Back to Journals » Drug Design, Development and Therapy » Volume 18
Guidelines for Rational Clinical Use of Fentanyl Transdermal Patch
Authors Fu Q ![]() , Han N, Li N, Gui L, Shi C, Rong P, Zeng F, Rao H, Chen Y
, Han N, Li N, Gui L, Shi C, Rong P, Zeng F, Rao H, Chen Y
Received 26 March 2023
Accepted for publication 11 January 2024
Published 1 February 2024 Volume 2024:18 Pages 233—255
DOI https://doi.org/10.2147/DDDT.S414318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Video abstract of “Guidelines for clinical use of fentanyl transdermal patch” [414318].
Views: 1774
Qiang Fu,1 Na Han,1 Na Li,2 Ling Gui,3 Chen Shi,4 Peipei Rong,5 Fan Zeng,1 He Rao,6 Yuan Chen1 On behalf of Cancer Rehabilitation and Palliative Treatment Professional Committee of Hubei Anti Cancer Association
1Department of Oncology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430030, People’s Republic of China; 2Cancer Center, Renmin Hospital of Wuhan University, Wuhan, Hubei, 430060, People’s Republic of China; 3Department of Pharmacy, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430030, People’s Republic of China; 4Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 5Department of Pharmacy, Renmin Hospital of Wuhan University, Wuhan, Hubei, 430060, People’s Republic of China; 6Department of Oncology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, 430071, People’s Republic of China
Correspondence: Qiang Fu; Yuan Chen, Department of Oncology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1095 Jiefang Avenue, Qiaokou District, Wuhan, Hubei, 430030, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Pain is one of the most common clinical symptoms of cancer patients, seriously affecting the quality of life of patients and bringing heavy mental and economic burden to families and society. The treatment of cancer pain in China is facing numerous challenges, one of which includes the irrational usage of analgesic drugs in clinical practice. As a strong opioid analgesic, transdermal fentanyl patch has been widely used due to its convenient clinical application and obvious therapeutic effect. Several basic-level hospitals and even general hospitals in China fail to appropriate the application of drugs in clinical application due to the lack of understanding of the pharmacological characteristics and clinical application of fentanyl transdermal patch by medical staff, seriously affecting the treatment quality. Therefore, it is imperative to strengthen the rational use and management of fentanyl transdermal patches. Accordingly, the initiation by the Cancer Rehabilitation and Palliative Treatment Professional Committee of the Hubei Anti-cancer Association launched the compilation of the “Guidelines for Rational Clinical Use of Fentanyl Transdermal Patch” (from now on referred to as the “Guidelines”) in Hubei Province, China. The experts in the preparation group are experts in many disciplines, such as medicine, pharmacy, and nursing. The expert group determines the outline, prepares the required regulations, and revises it repeatedly. Moreover, these experts put forward suggestions for revision to strictly control the accuracy and scientific authenticity of the contents of the “Guide”. Finally, all experts of the preparation team certify and finalize the draft. This “Guide” prepared by experts of the Cancer Rehabilitation and Palliative Treatment Professional Committee of the Hubei Anti-cancer Association and the expert advisory group with joint efforts, aims to play a positive role in promoting the rational clinical use of fentanyl transdermal patch, reducing the mental and economic burden of patients, and ensuring medical quality and medical safety.
Keywords: fentanyl transdermal patch, reasonable application, medication guidelines
Introduction
The transdermal fentanyl patch was listed in the United States-Food Drug Administration in 1990 and approved for listing in China in 1999. The transdermal fentanyl patch offers the characteristics of a stable drug release rate, action time of up to 72 hours, and convenient use, among others. In addition, it has become one of the most widely used cancer analgesics in clinical application. According to the WHO Guidelines for the Administration of Drugs and Radiotherapy for Cancer Pain for Adults and Adolescents in 2018, fentanyl transdermal patch was a commonly used strong opioid analgesic for cancer pain,1 including in the WHO list of essential drugs in 2019.2
With the increasing incidence rate of cancer cases, the demand for cancer pain treatment has subsequently increased, leading to the long-term and extensive use of opioids. Accordingly, the rational use of fentanyl transdermal patches (indications, correct use, and treatment of adverse reactions) has become increasingly prominent.3 Along this line, patients (~50%) receiving fentanyl treatment in the world have inappropriate prescription indications, as some countries in North America and Europe have even seen fentanyl abuse.4 Nevertheless, there is a serious shortage of opioids used by cancer pain patients in China.
Currently, the clinical diagnosis and treatment guidelines, expert consensus, or guiding principles mostly describe the application of fentanyl transdermal patches from the perspective of disease treatment. The reasonable use, pharmaceutical care, and management of fentanyl transdermal patches are relatively lacking. Owing to these aspects, the guideline formulation working group focused on consulting a large number of authoritative documents for the pharmaceutical care of fentanyl transdermal patch, including clinical use regulations, medication scheme, route of administration, mode of administration, frequency and time of administration, specific population medication, drug interactions, preparation and preservation, as well as safety. Combined with the experience of multi-specialist physicians, pharmacists, nurses, and drug economists, and referring to the wishes of patients, pharmacists and nurses provide a comprehensive proposal on rational clinical application of fentanyl transdermal patch. In this regard, a view has been proposed to play an active role in promoting rational clinical drug use, reducing the mental and economic burden of patients, ensuring medical quality, and improving medical safety in clinical work. By a Delphi method, we selected the consulted documents and ranked 4 stars in the STAR group to provide comprehensive guidelines, promoting rational clinical drug use and improving medical safety.
Evidence Category and Recommendation Level in the Diagnosis and Treatment Guidelines of the Chinese Society of Clinical Oncology
The guidelines are based on evidence-based medicine, classifying the quality of evidence and the recommended levels according to the evidence category in the diagnosis and treatment guidelines of the Chinese Society of Clinical Oncology (CSCO).5 Accordingly, the evidence levels are broadly divided into 1A, 1B, 2A, 2B, and 3. In addition, the recommendation levels are divided into Level I, Level II, and Level III recommendations. Firstly, the scheme with a high evidence category and good accessibility is recommended as Level I. Secondly, the scheme with a high evidence category, low expert consensus, or poor accessibility is recommended as Level II. In the clinically practical cases but not the high evidence category, it is recommended as Level III. (Tables 1 and 2). It should be noted that the consensus degree of this guide is obtained through statistical analysis in the form of expert voting after finalizing the guide.
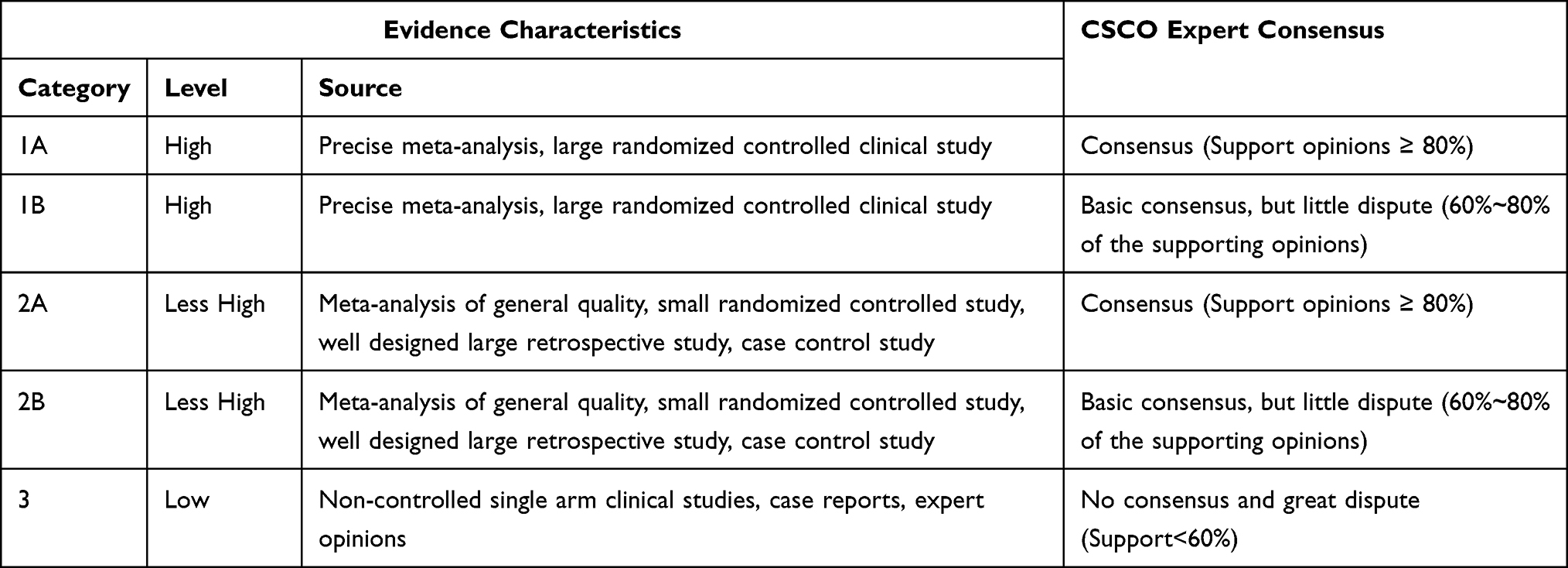 |
Table 1 A Classification Presents the Evidence Category of CSCO Diagnosis and Treatment Guidelines |
 |
Table 2 A Summary of Recommended Levels of CSCO Diagnosis and Treatment Guidelines |
Clinical Pharmacology
In this section, we present the clinical pharmacological views of the Fentanyl. The chemical formula of Fentanyl is N-[1-(2-phenylethyl)-4-piperidinyl]-N-phenyl-propanamide, with the molecular weight of 336.46. Due to its small molecular weight, high-fat solubility, and low skin irritation, this drug can be formulated into transdermal drug delivery preparations. The transdermal delivery systems offer high comfort to the patients along with several characteristics of low irritation, low sensitization, good viscosity, softness, and easy peeling. Simultaneously, this percutaneous drug delivery eliminates the first-pass effect of the liver, greatly improving the bioavailability of drugs. Currently, there are two types of fentanyl transdermal patches in clinics, ie, skeleton and reservoir types. The reservoir type of fentanyl transdermal patch consists of four layers: coating layer, drug storage tank, controlled release film, and adhesive layer. The drug storage system in the reservoir-type combines fentanyl, ethanol, and hydroxyethyl cellulose, in which ethanol acts as a transdermal absorption enhancer for fentanyl. In addition, the polyester film acts as a backing film, in which the ethylene vinyl acetate copolymer controls the fentanyl release. The outer layer of the controlled release film referred to as a polysiloxane pressure-sensitive adhesive, is protected with a film made of silicified paper. The properties of controlled-release membranes substantially control the release rate of fentanyl. To this end, he skeleton-type fentanyl transdermal patches are designed to dissolve fentanyl in a self-adhesive acrylic polymer. The colloid containing fentanyl is covered by a polypropylene protective film, in which waterproof properties attain the drug backing. The layer applied to the skin surface is an acrylic polymer, which can control the release of active ingredients. The colloid is covered by an anti-stick layer, which must be removed before using it.
