")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
GSTP1 rs4147581 C>G and NLRP3 rs3806265 T>C as Risk Factors for Chronic Obstructive Pulmonary Disease: A Case-Control Study
Authors Li H, Wang R, Wei X, Zhang C, Pei W, Zhang X, Yang Z, Li Z, Zhang Y, Shi Y, Wang Y, Wang X
Received 20 October 2023
Accepted for publication 31 January 2024
Published 22 February 2024 Volume 2024:19 Pages 489—500
DOI https://doi.org/10.2147/COPD.S445680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Honge Li,1,* Raorao Wang,1,* Xueyan Wei,1,* Chunyan Zhang,1 Wenhui Pei,1 Xuhui Zhang,2 Zhen Yang,1 Zhi Li,3 Yuhuan Zhang,1 Yanli Shi,1 Yunchao Wang,4 Xinhua Wang1
1Institute of Public Health, Gansu University of Chinese Medicine, Lanzhou, Gansu, People’s Republic of China; 2Department of Respiratory Medicine, Affiliated Hospital of Gansu University of Chinese Medicine, Lanzhou, Gansu, People’s Republic of China; 3The State Key Laboratory of Respiratory Disease, The First Affiliated Hospital, Institute of Public Health, Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 4Institute of Basic Medicine, Gansu University of Chinese Medicine, Lanzhou, Gansu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunchao Wang, Institute of Basic Medicine, Gansu University of Chinese Medicine, Lanzhou, Gansu, 730000, People’s Republic of China, Tel +86 18609404912, Email [email protected] Xinhua Wang, Institute of Public Health, Gansu University of Chinese Medicine, Lanzhou, Gansu, 730000, People’s Republic of China, Tel +86 13893602359, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a chronic respiratory ailment influenced by a blend of genetic and environmental factors. Inflammatory response and an imbalance in oxidative-antioxidant mechanisms constitute the primary pathogenesis of COPD. Glutathione S-transferase P1(GSTP1) plays a pivotal role as an antioxidant enzyme in regulating oxidative-antioxidant responses in the pulmonary system. The activation of the NOD-like receptor thermal protein domain (NLRP3) inflammatory vesicle can trigger an inflammatory response. Several investigations have implicated GSTP1 and NLRP3 in the progression of COPD; nonetheless, there remains debate regarding this mechanism.
Methods: Employing a case-control study design, 312 individuals diagnosed with COPD and 314 healthy controls were recruited from Gansu Province to evaluate the correlation between GSTP1 (rs4147581C>G and rs1695A>G) and NLRP3 (rs3806265T>C and rs10754558G>C) polymorphisms and the susceptibility to COPD.
Results: The presence of the GSTP1 rs4147581G allele substantially elevated the susceptibility to COPD (CGvs.CC:OR=3.11,95% CI=1.961– 4.935, P< 0.001;GGvs.CC:OR=2.065,95% CI=1.273– 3.350, P=0.003; CG+GGvs.CC:OR=2.594,95% CI=1.718– 3.916, P< 0.001). Similarly, the NLRP3rs3806265T allele significantly increased the susceptibility to COPD (TC:TT:OR=0.432,95% CI=0.296– 0.630; TC+CCvs.TT:OR=2.132,95% CI=1.479– 3.074, P< 0.001). However, no statistically significant association was discerned between the rs1695A>G and rs10754558G>C polymorphisms and COPD susceptibility (P> 0.05).
Conclusion: In summary, this study ascertained that the GSTP1 rs4147581C>G polymorphism is associated with increased COPD susceptibility, with the G allele elevating the risk of COPD. Similarly, the NLRP3 rs3806265T>C polymorphism is linked to elevated COPD susceptibility, with the T allele heightening the risk of COPD.
Keywords: chronic obstructive pulmonary disease, GSTP1, NLRP3, polymorphism
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by persistent respiratory symptoms and airflow limitation due to airway and/or respiratory disease, accompanied by dyspnea, cough, and sputum production.1–6 The global prevalence of COPD is 10.3%, with the prevalence among Chinese adults aged 40 years and older reaching as high as 13.6%, making it the third leading cause of death in the country.
The causes of COPD are complex, and its development is strongly associated with both genetic and environmental factors.7–9 Familial aggregation of COPD indicates the significant role of genetic factors in its development. Studies have indicated that only 10% to 20% of smokers eventually develop COPD, while 25% of COPD patients have never smoked.10–13 This suggests that COPD results from the interplay between genetic and environmental factors.14 Although the pathogenesis of COPD remains unclear, inflammation, protease-antiprotease imbalance, and oxidative-antioxidant imbalance are believed to be the primary mechanisms. Recently, Confalonieri et al propose to also include the concept of “structural changes due to failed regeneration by the distal airways progenitor cells” into the new definition of COPD “structural changes due to failed regeneration by the distal airways progenitor cells”.15 In recent years, several genetic polymorphisms have been linked to COPD development, including polymorphisms in glutathione S-transferase and inflammation-related genes.16,17
Glutathione S-transferase P1 (GSTP1) is a vital antioxidant enzyme highly expressed in the lungs.18,19 The GSTP1 gene, located on chromosome 11q13, has multiple single-nucleotide mutation sites.20 Polymorphisms at these mutant loci may impact their antioxidant function, leading to an oxidative-antioxidant imbalance that could induce COPD. Currently, there is controversy regarding the association between GSTP1 polymorphisms and COPD. While Yan and Ishii found an association, Yim and Yang’s study did not support a correlation between the two.21–26
The early immune response in the lungs against harmful stimuli is primarily mediated by inflammasomes, intracellular polyprotein complexes that recognize signals of injury and pathogens. NOD-like receptor thermal protein domain-associated protein 3 (NLRP3) is a crucial member of the inflammasome responsible for recognizing these signals.27 Mutations in the NLRP3 gene locus may result in abnormal inflammasome activation, leading to an excessive inflammatory response and exacerbating lung tissue damage.28–31 Faner et al and Eltom et al discovered that the rs35829419 mutation at the NLRP3 locus in lung tissues of COPD patients affects interactions with other proteins, further intensifying the inflammatory response and the release of inflammatory mediators.32,33 NLRP3 is also genetically polymorphic and has been linked to the development of several inflammatory diseases. However, although there are fewer studies on NLRP3 polymorphisms and COPD.34,35
In summary, COPD poses a heavy disease burden worldwide due to its high prevalence and mortality. However, the causes of COPD are complex, and its pathogenesis and causes have not been fully elucidated. Currently, it is mainly believed that the development of COPD is related to genes and environmental factors, and gene polymorphisms are also believed to be involved in many aspects of the pathogenesis of COPD. However, there is controversy at home and abroad about the association of GSTP1 gene polymorphisms with the risk of COPD and there are fewer studies on the association of NLRP3 gene polymorphisms with the risk of COPD. COPD is also less studied. Therefore, we conducted a case-control study in Gansu Province, including 312 COPD patients and 314 healthy controls, and used molecular epidemiological methods and real-time fluorescence quantitative PCR to analyse the association between GSTP1 and NLRP3 gene polymorphisms and COPD, with a view to providing theoretical basis for the early prevention programme and treatment of COPD-susceptible population.
