")
Back to Journals » Journal of Pain Research » Volume 16
Global Trends of Gastrointestinal Endoscopy Anesthesia/Sedation: A Bibliometric Study (from 2001 to 2022)
Authors Xiong Y , Yan H, Qu L, Wang S , Meng X, Zhu X, Zhang P, Yuan S , Shi J
Received 1 March 2023
Accepted for publication 6 July 2023
Published 15 July 2023 Volume 2023:16 Pages 2393—2406
DOI https://doi.org/10.2147/JPR.S408811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Yujun Xiong,1,* Haoqi Yan,2,* Lang Qu,3 Shuqi Wang,4 Xiangda Meng,5 Xingyun Zhu,6 Pan Zhang,1 Su Yuan,2 Jihua Shi1
1Department of Gastroenterology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Anesthesiology, Fuwai Hospital, National Center of Cardiovascular Diseases, Chinese Academy of Medical Sciences; Peking Union Medical College, Beijing, 100037, People’s Republic of China; 3Department of Anesthesiology, Shanghai General Hospital, Shanghai, People’s Republic of China; 4Department of Otolaryngology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 5Department of Neurosurgery, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 6Department of Endocrinology, Beijing Jishuitan Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su Yuan, Department of Anesthesiology, Fuwai Hospital, Chinese Academy of Medical Sciences; Peking Union Medical College, Xicheng District, Beijing, People’s Republic of China, Email [email protected] Jihua Shi, Department of Gastroenterology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, 100370, People’s Republic of China, Email [email protected]
Background: Gastrointestinal (GI) endoscopy becomes more and more common now in order to diagnose and treat GI diseases, and anesthesia/sedation plays an important role. We aim to discuss the developmental trends and evaluate the research hotspots using bibliometric methods for GI endoscopy anesthesia/sedation in the past two decades.
Methods: The original and review articles published from 2001 to December 2022 related to GI endoscopy anesthesia/sedation were extracted from the Web of Science database. Four different softwares (CiteSpace, VOSviewer, and Bibliometrix, Online Analysis Platform of Literature Metrology (Bibliometric)) were used for this comprehensive analysis.
Results: According to our retrieval strategy, we found a total of 3154 related literatures. Original research articles were 2855, and reviews were 299. There has been a substantial increase in the research on GI endoscopy anesthesia/sedation in recent 22 years. These publications have been cited 66,418 times, with a mean of 21.04 citations per publication. The US maintained a leading position in global research, with the largest number of publications (29.94%), and China ranked second (19.92%). Keyword burst and concurrence showed that conscious sedation, colonoscopy and midazolam were the most frequently occurring keywords.
Conclusion: Our research found that GI endoscopy anesthesia/sedation was in a period of rapid development and demonstrated the improvement of medical instruments and surgical options that had significantly contributed to the field of GI endoscopy anesthesia/sedation. The US dominates this field, and the selection and dosage of sedative regimens have always been the foci of disease research to improve comfort and safety, while adverse events and risks arouse attention gradually. In the past 20 years, hotspots mainly focus on upper gastrointestinal endoscopy, gastroscopy, and esophagogastroduodenoscopy. These data would provide future directions for clinicians and researchers regarding GI endoscopy anesthesia/sedation.
Keywords: gastrointestinal endoscopy anesthesia, sedation, bibliometric analysis, CiteSpace, VOSviewer
Introduction
Gastroscopy and colonoscopy are the principal means for examining, diagnosing, and treating upper and lower GI diseases and conditions involving the esophagus.1,2 GI endoscopy procedure is invasive, and patients often do not cooperate or even refuse GI endoscopy because of the pain caused by the procedure and the psychological fear of the procedure itself, just like the bronchoscopy.3,4 However, the application of anesthesia or sedatives can significantly reduce the pain and tension of patients and promote the spread of painless gastrointestinal endoscopy. Therefore, anesthesia or sedation is also essential for diagnosing and treating GI diseases during endoscopy.5
Qin et al6 have ever made a bibliometric analysis of endoscopic sedation research from 2001 to 2020, but they mainly focused on sedative drugs, complications and endoscopy quality control in endoscopic sedation. Although moderate and deep sedation is quite widely applied in GI endoscopy procedures, general anesthesia is usually applied in those patients who have high risks, like aspiration pneumonia, severe obesity, which would be much safer. With increasing GI endoscopic procedures, sedation alone is no longer sufficient for GI endoscopy needs.
In this study, we used bibliometric methods to analyze the trends, hotspots and relationships of research on GI endoscopy anesthesia/sedation, aiming to supply more updated and extensive information to clinical physicians and researchers.
Materials and Methods
Data Sources
In this study, the original data were downloaded from the SCI-expanded database in the Web of Science Core Collection on 31 December 2022. The search was finished on the same day to eliminate any bias caused by the database update. The search strategies used in this study were as follows: [TS=(gastroscopic OR gastroscopy OR gastroscopies OR colonoscopy OR colonoscopies OR colonoscopic OR (upper endoscopy) OR (lower endoscopy) OR (endoscopic mucosal resection) or EMR OR (endoscopic submucosal dissection) OR ESD OR ERCP OR (endoscopic retrograde cholangiopancreatography)) AND TS=((general anesthesia) OR (general anaesthesia) OR (general anesthesi*) OR (general anaesthesi*) OR ((“Conscious Sedation”) OR (“minimal Sedation”) OR (anxiolysis) OR (“Sedation, Moderate”) OR (“Moderate Sedation”) OR (“Sedation, Conscious”) OR (“Sedation, deep”) OR (“Painless”) OR (sedation) OR (sedative) OR (sedated)))]. The detailed search strategy is shown in Figure 1.
 |
Figure 1 Flow chart of literature filtering. |
Data Collection
Raw data were initially extracted from the Web of Science SCI-expanded database. Two authors (YX and HY) independently searched information online and set the primary database, including countries, institutions, journals, authors, H-index, etc., and reached a consensus after making comparisons.
Statistical Analysis
Microsoft Excel 2019 and Online Analysis Platform of Bibliometrics (http://bibliometric.com/) were used to analyze the article counts, the total number of citations, the average number of citations, countries, institutions, journal sources, H-index, and impact factor (IF).
Furthermore, VOSviewer (1.6.18) for identifying countries, institutions and keywords, and building related visual networks and adding different graphical representations in bibliometric maps by displaying large bibliometric maps. What’s more, we also used CiteSpace (6.1.R3) to connect different features for bursts of keywords and references, and then deeply analyzed the trends and main ideas. R (Version 4.2.0) is the language and environment for statistical computing and graphics. The Bibliometrix package in R was used to illustrate further the changes in the annual document.7
Results
The Searched Results of GI Endoscopy Anesthesia/Sedation Related Literatures
A total of 3154 publications were extracted from the Web of Science. Based on the inclusion criteria, all the publications related to GI endoscopy anesthesia/sedation were extracted from the Web of Science. The total number of citations was 66,418 (48,257 without self-citation), and the average citing frequency was 21.06 times per article. The H-index of all the publications related to GI endoscopy anesthesia was 98.
