")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Growth Monitoring Practice and Associated Factors Among Health Professionals at Public Health Facilities of Bahir Dar Health Centers, Northwest Ethiopia, 2021
Authors Tesfa M, Gonete KA , Chane Y, Yohannes S
Received 13 January 2022
Accepted for publication 9 May 2022
Published 20 May 2022 Volume 2022:13 Pages 195—215
DOI https://doi.org/10.2147/PHMT.S355214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Roosy Aulakh
Migbaru Tesfa,1 Kedir Abdela Gonete,2 Yawkal Chane,3 Senay Yohannes4
1Ministry of Health Ethiopia, Eka Kotebe General Hospital, Addis Abeba, Ethiopia; 2Department of Human Nutrition, College of Medicine and Health Science, Institute of Public Health, University of Gondar, Gondar, Ethiopia; 3Department of Nutrition, College of Medicine and Health Science, Kotebe Metropolitan University, Addis Ababa, Ethiopia; 4Department of Surgical Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Senay Yohannes, Tel +251 918-232-916, Email [email protected]
Background: Growth monitoring and promotion are one of the health priorities in assessing the growth rate of a child. Appropriate growth monitoring and promotion services enable health professionals to control growth faltering and child mortality. However, there is limited information on the growth monitoring practice of health professionals and their associated factors at public health facilities of Bahir Dar health centers. Therefore, this study aimed to assess the growth monitoring practice of health professionals and associated factors at public health facilities of Bahir Dar health centers, northwest Ethiopia.
Methods: Institutional-based cross-sectional study for quantitative and phenomenology for qualitative was conducted from April 15 to May 15, 2021, among 314 health professionals, in Bahir Dar town, northwest Ethiopia. Census was used. A self-administered questionnaire was employed for quantitative data. Data were cleaned and entered into Epi-info version 7.1 and exported to SPSS version 20 for further analysis, and the binary logistic regression was employed. In the bi-variable analysis, those variables with a p-value less than 0.2 were fitted to multivariable analysis. Qualitative data were analyzed by using thematic analysis.
Results: The overall growth monitoring practice of health professionals at Bahir Dar public health centers was 30.3%, with a response rate of 98.1. The number of participants who had at least a degree was [AOR = 3.57; 95% CI: 1.54, 8.26], health professionals who had greater than 11 years of work experience [AOR = 2.98; CI: 1.36, 6.53], those who took training [AOR = 5.11; CI: 2.20, 11.90], availability of growth monitoring equipment [AOR = 4.44; CI: 1.97, 9.98], those who had lesser workload (saw less than 25 children’s per day) [AOR = 3.02; CI: 1.16, 7.86], those who had good knowledge [AOR = 4.60; CI: 2.06, 10.31] and favorable attitude [AOR = 2.58; CI: 1.14, 5.83] were significantly associated with growth monitoring practice.
Conclusion: The overall growth monitoring practice among health professionals of Bahir Dar public health centers was low. Work experience, age, educational status, knowledge, attitude, workload, training, and availability of growth monitoring equipment were key predictors of growth monitoring practice among health professionals in Bahir Dar public health centers. Therefore, regular supportive supervision from the regarded body, provision of training to health professionals and fulfill growth monitoring equipment are all necessary measures to provide a better growth monitoring service.
Keywords: growth monitoring, health professionals, health facility, Bahir Dar
Background
Growth monitoring (GM) is the regular measurement of a child’s size (weight, height or length, and head circumference) to document growth. The child’s size measurements must then be plotted on a growth chart. This is important to detect the growth rate of a child in comparison to a standard by periodic anthropometric measurements to assess growth adequacy and identify faltering at early stages and assessing growth allows for capturing growth faltering before the child reaches the status of under-nutrition.1,2
The importance of growth monitoring is to instigate effective action in response to growth faltering, to teach mothers, families, and health workers how diet and illness can affect child growth, to provide regular contact with primary health-care services, and so facilitate their utilization, for community mobilization and social action, to determine eligibility for entry to supplementary feeding programs, to reporting the prevalence of underweight.3
Growth monitoring practices are mandatory for better child health, but national and international reports have shown that there is a discrepancy between the purpose and the practice of growth monitoring and promotion. The high prevalence of malnutrition in many developing countries seems to confirm this fact. According to the World Health Organization, 2019 report 155 million children under 5 are stunted, 52 million are wasted, 17 million are severely wasted, and 42 million are overweight and obese.4 Another report shows in 2019, 144 million children less than 5 years of age suffer from stunting; 47 million were wasted of which 14.3 million were severely wasted. There are now 38.3 million overweight children on the globe.1,5
In sub-Saharan Africa, 32.7% of fewer than 5 years of children are stunted, 6.9% are wasted and 1.8% are severely wasted and 3.1% are overweight. In eastern Africa, 34.5% of fewer than 5 years of age children are stunted, 5.3% are wasted and 1.1% of them are severely wasted and 3.7% are overweight.1
Ethiopian Demographic Health Survey (EDHS) 2016 report shows that 38% of children under age 5 are stunted. Ten percent are wasted, 24% are underweight and 1% had overweight. In Amhara regional state 46% of fewer than 5 children are stunted which is the highest prevalence in Ethiopia.6
According to the 2019 EDHS mini-report shows that 36.8% of children less than 5 years of age are stunted and 12% are severely stunted, 7.2% are wasted and 21.1% are underweight in Ethiopia. In Amhara regional state 41.3% of fewer than 5 children are stinting, 7.6% are wasted and 26.7% are underweight.7
Globally, 186 countries practice growth monitoring in 2018.8 One hundred and fifty-four countries were used in the growth chart.9 In 2019, coverage of growth monitoring and promotion was 55% in Ethiopia. In Amhara regional state, GM coverage had 48%.10
Jobs, educational status, work experience, attitude, knowledge, availability of GM materials, workload, lack of training and support, and supervision were associated factors that affect growth monitoring practice.11 Other factors influencing growth monitoring practice were poor knowledge and attitude of mothers and caregivers, occupational and educational status of mothers, availability, and accessibility of health services, and growth monitoring service.12,13
In Ethiopia, the GMP is one of the health extension packages that has been given by Health extension workers (HEWs) to provide a health development army (HDA), and also growth monitoring is one component of the health sector transformation plan.14,15
Nutrition initiatives are instead generated mainly through donors. There is a gap in capacity and specifically human resources challenges in the MOH, which leads to a significant obstacle to resolving the lack of coordination around nutrition policy. In terms of nutrition implementation, it is not as strong, being undermined by a lack of incentives to coordinate at higher levels of the government structure, and by the lack of a specific nutrition mandate and weak reporting and monitoring mechanisms at the woreda level. GMP responsibility is given to HEWs. Due to the workload, lack of training, knowledge, and equipments to do technical aspects; they are unable to conduct GMP.16,17
Despite low coverage of GMP in our setting, there were not enough studies conducted to assess growth and monitoring practice and its associated factors of health-care professionals at the health center of Bahir Dar. Therefore, this study was carried out to determine the proportion of GMP and factors contributing to it among health professionals in public health centers of Bahir Dar, Amhara region, Ethiopia.