Methods
Study Population
Between January 2020 and November 2022, we conducted a case-control study at the Affiliated Hospital of Gansu University of Traditional Chinese Medicine involving 312 COPD patients and 314 healthy controls from both rural and urban natural population cohorts in Gansu, the cases were mainly included in stable COPD patients with stable or mild symptoms such as cough, sputum, and shortness of breath. Our aim was to evaluate the association of GSTP1 (rs4147581C>G and rs1695A>G) and NLRP3 (rs3806265T>C and rs10754558G>C) polymorphisms in relation to COPD susceptibility.
Diagnostic Criteria and Pulmonary Function Tests for COPD
In accordance with the COPD Global Initiative for 2023, COPD is considered diagnosed when there are risk factors associated with dyspnea, cough, sputum production, and smoking, and the ratio of Forced Expiratory Volume in 1 second (FEV1) to Forced Vital Capacity (FVC), measured after a half-hour inhalation of 400 µg of salbutamol, falls below 70%. Pulmonary function tests were conducted using an EasyOne spirometer (NDD Medizintechnik AG, Switzerland) following the manufacturer’s instructions.36
Single Nucleotide Polymorphism (SNP) Selection and Genotyping
We identified potential risk SNPs by consulting the dbSNP database (http://www.ncbi.nlm.nih.gov/SNP) with the following selection criteria: SNPs located within the upper and lower 2000 bp of GSTP1 and NLRP3, Minor Allele Frequencies (MAFs) exceeding 0.05 in the Chinese population, and low linkage disequilibrium (LD, r2<0.8). Finally, we selected rs4147581C>G, rs1695A>G, rs3806265T>C, and rs10754558G>C for further analysis.
DNA extraction from collected peripheral blood samples was carried out using Tiangen Biochemical’s Blood Genomic DNA Extraction System Kit (DP349). Genotyping was performed using the TaqMan-MGB probe method. To ensure the reliability of PCR reactions, a negative control was included on each plate, and 10% of the samples were randomly selected for repeat testing.
Fluorescence-Based Quantitative PCR Technique
Mix configuration: Prepare PCR reaction mixture with Takara Premix Ex Taq™ (Probe qPCR) kit and vortex oscillation for 15 sec to mix the mixture well. Add sample: Standard DNA sample to 30 ng /μ l, add 18.5 μL PCR reaction mixture to 384 / 96 well plate, add l.5 μ l DNA template to 384 / 96 well plate, seal with sealing plate film and place at low speed, he centrifuwas centrifuged at 2000rpm for 2min. PCR amplification reaction: Place 384 / 96 well plate into 7900 HT quantitative PCR instrument / StepOnePlus quantitative PCR instrument and perform the following steps: Pre read → predenaturation 95°C 10min → denaturation 95°C 15s + annealing extension 60°C 1min (Repeat: 40 cycles) → 60°C 1min → Post read.
Methods of Statistical Analysis
Measurement data are presented as mean±standard deviation (X±SD), and count data are expressed as percentages (%). For group comparisons involving both categorical and continuous data, we employed χ2 tests and t-tests as appropriate.
In examining the association between genetic polymorphisms and COPD susceptibility, we utilized a multifactorial logistic regression model to calculate the odds ratio (OR) and its 95% confidence interval (CI). This analysis was adjusted for potential confounders such as age, gender, and smoking status. We conducted stratified analysis and interaction analysis for each stratum under each factor to assess the association between genotype and COPD risk. The Breslow-Day test was employed to evaluate heterogeneity between strata, with a significance level set at P<0.05. Statistical analysis was performed using SPSS version 25.0.
Results
Demographic Characteristics
Table 1 presents the demographic characteristics of our case-control study, including 312 COPD patients and 314 healthy controls in Gansu Province. Significant disparities in age, smoking status were observed between the two groups, with both demonstrating statistical significance (both P<0.05).
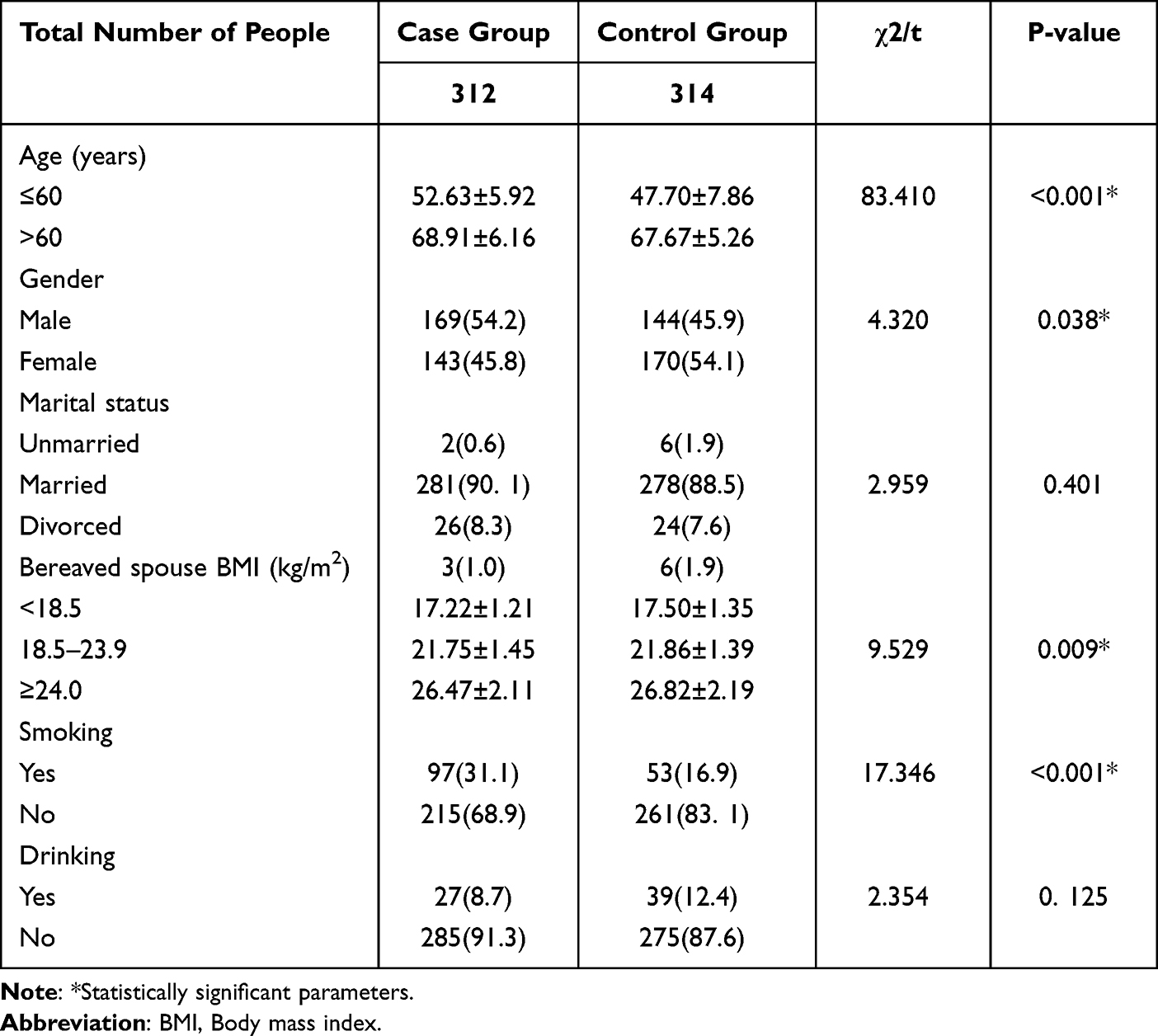 |
Table 1 Basic Demographic Characteristics of the Study Population |
Association Analysis of SNPs in the GSTP1 and NLRP3 Genes with the Risk of COPD
As depicted in Table 2, the GSTP1 rs4147581 G allele markedly elevated the risk of COPD within the Gansu Province, China population (CGvs.CC:OR=3.11,95% CI=1.961–4.935, P<0.001;GGvs.CC:OR=2.065,95% CI=1.273–3.350, P=0.003;CG+GGvs.CC:OR=2.594,95% CI=1.718–3.916, P<0.001). In contrast, the GSTP1 rs1695A allele did not demonstrate a significant association with COPD risk. Nevertheless, logistic regression analysis, adjusting for age, gender, smoking, and BMI, revealed that the GSTP1 rs1695A>G allele was linked to an increased COPD risk within the Gansu Province, China population (AG:AA: adjusted Odds Ratio (OR)=2.495, 95% CI=1.558–3.996;AG+GGvs.AA: adjusted Odds Ratio (OR)=2.619, 95% CI=1.428–3.294, both P<0.001).