In 2009, it was reported that the reservoir-type fentanyl transdermal patch possessed the risk of internal drug leakage to the outside of the package, which was recalled by the FDA and related manufacturers.6 Since then, the reservoir-type fentanyl transdermal patch has been improved to the skeleton-type fentanyl transdermal patch, with the structure of coating and drug-containing skeleton-type adhesive layer (Figure 1). The skeleton transdermal fentanyl patch is a controlled-release transdermal delivery formulation containing fentanyl prepared by modern pressure-sensitive adhesive technology to ensure that the drug can enter the blood circulation system through the skin at a constant rate, offering a lasting and stable analgesic role in the whole body. Notably, the area of the skeleton-type transdermal fentanyl patch is 1/2 smaller than that of the reservoir type. Moreover, the skeleton type has better adhesion and elongation with the skin, lesser irritation to the local skin, faster absorption, no drug burst risk, and higher safety over the reservoir type.7
 |
Figure 1 Images show the two formulations of fentanyl transdermal patch, (A) Skeleton, and (B) Reservoir types. |
Action Mechanism
As a synthetic pure opioid receptor agonist, fentanyl offers similar pharmacological effects to morphine and other opioid drugs, mainly acting on μ Opioid receptor,8 producing a stronger central analgesic effect and faster onset time of action (100-fold) than morphine. Fentanyl binding μ-Opioid receptor (μ-OR) activates the downstream G-protein coupled signaling pathway to exert analgesic effects. Compared to morphine, fentanyl possesses a more significant effect on TM2 and TM3. The outer side of μ-OR containing cells occupies an additional binding pocket. The side chains of the fentanyl aniline ring form π-π hydrophobic interactions with residues W295 and Y328. The interaction time of fentanyl and μ-OR is relatively long, along with a higher (50–100 times) potency of fentanyl than morphine.9
Pharmacokinetics
Typically, the release rate of fentanyl from the transdermal patch remained relatively constant. In the case of the first application of the patch, the serum concentration of fentanyl gradually increases, reaching the effective concentration in 6–12 hours and a steady state concentration in 12–24 hours, and then remaining relatively stable to 72 hours. Accordingly, the peak time is generally considered to be 24–72 hours after the first use. Considering the pharmacokinetics, the serum concentration of fentanyl is in direct proportion to the size (dose) of the patch. The stable serum concentration of fentanyl that the patient can reach depends on the skin permeability and clearance rate of the individual. Moreover, it has been observed that there exists an individual difference in the serum concentration of fentanyl, indicating that an increasing skin temperature can increase drug absorption. Furthermore, the analgesic and other potential therapeutic effects of fentanyl are influenced by various factors, such as patient age, sensitivity, medication regimen, and disease status. In an instance, Thompson et al10 showed that the increase rate of blood drug concentration in elderly patients (aged 64–82) was significantly slower than that in young patients (aged 25–38). In another instance, Collins et al11 showed that the peak time was 18–66 hours in children administered with 25 μg/h patch, and the average clearance rate and distribution volume were similar to those of these adults. Fentanyl could rapidly and extensively be metabolized by cytochrome P-450 family metabolic enzymes (CYP3A4) in the liver without skin metabolism, resulting in the main metabolite of inactive norfentanyl. After removing the patch for 24 hours, the concentration of fentanyl in the serum gradually decreased to about 50% after 17 hours (range: 13–22 hours). These results indicated that the fentanyl continued to be released into the blood from the skin after drug withdrawal. The serum concentration decreased more slowly than that of intravenous injection. Notably, fentanyl is inactivated by liver metabolism, and its biological half-life is 2–4 hours. Approximately 75% of fentanyl is mainly excreted in urine in the form of inactive metabolite within 24 hours. The prototype drug in urine is less than 10%, and about 9% of fentanyl is excreted in feces in the form of metabolite.
Absorption and Distribution
The fentanyl from the transdermal patch is often absorbed through the skin and enters the bloodstream. The plasma protein binding rate is around 84%, with a large steady-state volume distribution, large tissue/blood gas distribution coefficient, fast tissue uptake and storage, and short onset time. Notably, the release rate of fentanyl is often limited by its skin permeability. The blood drug concentration during transdermal drug delivery is related to the following sequential steps: release of the drug from the transdermal drug delivery system, epidermal diffusion of the drug, movement within the vascular dermis, diffusion within the vascular system, movement of the drug from the blood vessels to the central chamber, and drug clearance.12 Recent literature indicated that fentanyl transdermal patches had been subjected to various animal experiments,13 indicating an average steady-state concentration of 1.6 ng/mL in dogs.14 In a case, Egger et al15 measured that the average blood concentration of 8 anesthetized cats with a body weight of 2.3–4.3 kg was 2.6, 4.1, 2.4, and 1.6 ng/mL at 8, 25, 49, and 73 hours after administration was lower than the blood concentration values of animals under anesthesia. The maximum concentration of fentanyl in the intestinal wall, liver, and muscles slightly lags behind that of well-perfused tissues. In contrast, the maximum concentration of fat appeared about 30 minutes after injection.16,17 The concentration-time curve of its three human bodies was best expressed in the three-compartment model, with a half-life of 1.7 minutes in the fast distribution phase, 13 minutes in the slow distribution phase, and 219 minutes in the end clearance phase. Owing to its weakly alkaline nature, fentanyl existed in both ionized and non-ionized forms in physiological pH environments.18
Within the brain, fentanyl binding to receptors depends on the affinity between the drug and the receptor, as well as the degree of binding to non-receptor sites. Fentanyl from the transdermal patch penetrates into the skin through special micropores and is absorbed by capillaries, with an absorption rate of 92% to 94%. Further, the blood concentration of absorbed fentanyl remains relatively stable 12–24 hours after administration, reaching its peak concentration about 24–72 hours.19 After removing the patch, the blood drug concentration slowly decreases, with an average elimination half-life of 17 hours.
Metabolism and Excretion
Fentanyl is predominantly metabolized rapidly and extensively through the CYP3A4 pathway in the liver. The main metabolite is inactive norfentanyl, with about 75% being excreted in the urine as a metabolite, with which 10% is excreted in its original form, and a small amount is excreted in the stool and bile. The attenuation of fentanyl concentration in plasma follows an open two-compartment model, with a clearance rate of 11.6–13.3 (mL/kg • min) and an elimination half-life of about 2–4 hours. Moore et al20 observed metabolites (76% in urine and 8% in feces) in approximately 80% of patients who received intravenous fentanyl. Metabolites were detected in plasma 2 minutes after administration, and the content exceeded that of the original drug 30 minutes after administration. Mass spectrometry results indicated that the urinary tract excretion was mainly composed of 4-N(-N-propionamide)piperidyl, 4-N(- N-hydroxypropionaldehyde aniline) piperidyl, and l-(2-phenylethyl)-4-N-(N-hydroxypropionaldehyde aniline) piperidyl, which were inactive and toxic. After 24 hours of medication, the patch was removed, and the serum concentration of fentanyl gradually decreased, reaching around 50% after approximately 17 (range: 13–22) hours. After 72 hours of medication, the average half-life was recorded as 20–27 hours. After discontinuation, the skin continued to absorb fentanyl, resulting in the slower elimination of the drug from the bloodstream compared to intravenous infusion. The apparent half-life was recorded as approximately 7 (range 3–12) hours. After an intravenous infusion of fentanyl for 72 hours, approximately 75% of fentanyl was excreted through urine, mainly as a metabolite, with less than 10% of the original drug. Approximately 9% of the dose was excreted in the form of metabolites from the feces.
Clinical Application
Indications
Notably, the fentanyl-based transdermal patch can treat moderate to severe chronic pain. In case of any challenges to treat, it can only be treated with opioid analgesics.
Preferred Population
The transdermal fentanyl patch, suitable for patients with moderate to severe cancer pain, has the characteristics of non-invasive administration, stable blood concentration, long-term analgesia for 72 hours, absorption not affected by gastrointestinal status, and inactive metabolites. It should be noted that, while using fentanyl transdermal patches in the above-preferred population, it is not necessary for any special preventive measures due to its advantages over morphine or oxycodone and fewer usage restrictions. Morphine and oxycodone may be contraindicated for patients with severe damage to liver and kidney functions due to the presence of active metabolites, exacerbating side effects and endanger life. Moreover, the metabolites of fentanyl transdermal patches are inactive and relatively safe to use. The preferred population for transdermal fentanyl patch is as follows:
Opium Demand
[Recommended by experts]
For patients with stable opioid demand, a fentanyl transdermal patch is recommended for analgesic treatment. ESMO (2018) cancer pain guidelines recommend that, for patients with stable opioid demand,21 fentanyl and buprenorphine-based transdermal patches are the appropriate choices. In addition, NCCN (2021) adult cancer pain guidelines recommend that patients with stable opioid demand within 24 hours be converted to fentanyl transdermal patches or other opioid sustained release preparations22 (recommendation level I, evidence level 2A, consensus level of 96.15%).
People Unable or Unwilling to Take Orally [4,6-8]
- Difficulty in swallowing: (a) Patients who cannot swallow could be due to esophageal fistula, tracheal fistula, and recurrent laryngeal nerve paralysis, among others.21 (b) Patients could suffer from dysphagia caused by tumors, including oral cancer, nasopharyngeal cancer, laryngeal cancer, esophageal cancer, thyroid cancer, mediastinal metastatic cancer, and other tumors.23 (c) Dysphagia might be caused by other reasons: stroke, fasting, cachexia, end-stage patients, loss of consciousness hindering oral administration, among others.24 (d) Patients with severe oral mucositis caused by radiotherapy, chemotherapy, and targeted therapy.25
- Unwillingness to take orally.
[Recommended by experts]
- For patients who cannot take it orally, a fentanyl transdermal patch is recommended for analgesia (recommendation grade I, evidence grade 1A, consensus degree: 100.00%).
- For patients who do not want to take oral administration, a fentanyl transdermal patch is recommended for analgesic treatment (recommendation grade I, evidence grade 2A, consensus degree: 100.00%).
Population with Moderate and Severe Liver and Kidney Dysfunction
The progress of cancer and its complications, as well as the impact of anti-tumor treatment, may substantially lead to liver and kidney dysfunction in cancer patients.26 Despite the efficacy, the metabolic processes and resultant metabolites of different opioids are different, affecting these metabolic organs. In the cases of patients using opioids with liver and kidney dysfunction, they should pay close attention to the safety of patients and strictly follow the contraindications.21 To this end, fentanyl is significantly metabolized in the liver, and the resultant norfentanyl metabolite has no biological activity. Nevertheless, the liver dysfunction has little effect on the pharmacokinetics of fentanyl. The fentanyl-based transdermal patch is relatively safe for patients with moderate to severe liver dysfunction. It should be noted that the long-term usage of fentanyl could require close monitoring of adverse reactions.27 After metabolism in the body, approximately 10% of fentanyl is excreted in urine in its original form. Notably, mild renal insufficiency requires no alteration in the dosage. However, appropriate attention is required in the case of moderate and severe renal insufficiency. Tables 3 and 4 illustrate the use and dosage adjustment of opioids in patients with liver and kidney dysfunction.
 |
Table 3 A Summary Presents the Dose Adjustment of Opioids in Liver Dysfunction |
 |
Table 4 A Summary Indicates the Dose Adjustment of Opioids in Renal Insufficiency |
[Recommended by experts]
The fentanyl transdermal patch is recommended for patients with moderate and severe liver and kidney dysfunction for analgesic treatment. Nevertheless, it should be noted that adverse reactions should be closely monitored for long-term use (recommendation grade I, evidence grade 2A, consensus degree: 100.00%).
