Back to Journals » Drug Design, Development and Therapy » Volume 20
Granisetron Reduces Norepinephrine Requirement for Preventing Post‑Induction Hypotension in Elderly Patients Undergoing Laparoscopic Gastrointestinal Surgery
Authors Zhang Y, Chu M, Zhou Y, Chen G ![]()
Received 16 March 2026
Accepted for publication 3 June 2026
Published 23 June 2026 Volume 2026:20 609499
DOI https://doi.org/10.2147/DDDT.S609499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Yanting Zhang,1,* Miaofei Chu,1,2,* Youfa Zhou,1 Gang Chen1
1Department of Anesthesiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Department of Anesthesiology, Zhejiang Greentown Cardiovascular Hospital, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Youfa Zhou, Gang Chen, Department of Anesthesiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Qingchun East Road No. 3, Hangzhou, 310020, People’s Republic of China, Tel +8613615719892, Fax +86 571 86044817, Email [email protected]; [email protected]
Background: Prophylactic antiemetics are routinely used in gastrointestinal surgery. This study investigated whether granisetron pretreatment alters norepinephrine requirements for preventing post-induction hypotension in elderly patients.
Methods: In this randomized double-blind trial, 64 patients (60– 74 years) undergoing laparoscopic gastrointestinal resection received intravenous granisetron (3 mg) or saline placebo before induction. The 50% effective dose (ED50) of norepinephrine to prevent hypotension (> 20% decrease in mean arterial pressure) within 30 min post-induction was determined using the up-down sequential method, with probit regression as confirmatory analysis.
Results: Baseline characteristics were comparable between the two groups. The up-down sequential analysis revealed that the ED50 of norepinephrine was significantly lower in the granisetron group (0.037 μg/kg/min [95% CI 0.031– 0.040 μg/kg/min]) than in the control group (0.049 μg/kg/min [95% CI 0.043– 0.052 μg/kg/min]) (P < 0.001) representing an approximate 24% reduction. This finding was supported by probit regression analysis, which estimated ED50 values of 0.040 μg/kg/min [95% CI 0.033– 0.051 μg/kg/min] and 0.052 μg/kg/min [95% CI 0.045– 0.064 μg/kg/min] for the granisetron and control groups, respectively. No significant difference was observed in the incidence of postoperative nausea and vomiting between the two groups.
Conclusion: Granisetron pretreatment significantly reduces the ED50 of norepinephrine required to prevent post-induction hypotension in elderly patients by approximately 24% indicating a pharmacodynamic interaction consistent with enhanced vasopressor efficacy. These findings indicate that pre-induction antiemetic administration may represent a potentially favorable timing strategy.
Keywords: hypotension, norepinephrine, granisetron, elderly, laparoscopic gastrointestinal surgery, effective dose 50, ED50
Background
Hypotension after the induction of general anesthesia (GAIH) is a frequent and clinically significant complication during the peri-induction period. Studies indicate a high incidence, with rates of 73.2% observed between anesthesia induction and endotracheal intubation, and up to 96.8% from intubation until skin incision.1 GAIH is typically defined as a reduction in mean arterial pressure or systolic blood pressure exceeding 20% from baseline values.
Laparoscopic gastrointestinal surgery requires general anesthesia and the creation of an artificial pneumoperitoneum, which increases intra-abdominal pressure and may compromise cardiovascular and respiratory function.2–4 Patients undergoing gastrointestinal surgery are at increased risk due to prolonged preoperative fasting, potential chronic hypovolemia from inadequate nutrient absorption, and bowel preparation—all of which may contribute to relative intravascular volume depletion and electrolyte disturbances.5–8 This risk is further amplified in elderly patients, whose diminished cardiovascular reserve makes them particularly susceptible to GAIH and subsequent imbalances in myocardial oxygen supply and demand, even with adjusted anesthetic dosing.
Prophylactic administration of vasoactive agents to prevent GAIH has been extensively investigated, among which norepinephrine has emerged as the most commonly used and first-line vasopressor due to its potent α-adrenergic-mediated vasoconstriction and moderate β1-adrenergic effects that counteract anesthesia-induced vasodilation and myocardial depression.5,9,10 From a clinical perspective, reducing the required dose of norepinephrine is desirable, as it may minimize dose‑dependent adverse effects including tachycardia, arrhythmias, and excessive vasoconstriction-induced tissue hypoperfusion, particularly in elderly patients with limited cardiovascular reserve.