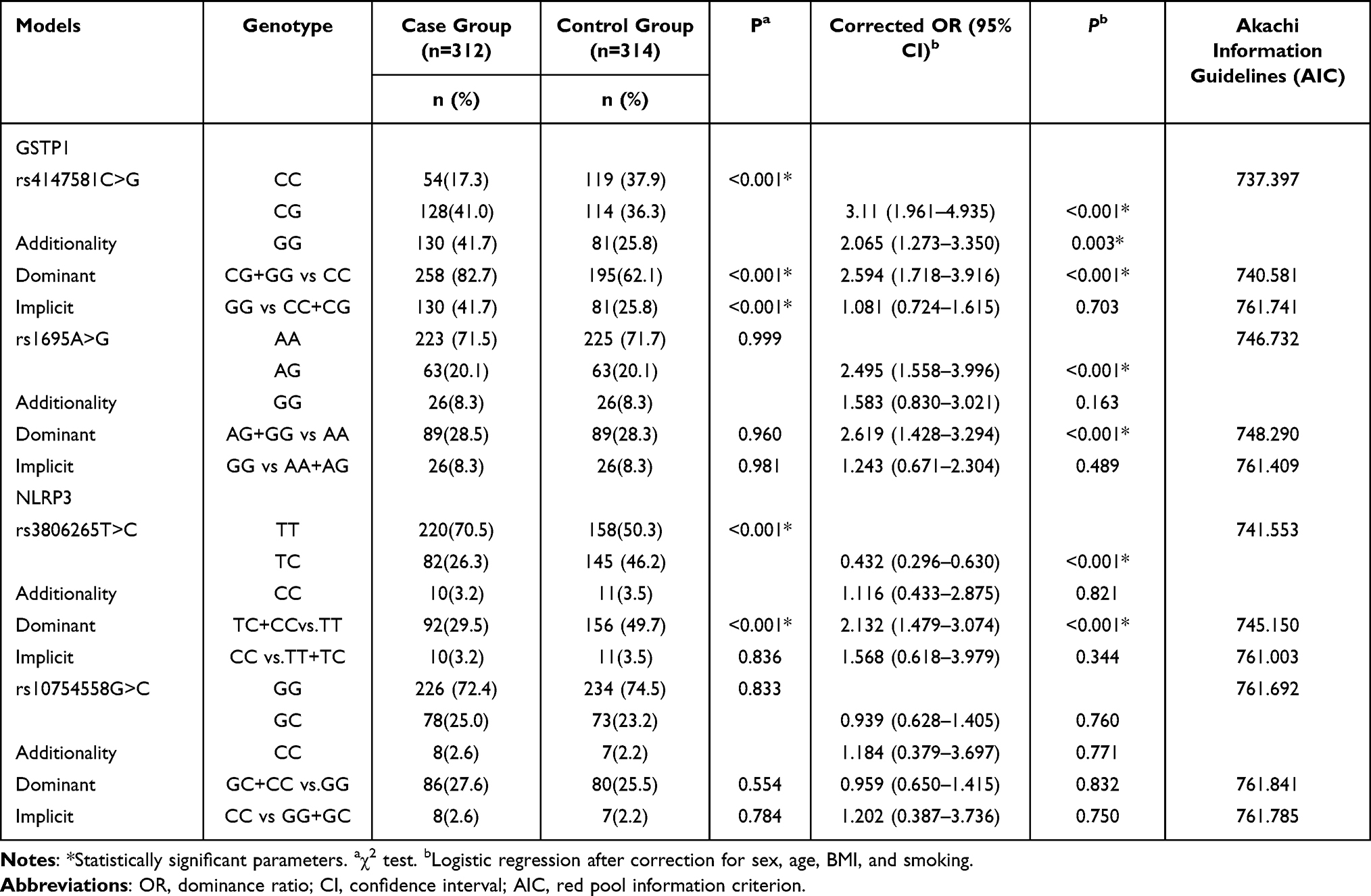 |
Table 2 Association of SNPs in GSTP1 and NLRP3 with COPD Susceptibility |
The NLRP3 rs3806265T allele was also associated with COPD risk within the Gansu Province, China population (TC:TT: OR=0.432,95% CI=0.296–0.630; TC+CCvs.TT: OR=2.132, 95% CI=1.479–3.074, both P<0.001). Conversely, no significant association was detected between rs10754558G>C and the prevalence of COPD.
Stratified Analysis and Interaction Analysis of SNPs and Risk of COPD
Stratification and Interaction Analysis of GSTP1 rs4147581C>G and COPD Prevalence Risk
Table 3 presents the findings from the stratification and interaction analysis. Rs4147581C>G in the dominant model, when comparing the CC genotype to the GG/GC genotype, we observed variations in COPD risk across different strata defined by age, sex, and smoking history. Notably, there was no homogeneity between the strata (P<0.05). In the population aged over 60 years, the CC genotype (GG+GCvs.CC: OR=11.176,95% CI = 5.709–21.879) significantly increased the risk of COPD. Similarly, in the male population (GG+GCvs.CC: OR=22.784,95% CI=6.883–75.418), in individuals with a smoking history (GG+GCvs.CC: OR=24.429,95% CI=5.389–110.737), and in those without a smoking history (GG+GCvs.CC: OR=1.979,95% CI=1.327–2.950), the CC genotype was associated with an elevated risk of COPD. Furthermore, in individuals without a smoking history (GG+GCvs.CC: OR=1.327–2.950), the CC genotype exhibited an increased risk of COPD. Regarding BMI, marital status, alcohol consumption, and a history of previous diseases, we observed homogeneity between strata (P>0.05). In these strata, the CC genotype in the dominant model was associated with an increased risk of COPD: BMI (GG+GCvs.CC: OR=2.862,95% CI=1.968–4.162), marital status (GG+GCvs.CC: OR=2.950, 95% CI=2.031–4.286), alcohol consumption (GG+GCvs.CC: OR=3.046,95% CI=2.090–4.439), and a history of previous illnesses(GG+GCvs.CC: OR=2.898,95% CI=1.997–4.205).The results of multiplicative interaction analysis demonstrated that age and sex exhibited significant interactions with the genetic variation of rs4147581C>G, with a statistically significant difference observed between the case and control groups (P<0.05).
