Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Health Cadre Mentoring Model in Stunting Prevention Programs: A Systematic Literature Review
Authors Husnida N ![]() , Rahmatina AN
, Rahmatina AN ![]() , Wiwaha G, Adnani QES
, Wiwaha G, Adnani QES ![]() , Hilmanto D
, Hilmanto D
Received 7 January 2026
Accepted for publication 7 May 2026
Published 22 May 2026 Volume 2026:19 594400
DOI https://doi.org/10.2147/JMDH.S594400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David C. Mohr
Nintinjri Husnida,1,2 Arina Nursafrina Rahmatina,3 Guswan Wiwaha,4 Qorinah Estiningtyas Sakilah Adnani,4 Dany Hilmanto5
1Doctoral Program in Medical Sciences, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Midwifery, Poltekkes Kemenkes Banten, Serang, Banten, Indonesia; 3Master of Midwifery Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 5Department of Pediatrics, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Dany Hilmanto, Department of Pediatrics, Faculty of Medicine, Universitas Padjadjaran, Jl. Eyckman No. 38, Bandung, West Java, 40161, Indonesia, Email [email protected]
Aim: Stunting remains a major public health problem in low- and middle-income countries, including Indonesia, with long-term consequences for physical growth, cognitive development, and adult productivity. Health cadres (community health workers/CHWs) play a crucial role in community-based stunting prevention; however, evidence regarding effective mentoring models remains fragmented.
Purpose: This review aims to synthesize evidence on health cadre mentoring models in stunting prevention, with particular attention to behavioral change components and their theoretical underpinnings.
Patients and Methods: A systematic literature review was conducted following PRISMA 2020 guidelines. Articles published between 2014 and 2025 were retrieved from five databases: PubMed, ScienceDirect, Google Scholar, SpringerLink, and Scopus. A total of 1475 records were identified, with 1310 articles remaining after duplicate removal. After title and abstract screening, 99 full-text articles were assessed for eligibility, and 52 studies were included. Methodological quality was appraised using the Joanna Briggs Institute (JBI) tools. Data were analyzed using a thematic (narrative) synthesis and mapped to behavior change theories.
Results: The 52 included studies describe diverse mentoring models, including structured training, interpersonal communication, participatory approaches, growth monitoring, quality improvement, and digital platforms. These interventions were associated with improvements in cadre knowledge, skills, and engagement, and with changes in family health behaviors. Evidence regarding impacts on child growth and stunting outcomes was mixed and context-dependent. Key enabling factors included continuous supervision, cultural adaptation, and multisectoral collaboration, while challenges related to sustainability and resource constraints were frequently reported.
Conclusion: Health cadre mentoring models show potential to strengthen cadre capacity and support behavior change for stunting prevention. However, the effectiveness of these interventions varies across contexts and implementation characteristics, and evidence on long-term impacts on child nutritional status remains limited. Further research is needed to develop sustainable, context-specific, and system-integrated mentoring approaches.
Keywords: stunting, health cadres, mentoring models, behavior change
Introduction
Stunting remains an urgent public health issue in Indonesia, particularly during the first 1000 days of life (from conception to a child’s second birthday). This condition is characterized by impaired physical growth in children (height below the age-standard) and has long-term impacts on cognitive development, metabolic health, and productivity in adulthood.1–3 Globally, approximately 22% of children under five years old experience stunting, equivalent to more than 149 million children.4,5 The prevalence of stunting in Indonesia has declined from 24.4% in 2021 to 21.5% in 2023; however, this remains above the WHO threshold (<20%) and national targets.6,7
Various efforts have been implemented to address stunting, including nutrition supplementation, breastfeeding promotion, and community-based interventions. One key strategy is a family-based approach involving health cadres (community health workers/CHWs), who provide mentoring to families at risk of stunting across the life cycle. Cadres play a central role due to their close social relationships with the community.8–11 The effectiveness of cadres in performing their roles is strongly influenced by the mentoring models applied. Well-designed mentoring can enhance cadre competencies, strengthen motivation, and improve program continuity and community acceptance.12,13
In this review, mentoring models are defined as structured approaches that include training, supervision, feedback mechanisms, and community-based interactions such as home visits and participatory activities. Previous studies have highlighted the importance of continuous support for cadres, including training, supervision, and appropriate educational tools, in improving child feeding practices and service delivery.14 However, these studies are often fragmented and context-specific. Although the role of health cadres in stunting prevention is well recognized, there remains a lack of systematic evidence comparing different mentoring models. Most existing studies are descriptive and focus on local program implementation, without providing comprehensive analysis of mentoring structures, key components, and their relative effectiveness across settings.
Furthermore, the literature synthesizing essential elements of mentoring models such as training approaches, supervision mechanisms, communication strategies, and sustainability remains limited. This gap hinders the development of scalable and evidence-based mentoring frameworks.
Therefore, a systematic literature review (SLR) is needed to identify, evaluate, and synthesize health cadre mentoring models in stunting prevention programs. This review aims to provide a comprehensive understanding of existing approaches, highlight their strengths and limitations, and inform the development of more effective, adaptive, and sustainable interventions.
Based on this rationale, the present review addresses the following research questions:
- What types of cadre mentoring interventions have been implemented to prevent stunting?
- What behavioral change components (knowledge, skills, attitudes, motivation, advocacy, and communication) are addressed in these interventions?
- How do these interventions align with behavior change theories in influencing family practices such as exclusive breastfeeding, complementary feeding, and health service utilization?
This review further maps intervention components to behavior change constructs (knowledge, skills, attitudes, motivation, communication, and advocacy) using established theories, including the Theory of Planned Behavior, Social Cognitive Theory, and the Health Belief Model, to better understand the mechanisms underlying mentoring effectiveness.
Materials and Methods
Study Design
This study is a systematic literature review conducted in accordance with the PRISMA 2020 guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).15 The review aims to identify, evaluate, and synthesize current evidence on health cadre mentoring models in stunting prevention programs.