Methods and Materials
Study Design, Area, and Period
Institution-based cross-sectional study for quantitative and Phenomenology for qualitative study was conducted.
Bahir Dar is the capital city of the Amhara regional state of Ethiopia. This is located at the exit of the Nile from Lake Tana at an altitude of 1820 meters (5970 ft.) above sea level. The city was founded in 1922. The city is located approximately 578 km north-northwest of Addis Ababa., the capital of Ethiopia. Bahir Dar is one of the leading tourist destinations in Ethiopia, with a variety of attractions in the nearby Lake Tana and Blue Nile River. The city is known for its avenues lined with palm trees and a variety of colorful flowers. Bahir Dar is a clean and well-maintained city by African city standards. Based on the 2007 census total population of Bahir Dar was 221, 991, of those 108,456 are men and 113,535 are female.18 According to Bahir Dar city health office human resource unit information, Bahir Dar has 6 sub-cities, 3 public hospitals, and 10 public health centers. There are 410 health professionals. The study was conducted from April 15 to May 15, 2021.
Eligibility Criteria
Inclusion Criteria
All health professionals working in Bahir Dar public health centers during the study period were included.
Exclusion Criteria
Laboratory, pharmacy, environmental health, and HIT professionals were excluded.
Sample Size Determination and Sampling Procedure
Sample Size Determination
A single population proportion formula was used to estimate the sample size with the assumption of the prevalence rate is 50.4% which is taken from a previous study done in north Gondar zone public health facilities, to get the possible sample size with a z-value of 1.96 and marginal error of 5% was calculated.11


Z-critical value for normal distribution at 95% confidence level that is equal to 1.96 (Value at α=0.05)
P- 0.504 from a study done on the prevalence of growth monitoring practice and associated factors among health professionals in public health facilities of North Gondar. And d- 0.05 (5% marginal error)
Assuming my study population is less than 10,000 or a finite population (N = 320, based on the data from Bahir Dar city Health Office human resource unit), using the following correction formula.

10% non-respondent will be added
= 175*0.1=18
=193
Where: no - sample size calculated early
N - total population in the study area
n- corrected sample size
Based on the data from the Bahir Dar City Health Office human resource unit, the total population of the sample size is 320. Hence, the whole population is manageable (Census was used).
For the qualitative method, a semi-structured probing question was used as a guideline to interview five managers of health facilities. A purposive sampling technique was applied to select those five health center managers.19
Sampling Procedure
There are 10 public health centers in Bahir Dar city administration. A total number of study participants was obtained from the human resource unit of Bahir Dar city Health Office. By using the census method, all health centers were included in the study. All health professionals who worked in those 10 public health centers were included in the study.
For the qualitative part, five health center medical directors were interviewed using probing semi-structured questions.20 A purposive sampling technique was applied.
Operational Definitions
Growth monitoring: is a regular measurement of growth that enabled the visualized growth or lack of it and obtain specific, relevant, and practical guidance to ensure continued regular growth and health of children.2
Measurement of knowledge: to measure the health professional’s knowledge about growth monitoring was scored 1 for each correct response and score 0 for each incorrect response. To assess the respondent’s knowledge, 15 knowledgeable questionnaires were prepared. Poor knowledge is defined as a score of <75% and good knowledge is a score of >75% will conduct.21
Measurement of attitude: the attitude of health professionals about growth monitoring was measured by 10 items of 5-point Likert scale questions, which are scored 50. Variables in the questionnaire were given a total score ranging from 1 to 5. An unfavorable attitude was defined as a score of <75% while a score of ≥75% was considered a favorable attitude.21
Measurement of practices: To measure the practices of the health workers on growth monitoring, a scoring system was used. Each correct response was scored as 1 and the incorrect response was scored as 0 (zero). Variables in the questionnaire were given a total score ranging from 0 to 10 number of practice questions. Using a frequency distribution, the poor practice was defined as a score of <75% while a score of ≥75% was considered good practice.21
Workload: greater than 40 children seen per day is a very busy practice and 26–39 children per day are busy, practice with a workload of 25 patients and less than 25 children are ideal.21
Data Collection Tool and Procedure
For the quantitative part, eligible study participants were approached in each ward unit. Participants were provided with appropriate information about the study, then informed consent was been obtained to assure their willingness to participate in the study. Five trained BSc nurses collected the data and five trained MSc nurses closely followed the data collection process.
For the qualitative part, a semi-structured probing question is used for the phenomenology method. An in-depth interview, the questionnaire, was prepared for public health center medical directors to understand views of growth monitoring practice at their public health facility. Five health center medical directors were interviewed to assess qualitative information on the importance of growth monitoring, factors affecting growth monitoring practice, and mechanisms of improving growth monitoring and promotion services. The qualitative data were collected by the principal investigator.
Data Quality Assurance
The self-administered questionnaire was prepared in the English language. The one-day training was given to data collectors and supervisors on how to approach participants. Check unclear questionnaires and modify accordingly. The completeness of the collected data was checked every day. A pre-test was given to 5% of health professionals working in one selected Malawi health center around Bahir Dar. The overall data collection process was controlled by the principal investigator. The qualitative part of the in-depth interview was immediately transcribed, from Amharic to English on the day of data collection.
Data Processing and Analysis
For the quantitative part, the data was entered using Epi-info version 7.1, and it was exported to SPSS Version 20 for further analysis. Descriptive statistics were computed and presented using tables, figures, and charts. Binary logistic regression was used and those independent variables which had a p-value of less than 0.2 during bi-variable analysis, and then selected factors were entered into multivariable logistic regression analysis. Then, those having P-value <0.05 were identified as factors significantly associated with growth monitoring practice and Model adequacy was checked by using Hosmer and Lemeshow test.
For the qualitative part, the information was collected through in-depth interviews with selected public health center medical directors. The information was translated to English and analyzed with the support of ATLAS.ti v7.5.7 software and thematic analysis was applied for the qualitative study.
Results
Socio-Demographic Characteristics
Among the total of 320 health professional participants, 314 participated with a 98.1% response rate. The mean age of health professionals was 33.66 (±6.5). More than two-thirds of 215 (68.5%) participants were female. One hundred and fifty (47.8%) health professionals were in the age range of 30–39 years. Two hundred and seven (65.9%) respondents were married, 117 (37.3%) respondents were nurses, 172 (54.8%) were Diploma health professionals, 195 (62.1%) health professionals had less than 10 years of work experience. Around 293 (93.3%) were Orthodox in religion, and the majority of 310 (98.7%) were Amhara in Ethnicity (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Health Professionals at Public Health Centers of Bahir Dar, Northwest Ethiopia, 2021 (n = 314) |
Health Professional’s Knowledge on Growth Monitoring
Out of the total respondents, more than one-third of 109 (34.7%) answered the defined acceptable total knowledge score of 75% among 15 knowledgeable questions. The majority of 308 (98.1%) health professionals had known about the concept of growth monitoring and promotion and most of the respondents 297 (94.6%) had awareness of the growth chart. The majority of respondents 305 (97.15%) knew about the purpose of Growth monitoring and only 212 (67.5%) interpreted the child growth curve 224 (70.4%) of health professionals knew that children from 0-to 2 years should attend Growth monitoring every month (Table 2).
 |
Table 2 Knowledge of Growth Monitoring Practice Among Health Professionals at Public Health Centers of Bahir Dar, Northwest Ethiopia, 2021 (n = 314) |
Attitudes of Health Professionals About Growth Monitoring
More than one-third of 93 (29.6%) health professionals were a favorable attitude toward Growth Monitoring. Nearly 166 (52.9%) of health professionals strongly agreed about growth monitoring is necessary for every child. Almost half of 156 (49.7%) health professionals had strongly agreed that tanning was needed to enhance health professionals’ activity to do growth monitoring. Almost three-fourth 231 (73.6%) health professionals believed that growth monitoring is effective in preventing childhood malnutrition (Table 3).
