Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Global, Regional, and National Burden Trends in Chronic Obstructive Pulmonary Disease Attributable to Particulate Matter Pollution: 1990–2021 and Projections to 2036
Authors Duan H, Li P, Wang Y ![]() , Jiang L
, Jiang L ![]() , Wang Y, Wu W
, Wang Y, Wu W ![]() , Liu X
, Liu X
Received 10 March 2025
Accepted for publication 18 July 2025
Published 1 August 2025 Volume 2025:20 Pages 2671—2683
DOI https://doi.org/10.2147/COPD.S527263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Hongxia Duan,1 Peijun Li,1 Yingqi Wang,1 Linhong Jiang,1 Yide Wang,2 Weibing Wu,3 Xiaodan Liu1
1School of Rehabilitation Science, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Department of Rehabilitation, Fourth Clinical Medical College of Xinjiang Medical University, Xinjiang, People’s Republic of China; 3Department of Sports Medicine, Shanghai University of Sport, Shanghai, People’s Republic of China
Correspondence: Xiaodan Liu, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of death worldwide, of which 41.27% of the burden may be related to particulate matter (PM) pollution. Understanding the PM-related burden of COPD at global, national and regional levels can provide evidence for public health policies.
Methods: First, the numbers of death and disability-adjusted life year (DALY), and the corresponding age-standardized rates were assessed globally and by subtype, including age, sex, sociodemographic index (SDI), country, and region from 1990 to 2021. Second, the temporal trend in disease burden was estimated by joinpoint regression analysis. Furthermore, an international health inequality analysis was used to assess the inequality slope indices and concentration indices, and frontier analysis was performed to explore the current situation and potential improvement of disease burden control. Finally, we constructed an auto regressive integrated moving average model to predict PM-related burden of COPD in the next 15 years.
Results: In 2021, the number of COPD deaths and DALYs attributed to PM were approximately 1.54 million and 33.24 million, respectively. The age-standardized death rate (ASMR) and age-standardized DALY rate (ASDR) were 1.66 and 1.50 times higher in males than in females. Interestingly, the ASMR and ASDR exhibited an increase from 2020 to 2021. The highest COPD burden attributed to PM was in low and low-middle SDI regions. Countries with an SDI between 0.3 and 0.6 had the greatest potential to reduce the COPD burden attributed to PM, especially in Asia, Oceania, and Africa. In the next 15 years, the ASMR and ASDR of COPD attributable to PM for both sexes will decrease, and the difference between male and female patients will be almost nonexistent.
Conclusion: The COPD burden attributable to PM remains a long-term problem globally, especially in males, the older adults, and low and low-middle SDI regions.
Keywords: particulate matter pollution, chronic obstructive pulmonary disease, death, disability-adjusted life year, disease burden, GBD
Graphical Abstract:

Introduction
Chronic obstructive pulmonary disease (COPD), a common respiratory disease, is a major healthcare burden and a cause of morbidity and mortality worldwide.1 The most recent Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 data show that COPD is the fourth leading cause of death worldwide, with a mortality rate of 5.48% (4.96%–5.92%).2 And COPD will remain the third leading cause of death globally by 2050.3 The total direct cost of COPD is 6% of the total health-care budget (38.6 billion Euros annually) and accounts for 56% of the total cost of treating respiratory diseases in the European Union.4 Air pollution has been a major contributor to COPD pathogenesis for many years.5,6 Air pollution includes particulate matter (PM) pollution, ambient ozone pollution, and nitrogen dioxide pollution, among which PM pollution is the largest contributor to COPD. Indeed, most recent estimates suggest that 41.27% of the total attributable risk of COPD may be related to PM pollution.7
PM is a mixture of solid, liquid, and gaseous substances in air, and its sources are mainly of two kinds: anthropogenic activities and natural sources. The close relationship between PM and chronic respiratory diseases is primarily based on the easy deposition of certain particle sizes in the respiratory tract.8 Smaller particles have been suggested to achieve greater total lung deposition, greater distal airway penetration, and greater peripheral lung deposition.9,10 It has been revealed that PM can significantly affect pulmonary surfactants by altering their physiological, biophysical, and morphological properties11 and may also penetrate through the surfactant lining to induce inflammation and oxidative stress on surfactant and epithelial cells, ultimately causing lung injury.12–14 According to the 2023 World Air Quality Report, a total of 124 (92.5%) out of 134 countries and regions exceeded the World Health Organization (WHO) annual PM2.5 guideline value of 5 µg/m3,15 indicating that less than 10% of the world’s countries, areas, and territories breathe air that does not pose a health risk.16 In short, there is still a long way to go to combat PM pollution and ensure environmental equality worldwide.