Eligibility Criteria
The research questions were formulated using the PICCO framework (Population, Intervention, Context, Comparison, and Outcome). The detailed PICCO components, along with the inclusion and exclusion criteria, are presented in Table 1.
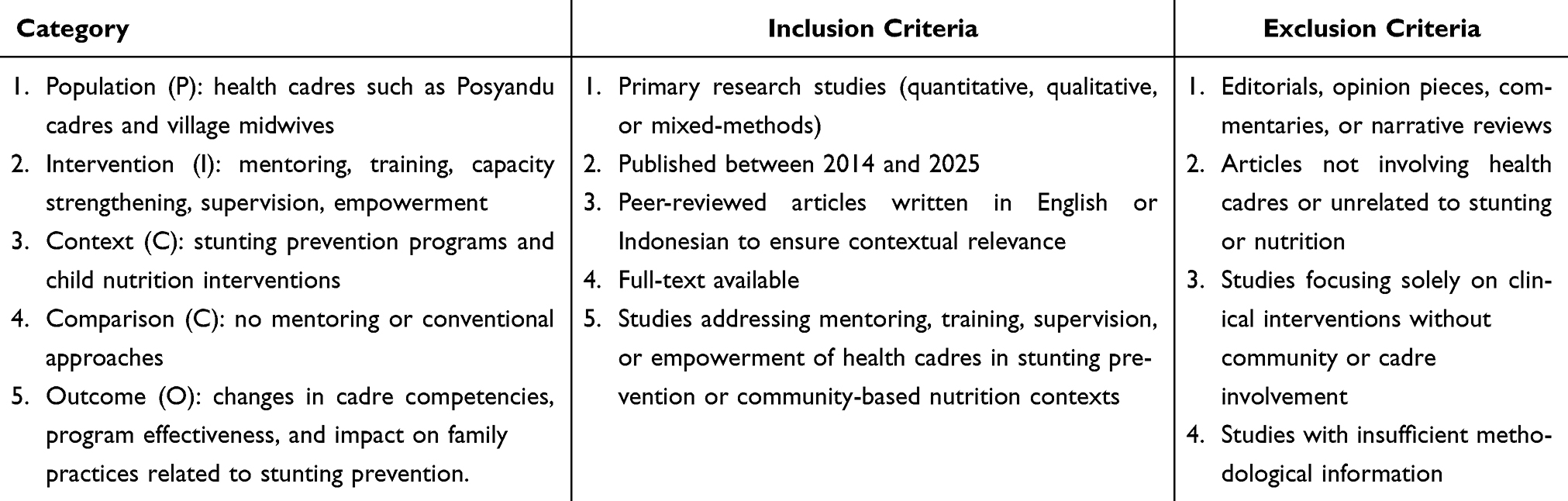 |
Table 1 The PICCO Framework, Inclussion and Exclussion Criteria |
Selection Process
A systematic search was conducted across five electronic databases: PubMed, Scopus, ScienceDirect, SpringerLink, and Google Scholar. The search covered publications from 2014 to 2025. The search strategy combined keywords and MeSH terms related to stunting, community health workers, and mentoring. An example of the search string used was: (“stunting” OR “child malnutrition”) AND (“health cadres” OR “community health workers”) AND (“mentoring” OR “training” OR “capacity building”). The search strategy was adapted for each database. In addition to database searching, supplementary searches were conducted through manual searching and snowballing of reference lists from relevant articles.
All retrieved records were exported and screened using Rayyan web-based systematic review software (Rayyan QCRI) to facilitate blinded screening. Title and abstract screening, followed by full-text assessment, were conducted independently by two reviewers. Discrepancies between reviewers were resolved through discussion and consensus. The study selection process is presented in a PRISMA 2020 flow diagram.
Quality Appraisal and Risk of Bias Management
The results of this process were presented in a PRISMA 2020 flow diagram (Figure 1). The methodological quality of the included studies was assessed using the JBI Critical Appraisal Tools, with adjustments made according to each study design (quantitative, qualitative, or mixed-methods). This appraisal ensured that only studies with sufficient methodological rigor were considered reliable for inclusion in the synthesis. No studies were excluded solely based on quality assessment; instead, studies were categorized according to their methodological quality and this was taken into account during data interpretation to maintain the validity and credibility of the review findings.16 Data from the selected studies were systematically extracted, including authors, year, study location, research design, participant characteristics, type of intervention, and main outcomes. Data analysis was conducted using a thematic synthesis approach, allowing grouping of data according to key themes such as mentoring forms, training media, the role of cadres in stunting prevention, and the intervention’s impact on child nutritional status.17 Visualization of the synthesis results could include thematic tables, inter-theme relationship matrices, or word clouds using software such as NVivo.18
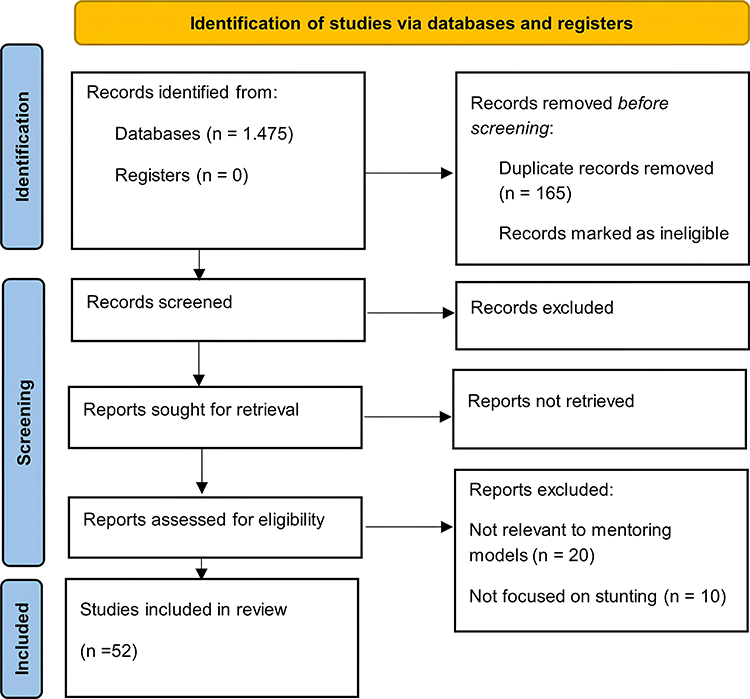 |
Figure 1 Prisma Flow Diagram. |
In addition to thematic grouping, the extracted findings were further mapped onto established behavior change theories to analyze how mentoring interventions address components such as knowledge, skills, attitudes, motivation, advocacy, and communication. Theoretical lenses applied in this review included the Theory of Planned Behavior (Ajzen, 1991), Social Cognitive Theory (Bandura, 1986), and the Health Belief Model (Rosenstock, 1974). This step enabled a structured interpretation of the behavioral mechanisms underlying cadre mentoring models, ensuring that the synthesis not only describes interventions but also explains how they align with behavior change frameworks.