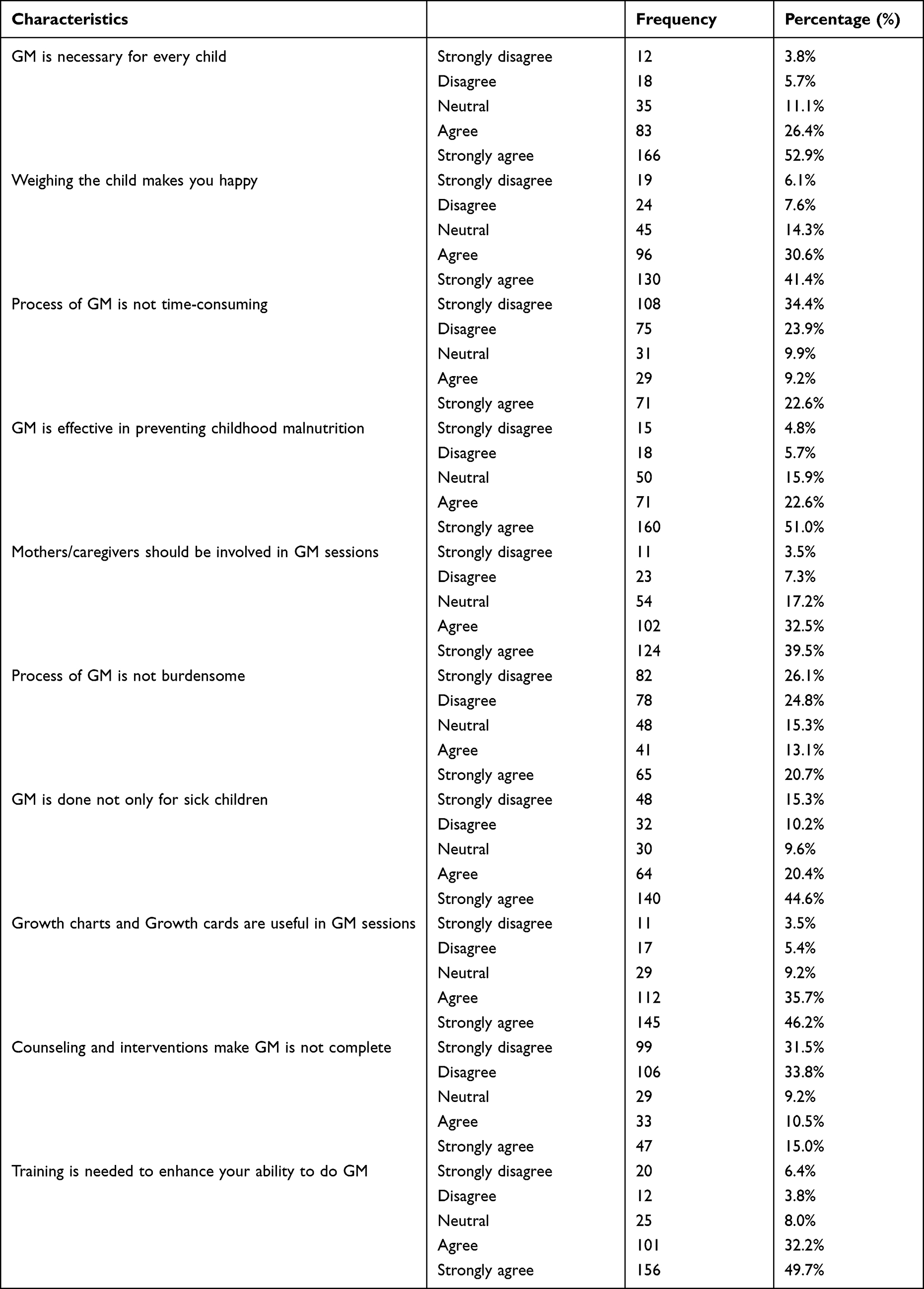 |
Table 3 Attitude Towards Growth Monitoring Practice of Health Professionals at Public Health Centers of Bahir Dar, Northwest Ethiopia, 2021 (n = 314) |
The Practice of Growth Monitoring
The overall growth monitoring practice was 95 (30.3%) (95% CI, 25.5, 35.4). About 223 (71%) health professionals have used a growth chart at the time of growth monitoring practice. More than half 166 (52.9%) and 158 (50.3%) of respondents were plotted children’s age and weight per standard procedures and interpreted the growth curve of each child, respectively. Two hundred and forty-three (77.4%) of respondents did not clean the scale after each child was weighted (Table 4).
 |
Table 4 The Practice of Growth Monitoring Health Professionals at Public Health Centers of Bahir Dar, Northwest Ethiopia, 2021 (n = 314) |
Training of Health Professionals
More than one-third of 115 (36.6%) health professionals took in-service training. There were 59 (51.3%), 32 (27.2%), and 30 (26.1%) health professionals who received integrated management of neonatal and childhood illnesses, nutrition, and EPI type training, respectively. A trained health professional reported that the training covered 70 (60.9%) weighting skills, 79 (66.7%) plotting techniques, 84 (73%) counseling techniques, and 35 (30.4%) nutritional education (Figure 1).
 |
Figure 1 Percentage of health professionals who took types of training to give growth monitoring service in Bahir Dar public health centers, 2021. |
Support and Supervision
In this study, 76 (24.2%) of health professionals got supportive supervision. More than one-third of 34 (44.7%) got immediate feedback from the supportive supervision, 24 (31.6%) were provided reference materials on growth monitoring, 14 (18.4%) were assisted to organize and to plane growth monitoring tasks and 12 (15.8%) of them were provided growth monitoring in-service training (Figure 2).
 |
Figure 2 Percentage of health professionals who gets supportive supervision to give growth monitoring service (Based on the chi-square result) in Bahir Dar public health centers, 2021. |
Availability of Growth Monitoring Equipment
Nearly 185 (41.1%) of health professionals reported that there was a lack of growth monitoring equipment. About those 126 (68.1%) were lack of weight scale, 136 (73.5%) were lack of growth cards, 130 (70.3%) lack of stationery materials, 112 (60.5%) lack of pamphlets, and 97 (52.4%) were lack of height board (Figure 3).
 |
Figure 3 Percentage of unavailable growth monitoring equipment in Bahir Dar public health centers, 2021. |
Workload
One hundred fifty-two (48.4%) of health professionals saw greater than 40 children per day. Most 298 (94.9%) health professionals agreed that the ideal number of patients seen per day was improved growth monitoring practice activities (Figure 4).