Understanding the PM pollution-related burden of COPD at global, national and regional levels can provide evidence and directions for environmental control, public health policies and disease prevention and control strategies. Several previous studies have focused on the burden of chronic respiratory diseases or the disease burden attributable to PM pollution in the past decades.17–19 Only a few studies have focused on the burden of COPD attributable to PM pollution, but these studies were limited to a single country or region, and they are somewhat outdated.20,21 To address these gaps, we used the latest GBD 2021 study database to summarize the PM pollution-attributable COPD burden according to age, sex, region, country, and sociodemographic index (SDI).
Methods
Overview
GBD 2021 estimates were given for 371 diseases and injuries; 88 risk factors; 204 countries and territories; 54 GBD regions; 22 GBD super regions; five SDI categories; 25 age groups; females, males, and both sexes combined; and for the years 1990–2021.22,23 The indicators produced by GBD 2021 include deaths, DALYs (quantifying both years lost to premature mortality and years lived with disability (YLDs)), YLDs (quantifying non-fatal health loss), and years of life lost (YLLs; quantifying fatal health loss). Data sources include vital registration and verbal autopsy data, as well as surveys, censuses, surveillance systems, and cancer registries.24 In this study, we used the concept of age-standardized death rate (ASMR), age-standardized DALY rate (ASDR), estimated annual percentage change (EAPC), and SDI, as explained below.
The ASMR represents the number of deaths per 100000 persons after age standardization, and the ASDR represents the YLDs and YLLs per 100000 persons after age standardization. The EAPC can reflect trends in the ASMR/ASDR over specific time intervals.25,26 When the EAPC is positive, then the overall trend is increasing, and a higher absolute value indicates a greater change in the trend. The SDI is a composite indicator of development status that is strongly correlated with health outcomes.27 A location with an SDI of 1 would have a theoretical maximum level of health-related development.
Study Data
All data used in this study were extracted from the GBD 2021 results,2 including the following: (1) Global PM pollution-attributable COPD age- and sex-specific deaths and DALYs, death rates, and DALY rates, from 1990 to 2021; (2) PM pollution-attributable COPD deaths and DALYs, ASMR, and ASDR by 204 countries and territories from 1990 to 2021; (3) PM pollution-attributable COPD sex-specific deaths and DALYs, ASMR, and ASDR by SDI categories from 1990 to 2021; (4) PM pollution-attributable COPD deaths and DALYs, ASMR, and ASDR by 54 GBD regions from 1990 to 2021; and (5) PM pollution-attributable COPD deaths and DALYs, ASMR, and ASDR by 22 GBD super regions. The PM pollution-attributable COPD burden in the population younger than 25 years was almost zero, so we divided the population aged over 25 years into 15 groups: 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, and 95+ years of age.
Statistical Analysis
First, the COPD deaths and DALY number, ASMR, and ASDR attributable to PM pollution were reported globally and by different sub-types, including age, sex, SDI, countries, and regions, from 1990 to 2021. Second, the corresponding EAPC values from 1990 to 2021 were estimated using the linear regression model. Third, joinpoint regression analysis was performed to obtain the annual percentage change (APC) in the ASMR and ASDR of COPD attributable to PM pollution at the global level for both males and females, which is one of the most effective methods for studying disease time trends.28 In addition, an international health inequality analysis29 was used to assess the inequality slope indices and concentration indices for deaths and DALYs of COPD attributable to PM pollution from 1990 to 2021 worldwide. Frontier analysis30 was performed to explore the current situation and potential improvement in disease burden control in each country under the SDI conditions for each year. Finally, we constructed an auto-regressive integrated moving average (ARIMA) model31 to predict disease burden between 2021 and 2036. Joinpoint 5.2.0 and R 4.4.1 software were used for database construction, collation, and analysis. A P-value < 0.05 was considered statistically significant.
Results
COPD Burden Attributable to PM Pollution Globally from 1990 to 2021
In 2021, the numbers of COPD deaths and DALYs attributed to PM pollution were approximately 1.54 million [95% uncertainty intervals (UI): 1.21–1.92] and 33.24 million (95% UI: 26.68–41.34), respectively, accounting for 41.27% of all deaths and 41.66% of all DALYs of COPD. The corresponding ASMR and ASDR values were 18.51 (95% UI: 14.64–23.13) and 389.5 (95% UI: 312.59–484.62) per 100,000 population, respectively (Table 1). The number of deaths and DALYs were 1.28 and 1.26 times higher in males than in females, and the corresponding ASRs (ASMR and ASDR) were 1.66 and 1.50 times higher, respectively (Table 1). The global burden of COPD attributable to PM pollution across age and sex groups separately in 2021 is shown in Figure 1.
