Back to Journals » Risk Management and Healthcare Policy » Volume 16
Having a Say Matters: The Association Between Home Health Aides’ Voice and Job Satisfaction
Authors Bensson-Ravunniarath M, Bryan Ringel J, Avgar A, Wiggins F, Lee A, McDonald MV, Guerrero LR, Kallas J ![]() , Gusoff G, Shen M, Tseng E
, Gusoff G, Shen M, Tseng E ![]() , Dell N
, Dell N ![]() , Czaja S, Lindquist LA, Sterling MR
, Czaja S, Lindquist LA, Sterling MR
Received 6 May 2023
Accepted for publication 18 August 2023
Published 8 September 2023 Volume 2023:16 Pages 1791—1800
DOI https://doi.org/10.2147/RMHP.S420207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Mara Bensson-Ravunniarath,1 Joanna Bryan Ringel,2 Ariel Avgar,3 Faith Wiggins,4 Ann Lee,4 Margaret V McDonald,5 Lourdes R Guerrero,6 John Kallas,3 Geoffrey Gusoff,7 Megan Shen,8 Emily Tseng,9 Nicola Dell,9 Sara Czaja,2 Lee A Lindquist,10 Madeline R Sterling2
1Department of Medicine, Massachusetts General Hospital, Boston, MA, USA; 2Department of Medicine, Weill Cornell Medicine, New York, NY, USA; 3Cornell University, School of Industrial Labor Relations, Ithaca, NY, USA; 4 1199SEIU Training and Employment Fund, New York, NY, USA; 5Center for Home Care Policy & Research, VNS Health, New York, NY, USA; 6Department of Neurosciences, UC San Diego, San Diego, CA, USA; 7Department of Family Medicine, UCLA, Los Angeles, CA, USA; 8Clinical Research Division, Fred Hutch Cancer Center, Seattle, WA, USA; 9Cornell Tech, Cornell University, New York, NY, USA; 10Division of Geriatrics, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA
Correspondence: Madeline R Sterling, Department of Medicine, Division of General Internal Medicine, Weill Cornell Medicine, 420 East 70th Street, Room LH-357, New York, NY, 10021, USA, Tel +1646-962-5029, Email [email protected]
Purpose: Despite a rapidly growing need for home health aides (HHAs), turnover rates are high. While this is driven in large part by the demanding nature of their work and low wages, another factor may be that HHAs are often not considered part of the medical team which can leave them feeling unheard by other healthcare professionals. We sought to determine whether this concept, or HHAs’ perceived voice, was associated with job satisfaction.
Methods and Design: This cross-sectional survey of English- and Spanish-speaking HHAs caring for adults with heart failure (HF) was conducted from June 2020 to July 2021 in New York, NY in partnership with a labor management fund of a large healthcare union that provides benefits and training to HHAs. Voice was assessed with a validated 5-item scale (total score range 5 to 25). Job Satisfaction was assessed with the 5-item Work Domain Satisfaction Scale (total score range 5 to 35). Multivariable linear regression analysis was used to examine the association between voice and job satisfaction.
Results: A total of 413 HHAs employed by 56 unique home care agencies completed the survey; they had a mean age of 48 years, 97.6% were female, 60.2% were Hispanic, and they worked as HHAs for a median of 10 years (IQR, 5, 17). They had a median Voice score of 18 (IQR 15– 20) and mean job satisfaction score of 26.4 (SD 5.6). Higher levels of voice (1.75 [0.46– 3.04]) were associated with greater job satisfaction (p=0.008). When adjusting for Race/Ethnicity, HF training, and HF knowledge, the association between Voice and job satisfaction remained significant ((1.77 [0.40– 3.13])
Conclusion: HHAs with a voice in the care of their patients experienced greater job satisfaction. Voice may be an important target for interventions aiming to improve HHAs’ retention in the field.
Keywords: long-term care, home health aide, communication, healthcare team
Introduction
Home health aides and attendants (HHAs), also known as paid or formal caregivers, represent one of the most rapidly growing workforces in the US.1 There are currently 3.4 million HHAs and this number is expected to grow by 34% by 2030.2 HHAs are trained and certified health professionals often employed through Medicare or Medicaid funded home care agencies, who assist patients with activities of daily living (eg bathing, grooming, eating) and instrumental activities of daily living (eg cooking, cleaning, grocery shopping). These activities are critical for the care of older adults aging in place, a group which is expected to increase by 112% by 2060.3,4 Beyond personal care, prior research has found HHAs contribute to medically- oriented care, and often are the first to recognize and respond to patients’ clinical changes in the home.5,6 However, despite this, HHAs are not formally considered members of the medical team and their training varies by their model of employment.
