")
Back to Journals » Open Access Surgery » Volume 16
Gossypiboma – A Rare Cause of Palpable Intra-Abdominal Mass: A Case Report
Authors Taeme Gebretsion M , Alemu TS, Mergiyaw YA
Received 9 February 2023
Accepted for publication 9 May 2023
Published 12 May 2023 Volume 2023:16 Pages 25—31
DOI https://doi.org/10.2147/OAS.S407868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Mulugeta Taeme Gebretsion,1 Tilahun Sisay Alemu,2 Yimam Ali Mergiyaw1
1Department of Surgery, School of Medicine, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia; 2Surgery Department, Kemisse General Hospital, Kemisse, Ethiopia
Correspondence: Mulugeta Taeme Gebretsion, Department of Surgery, School of Medicine, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia, Tel +251904690867, Email [email protected]
Introduction: Gossypiboma is the accidental retention of surgical gauze with inflammatory reaction in the body cavity after surgical procedures. It is an uncommon but preventable surgical mistake. This serious medical condition could have a substantial impact on morbidity and mortality as well as medico-legal issues.
Case Report: We present here a case of a 30-year-old female referred to our surgical outpatient department with progressive lower abdominal swelling, pain, and low-grade fever of 4 months’ duration after she had undergone cesarean section 6 months back at the primary hospital. On physical examination, she was tachycardic and had a 15× 15 cm firm, mobile, non-tender, infra-umbilical abdominal mass. Abdominal ultrasound suggested possible gossypiboma, which was confirmed after exploratory laparotomy.
Discussion: Any type of surgery can be a reason for retained surgical gauze, but its incidence can be significantly reduced if surgical checklists are used seriously and routinely in every patient. A strong index of suspicion continues to be crucial in the diagnosis of surgical gauze retention, particularly when a patient has experienced an unexplained bad course following surgery.
Conclusion: : In patients who present with palpable abdominal mass and a history of previous abdominal surgical operations, the diagnosis of gossypiboma should be included in the differential diagnosis. Prevention of retained surgical items is the collective responsibility of the surgical team, the nursing team, and operation theatre technicians. Furthermore, strict measures should be implemented to avoid it.
Keywords: case report, gossypiboma, retained foreign body, abdominal sponge, abdominal mass
Introduction
Gossypiboma, textiloma, or retained foreign object is a post-surgery complication due to foreign materials, such as a surgical gauze, inadvertently left inside a patient’s body. The term gossypiboma comes from the Latin “gossypium”, which means cotton, and the Swahili word “boma”, which means a place to hide.1 Although it is a rare surgical complication, it can have serious morbidity and death consequences.
The majority of gossypiboma cases are found within a few days of surgery. However, they can go unnoticed for years.2,3 Late-presenting gossypibomas can cause considerable diagnostic confusion, so they should be considered as a differential diagnosis in patients with intra-abdominal masses who have had surgery in the past. Since clinical diagnosis is difficult to make, imaging techniques including conventional radiography, ultrasonography, computed tomography, and magnetic resonance imaging (MRI) may be used to make an accurate diagnosis.3
Medico-legal implications may cause many instances to be shelved, especially in underdeveloped nations, making it impossible to determine the incidence. Report from literature showed that an estimated 1:1000 to 1:1500 intra-abdominal surgeries result in a retained foreign body.4
Case Report
Case Presentation
The patient was a 30-year-old female who presented to our surgical outpatient department with progressive lower abdominal swelling of 4 months' duration after she was referred from another hospital. Associated with this she had intermittent dull aching lower abdominal pain, unquantified weight loss, and low-grade intermittent fever. She had undergone cesarean section 6 months back for intrauterine fetal death (IUFD) with hydrocephalus at the primary hospital. She was diagnosed to have sepsis of wound focus with surgical site infection and superficial wound dehiscence on the 7th post-operative day which was treated with broad-spectrum intravenous antibiotics and wound care. She stayed in the hospital for 11 days; the wound closed, and the patient was discharged with improvement. Otherwise, the patient had no concomitant morbidity, no other surgical or medical history, and no relevant family history.