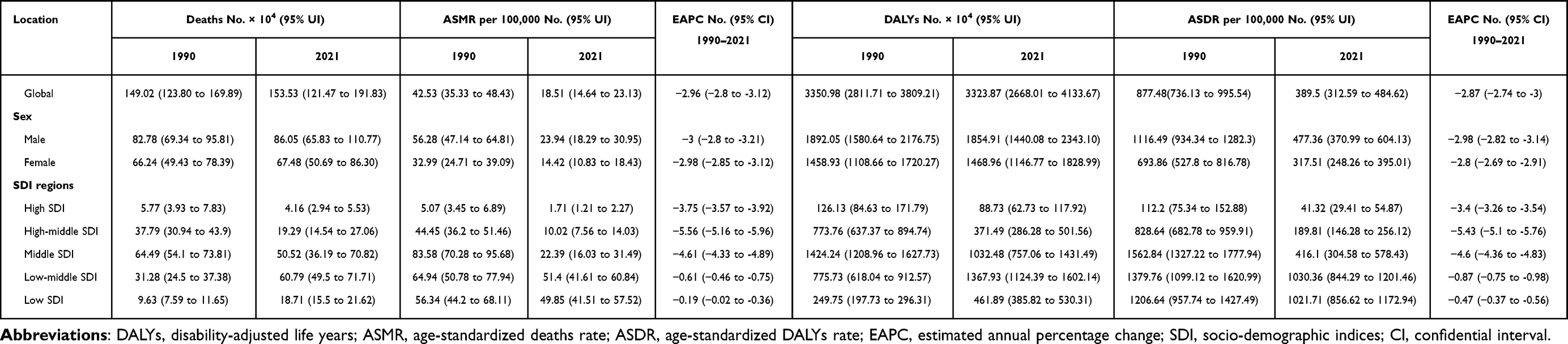 |
Table 1 COPD Deaths and DALYs, ASMR and ASDR Attributable to PM Pollution Globally, and by Sex, SDI Regions, and Its EAPC from 1990 to 2021 |
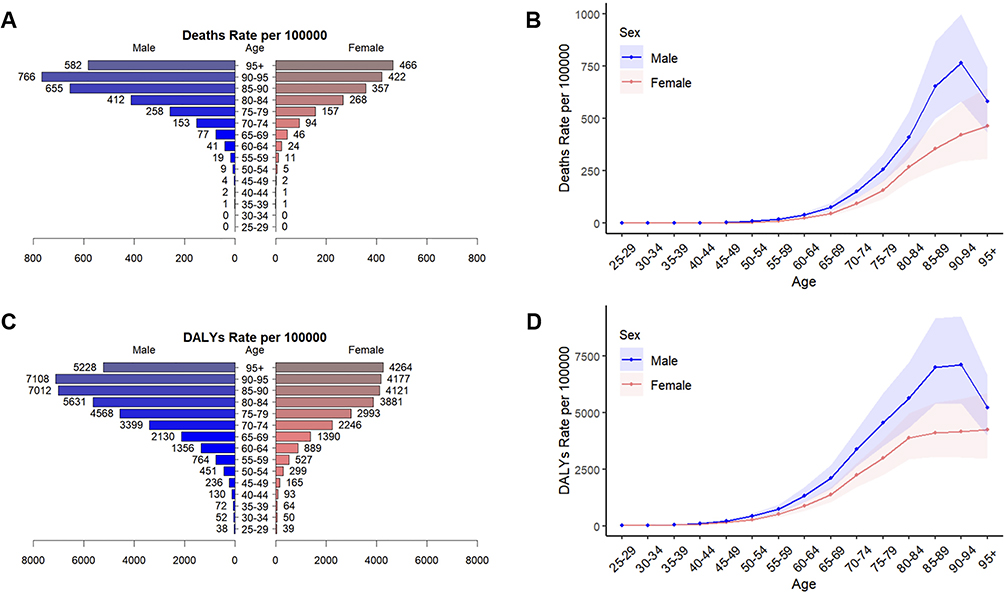 |
Figure 1 Global burden of COPD attributable to PM pollution among different sexes and ages in 2021. (A–B) ASMR of COPD attributable to PM pollution, (C-D) ASDR of COPD attributable to PM pollution. Abbreviations: COPD, chronic obstructive pulmonary disease; PM, particulate matter; DALY, disability-adjusted life year; ASMR, age-standardized death rate; ASDR, age-standardized DALY rate. |
Globally, the ASRs for deaths and DALYs exhibited a continuous downward trend from 1990 to 2021 [(ASMR: 1990−1995 APC = −0.60; 1995−2004 APC = −2.32; 2004−2007 APC = −5.08; 2007−2016 APC = −2.98; 2016−2019 APC = −4.90), (ASDR: 1990−1995 APC = −0.87; 1995−2004 APC = −2.41; 2004−2007 APC = −4.34; 2007−2021 APC = −3.11)]. Similarly, the ASRs for deaths and DALYs showed a persistent downward trend in both males and females. It is worth noting that there was an increase in males and females from 2020 to 2021 (Figure A.1 and Table A.1).