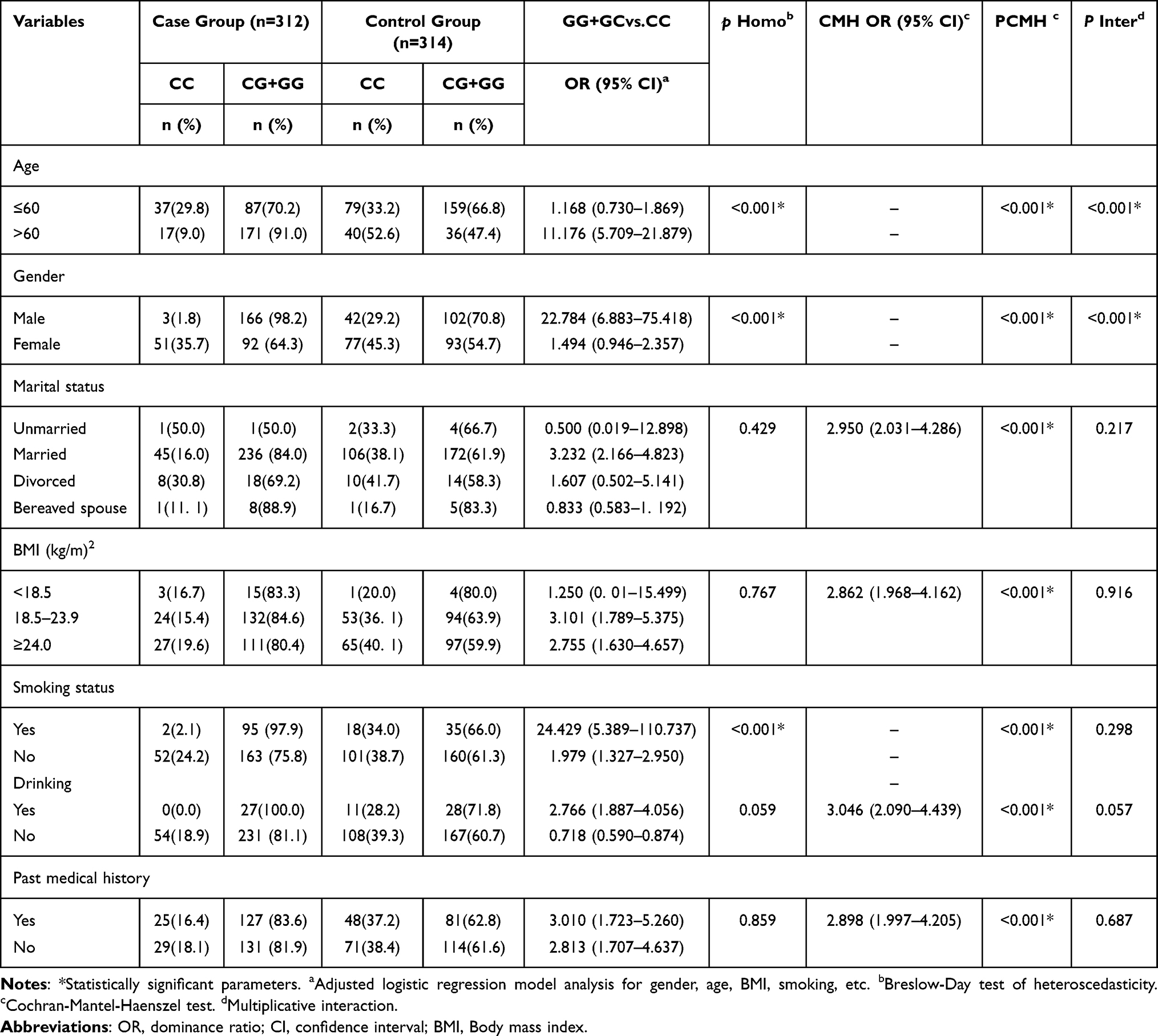 |
Table 3 Stratification Analysis and Interaction Analysis Between GSTP1 rs4147581C>G and COPD Susceptibility |
Stratification and Interaction Analysis of NLRP3 rs3806265 T>C and COPD Prevalence Risk
The results of the stratification and interaction analysis are presented in Table 4. In the dominant model, rs3806265T>C, compared to the TT genotype, displayed variations in strata involving marital status and smoking. Notably, a lack of homogeneity between strata (P<0.05) was evident in the married population (TC+CCvs.TT: OR=2.816,95% CI=1.979–4.008), and the population with a smoking history (TC+CCvs.TT: OR=7.130,95% CI=3.291–15.451), and those without a smoking history (TC+CCvs.TT: OR=1.673,95% CI=1.156–2.421) increased the risk of COPD. In the dominant model, when stratified by TC/CC genotypes compared to TT genotypes, and across various strata, including age, sex, BMI, alcohol consumption, and history of previous diseases, we observed homogeneity between these strata (P>0.05). In each of these strata, the TC/CC genotypes were associated with an increased risk of COPD: age (TC+CCvs.TT:OR=2.088,95% CI=1.469–2.968), sex(TC+CCvs.TT:OR=2.268,95% CI=1.619–3.176), BMI(TC+CCvs.TT: OR=2.432,95% CI=1.743–3.392), alcohol consumption (TC+CC vs.TT: OR=2.339,95% CI=1.683–3.251), and history of previous illness (TC+CCvs.TT: OR=2.336,95% CI=1.680–3.247). Furthermore, the results of the multiplicative interaction analysis revealed that the interaction between smoking and alcohol consumption, in relation to the genetic variation in rs3806265 T>C, exhibited a statistically significant difference between the case and control groups (P<0.05).