The Annual Trends of GI Endoscopy Anesthesia/Sedation-Related Publications
The number of research articles on GI endoscopy anesthesia trended upward from 2001 to 2022 (Figure 2A). From 2001 to 2016, the annual number of publications increased gradually, and in 2016 the number of articles published each year reached the peak because during this period, professional theories in this field developed rapidly. The annual number of publications increased from 64 in 2001 to 217 in 2022, demonstrating that GI endoscopy anesthesia/sedation had attracted growing attention and interests among global researchers as time flew.
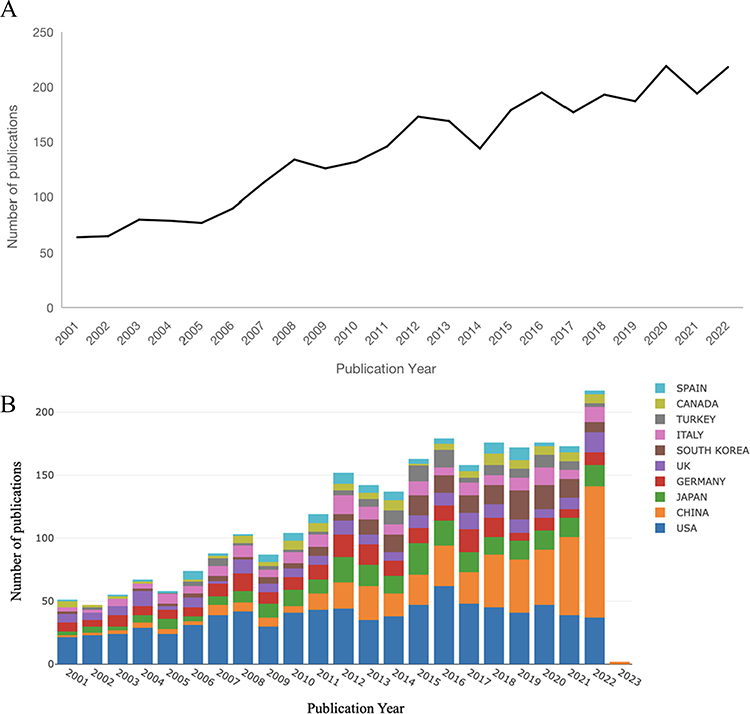 |
Figure 2 (A) The number of annual publications. (B) Growth trends of the top 10 countries (Conducted by online analysis platform of Bibliometrics). |
The Contributions of Countries and Institutions to Global Publications
In the past 20 years, the United States has made the most significant contribution to the study of GI endoscopy anesthesia/sedation, followed by China, Japan, Germany, etc. (Figure 2B).
The analysis of international cooperation shows that the United States cooperated frequently with other countries. Although China ranked second in the number of articles published, it had less cooperation with other countries compared with other countries (Figure 3A). In terms of research institutions, the top 10 were (Table 1) Mayo Clin (83), Yonsei Univ (76), Univ Calif Los Angeles (42), Cleveland