Population with Malignant Intestinal Obstruction
Intestinal obstruction caused by malignant tumors, one of the late tumor complications, is common in advanced gastrointestinal and pelvic tumors. Several complications are accompanied by abdominal pain, including abdominal distension, anorexia, sleep disorders, and other symptoms.22 For patients with malignant intestinal obstruction with moderate or severe cancer pain, a fentanyl patch can effectively relieve the pain.28,29
[Recommended by experts]
For cancer pain patients with malignant intestinal obstruction, a fentanyl transdermal patch is often recommended for analgesia (recommendation grade I, evidence grade 1A, consensus degree: 94.23%).
People with Intolerable Severe Nausea and Vomiting Caused by Oral Opioids
For instance, Yang et al conducted a systematic meta-analysis study on the Chinese population,30 including 32 separate clinical trials totaling 2651 cases. The analysis results showed that the transdermal fentanyl patch resulted in the same analgesic effect as the long-acting oral opioids. However, the probability of adverse reactions, such as constipation, nausea and vomiting, dizziness, and lethargy was significantly reduced. The NCCN Guidelines for Cancer Pain in Adults (2021)22 pointed out that “when nausea lasts for more than one week, opioid replacement should be considered”. Similarly, EAPC Guidelines for Opioids in the Treatment of Cancer Pain (2012)31 also pointed out that “when nausea and vomiting occur, it is recommended to switch opioids and change the route of administration, such as changing from oral administration to transdermal administration or parenteral administration or reducing drug dosage”. Accordingly, the transdermal route of administration should be an ideal route for patients with nausea and vomiting, especially those with long-term nausea and vomiting. Vomiting grades are classified as (Table 5): ① Grade I–Vomiting 1~4 times a day; ② Grade II–Vomiting 5~9 times a day; ③ Grade III–Vomiting 10 times or more a day.
 |
Table 5 Classification of Different Grades of Vomiting |
[Recommended by experts]
- For patients with severe nausea caused by oral morphine, oxycodone, and other opioids, it is recommended to replace the fentanyl transdermal patch for analgesia (recommendation level I, evidence level 1A, consensus level: 100.00%).
- For patients with vomiting reactions above grade II caused by oral morphine, oxycodone, and other opioids, it is recommended to replace the fentanyl transdermal patch for analgesia (recommendation grade I, evidence grade 1A, consensus degree: 98.08%).
People with Obstinate Constipation and Chronic Constipation
The drug distribution ratio of fentanyl in the central and gastrointestinal tract is 1:1.1, while that of morphine and other oral opioids is 1:3.4. Compared with oral opioids, fentanyl shows lesser drug distribution in the gastrointestinal tract μ-OR binding, greatly reducing the risk of constipation caused by fentanyl transdermal patch.32–34 The drug distribution ratio of fentanyl transdermal patches in the central and gastrointestinal tracts is 1:1 to 1.1. To this end, the drug distribution ratio of oral morphine and sustained-release corticosterone preparations in the central and gastrointestinal tracts is 1:3.4. Compared to oral opioid drugs (sustained-release morphine and oxycodone), fentanyl transdermal patches possess poorer bind efficiency to gastrointestinal receptors, resulting in a lower incidence of constipation. Due to the fact that fentanyl transdermal patches are administered through the skin and do not pass through the gastrointestinal system, the incidence rates of adverse reactions, such as nausea, vomiting, and constipation, are significantly lower than those of oral opioid drugs.35 NCCN Guidelines for Cancer Pain in Adults (2021)36 indicates that “when intractable constipation occurs, it is recommended to consider converting to fentanyl transdermal patch for analgesia”.
[Recommended by experts]
For patients with oral morphine, oxycodone, and other opioid drugs with constipation of more than grade III or reactions lasting more than 1 week, it is recommended to replace the fentanyl transdermal patch for analgesia (recommendation grade I, evidence grade 1A, consensus degree: 98.08%).
People with Poor Compliance with Oral Drugs
[Recommended by experts]
The fentanyl transdermal patch can relieve pain for 72 hours, which is better than the compliance of patients prescribed with oral morphine. Accordingly, the fentanyl transdermal patch is recommended for analgesic treatment for patients who cannot take medicine on time and have poor compliance with oral medicine (recommendation level I, evidence level 2A, consensus: 98.08%).37
Choose the Time
First-Line Medication
Pain is the fifth vital sign of human beings. The incidence of pain in newly diagnosed cancer patients is approximately 25%, while the incidence of pain in patients with advanced cancer is up to 60%~80%, of which 1/3 is severe pain. Clinical research shows that 4492 cancer pain patients were included in 136 centers nationwide, and the overall effective rate of fentanyl transdermal patches in relieving cancer pain can reach 96.8%.19 In 2018, the WHO Guidelines for the Administration of Drug Treatment and Radiotherapy for Cancer Pain in Adults and Adolescents put forward that fentanyl transdermal patches, as well as morphine and oxycodone oral, are commonly used strong opioid analgesics for cancer pain.1
[Recommended by experts]
It is recommended that the fentanyl transdermal patch is one of the first-line drugs for patients with moderate and severe cancer pain (recommendation grade I, evidence grade 2A, consensus degree: 88.46%).
Opioid-Tolerant Patients
Definition of opioid tolerance:22 Opioid tolerance refers to the phenomenon that the analgesic effect of patients using opioid drugs decreases without the disease progression. The same analgesic effect can be maintained only with a continuously increased dosage. According to FDA standards, opioid tolerance refers to having taken opioids on time for at least one week, including 25 μg/h fentanyl transdermal patch, oral morphine 60 mg/d, oxycodone 30 mg/d, hydromorphone 8mg/d, hydromorphone 25 mg/d, or other opioid drugs of equivalent dose. In the cases of unmet requirements for duration and dosage of pain relief, it is defined as opioid intolerance.
[Recommended by experts]
The equivalent dose conversion is conducted according to the total dose of opioids used in the past 24 hours. Table 6 presents the specific dose conversion relationship. The treatment dose of explosive pain includes 10–20% of the total dose of opioids used in the past 24 hours. In the case of the number of rescue drugs for short-acting opioids is ≥ 3 times per day, it should be considered to convert the total amount of the first 24 drugs into the total dose of fentanyl transdermal patch, administering the drug on time. Notably, the patch can be replaced on time within 72 hours according to the time recorded during use, or it can be uniformly replaced with a new patch (recommendation level I, evidence level 2A, consensus degree: 98.08% Table 6).
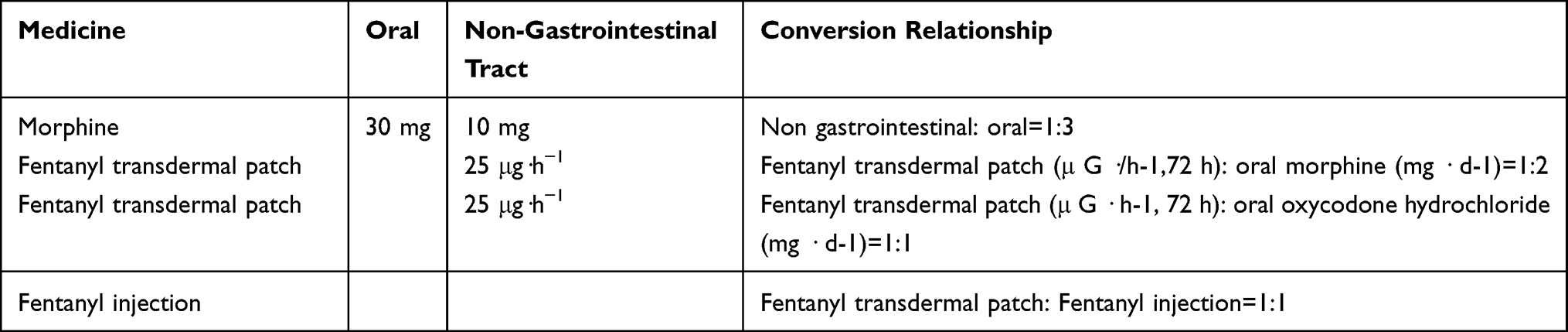 |
Table 6 A Summary Presents the Dose Conversion Relationship.9,34 |
Opioid-Intolerant Patients Who Do Not Want or Cannot Take Orally
The application of fentanyl transdermal patches in patients with opioid intolerance is controversial in clinical practice. The fentanyl transdermal patch can also be used for patients with chronic moderate to severe cancer pain who have used codeine, tramadol, and other weak opioids or compound preparations for initial analgesia. A number of studies indicated that it was also safe and effective to give low-dose transdermal fentanyl to cancer pain patients with no history of strong opioid drugs for initial analgesic treatment.38,39
[Recommended by experts]
Patients with opioid intolerance who do not want or cannot take orally can choose transdermal fentanyl for analgesia. Initially, the low-dose transdermal fentanyl patch (12.5 or 25 μg/h) can be used. Further, the pain must be evaluated every hour, treating the explosive pain. In the cases of the rescue medication, times of short-acting opioids are ≥ 3 times/d. The current background dose is insufficient, requiring an increase in the dosage (12.5 or 25 μg/h). In the case of the number of rescue drugs for short-acting opioids is less than or equal to 2 times/d, the current dose should be maintained, and administering the drug should be on time. After 72 h, the patch can be replaced on time according to the time recorded during use, or it can be uniformly replaced with a new patch (recommendation level II, evidence level 2A, consensus degree: 94.23%).
Special Types of Cancer Pain
Neuropathic Cancer Pain
Neuropathic pain, also known as neuralgia, refers to pain caused by peripheral or central nervous system (CNS) injuries, lesions, or functional disorders, which can be divided into peripheral and central neuropathic pains. The pathogenesis of neuropathic pain is complex and can be caused by numerous mechanisms. Specifically, the peripheral mechanisms include increased excitability of cell membrane and peripheral sensitization, while the central mechanisms include increased excitability of cell membrane, central sensitization, and denervation hypersensitivity. The changes of ion channels in peripheral mechanisms play an important role in neuropathic pain. After peripheral nerve injury, calcium channels discharge abnormally and repeatedly, leading to a large amount of calcium ions flowing in, causing hyperalgesia and abnormal pain. The common causes of cancerous neuropathic pain can be divided into various self-factors and tumor treatment factors. The self-factors include bone metastasis, tumor compression, nerve invasion, and changes in the surrounding environment caused by the tumor (pH change, cytokine production, release of tumor pain-causing agents, and chemical activators). To this end, the tumor treatment factors include chemotherapy-related pain (common drugs: vincristine, paclitaxel, cisplatin, and dipeptide boric acid), radiotherapy (damage to the peripheral nervous system), surgery (damage to nerves during tumor surgery).40
[Recommended by experts]
- Opioid drugs (oral morphine) can be combined with anti-convulsant drugs (such as pregabalin and gabapentin) for reducing pain, discharge-like pain, and burning pain caused by nerve injury41 (recommended level II, evidence level 2A, consensus level: 100.00%).