In addition to presenting a data synthesis, this review also identifies research gaps, such as the absence of mentoring models specifically designed for rural communities with limited resources, and the lack of longitudinal studies measuring the sustained impact of interventions. The theoretical contribution of this review lies in expanding the understanding of evidence-based cadre capacity-building models, while its practical contribution provides recommendations for policies aimed at improving cadre quality to support stunting prevention programs at the community level.
To reduce bias, we adopted several strategies: (1) using two independent reviewers for screening, data extraction, and coding; (2) applying the JBI appraisal tools and recording study quality within the synthesis; (3) conducting sensitivity analyses by excluding low-quality studies to test the robustness of the findings; (4) triangulating evidence across multiple outcomes (knowledge, practice, anthropometry) rather than relying on single indicators; and (5) explicitly addressing potential language and publication bias in the limitations section.
Results
A total of 52 studies were included in this review. The characteristics of the included studies are summarized in Table 2. The studies were identified from multiple electronic databases, including PubMed, ScienceDirect, and Google Scholar, the latter of which enabled the inclusion of relevant Indonesian-language studies indexed in SINTA. Articles indexed in SINTA are provided in Table S1. The studies were conducted across various low and middle-income countries and employed diverse designs, including quasi-experimental, randomized controlled trials, qualitative, and mixed-methods approaches. The study populations primarily involved health cadres or community health workers, as well as target groups such as pregnant women and mothers of young children.
 |
Table 2 Characteristics Study |
The interventions identified were heterogeneous, encompassing training, home visits, group education, and digital-based approaches, with durations ranging from single-session activities to long-term programs. Most studies implemented structured training interventions, often combined with home visits or supportive supervision. The outcomes assessed across studies included improvements in cadre capacity, maternal health practices, and child nutritional status. The majority of studies reported improvements in cadre knowledge, skills, and engagement, while only a smaller proportion reported direct effects on child nutritional outcomes such as stunting reduction or anthropometric improvements.
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools, with the results presented in Table 3. Overall, most studies were classified as moderate quality, while a substantial proportion achieved high quality. Randomized controlled trials generally demonstrated higher methodological rigor, whereas quasi-experimental and descriptive studies tended to show moderate quality due to limitations such as the absence of control groups, shorter intervention duration, and incomplete reporting of follow-up or attrition. No studies were excluded based on quality assessment, as all met the minimum inclusion criteria.
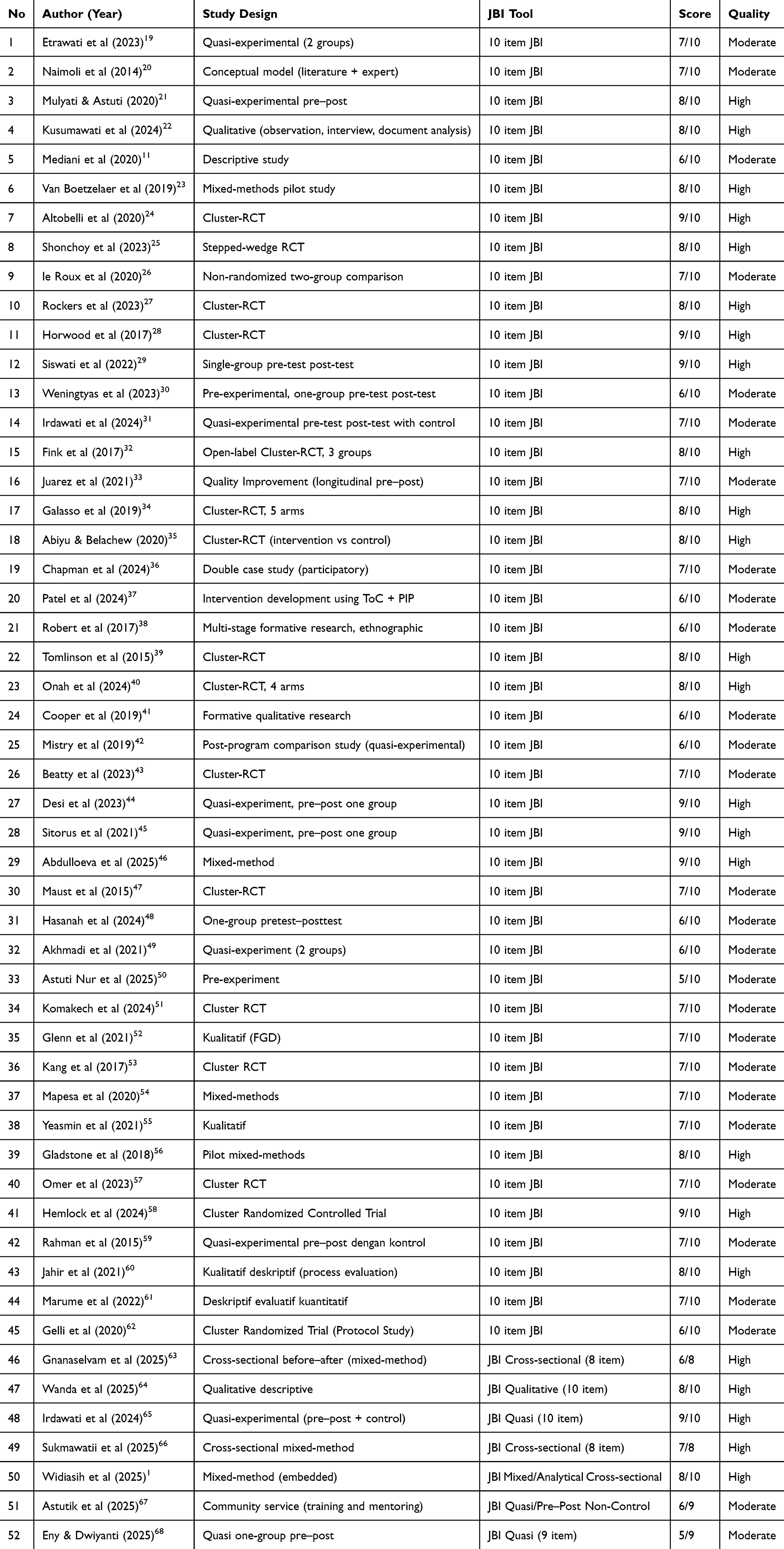 |
Table 3 Quality Assessment of Included Studies (JBI) |
The findings were further synthesized using a thematic approach to identify key patterns in mentoring interventions for stunting prevention. This synthesis generated five major themes: forms of mentoring, training media, duration of intervention, roles of health cadres, and impact on outcomes. The summary of this thematic synthesis is presented in Table 4. Interventions that incorporated participatory approaches and continuous supervision were more frequently associated with positive outcomes compared to short-term or one-time interventions.