Clin Fdn (41), Tech Univ Munich (41), Harvard Univ (41), Chinese Univ Hong Kong (40), Indiana Univ (39), Cleveland Clin (39), Univ Toronto (39). The network density of GI endoscopy anesthesia/sedation research was only 0.0052 (Figure 3B), meaning that the research teams were relatively dispersed in several institutions and do not cooperate closely enough.
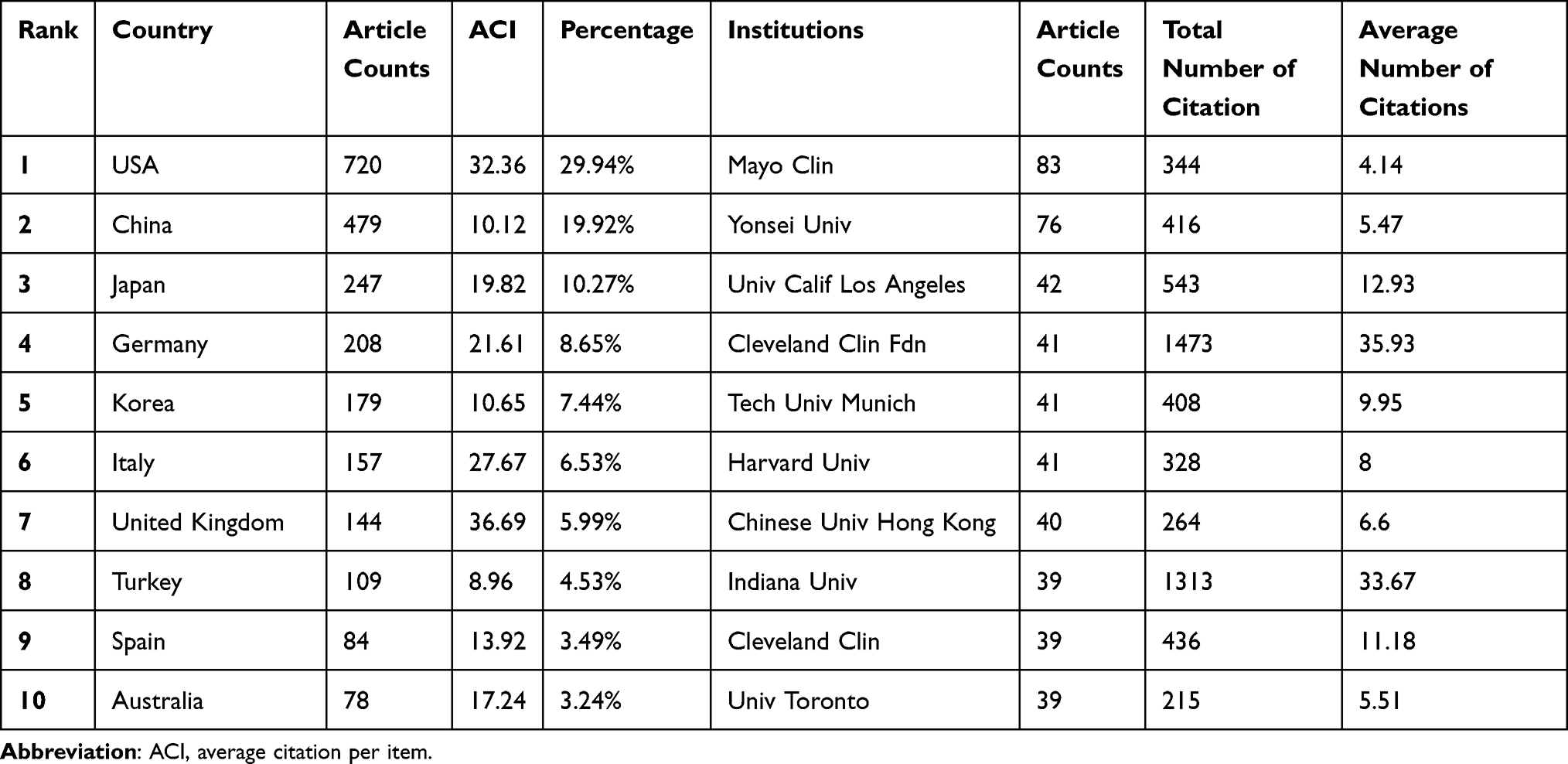 |
Table 1 The Top 10 Countries/Regions and Institutions Contributing to Publications in GI Endoscopy Anesthesia Research (Sorted by Count) |
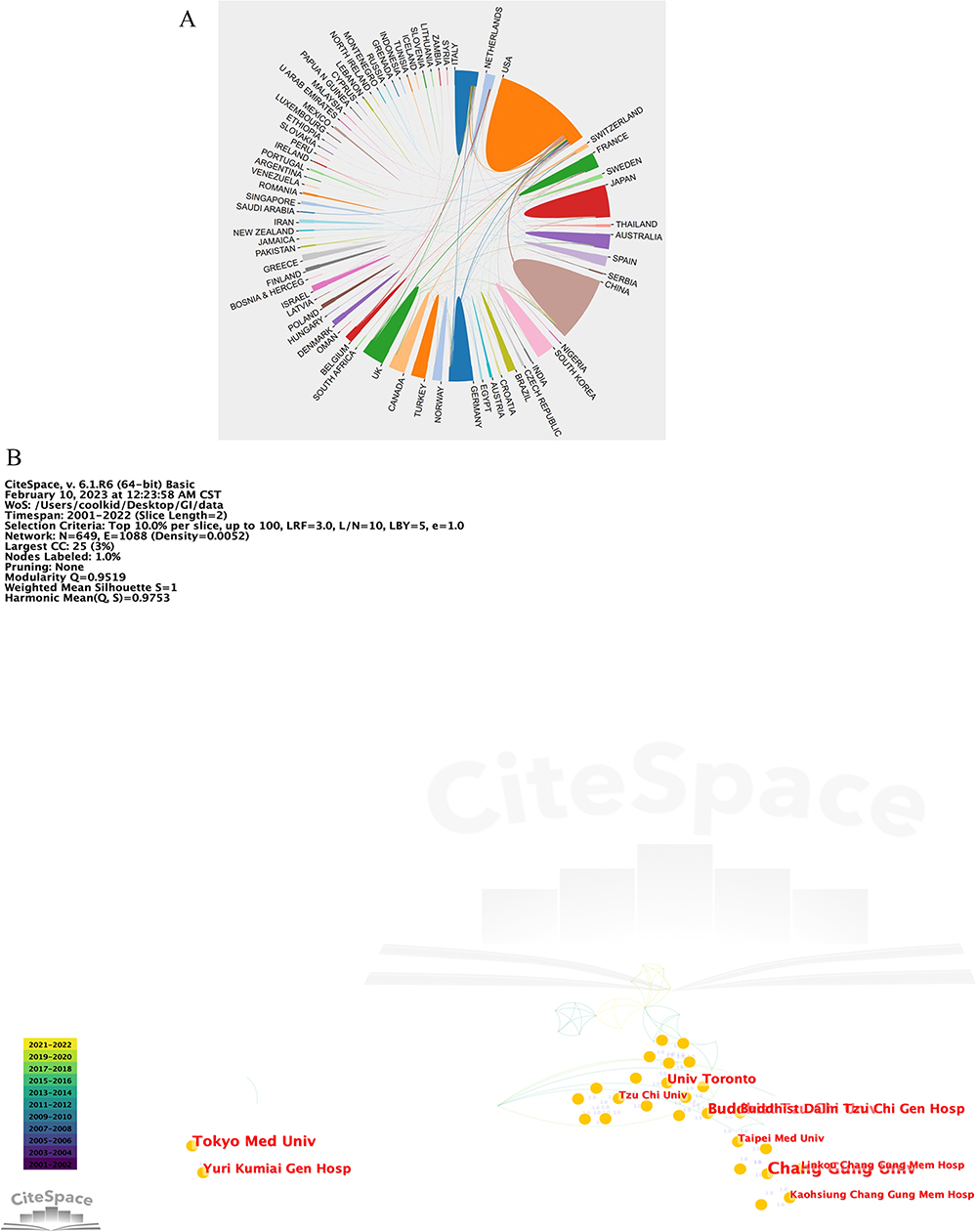 |
Figure 3 The distribution of countries/regions and institutions. Cooperative relations among countries/regions. (A) (The area represents the number of articles, and the connection represents the cooperative relationship. Conducted by online analysis platform of Bibliometrics) and institutions (B). [Conducted by CiteSpace (version 5.7.R3, Drexel University)]. |
Journals Publishing Researches on GI Endoscopy Anesthesia/Sedation
In these 20 years, 654 journals have published in the field of GI endoscopy anesthesia/sedation. Of the 3154 articles on GI endoscopy anesthesia/sedation we studied, the top 10 journals published 955 (30.28%) (Table 2). In terms of the number of publications, the top 3 journals are GASTROINTESTINAL ENDOSCOPY (IF = 10.396), ENDOSCOPY (IF = 9.776) and WORLD JOURNAL OF GASTROENTEROLOGY (IF = 5.374). According to JCR of 2022, the 3 journals belong to Q1/Q2.