COPD Burden Attributed to PM Pollution by SDI Categories from 1990 to 2021
In 2021, the low-middle SDI region had the highest number of deaths at 607,910 and DALYs at 13,679,316, and the highest ASRs also occurred in the low-middle SDI region (Table 1 and Figure 2). For males, the highest ASRs were observed in the low-middle SDI region, followed by those in the low SDI, whereas for females, the highest ASRs were observed in the low SDI region, followed by the low-middle SDI region (Figure 2 and Table A.2).
 |
Figure 2 Change trends in the ASMR and ASDR of COPD attributable to PM pollution by SDI regions for both, males and females from 1990 to 2021. (A–C) ASMR of COPD attributable to PM pollution, (D–F) ASDR of COPD attributable to PM pollution. Abbreviations: COPD, chronic obstructive pulmonary disease; PM, particulate matter; DALY, disability-adjusted life year; ASMR, age-standardized death rate; ASDR, age-standardized DALY rate. |
From 1990 to 2021, the ASMR and ASDR of COPD attributed to PM pollution showed a declining trend in all SDI regions; the percentage change was the largest in the high-middle SDI region, and the absolute change was the largest in the middle SDI region (Figure 2 and Table A.2). In the high-SDI, low-middle-SDI, and low-SDI regions, the downward trend of ASRs was higher in females than in males. However, a reverse trend was observed in the high-middle SDI and middle SDI regions (Table A.2). Notably, there was an increase in the high-middle SDI, middle SDI, and low-middle SDI regions for males and females from 2020 to 2021 (Figure 2).
Additionally, there was an adaptive association between ASRs and SDI. The ASRs for deaths and DALYs showed an inverted “U” relationship with SDI, with the rate exhibiting a gradual increase when the SDI was <0.4 but a decrease after the SDI became >0.4 and a slow decrease when the SDI was >0.7 (Figure A.2).
COPD Burden Attributed to PM Pollution by Country and Region
In 2021, the highest numbers of COPD deaths and DALYs attributed to PM pollution were observed in India (deaths: 651,899.64, 95% UI: 531,634.17–778,203.14; DALYs: 14,540,058.44, 95% UI: 11,973,481.80–17,162,069.56), followed by China and Bangladesh. As for the corresponding ASRs, the country with the highest ASRs was Papua New Guinea (ASMR: 106.04, 95% UI: 77.11–136.03; ASDR: 2015.1, 95% UI: 1497.62–2565.92), followed by Nepal and the Democratic People’s Republic of Korea. The lowest ASRs for both deaths and DALYs were observed in Finland (ASMR: 0.17, 95% UI: 0.02–0.37; ASDR: 4.40, 95% UI: 0.63–9.59), followed by Estonia and Iceland (Figure 3 and Table A.3).
 |
Figure 3 COPD deaths and DALY number, ASMR, and ASDR attributable to PM pollution globally, by different countries and territories in 2021. (A) Deaths number of COPD attributable to PM pollution, (B) ASMR of COPD attributable to PM pollution, (C) DALYs number of COPD attributable to PM pollution, (D) ASDR of COPD attributable to PM pollution. Abbreviations: COPD, chronic obstructive pulmonary disease; PM, particulate matter; DALY, disability-adjusted life year; ASMR, age-standardized death rate; ASDR, age-standardized DALY rate. |
In 2021, across the 54 GBD regions, Asia had the highest number of deaths and DALY cases (deaths: 1,391,256.98, 95% UI: 1,102,884.05–1,738,830.18; DALYs: 29,470,959.98, 95% UI: 23,749,777.24–36,544,637.12), followed by the World Bank Lower Middle Income and Limited Health System. The region with the highest ASRs was Oceania (ASMR: 75.80, 95% UI: 55.55–96.04; ASDR: 1,494.73, 95% UI: 1,120.13–1,893.97), followed by South Asia and South Asia – WB. The region with the lowest ASMR was the high-income Asia Pacific (0.91, 95% UI: 0.52–1.38), whereas the country with the lowest ASDR was Australasia (21.84, 95% UI: 12.67–31.31) (Table A.4).
