Back to Journals » Clinical Ophthalmology » Volume 20
Glucagon-Like Peptide-1 Analogs Associated with a Reduced Risk of Legal Blindness in Type 2 Diabetics with Cardiovascular Risks
Authors Jarrett E, Muayad J ![]() , Ryu BU, Lee AG, Gupta PK
, Ryu BU, Lee AG, Gupta PK ![]()
Received 1 December 2025
Accepted for publication 28 January 2026
Published 3 February 2026 Volume 2026:20 581826
DOI https://doi.org/10.2147/OPTH.S581826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Ethan Jarrett,1 Jawad Muayad,2 Byoung U Ryu,3 Andrew G Lee,1– 8 Praveena K Gupta3
1John Sealy School of Medicine, University of Texas Medical Branch, Galveston, TX, USA; 2School of Medicine, Texas A&M University, Houston, TX, USA; 3Department of Ophthalmology and Vision Sciences, University of Texas Medical Branch, Galveston, TX, USA; 4Department of Ophthalmology, Blanton Eye Institute, Houston Methodist Hospital, Houston, TX, USA; 5Department of Ophthalmology, Cullen Eye Institute, Baylor College of Medicine, Houston, TX, USA; 6Departments of Ophthalmology, Neurology, and Neurosurgery, Weill Cornell Medicine, New York, NY, USA; 7Department of Ophthalmology, University of Texas MD Anderson Cancer Center, Houston, TX, USA; 8Department of Ophthalmology, the University of Iowa Hospitals and Clinics, Iowa City, IA, USA
Correspondence: Praveena K Gupta, University Eye Center, Department of Ophthalmology and Vision Sciences at the University of Texas Medical Branch, 700 University Blvd, Galveston, TX, 77550, USA, Tel +1 617 4160825, Email [email protected]
Purpose: To evaluate whether glucagon-like peptide-1 receptor agonist (GLP-1 RA) therapy influences the risk of legal blindness and ischemic optic neuropathy (ION) among patients with type 2 diabetes mellitus (T2DM) and cardiovascular risk factors (CVRF).
Design: A retrospective cohort study using de-identified electronic medical record (EMR) data from TriNetX, encompassing 72 healthcare organizations across the United States between January 2018 and January 2025.
Participants: Adults (≥ 18 years) with T2DM (A1c < 10%) and at least one CVRF (hyperlipidemia, essential hypertension, overweight/obesity, or chronic ischemic heart disease) who were prescribed or not prescribed a GLP-1 RA.
Methods: Patients with type 1 diabetes, optic neuritis, giant cell arteritis, or phosphodiesterase-5 inhibitor use were excluded. GLP-1 RA users were required to have ≥ 2 prescription records. A 1:1 propensity score matching (PSM) was performed to balance demographics, comorbidities, laboratory values, and concurrent antidiabetic medications. Outcomes were assessed at 1-, 3-, and 5-year follow-ups. Hazard ratios (HR) with 95% confidence intervals (CI) were calculated using univariable survival analyses.
Main Outcome Measures: Incidence of legal blindness and ischemic optic neuropathy.
Results: After PSM, each cohort included 350,536 patients (mean age 58.7 ± 12.6 years; 61.6% female). GLP-1 RA use was associated with a significantly reduced risk of legal blindness at 1 year (HR 0.589, 95% CI 0.476– 0.728), 3 years (HR 0.677, 95% CI 0.583– 0.788), and 5 years (HR 0.669, 95% CI 0.583– 0.768). There was no significant difference in ION incidence between cohorts at 1 year (HR 0.872, 95% CI 0.627– 1.212), 3 years (HR 1.002, 95% CI 0.792– 1.268), or 5 years (HR 0.978, 95% CI 0.789– 1.211).
Conclusion: GLP-1 receptor agonist therapy was associated with a significantly lower risk of legal blindness and no difference in ION incidence. These findings indicate potential ocular benefits of GLP-1 RAs beyond glycemic and cardiovascular outcomes.
Plain Language Summary: People living with type 2 diabetes have a higher risk of serious vision problems, including legal blindness and a condition called ischemic optic neuropathy, which occurs when the optic nerve does not get enough blood flow. New medications known as GLP-1 receptor agonists, originally developed to help manage blood sugar, have also been shown to improve cardiovascular health. Because circulation plays an important role in eye health, we wanted to understand whether these medicines might also influence the risk of major vision loss.
We studied a large group of adults with type 2 diabetes and cardiovascular risk factors using medical records collected from clinics across the United States. We compared people who were taking GLP-1 medicines with those who were not. We followed both groups for up to five years to see how many developed legal blindness or ischemic optic neuropathy.
