")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Guidance Value of Procalcitonin Detection in Selecting Switching Points for Sequential Therapy in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease Complicated by Respiratory Failure
Authors Ding F, Liu W, Wang H, Wang W, Yang C
Received 11 March 2022
Accepted for publication 28 August 2022
Published 18 October 2022 Volume 2022:17 Pages 2693—2699
DOI https://doi.org/10.2147/COPD.S366028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Min Zhang
Fang Ding,1 Wenjing Liu,2 Huiqing Wang,3 Weiwei Wang,1 Caixia Yang1
1Department of Geriatrics, Hengshui People’s Hospital, Hengshui City, Hebei Province, People’s Republic of China; 2Department of Respiratory Medicine, Hengshui People’s Hospital, Hengshui City, Hebei Province, People’s Republic of China; 3Department of Intensive Care Medicine, Hengshui People’s Hospital, Hengshui City, Hebei Province, People’s Republic of China
Correspondence: Fang Ding, Department of Geriatrics, Hengshui People’s Hospital, No. 180, Renmin East Road, TaoCheng District, Hengshui City, Hebei Province, 053000, People’s Republic of China, Tel +86 0318-2187239, Email [email protected]
Objective: To analyse the guiding value of procalcitonin (PCT) for the selection of ventilation switching points in sequential mechanical ventilation for patients with acute exacerbation of chronic obstructive pulmonary disease (COPD) and respiratory failure, and to provide a reference for the optimisation of mechanical ventilation for patients with COPD and respiratory failure.
Methods: The study included 160 patients with an acute exacerbation of COPD complicated by respiratory failure who received sequential mechanical ventilation treatment. They were divided into two groups of 80 participants. The critical point of the pulmonary infection observation window (PIC) was used as the switching point for sequential mechanical ventilation treatment in the control group, and PCT clinical node was used as the switching point for sequential mechanical ventilation treatment in the observation group. The invasive ventilation time, non-invasive mechanical ventilation time, total mechanical ventilation time, intensive care unit (ICU) treatment time, complication rate and prognosis were compared for the two groups.
Results: (1) There was no significant difference in the respiratory rate, heart rate, arterial systolic pressure, arterial oxygen partial pressure, arterial carbon dioxide partial pressure or pH value between the two groups after 1 day of treatment, and (2) invasive mechanical ventilation time, non-invasive mechanical ventilation time, total mechanical ventilation time, ICU treatment time and the incidence of complications were significantly different in the two groups (P = 0.0001).
Conclusion: Detecting PCT can guide the selection of ventilation switching points in sequential mechanical ventilation therapy for patients with COPD with respiratory failure in the acute exacerbation stage, effectively reduce the misevaluation of PIC switching points so that patients can obtain stable criteria for judgement and effectively improve the efficiency and safety of mechanical ventilation treatment for patients in the acute exacerbation stage.
Keywords: acute exacerbation of chronic obstructive pulmonary disease, respiratory failure, sequential mechanical ventilation, selection of ventilation mode switching point, procalcitonin, observation window of pulmonary infection, clinical value
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most common chronic respiratory diseases among elderly patients. Its clinicopathological manifestations are pathological changes in the airways, lung parenchyma and pulmonary vasculature. Patients exhibit the clinical symptoms of airflow limitation, such as dyspnoea, cough and expectoration, accompanied by shortness of breath, panting and fatigue, which have serious impacts on patients’ daily lives, work and study.1 Patients with an acute exacerbation of COPD combined with respiratory failure have progressed to a critical condition, and admission to an intensive care unit (ICU) for monitoring and mechanical ventilation treatment is one of the most important elements of clinical treatment. Mechanical ventilation is divided into two types: non-invasive and invasive.2 Invasive mechanical ventilation is of great value in clinical practice for the rescue of critically ill patients. It has many advantages, such as good airtightness, ease of achieving airway management goals, good human–machine cooperation and rapid improvement of airway symptoms, but its long-term use can also produce substantial complications and adverse events such as ventilator dependence. Sequential mechanical ventilation is the most common treatment for acute exacerbation of COPD combined with respiratory failure, and its efficiency and safety have been clinically proven to be much higher than that of conventional mechanical ventilation.3 However, how to switch from invasive mechanical ventilation to non-invasive ventilation smoothly and safely is an important clinical issue. In this study, procalcitonin (PCT) was used as a criterion to guide the selection of the switching point, and the feasibility and clinical value of PCT for guiding the switching point were investigated by comparing it with the commonly used pulmonary infection control (PIC) window.