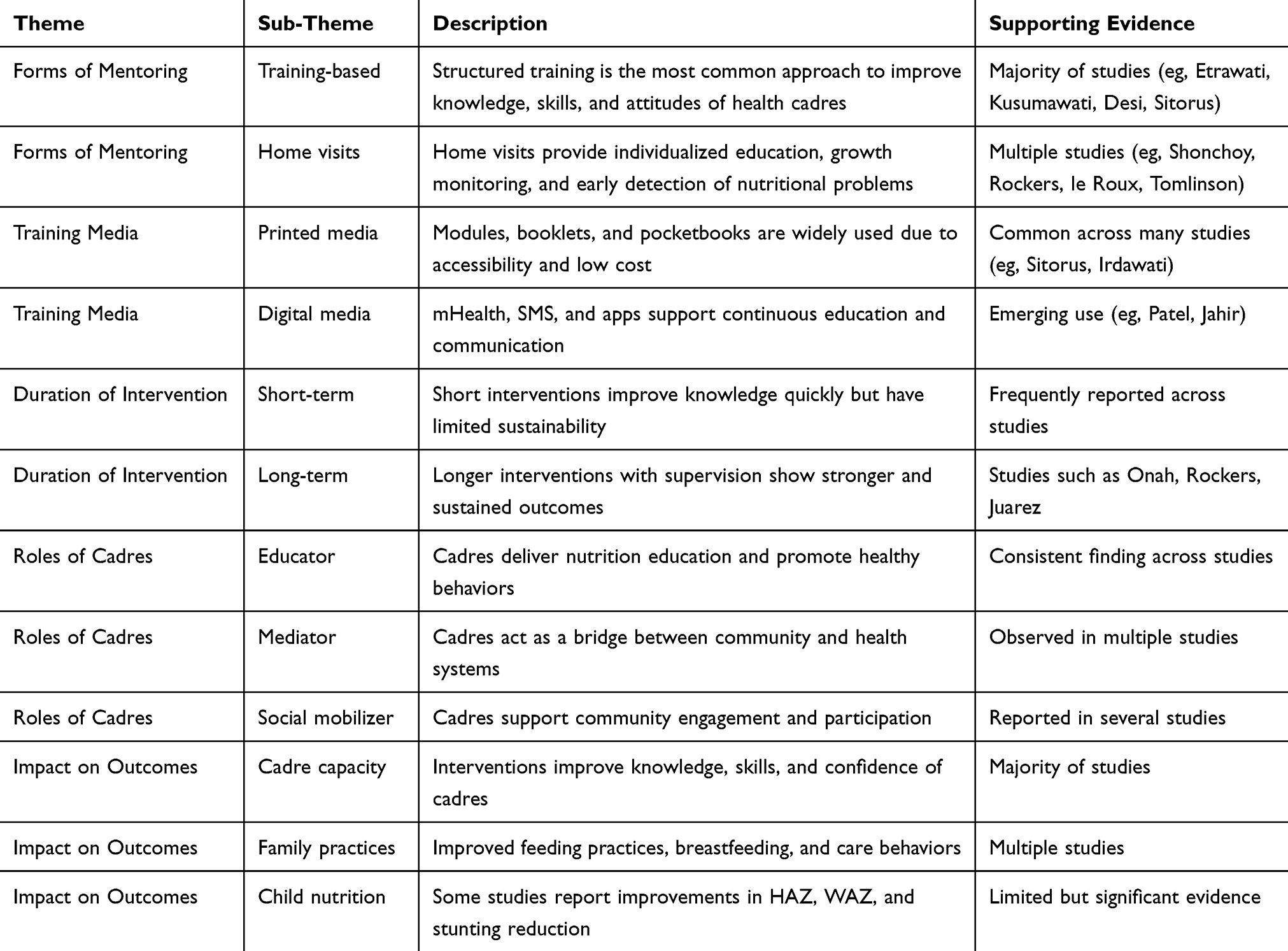 |
Table 4 Thematic Synthesis of Findings |
Importantly, the identified themes also highlight the influence of social and cultural contexts in shaping the implementation and effectiveness of mentoring interventions. Variations in community engagement, local beliefs, and resource availability were found to affect how mentoring strategies were delivered and adopted, indicating the need for a context-sensitive mentoring model for stunting prevention. Several studies reported that culturally adapted and community-based approaches were associated with better acceptance and sustainability of interventions.