We found that people taking GLP-1 medicines had a lower chance of developing legal blindness compared with those who were not taking these medications. We did not find a difference between groups in the number of people who developed ischemic optic neuropathy.
These findings suggest that GLP-1 medicines may provide benefits for eye health in addition to their known effects on blood sugar and heart health. While our results are encouraging, future research—especially long-term studies that follow individuals over time—is needed to confirm whether GLP-1 medicines directly protect vision.
Keywords: visual impairment, neuro-ophthalmology, retrospective study, ischemic optic neuropathy
Introduction
Type 2 diabetes mellitus (T2DM) is a leading cause of vision loss and legal blindness worldwide. Among its most devastating complications are ischemic optic neuropathies (ION) which are often linked to microvascular disease.1 Patients with additional cardiovascular risk factors (CVRF), such as hypertension and dyslipidemia, are especially vulnerable to vision-threatening sequelae including ION.2
Glucagon-like peptide-1 receptor analogs (GLP-1 RAs) have gained significant traction in the management of T2DM due to favorable metabolic, cardiovascular, and renal outcomes.3 Beyond glycemic control, GLP-1 RAs have demonstrated significant cardioprotective effects, such as improving vascular endothelial function, reducing inflammation, and preventing atherosclerosis.4 These systemic effects suggest a potential benefit for ocular vascular health as well.
Recent studies5–8 have yielded conflicting results regarding the potential relationship between GLP-1 RAs and optic nerve pathologies, particularly non-arteritic anterior ischemic optic neuropathy (NAION). ION can be arteritic anterior ION (due to giant cell arteritis) or NAION. Some authors have raised concerns about a possible increased risk of NAION5,8 with GLP-1 RA use, while other studies demonstrated no statistical differences between cohorts.6,7 However, large-scale studies evaluating the combined effects of T2DM and CVRFs have not yet been conducted. To address this gap, our study investigates whether GLP-1 RA therapy influences the incidence of legal blindness and ION in a propensity-matched cohort of T2DM patients with underlying cardiovascular risk factors. Recent reviews have highlighted the complex evidence regarding the ocular effects of GLP-1RAs. While some studies suggest potential microvascular, neuroprotective, and anti-inflammatory benefits that may confer protection against severe visual outcomes, other reports have raised safety concerns regarding ischemic optic neuropathy and other optic nerve disorders.9–11 These conflicting findings underscore the importance of further research. We aimed to investigate whether GLP-1 RA use would be associated with a reduced risk of legal blindness and ischemic optic neuropathy due to GLP-1 RA’s vascular and potential neuroprotective effects.
Methods
This retrospective cohort study used data from TriNetX, a health research database with de-identified electronic medical records from 72 health care organizations throughout the United States of America. TriNetX is able to comply with the Health Insurance Portability and Accountability Act and receive a waiver from the Western Institutional Review Board (IRB) by only providing cumulative counts of de-identified patient data. Informed consent was neither obtained nor required for this retrospective study as patients consented to provide their healthcare information to the TriNetX database while meeting their healthcare provider. This study was conducted in accordance with the principles of the Declaration of Helsinki. All diagnoses on the TriNetX medical database are classified by the International Classification of Diseases (ICD), Tenth Revision, Clinical Modification (ICD-10-CM) code set, which is a modified version of the World Health Organization ICD, Tenth Revision, standard. As TriNetX is a global dataset we also utilized TriNetX Curated (TNX Curated) codes, which are similar terms combined to minimize redundancy of database coding, Anatomical Therapeutic Chemical (ATC), RxNorm, and ICD-9 coding systems. The data for this study were collected on September 16th, 2025. The study analyzed the database for electronic medical records from January 1, 2018, to January 1, 2025.
Study Sample
The Supplementary Table 1 provides the diagnostic codes for exclusion and inclusion criteria in our study. Inclusion criteria required patients aged 18 years or older with type 2 diabetes mellitus (T2DM), with A1c values less than 10%, and at least one cardiovascular risk factor (CVRF) including hyperlipidemia, essential hypertension, overweight or obesity, and/or chronic ischemic heart disease. All included patients were either prescribed or not prescribed a GLP-1 receptor analog between January 1, 2018, and January 1, 2025. To ensure adequate use of GLP-1 analog medications, patients in the GLP-1 cohort were required to have at least one further documentation of GLP-1 analog use following the index event. We observed outcomes at 1, 3, and 5 years of follow-up. Patients with diagnosis codes of “optic neuritis” or “giant cell arteritis” were considered exclusion criteria to reduce the likelihood of misclassification and to help isolate cases of ION, consistent with standards established in prior publications.5–8 However, due to limitations in the specificity of the ICD-10-CM code H47.01, which does not reliably distinguish NAION from other forms of ION, this study refers to outcomes using the broader term “ischemic optic neuropathy” (ION) when describing our outcomes. Moreover, patients with prior ION were excluded at cohort creation to minimize confounding. Patients were also required to not have type 1 diabetes mellitus or use of the phosphodiesterase-5 inhibitors sildenafil, tadalafil, avanafil, or vardenafil. Figure 1 illustrates the inclusion and exclusion criteria for the study cohort.