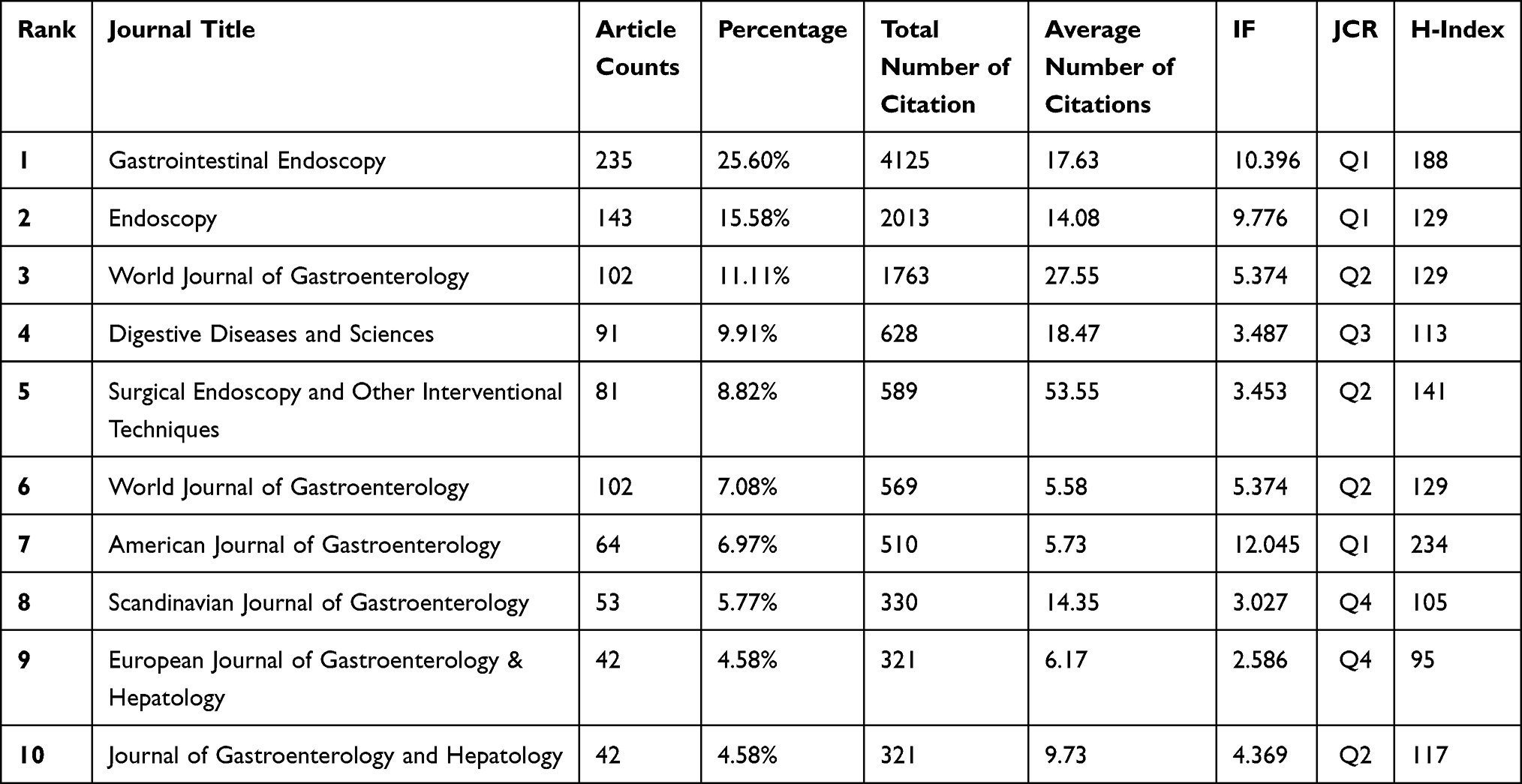 |
Table 2 The Top 10 Most Active Journals Published Articles in GI Endoscopy Anesthesia Research (Sorted by Count) |
The Contributions of Authors to GI Endoscopy Anesthesia/Sedation Research
The top 10 authors (the number of literatures published) are listed in Table 3. Among those, Leung, Felix W, from West Los Angeles and Sepulveda Veterans Administration Hospital Center, UCLA School of Medicine, ranked first. Those show that Leung, Felix W has made outstanding achievements in GI endoscopy anesthesia/sedation research and his achievements not only focus on animal experiments but also include clinical studies, like randomized controlled studies. Figure 4 shows clusters of authors that collaborated. For example, Cohen lb collaborated closely with Drake lm and Heuss, lt, and dumonceau, jm collaborated closely with Nishizawa, t.
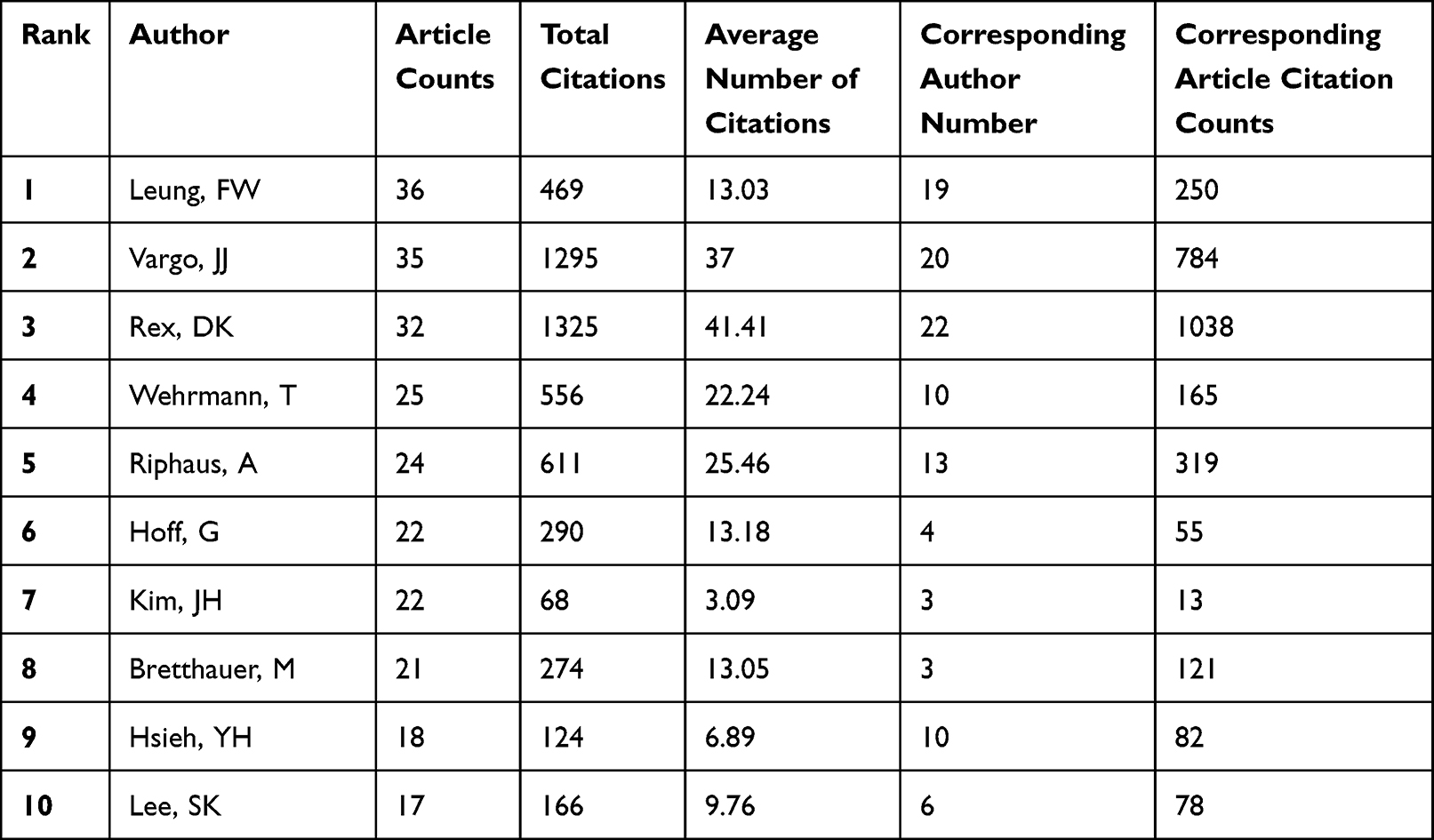 |
Table 3 The Top 10 Most Productive Authors and Corresponding Authors Contributed to Publications in GI Endoscopy Anesthesia Research |
 |
Figure 4 Cooperation map of authors in the studies of GI endoscopy anesthesia/sedation. Different colors represent different institutions that cooperate closely, the size of the circle is proportional to the total number of articles in that institution, and the distance between two institutions is inversely proportional to the degree of cooperation between them. |
Top Cited Papers on GI Endoscopy Anesthesia/Sedation
In order to analyze the most influential papers in this field from 2001 to December 2022, we shortlisted the top 10 publications with the most citations. We listed them in Table 4 regarding the title, first author, journal, publication year, total citation, JCR and IF. The work of Rajkomar et al ranked first with the highest citation number (915). This paper, published on The New England Journal of Medicine, mainly focused on machine-learning models to assist diagnosis of diseases.8 The paper “Inflammatory bowel disease in children and adolescents: Recommendations for diagnosis - The Porto criteria”, ranked second, which talked about the workup and criteria used for diagnosis of IBD patients before 20.9 The paper by Bowles et al, “A prospective study of colonoscopy practice in the UK today: are we adequately prepared for national colorectal cancer screening tomorrow?”, ranked third.10
 |
Table 4 The Top 10 High-Cited Papers in GI Endoscopy Anesthesia Research from 2001 to 2022 |
What’s more, we analyzed the most influential papers from 2021 to 2022 December in Table 5; considering the time issue, all articles were published in 2021, and the top 3 most cited papers mainly focused on remimazolam or clinical trials, different from hot keywords including IBD and machine learning models before.
