")
Back to Journals » International Journal of General Medicine » Volume 16
HDL-C/LDL-C and Risk of Cerebral White Matter Hyperintensities: A Cross-Sectional Study
Authors Wei C, Chen Y, Yu X, Yang T, Li J, Chen X
Received 7 September 2023
Accepted for publication 3 November 2023
Published 7 November 2023 Volume 2023:16 Pages 5175—5182
DOI https://doi.org/10.2147/IJGM.S439150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Cunsheng Wei,* Yuan Chen,* Xiaorong Yu, Tingting Yang, Junrong Li, Xuemei Chen
Department of Neurology, The Affiliated Jiangning Hospital with Nanjing Medical University, Nanjing, Jiangsu, 211100, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuemei Chen, Department of Neurology, The Affiliated Jiangning Hospital with Nanjing Medical University, 169 Hushan Road, Nanjing, Jiangsu, 211100, People’s Republic of China, Tel +86 13347808579, Email [email protected]
Background and Purpose: At present, there is still a lack of metabolic indices to predict white matter hyperintensities. This study aimed to explore the correlations of the high-density lipoprotein cholesterol (HDL-C)/low-density lipoprotein cholesterol (LDL-C) ratio with the risk of white matter hyperintensities.
Methods: Hospitalized patients who underwent inpatient treatment or physical examination due to various chronic diseases between January 18, 2018, and March 20, 2023, were enrolled. Fazekas scores were used to assess the severity of white matter hyperintensities. Logistic regression analysis was used to adjust for possible confounders.
Results: Of the 1162 enrolled patients, 770 (66.27%) patients were classified as having no or mild WMHs, and 392 (33.73%) were classified as having moderate or severe WMHs. After adjusting for covariates, the logistic regression analysis indicated that the ratio of HDL-C to LDL-C was related to the severity of WMHs (Model 1, OR = 0.23, 95% CI: 0.07– 0.73, P=0.012; Model 2, OR = 2.03, 95% CI: 1.12– 3.67, P=0.019).
Conclusion: Our findings suggest that the ratio of HDL-C to LDL-C is related to the severity of WMHs and that a high ratio of HDL-C to LDL-C is a protective factor against WMHs. This suggests that the ratio of HDL-C to LDL-C could be used as a metabolic prediction index of WMH severity.
Keywords: high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, white matter hyperintensities, risk, Fazekas scale
Introduction
White matter hyperintensities (WMHs) are very common in older individuals and confer an increased risk of stroke, dementia and death.1,2 Existing studies suggest that WMHs are indicative of cerebral small vessel disease and are associated with age and hypertension.3,4 In recent years, the relationship between abnormal lipid metabolism and WMHs has attracted increasing attention from scholars. A multicenter, large-sample cohort study used circulating metabolomic measures to show that multiple lipid measures (eg, lysophosphatidylcholines, hydroxysphingomyelin, low-density lipoprotein size and composition) were associated with WMHs in a general population of middle-aged and older adults.5 Another study revealed strong associations of metabolic syndrome with WMHs and cognitive deficits.6
At present, there is still a lack of metabolic indices to predict WMHs. Both high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) are indicators of lipid metabolism and are related to the risk of cardiovascular and cerebrovascular diseases. As a new marker of lipid metabolism, the HDL-C/LDL-C ratio can better reflect the balance of atherogenic and antiatherogenic cholesterol than HDL-C or LDL-C alone and is a predictor of the risk of atherosclerosis and cardiovascular and cerebrovascular diseases.7 A recent study showed that an HDL-C/LDL-C ratio of 0.4–0.6 was correlated with lower MI risk, all-cause mortality, hemorrhagic stroke and ischemic stroke.8 Therefore, we designed a cross-sectional study to explore the correlations of the HDL-C/LDL-C ratio with the risk of WMHs.
Methods
Study Population
In our cross-sectional study, the study group consisted of hospitalized patients who underwent inpatient treatment or physical examination due to various chronic diseases in the Department of Neurology, Affiliated Jiangning Hospital of Nanjing Medical University between January 18, 2018, and March 20, 2023. The inpatient medical record system contains data on patient demographics, clinical and imaging features and treatment details. Data on patient demographics, clinical history, and clinical presentation were collected. The inclusion criteria were as follows: 1) aged 45 or older and 2) underwent cerebral MRI. The exclusion criteria were as follows: participants with severe head injury; severe cerebral infarction, defined as an NIH Stroke Scale score ≥ 14; severe cerebral hemorrhage, defined as a baseline intraparenchymal hemorrhage volume ≥ 30 mL or intraventricular hemorrhage; vascular malformation or brain malignancy; or the presence of multiple sclerosis or a lack of complete clinical data. A total of 1766 middle-aged and elderly inpatients with various chronic diseases or who were physically examined were enrolled in the study. All patients provided informed consent and were enrolled if all inclusion criteria and none of the exclusion criteria were met. At the end of the study, 1162 eligible patients were analyzed, and a detailed study flowchart is shown in Figure 1.