Despite these contributions, HHAs face numerous challenges as a workforce, including not feeling valued by the medical community or society at large.5,7 This is problematic and likely contributing to high levels of turnover currently plaguing the HHA workforce.8 Some of this is due to the fact that HHAs – who are predominantly women and people of color – experience structural disadvantages including low wages ($12/hr.), erratic employment (ie numerous shifts which can be physically and mentally taxing), and limited opportunities for career advancement.2,3,9 Studies have found that due to the nature of their work (eg providing home-based care rather than institution-based care), HHAs are often poorly integrated into the medical team.5,6,10 For example, prior studies have demonstrated that they experience communication challenges when they try to convey their observations to supervisors and nurses at their home care agencies or to patients’ physicians.5,6,11–14 However, whether having a voice – defined here as the ability or opportunity to provide input regarding patient care– impacts HHAs’ experience caregiving and attitude towards their job has not been investigated. Should an association exist, efforts to improve HHAs’ voice may be a novel target for interventions aiming to improve this workforce’s experience on the job, their contributions to patient care, and ultimately, the health and well-being of their patients.
To that end, we examined whether higher levels of perceived voice among HHAs were associated with job satisfaction, hypothesizing that higher levels of voice would be associated with greater job satisfaction.
Methods
Guiding Conceptual Model
This study was conceived using the conceptual framework by Zarska et al, 2021 (Supplemental Figure 1) which elucidates the relationships between HHAs providing care to patients and how policies and working conditions influence them and the care they deliver.15 For this study, we considered voice (main exposure) a working condition and job satisfaction (main outcome) as a worker’s outcome. In addition to conceptualizing the study question and main variables of interest, the framework was also used to select covariates and inform the analytic plan.
Study Design, Setting, and Population
This cross-sectional study was part of a larger survey which aimed to understand HHAs’ experiences caring for adults with heart failure (HF) in New York, NY. Although our main study question is not specific to HF, HF is a complex condition in which HHAs frequently provide care and experience job-related stress.5,6,16 Therefore, it was an appropriate condition to frame the study.
The study was conducted from June 2020 to July 2021 in partnership with the 1199SEIU Training and Employment Funds (TEF), a benefit fund of the 1199 Service Employees International Union (1199SEIU) United Healthcare Workers East, the largest health care union in the US. TEF is a non-profit labor management organization that provides training and services to 55,000 HHAs in New York, NY.17
To be eligible, HHAs had to be a member of the 1199SEIUTEF, speak English or Spanish, be employed by a licensed or certified home care agency in New York, NY, and have cared for an HF patient in the past. TEF staff administered an electronic survey to HHAs on their listservs via an electronic link generated by Research Electronic Data Capture (REDCap), a web-based, secure, data collection and storage system. Eligibility was assessed (in both languages) by HHAs’ self-report upon opening the survey link. Participation was voluntary and all participants provided electronic consent electronically. Participants were notified in the informed consent that their anonymized data could be used in publications, and they received a $10 gift card for their participation. This study was approved by the IRB at Weill Cornell Medicine (IRB # 19–07020476) and conducted in accordance with the ethical principles outlined in the World Medical Association’s Declaration of Helsinki.
Voice
Voice was assessed using the 5-item validated scale by Clark et al in which it was first used as part of the Dimensions of Climate for Patient Care Questionnaire – a survey used to understand the experiences of registered nurses (Table 1).18 It has since been used by other employment relation scholars interested in investigating frontline worker voice in patient care.19,20 We adapted the measure to the home care setting. As such, questions from the Voice scale aim to measure different aspects of HHAs’ voice in their home care agency and in the medical team. Each of the 5 items are shown in Supplemental Table 1 and include: (1) I have a good deal of say about the quality of patient care at my home care agency; (2) My supervisor asks for my input about patient care; (3) My suggestions are listened to by higher ups; (4) Nobody ever asks for my opinion regarding patient care issues; and (5) Whenever I make a suggestion about patient care, it is usually ignored. Respondents could select a response using a 6-level Likert scale: strongly disagree, disagree, neutral, agree, strongly agree, and does not apply to me (which was scored as “zero”). The total score ranges between 5 and 25, with a higher score indicating a higher degree of voice.