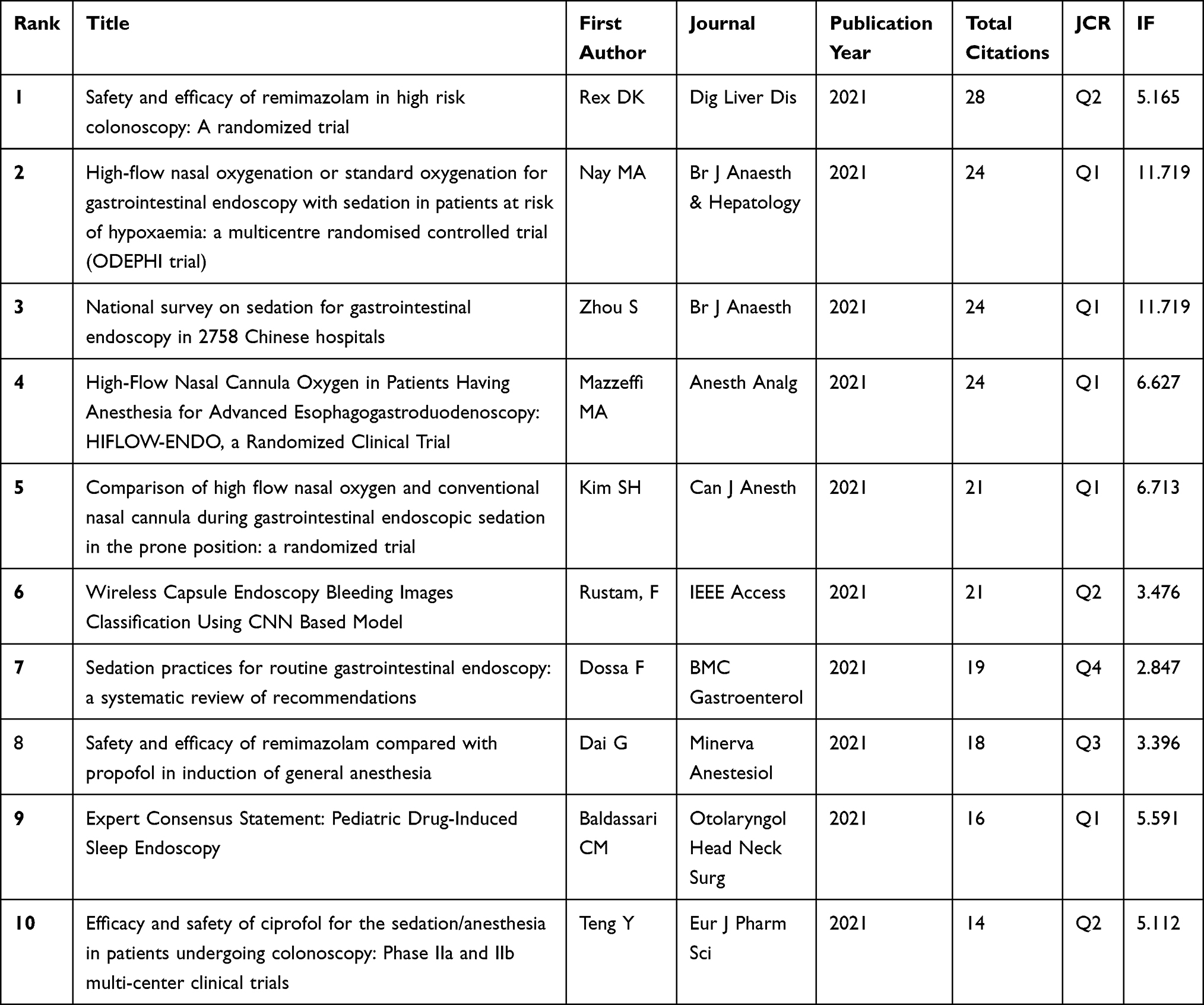 |
Table 5 The Top 10 High-Cited Papers in GI Endoscopy Anesthesia Research from 2021 to 2022 |
Analysis of Keywords
In Figure 5A, a blue line is used to mark the timeline. The red segment on top of the blue line represents burst detections by showing the burst’s start year, end year, and duration. We intended to find keywords with research significance to reflect the evolutionary trend of this field. “Upper gastrointestinal endoscopy” showed the most robust burst strength, followed by “gastroscopy”, “esophagogastroduodenoscopy”, and “registered nurse”.