Concurrently, patients undergoing gastrointestinal surgery are at high risk for postoperative nausea and vomiting (PONV), for which 5-HT3 receptor antagonists like granisetron are routinely administered. Intriguingly, emerging evidence suggests that 5‑HT3 antagonists may also modulate cardiovascular reflexes. For instance, ondansetron and granisetron have been shown to attenuate hypotension and bradycardia associated with neuraxial anesthesia, an effect attributed to blockade of the Bezold–Jarisch reflex.11–14 Recent clinical data further indicate that prophylactic granisetron can reduce the incidence of GAIH in elderly patients.15 However, these studies focused primarily on hypotension incidence rather than vasopressor dose requirements, leaving the potential pharmacodynamic interaction between granisetron and norepinephrine largely unexplored. It is currently unknown whether pre‑administration of granisetron influences the dose requirement or efficacy of norepinephrine in preventing GAIH.
Therefore, beyond simply reducing the incidence of hypotension, understanding whether granisetron alters the norepinephrine dose requirement has direct clinical implications. A reduced norepinephrine 50% effective dose (ED50) would suggest a pharmacodynamic sparing effect, potentially allowing clinicians to achieve adequate blood pressure control with lower vasopressor exposure. This study aimed to investigate the effect of granisetron pretreatment on the ED50 of norepinephrine for preventing hypotension following anesthesia induction in elderly patients undergoing elective laparoscopic gastrointestinal surgery.
Materials and Methods
Ethical Approval and Trial Registration
This prospective, randomized, double-blind, controlled trial was approved by the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine (Approval No. 2022–0030) and registered at the Chinese Clinical Trial Registry (Registration No. ChiCTR2200061900). Written informed consent was obtained from all participants. The study was conducted in accordance with the CONSORT guidelines and the Declaration of Helsinki.
Study Subjects
Seventy patients, aged 60–74 years, scheduled for elective laparoscopic gastroenterectomy were initially enrolled. Inclusion criteria were: American Society of Anesthesiologists physical status II, body mass index (BMI) between 18.0 and 24.0 kg/m2, and the presence of one or two high-risk factors for postoperative nausea and vomiting (PONV).
Exclusion criteria included: a significant history of cardiovascular or cerebrovascular disease; severe arrhythmia, cardiac insufficiency, or severe valvular heart disease; severe respiratory disease; uncontrolled hypertension (grade II or above) or long-term use of angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB); hyperthyroidism; hepatic or renal insufficiency; uncontrolled diabetes mellitus; gastrointestinal obstruction; known allergy to the study drugs or anesthetic agents; and being part of a vulnerable population (eg., those with mental illness, critical illness, cognitive impairment, or illiteracy).
Intraoperative exclusion criteria were: requirement for drug doses exceeding the predefined induction regimen, difficult airway management, failure of radial artery or internal jugular vein catheterization, or voluntary withdrawal by the subject. Patients who were excluded were replaced, with the next enrolled subject assigned to the same group. Dose allocation was performed by an independent researcher who was not involved in patient recruitment. This ensured that allocation concealment was maintained throughout the replacement process.
Study Protocol and Intervention
Eligible patients were randomly allocated into one of two groups using a computer-generated sequence. Allocation concealment was achieved using sequentially numbered, opaque, sealed envelopes. The granisetron group (Group G) received 3 mg of granisetron diluted in 20 mL of normal saline intravenously 30 minutes before anesthesia induction, whereas the control group (Group C) received 20 mL of normal saline at the same time point. To ensure that all patients received prophylaxis against postoperative nausea and vomiting (PONV), Group C was administered 3 mg of granisetron diluted in 20 mL of normal saline at the end of surgery, while Group G received 20 mL of normal saline at that time. The investigators, attending anesthesiologists, and outcome assessors were blinded to group assignment.
Up-and-Down Sequential Method
A sequential up-and-down method was employed to determine the 50% effective dose (ED50) of norepinephrine for preventing hypotension. The starting infusion rate of norepinephrine was set at 0.03 μg/kg/min, initiated immediately after anesthesia induction. The response of each patient determined the dose for the subsequent patient in the same group. If hypotension (defined as a mean arterial pressure decrease >20% from baseline or systolic blood pressure <90 mmHg) occurred within 30 minutes post-induction, the norepinephrine dose for the next patient was increased by 0.005 μg/kg/min. If hypotension did not occur, the dose for the next patient was decreased by the same increment.
Anesthetic Management and Monitoring
Upon arrival in the operating room, standard monitoring was established, including electrocardiography, pulse oximetry, and spectral entropy (SE). A 20G intravenous catheter was inserted for fluid administration (lactated Ringer’s solution, 5–7 mL/kg as a preload). Invasive arterial pressure monitoring via radial artery catheterization and central venous access via the right internal jugular vein were established.