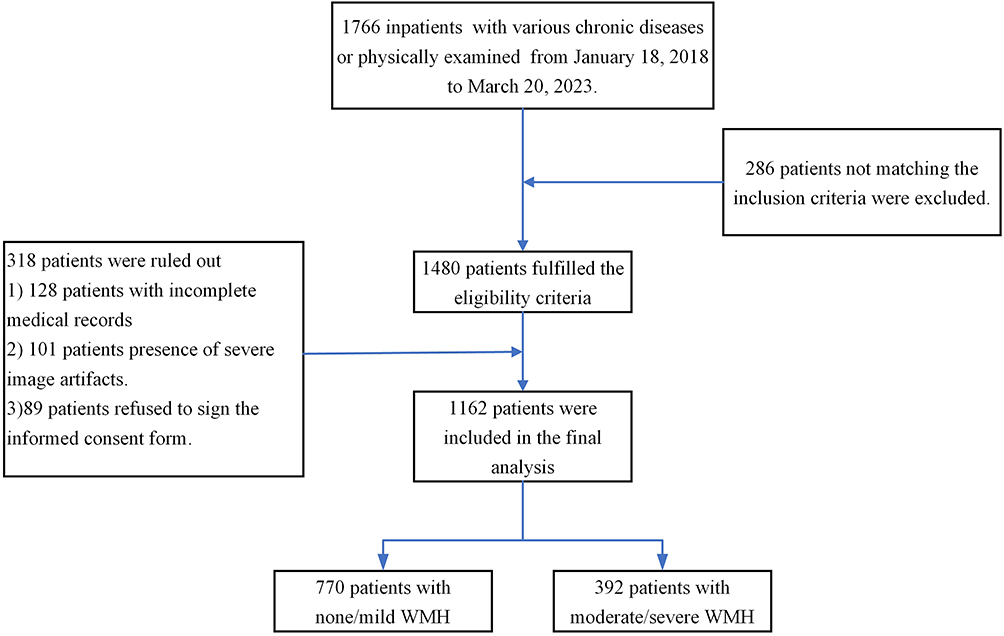 |
Figure 1 Flow chart of patient inclusion for this study. |
Data Collection
To assess relevant risk factors at baseline, we examined patient demographic characteristics (age, sex, body mass index (BMI) and medical history), history of hypertension, history of diabetes mellitus, presence of coronary heart disease, history of atrial fibrillation, history of cerebral hemorrhage, history of ischemic stroke, past or present cigarette or alcohol use, and antiplatelet or statin treatment. Patients underwent a physical examination, systolic and diastolic blood pressure (SBP & DBP) was measured, and laboratory examinations including tests for glucose (white blood cell counts, D-dimer, fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c), homocysteine (HCY), total cholesterol (TC), high-density lipoprotein cholesterol (HDL), triglyceride (TG), low-density lipoprotein (LDL), lipoprotein-a (LP-A), creatinine (Cr) and uric acid (UA) were performed.
MRI Acquisition
Enrolled patients underwent a brain MRI examination with a 3.0 T scanner (Philips Medical Systems, the Netherlands) with an 8-channel receiver array head coil. Standardized parameters of the MRI sequences, including T1-weighted, T2-weighted and fluid-attenuated inversion recovery images, were obtained. Detailed parameters of the MRI scans were reported in our previous study.9,10
Fazekas Scores for Assessment of the Severity of WMHs
The Fazekas scale divides the white matter into periventricular and deep white matter, and each region is given a grade depending on the size and confluence of lesions:11 (1) periventricular white matter hyperintensities (PVWMHs), for which 0 = absent, 1 = “caps” or pencil-thin lining, 2 = smooth “halo”, and 3 = irregular periventricular signal extending into the deep white matter; and (2) deep white matter hyperintensities (DWMHs), for which 0 = absent, 1 = punctate foci, 2 = beginning confluence, and 3 = large confluent areas. Two experienced neurologists and a neuroradiologist participated in the evaluation of the MRI results. WMHs were analyzed as none/mild (Fazekas score 0–1) vs moderate/severe (Fazekas score 2–3) according to Fazekas scores. If scores for the two samples were discordant, the final score for the classification was upgraded to the higher score.