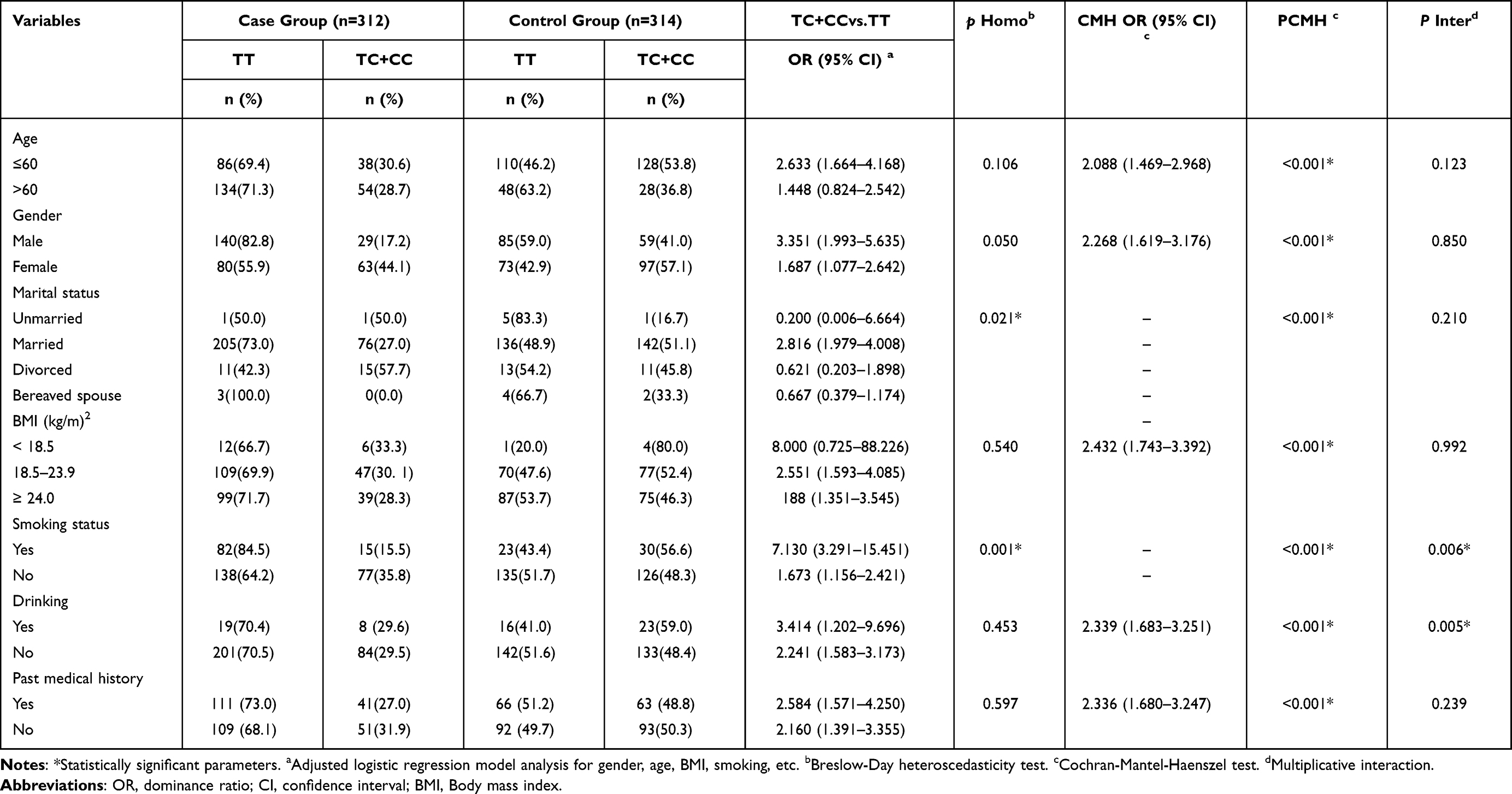 |
Table 4 Stratified Analysis and Interaction Analysis Between NLRP3 rs380626 T>C and COPD Susceptibility |
Analysis of the Relationship Between COPD Severity and SNPs
A total of 110 COPD patients with complete pulmonary function indicators and stable stage were selected from the case group. The severity of COPD was divided into four levels according to the percentage of the expected value of forced pulmonary capacity in the first second. Among them, the predicted value of FEV1 ≥ 80% was mild, and the predicted value of 50% ≤ FEV1 < 80% was moderate. 30% ≤FEV1 < 50% is expected to be severe, and FEV1 < 30% is expected to be extremely severe. The correlation between GSTP1 (rs4147581C>G and rs1695A>G) and NLRP3 (rs3806265T>C and rs10754558G>C) and COPD severity was analyzed. As shown in Table 5, the group of cases with complete lung function was analysed by chi-square test, and it was found that rs4147581C>G, rs1695A>G, rs3806265T>C, and rs10754558G>C were unassociated with the severity of COPD.
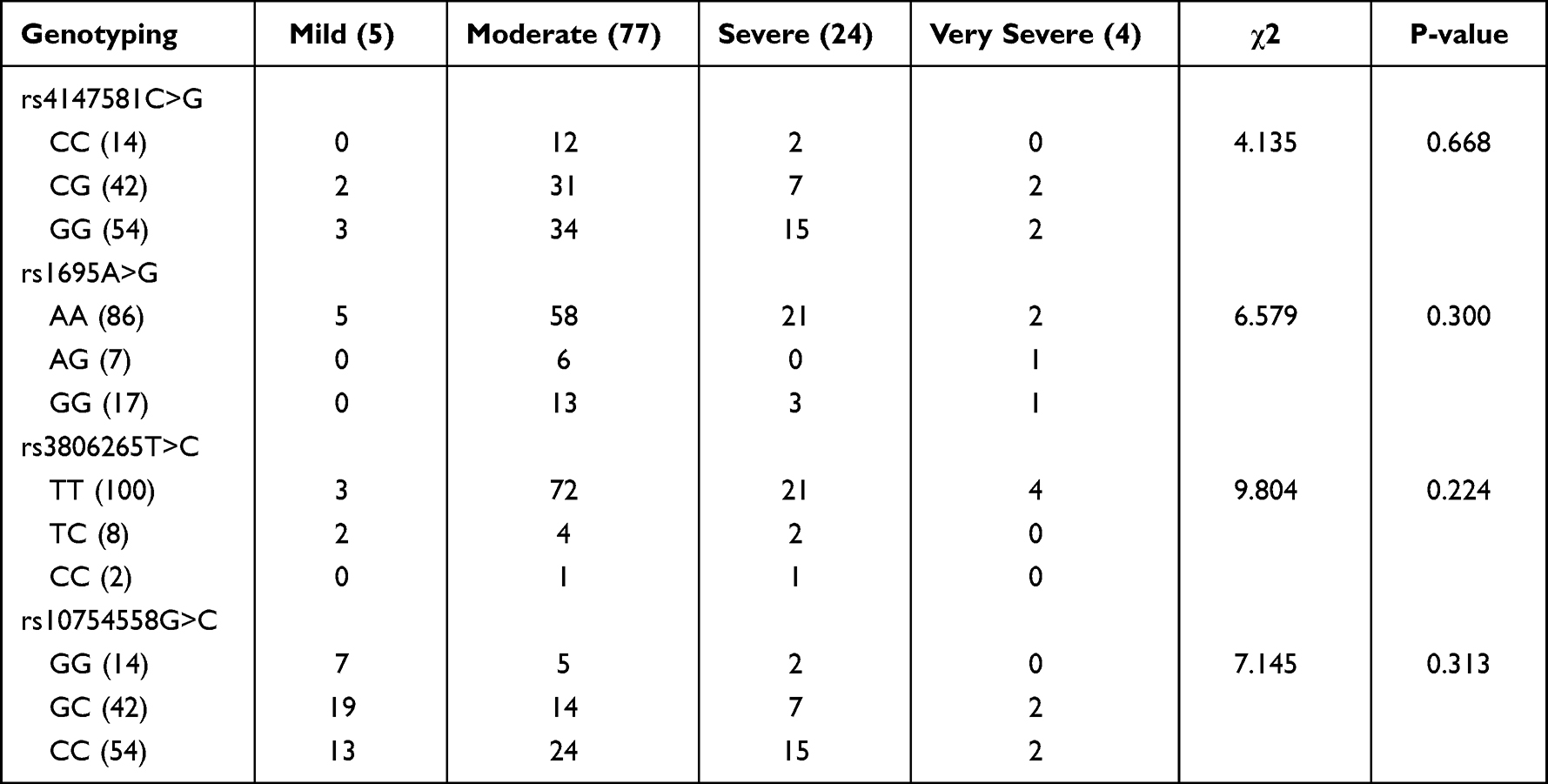 |
Table 5 Analysis of the Relationship Between COPD Severity and SNPs |
Discussion
Gene polymorphisms are thought to be involved in several aspects of COPD pathogenesis, and the association between polymorphisms in the GSTP1 gene and the risk of COPD is controversial both nationally and internationally, and there have been fewer studies on polymorphisms in the NLRP3 gene and COPD. To elucidate the role of GSTP1 and NLRP3 polymorphisms in COPD development, our study examined the relationship between two SNPs in the GSTP1 gene (rs4147581C>G, rs1695A>G) and two SNPs in the NLRP3 gene (rs3806265T>C, rs10754558G>C) and COPD risk in the Gansu population, China. Notably, GSTP1 rs4147581C>G allele exhibited an elevated COPD risk, with CG and GG genotypes demonstrating higher susceptibility compared to the rs4147581CC genotype within the age>60 years, male, smoking population (P<0.05). Furthermore, the NLRP3 rs3806265T>C allele was linked to an increased COPD risk, with the TT genotype displaying a higher prevalence in the married and smoking populations (P<0.05) compared to the rs3806265TC/CC genotype. And neither rs4147581 nor rs3806265 was associated with COPD severity.