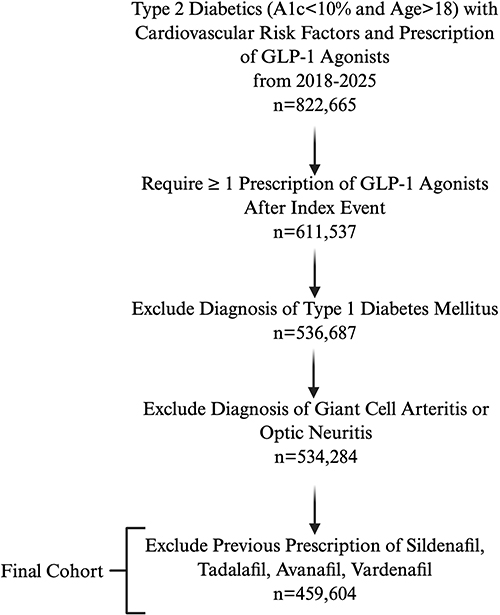 |
Figure 1 Inclusion and Exclusion Criteria for Study Cohort of Type 2 Diabetic Patients with Cardiovascular Risk Factors on GLP-1 Receptor Agonists. Flowchart that illustrates the process of inclusion and exclusion criteria for the study cohort of patients with type 2 diabetes and cardiovascular risk factors receiving GLP-1 receptor analog therapy. After requiring a secondary prescription of GLP-1 receptor analogs following the index event, the cohort consisted of 611,537 patients. Exclusion criteria were being less than or equal to 18 years old at time of index event, diagnosis of type 1 diabetes mellitus, diagnosis of giant cell arteritis or optic neuritis, and prescription of Sildenafil, Tadalafil, Avanafil, or Vardenafil. After exclusions, 459,604 patients remained. Created by Ethan Jarrett in BioRender (https://biorender.com/shortURL) is licensed under CC BY 4.0. |
Covariates
The TriNetX platform was utilized to conduct a 1:1 propensity score matching (PSM) for characteristics and comorbidities to ensure balance between cohorts. Matching was performed using a greedy nearest-neighbor matching algorithm with a caliper of 0.1 standard deviation, a technical standard widely accepted in published literature.12 The matched factors included demographics (age at index event, sex, race, and ethnicity), diagnoses (chronic kidney disease, obstructive sleep apnea, and nicotine dependence), medications (amiodarone, dipeptidyl peptidase 4 (DPP-4) inhibitors, insulin and insulin analogs, sulfonylureas, biguanides, sodium-glucose co-transporter 2 (SGLT2) inhibitors, and thiazolidinediones), and clinical laboratory values like body mass index and hemoglobin A1c levels. In TriNetX, propensity score matching is performed using observed baseline covariates, such that patients without documented laboratory values (eg, hemoglobin A1c or body mass index) are excluded from the matched cohorts in favor of individuals with available data.
Statistical Analyses
The index date of each patient was specified as the date the patient met all inclusion criteria. Age at index was defined by TriNetX as the age on the index date, and the ≥ 18-year filter was applied at cohort creation. The risk of ION (ICD-10-CM:H47.01) and legal blindness as defined by the USA (ICD-10-CM:H54.8) were the primary outcomes measured in this study. Patients with documentation of primary outcomes prior to index event were excluded from the study. Hazard ratios (HRs) with their respective 95% confidence intervals (CIs) were generated using TriNetX univariable analyses. Consistent with established methodology for large-scale database studies, we utilized univariable survival analysis following propensity score matching as the matching process effectively balanced baseline covariates to mimic a randomized environment.12 The threshold for statistical significance, using 2-sided tests, was set at p < 0.05. PSM results were analyzed using standardized mean differences (SMD), where a SMD < 0.1 between cohorts was considered effective matching. To address the concern regarding insufficient follow-up, our analysis utilized TriNetX’s built-in Cox Proportional Hazards and Kaplan-Meier logic. Specifically, patients were censored on the day after the last clinical fact recorded in their electronic health record if they had not yet experienced the outcome. This approach ensures that “late entrants” (eg, those entering in January 2025) contribute data only for the duration of their observed follow-up and are appropriately censored before reaching the 1-, 3-, or 5-year marks if their record does not extend that far.