Statistics
Continuous data are summarized as the mean values with SDs for data with a normal distribution or the median values with interquartile ranges for data with a skewed distribution. Categorical data are presented as frequencies with proportions. A two-sample t test was used to compare continuous data. Categorical data were analyzed using the chi-square test. Multivariable logistic regression analysis was used to adjust for possible confounding factors. All statistical analyses were performed using SPSS 25.0 software (SPSS, Chicago, IL).
Results
Of the 1162 enrolled patients, 770 (66.27%) patients were classified as having no or mild WMHs, and 392 (33.73%) were classified as having moderate or severe WMHs. Patients with no or mild WMHs were younger (62.67±9.93 vs 70.72±9.43, y, P <0.001) than those with moderate or severe WMHs. In addition, the asymptomatic or mild-illness patient groups had a lower ratio of hypertension (60.78% vs 78.32%; P<0.001), diabetes (23.25% vs 30.87%; P=0.007), previous cerebral hemorrhage (1.69% vs 4.59%; P=0.041), previous ischemic stroke (36.36% vs 47.19%; P<0.001), atrial fibrillation (2.21% vs 4.59%; P=0.023), oral antiplatelet drugs (50.39% vs 62.76%; P <0.001) and oral statins (47.79% vs 54.85%; P =0.031) than the group of patients with moderate or severe WMHs. Moreover, patients with no or mild WMHs presented with lower levels of SBP (136.99±20.25 vs 147.44±22.71, mmHg, P<0.001), DBP (80.46±12.89 vs 82.82±12.73, mmHg, P=0.006), pulse pressure (56.13±16.61 vs 64.45±18.31, mmHg, P<0.001), D-dimer (0.49±0.82 vs 0.96±0.72, mg/L, P<0.001), glycated hemoglobin (5.99±1.30 vs 6.26±1.55, %, P=0.009), lipoprotein(a) (233.76±223.61 vs 266.50±254.88, mg/dL, P=0.028), creatinine (64.54±20.86 vs 72.27±27.23, µmmol/L, P<0.001), uric acid (308.50±87.69 vs 321.42±92.02, µmmol/L, P=0.020) and homocysteine (13.30±6.96 vs 17.23±10.05, µmmol/L, P<0.001) than patients with moderate or severe WMHs. However, patients with no or mild WMHs had higher levels of HDL-C (1.25±0.49 vs 1.08±0.30, mmol/L, P<0.001) and a higher ratio of HDL-C to LDL-C (0.65±0.54 vs 0.50±0.25, P<0.001) than control subjects. The details are presented in Table 1.
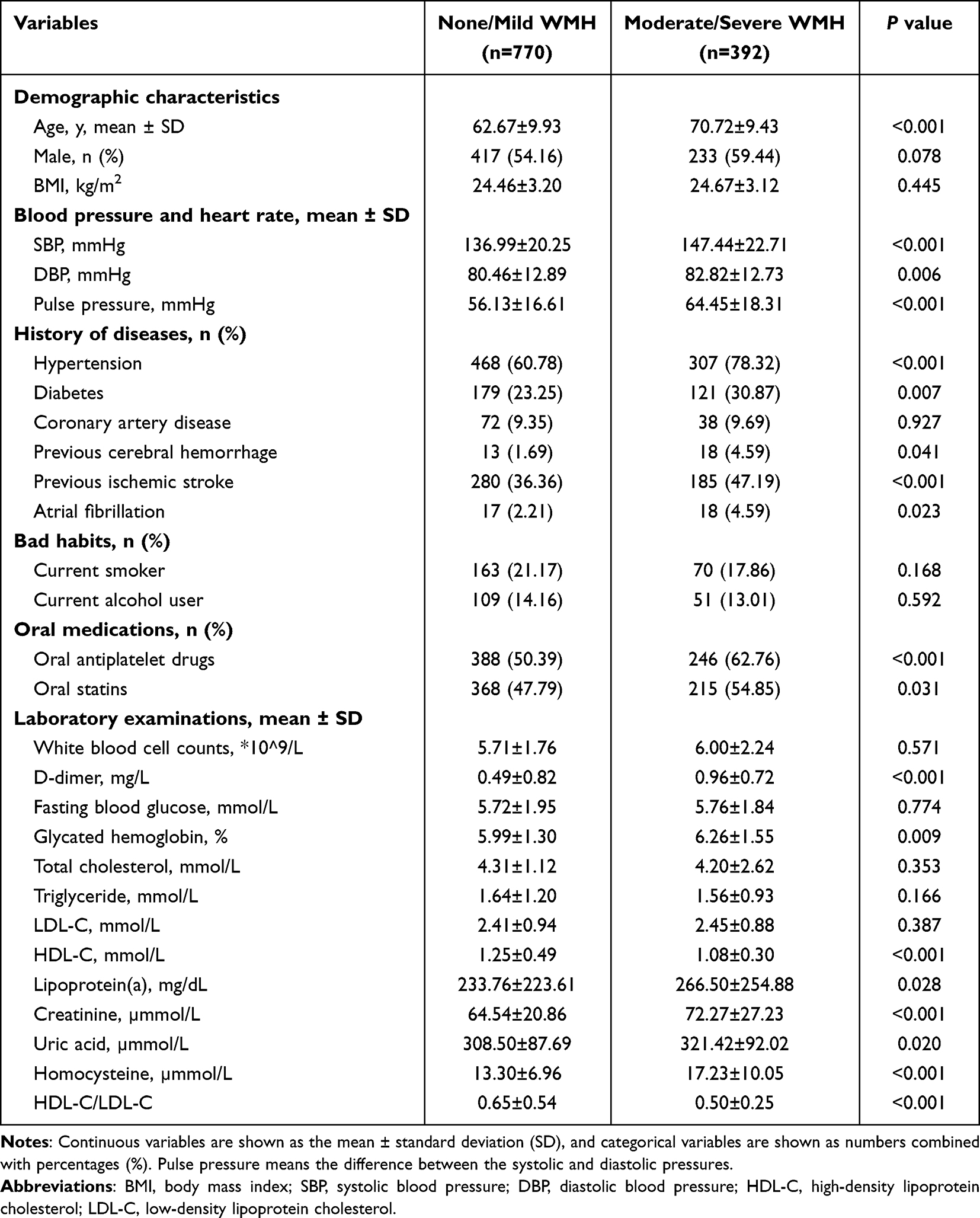 |
Table 1 Clinical Characteristics of the Included Patients (n=1162). WMHs Were Analyzed as None/Mild vs Moderate/Severe Signal Attenuation |
After adjusting for covariates, the logistic regression analysis indicated that the ratio of HDL-C to LDL-C was related to the severity of WMHs (Model 1, OR = 0.23, 95% CI: 0.07–0.73, P=0.012). In addition, age (OR = 1.07, 95% CI: 1.04–1.09, P<0.001), history of cerebral hemorrhage (OR = 3.26, 95% CI: 1.07–9.97, P=0.038), history of ischemic stroke (OR = 1.87, 95% CI: 1.22–2.87, P=0.004) and oral antiplatelet drugs (OR = 1.78, 95% CI: 1.09–2.89, P=0.020) were also associated with a risk of severe WMHs (Table 2).