GSTP1, a member of the GST enzyme family, serves various physiological functions.37 GSTs have been reported to participate in antioxidant processes within the body.38 Among the GSTs, GSTP1 and its close association with oxidative stress and inflammatory responses in COPD are notable GSTP1 polymorphisms contribute to an imbalance in oxidative-oxidative processes, affecting the ability to counter oxidative stress and other lung disease-associated biological mechanisms. This, in turn, impacts COPD development and severity.39 Additionally, GSTP1 plays a protective role against airway cell damage induced by smoking. Consequently, the association between GSTP1 and COPD has garnered increased attention. NLRP3 protein primarily resides in cells, serving to detect in vivo danger signals, thus, promoting the release of inflammatory factors such as IL-1β and IL-18.40 NLRP3 plays a crucial role in macrophage and neutrophil migration and aggregation, as well as in oxidative stress generation.41 Inhibition of NLRP3 inflammatory vesicles indirectly mitigates the inflammatory effects of IL-1β and IL-18, presenting an ideal target for COPD treatment.
In this study, we selected two SNPs from the GSTP1 gene (rs4147581C>G and rs1695A>G) and two from the NLRP3 gene (rs3806265T>C and rs10754558G>C) for investigation. Online tools such as NCBI, Ensembl, and SNP info Web Server were used to obtain information on the location and function of these SNPs. The GSTP1 gene, located on chromosome 11q13, spans approximately 3 kb with 7 exons.42 Specifically, rs4147581C>G, positioned at Chr11: 67584114, has demonstrated significant associations with survival in patients with hepatocellular carcinoma, where its mutant genotype reduces the risk of death in these patients.43–46 Meanwhile, rs1695A>G at Chr11: 67585218 has shown associations with conditions such as cervical cancer, asthma, cyclophosphamide efficacy, and adverse effects. The NLRP3 gene, situated on chromosome 1q44, extends over approximately 40 kb.47,48 Within this gene, rs3806265T>C, located at Chr1: 247423034, has been linked to multiple sclerosis, juvenile systemic lupus erythematosus, and myasthenia gravis in recent studies.49–51 Similarly, rs10754558G>C at Chr1: 247448734 has been reported to be associated with rheumatoid arthritis, chronic kidney disease, psoriasis, and others.
Our study findings indicate an association between the GSTP1 rs4147581C>G variant and the risk of developing COPD. Patients with the CG/GG genotype exhibited a higher incidence of COPD compared to those with the CC genotype. GSTP1 functions as a detoxifying enzyme involved in intracellular oxidative stress responses and the removal of toxic metabolites.52 The rs4147581C>G variant may lead to reduced activity and function of the GSTP1 enzyme, diminishing its capacity to bind and eliminate toxicants and harmful metabolites. This can result in intracellular toxicant accumulation, increased oxidative stress, and exacerbated inflammatory responses, thereby elevating the risk of cardiovascular diseases like coronary artery disease, hypertension, and myocardial infarction.
Furthermore, we found an association between the NLRP3 rs3806265T>C variant and the risk of developing COPD, with a higher prevalence of the TT genotype compared to the TC/CC genotype.53 NLRP3 rs3806265 may play a pivotal role in inflammatory injury in COPD. The variant could lead to aberrant NLRP3 protein function, impacting the abnormal activation of inflammatory vesicles and deviating inflammatory signaling pathways. This, in turn, increases intracellular stress levels and contributes to the development and exacerbation of inflammatory diseases.
In this study, we investigated the role of GSTP1rs4147581C>G and NLRP3rs3806265T>C variants as risk factors for chronic obstructive pulmonary disease (COPD). Our findings provide a new way to predict and prevent COPD.54 In addition, studies by Yadav et al in North Indian populations found that GST gene polymorphisms can be used as susceptibility biomarkers for COPD, which also provides support for our study.55 The study of the effect of IL5RA variants on COPD in a Chinese population by Li et al provides new evidence to further our understanding of the genetic susceptibility to COPD. This study reveals an association between IL5RA gene variants and COPD, which could help us better predict and prevent COPD.56 The study of Castro et al on the influence of gene polymorphism on the severity of silicosis provides us with a new perspective. The study, conducted in silicon-exposed Brazilian workers, explored the effect of genetic polymorphisms on the severity of silicosis, providing useful information for the prevention and treatment of lung disease.57 Finally, Cheng et al ‘s study that circular RNA-SNPs may increase susceptibility to silicosis provides new clues to our understanding of genetic susceptibility to silicosis. The study, conducted in a Chinese population, identified a novel circular RNA-SNP that may increase susceptibility to lung lesions. Taken together, these studies provide valuable information for our understanding of the genetic susceptibility to COPD and lung-related diseases, which can help us better prevent and treat these diseases. In future studies, we will continue to explore the role of these gene variants in COPD, with a view to providing more guidance for clinical diagnosis and treatment.
This study explored the genetic role of GSTP1 and NLRP3 genes in the risk of developing COPD using a case-control design in Gansu Province. The results showed that genetic polymorphisms in these genes were correlated with the occurrence of COPD in Gansu Province. However, this study has its limitations. Firstly, the sample size is limited, and further validation with an expanded sample size is necessary. Secondly, the study subjects were sourced from specific hospitals, potentially introducing selection bias. Thirdly, there might be recall bias in the collection of past information during the questionnaire survey. Lastly, as this study is a case-control design, establishing the temporal sequence of genetic polymorphisms and COPD is challenging. Future research should consider cohort and experimental studies to further validate these findings.
Conclusion
In conclusion, GSTP1 rs4147581C>G allele exhibited an elevated COPD risk, with CG and GG genotypes demonstrating higher susceptibility compared to the rs4147581CC genotype within the age>60 years, male, smoking population. Furthermore, the NLRP3 rs3806265T>C allele was linked to an increased COPD risk, with the TT genotype displaying a higher prevalence in the married and smoking populations compared to the rs3806265TC/CC genotype.