Results
Baseline Demographics
Before matching, inclusion criteria were met by 459,604 patients in the GLP-1 RA group and 2,326,599 in the control group at the 5-year follow-up. After propensity score matching, both cohorts included 350,536 patients each. The mean age post-PSM was 58.7 ± 12.6 years for the GLP-1 RA group and 58.6 ± 13.6 years for the control group. The GLP-1 RA cohort consisted of 35.8% males and 61.6% females, while the control group included 34.8% males and 62.7% females. Racial distribution in the GLP-1 RA group was 62.9% White, 19.4% Black or African American, and 4.5% Asian, comparable to 63.3%, 19.8%, and 4.1% respectively in the control group. Regarding comorbidities, chronic kidney disease was present in 17.4% of both cohorts, and obstructive sleep apnea occurred in 26.6% of the GLP-1 RA group and 26.7% of the control group. For medication usage, 2.6% of both cohorts were prescribed amiodarone; 17.6% of the GLP-1 RA cohort and 14.5% of the control cohort were prescribed SGLT2 inhibitors; biguanide use was 69.2% and 69.9%; sulfonylurea use was 27.3% and 26.9%; thiazolidinedione use was 6.3% and 6.0%; DPP-4 inhibitor use was 16.4% and 15.7%; and insulin or insulin analog use was 45.4% and 45.0%, respectively. Mean hemoglobin A1c and body mass index values were well balanced between cohorts (SMD < 0.1). The remaining baseline characteristics and pre- and post-matching comparisons are presented in Figure 1.
The follow-up time for the 1-year mean follow-up for the GLP-1 RA cohort was 328 days with a standard deviation of 85 days, while the control was 330 days with a standard deviation of 90 days. The 3-year mean follow-up for the GLP-1 RA cohort was 708 days with a standard deviation of 355 days, while the control was 821 days with a standard deviation of 365 days. Lastly, the 5-year mean follow-up for the GLP-1 RA cohort was 845 days with a standard deviation of 542 days, while the control was 1132 days with a standard deviation of 645 days. These follow-up times represent the mean available observation windows due to staggered enrollment within the study period.
Risk of Legal Blindness and Ischemic Optic Neuropathy