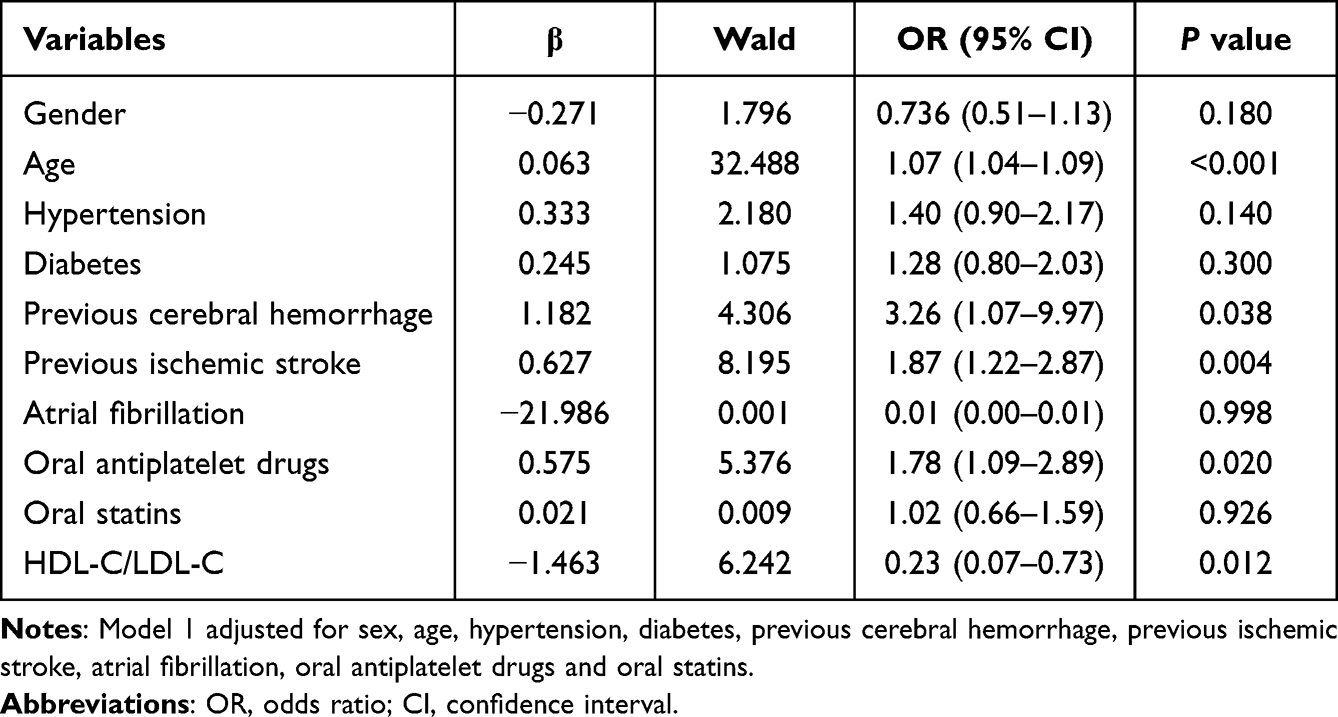 |
Table 2 Correlation Between the Severity of WMHs and Risk Factors in Model 1 |
After adjusting for sex, age, SBP, DBP, previous cerebral hemorrhage, previous ischemic stroke, atrial fibrillation, oral antiplatelet drugs, oral statins, D-dimer, glycated hemoglobin, lipoprotein(a), creatinine, uric acid and homocysteine, the logistic regression analysis also indicated that a high ratio of HDL-C to LDL-C was a protective factor against WMHs (Model 2, OR = 0.19, 95% CI: 0.04–0.86, P=0.031). In addition, age (OR = 1.05, 95% CI: 1.02–1.08, P=0.001), previous cerebral hemorrhage (OR = 4.79, 95% CI: 1.35–16.91, P=0.015), previous ischemic stroke (OR = 1.75, 95% CI: 1.04–2.93, P=0.035) and oral antiplatelet drugs (Model 2, OR = 2.03, 95% CI: 1.12–3.67, P=0.019) were also associated with a risk of severe WMHs (Table 3).
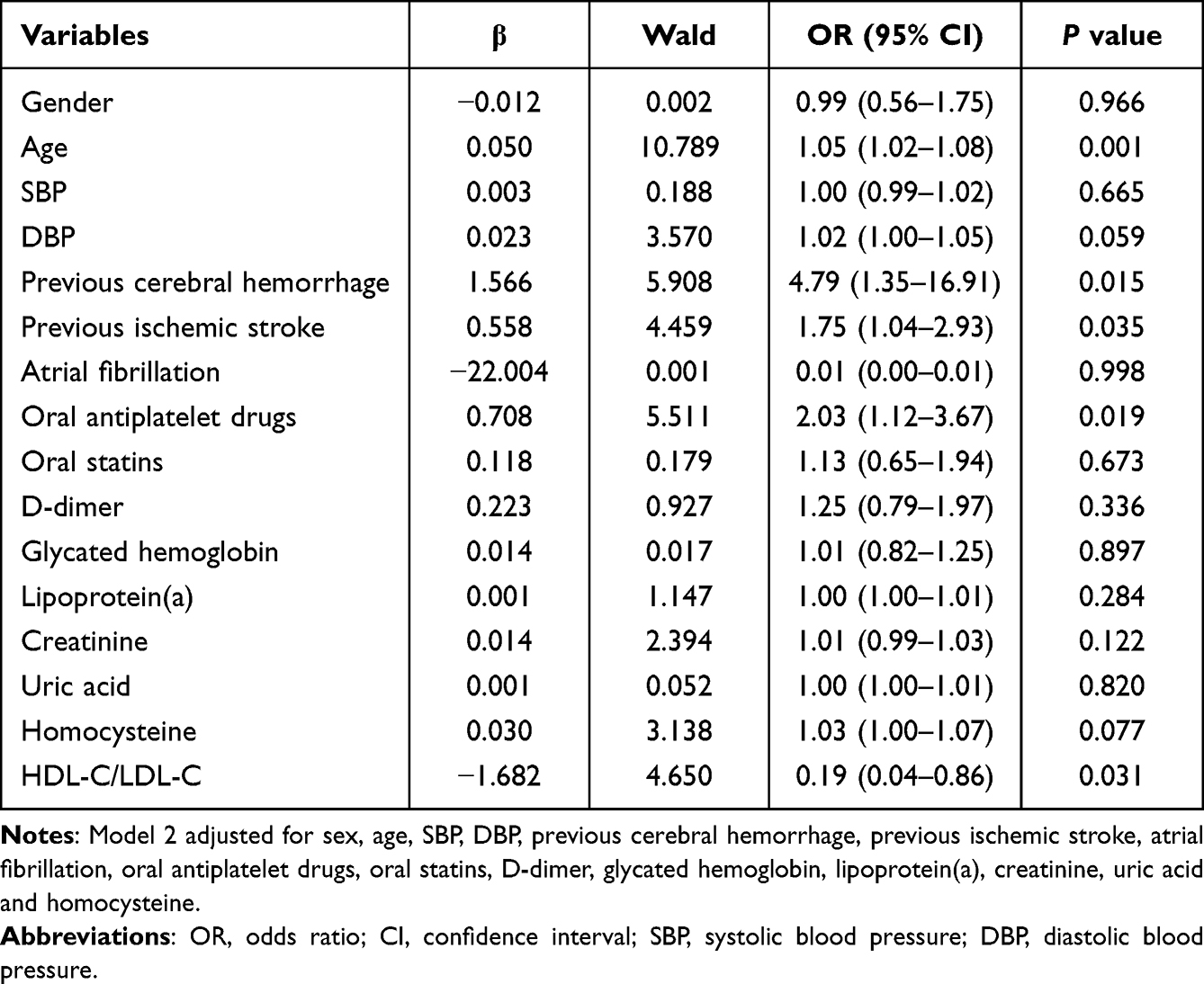 |
Table 3 Correlation Between the Severity of WMHs and Risk Factors in Model 2 |