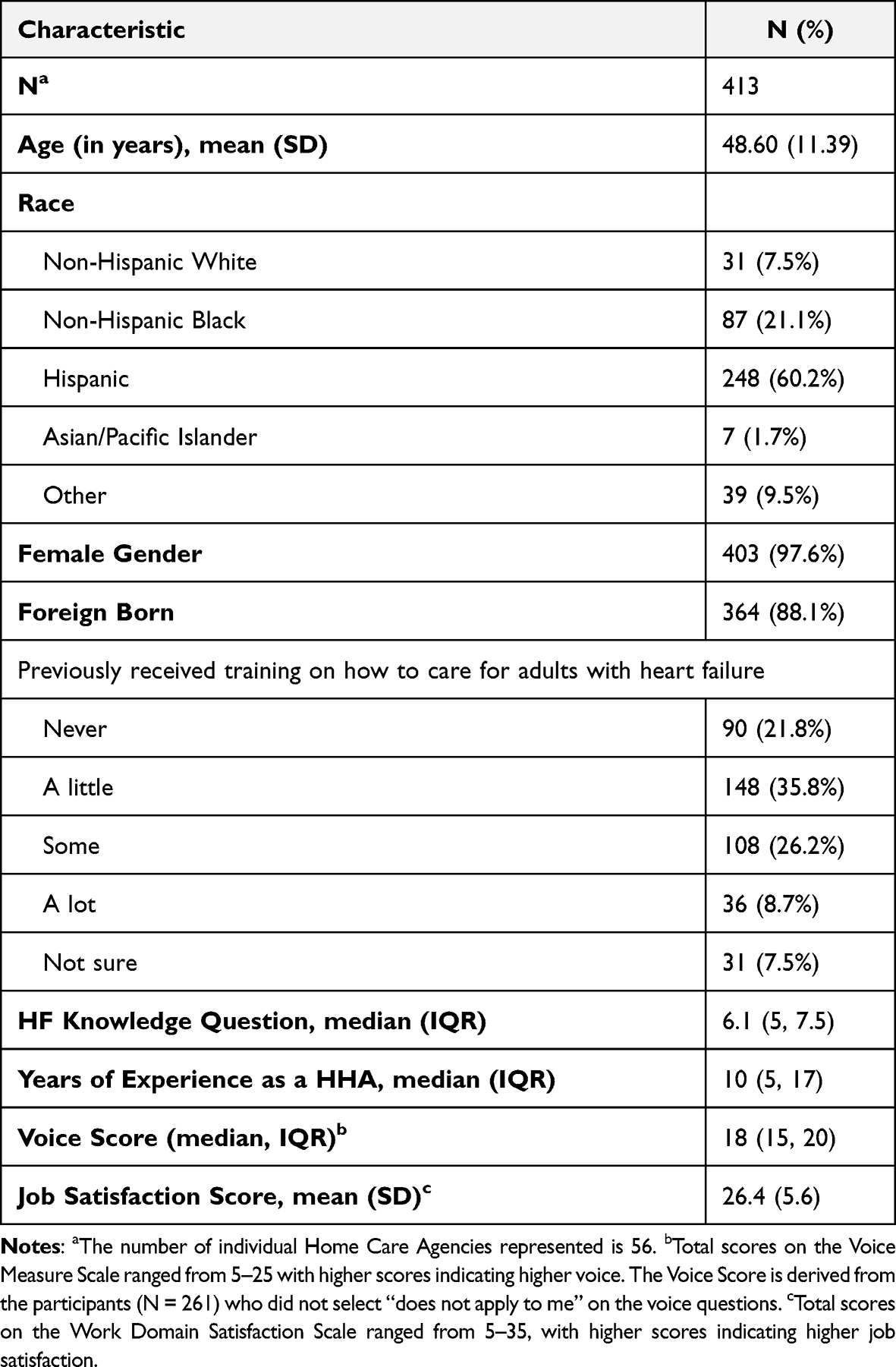 |
Table 1 Characteristics of Study Participants |
Job Satisfaction
Job satisfaction was assessed using the 5-question Work Domain Satisfaction Scale which was validated by Berube et al in 2016.21 This measure has been used previously in the healthcare setting to understand nurse work satisfaction during the COVID pandemic.22 Respondents could choose from a 7-level Likert scale: very strongly disagree, strongly disagree, disagree, neutral, agree, strongly agree, very strongly agree – with total score ranges between 5 and 35. A higher score indicates a higher degree of job satisfaction. Use of this scale was reviewed favorably by the NIH study section and grant funding for this work.
Covariates
Socio-demographic data collected from all participants included age (years), race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Hispanic, other), gender (male/female), and nativity status (foreign born[(yes/no)]). Employment history included years spent as a paid HHA. Experience with HF included receipt of HF training (never, a little, some, a lot, not sure) and HF knowledge (self-reported range 1–10).
Statistical Analysis
Percentages, means, and medians for HHA characteristics, voice and job satisfaction were calculated. Differences in characteristics and job satisfaction by high vs low voice scores were assessed using a chi-square or Wilcoxon rank-sum test. Next, median job satisfaction scores by each individual aspect of voice were observed and p-values for trend were calculated with a Spearman’s rank correlation test. Lastly, linear regression was used to examine the association between voice and job satisfaction and ascertain coefficients and 95% confidence intervals, adjusting for covariates that had a p-value <0.20 in bivariate analyses (Table 2).
 |
Table 2 Characteristics of Study Participants by Level of Voicea |
Assumptions of linearity and normality were explored through preliminary exploration of the data with box plots. To account for the skewed distribution of job satisfaction, we used robust standard errors for model estimates.