Abbreviations
COPD, chronic obstructive pulmonary disease; GSTP1, Glutathione S-transferase P1; NLRP3, NOD-like receptor thermal protein domain associated protein 3; LD, Linkage disequilibrium; GWAS, genome-wide association analysis; SNPs, the single nucleotide polymorphisms; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MAFs, the minor allele frequencies; PCR, TaqMan real-time polymerase chain reaction.
Acknowledgment
We thank the Institute of Public Health, Gansu University of Traditional Chinese Medicine. We thank the researchers in our laboratory for their guidance on experimental techniques.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the following grants: National Key Research and Development Project of China 2017YFC0907202 (Xinhua Wang); National Natural Science Foundation of China (82260889) (Xuhui Zhang); Central Guided Local Science and Technology Development Funds Project No.22ZY1QA003(Xinhua Wang); 2022 Gansu Province Higher Education Institutions Industry Support Program Project No.2022CYZC-53(Xinhua Wang).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
2. Soler N, Esperatti M, Ewig S, et al. Sputum purulence-guided antibiotic use in hospitalised patients with exacerbations of COPD. Europ resp J. 2012;40:1344–1353. doi:10.1183/09031936.00150211
3. Blakemore A, Dickens C, Chew-Graham CA, et al. Depression predicts emergency care use in people with chronic obstructive pulmonary disease: a large cohort study in primary care. Int J Chronic Obstr. 2019;14:1343–1353. doi:10.2147/COPD.S179109
4. Agustí A, Vogelmeier C, Faner R. COPD 2020: changes and challenges. Am J Physiol Lung Cell Mol Physiol. 2020;319:L879–L883. doi:10.1152/ajplung.00429.2020
5. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391:1706–1717. doi:10.1016/S0140-6736(18)30841-9
6. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387:251–272. doi:10.1016/S0140-6736(15)00551-6
7. Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Europ resp J. 2011;37:264–272. doi:10.1183/09031936.00051110
8. Montes de Oca M, Perez-Padilla R, Tálamo C, et al. Acute bronchodilator responsiveness in subjects with and without airflow obstruction in five Latin American cities: the PLATINO study. Pulmon Pharmacol Ther. 2010;23:29–35. doi:10.1016/j.pupt.2009.09.005
9. Silverman EK. Genetics of COPD. Annu Rev Physiol. 2020;82:413–431. doi:10.1146/annurev-physiol-021317-121224
10. He Y, Jiang B, Li LS, et al. Secondhand smoke exposure predicted COPD and other tobacco-related mortality in a 17-year cohort study in China. Chest. 2012;142(4):909–918. doi:10.1378/chest.11-2884
11. Forey BA, Thornton AJ, Lee PN. Systematic review with meta-analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC Pulm Med. 2011;11:36. doi:10.1186/1471-2466-11-36
12. Eisner MD, Balmes J, Katz PP, et al. Lifetime environmental tobacco smoke exposure and the risk of chronic obstructive pulmonary disease. Environ Health. 2005;4:7. doi:10.1186/1476-069X-4-7
13. Wang B, Xiao D, Wang C. Smoking and chronic obstructive pulmonary disease in Chinese population: a meta-analysis. Clin Respir J. 2015;9:165–175. doi:10.1111/crj.12118
14. Lai HC, Lin TL, Chen TW, et al. Gut microbiota modulates COPD pathogenesis: role of anti-inflammatory Parabacteroides goldsteinii lipopolysaccharide. Gut. 2022;71:309–321. doi:10.1136/gutjnl-2020-322599
15. Confalonieri M, Braga L, Salton F, et al. Chronic obstructive pulmonary disease definition: is it time to incorporate the concept of failure of lung regeneration? Am J Respir Crit Care Med. 2023;207(3):366–367. doi:10.1164/rccm.202208-1508LE
16. Zhou H, Yang J, Li D, et al. Association of IREB2 and CHRNA3/5 polymorphisms with COPD and COPD-related phenotypes in a Chinese Han population. J Human Gene. 2012;57:738–746. doi:10.1038/jhg.2012.104
17. Yuan C, Chang D, Lu G, et al. Genetic polymorphism and chronic obstructive pulmonary disease. Int J Chronic Obstr. 2017;12:1385–1393. doi:10.2147/COPD.S134161
18. Stankovic M, Nikolic A, Nagorni-Obradovic L, et al. Gene-gene interactions between glutathione S-transferase M1 and matrix metalloproteinases 1, 9, and 12 in chronic obstructive pulmonary disease in serbians. COPD. 2017;14:581–589. doi:10.1080/15412555.2017.1369022
19. Zuntar I, Petlevski R, Dodig S, et al. GSTP1, GSTM1 and GSTT1 genetic polymorphisms and total serum GST concentration in stable male COPD. Acta Pharm. 2014;64:117–129. doi:10.2478/acph-2014-0003
20. Zhong L, Zhang YP, Fu WP, et al. The relationship between GSTP1 I105V polymorphism and COPD: a reappraisal. Am J Respir Crit Care Med. 2010;181:763–765. doi:10.1164/ajrccm.181.7.763
21. Yan F, Chen C, Jing J, et al. Association between polymorphism of glutathione S-transferase P1 and chronic obstructive pulmonary disease: a meta-analysis. Respir Med. 2010;104:473–480. doi:10.1016/j.rmed.2010.01.009
22. Ishii T, Matsuse T, Teramoto S, et al. Glutathione S-transferase P1 (GSTP1) polymorphism in patients with chronic obstructive pulmonary disease. Thorax. 1999;54:693–696. doi:10.1136/thx.54.8.693
23. Yim JJ, Park GY, Lee CT, et al. Genetic susceptibility to chronic obstructive pulmonary disease in Koreans: combined analysis of polymorphic genotypes for microsomal epoxide hydrolase and glutathione S-transferase M1 and T1. Thorax. 2000;55:121–125. doi:10.1136/thorax.55.2.121
24. Yang L, Li X, Tong X, et al. Association between glutathione S-transferase P1 Ile (105) Val gene polymorphism and chronic obstructive pulmonary disease: a meta-analysis based on seventeen case-control studies. Meta Gene. 2015;6:59–64. doi:10.1016/j.mgene.2015.08.007
25. Yang Q, Huang W, Yin D, et al. EPHX1 and GSTP1 polymorphisms are associated with COPD risk: a systematic review and meta-analysis. Front Genetics. 2023;14:1128985. doi:10.3389/fgene.2023.1128985
26. Du Y, Zhang H, Xu Y, et al. Association among genetic polymorphisms of GSTP1, HO-1, and SOD-3 and chronic obstructive pulmonary disease susceptibility. Int J Chronic Obstr. 2019;14:2081–2088. doi:10.2147/COPD.S213364
27. Mo R, Li J, Chen Y, et al. lncRNA GAS5 promotes pyroptosis in COPD by functioning as a ceRNA to regulate the miR-223-3p/NLRP3 axis. Molecul Med Rep. 2022;26:219. doi:10.3892/mmr.2022.12735
28. Faner R, Sobradillo P, Noguera A, et al. The inflammasome pathway in stable COPD and acute exacerbations. ERJ Open Res. 2016;2:2. doi:10.1183/23120541.00002-2016
29. Eltom S, Stevenson CS, Rastrick J, et al. P2X7 receptor and caspase 1 activation are central to airway inflammation observed after exposure to tobacco smoke. PLoS One. 2011;6:e24097. doi:10.1371/journal.pone.0024097
30. Mahalanobish S, Dutta S, Saha S, et al. Melatonin induced suppression of ER stress and mitochondrial dysfunction inhibited NLRP3 inflammasome activation in COPD mice. Food and Chemical Toxicology. 2020;144:111588.
