurs J. 2023;8(1):113–131. doi:10.21608/menj.2023.289272
42. Zhang P, Xing FM, Li CZ, Wang FL, Zhang XL. Effects of a nurse-led transitional care programme on readmission, self-efficacy to implement health-promoting behaviours, functional status and life quality among Chinese patients with coronary artery disease: a randomised controlled trial. J Clin Nurs. 2018;27(5–6):969–979. doi:10.1111/jocn.14064
43. Boroumand S, Moeini M. The effect of a text message and telephone follow-up program on cardiac self-efficacy of patients with coronary artery disease: a randomized controlled trial. Iran J Nurs Midwifery Res. 2016;21(2):171–176. doi:10.4103/1735-9066.178243
44. Ahmadi Z, Abolhassani S, Hasheminia A, Kheiri S. The effects of a multimedia education on self-efficacy and self-esteem among patients with acute coronary syndrome: a clinical randomized trial. Iran J Nurs Midwifery Res. 2022;27(3):181–187. doi:10.4103/ijnmr.IJNMR_92_20
45. Pitta NC, Furuya RK, Freitas NDO, et al. Effect of an educational program on physical activity in individuals undergoing their first percutaneous coronary intervention: a randomized clinical trial. Braz J Phys Ther. 2022;26(5). doi:10.1016/j.bjpt.2022.100443
46. Nikraftar F, Heshmati Nabavi F, Dastani M, Mazlom SR, Mirhosseini S. Acceptability, feasibility, and effectiveness of smartphone-based delivery of written educational materials in Iranian patients with coronary artery disease: a randomized control trial study. Health Sci Rep. 2022;5(5):1.
47. Yazdanparast E, Davoudi M, Safavinejad M, Ghorbani SH, Nadimi S, Dehaghani BR. Effect of teach back learning strategy on illness perception, nutritional knowledge and dietary adherence in people with hypertension. Cardiovasc Nurs J. 2018;7(3):1.
48. Hasanica N, Ramic-Catak A, Mujezinovic A, Begagic S, Galijasevic K, Oruc M. The effectiveness of leaflets and posters as a health education method. Mater Sociomed. 2020;32(2):135–139. doi:10.5455/msm.2020.32.135-139
49. Salimi NT, Ezbarami ZT, Tabari-Khomeiran R, Roushan ZA, Hashemian H, Astaneh HK. Comparing the effects of mobile-based education and booklet-based education on iranian mothers’ perception on antibiotics: a Quasi-Experimental Study. J Pediatr Nurs. 2021;61:122–129. doi:10.1016/j.pedn.2021.04.034
50. Sun L, Hu J, Gao H, et al. Long-term effect of mobile phone-based education and influencing factors of willingness to receive HPV vaccination among female freshmen in Shanxi Province, China. Hum Vaccin Immunother. 2022;18(5):2051990. doi:10.1080/21645515.2022.2051990
51. Lee M, Lee H, Kim Y, et al. Mobile app-based health promotion programs: a systematic review of the literature. Int J Environ Res Public Health. 2018;15(12). doi:10.3390/ijerph15122838
52. Tsiamparlis-Wildeboer AHC, Feijen-De Jong EI, Scheele F. Factors influencing patient education in shared medical appointments: integrative literature review. Patient Educ Couns. 2020;103(9):1667–1676. doi:10.1016/j.pec.2020.03.006
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Self-Efficacy in Self-Care and Its Related Factors Among Patients with Coronary Heart Disease in Indonesia: A Rasch Analysis
Nuraeni A, Sugiharto F, Anna A, Sari E, Mirwanti R, Trisyani Y, Emaliyawati E
Vascular Health and Risk Management 2023, 19:583-593
Published Date: 5 September 2023
A Scoping Review of Predictors Associated with Self-Efficacy Among Patients with Coronary Heart Disease
Sugiharto F, Nuraeni A, Trisyani Y, Putri AM, Armansyah NA, Zamroni AH
Vascular Health and Risk Management 2023, 19:719-731
Published Date: 9 November 2023
5G Bedside Interactive Terminal Health Education to Enhance Treatment Adherence in Elderly Patients with Chronic Diseases: The Mediating Role of Self-Efficacy
Zhang S, Ruan X
Patient Preference and Adherence 2026, 20:596556
Published Date: 23 April 2026
Social Support and Hospital Discharge Readiness in CHD Patients: Mediating Roles of Self-Efficacy and Adherence
Wang D, Yang N, Wei C, Wang J, Yuan L, Sun R
Patient Preference and Adherence 2026, 20:601646
Published Date: 4 June 2026