From 1990 to 2021, the EAPC of COPD ASMR attributable to PM pollution was positive in 5.88% of countries and territories, indicating an overall upward trend in 12 of 204 countries, and the top three countries with increasing death burden were Antigua and Barbuda, Libya, and Georgia (Table A.3). Additionally, the EAPC of COPD ASDR attributable to PM pollution was positive in 5.88% of countries and territories, and the top three countries with increasing DALY burden were Antigua and Barbuda, Lesotho, and Libya (Table A.3).
Health Inequality Analysis
The slope index of COPD deaths attributable to PM pollution increased slightly from −7.93 (95% C1: −10.05 to −5.80) in 1990 to −5.76 (95% C1: −6.91 to −4.62) in 2021, and the concentration index decreased from 0.25 in 1990 to 0.18 in 2021 (Figure A.3). Similarly, the slope index of COPD DALYs attributable to PM pollution increased slightly from −236.21 (95% C1: −288.18 to −184.25) in 1990 to −186.34 (95% C1: −215.87 to −156.81) in 2021, and the concentration index decreased from 0.26 in 1990 to 0.22 in 2021 (Figure A.3).
Frontier Analysis of the Association Between ASRs of PM Pollution-Associated COPD and SDI
The results of the frontier analysis based on the ASMR and ASDR for COPD attributed to PM pollution were consistent. The 15 countries furthest from the frontier fit line include Papua New Guinea, Nepal, Democratic People’s Republic of Korea, India, Myanmar, Vanuatu, Lesotho, the Solomon Islands, Pakistan, Kiribati, Bangladesh, Madagascar, Samoa, Lao People’s Democratic Republic, Sao Tome and Principe. The five countries closest to the frontier fit line in the lower SDI countries were Burkina Faso, Somalia, Niger, Mozambique, and Djibouti. The five countries furthest from the frontier fit line in the higher SDI countries were the Republic of Korea, Taiwan (Province of China), the Netherlands, Denmark, and the United Kingdom (Figure 4). Notably, only Lesotho showed an increase in the burden of ASMR and ASDR from 1990 to 2021.
 |
Figure 4 Frontier analysis based on the ASMR and ASDR of COPD attributable to PM pollution and SDI in 204 countries and territories. (A–B) ASMR of COPD attributable to PM pollution, (C–D) ASDR of COPD attributable to PM pollution. The solid black line is the frontier, and the dots represent countries and territories. Black fonts represent the 15 countries and territories with the largest effective difference (e.g., Papua New Guinea, Nepal, Democratic People's Republic of Korea). Blue fonts represent the 5 frontier countries and territories with low-SDI (<0.5) and low effective difference (e.g., Burkina Faso, Somalia, Niger), and red fonts represent the 5 countries and territories with high–SDI (>0.85) and relatively high effective difference [e.g., Korea, Taiwan (Province of China), the Netherlands]. Overall, the greater the effective difference (where the distance between the solid black line and the dots is far), the greater the potential for improving the disease burden. This result indicates that countries with SDI ranging from 0.2 to 0.6 have greater potential for improving COPD burden attributed to PM. Abbreviations: COPD, chronic obstructive pulmonary disease; PM, particulate matter; DALY, disability–adjusted life year; ASMR, age–standardized death rate; ASDR, age–standardized DALY rate; SDI, socio–demographic index. |
Predicted Results from 2021 to 2036
The predicted results of the ARIMA model showed that the ASMR and ASDR of COPD attributable to PM pollution for both sexes will decrease from 2021 to 2036. When predicting the ASMR, for males and females, the ARIMA(0, 1, 1) and ARIMA(0, 1, 1) models were selected, respectively, with AIC values of 69.26 and 26.85, AICc values of 70.15 and 27.74, and BIC values of 73.56 and 31.15, respectively. The global ASMR of males and females was projected to decrease by 57.56% (2036: 10.16, 95% CI: 2.21 to 18.11) and 54.99% (2036: 6.49, 95% CI: 2.49 to 10.50), respectively, and the difference between males and females was expected to decrease slightly. When predicting the ASDR, for males and females, the ARIMA(0, 1, 0) and ARIMA(1, 1, 0) models were selected, respectively, with AIC values of 241.43 and 207.69, AICc values of 241.86 and 208.58, and BIC values of 244.3 and 212, respectively. The global ASDR of males and females is projected to decrease by 64.79% (2036: 168.10, 95% CI: 82.13 to 254.08) and 47.36% (2036: 167.14, 95% CI: 81.23–253.05), respectively, and the difference between males and females is expected to be almost nonexistent (Figure 5 and Table A.5).