Anesthesia was induced with intravenous midazolam (0.03 mg/kg), sufentanil (0.5 μg/kg), cisatracurium (0.15 mg/kg), and propofol (1.5 mg/kg). Supplemental propofol (0.5 mg/kg) was given if SE remained above 60. Tracheal intubation was performed when SE reached 40–60. Anesthesia was maintained with propofol infusion (3 mg/kg /h), remifentanil (6 μg/kg/h), dexmedetomidine (0.4 μg/kg/h), and sevoflurane (1–1.5%). Mechanical ventilation was set to volume-controlled mode. Intraoperative fluid maintenance consisted of lactated Ringer’s solution at 5 mL/kg/h. During the observation period, if a patient’s blood pressure decreased by more than 20% from the baseline value following norepinephrine infusion after the induction of general anesthesia, ephedrine (6 mg) was administered intravenously to elevate blood pressure. If blood pressure increased by more than 20% above the baseline, the norepinephrine infusion was temporarily discontinued, and anti-hypertensive treatment was administered if necessary. In cases of severe bradycardia (heart rate < 45 beats per minute), atropine (0.3 mg) was given to increase the heart rate.
Data Collection
Demographic and baseline clinical data were recorded. For each patient, the assigned norepinephrine dose and the occurrence of hypotension were documented. Hemodynamic parameters—systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and heart rate (HR)—were recorded at predefined time points: 1 minute before induction; 1, 3, and 5 minutes after induction; and 1, 3, 5, 10, 15, and 20 minutes after tracheal intubation. Moreover, The incidence of adverse events, including hypertension (MAP >120% of baseline), hypotension (MAP <80% of baseline), bradycardia (heart rate <60 beats per minute), and postoperative nausea and vomiting (PONV) within 24 hours after surgery, was documented during the study observation period.
Sample Size Determination and Statistical Analysis
The sample size was determined a priori. According to established methodological recommendations for sequential design trials, a sample of 20 to 40 participants per group is generally considered sufficient to obtain a reliable estimate of the ED50.16 Accordingly, we planned to enroll 32 patients in each group. We acknowledge that no externally validated minimal clinically important difference (MCID) for norepinephrine ED50 has been published in this specific clinical setting. Therefore, we prospectively defined a ≥20% reduction as clinically meaningful based on a 26% reduction in phenylephrine ED50 by ondansetron (another 5‑HT3 antagonist) has been reported as clinically beneficial.13
The primary outcome was the ED50 of norepinephrine for preventing post-induction hypotension, calculated using the up-and-down sequential method. The ED50 was initially determined by calculating the mean of the crossover midpoints for all independent pairs of subjects within the sequence, where the response transitioned from “ineffective” to “effective”. The corresponding 95% confidence interval (CI) and standard error were computed using the method described by Choi,17 and group differences in ED50 values were compared using the “estimate()” and “compare()” function from the R package “ed50simulation” (version 0.1.1).
Continuous variables were expressed as mean ± standard deviation or median [interquartile range] based on their distribution, which was assessed using the Kolmogorov–Smirnov test. Comparisons between groups were performed using the independent Student’s t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were presented as counts (percentages) and analyzed using the Chi-square test or Fisher’s exact test.
A probit regression analysis was performed as a sensitivity analysis to validate the primary ED50 estimation. The numbers of patients with “effective” and “ineffective” responses at each administered dose level were used for the model fit. This analysis provided an alternative estimate of the ED50 and its 95% CI for each group.
Statistical analyses were performed using GraphPad Prism (version 6.0, GraphPad Software, San Diego, CA, USA) and R (version 4.3.1). A two-tailed P-value < 0.05 was considered statistically significant.
Results
From July 15 to November 15, 2022, a total of 70 patients were screened for eligibility. Of these, five did not meet the inclusion criteria, and one declined to participate. Ultimately, 64 subjects provided written informed consent, were randomized, and completed the study, with 32 patients assigned to each group. The study flow diagram is presented in Figure 1.
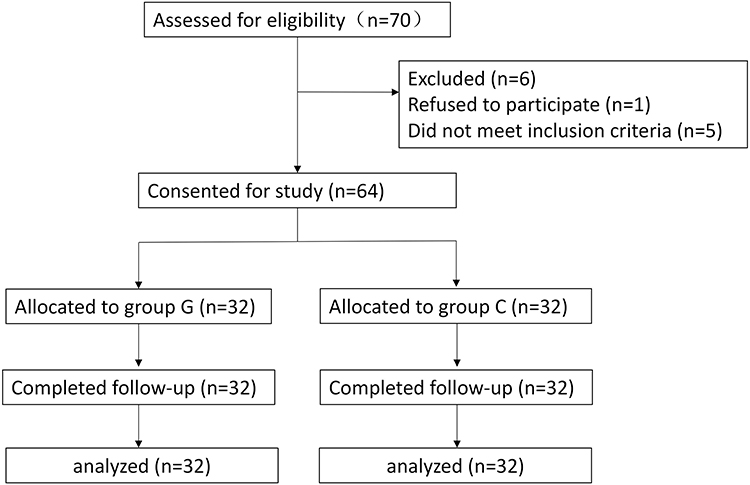 |
Figure 1 CONSORT diagram showing the flow of patients through the study. |
Baseline characteristics were well balanced between the two groups. No significant differences were observed between the two groups of elderly patients in terms of age, sex, height, weight, metabolic equivalent of task (MET) classification, history of cardiovascular or cerebrovascular diseases, arrhythmia, liver function, baseline MAP, or baseline HR (all P > 0.05), as summarized in Table 1.