Materials and Methods
Clinical Data
A total of 160 patients with acute exacerbation COPD combined with respiratory failure who underwent sequential treatment with mechanical ventilation in Hengshui People’s Hospital between January 2019 and June 2020 were selected as the study subjects. They were numbered according to their order of enrolment, with odd numbers allocated to the observation group and even numbers allocated to the control group, with 80 participants in each group. There were 75 male participants and 85 female participants, all aged 38–74 years. This study was approved by the Medical Ethics Committee of our Hospital.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) All patients met the diagnostic criteria for an acute exacerbation of COPD according to the “Guidelines for the Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease” (2013 Revision)4 as well as the indications for admission to the ICU for treatment: a. severe dyspnoea with poor improvement of clinical symptoms after initial treatment, b. drowsiness or coma and other impairments of consciousness at the time of consultation, and c. PaO < 50 mmHg and/or PaCO2 > 70 mmHg after oxygen inhalation or non-invasive simultaneous treatment and continued deterioration, and/or pH < 7.30 or even deteriorated; (2) the consultation occurred less than 8 hours after the acute attack; (3) no serious cardiac, hepatic, renal, metabolic or haematologic diseases; (4) normal cognitive and neurological functions and able to understand and cooperate with medical staff in the assessment of relevant indicators and scales; (5) met the indications for sequential mechanical ventilation; and (6) patients and/or family members understood the advantages and disadvantages of participating in this study and signed an informed consent form. Exclusion criteria: (1) Those with a history of thoracic or abdominal surgery within 1 year prior to enrolment; (2) those with other factors that the investigator believed would affect the study’s results; or (3) those with incomplete clinical data collection.
Methods
All patients were given the conventional treatment for acute exacerbation of COPD combined with respiratory failure after the diagnosis and assessment of the indications for ICU admission, including drug therapies such as antibiotics, prednisolone or anticholinergics, expectoration, airway clearance and drainage, and correction of water-electrolyte disorders according to the patient’s condition. At the same time, invasive mechanical ventilation was performed using a low-level pressure support mode, with inspiratory pressure ≥25 cmH2O and expiratory pressure ≤5 cmH2O, maintaining positive end-expiratory pressure ventilation and inhaled oxygen concentration in a constant range. The control group used the PIC window threshold as the switching point of sequential mechanical ventilation treatment, and the observation group used the PCT clinical node as the switching point of sequential mechanical ventilation treatment.
PCT Detection Guided the Ventilation Switching Point in the Observation Group
Patients received daily bedside chest X-rays after the invasive ventilation treatment, and peripheral blood was collected to measure the PCT level in the serum using a double antibody sandwich enzyme-linked immunosorbent assay (Procalcitonin Human ELISA Kit, Invitrogen). When the PCT in peripheral blood was less than 0.25 μg/L, the sputum volume became thin, and the chest radiograph showed significant absorption of lung infection, the PCT window was judged, and the patient was switched to non-invasive ventilation treatment. Patients were readmitted to invasive mechanical ventilation if they experienced respiratory or cardiac arrest, their consciousness was impaired, PaCO2 > 45 mmHg after oxygen therapy, pH ≤ 7.2, breath rate ≥ 140 breaths/min or ≤7 breaths/min occurred after non-invasive ventilation.
PIC Assessment Guided the Ventilation Switching Point in the Control Group
During the invasive ventilation period, patients received daily bedside chest X-rays, patients’ body temperatures were monitored, peripheral blood was collected for leukocyte counts and daily sputum volume and appearance traits were observed by trained and experienced clinicians. A rebounded complex temperature, decreased white blood cell count, X-rays showing absorption of infection, significantly reduced sputum volume and whitened or less viscous sputum were judged to be a window of control for pulmonary infection, and conversion to non-invasive ventilation was performed. Patients were converted to invasive ventilation if they presented with the indications for invasive ventilation mentioned in 1.3.1.
Observation Indexes and Methods
The blood and hemodynamic indexes of the two groups were compared after 1 day of sequential mechanical ventilation treatment, and the invasive ventilation time, non-invasive mechanical ventilation time, total mechanical ventilation time, ICU treatment time, complication rate and patient mortality of the two groups were statistically analysed and compared. Blood gas and hemodynamic monitoring: Patients’ hemodynamic indexes, including respiratory rate, heart rate and arterial systolic pressure, were collected as observation indexes at fixed times after 1 day of treatment, and their arterial partial pressure of oxygen, arterial partial pressure of carbon dioxide and pH were collected as observation indexes for blood gas indexes.