The GLP-1 cohort had a statistically significant reduction in risk of legal blindness, at all measured time periods, as compared to the control, with a 1-year hazard ratio of 0.589 (95% CI: 0.476–0.728), 3-year HR of 0.677 (95% CI: 0.583–0.788), and 5-year HR of 0.669 (95% CI: 0.583–0.768). There was no statistical significance in the development of ION between cohorts, 1-year hazard ratio of 0.872 (95% CI: 0.627–1.212), 3-year HR of 1.002 (95% CI: 0.792–1.268), and 5-year HR of 0.978 (95% CI: 0.789–1.211). These results are depicted in Table 1 and summarized in the forest plot shown in Figure 2. To provide context for the relative risk estimates, absolute incidence, absolute risk reduction, and number needed to treat for legal blindness were calculated at 1-, 3-, and 5-year follow-up (Table 2).
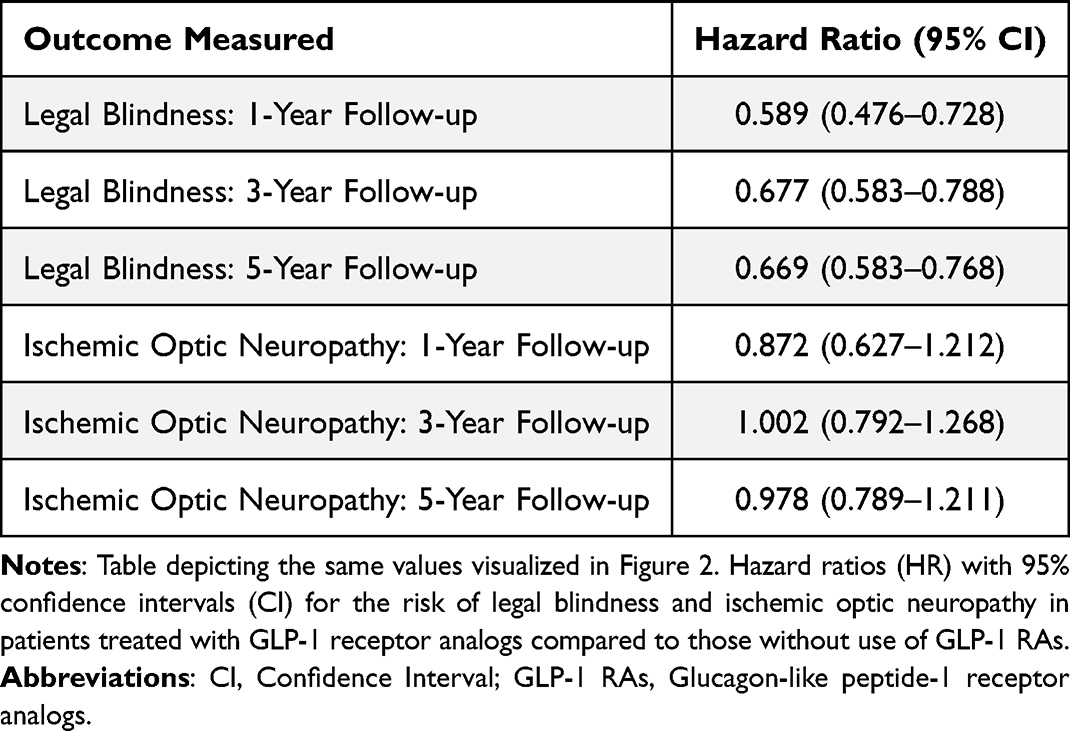 |
Table 1 Hazard Ratios (95% CI) for Legal Blindness and Ischemic Optic Neuropathy in Type 2 Diabetics with Cardiovascular Risk Factors with GLP-1 RA Use versus Nonuse |
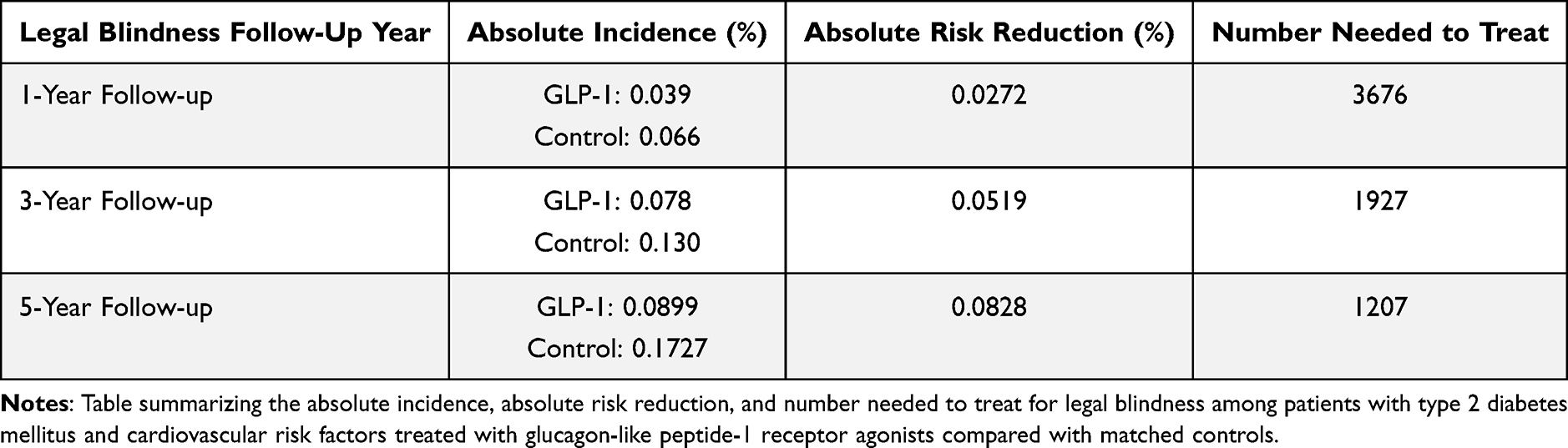 |
Table 2 Absolute Incidence, Absolute Risk Reduction, and Number Needed to Treat for Legal Blindness at 1-, 3-, and 5-Year Follow-Up |
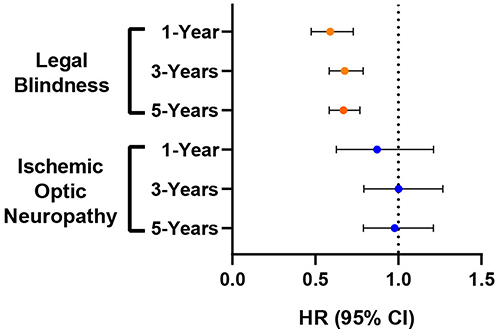 |
Figure 2 Comparison of Hazard Ratios (95% CI) for Legal Blindness and Ischemic Optic Neuropathy in Type 2 Diabetics with Cardiovascular Risk Factors Regarding GLP-1 RA Use versus Nonuse. Graph for visualizing the hazard ratios (HR) with 95% confidence intervals (CI) for the risk of legal blindness and ischemic optic neuropathy in patients treated with GLP-1 receptor analogs compared to those without use of GLP-1 RAs. The outcomes at 1-year, 3-year, and 5-year follow-up are shown for each outcome. A HR<1 indicates there was a statistically significant reduction in risk of the outcome in patients using GLP-1 RAs compared to the control. |
Discussion
Based upon our review of the English language medical literature, this is the first large-scale, propensity-matched cohort study to demonstrate a significant association between GLP-1 receptor analog use and reduced risk of legal blindness in patients with T2DM and CVRF. While prior studies have primarily focused on the potential risks of GLP-1 RAs in relation to ION, our findings showed no increased risk of ION and a possible protective benefit. We found no statistically significant difference in the incidence of ION between GLP-1 RA users and non-users in this high-risk population.