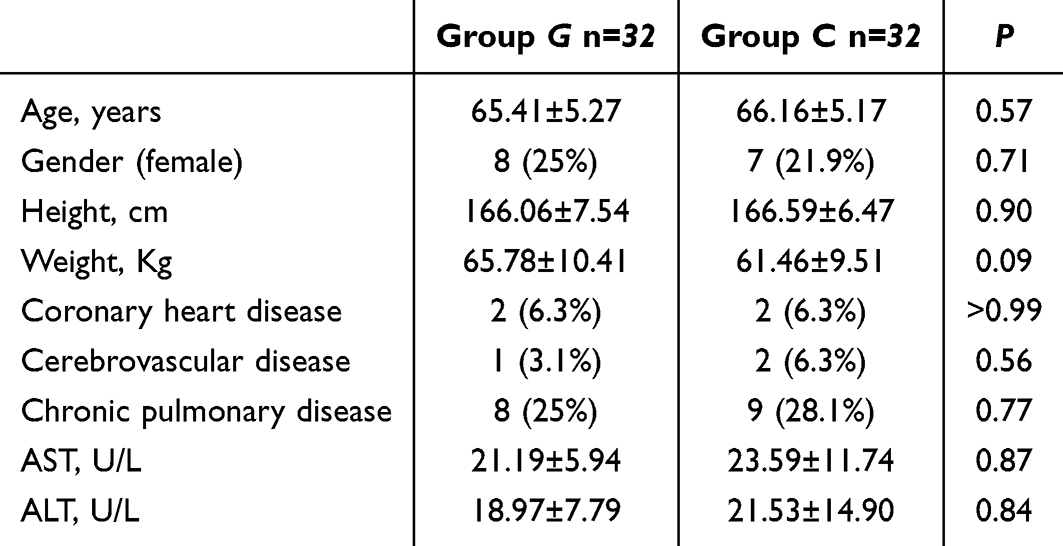 |
Table 1 Characteristics of the Study Subjects. Data are Presented as Mean ± SD or Number (Percentage) |
The individual response sequences to prophylactic norepinephrine for preventing post-induction hypotension in both groups are shown in Figure 2. The ED50 of norepinephrine, determined by the up-down sequential method, was 0.049 μg/kg/min (95% CI 0.043–0.052 μg/kg/min) in the Group C and 0.037 μg/kg/min (95% CI 0.031–0.040 μg/kg/min) in the Group G, representing an approximate 24% reduction with granisetron pretreatment, which exceeded the predefined minimal clinically important difference (MCID) of 20% (P < 0.05). This finding was corroborated by probit regression analysis, which yielded similar ED50 estimates of 0.052 μg/kg/min (95% CI 0.045–0.064 μg/kg/min) for Group C and 0.040μg/kg/min (95% CI 0.033–0.051 μg/kg/min) for Group G (P < 0.05) (Figure 3).
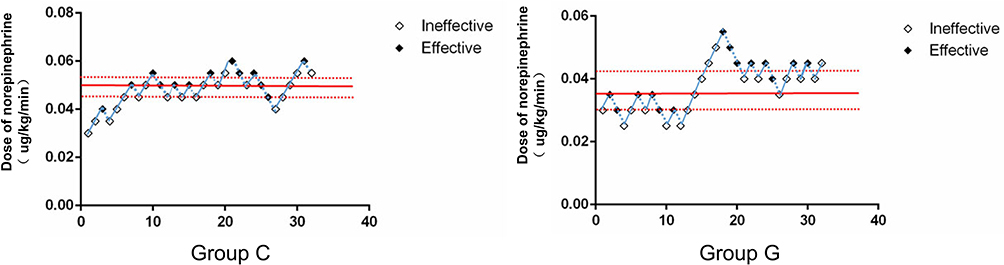 |
Figure 2 Individual responses to prophylactic norepinephrine at corresponding infusion rates (μg/kg/min) in the control group (Group C and granisetron group (Group G). The ED50 of norepinephrine calculated by up-down sequential analysis was 0.049 μg/kg/min (95% CI, 0.043–0.052 μg/kg/min) in Group C and 0.037 μg/kg/min (95% CI, 0.031–0.040 μg/kg/min) in Group G. Solid horizontal lines represent the ED50 values, and dashed lines represent the 95% confidence intervals. CI indicates confidence interval; ED50, effective dose in 50% of subjects. |
 |
Figure 3 Dose-response curves and 95% confidence intervals for the ED50 of norepinephrine in the two groups, derived from probit regression analysis. The ED50 of norepinephrine was 0.052 μg/kg/min (95% CI, 0.045–0.064 μg/kg/min) in the control group (Group C and 0.040 μg/kg/min (95% CI, 0.033–0.051 μg/kg/min) in the granisetron group (Group G). CI indicates confidence interval; ED50, effective dose in 50% of subjects. |
No statistically significant differences were observed between the groups in the incidence of adverse events, including hypotension, hypertension, bradycardia, or postoperative nausea and vomiting (PONV) within 24 hours after surgery (Table 2).