- In addition, these opioid drugs can be combined with tricyclic antidepressants (amitriptyline) for numbness-like pain and burning pain caused by central or peripheral nerve injury41 (recommended level II, evidence level 2A, consensus: 100.00%).
Bone Metastatic Cancer Pain
Bone is a common metastatic site in the late stage of malignant tumors, and bone metastasis is most common in breast cancer, prostate cancer, and lung cancer, among others.42 Currently, the clinical treatment of bone metastatic cancer pain43 is divided into etiological and symptomatic treatments. The symptomatic treatment is based on a three-step analgesic treatment, covering an analgesia pump, traditional Chinese medicine acupuncture, and moxibustion, as well as traditional Chinese medicine penetration, thermotherapy, and physiotherapy. According to the WHO three-step analgesic principle for cancer pain, 80%~90% of the pain caused by tumor bone metastasis can be effectively relieved.
[Recommended by experts]
Opioids (fentanyl transdermal patch, morphine) combined with bisphosphonates (pamidronate disodium and zoledronic acid) or denosumab are recommended for the treatment of bone metastatic cancer pain (recommendation level II, evidence level 2A, consensus level 98.08%).
Cancer Pain with Intestinal Obstruction29
[Recommended by experts]
For patients with cancer pain accompanied by intestinal obstruction, a fentanyl transdermal patch combined with anti-gastrointestinal secreting drugs such as anticholinergic drugs (scopolamine hydrobromide and anisodamine), somatostatin analogs (octreotide and long-acting octreotide), hormone drugs, antiemetic drugs and fluid infusion can be used for analgesia22,44 (recommended level II, evidence level 2A, consensus: 98.08%).
Adverse Reactions
The transdermal fentanyl patch belongs to opioid drugs, which have common adverse reactions similar to opioid drugs, such as constipation, nausea, vomiting, and lethargy. These adverse reactions can be gradually tolerated over time, generally 3 to 7 days. The adverse reaction of life-long intolerance was constipation. As fentanyl transdermal patch is administered through the skin without passing through the gastrointestinal system, the incidence rates of adverse reactions, such as nausea, vomiting, and constipation, are significantly lower than those of oral opioids. The serious adverse reaction caused by fentanyl transdermal patch is respiratory depression, which can be alleviated by symptomatic treatment. The treatment of these notified adverse reactions is discussed as follows.
Nausea and Vomiting
Fentanyl can directly stimulate medullary chemoreceptors and also act on gastrointestinal receptors, causing nausea and vomiting. The incidence of nausea and vomiting is about 30%, which generally occurs in the early stage of drug use. The symptoms are usually relieved within a week. The occurrence and severity of such adverse reactions are related to individual differences. Notably, for the patient with nausea and vomiting, other reasons should be ruled out, such as constipation, brain metastasis, radiotherapy and chemotherapy, and hypercalcemia, among others. For mild nausea, metoclopramide, chlorpromazine, or haloperidol can be chosen as treatment options. Patients with severe nausea and vomiting should be given antiemetic drugs and intravenous nutrient solution on time according to the clinical practice,45 strengthening the nursing work of patients along with the following options.
- The patient’s diet should be light and easy to digest, with a small number of meals, avoiding sweet food or greasy, spicy, and stimulating food.
- It is required to rinse the mouth after meals to keep it clean and the dining environment clean.
- Patients with a previous history of opioid nausea and vomiting and a sensitive constitution should be treated with antiemetic drugs according to the doctor’s advice to prevent nausea and vomiting.
[Recommended by experts]
In the first week after the first use of fentanyl transdermal patch, antiemetic drugs, such as metoclopramide, should be given at the same time.46 (Recommendation level I, evidence level 1A, consensus degree: 96.15%).
Constipation
Several clinical studies confirmed that opioid receptors were widely distributed in gastrointestinal smooth muscle cells, sympathetic nerve endings, and peripheral sensory nerve endings. Fentanyl could act on the gastrointestinal tract, spinal cord, and other parts. The causes of constipation are as stated in the following. μ-OR binding blocks the rhythmic contraction of the intestinal wall required for intestinal motility and damages intestinal function, making intestinal peristalsis slow, intestinal fluid secretion reduced, and absorption increased. It can reduce the activity of excitatory and inhibitory neurons in the intestinal muscular plexus and make patients insensitive to the stimulation that causes the defecation reflex. The tension of intestinal smooth muscle is increased, and coordinated peristalsis is inhibited, thus increasing non-peristaltic contraction. By activating μ Receptors and δ Receptors, it can reduce epithelial secretion and promote the reabsorption of water and electrolytes, thus promoting the formation of constipation. Constipation, as a common adverse reaction of opioids, is often lifelong and intolerable to many patients.47,48 It is necessary to pay attention to the prevention of constipation in the clinics, and the following ways can be taken to strengthen nursing:
- It is required to comprehensively understand the patient’s daily defecation, stool characteristics, anal exhaust, abdominal distension, and intestinal peristalsis.
- It is required to assess the patient’s eating habits, encourage the patient to drink more water, and eat more vegetables and fresh fruits rich in crude fiber.
- Activities in bed or under bed should be encouraged according to the patient’s condition.
- A circular clockwise massage on the abdomen is required, as well as Chinese patent medicine on the abdomen to promote intestinal peristalsis.49
- During the use of a transdermal fentanyl patch for intractable constipation, a laxative can be used. Use laxatives such as senna and lactulose to prevent constipation according to the patient’s stool habits. It is optimal for patients to drink more water and eat more vegetables and fruits containing fiber to prevent it.
- Kaiselu is given when the defecation intention is obvious, defecation is difficult, and an enema can be given at the required conditions.
- It is recommended to provide specific guidelines for the duration of storage, such as the expiration date or recommended replacement interval for fentanyl patches.50
- In the initiating therapy, plasma concentrations should be monitored, and doses should be adjusted based on age and weight, which would assist healthcare professionals in managing pain in pediatric patients effectively and safely.51
[Recommended by experts]
During the use of the fentanyl transdermal patch, the laxative can be prepared and used according to the patient’s stool habits (recommended level I, evidence level 1A, consensus: 100.00%).
Drowsiness and Excessive Sedation
The excessive sedation caused by opioids is related to CNS inhibition. In the case of relatively “excessive” opioids combined with opioid receptors in the brain, they will cause membrane potential hyperpolarization and reduce the release of neurotransmitters, including acetylcholine, noradrenaline, dopamine, and substance P, thus blocking the transmission of nerve impulses and producing sedation, as well as analgesia. These effects can be combined with the respiratory inhibition of sedatives and sedative-hypnotics.52
[Recommended by experts]
- In case of excessive sedation, dosage reduction or drug withdrawal are initial considerations, and then the rotation of opioids is done (recommendation level III, evidence level 2B, consensus degree: 96.15%).
- Patients who have experienced excessive sedation can be given central stimulants such as methylphenidate and dexamphetamine preventively (recommendation grade III, evidence grade 2B, consensus degree: 92.31%). The use of central stimulants to prevent excessive sedation can be considered in specific clinical situations. However, it is a complex decision that should be made on a case-by-case basis.53 The potential benefits of improving alertness and functionality must be weighed against the potential risks of drug interactions, tolerance, and other adverse effects. Furthermore, healthcare providers should closely monitor patients and consider alternative strategies appropriately. By taking into account their preferences and values, collaborative decision-making with patients is essential in such cases.54,55
Urinary Retention
The mechanism of urinary retention can be divided into peripheral and central effects. Opioids often increase the tension of smooth muscle, causing bladder spasms. Increasing the tension of the sphincter will lead to urinary retention. In addition, morphine combines with spinal opioid receptors to inhibit the release of sacral parasympathetic nerve impulses, making the ureter contract and the bladder detrusor relax. Simultaneously, with increased sphincter tension and bladder capacity, the bladder internal pressure cannot overcome urethral sphincter resistance, leading to urinary retention.56 Currently, it is believed that the mechanism of urinary retention caused by opioids is mainly due to the spinal cord mechanism. In case of urinary retention, self-urination can be induced first by running water, flushing the perineum with hot water, and massaging the bladder area. Nevertheless, catheterization can be considered in the case of unsuccessful induced urination. The analgesics can be changed for patients with persistent urinary pond.
[Recommended by experts]
If urinary retention cannot be alleviated with fentanyl transdermal patch, corresponding measures can be taken for symptomatic treatment (recommendation level III, evidence level 2B, consensus degree: 100.00%).
Pruritus
Since ancient times, opioids have been used as predominant analgesics to inhibit pain. Neurons receiving multiple senses in the axon of the spinal cord may receive itch- and pain-related signals simultaneously, confusing the two signals and aggravating itching symptoms.57 The skin itching caused by opioids is considered pruritus and accounts for about 2–10%, which generally occurs in epidural or spinal injections of opioids. The incidence of skin itching caused by fentanyl transdermal patch is relatively low. The plausible mechanism is centrally mediated by the histamine release. In case of itching, the patient is instructed to gently pat the local skin with his finger pulp or palm or press the bloodstream, and Zusanli points with his fingers for 2–3 minutes. In addition, the patients are advised not to scratch the skin or scald the itchy part with hot water or use soap and other irritants. Moreover, it is required to ask the patient to wear loose cotton clothes. In the cases of severe itching, the patients are required to visit and follow the doctor’s instructions.
[Recommended by experts]
- Skin pruritus is generally a toxic side effect of opioid drugs. In the case of fentanyl transdermal patch, allergy-related itching should also be considered (recommendation level II, evidence level 1B, consensus degree: 98.08%).
- Typically, several kinds of antihistamines are usually applied to treat itching symptoms, including cetirizine, diphenhydramine, and loratadine, among others. (recommendation grade I, evidence grade 2A, consensus degree: 100.00%).58
Vertigo
Drug-induced vertigo generally refers to vertigo caused by vestibular and cochlear damage caused by drugs.59 The mechanism of opioid-induced vertigo is predominantly based on CNS inhibition. Inhibiting the cortical center shows dizziness and slight imbalance with no motion illusion. However, with the use of opioid drugs that result in the strong inhibition of the cortical center, various afferent information about balance cannot be synthesized and analyzed in the center. Hence, the patient has dizziness symptoms, with the chief complaint being lethargy. Nevertheless, it does not belong to the category of true vertigo. Specific measures for managing drug-induced vertigo are required to be taken if necessary, such as patient education, dose adjustment, or referral to a specialist.
[Recommended by experts]
- The dosage of opioids should be low for the first time, which should be gradually increased from the low dosage to the optimal dosage. Mild vertigo can be relieved by itself after several days of medication. For moderate and severe vertigo, it is necessary to consider reducing the dosage of opioids appropriately. In severe cases of vertigo, medicine must be prescribed to relieve symptoms. Simultaneously, the patient needs to pay attention to slowing down while resting and changing positions, avoiding squatting and rotation, and monitoring blood pressure and heart rate (recommendation level I, evidence level 2A, consensus: 98.08%).