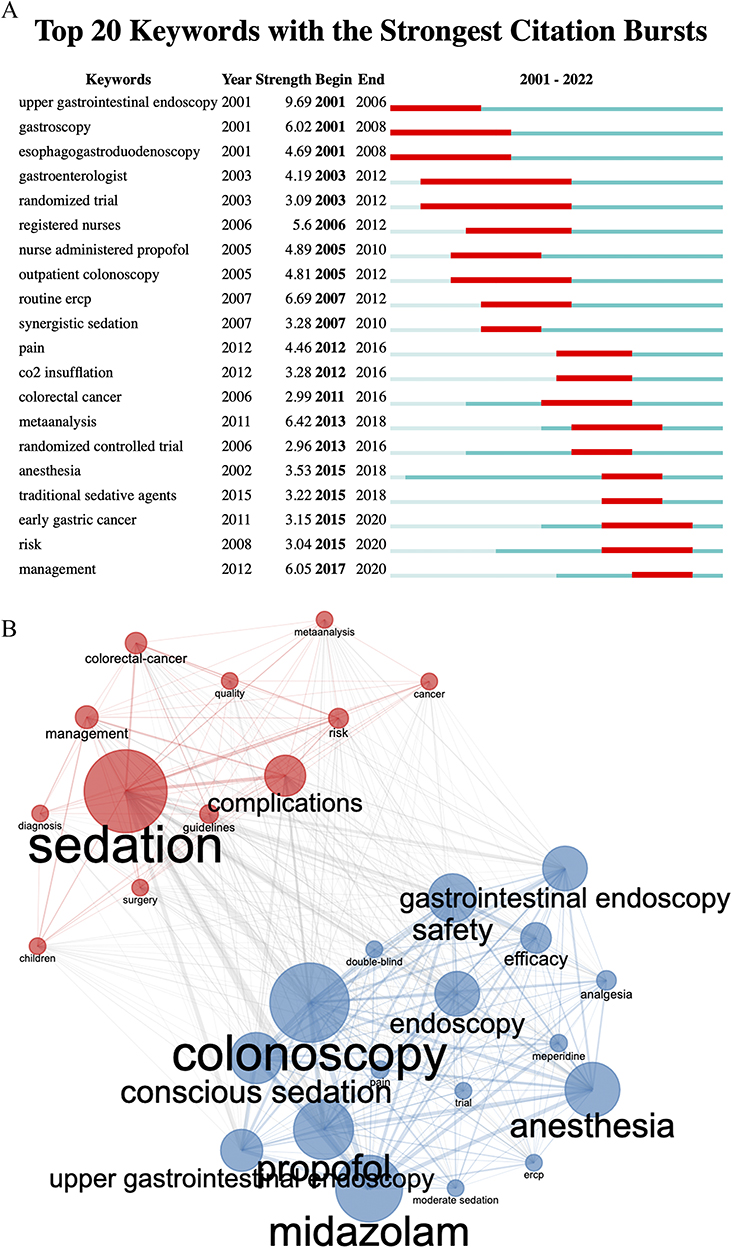 |
Figure 5 (A) Top 20 keywords with the strongest citation bursts in the studies of GI endoscopy anesthesia/sedation. (B) Analysis of keywords. |
As shown in Figure 5B, conscious sedation, colonoscopy and midazolam were the most frequently occurring keywords and were divided into two clusters. The first one (blue circles) was mainly about applying sedative medicines and analgesics in GI endoscopy anesthesia/sedation research. The second cluster (red circles), was mainly about the risks, meta-analysis, and randomized controlled trial in the examination and treatment of various digestive diseases.
References with the Strongest Citation Bursts
We conducted CiteSpace to investigate citation burstness, which indicated references that attracted a surge of citations from scholars in a specific period of time. Figure 6 displays the top 10 most cited references, with the minimum duration of an outbreak set at 2 years, and the red line segments represented the beginning and last years of the duration of an outbreak associated with academia for a particular period.
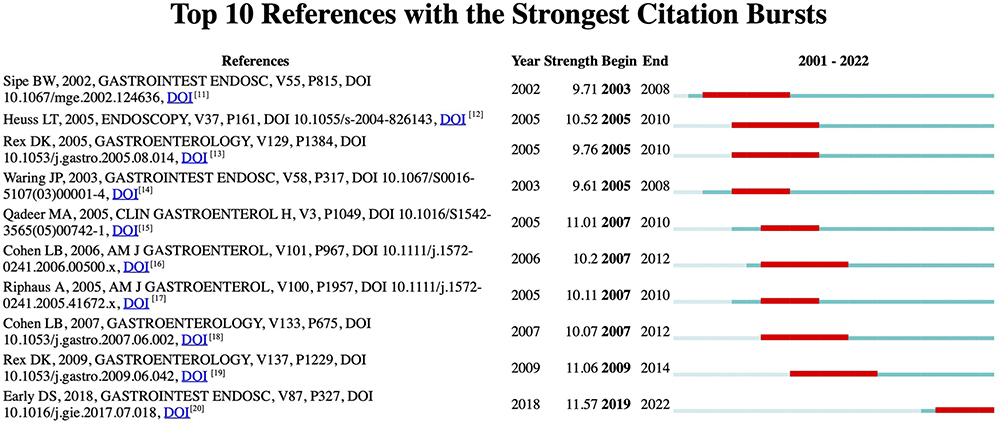 |
Figure 6 Top 10 references with strong citation burstiness (MD = 2). The red bars mean some references are cited frequently; the blue bars represent references cited infrequently. |
Among the top 10 references, the strongest burstiness (n = 15.86) was caused by the paper, “Propofol versus midazolam/meperidine for outpatient colonoscopy: administration by nurses supervised by endoscopists”, authored by Sipe et al with citation burstiness from 2003 to 2008.11 This was followed by the paper, “Changing patterns of sedation and monitoring practice during endoscopy: results of a nationwide survey in Switzerland” published in the journal ENDOSCOPY by Heuss et al.12 Besides, the research titled “Trained registered nurses/endoscopy teams can administer propofol safely for endoscopy”,13 published in 2005 emerged third. In this article, the author found that trained nurses and endoscopists can administer propofol safely for endoscopic procedures, which can decrease anesthesia associated high costs.
Discussion
General Information
In the present study, we utilized VOSviewer, Citespace and R to analyze literature related to endoscopy anesthesia/sedation. We retrieved a total of 1244 original articles and reviews published since 2001. Our results indicated that the annual publications and citations of endoscopy anesthesia/sedation had shown an upload trend in recent years. China and the United States are now world leaders in the field of endoscopy anesthesia/sedation research. Furthermore, four of the top 10 prolific institutions were from the United States, such as Mayo Clinic and Yonsei University. In addition, American institutions were observed with more worldwide cooperations, which maximized its geographical advantages and further strengthened its academic influence on GI endoscopy anesthesia/sedation research. Although China ranked second in the number of publications in this field, it cooperated less with other countries compared with the other countries/regions in the top 10 categories. This phenomenon may be accounted by a late start of China in this field.
We found that more than half of productive journals were classified as Q1 or Q2, and according to the latest Journal Citation Reports (JCR), The New England Journal of Medicine (IF 176.079, Q1) had the highest IF. However, European Archives of Oto-Rhino-Laryngology (IF 3.236, Q2) and Journal of Pediatric Gastroenterology and Nutrition (IF 3.288, Q2) were two of the top ten productive journals, and their IF values were less than 5, showing IF values cannot fully reflect the levels of journals. This finding indicated that improving research quality while increasing output might enhance their scholarly impact.
Furthermore, our results demonstrated that Leung, Felix W has made outstanding achievements in GI endoscopy anesthesia/sedation research. His achievements not only focus on animal experiments but also include clinical studies, like randomized controlled studies. He mainly focused on the animal experiments and clinical studies on GI endoscopy anesthesia/sedation. The top-cited articles were most often published in top journals within the research field of GI endoscopy, including GASTROINTESTINAL ENDOSCOPY and ENDOSCOPY. Notably, the distribution of highly cited journals in the references was similar to the actively published journals.