Missing data was handled with a listwise approach. Two percent of the data was dropped from the fully adjusted model due to missing data.
Results
Of the 640 HHAs who were eligible and consented to take the survey, 413 completed all five Voice questions. Among these, 152 responded “does not apply to me” for one or more of the voice questions. Since a composite voice score could not be calculated for these respondents, they were excluded from the final analysis (Supplemental Figure 2). The final analytic sample was comprised of 261 HHAs.
In the overall sample, the 413 participants were employed by 56 unique home care agencies. They had a mean age of 48.6 years (SD: 11.39), 97.6% were female, and 88.1% were foreign born. A total of 60.2% identified as Hispanic. Participants reported a median of 10 years (IQR: 5, 17) of experience as a HHA. HHAs with complete voice data (scores for all 5 questions) had a median score of 18 (IQR: 15, 20). The 152 participants who reported that one of more items of the voice scale “did not apply” (and thus a score could not be calculated) differed from the main sample by foreign-born status (93.4% vs 85.1%, respectively) and by Hispanic ethnicity (87.5% vs 44.2%, respectively) (Supplemental Table 2). Finally, the overall sample (of 261 HHAs) had a mean job satisfaction score of 26.4 (SD: 5.6).
Among those who had a voice score (n=261), a total of 53.3% of participants had low voice and 46.7% had high voice; low vs high was defined using a median split (score of 18) (Table 2). Participants with high voice did not differ from those with low voice by most socio-demographic and employment factors. However, they did differ by race/ethnicity. That is, a higher proportion of HHAs with low voice were of Hispanic ethnicity (48.6% low vs 39.3% high, p=0.007, chi-square test). They also differed by experience with HF, such that a higher proportion of HHAs with low voice had lower HF knowledge than those with high voice (5 [5, 6.7] vs 5.2 [5, 7.7], p=0.023, Wilcoxon rank-sum test). Notably, participants with high voice had greater job satisfaction scores (25.6 vs 23.9, p=0.008, ANOVA test).
The association between the individual aspects of voice (domains) and job satisfaction is shown in Table 3. Overall, we found that a high proportion of HHAs agreed (51%) and strongly agreed (22.6%) that they had a voice in the quality of patient care at their agency and that a high proportion of HHAs agreed (44.8%) and strongly agreed (21.1%) that their supervisors asked for their input about important patient care. Additionally, in general, 35.2% and 17.6% of HHAs disagreed and strongly disagreed, respectively, that in general nobody asks for their opinion regarding patient care issues. Across the 5 individual domains of voice, higher voice was associated with higher job satisfaction (p for trends derived from Spearman correlation test in Table 3).
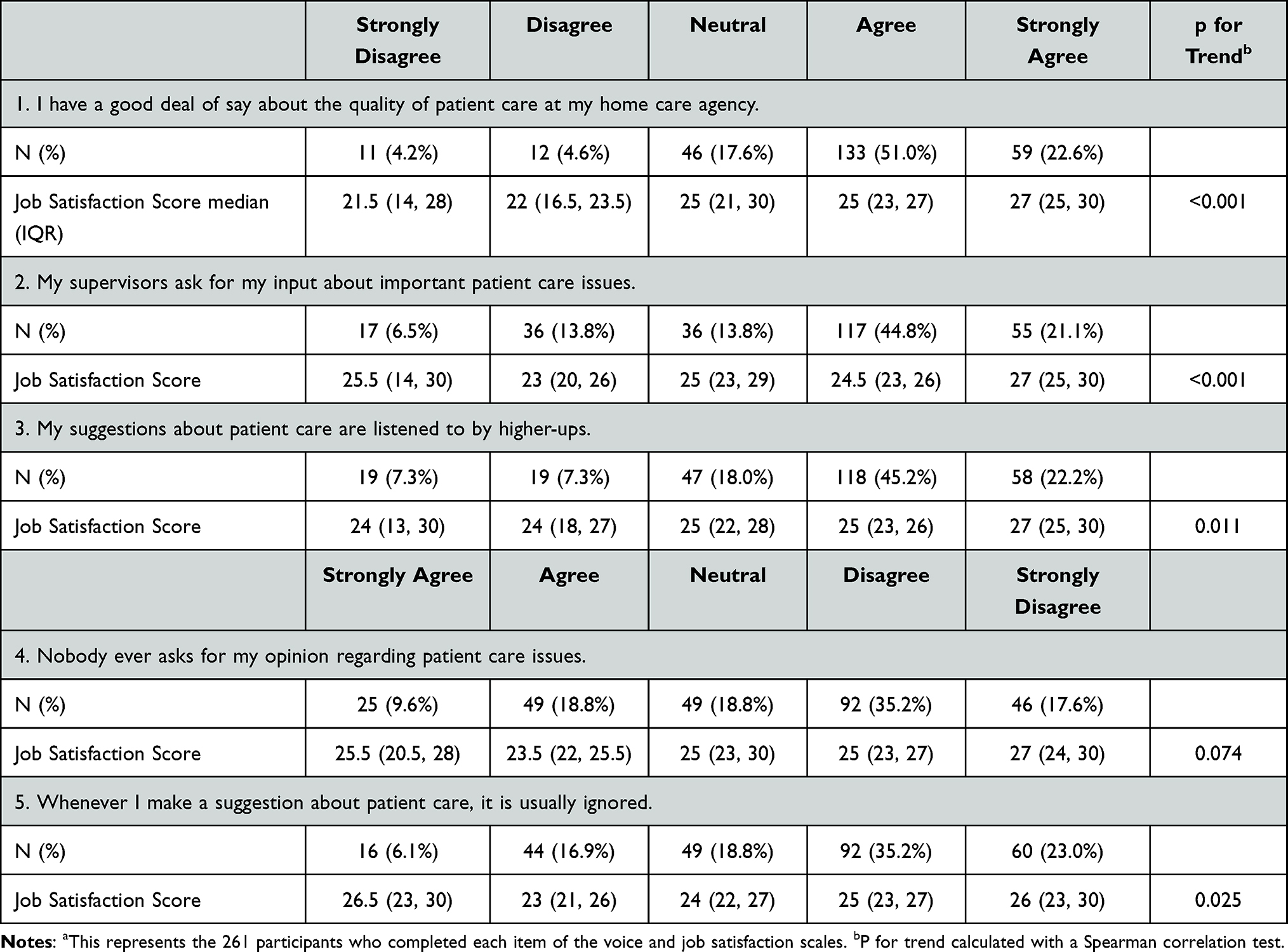 |
Table 3 The Association Between the Individual Voice Domains and Job Satisfactiona |
Models examining the association between overall voice score and job satisfaction are shown in Table 4. In an unadjusted model, higher voice was found to be independently associated with greater job satisfaction (coefficient: 1.75 [0.46–3.04], p=0.008). In a fully adjusted model that accounted for race/ethnicity, HF training and HF knowledge, higher voice remained significantly associated with greater job satisfaction (coefficient: 1.77 [0.40–3.13], p=0.012).
 |