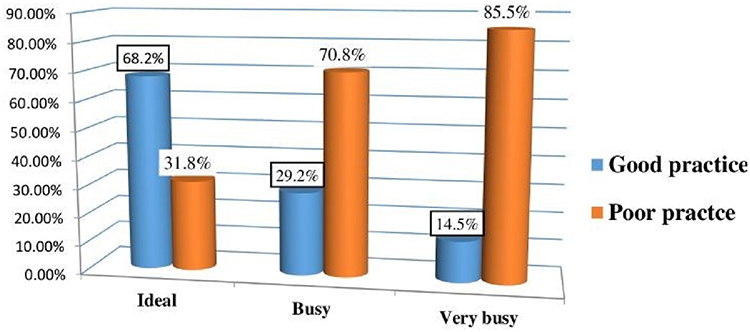 |
Figure 4 Percentages of health professionals work load and growth monitoring practice level in Bahir Dar public health centers, 2021. |
Encountered Problems
Around 161 (51.3%) of health professionals have encountered problems during growth monitoring practice. The challenges were 122 (38.9%) difficulty in interpreting the growth curve, 86 (27.4%) difficulty in counseling the mother, and 65 (20.7%) difficulty in plotting weight on the growth chart (Figure 5).
 |
Figure 5 Percentage of encountered problems during growth monitoring practice among health professionals of Bahir Dar public health centers, 2021. |
Factors Associated with Growth Monitoring Practice
In the Bivariate logistic regression analysis educational status, work experience, training, regular support and supervision, availability of growth monitoring equipment, workload, separate GMP room, knowledge, and attitude were significantly associated with the growth monitoring practice of health professionals. In multivariable logistic regression analysis; educational status, work experience, workload, knowledge, attitude, availability of growth monitoring equipment, and training were significantly associated with the growth monitoring practice of health professionals.
Health professionals who had a degree and above educational status were 3.57 times more likely to practice growth monitoring compared to diploma-level health professionals [AOR = 3.57; 95% CI: 1.54, 8.26]. With more than 11 years of work experience, health professionals were 2.98 times more likely to practice growth monitoring compared to health professionals who had less than 10 years of work experience [AOR = 2.98; 95% CI: 1.36, 6.53].
Respondents who had good knowledge of 4.60 were more likely to practice growth monitoring compared to health professionals who had poor knowledge [AOR = 4.60; 95% CI: 2.06, 10.31]. Health professionals who had favorable attitudes were 2.58 more likely to practice growth monitoring compared to health professionals who had unfavorable attitudes [AOR = 2.58; 95% CI: 1.14, 5.83]. Health professionals who had received training on growth monitoring practice were 5.11 times more likely to practice growth monitoring compared to health professionals who had not received training [AOR = 5.11; 95% CI: 2.20, 11.89].
Health professionals who saw greater than 40 children per day were 3.02 times less likely of practicing growth monitoring compared to health professionals who saw less than 25 children per day [AOR = 3.02; 95% CI: 1.16, 7.86]. Respondents who had adequate growth monitoring equipment were 4.44 times more likely to practice growth monitoring compared to those who had inadequate growth monitoring equipment [AOR = 4.44; 95% CI: 1.97, 9.98] (Table 5).
 |
Table 5 Multivariable Analysis for Growth Monitoring Practice Among Health Professionals at Public Health Centers of Bahir Dar, Northwest Ethiopia, 2021 (n = 314) |
Qualitative Result
Five in-depth interviews were conducted in the local language of Amharic with five health center medical directors. The duration of each interview was between 40 and 60 minutes. All the in-depth interviews were conducted workplace of each medical director. The in-depth interview was conducted by the principal investigator. Semi-structured open-ended interview guideline questions were prepared for an in-depth interview.
All of them had less than 10 years of work experience. Of the five medical directors, three of them were degrees and above in their level of education. Three of the medical directors were health officers in the profession and all medical directors were married.
Responsibilities of Health Facility Medical Directors
The main responsibilities of health center medical directors on growth monitoring services are facilitating and assigning GMP rooms, assigning trained and skilled health professionals for GMP services, fulfilling growth monitoring equipment, and practicing growth monitoring service as a health professional.
A 34 years old male health center medical director mentioned that
On growth monitoring, I have responsibility for the fulfillment of growth monitoring equipment, assigning health professionals, and enduring growth monitoring rooms separately. I support and supervise professionals assigned to growth monitoring who interpret growth cards and growth curves. As well, I try to participate with health professionals who assigned GMP.
A 30 years old male health officer health center manager says that
Facilitation of classroom, arrange skilled and trained health professional, fulfill materials that are necessary for GMP and follow and check how growth monitoring is done correctly are my main responsibilities.
A 32-year-old health center manager reported that
Fulfilling growth monitoring equipment, assigning professional who works in GMP program and to differentiate and give training that has gaps of ability in the health professionals are main of my responsibility in growth monitoring practice.
What Has Been Done?
Most medical directors mentioned that a growth monitoring service was mainly provided for below two years of children when there is vaccination. A 32-year-old clinical nurse, health center medical director says,
We are giving growth monitoring service with EPI in one room only a selected one day in a month. Otherwise, growth monitoring service is given by health extension worker and family health team in the community.
A 34-year-old male health center medical director reported that
Now we had built small separated room for growth monitoring until we have standard and permanent growth monitoring room …. In addition to the service that we give in our health facility, we are also giving growth monitoring service for the community with health extension professionals and with our 4 family health teams.
Importance of GMP
All health center medical directors accepted that GMP is used for children to have a healthy mental and physical structure, and also it is useful to prevent childhood malnutrition. Those medical directors said that growth monitoring and promotion service is important to build or make the future generation both mentally and physically healthy and effective society.
A 34 years old male health center medical director mentioned that
Growth monitoring is used for a child to have a healthy mental and physical structure. Especially, 1000 days of children are very necessary for children’s growth. Social development starts with the individual. If we developed the children with healthy mental and physical growth, we can also develop the society with a better cast of minds.
A 32 years old health center manager answered that “ … Children’s mental growth process time is up to 2 years old. So, at this time, practicing growth monitoring means building the society.” A 32 years old clinical nurse health center medical director says
GMP is not important only for physical growth; it has also important in mental growth, therefore, it is better to give attention through at all levels of health structure. It helps to decrease child malnutrition.
Challenges of Growth Monitoring Practice
Many challenges were identified in the growth monitoring and promotion programs. Health center medical directors mentioned that lack of growth monitoring equipment, lack of awareness of mothers and caregivers, knowledge and attitude of health professionals, increasing of unexpected and unplanned works and events, building problems, absence of support and supervision from the regarded body, absence of OTP, lack of training, attitude of the society and reporting system are the common problems that had faced during growth monitoring practice.