Statistical Analysis
All data were processed and analysed using SPSS 20.3. The measurement data that conformed to a normal distribution were described by mean ± standard deviation (x ± SD), and the t-test for independent samples was used for a comparison of the two groups. The count data were described by the rate or composition ratio (%), and a chi-square test was performed to compare the groups; P < 0.05 was considered a statistically significant difference.
Results
Comparison of Hemodynamic Indexes and Blood Gas Indexes After 1 Day of Treatment
The differences in arterial oxygen partial pressure, arterial carbon dioxide partial pressure and pH after 1 day of treatment were not statistically significant in either group (P > 0.05), as shown in Table 1.
 |
Table 1 Comparison of Hemodynamic Indexes and Blood Gas Indexes After 1 Day of Treatment Between the Two Groups (n=80) |
Comparison of the Duration of Different Treatment Phases
The invasive mechanical ventilation time (7.59 ± 2.45 vs 13.35 ± 3.37), non-invasive mechanical ventilation time (6.78 ± 1.97 vs 12.63 ± 2.32), total mechanical ventilation time (16.73 ± 4.42 vs 21.52 ± 5.73) and ICU treatment time (18.28 ± 4.53 vs 26.15 ± 5.94) were lower in the observation group than in the control group, and the differences were statistically significant (P < 0.05). See Table 2.
 |
Table 2 Comparison of Duration of Different Treatment Phases Between the Two Groups (n=80) |
Comparison of Complication Rates Related to Mechanical Ventilation During Treatment
A comparison of the complication rates related to mechanical ventilation during treatment shows that more patients in the control group had ventilator-associated pneumonia (five cases) and airway obstruction (four cases), whereas some patients in the observation group had hypoventilation (four cases). The complication rate in the observation group was lower than that in the control group (P < 0.05), as shown in Table 3.
 |
Table 3 Comparison of Complication Rates Related to Mechanical Ventilation During Treatment in the Two Groups (n=80) |
Comparison of the Prognosis of Patients
The mortality rate was 6.25% in the control group and 5.00% in the observation group, and there was no statistically significant difference in the quality of prognosis between the two groups (P > 0.05), as shown in Table 4.
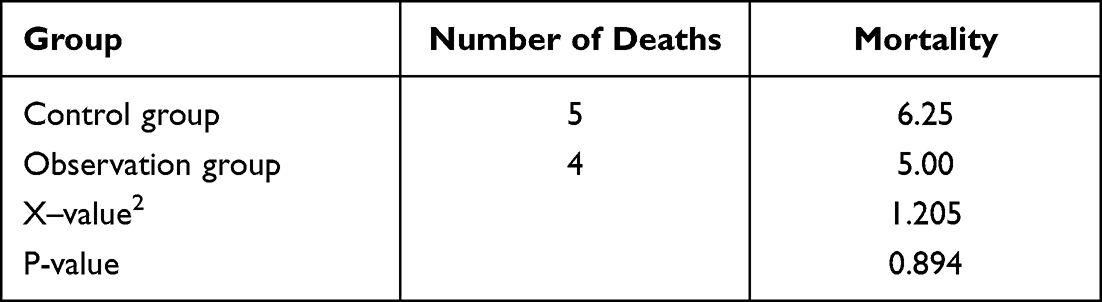 |
Table 4 Comparison of the Mortality of Patients in the Two Groups (n=80) |
Discussion
With the ageing of the population, the deterioration of environmental air, and unhealthy dietary and behavioural habits, the incidence of COPD is on the rise,5 and COPD has been assessed to be the third deadliest disease in the world by the Global Burden of Disease Research Project. According to the World Bank and World Health Organization, COPD ranked fifth among global diseases and burdens in 2020. The goals of COPD prevention and treatment are to reduce patient pain, improve quality of life and reduce the rate of death and disability.6 Patients with COPD can be divided according to the course of the disease into those with acute exacerbations and those in chronic stable phases. Patients with COPD are clinically considered to be in an acute exacerbation stage if they present with a continuous deterioration of respiratory symptoms compared with the daily variation range, and they require drug therapy to change the course of deterioration, with aggravations of coughing, shortness of breath and/or wheezing, purulent mucus in sputum and fever in a short period of time.7 The most common causes of acute exacerbation of COPD are viral and bacterial infections of the airways and bronchi.8 Patients with COPD with acute exacerbation are more likely to develop respiratory failure as their disease progresses, and those with PaO < 60 mmHg and/or PaCO2 > 50 mmHg are clinically considered to be in respiratory failure. Admission to an ICU for mechanical ventilation and close monitoring is required when PaO < 50 mmHg and/or PaCO2 > 70 mmHg and pH < 7.30. Mechanical ventilation is an important measure for patients with acute exacerbation COPD combined with respiratory failure, and sequential mechanical ventilation is now widely used in clinical practice to improve the accuracy of treatment, reduce ventilator-related complications and reduce unnecessary additional harm to patients.9