Table 4 The Unadjusted and Fully Adjusted Model for High Voice and Job Satisfaction for 261 Participants.c |
Discussion
More than half of HHAs reported having low levels of voice in caring for their patient. Those HHAs who had a higher level of voice experienced higher satisfaction with their work as higher voice was independently associated with a 1.77-point increase in job satisfaction. Our findings suggest that HHAs’ perceived voice in the care team or at their agency may be a potential target for interventions aiming to improve the workforces’ experience on the job.
To our knowledge, this is the first study to evaluate HHAs’ perception of their own voice within the context of providing patient care at their home care agency. Historically, voice in the health care team has been studied in the context of other occupational groups like nursing. This is important because historically, despite providing day-to-day personal and medical care,23,24 HHAs have not been recognized as full members of a patient’s care team.25 For example, studies have found that HHAs are not part of systematic handoffs between care settings (eg, hospital to home), lack information at the beginning of a care episode (ie, patients’ medical history), and are not included in patients’ healthcare encounters at doctors’ offices, despite often taking them to these appointments.26 Prior literature, however, has been limited to qualitative or descriptive studies, and most data point to communication challenges whereby HHAs cannot reach their supervisor (nurse) or patients’ doctor when they have an issue in the home.5,6,11,12,14,25 Our study expands on this by quantitatively determining HHAs’ voice across several domains – ranging from having a say in the patients’ overall care to having suggestions listened to by higher ups. Additionally, we examine the association between voice and job satisfaction, an important outcome for this workforce which is currently amid a worker shortage and plagued by high turnover rates.8,27,28 Notably, like other studies, we found that a high proportion of HHAs reported high job satisfaction.29 This is not surprising as prior studies have found that despite challenging working conditions and low wages, HHAs’ cite a love for the job and providing care as a “calling.”5,30 We did find a strong association between higher voice and job satisfaction, though, signaling that having a say about their patients’ care is important to this workforce, and may be a lever for future interventions aiming to retain workers and grow the workforce. Future investigations are needed to examine the relationship between voice and worker outcomes like turnover.
It is important to note that a sizable proportion (37%) of the overall sample answered that 1 or more of the voice domains did not apply to them. And within the domains, “having a say about the quality of patient care” had the highest proportion of “does not apply to me” responses (28.6% of the total participants). There are a few possible explanations for these findings. One is that they are reflective of this workforces’ historical marginalization and lack of agency they hold within the medical team. It might not be apparent to them that they in fact could or should have a say about the overall quality of care of the patients for whom they are caring. Second is that the question may not be specific enough to their role such that HHAs felt they could answer. Regardless, this finding requires additional investigation at the HHA and agency level.