Discussion
The findings of this review indicate that mentoring interventions for health cadres generally show positive effects on cadre capacity and family-level practices. Most of the included studies reported improvements in cadre knowledge, skills, and engagement, indicating consistent positive effects at the individual level. However, the results across studies are mixed and context dependent, particularly when considering variations in study design, intervention characteristics, and outcome measures.
Most studies consistently reported improvements in cadres’ knowledge, skills, and engagement following training and mentoring interventions. Training and home visits appear to play complementary roles, where training provides foundational competencies and home visits facilitate practical application and closer interaction with families. A substantial number of studies implemented structured training, often combined with supervision or home visits, suggesting that multi-component interventions are more effective. Nevertheless, the effectiveness of these approaches is influenced by how they are implemented. Participatory1,67 and experience-based methods24 tend to produce better engagement and learning outcomes compared to one-way instructional approaches.
Despite these positive findings, not all studies demonstrated significant effects, particularly on child nutritional outcomes. Only a smaller proportion of studies reported measurable improvements in child nutritional outcomes, such as stunting reduction or anthropometric indicators. Some large-scale or multisectoral interventions reported no significant impact on stunting reduction, suggesting that improvements in cadre capacity do not always directly translate into measurable child health outcomes. In addition, several studies indicated that the effectiveness of interventions depends on contextual factors, such as the consistency of home visits46,63,64,66 and duration of the program. For example, interventions were more effective when implemented continuously and supported by regular supervision, while short-term or less intensive programs showed more limited and less sustainable effects. Furthermore, we found that the majority of mentoring programs were short-term, lasting less than six months. Some were even conducted in a single training session without adequate follow-up, as shown in the studies by Mediani et al and Etrawati et al.11,19 Only a small number of studies have medium- to long-term interventions (≥6 months), carried out in a phased and sustained manner, such as those by Onah et al, Rockers et al, and Juarez et al.27,40
This discrepancy may be explained by the imbalance in intervention focus. Most mentoring programs primarily targeted knowledge and skill development, while fewer interventions explicitly addressed behavioral determinants such as motivation, social norms, and environmental constraints. When mapped to behavior change theories, most interventions aligned with constructs from the Social Cognitive Theory and Theory of Planned Behavior, particularly in improving knowledge and self-efficacy, while components of the Health Belief Model were less frequently addressed.
This review also highlights differences in outcomes across levels. While improvements in intermediate outcomes, such as cadre knowledge and family practices, were frequently observed, evidence on long-term outcomes, including child nutritional status, remains limited and inconsistent. This suggests that strengthening cadre capacity alone may not be sufficient without broader system support and sustained implementation.
Variations in findings may also be influenced by differences in study design and methodological quality. Studies with more rigorous designs, such as randomized controlled trials25,27,28,32,34,35,39,40,43,47,51,53,57,58,69 tended to provide more robust evidence, whereas studies with simpler designs often reported improvements primarily in short-term or self-reported outcomes. This underscores the importance of interpreting the findings cautiously in light of the overall quality of evidence.
In addition, contextual and cultural factors play an important role in determining intervention effectiveness. Most mentoring models identified in this review were relatively generic and not specifically tailored to local cultural contexts, which may limit their relevance and long-term sustainability. Several studies highlighted the importance of culturally adapted and community-based approaches in improving intervention acceptance and sustainability.49,66 Interventions that incorporated culturally adapted approaches and community engagement strategies tended to show more meaningful and contextually appropriate outcomes.
Limitation
This review has several limitations. The heterogeneity of study designs, intervention types, and outcome measures precluded a quantitative synthesis. In addition, many studies focused on short-term outcomes, with limited evidence on long-term impacts. Although this review included studies published in both English and Indonesian, differences in language and database indexing may still introduce potential bias.
Conclusion
This systematic literature review synthesizes evidence from 52 studies on health cadre mentoring models for stunting prevention. The findings indicate that most mentoring interventions are effective in improving cadre knowledge, skills, and engagement; however, only a smaller proportion of studies demonstrate direct effects on child nutritional outcomes. Mentoring approaches that combine structured training, supervision, and community-based activities appear to be more effective, particularly when implemented continuously rather than as short-term interventions. Participatory and culturally adapted approaches were also associated with better acceptance and sustainability of interventions.
Despite these positive findings, the limited impact on child nutritional outcomes suggests that strengthening cadre capacity alone may not be sufficient. Future interventions should integrate behavior change theory more explicitly and address broader determinants such as motivation, social norms, and environmental factors to achieve sustained improvements. Overall, health cadre mentoring models have strong potential to support stunting prevention programs; however, their effectiveness depends on implementation quality, contextual adaptation, and long-term system support. Further research is needed to develop and evaluate sustainable, context-sensitive, and theory-informed mentoring models.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). The first author is supported by a doctoral scholarship from the Ministry of Health, Republic of Indonesia, with grant number HK.02.03/F/2582/2024, which enables her to continue her doctoral studies at the Faculty of Medicine, Universitas Padjadjaran.
Disclosure
The authors declare that there are no conflicts of interest in the writing or publishing of this article.
References
1. Widiasih R, Sunjaya DK, Rahayuwati L, et al. Evaluating the knowledge, roles, and skills of health cadres in stunting prevention: a mixed-method study in Indonesia. Belitung Nurs J. 2025;11(3):330–18. doi:10.33546/bnj.3722
2. UNICEF, WHO, World Bank. Levels and trends in child malnutrition [Internet]; 2021. Available from: https://www.who.int/publications/i/item/9789240025257.
3. Dhar U, Asian Development Bank. Asian development outlook 2020: what drives innovation in Asia? [Internet]. New Delhi: Asian Development Bank; 2020:145. Available from: https://www.adb.org/sites/default/files/publication/575626/ado2020.pdf.
4. Unidas N, Nations U. On the road to the second world summit for social development: contributions from the regional commissions [Internet]; 2025. Available from: https://bit.ly/m/CEPAL.