The timing of switching from invasive to non-invasive ventilation has always been a challenge in sequential mechanical ventilation therapy, as prolonged retention of invasive ventilation increases the incidence of complications, whereas a premature change from invasive to non-invasive ventilation may result in secondary intubation caused by an inability to maintain ventilation.10 About 80–90% of acute exacerbations experienced by patients with COPD in China are caused by respiratory tract infections.11 Therefore, many clinical scholars have proposed the use of the PIC window as the switching point.12,13 When the patient’s pulmonary infection is effectively controlled, the condition is effectively relieved, and the patient can gradually resume spontaneous breathing. The transition to non-invasive ventilation at this stage is more conducive to the patient’s respiratory function recovery. However, the clinical application process shows that the PIC window is highly subjective, leading to great difficulties for clinical unification and standardisation.14 Finding a more objective, convenient and accurate index to guide the switching point has become an important clinical issue.15
The levels of PCT, which is a small molecule, are elevated in plasma in severe bacterial, fungal and parasitic infections. PCT can therefore be used as a biomarker for bacterial infections, and it is also able to respond to the active level of inflammatory response in the body. Some studies have found that patients with acute exacerbation COPD combined with respiratory failure develop a systemic inflammatory response, and an elevated PCT level is an indicator of oxidative stress and an inflammatory immune response in patients, providing an effective guide for stopping or starting antibiotics in patients with acute respiratory infections.16–18 A meta-analysis also showed that PCT-based protocols used to guide the usage of antibiotics in patients with COPD with acute exacerbations appeared to be clinically effective and safe. In addition, the concentration of PCT in the normal human body is very small, is stable when secreted, is independent of age, sex and other factors, is not affected by systemic steroids and may be an objective indicator for determining the ventilation switching point. The results of previous studies have shown that using the change rate of PCT as an indicator to switch the ventilation mode can reduce the reintubation rate, duration of invasive ventilation support and total time of mechanical ventilation support.19,20 Furthermore, the duration of non-invasive mechanical ventilation is also reduced, which might occur because PCT levels improve the prediction of infection control and provide an enhanced recovery. Patients with invasive ventilation treatment should have peripheral blood collected daily to measure and monitor the PCT level Based on the above findings, this study further investigated the value of PCT in the selection of ventilation mode switching points in patients with acute exacerbation COPD combined with respiratory failure by studying hemodynamic and blood gas indexes, treatment duration and related complications.
The results showed that PCT was more advantageous than PIC switching point selection in improving the efficiency of treatment, effectively reducing the incidence of ventilator-related complications in patients and the duration of each phase of treatment. Moreover, the PCT laboratory monitoring index is more objective, effectively reducing the influence of different physicians’ qualifications and experience levels on the results.
This was a single-centre non-randomised controlled study. This study has some limitations, such as small sample size, non-randomised grouping, non-blinded design and a lack of comparison of the distribution of underlying diseases between the two groups, which may lead to selection and admission rate bias, causing the results to be inconsistent with the true situation. It is expected that multi-centre randomised controlled trials and double-blind experiments will be conducted in the future, and the factors that influence PIC switching point selection will be explored to provide more adequate evidence for the application of PIC switching points in clinics.
In conclusion, it is important to detect PCT levels to guide the ventilation mode switching point for sequential mechanical ventilation therapy in patients with acute exacerbation COPD combined with respiratory failure. This method effectively reduces the arbitrariness of the subjective scoring of PIC switching point guidance, enables patients to obtain stable judgement criteria and effectively improves the efficiency and safety of mechanical ventilation therapy for patients.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Hengshui People’s Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Project of Hebei Provincial Health Department Project No. 20191760.