We then compared the distribution of HDL-C/LDL-C between patients with no or mild and moderate or severe WMHs by univariate analysis. The results showed that the ratios of HDL-C to LDL-C were significantly higher in patients with no or mild WMHs than in those with moderate or severe illness (Figure 2).
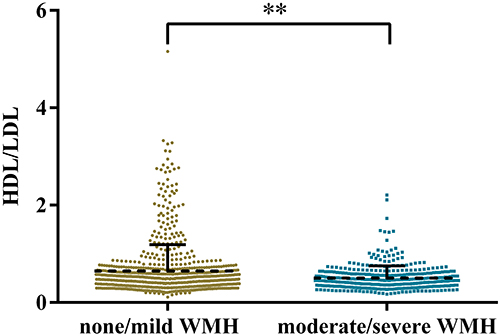 |
Figure 2 Comparison of HDL/LDL distribution between the two groups. Asterisks “**” represent P < 0.01 compared with the control group. |
Discussion
This study revealed that the ratio of HDL-C to LDL-C was related to the severity of WMHs and that a high ratio of HDL-C to LDL-C was a protective factor against WMHs. This suggests that the ratio of HDL-C to LDL-C could be used as a metabolic prediction index of WMH severity.
Hyperlipidemia, especially increased LDL-C levels and decreased HDL levels, are major risk factors for atherosclerosis.12 Studies have shown that the ratio of HDL-C to LDL-C can better reflect the balance of atherogenic and antiatherogenic cholesterol than HDL-C or LDL-C alone, and a decreased HDL-C/LDL-C ratio is an important risk factor for coronary heart disease.13,14 Our study suggested that the ratio of HDL-C to LDL-C can also predict the severity of WMHs even after adjusting for covariates.