5. Putri MM, Mardiah W, Yulianita H, Keperawatan F. Gambaran pengetahuan ibu balita tentang stunting. J Nurs Care. 2021;4(2):122–129.
6. Kementerian Kesehatan RI. The 2023 Indonesian Health Survey (SKI) in Figures [Internet]; 2023. Available from: https://www.badankebijakan.kemkes.go.id/ski-2023-dalam-angka/.
7. Head of the Health Development Policy Agency, Asnawi Abdullah P, JAWAB Plt Kepala Pusat Kebijakan Upaya Kesehatan Dwi Puspasari PIwan Ariawan K, Razak Thaha A, Lipoeto NI, et al. SSGI 2024 in Numbers [Internet]; 2024. Available from: https://kesprimkom.kemkes.go.id/assets/uploads/contents/others/SSGI_DALAM_ANGKA_LAUNCHING_250526_signed.pdf.
8. Septiani B, Ardiansyah L. Development of protein-rich canavalia biscuit from koro sword bean base on acceptance and nutritional content as additional food for pregnant women for stunting prevention. Amerta Nutr. 2024;8(3):335–343. doi:10.20473/amnt.v8i3.2024.335-343
9. O’Brien K, Robson K, Bracht M, et al. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial. Lancet Child Adolesc Health. 2018;2(4):245–254. PubMed PMID: 30169298. doi:10.1016/S2352-4642(18)30039-7
10. Damanik MRM. Policies and Strategies to Accelerate Stunting Reduction in Indonesia. Jakarta: BKKBN; 2021.
11. Mediani HS, Nurhidayah I, Lukman M. Empowerment of health cadres regarding stunting prevention in toddlers. Media Karya Kesehatan. 2020;3(1):82–90. doi:10.24198/mkk.v3i1.26415
12. Perry H, Morrow M, Borger S, et al. Care groups I: an innovative community-based strategy for improving maternal, neonatal, and child health in resource-constrained settings. Global Health Sci Pract. 2015;3(3):358–369.
13. Qar Bhutta ZA, Ahmed T, Black RE, et al. Maternal and child undernutrition 3 what works? Intervent Mater Child Undernutr Surv. 2008;371(9610). doi:10.1016/S0140-6736(07)61693-6
14. Lassi ZS, Das JK, Zahid G, Imdad A, Bhutta ZA. Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: a systematic review. BMC Public Health. 2013:1–10. PubMed PMID: 24564534. doi:10.1186/1471-2458-13-S3-S13
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021. PubMed PMID: 33780438. doi:10.1136/bmj.n71
16. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan ZE. JBI manual for evidence synthesis. JBI; 2024.
17. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1). PubMed PMID: 18616818. doi:10.1186/1471-2288-8-45
18. Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J Eval Clin Pract. 2018;24(3):459–467. doi:10.1111/jep.12884
19. Etrawati F, Lionita W, Amalia E, Rahmawati F, Meilinda N, Rahmawaty A. Improving the knowledge of health cadres for stunting prevention through emotional demonstration technique. Indonesian J Hum Nutr. 2023;10(2):116–123. doi:10.21776/ub.ijhn.2023.010.02.3
20. Naimoli JF, Frymus DE, Wuliji T, Franco LM, Newsome MH. A Community Health Worker “logic model”: towards a theory of enhanced performance in low- and middle-income countries. Hum Resour Health. 2014;12(1). PubMed PMID: 25278012. doi:10.1186/1478-4491-12-56
21. Mulyanti S, Astuti AB. Efforts to reduce the risk of stunting through an Interprofessional Collaboration approach (IPC). Jurnal Keperawatan Global; 2020.
22. Kusumawati PD, Suhita BM, Khasanah M, Mendieta G, Ambarsari F, Sucipto A. Increasing the capacity of health cadres in order to optimize primary service integration activities in Ternyang villages. Jurnal Locus Penelitian Dan Pengabdian. 2024;3(12):1011–1017. doi:10.58344/locus.v3i12.3472
23. Van Boetzelaer E, Zhou A, Tesfai C, Kozuki N. Performance of low-literate community health workers treating severe acute malnutrition in South Sudan. Matern Child Nutr. 2019;15(S1):1–9. PubMed PMID: 30748111. doi:10.1111/mcn.12716
24. Altobelli LC, Cabrejos-Pita J, Mary Penny SB. A cluster-randomized trial to test sharing histories as a training method for community health workers in Peru. Glob Health Sci Pract. 2020;9(2):422–424. PubMed PMID: 34234028. doi:10.9745/GHSP-D-21-00178
25. Shonchoy AS, Akram AA, Khan M, et al. A community health worker-based intervention on anthropometric outcomes of children aged 3 to 21 months in Urban Pakistan, 2019–2021. Am J Public Health. 2023;113(1):105–114. PubMed PMID: 36516383. doi:10.2105/AJPH.2022.307111
26. Le Roux KW, Almirol E, Rezvan PH, et al. Community health workers impact on maternal and child health outcomes in rural South Africa - a non-randomized two-group comparison study. BMC Public Health. 2020;20(1):1–14. PubMed PMID: 32943043. doi:10.1186/s12889-020-09468-w
27. Rockers PC, Leppänen JM, Tarullo A, et al. Evaluation of a community health worker home visit intervention to improve child development in South Africa: a cluster-randomized controlled trial. PLoS Med. 2023;20(4):e1004222. PubMed PMID: 37058529. doi:10.1371/journal.pmed.1004222
28. Horwood C, Butler L, Barker P, et al. A continuous quality improvement intervention to improve the effectiveness of community health workers providing care to mothers and children: a cluster randomised controlled trial in South Africa. Hum Resour Health. 2017;15(1). PubMed PMID: 28610590. doi:10.1186/s12960-017-0210-7
29. Siswati T, Iskandar S, Pramestuti N, et al. Effect of a short course on improving the cadres’ knowledge in the context of reducing stunting through home visits in Yogyakarta, Indonesia. Int J Environ Res Public Health. 2022;19(16):1–10. PubMed PMID: 36011477. doi:10.3390/ijerph19169843