- Frail and anemic patients are more likely to suffer from vertigo during the fentanyl transdermal patch application. Such patients need to reduce the dosage as appropriate (recommendation grade I, evidence grade 2A, consensus degree: 100.00%).
Respiratory Inhibition
The respiratory depression is the most serious adverse reaction to opioids. After binding to the μ-OR, it interferes with the respiratory center, controlling the respiratory rhythm in the pons and spinal cord and produces dose-related respiratory inhibition through direct action on the brainstem respiratory center. For example, high-dose use of opioids can cause asphyxia. Clinical manifestations of respiratory depression include needle-like pupils, decreased respiratory frequency (<8 times/min) and/or tidal volume, tidal breathing, cyanosis, lethargy or even coma, skeletal muscle relaxation, clammy skin, as well as occasionally bradycardia, and hypotension.26
The corresponding preventive measures include regular medication, starting with a small dosage and gradually increasing it according to the condition. While using opioid drugs, the elderly and weak and those with severe cardiopulmonary insufficiency should closely observe their respiratory, mental, and mental states. To this end, the treatment measures include 1 mL of naloxone (0.4 mg/mL) was added with 0.9% sodium chloride solution to dilute it to 10 mL, and 1~2 mL−1 is administered intravenously every 30~60 seconds until the symptoms improved. The administration procedure is repeated if necessary. If the drug is still ineffective within 10 minutes and the total amount of naloxone administration reaches 1 mg, the cause and severity of respiratory inhibition should be re-evaluated. Moreover, continuous intravenous infusion of naloxone is considered for opioids with a long half-life due to its short half-life.
[Recommended by experts]
- Patients with chronic obstructive pulmonary disease, severe emphysema, and cardiopulmonary insufficiency should be careful to use fentanyl transdermal patch (recommendation grade I, evidence grade 2A, consensus degree: 98.08%).
- For patients with end-stage tumors complicated with dyspnea, a fentanyl transdermal patch can be used after excluding factors such as respiratory obstruction (recommendation grade I, evidence grade 1A, consensus degree: 98.08%).
Drug Interactions
Interactions Between Fentanyl and CNS Inhibitors (Including Alcohol and Some Prohibited Drugs)
Fentanyl produces respiratory depression through direct action on the respiratory center of the brain stem. Therefore, the combination of fentanyl and other CNS inhibitors, including benzodiazepines and other sedatives/hypnotics, opioids, general anesthetics, phenothiazines, tranquilizers, muscle relaxants, sedative antihistamines, alcohol, and some prohibited drugs, can increase the inhibitory effect of the CNS disproportionately. These consequences may cause respiratory depression, hypotension, deep sedation, coma, or death.60,61
[Recommended by experts]
It is recommended not to drink alcohol during the use of fentanyl. Suppose patients need to use benzodiazepines and other CNS inhibitors due to limited alternative treatment options. In that case, they should try to use a small dose, a short course of treatment, and pay close attention to the patient’s respiratory inhibition and sedation symptoms (recommendation level I, evidence level 2A, consensus level: 100.00%).
Interactions Between Fentanyl and CYP3A4 Inhibitors
Fentanyl is mainly metabolized through CYP3A4. In combination with CYP3A4 inhibitors (such as ritonavir, ketoconazole, itraconazole, acezotocin, clarithromycin, nelfinavir, nefazodone, amiodarone, aminopanavir, alepidem, diltiazem, erythromycin, fluconazole, furazanavir, verapamil or grapefruit juice), the concentration of fentanyl in blood would increase, thus prolonging the efficacy and adverse reactions of fentanyl. In addition, it may cause severe respiratory depression.62 Increased plasma concentrations of fentanyl in the presence of potent CYP3A4 inhibitors significantly raise the possibility of a significant adverse pharmacological reaction. However, some studies indicated that only 8% of fentanyl was metabolized through the CYP3A4 pathway, even if powerful CYP3A4 inhibitors were used simultaneously, causing no major drug interactions.63,64
[Recommended by experts]
In the cases of ketoconazole or other powerful CYP3A4 inhibitors given at the same time, close monitoring should be carried out, adjusting the fentanyl dose appropriately (recommended level II, evidence level 2A, consensus degree: 100.00%).
Interactions Between Fentanyl and CYP3A4 Inducer
Fentanyl used in combination with CYP3A4 inducers (such as rifampicin, carbamazepine, phenobarbital, and phenytoin) may increase the clearance rate of fentanyl, decreasing the blood concentration and substantial therapeutic efficacy. Accordingly, the dosage may need to be adjusted.63–65 If CYP3A4 inducer treatment is stopped, the effect of the inducer gradually declines, leading to an increase in fentanyl blood concentration. Thus, increasing the efficacy and adverse reactions may also cause severe respiratory depression.
[Recommended by experts]
When combined with rifampicin, carbamazepine, phenobarbital, and phenytoin, among others, close monitoring must be carried out, and the dose of fentanyl shall be adjusted if necessary (recommendation level II, evidence level 2A, consensus level: 100.00%).
Interactions Between Fentanyl and Diuretics
The mechanism of fentanyl’s effect on the release of antidiuretic hormone is still unclear, which may be due to the effect of fentanyl on μ-OR, inducing the release of antidiuretic hormone.41,66 If fentanyl is used together with diuretics, the efficacy of diuretics may be reduced.
[Recommended by experts]
If used with diuretics, the patient’s diuretic lowering and/or blood pressure-affecting signs should be monitored. The dosage of diuretics should be increased if necessary (recommendation level III, evidence level 2B, consensus degree: 94.23%).
Interactions Between Fentanyl and 5-Hydroxytryptaminergic Drugs
Fentanyl, a 5-hydroxytryptamine agonist that belongs to the phenylpiperidine subclass of opioid drugs,67 can enhance the release of 5-hydroxytryptamine and weakly inhibit the reuptake of 5-hydroxytryptamine, thereby increasing the level of 5-hydroxytryptamine in the synapse. There is no report of 5-hydroxytryptamine syndrome caused by fentanyl alone.68–70 However, combination with other serotonin drugs or selective serotonin reuptake inhibitors may increase the risk of serotonin syndrome, which is a life-threatening disease.71
[Recommended by experts]
The risk of using fentanyl with serotonin should be assessed by an experienced doctor and closely monitored, especially at the beginning of treatment and during dose adjustment. If 5-hydroxytryptamine syndrome is suspected, fentanyl transdermal patch treatment should be stopped. Reportedly, during the simultaneous use of fentanyl patch and 5-hydroxytryptaminergic drugs, increasing the replacement frequency of fentanyl might trigger 5-hydroxytryptamine syndrome. Thus, it is not recommended to increase the replacement frequency of a fentanyl patch (recommendation level II, evidence level 2A, consensus level: 100.00%).
Security Management
Safety of High-Dose Fentanyl Transdermal Patch
There exist some concerns regarding the utilization of the fentanyl transdermal patch in large doses in clinical practice. The instructions also mention that the dosage of fentanyl transdermal patch exceeds 300 μg/h. Some patients may need to add or change the medication of opioids. As a strong opioid drug, the fentanyl-based transdermal patch has no dose limit in the clinical application. It was reported in the literature that the dose range of 300 to 1050 μg/h of fentanyl transdermal patch was used,72,73 which could safely and effectively relieve the pain of patients. Therefore, a large dose of fentanyl transdermal patch (>300 μg/h) treatment, if necessary, could be combined with non-drug therapy intervention.
[Recommended by experts]
During the clinical application of the transdermal fentanyl patch, the patient’s pain has not been alleviated. According to the comprehensive evaluation, if the dose is insufficient, the patient should follow the dosage principle if the patient can accept adverse reactions until the pain is alleviated (recommendation level II, evidence level 2A, consensus: 98.08%).
Elderly Patients
The elderly tumor patients were often affected by organ function degradation, low plasma protein levels, and other factors due to slow drug metabolism and high incidence of adverse drug reactions. The main adverse reactions of patients in the course of treatment were dysuria, constipation, pruritus, nausea, vomiting, and lethargy. Studies indicated that the incidence of adverse reactions to fentanyl transdermal patches in elderly cancer patients was significantly lower than that of oral morphine and oxycodone.44 Numerous clinical evidence and pharmacology suggested that the use of opioid drugs in elderly patients was safe. Like other drugs, opioid drugs were metabolized, transformed, and excreted through the liver and kidneys. People with normal liver and kidney function generally did not experience accumulation effects for patients with poor liver and kidney function, especially in elderly patients.74 It is recommended to use fentanyl patches for pain relief treatment. However, the liver and kidney reserve capacity of older adults is poor, with specific dosage adjustments and currently lacking monitoring parameters. Like other drugs, the use of painkillers must also start at a small dosage, and the increase in dosage should be slow. At the same time, the level of renal function should be tested, and attention should be paid to observing adverse reactions.75
[Recommended by experts]
- For elderly patients (≥ 65 years old), the initial dose of fentanyl transdermal patch can be equal to the adult dose (25 ug/h) and started to use (recommendation level I, evidence level 2A, consensus degree: 98.08%).
- For elderly patients with oral morphine, oxycodone, and other opioid drugs that have grade II or higher adverse reactions and cannot be tolerated, it is recommended to replace them with fentanyl transdermal patch (recommendation grade II, evidence grade 2A, consensus degree: 96.15%).
Children48–50
The instructions for the fentanyl patch indicate that the efficacy and safety of this product in children have not been clarified. Research showed that it was safe and valuable to use a fentanyl transdermal therapy system to control pain in opioid-tolerant children ≥ 2 years old. Pharmacokinetic studies displayed that it seemed that children took a longer time to reach the steady-state serum drug concentration, the clearance rate (expressed in kg/h) was higher, and the elimination half-life of children was shorter than that of adults. Compared with adults, there was no fundamental difference in the impact or characteristics of adverse reactions.
Because children metabolize fentanyl faster than adults, it may take longer for children than adults to reach a stable plasma fentanyl concentration. Compared with older children or adults, younger children may need higher doses. However, it should be used with caution to avoid serious adverse reactions, such as overdose-induced respiratory depression. Research showed that the pharmacokinetics of fentanyl in children were similar to those in adults.50,51 However, it is required to be cautious during practical applications due to a lack of experience and advice for children in the instructions for the use of fentanyl transdermal patches. Monitoring plasma concentrations and adjusting the dose according to age and body weight are appropriate.
[Recommended by experts]
The initial dose of fentanyl transdermal patch for children with tumor pain can be reduced from 12.5 μg/h starting (recommendation level III, evidence level 2B, consensus degree: 92.31%).
Storage
[Recommended by experts]
The fentanyl-based transdermal patches should be stored at room temperature and kept out of sight and contact with children and pets. After use, the patch should be folded along the adhesive side and then put back into the original package for treatment according to the doctor’s instructions. Any non-drug users who accidentally come into contact with the adhesive surface of the fentanyl patch shall be immediately removed and immediately referred to a doctor (recommendation level II, evidence level 2A, consensus degree: 96.15%).