However, interpretation must remain cautious, and prospective studies incorporating fundus imaging, visual field testing, and optical coherence tomography (OCT) evaluation will be critical to clarify whether GLP-1 RAs influence ION risk. Although this study could not assess the impact of cumulative GLP-1 RA exposure or dosage variability, we sought to minimize this limitation by requiring documentation of continued GLP-1 RA use following the index event.
Our results contrast with prior investigations that raised concerns about an increased risk of NAION among GLP-1 RA users. Chou et al7 and Hsu et al8 reported conflicting findings regarding the possible association of NAION and GLP-1 use. It is important to note that the ICD-10 code H47.01, which is utilized in our study, and previous studies, is limited by the ICD-10 coding system. This ICD-10 code includes the many variants of ION, including arteritic anterior ION. Therefore, it is vital to exclude a diagnosis of giant cell arteritis and optic neuritis to better examine ION outcomes. Even with these exclusions, this administrative database lacks the clinical resolution to reliably isolate NAION cases.
Moreover, as with all retrospective observational studies relying on ICD coding, outcomes may be influenced by variability in diagnostic documentation practices across providers and institutions, which could introduce heterogeneity in case identification. To partially mitigate this limitation, we did not make direct claims about NAION incidence alone but instead examined a more clinically relevant and objective outcome of “legal blindness”. The low prevalence of NAION and the limitations of small sample sizes in the database (eg, TriNetX rounding patient counts <10) further complicate meaningful statistical interpretation for uncommon events like ION. By focusing on “legal blindness”, a definitive endpoint less vulnerable to diagnostic misclassification, we aimed to reduce noise introduced by ambiguous coding. However, we acknowledge that the coding accuracy for “legal blindness” is variable across institutions, as use of H54 codes may not be universal. Such variability would likely be non-differential between groups and therefore bias results toward the null, making the observed association conservative. Because the cohorts were effectively matched across demographic, systemic, and ocular comorbidities, the primary distinguishing variable was GLP-1 RA use. Thus, we would not expect GLP-1 RA treatment status itself to be associated with differences in specialist visit frequency or other factors that would increase the likelihood of receiving a “legal blindness” code. Moreover, because some patients entering the cohort closer to our study timeframe endpoints (2018–2025) did not yet have the opportunity for five full years of follow-up, our ability to capture long-term blindness risk remains constrained. The TriNetX database does not contain structured visual acuity fields, precluding adjustment for baseline visual function in propensity matching. This represents a significant limitation, as pretreatment vision status may influence subsequent blindness risk. We attempted to partially address this confounding by matching across multiple systemic and ocular risk factors, but residual confounding is possible. Additionally, given the results found by Galvez-Ruiz et al13 which suggest a potential association between phosphodiesterase-5 (PDE5) inhibitor use and increased risk of NAION, we excluded patients with documented PDE5 inhibitor prescriptions to minimize confounding.
The observed reduction in legal blindness among GLP-1 RA users may be attributed to the drug class’s systemic vascular and metabolic benefits, which could mitigate several sight-threatening complications of diabetes.14 In T2DM, legal blindness most often results from proliferative diabetic retinopathy, diabetic macular edema, neovascular glaucoma, or retinal detachment, each driven by chronic microvascular damage and ischemia. GLP-1 RAs are known to improve glycemic control while providing anti-inflammatory and endothelial-stabilizing effects, which may collectively reduce the progression of diabetic retinal disease.15 Additionally, by supporting better blood pressure control and vascular function, GLP-1 RAs may offer protection against hypertensive retinopathy and retinal vascular occlusions such as central or branch retinal artery or vein occlusions.16 The observed association between GLP-1 receptor agonist use and reduced risk of legal blindness may be biologically plausible given their established anti-inflammatory and neuroprotective effects, including modulation of neuroinflammation and preservation of neuronal integrity. Experimental and translational studies suggest that GLP-1 receptor agonists may attenuate inflammatory signaling and microglial activation, mechanisms that could contribute to protection of retinal and optic nerve tissues in high-risk populations.9–11 In contrast, ischemic optic neuropathy is driven primarily by acute vascular hypoperfusion of the optic nerve head, which may explain the lack of a significant association observed for this outcome.17 Still, interpretation of long-term effects must be cautious, as the widening follow-up gap between cohorts at 5 years may influence risk estimates, even though our results remained stable across all intervals. Moreover, we cannot determine the specific etiology of “blindness” in specific patients, and it remains possible that the observed associations may be influenced by non-ocular contributors to visual disability. Although our propensity score matching controlled for use of other antidiabetic medication classes, we did not restrict the cohort to GLP-1 monotherapy. This decision reflects real-world clinical practice, where GLP-1 analogs are typically added to metformin or other agents rather than prescribed as standalone therapy. Restricting our study to monotherapy could have yielded a less representative and much smaller patient sample, limiting generalizability. Additionally, prescription records were used as a proxy for exposure, but true medication adherence could not be confirmed, which may attenuate or exaggerate observed associations. The act of initiating treatment for diabetes itself may reflect an inherent bias in the cohort, as patients on GLP-1 RAs may be systematically different in health behaviors or disease burden than non-users, even after matching. We attempted to mitigate bias from differential treatment by matching on demographic and clinical variables associated with disease severity, thereby strengthening the internal validity of our findings.