30. Weningtyas A, Ma’rufa PL, Fauziah D. the effect of short course interventions to improve knowledge of posyandu (Integrated Service Post) cadres in early detection of stunting. Indonesian J Public Health. 2023;18(3):530–539. doi:10.20473/ijph.v18i3.2023.530-539
31. Irdawati I, Arifah S, Muhlisin A, et al. Efforts of increase cadre capacity about stunting prevention. MethodsX. 2024;13:1–6. doi:10.1016/j.mex.2024.102720
32. Fink G, Levenson R, Tembo S, Rockers PC. Home-and community-based growth monitoring to reduce early life growth faltering: an open-label, cluster-randomized controlled trial. Am J Clin Nutr. 2017;106(4):1070–1077. doi:10.3945/ajcn.117.157545
33. Juarez M, Dionicio C, Sacuj N, Lopez W, Miller AC, Rohloff P. Community-based interventions to reduce child stunting in rural guatemala: a quality improvement model. Int J Environ Res Public Health. 2021;18(2):773. doi:10.3390/ijerph18020773
34. Galasso E, Weber AM, Stewart CP, Ratsifandrihamanana L, Fernald LCH. Effects of nutritional supplementation and home visiting on growth and development in young children in Madagascar: a cluster-randomised controlled trial. Lancet Glob Health. 2019;7(9):e1257–e1268. PubMed PMID: 31402006. doi:10.1016/S2214-109X(19)30317-1
35. Abiyu C, Belachew T, Adu-Afarwuah S. Effect of complementary feeding behavior change communication delivered through community-level actors on dietary adequacy of infants in rural communities of West Gojjam Zone, Northwest Ethiopia: a cluster-randomized controlled trial. PLoS One. 2020;15(9):e0238355. PubMed PMID: 32881945. doi:10.1371/journal.pone.0238355
36. Chapman AJ, Ebido CC, Tening RN, et al. Creating culturally-informed protocols for a stunting intervention using a situated values-based approach (WeValue InSitu): a double case study in Indonesia and Senegal. BMC Public Health. 2024;24(1):1–18. PubMed PMID: 38589810. doi:10.1186/s12889-024-18485-y
37. Patel AB, Kuhite PN, Khan SS, Puranik A, Alam A, Dibley MJ. M-SAKHI - Mobile health solutions to help community providers promote maternal and infant nutrition and health: a description of development of the Program Impact Pathway using Theory of Change. Public Health Nutr. 2024;27(1):1–10. PubMed PMID: 39436271. doi:10.1017/S1368980024001265
38. Robert RC, Creed-Kanashiro HM, Villasante R, Narro MR, Penny ME. Strengthening health services to deliver nutrition education to promote complementary feeding and healthy growth of infants and young children: formative research for a successful intervention in peri-urban Trujillo, Peru. Matern Child Nutr. 2017;13(2):1–15. PubMed PMID: 26931182. doi:10.1111/mcn.12264
39. Tomlinson M, Rotheram-Borus MJ, Harwood J, le Roux IM, O’Connor M, Worthman C. Community health workers can improve child growth of antenatally-depressed, South African mothers: a cluster randomized controlled trial. BMC Psychiatry. 2015;15(1). PubMed PMID: 26400691. doi:10.1186/s12888-015-0606-7
40. Onah MN, Khan GN, Kureishy S, et al. The cost-effectiveness of a cash-based transfer, specialised nutritious food, and social and behaviour change communication intervention package to prevent undernutrition among children 6–23 months in Pakistan: a cluster randomised controlled trial. J Glob Health. 2024;14. PubMed PMID: 39575728. doi: 10.7189/JOGH.14.04186
41. Cooper CM, Kavle JA, Nyoni J, et al. Perspectives on maternal, infant, and young child nutrition and family planning: considerations for rollout of integrated services in Mara and Kagera, Tanzania. Matern Child Nutr. 2019;15(S1):1–12. PubMed PMID: 30748120. doi:10.1111/mcn.12735
42. Mistry SK, Hossain MB, Arora A. Maternal nutrition counselling is associated with reduced stunting prevalence and improved feeding practices in early childhood: a post-program comparison study. Nutr J. 2019;18(1):1–9. PubMed PMID: 31455363. doi:10.1186/s12937-019-0473-z
43. Beatty A, Borkum E, Leith W, Null C, Suriastini W. A cluster randomized controlled trial of a community-based initiative to reduce stunting in rural Indonesia. Matern Child Nutr. 2024;20(1). PubMed PMID: 38041533. doi:10.1111/mcn.13593
44. Desi, Rafiony A, Hariyadi D, Nopriantini N, Petrika Y, Yulianingsih K. Empowerment model of integrated health post (Posyandu) cadres in controlling stunting in children aged 0–24 months through anthropometric measurement training. Gema Kesehatan. 2023;15(2):120–129. doi:10.47539/gk.v15i2.426
45. Sitorus SBM, Parwata NMRN, Noya F. The influence of mentoring on the knowledge and skills of Posyandu cadres in early detection of stunting. Poltekita. 2021;15(3):283–287. doi:10.33860/jik.v15i3.459
46. Abdulloeva S, Bhanot A, Khan MA, et al. Centering community-based maternal and child nutrition services in Bangladesh’s rural primary healthcare: what has potential to scale. Front Public Health. 2025;13. PubMed PMID: 39944067. doi: 10.3389/fpubh.2025.1464792
47. Maust A, Koroma AS, Abla C, et al. Severe and moderate acutemalnutrition can be successfully managed with an integrated protocol in Sierra Leone. J Nutr. 2015;145(11):2604–2609. PubMed PMID: 26423737. doi:10.3945/jn.115.214957
48. Hasanah Z, Gesang Kinanti R, Candra Puriastuti A, Puspita Ratna A, Putri Novembriani R. Improving knowledge of community health worker about stunting’s prevention through structured training program in Malang. Global Health Sci Group. 2024;5(2):759–766.