 |
Figure 5 Projections of the ASMR and ASDR of COPD attributable to PM pollution by 2036 based on the ARIMA model. (A–B) ASMR of COPD attributable to PM pollution, (C–D) ASDR of COPD attributable to PM pollution. Red lines represent the true trend of ASMR and ASDR of COPD attributable to PM pollution during 1990-2021; yellow dot lines and shaded regions represent the predicted trend and its 95% C1. Abbreviations: COPD, chronic obstructive pulmonary disease; PM, particulate matter; DALY, disability-adjusted life year; ASMR, age-standardized death rate; ASDR, age-standardized DALY rate; CI, confidence interval. |
Discussion
To the best of our knowledge, this is the first study to comprehensively assess and quantify the PM pollution-attributable COPD burden by age, sex, region, country, and SDI at the global level and then predict the future tendency of the disease burden. Using the latest GBD dataset, our study revealed several significant findings. (1) Globally, the COPD burden attributed to PM pollution has shown a downward trend from 1990 to 2021. Males and older adults remain high-risk populations. (2) The disease burden was significantly controlled in high-middle SDI and middle SDI regions. However, more attention should be paid to low and low-middle SDI regions, especially in countries with SDI less than 0.4. While pursuing economic development, positive measures should also be taken to balance the negative effects of environmental pollution on public health. (3) Antigua and Barbuda, Libya, Lesotho, these countries with a majority of African ethnicity, saw an increase in disease burden from 1990 to 2021. Now, Asia had the highest number of deaths and DALY cases, especially in India and China; Oceania has the highest ASRs, especially in Papua New Guinea.
The elderly male population remains the main group contributing to the disease burden of COPD attributable to PM pollution. The sex difference in COPD is consistently common, owing to congenital genetic susceptibility, acquired living habits, and other factors. Smoke is an important source of indoor PM. Although the lungs of females are more susceptible to smoking,32 the proportion and number of pack-years of smoking are much higher in males,33 resulting in a much heavier burden of COPD in males. Many human production activities, such as construction, fuel, factory dust, textiles, welding, and transportation, are important sources of PM.34 There is direct evidence that long-term exposure to different sizes and concentrations of PM is associated with lung function differently between sexes,35 which is consistent with the results of this study. More precisely, in north China, each 5 μg/m3 increase in PM2.5 and PM10 was associated with decreases in forced vital capacity (FVC) of 54.6 mL and 42.9 mL among males and of 38.7 mL and 31.1 mL among females, respectively. However, among the Indian population exposed to PM pollution, females had a higher prevalence of obstructive respiratory abnormalities than males.36 These different findings may be due to sex differences in the susceptibility to PM pollution from different sources37 and sex,38 region, or race differences39 in disease knowledge and awareness of medical treatment, which deserve further investigation in the future.
Since 1990, the ASMR and ASDR of COPD attributable to PM pollution have shown a significant downward trend in high-middle and middle SDI regions, indicating that PM pollution optimization policies and COPD management measures have achieved obvious effects and that people’s health awareness has increased in these regions. The frontier analysis identified the minimum disease burden that could be achieved at different SDI levels; this suggests that there are several countries, ie, those identified as having actual disease burdens that are higher than their potential minimum disease burdens, that can still improve the burden of COPD attributable to PM pollution by optimizing policies and resource allocation. Oceania had the highest disease burden worldwide, but the concentrations of PM2.5 and PM10 in Oceania were not more than 50% globally,40 suggesting that efforts to improve the disease burden should focus on the popularization of health-care services and the improvement of patient health awareness and COPD management. South Asia had the second highest disease burden globally, which may be related to the high concentration of PM2.5, low economic level, and lack of medical resources. In 2021, the top three cities with the highest PM2.5 concentration were Bangladesh, Pakistan, and India,41 all of which belong to South Asia, and this PM2.5 concentration far exceeded (by 10 times) the WHO standard,42 suggesting that reducing solid fuels such as municipal coal and wood for heating and using cleaner gas or liquid fuels is necessary and that a greater allocation of health-care resources toward low-income countries may also be an effective measure.