Clinical Findings
On physical examination, she was tachycardic, but other vital signs were within the normal range. There was a 15×15 cm firm, mobile, non-tender, infra-umbilical abdominal mass with more on to the left side (Figures 1 and 2). There was also a transverse scar in the suprapubic area.
 |
Figure 1 Lower abdominal mass (lateral view). |
 |
Figure 2 Lower abdominal mass with suprapubic transverse scar (AP view). |
Diagnostic Assessment
White blood cell count was 10,500 with a 78% neutrophil percentage. Abdominopelvic ultrasound showed a 7×7.7cm large and ill-defined homogeneously shadowing left lower abdominal mass lesion with increased adjacent mesenteric fat reflectivity (Figure 3) with an impression of gossypiboma. With a possible working diagnosis of gossypiboma, she was admitted to the surgical ward for elective exploratory laparotomy.
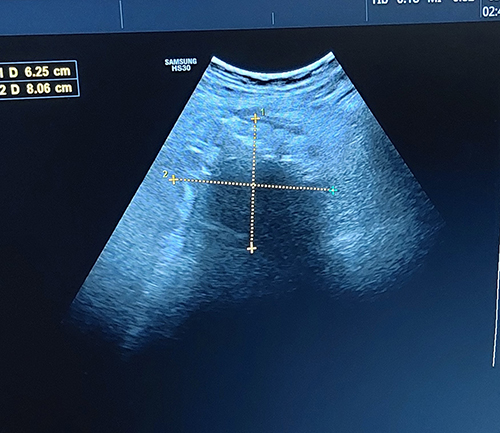 |
Figure 3 Abdominal ultrasound showed a 7×7.7cm large and ill-defined homogeneously shadowing left lower abdominal mass lesion with increased adjacent mesenteric fat reflectivity. |
Therapeutic Intervention
After informed consent was taken, exploratory laparotomy under general anesthesia was performed by a general surgeon with assistance of 3rd-year surgery resident. After prophylactic antibiotics were given, a midline incision was done. Intra-operatively, a boggy intraperitoneal mass was found, around 15×15 cm, formed by the omentum, mid-ileum, and descending and sigmoid colons (Figure 4). There was one big piece of gauze with 200 mL of thick offensive pus in a well-formed cavity formed by the above structures, and the gauze had eroded the antimesenteric side of the involved ileum 100 cm proximal to the ileo-cecal valve with a 0.5×0.5 cm size perforation (Figures 5 and 6). To safely remove the mass, meticulous adhesiolysis and full cavity dissection with blunt and sharp dissection were performed. Upon opening, the mass showed retained surgical gauze with thick pus (Figure 7). After ileal perforation was refreshed and repaired, peritoneum was washed with warm saline thoroughly. She had an uneventful postoperative period.