Disclosure
The authors report no personal, financial, commercial, or academic conflicts of interest in this work.
References
1. Labaki WW, Rosenberg SR. Chronic Obstructive Pulmonary Disease. Ann Intern Med. 2020;173(3):ITC17–ITC32. doi:10.7326/AITC202008040
2. Kang NM, Zhang N, Luo BJ, et al. Sequential non-invasive following short-term invasive mechanical ventilation in the treatment of tuberculosis with respiratory failure: a randomized controlled study. BMC Pulm Med. 2021;21(1):203. doi:10.1186/s12890-021-01563-x
3. Zhu RQ. Clinical efficacy of sequential treatment of severe chronic obstructive pulmonary type II respiratory failure with invasive ventilator and noninvasive ventilator. Chinese and Foreign Medical Care. 2017;36(36):72–73.
4. Vestbo J, Hurd SS, Rodriguez-Roisin R, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
5. Chronic Respiratory GBD, Kendrick PJ, Paulson KR, Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
6. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
7. Chronic Obstructive Pulmonary Disease Committee, Chinese Medical Association. Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease (2013 revised edition). Chin J Front Med. 2014;6(02):67–80.
8. Hao JJ. Clinical study of cefoxitin sodium cefixime sequential treatment for acute exacerbation of chronic obstructive pulmonary disease. J Math Med. 2018;31(09):1341–1343.
9. Ahmed SM, Athar M. Mechanical ventilation in patients with chronic obstructive pulmonary disease and bronchial asthma. Indian J Anaesth. 2015;59(9):589–598. doi:10.4103/0019-5049.165856
10. Zhao ZG. Clinical study of invasive-noninvasive sequential ventilation therapy for severe respiratory failure caused by chronic obstructive pulmonary disease. Information Medicine. 2018;31(11):110–112.
11. Hu H, Ji Z, Qiang X, et al. Chinese medical injections for acute exacerbation of chronic obstructive pulmonary disease: a network meta-analysis. Int J Chron Obstruct Pulmon Dis. 2021;2021(16):3363–3386. doi:10.2147/COPD.S335579
12. Wang SN. Clinical Efficacy Evaluation of Respiratory Eight-Danjin on Sequential Treatment of Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Guangzhou University of Traditional Chinese Medicine; 2018.
13. Lv Y, Lv Q, Lv Q, et al. Pulmonary infection control window as a switching point for sequential ventilation in the treatment of COPD patients: a meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;2017(12):1255–1267. doi:10.2147/COPD.S126736
14. Qiao Z, Yu J, Zhang M, et al. The benefit of daily sputum suction via bronchoscopy in patients of chronic obstructive pulmonary disease with ventilators: a randomized controlled trial. Medicine. 2018;97(31):e11631. doi:10.1097/MD.0000000000011631
15. Motegi T, Jones RC, Ishii T, et al. A comparison of three multidimensional indices of COPD severity as predictors of future exacerbations. Int J Chron Obstruct Pulmon Dis. 2013;8:259–271. doi:10.2147/COPD.S42769
16. Schuetz P, Briel M, Christ-Crain M, et al. Procalcitonin to guide initiation and duration of antibiotic treatment in acute respiratory infections: an individual patient data meta-analysis. Clin Infect Dis. 2012;55(5):651–662. doi:10.1093/cid/cis464
17. Schuetz P, Wirz Y, Sager R, et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev. 2017;10(10):CD007498. doi:10.1002/14651858.CD007498.pub3
18. Pandey S, Garg R, Gaur P, et al. Serum procalcitonin levels in chronic obstructive pulmonary disease patients in North Indian Population. Ann Afr Med. 2019;18(2):103–107. doi:10.4103/aam.aam_44_18
19. Kim SH, Ahn HS, Park JS, et al. A proteomics-based analysis of blood biomarkers for the diagnosis of COPD acute exacerbation. Int J Chron Obstruct Pulmon Dis. 2021;1(16):1497–1508. doi:10.2147/COPD.S308305
20. Lin SH, He YP, Lian JJ, et al. Procalcitonin kinetics to guide sequential invasive-noninvasive mechanical ventilation weaning in patients with acute exacerbation of chronic obstructive pulmonary disease and respiratory failure: procalcitonin’s adjunct role. Libyan J Med. 2021;16(1):1961382. doi:10.1080/19932820.2021.1961382
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.