Hotspots and Frontiers
Through the potent combination of top keywords and literature, we attributed the research hotspots as follows: 1) Complications of GI endoscopy with anesthesia/sedation assistance. Anesthesia/sedation-related adverse events including hemodynamic events,7 hypoxemia, respiratory depression,21 respiratory obstruction,22 reflux and aspiration, laryngospasm,23 postoperative nausea and vomiting (PONV), and delayed recovery still happen occasionally during or after anesthesia. 2) Risk factors including older age (Years >75),24 long time procedure,25 BMI ≤ 18 kg/m2, ASA ≥III26 contribute to the occurrence of sedation-related adverse events. What’s more, Kilic et al27 found that higher BMI was associated with an increased frequency of sedation-related complications. Although numerous studies have summarized the risk factors of sedation-related adverse events, there is still a lack of a well-recognized risk prediction model for the complications of GI endoscopy anesthesia. Further research should be conducted to minimize the complications of GI endoscopy anesthesia by establishing risk prediction models.
Qin et al6 searched keywords with the strongest citation burstiness and found that alfentanil and meperidine became the foci from 2001 to 2007/2008; however, we found that risks and adverse events became the hotspot keywords from 2015 to 2020/2022. The top 3 most cited papers in 2021–2022 mainly focused on remimazolam or clinical trials, indicating that new drug trials recently became the new research foci in GI endoscopy anesthesia/sedation.
The degree of sedation is determined by titration to achieve a safe, comfortable, and tolerable level. Different patients may require different levels of sedation when receiving the same procedure, and the same patient may achieve different levels of sedation in a single procedure. The purpose of sedation and analgesia is to relieve anxiety, discomfort, and pain and reduce the treatment process’s memory. With the development of GI endoscopy, traditional sedative methods using benzodiazepines or monitored anesthesia care (MAC) using propofol may not be safe enough for the patients. General anesthesia is applied in complicated gastrointestinal endoscopy patients with high risks and undergoing complex procedures—the level of sedation sufficient to operate ranges from minimal to complete anesthesia. In general, diagnostic and uncomplicated upper GI endoscopic and colonoscopy procedures can be successfully performed under moderate anesthesia (consciously).28 Endoscopic treatment without anesthesia is the standard in some countries outside the United States. Deeper sedation is applied to longer and more complex operations, including, but not limited to, endoscopic retrograde cholangiopancreatography (ERCP) or endoscopic ultrasonography (EUS). In addition, deep sedation may be considered for patients who have been or may not be regarded as unsuitable for standard sedation or those who cannot tolerate pain during the process of manipulation. These patients include long-term users of hallucinogens and benzodiazepines, alcoholics, drug addicts, and those with mental illnesses. Some authors recommend the routine use of short-acting anesthetics (eg, propofol) in standard endoscopic procedures to increase patient comfort.29 In addition, GI endoscopy anesthesia includes conscious sedation and deep sedation (anesthesia), and some complex procedures even require deep sedation analgesia and endotracheal intubation.30 As for bibliometric analysis conducted by Qin et al6 it mainly focused on endoscopic sedation research, and our research also included general anesthesia research related literatures, which was more widely covered in this field.
Anesthesia Practice
It is still controversial whether anesthesia specialists should perform GI endoscopy anesthesia. Considering the high cost and safety of patients, Daniela et al stated that propofol could still be administered safely by non-anaesthetic personnel, and even for advanced procedures.31 In the guidelines for sedation and anesthesia in GI endoscopy published in 2018,20 anesthesia provider assistance should be considered in the following situations: prolonged or therapeutic endoscopic procedures requiring deep sedation, anticipated intolerance to standard sedatives, increased risk for adverse events because of severe comorbidity (ASA class IV or V), increased risk for airway obstruction because of anatomic variant. Notably, registered nurses also played a significant role in GI endoscopy anesthesia. According to the guideline in 2018, medications targeting minimal and moderate sedation generally can be administered by an appropriately trained registered nurse (RN) under the supervision of an endoscopist. Several scientific societies have endorsed non-anesthesiologist sedation (NAS) during gastrointestinal endoscopy, considering it a safe procedure when administered by adequately trained personnel. Manno et al’s research showed that after completing the European Society of Gastroenterology and Endoscopy Nurses and Associates (ESGENA) sedation training course, the rate of adverse events was meager in their institution, which emphasizes the significance of training registered nurses.32
Besides the personal allocation during anesthesia, some researchers also paid attention to the monitoring and ventilation method during sedation. A randomized controlled study’s result showed that during sedation for EGD and colonoscopy, capnography played a crucial role in identifying apnea and changes in breathing patterns in mildly obese patients before their oxygen saturation (SpO2) levels drop. This early detection enabled healthcare providers to promptly intervene and reduce the incidence of severe hypoxia.33 In addition, a recent multicenter randomized controlled trial published in the British Journal of Anesthesia found that in patients at risk of hypoxemia undergoing gastrointestinal endoscopy under deep sedation, high-flow nasal oxygen significantly reduced the incidence of peripheral oxygen desaturation.34 Therefore, different ventilation methods should be applied according to the patient’s status. In implementing GI endoscopy anesthesia, many details are worth considering that need further study.
Conclusion
In recent decades, there has been a surge of interest in the field of anesthesia/sedation in GI endoscopy. The US dominates this field, represented by the largest number of publications (720) and extensive international collaborations. The selection and dosage of sedative regimens have always been the foci of disease research to improve comfort and safety, and adverse events and risks arouse attention gradually. In the past 20 years, hotspots mainly focus on upper gastrointestinal endoscopy, gastroscopy, and esophagogastroduodenoscopy. In summary, our results revealed a comprehensive scientometric analysis of research on GI endoscopy anesthesia/sedation from a global perspective. They may provide valuable clues for future research directions and scientific decision-making in this domain.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation, and the data can be requested from Yujun Xiong whose email is [email protected].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by supported by the National High Level Hospital Clinical Research Funding (2022-GSP-GG-36) and National High Level Hospital Clinical Research Funding (BJ-2021-233), and the funders had no role in the analyses and interpretation of the results or writing of the manuscript.
Disclosure
The authors report no conflicts of interest.
References
1. Daca-alvarez M, Martí M, Spinelli A, et al. Familial component of early-onset colorectal cancer: opportunity for prevention. Br J Surg. 2022;109(12):1319–1325. doi:10.1093/bjs/znac322
2. Zou W-B, Zhang T, He C, et al. A novel portable upper gastrointestinal endoscopy system with complete functions of both diagnosis and treatment. Endoscopy. 2022;55(S 01):E9–E10. doi:10.1055/a-1919-4443
3. Kerrison RS, Sheik-Mohamud D, Mcbride E, et al. Patient barriers and facilitators of colonoscopy use: a rapid systematic review and thematic synthesis of the qualitative literature. Prev Med. 2021;145:106413. doi:10.1016/j.ypmed.2020.106413
4. Min K, Wu Y, Wang S, et al. Developmental trends and research hotspots in bronchoscopy anesthesia: a bibliometric study. Front Med. 2022;9:837389. doi:10.3389/fmed.2022.837389
5. Shafiee H, Riahipour F, Hormati A, et al. Comparison of the sedative effect of ketamine, magnesium sulfate, and propofol in patients undergoing upper gastrointestinal endoscopy: double-blinded randomized clinical trial. CNS Neurol Disord Drug Targets. 2022;22(8):1259–1266.