Prescription Management
In the Chinese Pharmacopoeia (2020 edition), the Guiding Principles for Slow-Release and Controlled-Release Preparations clearly stipulate that slow-release preparations refer to the slow and non-constant release of drugs in the specified release medium as required. Compared with the corresponding ordinary preparations, the frequency of administration is reduced by half or a little. The Controlled Release Preparations refer to the drugs slowly released at a constant or near constant rate in the specified release medium as required. Compared with the corresponding ordinary preparations, the administration frequency is reduced by half or reduced to some extent. The transdermal fentanyl patch enters the body through the skin at a constant release rate so that the transdermal fentanyl patch can be categorized as the controlled release dosage form. The Prescription Management Measures issued and implemented in 2007 clearly stipulated the prescription dosage and days of anesthetic drug controlled sustained release dosage form, and the prescription management of fentanyl transdermal patch should refer to this provision.
It is issued for outpatient (emergency) patients, and each prescription shall not exceed 7 daily doses. It is issued for patients with portal (emergency) cancer pain and patients with moderate and severe chronic pain, and each prescription shall not exceed 15 daily doses. Each prescription for inpatients should be one time of common use.
Patient Education
Usage
Location Selection
[Recommended by experts]
The sticking site of the fentanyl transdermal patch shall be the flat area without hair on the chest, back, upper arm, inner thigh or abdomen, avoiding the spine, skin with injury, scar, radiotherapy, and easy moving parts. For patients with advanced cancer lying in bed, do not rub the patch when turning over to prevent it from curling or falling off. Moreover, it should not be applied to the inner thigh of patients with incontinence or bed stool. For patients with excessive sweating, it should not be attached to the back, chest, or abdomen. For thinner patients or patients with cachexia, the patch should be applied to the subcutaneous tissue as far as possible, avoiding bone protuberance. In the case of washing the selected parts with clean water, it is suggested to avoid rubbing the skin with force. It is forbidden to use soap, detergent, 75% ethanol or iodine tincture, and other organic solvents to rub the parts. The film is close to the skin, with no gap in the middle. The film is pressed gently with the palm of your hand for 30 seconds and pressed again with the finger along the edge of the film to ensure full contact between the film and the skin51,52 (recommendation level II, evidence level 2A, consensus: 100.00%).
Change the Sticker on Time
[Recommended by experts]
Under normal circumstances, the patch should be replaced on time for 72 hours, and a small number of patients need to be replaced for 48 hours (such as patients with end-stage pain) (recommendation level III, evidence level 2B, consensus level: 100.00%).
- If the analgesic effect is maintained for less than 72 h, the patient can be titrated (ie, morphine released) again on the same day, and the total amount of morphine released on the same day can be calculated. The equivalent fentanyl transdermal patch dose can be converted for administration. The titrated fentanyl patch dose plus the basic dose is taken as the total dose of the next dosing cycle.
- When morphine or oxycodone is taken orally and replaced by fentanyl transdermal patch, the patch can be replaced 6–12 hours after the last oral administration, and the principle of pain titration is still followed.
- If the analgesic effect of the patient is less than 60 h for three consecutive cycles, the pain situation of the patient needs to be re-evaluated. If necessary, the pain treatment should be carried out using the combined drug mode or non-drug mode.
- When replacing the patch, the old patch should be removed to avoid the fentanyl accumulation, and replace the sticking part at the same time.
Drug Withdrawal
[Recommended by experts]
The gradual reduction method should be adopted, with 10%~25% reduction every 3 days until the daily dose is equivalent to the dosage of 30 mg of oral morphine, ie, 12.5 μg/h fentanyl transdermal patch can be stopped after two more days of application20 (recommendation level II, evidence level 2A, consensus level: 100.00%).
Precautions
Avoid Contact with Heat Sources
The fentanyl transdermal patch should avoid contact with heat sources during use. The drug manual indicates that the blood drug concentration increases by 1/3 when the temperature is increased to 40° C.23 Heat can promote the release of fentanyl and increase the absorption of fentanyl through the skin, leading to serious adverse reactions.76 Patients should be instructed to avoid direct contact with heat sources at the application site of this product, such as heating pads, electric blankets, heating water beds, baking lamps or sunlight lamps, intense sunbathing, hot water bottles, and long hot water baths, among others. If there is a fever while using the patch, the doctor must be informed immediately.60
[Recommended by experts]
- It is not recommended for patients with fever, but it can be used as appropriate for patients with low fever. However, it needs to be closely observed (recommendation level III, evidence level 3, consensus degree: 98.08%).
- During the use of fentanyl transdermal patch, a simple shower can be carried out, but it should be avoided to wash the pasted part for a long time. Bathing is not recommended (recommendation level II, evidence level 2A, consensus: 98.08%).
Patients Prone to Sweating
[Recommended by experts]
Patients with excessive sweating should stick it on the inner side of the upper arm or the inner side of the thigh where there is less sweat and fix it with a breathable dressing to reduce the chance of curling or falling off (recommendation level III, evidence level 2B, consensus degree: 98.08%).
Another Effective Time After the Replacement
[Recommended by experts]
The first use of a fentanyl transdermal patch for 6 to 12 hours requires a transitional analgesic dose of opioids to go through the onset of the patch. If the patch is replaced, fentanyl is stored in the fat, and the blood concentration remains stable, so no opioid drugs for excessive analgesia are needed55,56 (recommendation level II, evidence level 2A, consensus level: 100.00%). During the transitional period, there is generally no need for opioid drugs due to the residual dosage of fentanyl in the subcutaneous fat of fentanyl transdermal patches. If there is an outbreak of pain, it can be titrated with opioid drugs (ie, morphine tablets).
Whether It Can Be Cut for Use
[Recommended by experts]
A skeletal transdermal fentanyl patch can be cut for use, which is more flexible than the storage type dosage adjustment. In contrast, the storage type fentanyl cannot be cut, which has the risk of drug leakage57 (recommendation level III, evidence level 2B, consensus degree: 100.00%).
Emergency Plan
[Recommended by experts]
For patients with serious adverse events, the patch must be immediately removed, and the local skin must be cleaned with a wet towel to prevent continued absorption of drugs. It is prohibited to use hot towels to scrub so as to avoid the expansion of pores and capillaries and accelerate the absorption of residual drugs on the skin. After that, the area must be monitored for at least 24 hours (recommendation level I, evidence level 2A, consensus degree: 100.00%).
Patient Management
- For patients with cancer pain or patients with moderate or severe chronic pain who need long-term use of fentanyl transdermal patch, the doctor should examine the patient in person first, establish corresponding medical records, and ask them to sign the Informed Consent Form. Further, copies of the following materials shall be retained in the medical record: the diagnosis certificate issued by a hospital above Grade II, the patient’s registered residence, ID card, or other relevant valid identification documents.
- For patients with portal (emergency) cancer and patients with moderate or severe chronic pain who have used fentanyl transdermal patch for a long time, they should be revisited or followed up every 3 months.
- A demonstration video of the correct use of fentanyl transdermal patches is provided for patients.
Follow Up
The follow-up system is required to be established and improved for cancer pain patients, conducting the first follow-up for patients receiving standardized treatment of cancer pain within one week after discharge. For pain relief, follow-up can be conducted once 1 to 2 weeks.77 Home visits are conducted once a week. Patients with an outbreak of pain of more than 8 points enter the next cycle of personalized treatment and follow-up.78 The follow-up contents include pain and adverse event evaluations. In addition, patient guidance, paying attention to humanistic care, meeting the patient’s pain relief needs to the maximum extent, and ensuring that they can receive continuous, reasonable, safe, and effective treatment.
With the progress of clinical practice and the development of clinical research, pain treatment drugs have been increasingly enriched in dosage forms, types, and routes of administration. As a long-term analgesic preparation, the fentanyl transdermal patch has enriched the analgesic means for clinical cancer pain patients. Simultaneously, the connotation and concept of the three-step pain treatment scheme have also been further developed, such as the weakening of the second-step drugs, the titration of slow-release preparations, and the change of pain management objectives for the early control of the evolution of cancer pain principle.79 The rational, regular, and effective use of existing analgesic drugs can not only alleviate the pain symptoms of tumor patients to the greatest extent but also reduce or even avoid adverse reactions, as well as improve the quality of life of patients. Pain medication diary is presented in Supplementary Table 1.
Looking forward to the future, we will continue to improve and update the guidelines, refine the diagnosis and treatment plans, and accumulate high-quality, evidence-based medical evidence in China. Thus, it improves the recognition, diagnosis, and treatment ability of doctors and nurses in the clinical application of fentanyl transdermal patches and reduces the differences in diagnosis and treatment levels in different regions.
Specific Recommendations
Neuropathic Cancer Pain
Consider combining opioid drugs (eg, fentanyl transdermal patch, morphine) with anticonvulsant drugs (eg, pregabalin and gabapentin) for specific types of nerve pain.
Opioid drugs can also be combined with tricyclic antidepressants (eg, amitriptyline) for other types of nerve pain.
Bone Metastatic Cancer Pain
Opioids (eg, fentanyl transdermal patch, morphine) combined with bisphosphonates (eg, pamidronate disodium, zoledronic acid) or denosumab are recommended for treating pain resulting from bone metastases.
Cancer Pain with Intestinal Obstruction
For patients with cancer pain and intestinal obstruction, fentanyl transdermal patches combined with anti-gastrointestinal secretory drugs can be used, such as anticholinergic drugs, somatostatin analogs, hormone drugs, antiemetic drugs, and fluid infusion for pain relief.
Dosage Adjustments in Special Populations
Patients with frailty, anemia, chronic obstructive pulmonary disease, or severe emphysema should be cautious when using fentanyl transdermal patches. The dosage should be adjusted as appropriate.
For end-stage tumor patients with dyspnea, fentanyl transdermal patches can be considered after excluding respiratory obstruction.
For patients experiencing excessive sedation, dosage reduction or drug withdrawal should be considered. Central stimulants like methylphenidate and dexamphetamine should be given preventively.
Potential Drug Interactions
CNS Inhibitors
Avoid combining fentanyl with CNS inhibitors, including alcohol, benzodiazepines, sedatives/hypnotics, opioids, and others. Such combinations can lead to excessive CNS depression, respiratory depression, and other adverse effects.
CYP3A4 Inhibitors
Fentanyl is metabolized through CYP3A4. Using it with CYP3A4 inhibitors like ketoconazole can increase blood concentrations of fentanyl, potentially leading to more pronounced effects and adverse reactions. Close monitoring and dose adjustment may be necessary.
CYP3A4 Inducers
Combining fentanyl with CYP3A4 inducers like rifampicin, carbamazepine, or phenobarbital can lead to increased fentanyl clearance, reducing its efficacy. Dose adjustments may be required. Stopping CYP3A4 inducer treatment may cause increased fentanyl concentrations and potential adverse effects.
Diuretics
The efficacy of diuretics may be reduced when used with fentanyl. Monitor diuretic effects and blood pressure and adjust diuretic dosages if necessary.