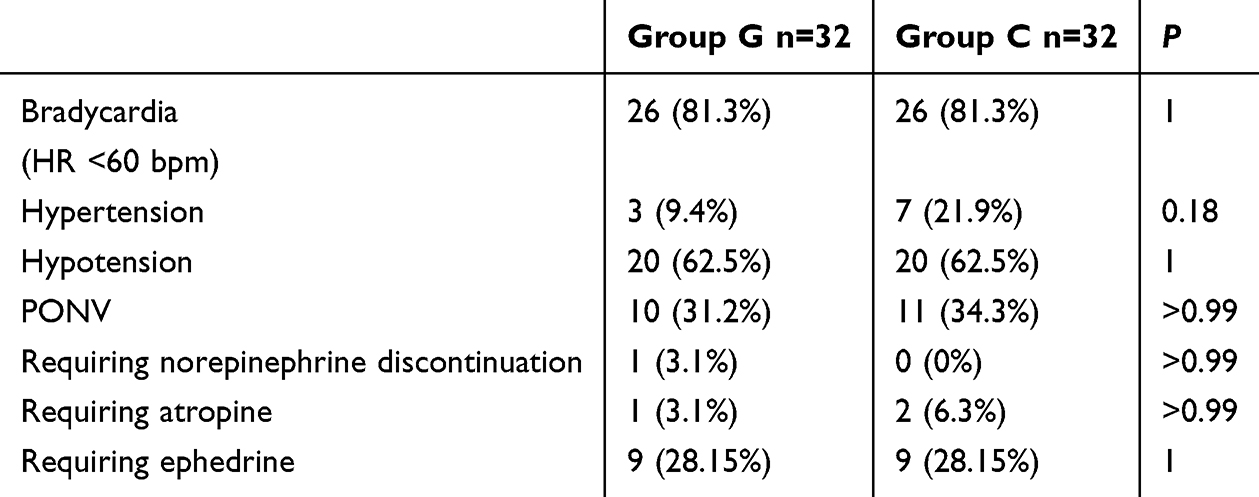 |
Table 2 Adverse Reactions. Data are Presented as Number (%) |
Discussion
This randomized placebo-controlled study is the first to investigate the effect of intravenous granisetron on the ED50 of norepinephrine for preventing post-induction hypotension in elderly patients undergoing laparoscopic gastrointestinal surgery. Our results demonstrate that prophylactic granisetron administration significantly reduces the norepinephrine requirement, with the ED50 decreasing from 0.049 μg/kg/min in the control group to 0.037 μg/kg/min in the granisetron group—a reduction of approximately 24%. This finding was consistently confirmed by both up-down sequential analysis and probit regression, supporting the robustness of our observations. Notably, this reduction in the vasopressor requirement was achieved without compromising the established prophylactic efficacy of granisetron against PONV.
Induction of general anesthesia frequently causes significant hemodynamic instability, particularly in elderly patients.18 The underlying mechanisms are multifactorial, including reduced systemic vascular resistance,19 decreased myocardial contractility,20 and impaired baroreflex function21 induced by anesthetic agents. Although no universally accepted definition of intraoperative hypotension exists,22 a common criterion is a >30% decrease in mean arterial pressure from baseline, which has been associated with increased risk of perioperative complications in elderly populations.23 In the present study, we defined hypotension as a >20% reduction in mean arterial pressure from baseline values, a threshold consistent with previous investigations in this field.24
Numerous studies have evaluated the effects of 5‑HT3 receptor antagonists on spinal anesthesia-induced hypotension, though results have been inconsistent.25–27 A meta-analysis of 17 randomized controlled trials demonstrated that prophylactic 5‑HT3 antagonists effectively reduce the incidence of hypotension and bradycardia in obstetric populations;28 however, this analysis did not quantitatively assess vasopressor dose requirements. Although granisetron and ondansetron share similar mechanisms as 5‑HT3 receptor antagonists, granisetron exhibits higher selectivity and minimal affinity for histaminergic or dopaminergic receptors.29 Moreover, previous work suggested that granisetron attenuates the decline in mean arterial pressure more effectively than ondansetron, a clinically relevant distinction.27 These observations provided the rationale for our investigation into granisetron’s hemodynamic effects on the ED50 of norepinephrine for preventing post-induction hypotension in elderly patients undergoing laparoscopic gastrointestinal surgery.