Health inequities, defined as disparities in access to health-care resources driven by social determinants,43 are particularly evident among COPD patients who reside in rural areas, belong to marginalized communities, have lower socioeconomic status, or live alone.44,45 These groups often experience delays in accessing timely and effective treatment and disease management. Between 1990 and 2021, the slope and concentration indexes for deaths and DALYs with PM pollution-attributable COPD showed modest global improvements. However, significant gaps remain, particularly in underserved populations. Integrating artificial intelligence (AI) technologies into the prediction, early warning, clinical decision-making, treatment, and rehabilitation management of COPD offers innovative solutions. For example, AI-driven tools like EBCare,46 a wearable smart mask that monitors breath condensation and analyzes biomarkers in exhaled air, are expected to offer a more sensitive, convenient and low-cost alternative to traditional spirometry for early warning, diagnosis, and disease monitoring. Additionally, AI can optimize resource allocation by predicting high-risk areas for PM pollution exposure and identifying vulnerable populations based on socioeconomic factors enabling targeted interventions.47,48 AI-powered telemedicine platforms further bridge healthcare access gaps by providing remote consultations and virtual diagnostics for underserved populations.49 By leveraging AI technologies, policymakers and health-care providers can implement equitable strategies to reduce the burden of PM pollution-attributable COPD. These innovations enhance early detection, timely intervention, and sustainable health-care solutions, ultimately contributing to global efforts to address health disparities and achieve universal health coverage.
Projected trends over the next 15 years suggested a sustained decline in the ASMR and ASDR of COPD attributed to PM pollution, with diminishing gender disparities. This positive trajectory reflects advancements in air quality regulations, healthcare accessibility, and awareness of environmental health risks in the future. Despite projected improvements in COPD burden, climate risks and energy emissions, which are closely linked to air pollution events,50 have shown worrying trends in recent years. According to the 2024 report of the Lancet Countdown on health and climate change, global climate change manifests through extreme weather events (eg, heatwaves, prolonged dry spells), posing unprecedented threats to human health worldwide.51 These extreme weather events elevated PM concentrations through dust storms. Additionally, in 2023, global energy-related carbon emissions did not decline, but reached an all-time high, indicating that reliance on fossil fuels remains unchanged.51 Therefore, climate action, energy choices, and end-control of pollution will be critical strategies in future decades, particularly in developing countries. Notably, socio-demographic factors, such as aging populations and declining baseline mortality rates, have emerged as more significant determinants than pollution exposure levels in shaping future health burdens.52 Consequently, proactive responses to aging populations through improving socio-economic conditions, and improving COPD healthcare equity, accessibility, and continuity will also be essential strategies for reducing the disease burden, especially in low- and middle-income countries. Although the ARIMA model is a powerful predictive tool, it relies on the stationarity assumption. As the prediction time span extends, uncertainty significantly increases, and it may fail to capture sudden changes or new influencing factors (such as major public health events, the rapid development of artificial intelligence technology, etc.) in a timely manner, all of which may affect the accuracy of the model’s predictions.
Despite the numerous findings on the COPD burden attributed to PM pollution, this study still has some limitations. Firstly, regarding data sources, this study primarily relies on the GBD estimates.53 However, disparities in medical standards, diagnostic criteria, and data collection capabilities across countries may compromise the quality of the GBD data. Additionally, the GBD study employed modeling techniques to estimate missing data, which inevitably introduces a degree of uncertainty. Secondly, concerning research methodology, as the GBD data was from observational study, the causal relationship between PM pollution and COPD cannot be regarded as absolute, only under specific hypothetical conditions. Furthermore, this article focuses on analyzing the impact of various factors, including age, sex, SDI, country, and region, on the COPD burden attributable to PM pollution, but does not account for other potential influencing factors, such as racial differences and genetic predispositions. Third, the PM pollution in the GBD database presents overall data without refinement of PM categories (eg, PM1, PM2.5, and PM10) and sources, so it is unclear whether the age and sex differences in COPD burden attributable to PM pollution are related to different PM particle sizes and different sources. Fourth, the GBD database covers 204 countries and territories, but the COPD burden attributed to PM pollution by provinces, cities, and towns could not be obtained. Fifth, in low SDI regions, the disease burden might be underestimated because of underdiagnosis of COPD due to limited equipment and supply for spirometry, limited financial and human resources, limited access to training and trained technicians, poor resident poverty, and lack of education.54 Nevertheless, compared with all sources, the data from the GBD study is the most comprehensive and standardized because it leverages the expertise of over 11,000 collaborators and uses improved methods to update the full time series estimates from 1990 to 2021.23
Conclusion
In conclusion, the COPD burden attributed to PM pollution has demonstrated a decline trend, but significant health inequities persist. Males, older adults, and populations in low SDI regions are high-risk groups for PM pollution-attributable COPD burden and deserve focused attention and targeted prevention and treatment. So, governments must implement region-specific strategies encompassing climate action, energy transition, precision exposure control, AI-powered COPD wearables, and telemedicine networks to sustainably mitigate related disease burdens from compounding environmental risks and COPD burden.
Highlights
- This study presents the latest results on the PM pollution-attributable COPD burden by age, sex, region, country, and SDI at the global level and then predicts trends over the next 15 years.
