Back to Journals » Orthopedic Research and Reviews » Volume 15
Hallux Valgus Interphalangeus with Large Ossicle Formation: A Case Report
Authors Primadhi RA ![]() , Aditya R, Hidajat NN
, Aditya R, Hidajat NN
Received 17 November 2022
Accepted for publication 8 February 2023
Published 23 February 2023 Volume 2023:15 Pages 13—17
DOI https://doi.org/10.2147/ORR.S395950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Raden Andri Primadhi, Rio Aditya, Nucki Nursjamsi Hidajat
Department of Orthopaedics and Traumatology, Universitas Padjadjaran Medical School / Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Raden Andri Primadhi, Department of Orthopaedics and Traumatology, Universitas Padjadjaran Medical School / Hasan Sadikin Hospital, Jalan Pasteur 38, Bandung, 40161, Indonesia, Tel/Fax +62 22 2035477, Email [email protected]
Abstract: Hallux valgus interphalangeus (HVIP) is a deviation of the distal phalanx in relation to the proximal phalanx. Its etiology is considered multifactorial, including growth development disturbances, external pressure, and biomechanical alteration involving the interphalangeal joint. Here, we report a case of HVIP with the presence of a large ossicle at the lateral side, which was considered related to HVIP development. A 21-year-old woman presented HVIP that had developed since childhood. She complained of pain in her right great toe that worsened in the previous several months, particularly when walking and wearing shoes. Surgical correction consisted of Akin osteotomy, fixation with headless screw, ossicle excision, and medial capsulorrhaphy. The interphalangeal joint angle was improved from 28.69⁰ pre-operatively to 8.93⁰ post-operatively. The wound healed uneventfully and the patient was satisfied. Akin osteotomy with concomitant ossicle excision was effective in this case. Gaining more knowledge regarding ossicles around the foot will provide a better understanding of deformity correction, especially from the biomechanical standpoint.
Keywords: hallux valgus, interphalangeal, ossicle, sesamoid bones
Introduction
Hallux valgus interphalangeus (HVIP) is a great toe deformity that can be seen as a lateral deviation of the distal phalanx in relation to the proximal phalanx. This deformity was first introduced by Daw nearly a century ago.1,2 Although HVIP is thought to be associated with hallux valgus or its corrective surgeries, HVIP is reportedly more common in normal feet than in hallux valgus feet. The hallux interphalangeal angle itself was also negatively correlated with the hallux valgus angle and intermetatarsal angle.3,4
The etiology of HVIP is likely multifactorial, including developmental and growth plate abnormalities of the distal toe, and external pressure resulting from shoe wear and mechanical force during the push-off phase.1,5 Parker et al reported HVIP in a patient who had a mutation in the Homeobox A Cluster 13 (HOXA13) gene which is known to be responsible for the development of hand-foot-genital syndrome.6 Previous studies had reported that the presence of ossicle or osteochondral fragment at the lateral side was associated with HVIP. Both bony fragments may cause HVIP when considering its proximity to the lateral collateral ligament or joint capsule, thus producing valgus deformity mechanically. However, an osteochondral lesion can also be formed secondary to the existing HVIP, as the lateral vascularity is disturbed and repetitive trauma occurs.1
HVIP by itself is rarely symptomatic, other than causing a cosmetic concern. However, pain resulted from HVIP may lead to painful motion of the joint or difficulty in daily joint activity. Pain occurs when the second toe is impinged by the great toe and distal phalanx.5 Initial management should be conservative, typically in patients presenting with painless and non-progressive deformities. Surgical intervention is necessary only when the problem persists. The objective of surgery is to realign the great toe clinically and relieve the pressure on the second toe. Proximal phalanx medial closing wedge osteotomy was introduced by Akin in 1925 and is still used in combination with other additional correction procedures.5,7 Fixation after correction can be done with various hardware including k-wire, screw, plate and screws, or bone staples. In case of percutaneous surgery, fixation might not be needed.
We report here a rare case of HVIP with accompanying ossicle at the lateral side of the great toes. Preoperative characteristics, intraoperative findings, and postoperative results are presented with the corresponding literature review.
Case Presentation
A 21-year-old, generally healthy woman presented to the foot and ankle clinic with concerns of pain at her right great toe. There was a valgus deformity of interphalangeal joints (Figure 1) that was present since her childhood. Recently, the patient felt pain at the medial side of her right great toe especially during walking and wearing shoes. We found tenderness at the medial aspect of the interphalangeal joint, with decreased range of motion. Plain radiograph showed 28.69⁰ lateral deviation of the right interphalangeal joint as well as the presence of a large ossicle (Figure 2).
 |
Figure 1 Hallux valgus interphalangeal deformity. |
 |
Figure 2 Lateral deviation of great toe interphalangeal joint as much as 28.69⁰ with the presence of an ossicle in lateral side. |
Surgical correction was done using Akin osteotomy and ossicle excision (Figure 3). The patient was operated under regional anesthesia in the supine position. Longitudinal incision was made on the medial side, deepened through the joint capsule to expose the osteotomy site. The guide wire was placed under an image intensifier visualization prior to the osteotomy. Medial closing wedge osteotomy was performed and fixed by a 3.2-mm diameter headless dual compression cannulated screw (Normed Medizin-Technik GmbH, Germany). After osteotomy, the ossicle and covering bursa at the lateral side was removed. Lateral capsule release and medial capsule imbrication were subsequently performed. Post-operative standard dressing was applied with particular spacing between the great toe and second toe. The patient was allowed to partially bear weight using a post-operative rocker bottom footwear. The post-operative interphalangeal joint angle was 8.93° (Figure 4). The surgical wound healed uneventfully.