The observed 24% reduction in norepinephrine ED50 provides proof of concept that pre-induction granisetron exerts a pharmacodynamic sparing effect on vasopressor requirements. The most plausible mechanism underlying our findings involves blockade of the Bezold–Jarisch reflex, a cardioinhibitory reflex mediated by serotonin receptors on cardiac vagal afferents.30 Activation of this reflex during anesthesia induction—triggered by reduced venous return, decreased ventricular volume, and increased myocardial contractility—can precipitate bradycardia and hypotension. By antagonizing 5‑HT3 receptors in cardiac sensory nerve endings, granisetron may attenuate this reflex, thereby enhancing hemodynamic stability and reducing exogenous vasopressor requirements. Although no studies have definitively established the occurrence of the Bezold–Jarisch reflex in elderly patients, evidence suggests a bimodal age distribution: younger patients are more prone to bradycardia, whereas elderly patients predominantly exhibit hypotension.31 The high incidence of both hypotension and bradycardia following anesthesia induction in elderly populations supports the potential relevance of this reflex and the therapeutic role of 5‑HT3 antagonists. It is noteworthy that the 62.5% hypotension incidence observed in both groups does not imply a lack of effect of the intervention, but is instead inherent to the up and down sequential design. Moreover, It is possible that the lower norepinephrine dose could translate into fewer dose-dependent adverse events (eg, arrhythmias, tissue hypoperfusion) in a larger, adequately powered trial focusing on clinical outcomes rather than ED50. For now, our results should be interpreted as a hypothesis-generating pharmacodynamic interaction, not as evidence of improved patient outcomes. Future studies should be designed with sample sizes sufficient to detect differences in clinically meaningful endpoints, such as postoperative myocardial injury, acute kidney injury, or length of hospital stay, while also evaluating the cost‑effectiveness of adding granisetron to standard anesthetic protocols.
The PONV rates (31.2% vs 34.3%) are in the expected range for elderly patients undergoing laparoscopic gastrointestinal surgery under general anesthesia, even with prophylactic antiemetics. The comparable incidence of PONV between groups confirms that our study design—administering granisetron to control patients at the end of surgery—provided equitable antiemetic prophylaxis without confounding the primary hemodynamic outcome. This approach maintained ethical standards for PONV prevention in this high-risk population while isolating the pre-induction effect of granisetron. However, these PONV findings are exploratory in nature, as the study was not powered for secondary endpoints; further investigations with adequate sample sizes are warranted to definitively assess the impact of pre-induction granisetron on postoperative nausea and vomiting.
The relatively high bradycardia rate in our study (81.3% in both groups) can be explained by two factors. First, both groups received a fixed low‑dose dexmedetomidine infusion (0.4 μg/kg/h), which is known to cause bradycardia via central α2‑adrenoceptor activation. The incidence did not differ between groups, indicating a protocol‑related phenomenon rather than a specific effect of granisetron.
Second, the bradycardia definition we used — heart rate < 60 bpm — is a standard but relatively sensitive threshold. Many elderly patients have baseline heart rates in the 60–70 bpm range, and even a small decrease during anesthesia can cross this cutoff, leading to a “bradycardia” event label. Importantly, all episodes in our study were asymptomatic and either self‑limited or responded to a single low‑dose atropine. None required discontinuation of dexmedetomidine or were associated with hypotension. If a more clinically selective threshold (eg, heart rate < 50 bpm) had been applied, the reported bradycardia rate would have been much lower, aligning with typical clinical expectations.
Several limitations should be acknowledged. First, this was a single-center study with a relatively modest sample size, which may limit generalizability. However, the sequential design methodology is well-established for ED50 estimation and provides efficient and reliable dose-finding with smaller cohorts.16 Second, our study population was restricted to patients aged 60–74 years with ASA physical status II and normal BMI; whether these findings extend to other age groups, higher-risk patients, or those with obesity requires further investigation. Third, the general anesthesia protocol included multiple agents (eg, propofol, opioids, and dexmedetomidine), each with significant hemodynamic effects. Consequently, the estimated ED50 of norepinephrine for preventing post‑induction hypotension may be subject to potential interference from these concomitant medications, and the isolated effect of granisetron on vasopressor requirement should be interpreted within this context. Fourth, we focused on the immediate post-induction period (30 minutes); the duration of granisetron’s vasopressor-sparing effect beyond this window remains unknown. Fifth, while we hypothesize involvement of the Bezold–Jarisch reflex, we did not directly measure cardiac vagal activity or serotonin concentrations; mechanistic studies are needed to confirm the underlying pathways. Finally, the ED50 represents a pharmacodynamic endpoint; whether the observed reduction in norepinephrine requirement translates into improved clinical outcomes—such as reduced postoperative complications, shorter hospital stay, or enhanced recovery—merits further investigation in larger trials.