We speculate that this may be caused by the following circumstances. First, WMHs are a common condition that often occurs in elderly individuals and shares common risk factors with cardiovascular and cerebrovascular diseases. Our previous research also suggested that hyperuricemia and small low-density lipoprotein cholesterol may increase the risk of WMHs.15,16 A reduced ratio of HDL-C to LDL-C is a risk factor for cardiovascular and cerebrovascular diseases, which can also lead to increased WMH risk.17 Second, low levels of HDL-C could cause lipid oxidation, hence inducing inflammation and accentuating tissue damage, and importantly, decreased HDL levels may further increase inflammation, thus perhaps eventually leading to small blood vessel damage, resulting in WMHs.18,19 Third, LDL-C tends to deposit in the walls of arteries, leading to plaque buildup in the artery wall, eventually blocking the artery. Plaque buildups can lead to heart attacks and dangerous blood clots. The accumulation of LDL-C inside the blood vessels serves as a major cause of arteriosclerosis, and even slightly elevated LDL cholesterol may have a negative impact on cardiovascular risk.20,21 Therefore, the ratio of HDL-C to LDL-C can better reflect the severity of inflammation, lipid metabolism and arteriosclerosis, all of which may be related to the risk of WMHs.
To the best of our knowledge, this is the first large-sample study demonstrating the relationship between HDL-C/LDL-C and the severity of WMHs. All data were subjected to rigorous quality controls, and rigorous statistical analyses were performed. Meanwhile, to further understand the relationship between HDL-C/LDL-C and WMHs, we performed logistic regression to adjust for confounding factors. This finding will encourage scholars to further understand the relationship between WMHs and metabolic indices. However, there are some limitations in the current study, which are listed as follows. First and most importantly, this study is based on clinical research and does not explore the mechanism. Second, this study is a single-center study involving individuals in the Han population in the same region. Therefore, further multicenter and in-depth mechanistic studies are needed to overcome the above limitations.
Taken together, our findings suggest that the HDL-C to LDL-C ratio was related to the severity of WMHs and that a high ratio of HDL-C to LDL-C was a protective factor against WMHs. Moreover, a longer follow-up period is needed to evaluate the relationship between WMHs and metabolic indices.
Abbreviations
WMHs, white matter hyperintensities; PVWMHs, periventricular white matter hyperintensities; DWMHs, deep white matter hyperintensities; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; HCY, homocysteine; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; LP-A, lipoprotein(a); Cr, creatinine; UA, uric acid; SD, standard deviation; OR, odds ratio; CI, confidence interval.
Data Sharing Statement
Study data are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
We obtained ethical approval for this study from the ethics committee of the Affiliated Jiangning Hospital of Nanjing Medical University and performed in accordance with the Declaration of Helsinki (reference number, 202203023K01). Written informed consent was obtained from all study participants.
Consent for Publication
All patients gave informed consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Scientific research project of Jiangsu Provincial Health Commission (M2022009); the Nanjing Health Science and Technology Development Special Fund Project (YKK22216); the Clinical Medical Science and Technology Development Fund of Jiangsu University (JLY2021153); Jiangning District Science and Technology Huimin Project (2022092S).
Disclosure
The author declares no competing financial interests.
References
1. Du Y, Song Y, Zhang X, et al. Leptin receptor deficiency protects mice against chronic cerebral hypoperfusion-induced neuroinflammation and white matter lesions. Mediators Inflamm. 2020;2020:7974537. doi:10.1155/2020/7974537
2. Tran P, Thoprakarn U, Gourieux E, et al. Automatic segmentation of white matter hyperintensities: validation and comparison with state-of-the-art methods on both multiple sclerosis and elderly subjects. Neuroimage Clin. 2022;33:102940. doi:10.1016/j.nicl.2022.102940