Lack of Growth Monitoring Equipment
Almost all medical directors reported that lack of growth monitoring equipment was the main problem when giving growth monitoring services. Growth monitoring materials that were not available in the market. GMP materials that exist in the market, the qualification problem were the major problems.
34 years old male health center medical director mentioned that
In growth monitoring room growth there is a shortage of growth charts, weight scales, measuring board/ height board growth monitoring registration book and pamphlets. Already we have reported to the responsible body, but we didn’t get any solution.
A 30 years old male health officer, health center manager, said that
The problem is the unavailability of growth monitoring equipment in the market that is used for growth monitoring practice. And also, the materials that exist in the market have their qualification problem.
Attitude and Awareness of Mothers and Caregivers
Mothers and caregivers have missed their GMP appointments because they give priority to social events and personal activities. However, some mothers are not happy to bring their children for GMP services because of a lack of awareness about GMP.
A 34 years old male health center medical director says that
There is a problem on their mothers and caregivers to bring their children in the health center. So, I believe this problem came from a lack of awareness and outlook of the parents. No any work done on the parents when and where their children’s must be weight and the importance of weighting.
Another 32-year-old male clinical nurse medical director mentioned that “ …. The society had not good attitude on growth monitoring practice ….”
A 30 years old male health officer medical director says that
Because of the lack of compassion and respect of health professionals, mothers and caregivers don’t think the importance of growth monitoring, as well as the attitude of these parents in growth monitoring, is already decreased.
Knowledge and Attitude of Health Professionals
Knowledge and attitude of health professionals had affected GMP program implementation, as mentioned by health center medical directors. A 34 years old male health center medical director mentioned that
I believe that all health professionals were learning how to give basic growth monitoring services when they learn their education. But all health professionals do not have equal attitudes, knowledge, and ability. So, it has also its influence in the carry-out process.
A 30 years old male health officer medical director mentioned
Usually, health professionals’ advents here through complicated guidance and lifestyle. So, these health professionals had low motivation to practice growth monitoring. Mainly servants are women, so they may have maternity leave plus social life. This action also had a high saddle on GMP service.
Unexpected and Unplanned Works
The main challenges in GMP service were identified, all medical directors reported having unplanned and unexpected activities in their health center and the community. Especially health insurance and the COVID-19 pandemic were stopped full growth monitoring and promotion services in a few months.
A 34-year-old male health center medical director mentioned that
Health extension program is one of the ways that we do GMP service … In this year all services including growth monitoring practice those are done by health extension workers were stopped for 2 months because of health insurance program. In addition to this, we have also stopped giving growth monitoring services because of the COVID-19 pandemic for a long period.
A 30 years old married clinical nurse medical director said that
In our health center, health extension workers give growth monitoring service. HEWs have also other additional works. In addition to this, when unplanned and unexpected works happen, the GMP services will completely stop for a few months, because of health insurance and COVID-19 pandemic works.
Problems of Building/Absence of Separated GMP Room
The major challenge identified by this study had the unavailability of a separate GMP room. It influences GMP service had given in EPI rooms in most health centers. The cause of the unavailability of separated GMP rooms had problems in the building.
A 34-year-old health center medical director said that
We don’t have standard growth monitoring room, so this also has its effect. Now we are giving service in a small and narrow room which builds from iron sheets. According to Bahir Dar’s humidity, it is difficult to work for a long time in the tin house.
Also, a 32-year-old male health officer medical director mentioned that “ … Because of building problems until now GMP does not have its separate room.” A 32-year-old clinical nurse medical director says “ … Because of the problem of the building we are giving growth monitoring service with EPI in one room.” Moreover, a 30 years old male health officer medical director says “ … Without fulfillment of infrastructure problems, trying to solve other problems become like fire extinction.”
Lack of Human Resource
All the interview medical directors mentioned that the lack of skilled health professionals had the main challenge in GMP service. Because of the shortage of health professionals, GMP services had not been given to apply separately as a program like IMNCI, ANC, and other services. This increases the workload of other health professionals to perform GMP.
A 34-year-old male health center medical director mentioned that
In our health center there is a high shortage of human resource. For example, the numbers of health extension workers were 50% lower than what we need. Because of this, we didn’t satisfy our society, and we couldn’t make society come here for growth monitoring service. Plus, in our health center, there is a lack of health professionals who works in other routine care services.
A 32 years old male health officer medical director says that
The ratio of health extension workers and households is very far from each other. For example: - in one kebele there are more than 17,000 households. But only 2 HEWs are assigned in the kebele. The advisable ratio of health extension workers and households is not to be more than 1 to 530. But now they have a ratio of 1:8500 … In our institution, we have 9 health extension workers. But we need more than 140 HEWs.
A 30 years old male health officer, health center manager mentioned that
As an institution, shortage of health professionals is one of our encountered problems when doing growth monitoring. Especially, there is a high shortage of health extension workers …. The lack of skilled health professionals is not only a problem for growth monitoring, it is also a problem for other health-related works. Because of this, we could not assign a health professional for only growth monitoring practice.
Absence of Support and Supervision
All five medical directors reported that there was no support and supervision from the regional health bureau and city health office regarding growth monitoring and promotion service. A 34 years old male health center medical director says “ … We didn’t get any supportive supervision for the growth monitoring and promotion service from regional health bureau and city health office.”
A 32-year-old male health officer mentioned that “ … According to GMP, we didn’t get any support and supervision either regional health bureau or city health office.” Also, a 32 years old male clinical nurse medical director says “ … We had never got any support and supervision in growth monitoring from regional health bureau and city health office.” A 30 years old married clinical nurse medical director “ … We never get any support and supervision from the regarded body.”
Absence of OTP
Accordingly, health center medical directors report there is no OTP service in the health facility. Because of the unavailability of OTP services, children who had outpatient therapeutic feeding services were referred to hospitals.
A 34-year-old male health center medical director mentioned that “ … Absence of OTP service in our health center has a big influence on intervention after growth monitoring was practiced.” Also, A 32-year-old male medical director says,
When the health extension workers weigh the children if they need inpatient service, they will refer them to the hospital because we didn’t have OTP service.
Lack of Training
Some health professionals reported that training is one method of full health professionals’ attitude, knowledge, and practical skill about the specific program. However, the regarded body had not prepared insight training about growth monitoring.
A 30 years old male health officer, health center manager believes that
I have been here for 2 years in these health institutions. There was no training that was given to health professionals …. Now we are practicing with health professionals who betake the training before 2 years.
Also, a 30 years old married clinical nurse medical director says that “ … As a health center there is no any training which is given for health professionals on GMP for the last few years.”
Problems with a Reporting System
A 30 years old married clinical nurse health center medical director reported
GMP reports indicate the hard worker as rusty and the rusty as hard workers. For example: - one health center stayed for 11 months without a growth monitoring service and if it is done 100% GMP in the 12th month, the report had done reported as the annual coverage of growth monitoring is 100% only by the GMP service of only one month. If you give growth monitoring service for 11 months and if didn’t do because of many tasks in the 12th month, your growth monitoring annual performance becomes zero.