Implications
It has been well established that retention of HHAs’ is exceedingly difficult given the challenging working conditions, low-wages, and inequities that HHAs face both on the job and off. As noted previously, our findings highlight that voice is a potentially modifiable factor, either at the interpersonal or organizational level. Future research needs to be done to explore the mechanism underlying voice and job satisfaction in order to identify particular areas for change. At the organizational level, for example, there are programs that include HHAs’ in the medical team and approach patient care with an interdisciplinary-team-based approach where physicians and nurses rely on HHAs’ observations in the home to adjust patient care plans (Program for All-Inclusive Care for the Elderly – PACE).26 Other studies have found that training programs for HHAs to assist with monitoring health conditions and how to communicate with different members of the clinical care team improves HHAs’ confidence and ability to participate. Such programs ought to be expanded to other team members (ie nurses, physical therapists, physicians) such that they are primed and receptive to including and hearing from HHAs during home care episodes. Agencies and primary care clinics might also provide pathways for inclusion of HHAs and ways to promote their voice.31
The findings also speak to the potential role for technology, and specifically designing technology that could support the workforce as they provide care. For example, tools that could connect HHAs (ie “chat”) to their clinical supervisors or allow them to relay their observations in real time may result in HHAs feeling more integrated and supported on the job.27,28,31–33, Newer technology involving voice assistants, which have been piloted among older adults and are starting to be designed for HHAs, may offer another vehicle for this workforce to receive support.34,35
Finally, broader efforts to better integrate care provided in the home, by both paid and family caregivers, into the health system are warranted.36 Currently, there is no systematic way for HHAs to communicate their observations to patients’ medical doctors. This could be done through EHRs (ie, some home care agencies and hospitals are integrated, but many are not) and patient portals,37 which sometimes allow one family caregiver to communicate with the team, but not all the caregivers that are involved in the home.38 In HF, for example, while numerous remote monitoring devices exist for the patient, few have been designed with caregivers as the end-users in mind. That is, data that HHAs collect (daily weight and vital signs, assessing edema), could be better integrated into ambulatory care in actionable ways, which might improve HHAs’ perceived sense of voice and influence on patient care.
Limitations
We note a few limitations. First, although a large, diverse, and representative sample, participants were all union-affiliated and employed by licensed and certified home care agencies in New York, NY. Thus, while their experiences and working conditions may be similar to one another, they may not be wholly generalizable to non-unionized HHAs or those employed by other models or in non-urban or non-northeast areas; in fact recent data shows unionization rates for home health care services from 2010 to 2022 to be 26.2% in New York City as opposed to 7.5% nationwide.39 Second, we lack data on HHAs who did not open or complete the survey, which may introduce selection bias. Third, due to the cross-sectional nature of our data we cannot infer causality. Additionally, there may be residual confounding as we lack data on important covariates, including HHAs’ wages, take-home pay, and workload (ie, hours worked), which can influence both voice and job satisfaction.40 Finally, as noted, a proportion of HHAs were excluded from the main analysis because they did not perceive that voice applied to them. This is both an important research finding in and of itself, but also a limitation worth noting.
Conclusion
As the demand for HHAs increases in the US, there is a need to identify factors which can promote HHAs’ job satisfaction to keep them in the workforce and improve their experience caring for patients. HHAs’ having a voice, or say, with matters regarding patient care, is one such factor. We found that increased voice, both overall and across 5 domains, was significantly associated with higher job satisfaction among HHAs. These findings have implications for the home care industry and the healthcare system, suggesting that interventions targeted at promoting HHAs’ voice may help improve HHAs’ experience on the job, and potentially patient care. These interventions could include institutional re-organization of the outpatient health care team towards an interdisciplinary module inclusive of HHAs, changes in the EHR to involve observations from HHAs, and providing HHAs with technological support to easily access other members of the health care team.
Acknowledgments
We would like to thank the staff at 1199SEIU Training and Employment Fund for their assistance administering the survey. We would also like to thank Cisco Espinosa and Yefrenia Henriquez Taveras for their assistance in preparing and submitting the manuscript.
Funding
National Heart, Lung, and Blood Institute, Grant K23HL150160 (PI: Sterling). Research reported in this publication was supported by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002384 and by the National Science Foundation under Award Number 2026577. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. U.S. Bureau of Labor Statistics. Employment Projections: 2019-2029 Summary. Available from: https://www.bls.gov/news.release/ecopro.nr0.htm.