Conclusion
Pre‑induction granisetron offers a significant norepinephrine‑sparing effect compared with end‑of‑surgery administration, representing a potentially favorable timing strategy. Future studies should explore the underlying mechanisms, investigate dose-response relationships, and determine whether this vasopressor-sparing effect translates into improved perioperative outcomes.
Data Sharing Statement
Individual participant data underlying the results reported in this article will be available from the corresponding author Youfa Zhou upon reasonable request, beginning 6 months after publication. The study protocol, statistical analysis plan, and clinical study report will also be made available.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the the National Natural Science Foundation of China (grant number: 82401396), and the Zhejiang Provincial Natural Science Foundation of China (grant number: LQ23H090015).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ida M, Kimoto K, Iwata M, et al. Retrospective evaluation of predictors and frequency of hypotension in hypertensive patients after induction of general anesthesia. Masui. 2014;63(6):614–9.
2. Smyth EC, Nilsson M, Grabsch HI, van Grieken NCT, Lordick F. Gastric cancer. Lancet. 2020;396(10251):635–648. doi:10.1016/s0140-6736(20)31288-5
3. Arnold M, Abnet CC, Neale RE, et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology. 2020;159(1):335–349.e15. doi:10.1053/j.gastro.2020.02.068
4. Wang W-K, Tu C-Y, Shao C-X, et al. Impact of enhanced recovery after surgery on postoperative rehabilitation, inflammation, and immunity in gastric carcinoma patients: a randomized clinical trial. Braz J Med Biol Res. 2019;52(5). doi:10.1590/1414-431x20198265
5. Hassani V, Movaseghi G, Safaeeyan R, Masghati S, Ghorbani Yekta B, Farahmand Rad R. Comparison of ephedrine vs. norepinephrine in treating anesthesia-induced hypotension in hypertensive patients: randomized double-blinded study. Anesthesiol Pain Med. 2018;8(4). doi:10.5812/aapm.79626
6. Jor O, Maca J, Koutna J, et al. Hypotension after induction of general anesthesia: occurrence, risk factors, and therapy. A prospective multicentre observational study. J Anesth. 2018;32(5):673–680. doi:10.1007/s00540-018-2532-6
7. Bijker JB, Persoon S, Peelen LM. Intraoperative hypotension and perioperative ischemic stroke after general surgerya nested case-control study. Anesthesiology. 2012. doi:10.1097/ALN.0b013e3182472320
8. Demirkaya M, Kelsaka E, Sarihasan B, Bek Y, Üstün E. The optimal dose of remifentanil for acceptable intubating conditions during propofol induction without neuromuscular blockade. J Clin Anesth. 2012;24(5):392–397. doi:10.1016/j.jclinane.2011.11.006
9. Liang T, Yu J, Li L, Xie Y, Wu F, Loardi C. Prophylactic norepinephrine infusion reduces postoperative complications and hospitalization time in elderly patients undergoing posterior lumbar spinal fusion. BioMed Res Int. 2021;2021:1–8. doi:10.1155/2021/2161036
10. Farhan M, Hoda M, Ullah H. Prevention of hypotension associated with the induction dose of propofol: a randomized controlled trial comparing equipotent doses of phenylephrine and ephedrine. J Anaesthesiol Clin Pharmacol. 2015;31(4):526. doi:10.4103/0970-9185.169083
11. Owczuk R, Wenski W, Polakkrzeminska A, et al. Ondansetron given intravenously attenuates arterial blood pressure drop due to spinal anesthesia: a double-blind, placebo-controlled study. Reg Anesth Pain Med. 2008;33(4):332–339. doi:10.1016/j.rapm.2008.01.010
12. Wang M, Zhuo L, Wang Q, et al. Efficacy of prophylactic intravenous ondansetron on the prevention of hypotension during cesarean delivery: a dose-dependent study. Int J Clin Exp Med. 2014;17:5210.