Recommendations of Health Facility Medical Directors
All health center medical directors recommended that all regarded bodies like health professionals, city health office managers, regional health bureau regarded bodies, federal ministry of health, NGOs, and the community members should be working with collaboration for good growth monitoring and promotion implementation program.
A 32 years old male health officer, health center manager recommended that
Both regional health bureau and city health office could be assigned professionals, to solve building problem, to make support and supervision for good coverage of GMP …
Other A 34-year-old male, health officer, health center medical director
Giving attention for growth monitoring and promotion service from the inspection regional health bureau and city health office like ANC, FP, TB and HIV to works perfectly ….
A 30 years old male clinical nurse medical director
I recommended for regional health bureau and city health office, that prepare training, to make regular supportive supervision, to fulfill lack of growth monitoring equipment, assigning skilled health professionals in GMP program, adjust annual GMP reporting system, build GMP room separately.
Discussion
This study showed that the overall prevalence of growth monitoring practice among health professionals was 30.3% (95% CI, 25.5, and 35.4). This is lower compared to the prevalence of the previous studies done in Gondar, Tigray, and South Africa, which was a prevalence of 50.4%, 53.6%, and 60%, respectively.17,22,23 Also, which is also lower compared to the 2016 EDHS and 2019 mini EDHS reports which were 62% and 48%, respectively.24,25 However, which is higher than to 2020 Bahir Dar city health office report which was 18% (63), and lower than the 2021 nine-month report which is 39% (64). The reason might be the effect of the COVID-19 pandemic26 this is supported by qualitative results and the health facility set up may be different,27 study setting,28–30 assessment method used, sample size of the study, lack of training of health professionals31 and socio-demographic factors.
Health professionals whose working experience is 11 years and more were 2.98 times more likely to practice growth monitoring than their counterparts. This is in line with the previous study conducted in Ethiopia.22 The reason might be increased work experience enable health professionals to have more chance to experience and perform procedures related to growth monitoring practice.32 However, a study done in South Africa shows work experience inversely affected growth monitoring practice.17
Having a BSc degree and above level of educational status health professionals were 3.57 times more likely to practice growth monitoring than diploma health professionals. This may be due to increased education status may have a positive effect to acquire theories and procedures to perform growth monitoring practices.33,34
Health professionals who had good knowledge about growth monitoring were 4.60 times more likely to practice growth monitoring than those who had poor knowledge. A similar finding was reported from the study done in Nepal,12 Ghana,21,35 South Africa,17 and Tigray.36 The reason might be, knowledge is the basis of any activities. Generally, knowledge and skill had important to practice and implement different health care.12,29,34,37,38
The odds of health professionals who had a favorable attitude about growth monitoring practice was 2.58 times more likely to practice growth monitoring than those who had unfavorable attitudes. This study was supported by qualitative results and contradicted a study in South Africa, Tigray, and Gondar.17,22,23 This might be due to differences in socio-demographic factors and lack of training.12,33,38
Respondents who had adequate growth monitoring equipment were 3.83 times more likely to practice growth monitoring than health professionals who had inadequate growth monitoring equipment. This result is in line with a study conducted in Brazil, Tigray, and Gondar22,23,39 and supported by a qualitative study. This might be due to the availability of equipment for service provision can directly influence the satisfaction of health professionals. Moreover, it is critical for the improvement of health professionals’ health care.28,40
Health professionals who received training were 4.44 times more likely to practice growth monitoring than health professionals who had not received any training towards GMP. This finding is consistent with studies conducted in Nepal12 and Tigray Ethiopia.23 The result was supported by a qualitative study. The possible reason might be health professionals who received training health professionals had to acquire technical skills, interpersonal skills, and solid knowledge to perform their jobs efficiently in the workplace. There most of the previous studies provide evidence that there is a strong positive relationship between training and growth monitoring practice.12,29,33,38,41–44
Health professionals who had seen less than 25 children per day were 3.02 times more likely to practice growth monitoring compared to health professionals who saw greater than 40 children per day. This finding was supported by a study done in Ghana, South Africa, and Tigray.17,21,23 The reason might be busy health professionals are only concerned for acutely sick children compared to healthy-looking children.32,45–48
The qualitative result showed that lack of awareness of mothers and caregivers, knowledge and attitude of health professionals, lack of health professionals, lack of growth monitoring equipment, an increase of unexpected and unplanned works and events, building problems, absence of support and supervision from the regarded body, absence of OTP, lack of training and reporting system are the common problems that had faced during growth monitoring practice. This result was supported by a study conducted by Tigray and Gondar.22,49 The reason might be lack of budget, lack of multi-sectoral collaboration, lack of motivation and knowledge of the society.
A qualitative finding indicated that “ … We had never gotten any support and supervision in growth monitoring from regional health bureau and city health office ….” Another 34-year-old medical director says “ … We didn’t get any supportive supervision for the growth monitoring and promotion service from regional health bureau and city health office.” The possible reason might be the regarded body had given supportive supervision at a specific period, it might be identified the problem and provided feedback on who was affecting the growth monitoring service and solving those factors appropriately. Also, this might be because supervision has a significant role in identifying the gaps and improving health workers’ performance.29,33,38,41,50
Unplanned and unexpected works had their effect on growth monitoring and promotion programs. A 34 years old male health center medical director says,
In this year all works including growth monitoring practice that are done by health extension workers were stopped for 2 months because of health insurance program. In addition to this, we have also stopped giving growth monitoring services because of the COVID-19 pandemic for a month.
Unplanned and unexpected work had a negative relationship with good work performance.26,30
A 34-year-old male medical director mentioned that lack of growth monitoring equipment had one of the factors to influence growth monitoring service
In growth monitoring room growth there is a shortage of growth charts, weight scales, measuring board/ height board growth monitoring registration book and pamphlets. Already we have reported to the responsible body, but we didn’t get any solution.
The challenges reported in our study are similar to the challenges found in the study conducted in Gondar, and Tigray.22,23,49 Also, there might be adequate equipment in direct relation to health professionals’ work performance.28
All the interviewed medical directors mentioned that the lack of skilled health professionals had the main challenge in GMP service. Because of the shortage of health professionals, GMP services had not been given to apply separately as a program like IMNCI, ANC, and other services. This lack of human resources overcomes the workload of other health professionals.
A 32 years old male health officer medical director says that
The ratio of health extension workers and households is very far from each other. For example: - in one kebele there are more than 17,000 households. But only 2 HEWs are assigned in the kebele. The advisable ratio of health extension workers and households is not to be more than 1 to 530. But now they have a ratio of 1:8500 … In our institution, we have 9 health extension workers. But we need more than 140 HEWs.
The finding reported in this study is similar to challenges identified in Gondar, and Tigray.22,23 The reason might be a shortage of health professionals had a direct relation to workload and workload affects health professionals’ work performance.37,45–47,51
Conclusion
The finding of the study suggested that the prevalence of growth monitoring practice among health professionals of Bahir Dar public health centers was low. This study had identified work experience, educational status, knowledge, attitude, workload, training, and availability of growth monitoring equipment were key predictors of growth monitoring practice among health professionals in Bahir Dar. Also, lack of support and supervision from the regarded body, attitude of mothers and caregivers, lack of OTP service, unplanned and unexpected work, and lack of health professionals were factors affecting growth monitoring service identified by the qualitative method.