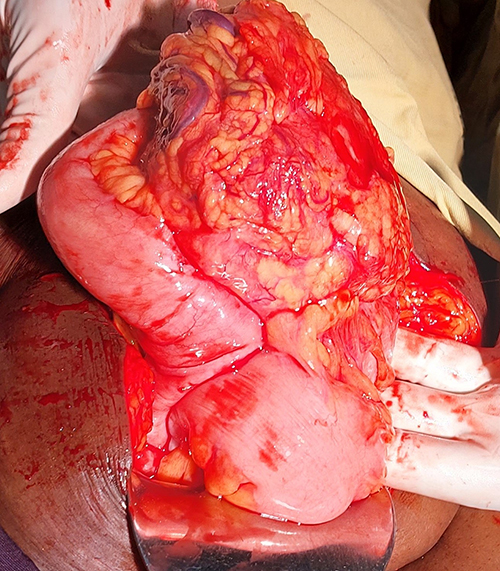 |
Figure 4 A mass formed by the omentum, mid-ileum, and descending and sigmoid colons. |
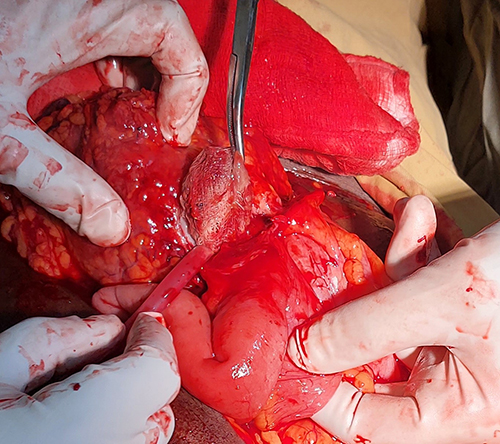 |
Figure 5 One big piece of gauze with 200 mL of thick offensive pus in a well-formed cavity; the gauze had eroded the antimesenteric side of the involved ileum 100 cm proximal to the ileo-cecal valve with 0.5×0.5 cm size perforation. |
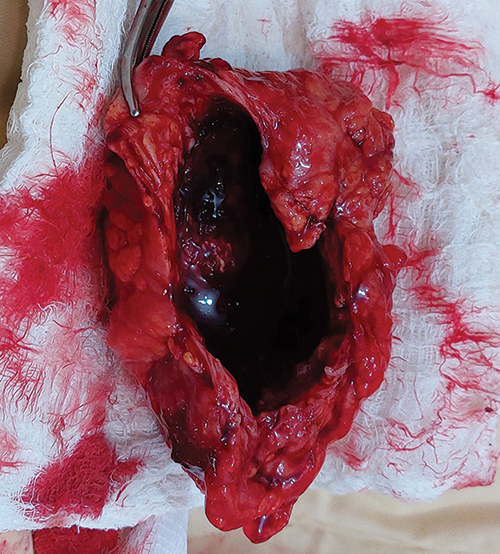 |
Figure 6 Resected surgical specimen with large cavity after surgical gauze removed. |
 |
Figure 7 Removed surgical specimen containing surgical gauze soaked with pus. |
Follow-Up and Outcomes
The patient tolerated the solid diet on the 3rd postoperative day. She was discharged on the 6th postoperative day with no complications. She had follow-up visits in 2nd week and 6th week at the outpatient department which were uneventful.
Discussion
Any type of surgery can be a reason for retained surgical gauze but typically after hysterectomy, appendectomy, and cholecystectomy.5 Risk factors associated with sponge retention are emergency surgery, unexpected change in the surgical procedure, poor organization of operating team, hurried sponge counts, prolonged operations, unstable intra-operative patient condition, inexperienced staff, inadequate staff numbers, and obesity.6 With a lack of reporting due to the medico-legal repercussions, it is difficult to estimate the exact incidence of retained surgical sponge at operation. But one out of 1000–1500 intra-abdominal procedures and one out of 300–1000 total operations are thought to have gossypibomas.4 Since Wilson first described gossypiboma in 1884, numerous reports have been written and published in the literature. But when more current data appear in the literature, it appears that this issue still has to be resolved after intra-abdominal procedures.7,8
The inflammatory response to retained sponge results in a number of impacts to the patients and the operating facility and staff. For instance, imaging tests to diagnose the problem, a further hospital stay for a second operation, legal costs, and patient reimbursement for alleged malpractice on the part of the facility and staff are all included. Clinically some cases may remain asymptomatic for many years after surgery. However, the main clinical presentations are abdominal pain (42%), palpable abdominal mass (27%), and fever (12%). Complications including fistula formation, intestinal obstruction, or bowel perforation are less common presentations.9 Possible differential diagnosis that can be confused with gossypiboma are abscess, tumor, or a hydrated or mesenteric cyst. In order to make correct diagnosis, imaging modalities including ultrasonography (USG) and computed tomography (CT) may help in the diagnosis.10 On ultrasound, it appears as a complex hypoechoic or cystic mass with wavy internal hyperechoic material, with major posterior shadowing like in the present case. Contrast-enhanced CT (CECT) is the diagnostic of choice for gossypiboma, revealing a well circumscribed capsulated mass with presence of air within and enhancement of the wall.8
The incidence of gossypiboma can be significantly reduced if surgical checklists are used routinely in every procedure. A quick but thorough routine post-procedure wound and body cavity exploration before closure should be done by the surgical team.3,11
In this case we do not know if surgical checklist is done regularly in the hospital where the patient had the cesarean section. The primary cause of our patient’s protracted morbidity was delayed presentation. So, a strong index of suspicion continues to be crucial in the diagnosis of surgical gauze retention, particularly when a patient has experienced an unexplained bad course following surgery. In addition to this, the diagnosis of gossypiboma should be considered in individuals who present with a palpable abdominal mass and a history of prior abdominal surgical procedures.