5-Hydroxytryptaminergic Drugs
Assess the risk of serotonin syndrome when combining fentanyl with serotonin drugs or selective serotonin reuptake inhibitors (SSRIs). Close monitoring is essential, especially during treatment initiation and dose adjustments.
Best Practices for Preparation and Preservation
Properly prepare and apply the fentanyl transdermal patch according to medical guidelines and manufacturer instructions.
Avoid Alcohol Consumption During Fentanyl Use
Ensure close monitoring for any adverse reactions and intervene as necessary.
When managing adverse effects, consider measures such as antiemetic drugs for nausea, laxatives for constipation, and antihistamines for itching.
Be Cautious with Fentanyl Use in Frail and Anemic Patients
Preventive central stimulants may be given to patients experiencing excessive sedation.
Monitor patients with end-stage tumors for respiratory complications.
Assess the risk of 5-hydroxytryptamine syndrome when using fentanyl alongside serotonin drugs.
Statement of Data
The data is available upon reasonable request.
Acknowledgment
Compiling group of “Guidelines for Clinical Rational Use of Fentanyl Transdermal Patch”.
Specially invited consultant
Yu Shiying, Tongji Hospital, Tongji Medical College, HUST; Wei Shaozhong, Hubei Cancer Hospital; Du Guang, Tongji Hospital, Tongji Medical College, HUST.
Committee of Directors
Chen Yuan, Tongji Hospital, Tongji Medical College, HUST.
Members of the expert group
Chu Qian, Tongji Hospital, Tongji Medical College, HUST; Cao Fengjun, SHIYAN RENMIN HOSPITAL; Chen Ping, SHIYAN RENMIN HOSPITAL; Chen Fengju, Tongji Hospital, Tongji Medical College, HUST; Deng Di, ZHONGNAN HOSPITAL OF WUHAN UNIVERSITY; Du Wei, JINGZHOU NO.1 RENMIN HOSPITAL; Duan Chunyan, Enshi Central Hospital; Dai Zhu, Hubei Cancer Hospital; Fan Houwu, Hubei Jianli Traditional Chinese Medicine Hospital; Guo Qinglin, Gong’an Traditional Chinese Medicine Hospital; Hu Zuowei, WUHAN NO.1 HOSPITAL; Ke Hong, Sinopharm Gezhouba Central Hospital; Kuang Li, Dongfeng General Hospital of Sinopharm; Li Linjun, Hubei Integrated Traditional Chinese and Western Medicine Hospital; Li Daojun, Yichang Central People’s Hospital; Liu Xiuli, YICHANG NO.1 RENMIN HOSPITAL; Liu Jing, Huanggang Central Hospital; Luo Xiuli, HUBEI PROVINCIAL HOSPITAL OF TCM; Li Jun, Hubei Xiaogan Central Hospital; Liu Jinmei, Union Hospital, Tongji Medical College, HUST; Li Xin, YICHANG NO.2 RENMIN HOSPITAL; Hu Jianli, Union Hospital, Tongji Medical College, HUST; Ming Bangchun, Shiyan Taihe Hospital; Pan Xianfeng, Jingzhou Central Hospital; Ran Fengming, Hubei Cancer Hospital; Ran Ruizhi, Enshi Central Hospital; Shu Chengrong, Xianning Central Hospital; Sun Jianhai, The Third People’s Hospital of Hubei Province; Tao Weiping, People’s Hospital of Wuhan University; Tang Ze, Huangshi Central Hospital; Wang Jianzhong, Wuhan Iron and Steel Second Hospital; Wang Chun, Wuhan Central Hospital; Wang Qun, Wuhan Fifth Hospital; Wang Huifen, Hubei Cancer Hospital; Xu Shuying, Hubei Cancer Hospital; Yang Bo, Central Theater Command General Hospital; Yin Yifa, YICHANG NO.2 RENMIN HOSPITAL; Yi Tienan, Xiangyang Central Hospital; Zhang Gong, ZHONGNAN HOSPITAL OF WUHAN UNIVERSITY; Zhao Yuanhua, Hubei Cancer Hospital; Zhao Yanxia, Union Hospital, Tongji Medical College, HUST; Zhao Yong, Central Theater General Hospital in Wuhan; Zhang Chengliang, Tongji Hospital, Tongji Medical College, HUST;
Writing group leader
Fu Qiang, Tongji Hospital, Tongji Medical College, HUST.
Writing group members
Han Na, Tongji Hospital, Tongji Medical College, HUST; Li Na, Renmin Hospital of Wuhan University; Gui Ling, Tongji Hospital, Tongji Medical College, HUST; Shi Chen, Union Hospital, Tongji Medical College of HUST; Rong Peipei, People’s Hospital of Wuhan University; Zeng Fan, Tongji Hospital, Tongji Medical College, HUST; Rao He, ZHONGNAN HOSPITAL OF WUHAN UNIVERSITY; Chen Yuan, Tongji Hospital, Tongji Medical College, HUST.
Funding
The research received funding from Investigation on standardized treatment of cancer pain (2012) No. YSATTJ-001.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization. WHO guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents. World Health Organization; 2018. Available from: https://apps.who.int/iris/handle/10665/279700.
2. World Health Organization. Model list of essential medicines; 2019. Available from: https://list.essentialmeds.org/.
3. Deng G. Integrative medicine therapies for pain management in cancer patients. Cancer J. 2019;25(5):343–348. doi:10.1097/PPO.0000000000000399
4. Davis MP. Fentanyl for breakthrough pain: a systematic review. Expert Rev Neurother. 2011;11(8):1197–1216. doi:10.1586/ern.11.63
5. Yang M, Z. X, M. M, et al. CSCO guidelines for metastatic colorectal cancer: personalized medicine in clinical practice. Cancer Biol Med. 2023;20:640–645. doi:10.20892/j.issn.2095-3941.2023.0211
6. Hair PI, Keating GM, McKeage K. Transdermal matrix fentanyl membrane patch (matrifen): in severe cancer-related chronic pain. Drugs. 2008;68:2001–2009. doi:10.2165/00003495-200868140-00005
7. Yu SY. New dosage form of fentanyl. Clin J Pract Hosp. 2006;3:94–95.
8. Pathan H, Williams J. Basic opioid pharmacology: an update. Br J Pain. 2012;6:11–16. doi:10.1177/2049463712438493
9. Zhuang Y, Wang Y, He B, et al. Molecular recognition of morphine and fentanyl by the human mu-opioid receptor. Cell. 2022;185:4361–75 e19. doi:10.1016/j.cell.2022.09.041
10. Thompson JP, Bower S, Liddle AM, Rowbotham DJ. Perioperative pharmacokinetics of transdermal fentanyl in elderly and young adult patients. Br J Anaesth. 1998;81(2):152–154. doi:10.1093/bja/81.2.152
11. Collins JJ, Dunkel IJ, Gupta SK. Transdermal fentanyl in children with cancer pain: feasibility, tolerability, and pharmacokinetic correlates. J Pediatr. 1999;134(3):319–323. doi:10.1016/S0022-3476(99)70457-9
12. Grond S, Radbruch L, Lehmann KA. Clinical pharmacokinetics of transdermal opioids: focus on transdermal fentanyl. Clin Pharmacokinet. 2000;38:59–89. doi:10.2165/00003088-200038010-00004
13. Pettifer GR, Hosgood G. The effect of inhalant anesthetic and body temperature on peri-anesthetic serum concentrations of transdermally administered fentanyl in dogs. Vet Anaesth Analg. 2004;31(2):109–120. doi:10.1111/j.1467-2987.2004.00158.x
14. Kyles AE, Papich M, Hardie EM. Disposition of transdermally administered fentanyl in dogs. Am J Vet Res. 1996;57:715–719.
15. Egger CM, Glerum LE, Allen SW, Haag M. Plasma fentanyl concentrations in awake cats and cats undergoing anesthesia and ovariohysterectomy using transdermal administration. Vet Anaesth Analg. 2003;30(4):229–236. doi:10.1046/j.1467-2995.2003.00109.x
16. Mather LE. Clinical pharmacokinetics of fentanyl and its newer derivatives. Clin Pharmacokinet. 1983;8(5):422–446. doi:10.2165/00003088-198308050-00004
17. Hess R, Herz A, Friedel K. Pharmacokinetics of fentanyl in rabbits in view of the importance for limiting the effect. J Pharmacol Exp Ther. 1971;179:474–484.
18. Camu F, Vanlersberghe C. Pharmacology of systemic analgesics. Best Pract Res Clin Anaesthesiol. 2002;16(4):475–488. doi:10.1053/bean.2002.0262
19. FDA. Duragesic: fentanyl transdermal system[EB/OL]; 2005. Available from: http://www.fda.gov/cder/foi/label/2005/19813s039lb.lpdf.
20. Moore RA, Hand CW, McQuay HJ. Opiate metabolism and excretion. Bailliere’s Clin Anaesthesiol. 1987;1:829. doi:10.1016/S0950-3501(87)80038-7
21. Fallon M, Giusti R, Aielli F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29:iv166–iv91. doi:10.1093/annonc/mdy152
22. 2021 NCCN Adult Cancer Pain. Version 1.2021, 02/26/2021 © 2021 National Comprehensive Cancer Network® (NCCN®). NCCN Clinical Practice Guidelines in Oncology-Adult Cancer Pain. (2021 Version2) [DB/OL]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/pain.pdf.
23. Mercadante S. Options for treating pain in cancer patients with dysphagia. Drugs. 2017;77(6):629–635. doi:10.1007/s40265-017-0710-8
24. Xing S-Z, Zhang Y. Efficacy and safety of transdermal fentanyl for the treatment of oral mucositis pain caused by chemoradiotherapy in patients with esophageal squamous cell carcinoma. Support Care Cancer. 2015;23(3):753–759. doi:10.1007/s00520-014-2419-5
25. Guo S-P, Wu S-G, Zhou J, et al. Transdermal fentanyl for pain due to chemoradiotherapy-induced oral mucositis in nasopharyngeal cancer patients: evaluating efficacy, safety, and improvement in quality of life. Drug Des Devel Ther. 2014;8:497–503. doi:10.2147/DDDT.S60187
26. Wang YQ, Wang MJ, Qiu ZM. Application of transdermal fentanyl patch in cancer pain patients with renal insufficiency. J Pract Cancer. 2012;27:529–53v.
27. Cheng Yi YS. The selective use of opioids in patients with liver and kidney dysfunction and cancer pain. Chin J Cancer. 2020;20:43–47.
28. Yu SY, Qin SK, Xie GR. Expert consensus on the treatment of advanced cancer patients with intestinal obstruction. Chin J Cancer. 2007;29:637–640.
29. Miyoshi T, Yamauchi H, Misumi N. [Efficacy and safety of transdermal fentanyl patches for opioid initiation in patients with gastrointestinal obstruction]. Gan Kagaku Ryoho. 2014;41(11):1401–1405. Japan.