Recommendation
For the Ministry of Health
Modify reporting format of growth monitoring promotion service.
For Bahir Dar City Health Office
A growth monitoring and promotion program will be needed to ensure a good training package, adequate growth monitoring equipment, regular supportive supervision, a separate growth monitoring room, adequate human resource, and strong community involvement.
For Health Facilities
- Growth monitoring and promotion are given as much attention as other health needs in childhood such as immunization, IMNCI programs.
- The health facility needs to support health extension programs and family health teams to have a continuous and regular GMP service.
For Health Professionals
- All health professionals that come in contact with mothers and caregivers should promote growth monitoring and promotion services.
- Instead of looking for higher official supervision and training, all health professionals need to update themselves and take the initiative of GMP service.
For Researchers
Further studies may conduct the mother’s perspective to address additional factors regarding growth monitoring practice.
For NGOs
NGOs need to work in partnership with governmental sectors to early detection of growth failure and prevent children’s undernutrition by supporting the provision of growth monitoring equipment, facilitating training, and building separate growth monitoring rooms.
Strength and Limitations of the Study
Due to the nature of this study design, it is limited to showing cause and effect relationships. Despite this limitation, mixed approach (qualitative and quantitative) is used to increase the validity of the data.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Crude Odds Ratio; EDHS, Ethiopian Demography, and Health Survey; EPHI, Ethiopian Public Health Institute; EPI, Expanded Program for Immunization; FDRE, Federal Democratic Republic of Ethiopia; GM, Growth Monitoring; GMP, Growth Monitoring and Promotion; IYCN, Infant and Young Child Nutrition; HAD, Health Development Army; HEWs, Health Extension Workers; KAP, Knowledge, Attitude, and Practice; KMU, Kotebe Metropolitan University; NI, Nutritional Intervention; OTP, Outpatient Therapeutic Feeding Program; PHW, primary Health Worker; PI, Principal Investigator; UNICEF, United Nation International Children’s Fund; WHO, World Health Organization.
Data Sharing Statements
All data are available upon reasonable request and the readers could contact the corresponding author.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the institutional review board of Kotebe metropolitan university, Menelik-II medical and health Science College (Reference no አጠ5/38/12/2781). The necessary permission to undertake the study was obtained from Amhara Region public health institute and the Bahir Dar city health office. Before data collection, each respondent was informed about the aim of the study, the possible benefit of the study, confidentiality, and publication of their anonymized responses. Written informed consent was obtained, and all respondents were assured that they have a full right to refuse to participate whenever during the interview without any negative connotation on their future service. All COVID-19 prevention measurements were applied at the time of data collection.
Acknowledgment
Public health facilities of Bahir Dar health center administrative and technical staff, data collectors, and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; They took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding has been received for the conduct of this study and/or the preparation of this manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Mangasaryan N, Arabi M, Schultink W. Revisiting the concept of growth monitoring and its possible role in community-based nutrition programs. Food Nutr Bull. 2011;32(1):42–53. doi:10.1177/156482651103200105
2. Malina RM, Bouchard C, Bar-Or O. Growth, Maturation, and Physical Activity. Human kinetics; 2004.
3. Ashworth A, Shrimpton R, Jamil K. Growth monitoring and promotion: review of evidence of impact. Matern Child Nutr. 2008;4:86–117. doi:10.1111/j.1740-8709.2007.00125.x
4. Achadi E, Ahuja A, Bendech MA, et al. Global nutrition report 2016: from promise to impact: ending malnutrition by 2030. International Food Policy Research Institute; 2016.
5. Sambu W. Child health: nutrition; 2019:234–239.
6. Wegayehu E. Determinants of underweight among under-five children in Ethiopia: ordinal and multilevel logistic regression model approach; 2019.
7. Edhs M. Ethiopia mini demographic and health survey. Ethiopia: Central Statistical Agency Addis Ababa; 2014.
8. Harris J, Frongillo EA, Nguyen PH, Kim SS, Menon P. Changes in the policy environment for infant and young child feeding in Vietnam, Bangladesh, and Ethiopia, and the role of targeted advocacy. BMC Public Health. 2017;17(2):107–123. doi:10.1186/s12889-017-4343-3
9. Abbas S, Mahmood MJ, Yaseen M. Assessing the potential for rooftop rainwater harvesting and its physio and socioeconomic impacts, Rawal watershed, Islamabad, Pakistan. Environ, Develop Sustain. 2021;4:1–22.
10. Scherdel P, Salaün J-F, Robberecht-Riquet M-N, et al. Growth monitoring: a survey of current practices of primary care paediatricians in Europe. PLoS One. 2013;8(8):e70871. doi:10.1371/journal.pone.0070871
11. De Onis M, Wijnhoven TM, Onyango AW. Worldwide practices in child growth monitoring. J Pediatr. 2004;144(4):461–465. doi:10.1016/j.jpeds.2003.12.034
12. Pollifrone MM, Cunningham K, Pandey Rana P, et al. Barriers and facilitators to growth monitoring and promotion in Nepal: household, health worker and female community health volunteer perceptions. Matern Child Nutr. 2020;16(4):e12999. doi:10.1111/mcn.12999
13. Taylor L. From food crisis to nutrition: challenges and possibilities in Ethiopia’s nutrition sector. Institute for Development Studies; 2012.
14. MoH F. Health sector transformation plan. Addis Ababa, Ethiopia; 2015.
15. Habtewold TD, Mohammed SH, Endalamaw A, et al. Higher educational and economic status are key factors for the timely initiation of breastfeeding in Ethiopia: a review and meta‐analysis. Acta Paediatrica. 2020;109(11):2208–2218. doi:10.1111/apa.15278
16. Ababa A. Federal Democratic Republic of Ethiopia central statistical agency population projection of Ethiopia for all regions at Wereda level from 2014–2017. Addis Ababa: Central Statistical Agency; 2014.
17. Smith S, Reji E. Doctors’ attitudes to and knowledge and usage of growth charts. South Afr Fam Pract. 2015;57(3):1–4. doi:10.1080/20786190.2014.976978
18. Wubie AM, de Vries WT, Alemie BK. A socio-spatial analysis of land use dynamics and process of land intervention in the peri-urban areas of Bahir Dar City. Land. 2020;9(11):445. doi:10.3390/land9110445
19. Admassie A, Abebaw D, Woldemichael AD. Impact evaluation of the Ethiopian health services extension programme. J Develop Effect. 2009;1(4):430–449. doi:10.1080/19439340903375724
20. Creswell JW, Poth C Qualitative Inquiry and Research Design: Choosing Among Five Approaches. Thousand Oaks, CA: Sage publications; 2007.