From a clinical standpoint, these findings carry important implications. As GLP-1 RAs continue to gain prominence in the reduction of BMI and management of T2DM—especially among patients with additional cardiovascular comorbidities—our study suggests that GLP-1 RAs may confer ancillary ophthalmic benefits beyond glycemic and cardiovascular control.
Future prospective studies should incorporate comprehensive ophthalmic assessment, including detailed history, fundus examination, and OCT imaging, to confirm NAION only after excluding other potential causes of optic neuropathy such as giant cell arteritis or optic neuritis. Such rigorous evaluation will help ensure diagnostic accuracy, facilitate the establishment of causality, elucidate potential pathophysiologic mechanisms linking GLP-1 RA therapy to optic nerve outcomes, and address limitations inherent to retrospective studies. In the interim, these findings may help inform clinician–patient discussions regarding the ocular safety profile of GLP-1 receptor agonists in individuals with type 2 diabetes who are at elevated vascular risk.
Human Subjects
The study did not meet the criteria for human subjects research, as this was an analysis of an existing anonymized dataset.
Institutional Review Board
This study was conducted in accordance with the tenets of the Declaration of Helsinki. Prior to study initiation, the University of Texas Medical Branch Institutional Review Board reviewed this project and determined that it does not constitute human subjects research because only de-identified, aggregate data obtained through the TriNetX global research network were analyzed. Because no identifiable private information was accessed and no direct interaction with individuals occurred, informed consent was not required. The Western IRB granted TriNetX a waiver because its federated design ensures that only aggregated, de-identified summary data are shared externally; no protected health information is exchanged, and no human subject activities occur during retrospective analyses.
Abbreviations
A1c, Hemoglobin A1c; ATC, Anatomical Therapeutic Chemical; BMI, Body mass index; CI, Confidence interval; CVRF, Cardiovascular risk factors; DPP-4, Dipeptidyl peptidase-4; EMR, Electronic medical records; GLP-1 RA, Glucagon-like peptide-1 receptor agonist; HbA1c, Hemoglobin A1c; HCO, Healthcare organizations; HIPAA, Health Insurance Portability and Accountability Act; HR, Hazard ratio; ICD, International Classification of Diseases; ICD-9, International Classification of Diseases, Ninth Revision; ICD-10, International Classification of Diseases, Tenth Revision; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification; ION, Ischemic optic neuropathy; IRB, Institutional Review Board; NAION, Non-arteritic anterior ischemic optic neuropathy; NIH, National Institutes of Health; PDE5, Phosphodiesterase-5; PSM, Propensity score matching; SGLT2, Sodium-glucose co-transporter-2; SMD, Standardized mean difference; T2DM, Type 2 diabetes mellitus; TNX Curated, TriNetX Curated; UTMB, University of Texas Medical Branch; WIRB, Western Institutional Review Board; WHO, World Health Organization; OCT, Optical Coherence Tomography.
Acknowledgments
This research was supported by the UTMB Institute for Translational Sciences, supported in part by a Clinical and Translational Science Award (UL1 TR001439) from the National Center for Advancing Translational Sciences at the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Funding
There is no funding to report.
Disclosure
Andrew G. Lee, MD has served as a consultant for the National Aeronautics and Space Administration (NASA), the National Football League (NFL), US Department of Justice, and is a consultant for Amgen, AstraZeneca, Argenx, Bristol-Myers Squibb, Alexion, Celgene, Stoke, Ethyreal, Catalyst, Dompe, and Viridian. Dr. Lee is also on the editorial board of JNO, CJO, JJO, Frontiers in Ophthalmology, and JAMA Ophthalmology. The other authors declare no conflicts of interest in this work.