30. Yang Q, Xie D, Jiang ZM. Efficacy and adverse effects of transdermal fentanyl and sustained-release oral morphine in treating moderate-severe cancer pain in Chinese population: a systematic review and meta-analysis. J Exper Clin Cancer Res. 2010;29:67. doi:10.1186/1756-9966-29-67
31. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–e68. doi:10.1016/S1470-2045(12)70040-2
32. Wang DD, Ma TT, Zhu HD, Peng CB. Transdermal fentanyl for cancer pain: trial sequential analysis of 3406 patients from 35 randomized controlled trials. J Cancer Res Ther. 2018;14:S14–S21. doi:10.4103/0973-1482.171368
33. Hadley G, Derry S, Moore RA, Wiffen PJ. Transdermal fentanyl for cancer pain. Cochrane Database Syst Rev. 2013;2013:CD010270. doi:10.1002/14651858.CD010270.pub2
34. Liu JY, Xue J, Zhu T. Risk comparison of morphine sulfate sustained-release tablets, oxycodone hydrochloride sustained-release tablets and fentanyl transdermal patch in the treatment of cancer pain and constipation. China Pharm. 2015;16:316–318.
35. Megens AA, Artois K, Vermeire J, Meert T, Awouters FH. Comparison of the analgesic and intestinal effects of fentanyl and morphine in rats. J Pain Symptom Manage. 1998;15:253–257. doi:10.1016/S0885-3924(97)00371-0
36. 2021 NCCN Adult Cancer Pain. Version 1.2021, 02/26/2021 © 2021 National Comprehensive Cancer Network® (NCCN®). NCCN Clinical Practice Guidelines in Oncology-Adult Cancer Pain. (2021 Version2) [DB/OL]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/pain.pdf.PMID:34551388.
37. Bemard B. Is transdermal fentanyl really better than sustained oral morphine. BMJ. 2015;322:1154–1158.
38. Kang JH, Oh SY, Song S-Y, et al. The efficacy of low-dose transdermal fentanyl in opioid-naive cancer patients with moderate-to-severe pain. Korean J Intern Med. 2015;30(1):88–95. doi:10.3904/kjim.2015.30.1.88
39. Fu Q, Ran FM, Wang JZ. Clinical efficacy and safety of fentanyl transdermal patch in the treatment of moderate to severe cancer pain within 3 days. Cancer Progress. 2014;4:317.
40. Yalcin S, Esin E. Neuropathic cancer pain: what we are dealing with? How to manage it. Oncot Ther. 2014;4:599–618. doi:10.2147/OTT.S60995
41. Vuong C, Van Uum SH, O’Dell LE, Lutfy K, Friedman TC. The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr Rev. 2010;31:98–132. doi:10.1210/er.2009-0009
42. Toru H. Molecular mechanisms of bone cancer pain. ClinCalc. 2014;24:1185–1191.
43. El Mouedden M, Meert TF. The impact of the opioids fentanyl and morphine on nociception and bone destruction in a murine model of bone cancer pain. Pharmacol Biochem Behav. 2007;87:30–40. doi:10.1016/j.pbb.2007.03.017
44. Yu SY, Sun Y, Wu YL. Clinical efficacy analysis of transdermal fentanyl patch in the treatment of 4492 cases of cancer pain. Chin J Cancer. 2005;27:369–372.
45. Cancer Clinical Chemotherapy Committee of China Anti Cancer Association. Cancer Support Therapy Committee of China Anti Cancer Association Chinese expert consensus on the prevention and treatment of nausea and vomiting related to tumor drug therapy (2019 edition). Chin J Med Front. 2019;11:16–26.
46. Jee YS, Yoon HJ, Jang CH. Prophylactic antiemetic effects in gynecologic patients receiving fentanyl IV-patient controlled analgesia: comparison of combined treatment with ondansetron and dexamethasone with metoclopramide and dexamethasone. Korean J Anesthesiol. 2010;59:335–339. doi:10.4097/kjae.2010.59.5.335
47. Nelson AD, Camilleri M. Opioid induced constipation: advances and clinical guidance. Ther Adv Chronic Dis. 2016;7:121–134. doi:10.1177/2040622315627801
48. G. JJ, Akbaral H. Molecular physiology of enteric opioid receptors. Am J Gastroenterol Suppl. 2014;2:17–21. doi:10.1038/ajgsup.2014.5
49. Yan L, Liu H, Yan R, Tan L, Tan J, Lei Y. Effect of traditional Chinese medicine external therapy for functional constipation: a meta-analysis. Am J Transl Res. 2023;15:13–26.
50. Ziesenitz VC, Vaughns JD, Koch G, Mikus G, van den Anker JN. Pharmacokinetics of fentanyl and its derivatives in children: a comprehensive review. Clin Pharmacokinet. 2018;57:125–149. doi:10.1007/s40262-017-0569-6
51. Paut O, Camboulives J, Viard L, Lemoing JP, Levron JC. Pharmacokinetics of transdermal fentanyl in the peri-operative period in young children. Anaesthesia. 2000;55:1202–1207. doi:10.1046/j.1365-2044.2000.01615-3.x
52. Lynn W, Megan A, Gregory S. Modafinil treatment of opioid-induced sedation. Pain Med. 2010;10:135–140.
53. Meng SQ, Shi J. Abuse of pharmaceutical drugs and its prevention. Fa Yi Xue Za Zhi. 2021;37:788–795.
54. Heal DJ, Smith SL, Henningfield JE. CNS stimulants. Neuropharmacology. 2014;87:1–3. doi:10.1016/j.neuropharm.2014.09.025
55. Dackis CA, Gold MS. Addictiveness of central stimulants. Adv Alcohol Subst Abuse. 1990;9:9–26. doi:10.1300/J251v09n01_02
56. Ibrahim AM, Obaidi Z, Ruan G, Adaramola D, Onguti S. Nalbuphine for opioid-induced urine retention. Ann Intern Med. 2018;169:894–895. doi:10.7326/L18-0387
57. Kim B, Sciascia T, Yosipovitch G. The role of kappa- and mu-opioid receptors in pruritus. SKIN J Cutaneous Med. 2021;5:s31.
58. Morita T, Tei Y. Skin reaction to both morphine and fentanyl attenuated by steroids and antihistaminics. J Pain Symptom Manage. 2006;32(2):100–101. doi:10.1016/j.jpainsymman.2006.04.002
59. Vertigo professional committee of Chinese medical education association, emergency physician branch of Chinese medical doctor association guidelines for emergency diagnosis and treatment of vertigo (2021). Chin J Emerg Med. 2021;30:402–406.
60. Sharma V, Simpson SH, Samanani S, Jess E, Eurich DT. Concurrent use of opioids and benzodiazepines/Z-drugs in Alberta, Canada and the risk of hospitalisation and death: a case cross-over study. BMJ Open. 2020;10(11):e038692. doi:10.1136/bmjopen-2020-038692
61. Liu EY, Tamblyn R, Filion KB, Buckeridge DL. Concurrent prescriptions for opioids and benzodiazepines and risk of opioid overdose: protocol for a retrospective cohort study using linked administrative data. BMJ Open. 2021;11(2):e042299. doi:10.1136/bmjopen-2020-042299
62. Ziesenitz VC, Konig SK, Mahlke NS, Skopp G, Haefeli WE, Mikus G. Pharmacokinetic interaction of intravenous fentanyl with ketoconazole. J Clin Pharmacol. 2015;55(6):708–717. doi:10.1002/jcph.469
63. Nozari A, Akeju O, Mirzakhani H, et al. Prolonged therapy with the anticonvulsant carbamazepine leads to increased plasma clearance of fentanyl. J Pharm Pharmacol. 2019;71:982–987. doi:10.1111/jphp.13079
64. Kuip EJ, Zandvliet ML, Koolen SL, Mathijssen RH, van der Rijt CC. A review of factors explaining variability in fentanyl pharmacokinetics; focus on implications for cancer patients. Br J Clin Pharmacol. 2017;83:294–313. doi:10.1111/bcp.13129
65. Geist MJP, Ziesenitz VC, Bardenheuer HJ, Burhenne J, Skopp G, Mikus G. Minor contribution of cytochrome P450 3A activity on fentanyl exposure in palliative care cancer patients. Sci Rep. 2019;9:14635. doi:10.1038/s41598-019-51279-6
66. Baneyx G, Parrott N, Meille C, Iliadis A, Lave T. Physiologically based pharmacokinetic modeling of CYP3A4 induction by rifampicin in human: influence of time between substrate and inducer administration. Eur J Pharm Sci. 2014;56:1–15. doi:10.1016/j.ejps.2014.02.002
67. Kokko H, Hall PD, Afrin LB. Fentanyl-associated syndrome of inappropriate antidiuretic hormone secretion. Pharmacotherapy. 2002;22(9):1188–1192. doi:10.1592/phco.22.13.1188.33526
68. Rastogi R, Swarm RA, Patel TA, Riou B. Case scenario: opioid association with serotonin syndrome: implications to the practitioners. Anesthesiology. 2011;115(6):1291–1298. doi:10.1097/ALN.0b013e31823940c0
69. Kitamura S, Kawano T, Kaminaga S, et al. Effects of fentanyl on serotonin syndrome-like behaviors in rats. J Anesth. 2016;30:178–182. doi:10.1007/s00540-015-2092-y
70. Baldo BA. Opioid analgesic drugs and serotonin toxicity (syndrome): mechanisms, animal models, and links to clinical effects. Arch Toxicol. 2018;92(8):2457–2473. doi:10.1007/s00204-018-2244-6
71. Rickli A, Liakoni E, Hoener MC, Liechti ME. Opioid-induced inhibition of the human 5-HT and noradrenaline transporters in vitro: link to clinical reports of serotonin syndrome. Br J Pharmacol. 2018;175(3):532–543. doi:10.1111/bph.14105
72. Kim JH, Kim M, Sung CW, et al. High-dose fentanyl patch for cancer pain of a patient with cholangiocarcinoma. Korean J Intern Med. 2010;25(3):337–340. doi:10.3904/kjim.2010.25.3.337
73. Dai YM, Cui TJ, Lin GS. Clinical observation of high-dose fentanyl transdermal patch in the treatment of advanced cancer pain. Mod Tumor Med. 2016;24:138–139.
74. Pergolizzi J, H. BR, Budd K, et al. Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain Pract. 2008;8:287–313. doi:10.1111/j.1533-2500.2008.00204.x
75. Singleton MA, Rosen JI, Fisher DM, Kitamura S, Kawano T, Kaminaga S. Pharmacokinetics of fentanyl in the elderly. Br J Anaesth. 1988;60:178–182. doi:10.1093/bja/60.6.619
76. H. SS, Ghosh P, Newman B, et al. On the road to development of an in Vitro Permeation Test (IVPT) model to compare heat effects on transdermal delivery systems: exploratory studies with nicotine and fentanyl. Pharm Res. 2017;34:1817–1830. doi:10.1007/s11095-017-2189-0
77. Chinese nursing society, expert consensus on nursing guidance for cancer pain patients (2017 edition). Chin J Nurs Manag. 2017;17:1585–1586.
78. Zhang HZ, Yu HY, Wen CD. Application and effect analysis of information-based whole process management in outpatient cancer pain management. Hosp Manag Forum. 2019;272:73–75.
79. Li WJ, Liu JY, Si Q. The development and change of the concept of cancer pain drug treatment. J Med. 2021;40:45–51.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.