2. U.S. Bureau of Labor HomeStatistics. Home health aides and personal care aides: occupational Outlook Handbook. U.S. Bureau of Labor Statistics. Available from: https://www.bls.gov/ooh/healthcare/home-health-aides-and-personal-care-aides.htm.
3. PHI. U.S. Home care workers: key facts. PHI; 2019. https://phinational.org/resource/u-s-home-care-workers-key-facts-2019/.
4. Ortman JM, Velkoff VA, Hogan H. Projections of the Size and Composition of the U.S. Population: 2014 to 2060. U.S. Census Bureau; 2014. Available from: https://www.census.gov/library/publications/2015/demo/p25-1143.html.
5. Sterling MR, Silva AF, Leung PBK, et al. “It’s like they forget that the word ‘health’ is in ‘home health aide’”: understanding the perspectives of home care workers who care for adults with heart failure. J Am Heart Assoc. 2018;7(23):e010134. doi:10.1161/jaha.118.010134
6. Sterling MR, Dell N, Piantella B, et al. Understanding the workflow of home health care for patients with heart failure: challenges and opportunities. J Gen Intern Med. 2020;35(6):1721–1729. doi:10.1007/s11606-020-05675-8
7. Sterling MR, Tseng E, Poon A, et al. Experiences of home health care workers in New York City During the coronavirus disease 2019 pandemic: a qualitative analysis. JAMA Intern Med. 2020;180(11):1453–1459. doi:10.1001/jamainternmed.2020.3930
8. Krebs N. A shortage of health aides is forcing out those who wish to get care at home. NPR; 2022. Available from: https://www.npr.org/sections/health-shots/2022/05/05/1095050780/a-shortage-of-health-aides-is-forcing-out-those-who-wish-to-get-care-at-home.
9. Cheney C, Home Health Aides Undervalued in U.S. Healthcare system. Healthleaders; 2022. Available from: https://www.healthleadersmedia.com/clinical-care/home-health-aides-undervalued-us-healthcare-system.
10. Franzosa E, Wyte-Lake T, Tsui EK, Reckrey JM, Sterling MR. Essential but excluded: building disaster preparedness capacity for home health care workers and home care agencies. J Am Med Dir Assoc. 2022;23(12):1990–1996. doi:10.1016/j.jamda.2022.09.012
11. Franzosa E, Tsui EK, Baron S. Who’s Caring for Us?”: Understanding and addressing the effects of emotional labor on home health aides’ well-being. Gerontologist. 2019;59(6):1055–1064. doi:10.1093/geront/gny099
12. Franzosa E, Tsui EK, Baron S. Home health aides’ perceptions of quality care: goals, challenges, and implications for a rapidly changing industry. NEW Solut J Environ Occup Health Policy. 2018;27(4):629–647. doi:10.1177/1048291117740818
13. Feldman PH, Ryvicker M, Evans LM, Barron Y. The homecare aide workforce initiative: implementation and outcomes. J Appl Gerontol. 2019;38(2):253–276. doi:10.1177/0733464817707298
14. Faul AC, Schapmire TJ, D’Ambrosio J, Feaster D, Oak CS, Farley A. Promoting sustainability in frontline home care aides: understanding factors affecting job retention in the home care workforce. Home Health Care Manag Pract. 2010;22:408–416. doi:10.1177/1084822309348896
15. Zarska A, Avgar AC, Sterling MR. Relationship between working conditions, worker outcomes, and patient care: a theoretical model for frontline health care workers. Am J Med Qual off J Am Coll Med Qual. 2021;36(6):429–440. doi:10.1097/01.JMQ.0000735508.08292.73
16. Sterling MR, Kern LM, Safford MM, et al. Home health care use and post-discharge outcomes after heart failure hospitalizations. JACC Heart Fail. 2020;8(12):1038–1049. doi:10.1016/j.jchf.2020.06.009
17. 1199SEIU Home Care Industry Education Fund. About Us. 1199SEIU home care industry education fund. Available from: https://www.1199seiuhomecareed.org/about/.