31. Zhang MY, Jiang YX, Yang YC, et al. Cigarette smoke extract induces pyroptosis in human bronchial epithelial cells through the ROS/NLRP3/caspase-1 pathway. Life Sci. 2021;269:119090. doi:10.1016/j.lfs.2021.119090
32. Cheng L, Yin R, Yang S, et al. Rs4612666 Polymorphism of the NLRP3 gene is associated with the occurrence of large artery atherosclerotic ischemic strokes and microembolic signals. Biomed Res. Int. 2018;2018:6345805. doi:10.1155/2018/6345805
33. Zhou D, Wang X, Chen T, et al. The NLRP3 rs10754558 polymorphism is associated with the occurrence and prognosis of coronary artery disease in the Chinese han population. Biomed Res. Int. 2016;2016:3185397. doi:10.1155/2016/3185397
34. Sui J, Li H, Fang Y, et al. NLRP1 gene polymorphism influences gene transcription and is a risk factor for rheumatoid arthritis in han Chinese. Arthritis Rheum. 2012;64:647–654. doi:10.1002/art.33370
35. Von Herrmann KM, Salas LA, Martinez EM, et al. NLRP3 expression in mesencephalic neurons and characterization of a rare NLRP3 polymorphism associated with decreased risk of Parkinson’s disease. NPJ Parkinson’s Dis. 2018;4:24. doi:10.1038/s41531-018-0061-5
36. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report). Avaliable from: https://goldcopd.org/2023-gold-report-2/.
37. Gattás GJ, Kato M, Soares-Vieira JA, et al. Ethnicity and glutathione S-transferase (GSTM1/GSTT1) polymorphisms in a Brazilian population. Braz J Med Biol Res. 2004;37:451–458. doi:10.1590/s0100-879x2004000400002
38. Tomaki M, Sugiura H, Koarai A, et al. Decreased expression of antioxidant enzymes and increased expression of chemokines in COPD lung. Pulmon Pharmacol Ther. 2007;20:596–605. doi:10.1016/j.pupt.2006.06.006
39. Ishii T, Matsuse T, Igarashi H, et al. Tobacco smoke reduces viability in human lung fibroblasts: protective effect of glutathione S-transferase P1. Am J Physiol Lung Cell Mol Physiol. 2001;280:L1189–L1195. doi:10.1152/ajplung.2001.280.6.L1189
40. Guo P, Li R, Piao TH, et al. Pathological mechanism and targeted drugs of COPD. Int J Chronic Obstr. 2022;17:1565–1575. doi:10.2147/COPD.S366126
41. Chen X, Liu G, Yuan Y, et al. NEK7 interacts with NLRP3 to modulate the pyroptosis in inflammatory bowel disease via NF-κB signaling. Cell Death Dis. 2019;10:906. doi:10.1038/s41419-019-2157-1
42. Wang Z, Qu K, Niu W, et al. Glutathione S-transferase P1 gene rs4147581 polymorphism predicts overall survival of patients with hepatocellular carcinoma: evidence from an enlarged study. Tumour Biol. 2016;37:943–952. doi:10.1007/s13277-015-3871-7
43. Phuthong S, Settheetham-Ishida W, Natphopsuk S, et al. Genetic Polymorphism of the Glutathione S-transferase Pi 1 (GSTP1) and susceptibility to cervical cancer in human papilloma virus infected Northeastern Thai Women. Asian Pac J Cancer Prev. 2018;19:381–385. doi:10.22034/APJCP.2018.19.2.381
44. Mukhammadiyeva GF, Bakirov AB, Karimov DO, et al. Analysis of the GSTP1 rs1695 polymorphism association with the development of asthma and phenotypic manifestations. J Asthma. 2022;59:1065–1069. doi:10.1080/02770903.2021.1910295
45. Dasgupta RK, Adamson PJ, Davies FE, et al. Polymorphic variation in GSTP1 modulates outcome following therapy for multiple myeloma. Blood. 2003;102:2345–2350. doi:10.1182/blood-2003-02-0444
46. Zhong S, Huang M, Yang X, et al. Relationship of glutathione S-transferase genotypes with side-effects of pulsed cyclophosphamide therapy in patients with systemic lupus erythematosus. Br. J. Clin. Pharmacol. 2006;62:457–472. doi:10.1111/j.1365-2125.2006.02690.x
47. Imani D, Azimi A, Salehi Z, et al. Association of nod-like receptor protein-3 single nucleotide gene polymorphisms and expression with the susceptibility to relapsing-remitting multiple sclerosis. Int J Immunogene. 2018;45:329–336. doi:10.1111/iji.12401
48. Agah E, Nafissi S, Saleh F, et al. Investigating the possible association between NLRP3 gene polymorphisms and myasthenia gravis. Muscle and Nerve. 2021;63:730–736. doi:10.1002/mus.27193
49. Cheng L, Liang X, Qian L, et al. NLRP3 gene polymorphisms and expression in rheumatoid arthritis. Exp Ther Med. 2021;22:1110.
50. La Russa A, Lofaro D, Montesanto A, et al. Association between NLRP3 rs10754558 and CARD8 rs2043211 variants and susceptibility to chronic kidney disease. Int J Mol Sci. 2023;24:1110. doi:10.3892/etm.2021.10544
51. Dawood A, Shehata W. Evaluation of NLRP3 (rs10754558) and PTPN22 (1858C/T) (rs2476601) functional polymorphisms in psoriasis susceptibility in Egypt. Appl Clin Gene. 2021;14:331–339. doi:10.2147/TACG.S319065
52. Qu K, Liu SS, Wang ZX, et al. Polymorphisms of glutathione S-transferase genes and survival of resected hepatocellular carcinoma patients. World J Gastroenterol. 2015;21:4310–4322. doi:10.3748/wjg.v21.i14.4310
53. Kelley N, Jeltema D, Duan Y, et al. The NLRP3 inflammasome: an overview of mechanisms of activation and regulation. Int J Mol Sci. 2019;20:3328. doi:10.3390/ijms20133328
54. Yadav H, Pandit D, Singh S, et al. GST polymorphism as a predictive biomarker for modulating the susceptibility to chronic obstructive pulmonary disease: a North Indian study. Exp Physiol. 2023. doi:10.1113/EP091339
55. Li S, Lin L, Zhao J, et al. The Study of the Influence of IL5RA variants on chronic obstructive pulmonary disease. COPD. 2023;20(1):338–347. doi:10.1080/15412555.2023.2270729
56. Castro MCS, Nani ASF, Salum KCR, et al. Genetic polymorphisms and their effects on the severity of silicosis in workers exposed to silica in Brazil. J Bras Pneumol. 2022;48(5):e20220167. doi:10.36416/1806-3756/e20220167
57. Cheng Z, Zhang Y, Zhao R, et al. A novel circRNA-SNP may increase susceptibility to silicosis. Ecotoxicol Environ Saf. 2022;242:113855. doi:10.1016/j.ecoenv.2022.113855
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.