21. Sulley I, Abizari A-R, Ali Z, et al. Growth monitoring and promotion practices among health workers may be suboptimal despite high knowledge scores. BMC Health Serv Res. 2019;19(1):1–9. doi:10.1186/s12913-019-4103-4
22. Melkamu AW, Bitew BD, Muhammad EA, Hunegnaw MT. Prevalence of growth monitoring practice and its associated factors at public health facilities of North Gondar zone, northwest Ethiopia: an institution-based mixed study. BMC Pediatr. 2019;19(1):1–8. doi:10.1186/s12887-019-1489-4
23. Baraki T, Gebru AA, Belay D. Knowledge attitude and practice of health extension workers towards growth monitoring and promotion program in Tigray region, Ethiopia. Eur J Biomed Pharm Sci. 2018;3(4):55–64.
24. Central Statistical Agency - CSA/Ethiopia, ICF. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
25. Ethiopian Public Health Institute - EPHI, Federal Ministry of Health - FMoH, ICF. Ethiopia mini demographic and health survey 2019. EPHI/FMoH/ICF. Addis Ababa, Ethiopia; 2021.
26. Menendez C, Gonzalez R, Donnay F, Leke RG. Avoiding indirect effects of COVID-19 on maternal and child health. Lancet Global Health. 2020;8(7):e863–e4. doi:10.1016/S2214-109X(20)30239-4
27. Getachew T, Kedir I, Bekele A, et al. Child health service provision in Ethiopia: outpatient, growth monitoring and immunization. Ethiop J Health Dev. 2017;31(2):67–74.
28. Merga H, Fufa T. Impacts of working environment and benefits packages on the health professionals’ job satisfaction in selected public health facilities in eastern Ethiopia: using principal component analysis. BMC Health Serv Res. 2019;19(1):1–8. doi:10.1186/s12913-019-4317-5
29. Fort AL, Voltero L. Factors affecting the performance of maternal health care providers in Armenia. Hum Resour Health. 2004;2(1):1–11. doi:10.1186/1478-4491-2-8
30. World Health Organization. The impact of the COVID-19 pandemic on noncommunicable disease resources and services: results of a rapid assessment; 2020.
31. Abebe AM, Kassaw MW, Mengistu FA. Assessment of factors affecting the implementation of integrated management of neonatal and childhood illness for treatment of under five children by health professional in health care facilities in Yifat Cluster in North Shewa Zone, Amhara Region, Ethiopia. Int J Pediatr. 2019;2019:45.
32. Lu Y, Hu X-M, Huang X-L, et al. Job satisfaction and associated factors among healthcare staff: a cross-sectional study in Guangdong Province, China. BMJ Open. 2016;6(7):e011388. doi:10.1136/bmjopen-2016-011388
33. Chmielewska M, Stokwiszewski J, Filip J, Hermanowski T. Motivation factors affecting the job attitude of medical doctors and the organizational performance of public hospitals in Warsaw, Poland. BMC Health Serv Res. 2020;20(1):1–12. doi:10.1186/s12913-020-05573-z
34. Bayona JA, Caballer A, Peiró JM. The relationship between knowledge characteristics’ fit and job satisfaction and job performance: the mediating role of work engagement. Sustainability. 2020;12(6):2336. doi:10.3390/su12062336
35. Nsiah-Asamoah C. Gaps in knowledge levels of health workers on recommended child feeding practices and growth monitoring and promotion actions. Ped Health Res. 2018;3(2):8.
36. Charlton KE, Kawana BM, Hendricks MK. An assessment of the effectiveness of growth monitoring and promotion practices in the Lusaka district of Zambia. Nutrition. 2009;25(10):1035–1046. doi:10.1016/j.nut.2009.03.008
37. Roberfroid D, Lefèvre P, Hoerée T, Kolsteren P. Perceptions of growth monitoring and promotion among an international panel of district medical officers. J Health Popul Nutr. 2005;34:207–214.
38. Shiferaw AM, Zegeye DT, Assefa S, Yenit MK. Routine health information system utilization and factors associated thereof among health workers at government health institutions in East Gojjam Zone, Northwest Ethiopia. BMC Med Inform Decis Mak. 2017;17(1):1–9. doi:10.1186/s12911-017-0509-2
39. Pedraza DF, Santos IS. Assessment of growth monitoring in child care visits at the Family Health Strategy in two municipalities of Paraíba State, Brazil. Epidemiologia e Serviços de Saúde. 2017;26:847–855. doi:10.5123/S1679-49742017000400015
40. Arora M, Gigras Y. Importance of supply chain management in healthcare of third world countries. Int J Supply Oper Manag. 2018;5(1):101–106.
41. Dieleman M, Toonen J, Touré H, Martineau T. The match between motivation and performance management of health sector workers in Mali. Hum Resour Health. 2006;4(1):1–7. doi:10.1186/1478-4491-4-2
42. Sendawula K, Nakyejwe kimuli S, Bananuka J, Najjemba Muganga G. Training, employee engagement and employee performance: evidence from Uganda’s health sector. Cogent Bus Manage. 2018;5(1):1470891. doi:10.1080/23311975.2018.1470891
43. Sal A, Raja M. The impact of training and development on employees performance and productivity. Int J Manag Sci Bus Res. 2016;5:7.
44. Irimu GW, Gathara D, Zurovac D, et al. Performance of health workers in the management of seriously sick children at a Kenyan tertiary hospital: before and after a training intervention. PLoS One. 2012;7(7):e39964. doi:10.1371/journal.pone.0039964
45. Roberfroid D, Kolsteren P, Hoeree T, Maire B. Do growth monitoring and promotion programs answer the performance criteria of a screening program? A critical analysis based on a systematic review. Trop Med Int Health. 2005;10(11):1121–1133. doi:10.1111/j.1365-3156.2005.01498.x
46. MacPhee M, Dahinten VS, Havaei F. The impact of heavy perceived nurse workloads on patient and nurse outcomes. Administrat Sci. 2017;7(1):7. doi:10.3390/admsci7010007
47. Goh ML, Ang EN, Chan Y-H, He H-G, Vehviläinen-Julkunen K. Patient satisfaction is linked to nursing workload in a Singapore hospital. Clin Nurs Res. 2018;27(6):692–713. doi:10.1177/1054773817708933
48. Kokoroko E, Sanda MA. Effect of workload on job stress of Ghanaian OPD nurses: the role of coworker support. Saf Health Work. 2019;10(3):341–346. doi:10.1016/j.shaw.2019.04.002
49. Bilal SM, Moser A, Blanco R, Spigt M, Dinant GJ. Practices and challenges of growth monitoring and promotion in Ethiopia: a qualitative study. J Health Popul Nutr. 2014;32(3):441.
50. Mor Barak ME, Travis DJ, Pyun H, Xie B. The impact of supervision on worker outcomes: a meta-analysis. Soc Serv Rev. 2009;83(1):3–32. doi:10.1086/599028
51. Schneider AM, Oppel E-M, Winter V. Explaining variations in hospitals’ use of strategic human resource management: how environmental and organizational factors matter. Health Care Manage Rev. 2021;46(1):2–11. doi:10.1097/HMR.0000000000000242
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.