13. Xiao F, Wei C, Chang X, et al. A prospective, randomized, double-blinded study of the effect of intravenous ondansetron on the effective dose in 50% of subjects of prophylactic phenylephrine infusions for preventing spinal anesthesia–induced hypotension during cesarean delivery. Anesth Analg. 2020;131(2):564–569. doi:10.1213/ane.0000000000004534
14. El Khouly NI, Meligy AM. Randomized controlled trial comparing ondansetron and placebo for the reduction of spinal anesthesia-induced hypotension during elective cesarean delivery in Egypt. Int J Gynecol Obstetr. 2016;135(2):205–209. doi:10.1016/j.ijgo.2016.06.012
15. Golparvar M, Golparvar M, Saadati M, Farsaei S. Effect of ondansetron on prevention of post-induction hypotension in elderly patients undergoing general anesthesia: a randomized, double-blind placebo-controlled clinical trial. Saudi J Anaesth. 2015;9(4):365–369. doi:10.4103/1658-354x.159455
16. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
17. Choi SC. Interval estimation of the LD50 based on an up-and-down experiment. Biometrics. 1990;46(2):485–492. doi:10.2307/2531453
18. Li B, Pop C, Johnson M, Sklar MC, Lawler PR, Elliott AM. Hemodynamic Effects of Propofol. JACC Adv. 2025;4(8):101769. doi:10.1016/j.jacadv.2025.101769
19. Claeys MA, Gepts E, Camu F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth. 1988;60(1):3–9. doi:10.1093/bja/60.1.3
20. Pagel PS, Warltier DC. Negative inotropic effects of propofol as evaluated by the regional preload recruitable stroke work relationship in chronically instrumented dogs. Anesthesiology. 1993;78(1):100–108. doi:10.1097/00000542-199301000-00015
21. Sellgren J, Ejnell H, Elam M, Ponten J, Wallin BG. Sympathetic muscle nerve activity, peripheral blood flows, and baroreceptor reflexes in humans during propofol anesthesia and surgery. Anesthesiology. 1994;80(3):534–544. doi:10.1097/00000542-199403000-00009
22. Sudfeld S, Brechnitz S, Wagner JY, et al. Post-induction hypotension and early intraoperative hypotension associated with general anaesthesia. Br J Anaesth. 2017;119(1):57–64. doi:10.1093/bja/aex127
23. Wesselink EM, Kappen TH, Torn HM, Slooter AJC, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018;121(4):706–721. doi:10.1016/j.bja.2018.04.036
24. Zhou Y, Wang C, Lin B, et al. The effect of intravenous granisetron on prophylactic ephedrine for preventing hypotension after general anaesthesia induction in elderly patients: a randomized controlled trial. Sci Rep. 2023;13(1):11590. doi:10.1038/s41598-023-38303-6
25. Mowafi HA, Arab SA, Ismail SA, Al-Ghamdi A. The effects of intravenous granisetron on the sensory and motor blockade produced by intrathecal bupivacaine. Anesth Analg. 2008;106(4):1322–5,tableofcontents. doi:10.1213/ane.0b013e318165e012
26. Ortiz-Gomez JR, Palacio-Abizanda FJ, Morillas-Ramirez F, Fornet-Ruiz I, Lorenzo-Jimenez A, Bermejo-Albares ML. The effect of intravenous ondansetron on maternal haemodynamics during elective caesarean delivery under spinal anaesthesia: a double-blind, randomised, placebo-controlled trial. Int J Obstet Anesth. 2014;23(2):138–143. doi:10.1016/j.ijoa.2014.01.005
27. Aksoy M, Dostbil A, Aksoy AN, Ince I, Bedir Z, Ozmen O. Granisetron or ondansentron to prevent hypotension after spinal anesthesia for elective cesarean delivery: a randomized placebo-controlled trial. J Clin Anesth. 2021;75:110469. doi:10.1016/j.jclinane.2021.110469
28. Heesen M, Klimek M, Hoeks SE, Rossaint R. Prevention of spinal anesthesia-induced hypotension during cesarean delivery by 5-hydroxytryptamine-3 receptor antagonists: a systematic review and meta-analysis and meta-regression. Anesth Analg. 2016;123(4):977–988. doi:10.1213/ANE.0000000000001511
29. Aapro M. Granisetron: an update on its clinical use in the management of nausea and vomiting. Oncologist. 2004;9(6):673–686. doi:10.1634/theoncologist.9-6-673
30. Campagna JA, Carter C, Carter C. Clinical relevance of the Bezold-Jarisch reflex. Anesthesiology. 2003;98(5):1250–1260. doi:10.1097/00000542-200305000-00030
31. Tan MP, Parry SW. Vasovagal syncope in the older patient. J Am Coll Cardiol. 2008;51(6):599–606. doi:10.1016/j.jacc.2007.11.025
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Dose–Response Study on the Infusion of Norepinephrine Combined with Crystalloid Coload versus Colloid Coload for Preventing Hypotension During Spinal Anesthesia for Cesarean Delivery
Jin WD, Mao JQ, Liu J, Liang G, Jiang C, Sheng ZM
Drug Design, Development and Therapy 2022, 16:2617-2626
Published Date: 6 August 2022
Norepinephrine or Phenylephrine to Prevent Spinal Anesthesia-Induced Hypotension During Cesarean Section: A Double-Blinded, Randomized, Controlled Study of Fetal Cerebral Perfusion
Liu J, Sheng Z, Guo F, Lin X, Xu L, Sun L, Qian X
Drug Design, Development and Therapy 2025, 19:7571-7580
Published Date: 2 September 2025