3. Waymont JMJ, Petsa C, McNeil CJ, Murray AD, Waiter GD. Validation and comparison of two automated methods for quantifying brain white matter hyperintensities of presumed vascular origin. J Int Med Res. 2020;48(2):300060519880053. doi:10.1177/0300060519880053
4. Mu R, Qin X, Guo Z, et al. Prevalence and consequences of cerebral small vessel diseases: a cross-sectional study based on community people plotted against 5-year age strata. Neuropsychiatr Dis Treat. 2022;18:499–512. doi:10.2147/NDT.S352651
5. Sliz E, Shin J, Ahmad S, et al. Circulating metabolome and white matter hyperintensities in women and men. Circulation. 2022;145(14):1040–1052. doi:10.1161/CIRCULATIONAHA.121.056892
6. Portet F, Brickman AM, Stern Y, et al. Metabolic syndrome and localization of white matter hyperintensities in the elderly population. Alzheimers Dement. 2012;8(5 Suppl):S88–S95.e81. doi:10.1016/j.jalz.2011.11.007
7. Kunutsor SK, Zaccardi F, Karppi J, Kurl S, Laukkanen JA. Is high serum LDL/HDL cholesterol ratio an emerging risk factor for sudden cardiac death? Findings from the KIHD study. J Atheroscler Thromb. 2017;24(6):600–608. doi:10.5551/jat.37184
8. Yuan S, Huang X, Ma W, et al. Associations of HDL-C/LDL-C with myocardial infarction, all-cause mortality, haemorrhagic stroke and ischaemic stroke: a longitudinal study based on 384 093 participants from the UK Biobank. Stroke Vasc Interv Neurol. 2023;8(2):119–126. doi:10.1136/svn-2022-001668
9. Chen X, Wang L, Jiang J, et al. Association of neuroimaging markers of cerebral small vessel disease with short-term outcomes in patients with minor cerebrovascular events. BMC Neurol. 2021;21(1):21. doi:10.1186/s12883-021-02043-9
10. Jiang J, Gao Y, Zhang R, et al. Differential effects of serum lipoprotein-associated phospholipase A2 on periventricular and deep subcortical white matter hyperintensity in brain. Front Neurol. 2021;12:605372. doi:10.3389/fneur.2021.605372
11. Ortega G, Espinosa A, Alegret M, et al. Combination of white matter hyperintensities and Aβ burden is related to cognitive composites domain scores in subjective cognitive decline: the FACEHBI cohort. Alzheimers Res Ther. 2021;13(1):141. doi:10.1186/s13195-021-00877-6
12. Wang Z, Li P, Wang C, et al. Protective effects of Arctium lappa L. root extracts (AREs) on high fat diet induced quail atherosclerosis. BMC Complement Altern Med. 2016;16(1):6. doi:10.1186/s12906-016-0987-2
13. Abbas MA, Boby N, Lee EB, Hong JH, Park SC. Anti-obesity effects of Ecklonia cava extract in high-fat diet-induced obese rats. Antioxidants. 2022;11(2). doi:10.3390/antiox11020310
14. Zhang R, Fan Y, Xue Y, et al. The LDL/HDL ratio predicts long-term risk of coronary revascularization in ST-segment elevation myocardial infarction patients undergoing percutaneous coronary intervention: a cohort study. Braz J Med Biol Res. 2022;55:e11850. doi:10.1590/1414-431x2021e11850
15. Yu X, Yu Y, Wei C, et al. Association between small dense low-density lipoprotein cholesterol and neuroimaging markers of cerebral small vessel disease in middle-aged and elderly Chinese populations. BMC Neurol. 2021;21(1):436. doi:10.1186/s12883-021-02472-6
16. Wei C, Yu X, Wang L, et al. Can hyperuricemia predict the progression risk of cerebral small vessel disease?. Neurol Res. 2022;44(10):910–917. doi:10.1080/01616412.2022.2067707
17. Chen Y, Wang X, Guan L, Wang Y. Role of white matter hyperintensities and related risk factors in vascular cognitive impairment: a review. Biomolecules. 2021;11(8):1102. doi:10.3390/biom11081102
18. Peng F, Lei S, Zhang Q, Zhong Y, Wu S. Triglyceride/high-density lipoprotein cholesterol ratio is associated with the mortality of COVID-19: a retrospective study in China. Int J Gen Med. 2022;15:985–996. doi:10.2147/IJGM.S346690
19. Macpherson ME, Halvorsen B, Yndestad A, et al. Impaired HDL function amplifies systemic inflammation in common variable immunodeficiency. Sci Rep. 2019;9(1):9427. doi:10.1038/s41598-019-45861-1
20. Valsdottir TD, Henriksen C, Odden N, et al. Effect of a low-carbohydrate high-fat diet and a single bout of exercise on glucose tolerance, lipid profile and endothelial function in normal weight young healthy females. Front Physiol. 2019;10:1499. doi:10.3389/fphys.2019.01499
21. Hu J, Liu M, Yang R, et al. Effects of high-intensity interval training on improving arterial stiffness in Chinese female university students with normal weight obese: a pilot randomized controlled trial. J Transl Med. 2022;20(1):60. doi:10.1186/s12967-022-03250-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.