Conclusion
Gossypiboma is an uncommon post-surgical complication that is typically asymptomatic and with vague radiological findings. However, in patients who present with palpable abdominal mass and a history of previous abdominal surgical operations, the diagnosis of gossypiboma must be suspected. The best diagnostic modality to rule out retained foreign body should be a CT scan with contrast. In addition to this, a gossypiboma can cause bowel perforation and adhesion to the surrounding structures. Regarding management, surgery is the only treatment for gossypiboma. Prevention of retained surgical items is the collective responsibility of the surgical team, the nursing team, and operation theatre technicians. Furthermore, strict measures should be implemented to avoid it.
Ethical Approval
The ethical approval was exempted as case reports do not require it.
Consent
Informed written consent was obtained from the patient for publication of this case report and accompanying images.
Funding
All authors have declared that no financial support or funding was received from any organization and have no financial relationships at present or within the past three years with any organizations that might have an interest in the submitted work.
Disclosure
Authors do not have any conflicts of interest.
References
1. Srivastava KN, Agarwal A. Case report gossypiboma posing as a diagnostic dilemma: a case report and review of the literature. Case Rep Surg. 2014;2014:3–6.
2. Colak T, Olmez T, Turkmenoglu O, Dag A. Small bowel perforation due to gossypiboma caused acute abdomen. Case Rep Surg. 2013;2013:1–3. doi:10.1155/2013/219354
3. Malhotra MK. Migratory surgical gossypiboma-cause of iatrogenic perforation: case report with review of literature.. Niger J Surg. 2012;18(1):27–29. doi:10.4103/1117-6806.95486
4. Dakubo J, Hodasi WM, Obaka HE, Toboh H, Asempa W. An intra-abdominal gossypiboma. Ghana Med J. 2009;43(1):43–45.
5. Asuquo ME, Ogbu N, Udosen J, et al. Case report acute abdomen from gossypiboma: a case series and review of literature. Niger J Surg Res. 2006;8(3):174–176.
6. Uranüs S, Schauer C, Pfeifer J, Dagcioglu A. Laparoscopic removal of a large laparotomy pad forgotten in situ.. Surg Laparosc Endosc. 1995;5(1):77–79.
7. Murad M, Bari V. Gossypiboma - A case report. Pakistan J Med Sci. 2003;19(2):138–140. doi:10.31729/jnma.646
8. Bairwa BL. Gossypiboma-an unusual cause of surgical abdomen and surgeon’s nightmare: a rare case report. Int J Surg Case Rep. 2021;80:105521. doi:10.1016/j.ijscr.2021.01.015
9. Macario A, Morris D, Morris S. Initial clinical evaluation of a handheld device for detecting retained surgical gauze sponges using radiofrequency identification technology. Archiv Surg. 2006;141:659–662.
10. El Zemity H, Hakami N, Alfaki MAA, et al. Intra-abdominal gossypiboma: a rare cause of palpable abdominal mass with a review of literature. Cureus. 2020;12(10):2–6. doi: 10.7759/cureus.10930
11. Mahajan RP. Best practice & research clinical anaesthesiology the WHO surgical checklist. Best Pract Res Clin Anaesthesiol. 2011;25:161–168. doi:10.1016/j.bpa.2011.02.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.