18. Clark PF, Clark DA, Day DV, Shea DG. Healthcare reform and the workplace experience of nurses: implications for patient care and union organizing. Ind Labor Relat Rev. 2001;55(1):133–148. doi:10.1177/001979390105500108
19. Wilkinson A, Avgar A, Barry M, Mowbray P. Voice bundles in healthcare: the reciprocal relationship between worker and patient-focused voice. In: Wilkinson A, Donaghey J, Dundon T, Freeman RB, editors. Handbook of Research on Employee Voice. Cheltenham: Edward Elgar; 2020:556–565. doi:10.4337/9781788971188.00042
20. Avgar AC, Sadler JA, Clark P, Chung W. Labor-management partnership and employee voice: evidence from the healthcare setting. Ind Relat. 2016;55:576–603. doi:10.1111/irel.12152
21. Bérubé N, Donia M, Gagné M, Houlfort N, Lvina E. Validation evidence for the work domain satisfaction scale in two languages. Int J Psychol Stud. 2016;8(3):26. doi:10.5539/ijps.v8n3p26
22. Gherman MA, Arhiri L, Holman AC, Soponaru C. The moral impact of the COVID-19 pandemic on nurses’ burnout, work satisfaction and adaptive work performance: the role of autobiographical memories of potentially morally injurious events and basic psychological needs. Int J Environ Res Public Health. 2022;19(13):7645. PMID: 35805304; PMCID: PMC9266140. doi:10.3390/ijerph19137645
23. Reckrey JM, Tsui EK, Morrison SR, et al. Beyond functional support: the range of health-related tasks performed in the home by paid caregivers in New York. Health Aff Proj Hope. 2019;38(6):927–933. doi:10.1377/hlthaff.2019.00004
24. Sterling MR, Ringel JB, Cho J, Riffin CA, Avgar AC. Utilization, contributions, and perceptions of paid home care workers among households in New York State. Innov Aging. 2022;6(2):igac001. doi:10.1093/geroni/igac001
25. Lai D, Cloyes KG, Clayton MF, et al. We’re the eyes and the ears, but we don’t have a voice: perspectives of hospice aides. J Hosp Palliat Nurs JHPN off J Hosp Palliat Nurses Assoc. 2018;20(1):47–54. doi:10.1097/NJH.0000000000000407
26. Sterling M, Ringel J, Riegle B, et al. Scope of Home health care workers’ interactions with medical providers, their home care agencies, and family members for their patients with heart failure. J Am Board Fam Med. 2023;36(2):369–375. doi:10.3122/jabfm.2022.220204R2
27. Chapman SA, Greiman L, Bates T, et al. Personal care aides: assessing self-care needs and worker shortages in rural areas. Health Aff Proj Hope. 2022;41(10):1403–1412. doi:10.1377/hlthaff.2022.00483
28. Shaw AL, Ringel JB, Avgar AC, Riffin CA, Kallas J, Sterling MR. Addressing the home care shortage: predictors of willingness to provide paid home care in New York. J Am Med Dir Assoc. 2022;23(10):1621–1626.e1. doi:10.1016/j.jamda.2022.07.006
29. Bercovitz A, Jones A, Harris-Kojetin LD, Squillace MR. An overview of home health aides: United States, 2007; 2011:32.
30. Hewko SJ, Cooper SL, Huynh H, et al. Invisible no more: a scoping review of the health care aide workforce literature. BMC Nurs. 2015;14(1):38. doi:10.1186/s12912-015-0090-x
31. Stone RI, Bryant NS. The future of the home care workforce: training and supporting aides as members of home-based care teams. J Am Geriatr Soc. 2019;67(S2):S444–S448. doi:10.1111/jgs.15846
32. HHAeXchange. Purpose-built technology for providers, MCOs, and state Medicaid programs (Mobile App); 2022. Available from: https://www.hhaexchange.com.
33. HHAeXchange. CareConnect (Mobile App); 2022. Available from: https://www.hhaexchange.com/partner-connect/careconnect.
34. Bartle V, Lyu J, El Shabazz-Thompson F, et al. “A Second Voice”: investigating Opportunities and Challenges for Interactive Voice Assistants to Support Home Health Aides. In:
35. O’Brien K, Liggett A, Ramirez-Zohfeld V, Sunkara P, Lindquist LA. Voice-controlled intelligent personal assistants to support aging in place. J Am Geriatr Soc. 2020;68(1):176–179. doi:10.1111/jgs.16217
36. Sterling MR, Shaw AL. Sharing the care—a patient and her caregivers. JAMA Intern Med. 2019;179(12):1617–1618. doi:10.1001/jamainternmed.2019.4231
37. Portz JD, Bayliss EA, Bull S, et al. Using the technology acceptance model to explore user experience, intent to use, and use behavior of a patient portal among older adults with multiple chronic conditions: descriptive qualitative study. J Med Internet Res. 2019;21(4):e11604. doi:10.2196/11604
38. Riffin C, Griffin JM, Brody L, et al. Engaging and supporting care partners of persons with dementia in health-care delivery: results from a national consensus conference. Public Policy Aging Rep. 2022;32(2):58–65. doi:10.1093/ppar/prac004
39. Milkman R, Van Der Naald J. The State of the Unions 2022: a Profile of Organized Labor in New York City, New York State, and the United States. CUNY Graduate Center; 2022. Available from: https://slu.cuny.edu/wp-content/uploads/2022/09/Union_Density-2022_D42.pdf.
40. Carvajal M, Popovici I, Hardigan P. Gender and pharmacists’ career satisfaction in the United States. Pharm Special Issue Pharmacist Job Satisf. 2021;9(4):173.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.