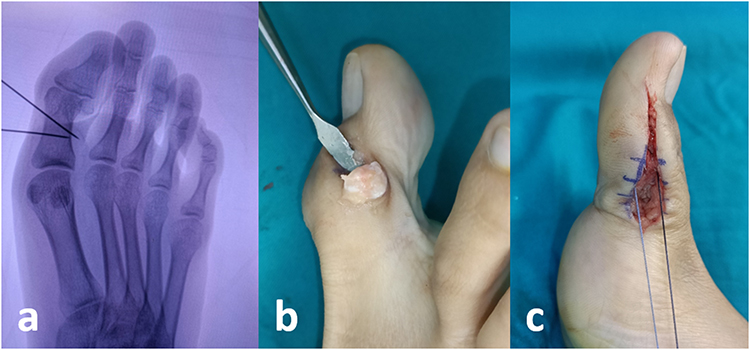 |
Figure 3 (a) Akin osteotomy design, (b) ossicle removal, and (c) medial capsulorrhaphy. |
 |
Figure 4 Post operative result depicting 8.93⁰ interphalangeal joint angle. |
This case report was registered and approved by the institutional review board of Hasan Sadikin Hospital, Bandung, Indonesia, No. LB.02.02/X.6.5/479/2022. The patient provided informed consent to publish their case details and any accompanying images.
Discussion
Ossicles, or specifically accessory ossicles, are supernumerary bones that originate from unfused primary or secondary ossification centers and may be unilateral or bilateral.8,9 Other than being derived from a failure of union, ossicles may result from a prior osteochondral fracture.10 They are considered normal variants but can also be associated with a particular pathological condition. Sesamoid bones are identical osseous structures, but differently there are embedded in tendons, either partially or completely.9 Os interphalangeus is one of the sesamoid bones of the great toe of the interphalangeal joint that is traditionally located at the plantar aspect, but rarely may be dorsal to the interphalangeal joint.11,12 Its prevalence has been reported variably at 2–13% in its ossified form.9 Os interphalangeus may be centrally or eccentrically located in the joint capsule and separated from the tendon by a bursa, thus considered an ossicle.12 Although it may alter the biomechanics of the joint and limit joint motion, there are limited report on the clinical significance of os interphalangeus other than its interposition into a dislocated hallucal interphalangeal joint, making it irreducible.9,13 Typically, HVIP is asymptomatic, but it can become symptomatic in some cases because of undue pressure, overuse, or trauma.14 It is difficult to distinguish the clinically irrelevant bones and the truly symptomatic ones.9
In our patient, HVIP had developed since childhood. Considering the absence of trauma history, the ossicle found at the lateral great toe may have previously been an osteochondral fragment resulting from a longstanding vascular disruption or the repetitive stress at the lateral side of the great toe may have caused the HVIP deformity itself; however, this could not be verified due to the lack of prior radiographs. This point of view is similar to a case reported by Kubo et al, wherein a small osteochondral fragment was formed at the lateral aspect of the great toe’s interphalangeal joint.1 In another report, Shimizu et al suggested that the non-union osteochondral fracture in the lateral head of the proximal phalanx was a cause of HVIP. In such cases, the lateral collateral ligament is affected by the displacement, thus resulting in lateral joint instability and HVIP development.15 Conversely, the presence of a large ossicle at the lateral side may pull the collateral ligament or capsule lateralward and likely be an etiological factor for HVIP development.
HVIP is diagnosed radiologically when the HVI angle (HVIA) is >10°. The objective of surgery is to realign the toe clinically and correct the HVIA to neutral.5 The HVIP deformity apex is at the interphalangeal joint.5 Akin osteotomy, a medial wedge closing osteotomy, was done using medial incision from the level of the first metatarsophalangeal (MTP) joint to 1–2-mm distal to the midpoint of the proximal phalanx diaphysis. The first limb of the osteotomy was conducted parallel to the MTP joint surface using a micro sagittal saw. The second distal limb of the osteotomy was carried out 1–3 mm to the first, aiming to meet the first cut at the lateral cortex.16 Image intensifier was used to determine the amount of bony resection. After correction, double compression headless bone screw was used for fixation. This type of screw allows for optimal reduction and safe fixation due to the cannulation, other than providing additional compression.17
The hallux interphalangeal joint is considered more stable in the transverse plane than the metatarsophalangeal joint, not only because of its firm collateral ligaments and joint capsule but also because of the bicondylar shape of the joint, the short lever arm of the distal phalanx, and its thickened fibrocartilaginous plantar plate.18 Shimizu et al attempted to fix the osteochondral fragment associated with HVIP in his previous report, owing to the instability at the fracture site that affected the interphalangeal joint.15 In this patient, we decided to remove the ossicle prior to osteotomy through an additional lateral incision by concomitantly releasing the lateral capsule and collateral ligament to facilitate realignment of the valgus joint, similar to lateral capsulotomy in hallux valgus surgery.