References
1. Sadun AA. Neuro-ophthalmic manifestations of diabetes. Ophthalmology. 1999;106(6):1047–9. doi:10.1016/S0161-6420(99)90242-7
2. Roșu CD, Bratu ML, Stoicescu ER, et al. Cardiovascular risk factors as independent predictors of diabetic retinopathy in type 2 diabetes mellitus: development of a predictive model. Medicina. 2024;60(10):1617. doi:10.3390/medicina60101617
3. Collins L, Costello RA. Glucagon-like peptide-1 receptor agonists. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
4. Hullon D, Subeh GK, Volkova Y, Janiec K, Trach A, Mnevets R. The role of glucagon-like peptide-1 receptor agonists in enhancing endothelial function: a potential avenue for improving heart failure with preserved ejection fraction. Cardiovasc Diabetol. 2025;24(1):70. doi:10.1186/s12933-025-02607-w
5. Hathaway JT, Shah MP, Hathaway DB, et al. Risk of nonarteritic anterior ischemic optic neuropathy in patients prescribed semaglutide. JAMA Ophthalmol. 2024;142(8):e241198. doi:10.1001/jamaophthalmol.2024.2296
6. Abbass NJ, Nahlawi R, Shaia JK, et al. Effect of semaglutide and glucagon-like peptide-1 receptor agonists on risk of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. 2025;277:24–31. doi:10.1016/j.ajo.2025.02.025
7. Chou CC, Pan SY, Sheen YJ, et al. Association between semaglutide and nonarteritic anterior ischemic optic neuropathy: a multinational population-based study. Ophthalmology. 2024. doi:10.1016/j.ophtha.2024.10.030
8. Hsu AY, Kuo HT, Wang YH, et al. Semaglutide and nonarteritic anterior ischemic optic neuropathy risk among patients with diabetes. JAMA Ophthalmol. 2025;143(5):400–407. doi:10.1001/jamaophthalmol.2025.0349
9. Albanese GM, Visioli G, Alisi L, et al. Ocular effects of glucagon-like peptide-1 receptor agonists: a review of current evidence and safety concerns. Diabetology. 2025;6:117. doi:10.3390/diabetology6100117
10. Zhang DL, Finn AP. Glucagon-like peptide-1 receptor agonists and the eye. Curr Opin Ophthalmol. 2025;36(5):407–413. doi:10.1097/ICU.0000000000001137
11. Kopp KO, Glotfelty EJ, Li Y, Greig NH. Glucagon-like peptide-1 receptor agonists and neuroinflammation: implications for neurodegenerative disease treatment. Pharmacol Res. 2022;186:106550. doi:10.1016/j.phrs.2022.106550
12. Hadi YB, Lakhani DA, Naqvi SF, Fatima NU, Sarwari AR. Outcomes of SARS-CoV-2 infection in patients with cystic fibrosis: a multicenter retrospective research network study. Respir Med. 2021;188:106606. doi:10.1016/j.rmed.2021.106606
13. Galvez-Ruiz A, Arishi N. Sequential nonarteritic anterior ischemic optic neuropathy in patients taking sildenafil: a report of ten cases. Saudi J Ophthalmol. 2013;27(4):241–246. doi:10.1016/j.sjopt.2013.07.010
14. Marx N, Husain M, Lehrke M, Verma S, Sattar N. Glucagon-like peptide-1 receptor agonists for the reduction of atherosclerotic cardiovascular risk in patients with type 2 diabetes. Circulation. 2022;146(24):1882–1894. doi:10.1161/CIRCULATIONAHA.122.059595
15. Xie Z, Yang Z, Tian D, Chen Y. Unlocking the potential of glucagon-like peptide-1 receptor agonists in ocular therapeutics: from molecular pathways to clinical impact. Front Pharmacol. 2025;16:12328412. doi:10.3389/fphar.2025.1618079
16. Pan SY, Weng CH, Tsai SF, et al. Risk of retinal vein occlusion between glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes: a retrospective cohort study. Ophthalmol Sci. 2025;5(4):100734. doi:10.1016/j.xops.2025.100734
17. Patel HR, Margo CE. Pathology of ischemic optic neuropathy. Arch Pathol Lab Med. 2017;141(1):162–166. doi:10.5858/arpa.2016-0027-RS
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review and Meta-Analysis of Efficacy and Safety of Liraglutide in Patients with Type 2 Diabetes Mellitus
Joshi S, Das AK, Khunti K, Khunti S, Choudhari SY
Diabetes, Metabolic Syndrome and Obesity 2026, 19:570273
Published Date: 8 March 2026