6. Qin Y, Chen S, Zhang Y, et al. A bibliometric analysis of endoscopic sedation research: 2001–2020. Front Med. 2021;8:775495. doi:10.3389/fmed.2021.775495
7. Vargo JJ. Sedation-related complications in gastrointestinal endoscopy. Gastrointest Endosc Clin N Am. 2015;25(1):147–158. doi:10.1016/j.giec.2014.09.009
8. Rajkomar A, Dean J, Kohane I. Machine learning in medicine. N Engl J Med. 2019;380(14):1347–1358. doi:10.1056/NEJMra1814259
9. Escher JC, Dias JA, Bochenek K, et al. Inflammatory bowel disease in children and adolescents: recommendations for diagnosis - The Porto criteria. J Pediatr Gastroenterol Nutr. 2005;41(1):1–7. doi:10.1097/01.MPG.0000163736.30261.82
10. Bowles CJA, Leicester R, Romaya C, et al. A prospective study of colonoscopy practice in the UK today: are we adequately prepared for national colorectal cancer screening tomorrow? Gut. 2004;53(2):277–283. doi:10.1136/gut.2003.016436
11. Sipe BW, Rex DK, Latinovich D. Propofol versus midazolam/meperidine for outpatient colonoscopy: administration by nurses supervised by endoscopists. Gastrointest Endosc. 2002;55(7):815–825. doi:10.1067/mge.2002.124636
12. Heuss LT, Froehlich F, Beglinger C. Changing patterns of sedation and monitoring practice during endoscopy: results of a nation wide survey in Switzerland. Endoscopy. 2005;37(2):161–166. doi:10.1055/s-2004-826143
13. Rex DK, Heuss LT, Walker JA, Qi R. Trained registered nurses/endoscopy teams can administer propofol safely for endoscopy. Gastroenterology. 2005;129(5):1384–1391. doi:10.1053/j.gastro.2005.08.014
14. Waring JP, Baron TH, Hirota WK. Guidelines for conscious sedation and monitoring during gastrointestinal endoscopy. Gastrointest Endosc. 2003;58(3):317–322. doi:10.1067/S0016-5107(03)00001-4
15. Qadeer MA, Vargo JJ, Khandwala F, et al. Propofol versus traditional sedative agents for gastrointestinal endoscopy: a meta-analysis. Clin Gastroenterol Hepatol. 2005;3(11):1049–1056. doi:10.1016/S1542-3565(05)00742-1
16. Cohen LB, Wecsler JS, Gaetano JN. Endoscopic sedation in the United States: results from a nationwide survey. Am J Gastroenterol. 2006;101(5):967–974. doi:10.1111/j.1572-0241.2006.00500.x
17. Riphaus A, Stergiou N, Wehrmann T. Sedation with propofol for routine ERCP in high-risk octogenarians: a randomized, controlled study. Am J Gastroenterol. 2005;100(9):1957–1963. doi:10.1111/j.1572-0241.2005.41672.x
18. Cohen LB, DeLegge MH, Aisenberg J. AGA Institute review of endoscopic sedation. Gastroenterology. 2007;133(2):675–701. doi:10.1053/j.gastro.2007.06.002
19. K RD, Deenadayalu VP, Eid E, et al. Endoscopist-directed administration of propofol: a worldwide safety experience. Gastroenterology. 2009;137(4):1229–37; quiz 518–9. doi:10.1053/j.gastro.2009.06.042
20. Early DS, Lightdale JR, Vargo JJ. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest Endosc. 2018;87(2):327–337. doi:10.1016/j.gie.2017.07.018
21. Bhatt M, Johnson DW, Chan J, et al. Risk factors for adverse events in emergency department procedural sedation for children. JAMA Pediatr. 2017;171(10):957–964. doi:10.1001/jamapediatrics.2017.2135
22. Vroegop AV, Vanderveken OM, Verbraecken JA. Drug-induced sleep endoscopy: evaluation of a selection tool for treatment modalities for obstructive sleep apnea. Respiration. 2020;99(5):451–457. doi:10.1159/000505584
23. Apfel CC, Roewer N. Ways to prevent and treat pulmonary aspiration of gastric contents. Curr Opin Anaesthesiol. 2005;18(2):157–162. doi:10.1097/01.aco.0000162834.33474.e0
24. Cooper GS, Kou TD, Rex DK. Complications following colonoscopy with anesthesia assistance: a population-based analysis. JAMA Intern Med. 2013;173(7):551–556. doi:10.1001/jamainternmed.2013.2908
25. Barends CRM, Driesens MK, Van amsterdam K, Struys MMRF, Absalom AR. Moderate-to-deep sedation using target-controlled infusions of propofol and remifentanil: adverse events and risk factors: a retrospective cohort study of 2937 procedures. Anesth Analg. 2020;131(4):1173–1183. doi:10.1213/ANE.0000000000004593
26. Leslie K, Allen ML, Hessian EC. Safety of sedation for gastrointestinal endoscopy in a group of university-affiliated hospitals: a prospective cohort. Br J Anaesth. 2017;118(1):90–99. doi:10.1093/bja/aew393
27. Kilic ET, Sayar S, Kahraman R, Kahraman R, et al. The effects of obesity on sedation-related outcomes of advanced endoscopic procedures. North Clin Istanb. 2019;6(4):321–326. doi:10.14744/nci.2019.93763
28. Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. An updated report by the American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non‐Anesthesiologists. Anesthesiology. 2002;96(4):1004–1017. doi:10.1097/00000542-200204000-00031
29. Chutkan R, Cohen J, Abedi M. Training guideline for use of propofol in gastrointestinal endoscopy. Gastrointest Endosc. 2004;60(2):167–172. doi:10.1016/S0016-5107(04)01699-2
30. Goudra B, Singh PM. Airway management during upper GI endoscopic procedures: state of the art review. Dig Dis Sci. 2017;62(1):45–53. doi:10.1007/s10620-016-4375-z
31. Godoroja-Diarto D, Constantin A, Moldovan C, et al. Efficacy and safety of deep sedation and anaesthesia for complex endoscopic procedures-a narrative review. Diagnostics. 2022;12(7):1523. doi:10.3390/diagnostics12071523
32. Manno M, Deiana S, Gabbani T, et al. Implementation of the European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastroenterology and Endoscopy Nurses and Associates (ESGENA) sedation training course in a regular endoscopy unit. Endoscopy. 2021;53(1):65–71. doi:10.1055/a-1197-6762
33. Wang Y, Liu F, Zhang Y, et al. The effect of capnography on the incidence of hypoxia during sedation for EGD and colonoscopy in mildly obese patients: a randomized, controlled study. BMC Anesthesiol. 2023;23(1):188. doi:10.1186/s12871-023-02151-8
34. Nay M-A, Fromont L, Eugene A, et al. High-flow nasal oxygenation or standard oxygenation for gastrointestinal endoscopy with sedation in patients at risk of hypoxaemia: a multicentre randomised controlled trial (ODEPHI trial). Br J Anaesth. 2021;127(1):133–142. doi:10.1016/j.bja.2021.03.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.