Conclusion
While HVIP is not uncommon, the presence of interphalangeal ossicles accompanying it is rarely reported. Gaining more knowledge regarding ossicles around the foot will provide a better understanding of the underlying pathology and deformity correction strategies, especially from the biomechanical standpoint. However, further studies are needed to better figure out the biomechanical significance of ossicles.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kubo M, Miyamoto W, Takao M, Yasui Y, Innami K, Matsushita T. Valgus deformity of the great toe interphalangeal joint treated by reversed sliding osteotomy of the proximal phalanx: a case report. Foot Ankle Int. 2011;32:448–451. doi:10.3113/FAI.2011.0448
2. Daw SW. An unusual type of hallux valgus (two cases). Br Med J. 1935;2:580.
3. Sorto JL, Balding MG, Weil LS, Smith SD. Hallux abductus interphalangeus: etiology, x-ray evaluation and treatment. J Am Podiatry Assoc. 1976;66:384–396. doi:10.7547/87507315-66-6-384
4. Park J-Y, Jung H-G, Kim T-H, Kang M-S. Intraoperative incidence of hallux valgus interphalangeus following basilar first metatarsal osteotomy and distal soft tissue realignment. Foot Ankle Int. 2011;32:1058–1062. doi:10.3113/FAI.2011.1058
5. Griend RV. Correction of hallux valgus interphalangeus with an osteotomy of the distal end of the proximal phalanx (Distal Akin Osteotomy). Foot Ankle Int. 2017;38:153–158. doi:10.1177/1071100716670389
6. Parker L, Mangwani J, Wakeling E, Singh D. Hallux valgus interphalangeus and a novel mutation in HOXA13. Part of the broadening spectrum of Hand-Foot-Genital syndrome. Foot Ankle Surg. 2011;17:e28–30. doi:10.1016/j.fas.2010.12.003
7. AKin O. The treatment of hallux valgus: a new operative procedure and its results. Med Sentin. 1925;33:678–679.
8. Keles-Celik N, Kose O, Sekerci R, Aytac G, Turan A, Guler F. Accessory ossicles of the foot and ankle: disorders and a review of the literature. Cureus. 2017;9:e1881. doi:10.7759/cureus.1881
9. Nwawka OK, Hayashi D, Diaz LE, et al. Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology. Insights Imaging. 2013;4:581–593. doi:10.1007/s13244-013-0277-1
10. Ferran J, Blanc T. Os subfibulare in children secondary to an osteochondral fracture. J Radiol. 2001;82:577–579.
11. Candan B, Torun E, Dikici R. The prevalence of accessory ossicles, sesamoid bones, and biphalangism of the foot and ankle: a radiographic study. Foot Ankle Orthop. 2022;7:1–10. doi:10.1177/24730114211068792
12. Mateen S, Kwaadu KY, Ali S. Diagnosis, imaging, and potential morbidities of the hallux interphalangeal joint os interphalangeus. Skeletal Radiol. 2022;51:1143–1151. doi:10.1007/s00256-021-03946-x
13. Roukis TS, Hurless JS. The hallucal interphalangeal sesamoid. J Foot Ankle Surg. 1996;35:303–308. doi:10.1016/S1067-2516(96)80078-0
14. Shin HY, Park SY, Kim HY, Jung YS, An S, Kang DH. Symptomatic hallucal interphalangeal sesamoid bones successfully treated with ultrasound-guided injection – a case report. Korean J Pain. 2013;26:173–176. doi:10.3344/kjp.2013.26.2.173
15. Shimizu A, Watanabe S, Kamada K, Tsuboi I, Yamamoto H. Hallux valgus interphalangeus following osteochondral fracture of the proximal phalanx: a case report. Foot Ankle Int. 2005;26:994–996. doi:10.1177/107110070502601116
16. Neumann JA, Reay KD, Bradley KE, Parekh SG. Staple fixation for akin proximal phalangeal osteotomy in the treatment of Hallux Valgus interphalangeus. Foot Ankle Int. 2015;36:457–464. doi:10.1177/1071100714559072
17. Goksel F, Ermutlu C, Golge UH, Kaymaz B. Treatment of juvenile hallux valgus interphalangeus with a double compression headless bone screw. BMJ Case Rep. 2015;4:bcr2015210204. doi:10.1136/bcr-2015-210204
18. Gong HS, Kim YH, Park MS. Varus instability of the hallux interphalangeal joint in a taekwondo athlete. Br J Sports Med. 2007;41:917–919. doi:10.1136/bjsm.2007.035501
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.