49. Akhmadi A, Sunartini S, Haryanti F, Madyaningrum E, Sitaresmi MN. Effect of care for child development training on cadres’ knowledge, attitude, and efficacy in Yogyakarta, Indonesia. Belitung Nurs J. 2021;7(4):311–319. doi:10.33546/bnj.1521
50. Nur A, Da Costa SLDV, Pantaleon MG, Nita MHD, Adi AAAM. Effectiveness of nutrition training in improving cadres’ knowledge and skills in Kupang City. Action Aceh Nutr J. 2025;10(1):77. doi:10.30867/action.v10i1.2165
51. Komakech JJ, Emerson SR, Cole KL, et al. Care groups in an integrated nutrition education intervention improved infant growth among South Sudanese refugees in Uganda’s West Nile post-emergency settlements: a cluster randomized trial. PLoS One. 2024;19(3):e0300334. PubMed PMID: 38489346. doi:10.1371/journal.pone.0300334
52. Glenn J, Moucheraud C, Payán DD, et al. What is the impact of removing performance-based financial incentives on community health worker motivation? A qualitative study from an infant and young child feeding program in Bangladesh. BMC Health Serv Res. 2021;21(1):1–11. PubMed PMID: 34535147. doi:10.1186/s12913-021-06996-y
53. Kang Y, Kim S, Sinamo S, Christian P. Effectiveness of a community-based nutrition programme to improve child growth in rural Ethiopia: a cluster randomized trial. Matern Child Nutr. 2017;13(1). doi:10.1111/mcn.12349
54. Mapesa J, Meme J, Muthamia O. Effect of community-based nutrition on infant nutrition and associated health practices in Narok, Kenya. Afr Health Sci. 2020;20(2):724–734. PubMed PMID: 33163037. doi:10.4314/ahs.v20i2.24
55. Yeasmin F, Winch PJ, Hwang ST, et al. Exploration of attendance, active participation, and behavior change in a group-based responsive stimulation, maternal and child health, and nutrition intervention. Am J Trop Med Hyg. 2021;104(4):1586–1595. PubMed PMID: 33534769. doi:10.4269/ajtmh.20-0991
56. Gladstone M, Phuka J, Thindwa R, et al. Care for child development in rural Malawi: a model feasibility and pilot study. Ann N Y Acad Sci. 2018;1419(1):102–119. PubMed PMID: 29791732. doi:10.1111/nyas.13725
57. Omer A, Hailu D, Whiting SJ. Child-owned poultry intervention effects on hemoglobin, anemia, concurrent anemia and stunting, and morbidity status of young children in Southern Ethiopia: a cluster randomized controlled community trial. Int J Environ Res Public Health. 2023;20(7):5406. PubMed PMID: 37048019. doi:10.3390/ijerph20075406
58. Hemlock C, Galasso E, Weber AM, et al. Integrating early child development into an existing health and nutrition program: evidence from a cluster-randomized controlled trial. BMC Public Health. 2024;24(1). PubMed PMID: 39334156. doi:10.1186/s12889-024-20149-w
59. Rahman M, Jhohura FT, Mistry SK, et al. Assessing community based improved maternal neonatal child survival (IMNCS) program in rural Bangladesh. PLoS One. 2015;10(9):1–15. PubMed PMID: 26340672. doi:10.1371/journal.pone.0136898
60. Jahir T, Winch PJ, Leontsini E, et al. Success factors for community health workers inimplementing an integrated group-based child development intervention in rural Bangladesh. Int J Environ Res Public Health. 2021;18(15):7891. PubMed PMID: 34360185. doi:10.3390/ijerph18157891
61. Marume A, Mahomed S, Archary M. Evaluation of the child growth monitoring programme in two Zimbabwean provinces. Afr J Prim Health Care Fam Med. 2022;14(1):1–8. PubMed PMID: 35924624. doi:10.4102/PHCFM.V14I1.3373
62. Gelli A, Margolies A, Santacroce M, et al. Improving child nutrition and development through community-based childcare centres in Malawi - The NEEP-IE study: study protocol for a randomised controlled trial. Trials. 2017;18(1). PubMed PMID: 28629471. doi:10.1186/s13063-017-2003-7
63. Gnanaselvam NA, Johnson AR, Shetty A. Evaluating the effectiveness of training on malnutrition for Anganwadi workers in Anekal Taluk, Bengaluru Urban District. J Family Med Prim Care. 2025;14(3):1029–1035. doi:10.4103/jfmpc.jfmpc_1442_24
64. Wanda D, Astuti A, Adawiyah R, et al. Exploring practical issues in children’s anthropometric measurements: a qualitative descriptive study involving Indonesian health professionals and community health workers. Belitung Nurs J. 2025;11(5):538–546. doi:10.33546/bnj.3987
65. Irdawati I, Arifah S, Muhlisin A, et al. Efforts of increase cadre capacity about stunting prevention. MethodsX. 2024;13:102720. doi:10.1016/j.mex.2024.102720
66. Sukmawati S, Hermayanti Y, Fadlyana E, Maulana I, Mediani HS. Health cadres’ experiences in detecting and preventing childhood stunting in Indonesia: a qualitative study. BMC Public Health. 2025;25(1). PubMed PMID: 40887655. doi:10.1186/s12889-025-24192-z
67. Astutik J, Suprapto B, Abidin Z. Training and mentoring of Posyandu cadres based on behavior change in an effort to prevent stunting in Mulyoagung village, Dau sub-district, Malang district. J Commun Serv Empower. 2025;6(1):133–146. doi:10.22219/jcse.v6i1.39052
68. Dwiyanti D. The effect of human development cadre mentoring on knowledge and attitude of stunting prevention in pregnant women in Sragen. Miracle J Public Health. 2025;8(1). doi:10.36566/mjph/Vol8.Iss1/413
69. Altobelli LC, Cabrejos-Pita J, Penny M, Becker S. A cluster-randomized trial to test sharing histories as a training method for community health workers in Peru. Glob Health Sci Pract. 2020;422–424. doi:10.9745/GHSP-D-19-00332
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.