- At the SDI level, the relationship between ASRs and SDI showed an inverted “U” shape, with a peak at SDI = 0.4.
- Males and older adults are at high risk for PM pollution-caused COPD deaths and DALYs.
- India, China, and Bangladesh have the greatest number of deaths and DALYs.
- Oceania, South Asia, and Africa have the greatest potential to reduce PM pollution-caused COPD.
Data Statement
Data will be made available on request.
Ethics Statement
Not applicable. The human data involved in this study were from a public database named Global Burden of Disease Study (GBD) 2021 (https://www.healthdata.org/), in which the data is open and anonymous. It conforms to item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China. Based on this, ethical approval can be exempted.
Acknowledgments
We thank LetPub (www.letpub.com.cn) for its linguistic assistance during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Discipline Leader Project of Shanghai Municipal Health Commission (grant number 2022XD044), the National Natural Science Foundation of China (grant number 82372573, 82072551, 82172551).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
2. Global Burden of Disease Collaborative Network. 2022. Global burden of disease study 2021 (GBD 2021) results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), https://vizhub.healthdata.org/gbd-results/.
3. GBD. 2021 forecasting collaborators. Lancet. 2024;403(10440):2204–2256. doi:10.1016/S0140-6736(24)00685-8
4. Forum of International Respiratory Societies. The global impact of respiratory disease. Third edition. European Respiratory Society, 2021. https://firsnet.org/publication/the-global-impact-of-respiratory-disease-3rd-edition/.
5. Global lnitiative for Chronic Obstructive Lung Disease. 2024. Global strategy for prevention, diagnosis and management of COPD: 2024 report. https://goldcopd.org/2024-gold-report/.
6. Sin DD, Doiron D, Agusti A. Air pollution and COPD: GOLD 2023 committee report. Eur Respir J. 2023;61(5):2202469. doi:10.1183/13993003.02469-2022
7. Institute for Health Metrics and Evaluation. 2024. GBD Compare—Viz Hub. https://vizhub.healthdata.org/gbd-compare/.
8. Brain JD, Valberg PA. Deposition of aerosol in the respiratory tract. Am Rev Respir Dis. 1979;120(6):1325–1373. doi:10.1164/arrd.1979.120.6.1325
9. Usmani OS, Biddiscombe MF, Barnes PJ. Regional lung deposition and bronchodilator response as a function of β2-agonist particle size. Am J Respir Crit Care Med. 2005;172(12):1497–1504. doi:10.1164/rccm.200410-1414OC
10. Cormier SA, Lomnicki S, Backes W, Dellinger B. Origin and health impacts of emissions of toxic by-products and fine particles from combustion and thermal treatment of hazardous wastes and materials. Environ Health Perspect. 2006;14(6):810–817. doi:10.1289/ehp.8629
11. Wang F, Liu J, Zeng H. Interactions of particulate matter and pulmonary surfactant: implications for human health. Adv Colloid Interface Sci. 2020;284:102244. doi:10.1016/j.cis.2020.102244
12. Barbier E, Carpentier J, Simonin O, et al. Oxidative stress and inflammation induced by air pollution-derived PM2.5 persist in the lungs of mice after cessation of their sub-chronic exposure. Environ Int. 2023;181:108248. doi:10.1016/j.envint.2023.108248
13. Hou T, Zhu L, Wang Y, Peng L. Oxidative stress is the pivot for PM2.5-induced lung injury. Food Chem Toxicol. 2024;184:114362. doi:10.1016/j.fct.2023.114362
14. Kaur M, Chandel J, Malik J, Naura AS. Particulate matter in COPD pathogenesis: an overview. Inflamm Res. 2022;71(7–8):797–815. doi:10.1007/s00011-022-01594-y
15. IQAir. 2024. 2023 world air quality report. https://www.iqair.com/us/world-air-quality-report.
16. Wise J. Pollution: 90% of world population breathes air that exceeds WHO targets on particulate matter. BMJ. 2023;380:615. doi:10.1136/bmj.p615
17. GBD. 2015 chronic respiratory disease collaborators. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X
18. GBD. Chronic respiratory disease collaborators. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
19. Sang S, Chu C, Zhang T, Chen H, Yang X. The global burden of disease attributable to ambient fine particulate matter in 204 countries and territories, 1990–2019: a systematic analysis of the Global Burden of Disease Study 2019. Ecotoxicol Environ Saf. 2022;238:113588. doi:10.1016/j.ecoenv.2022.113588
20. Cheng XF, Min SH, Guo RQ, Zhang JD, Zhang YL, Li B. Disease burden of COPD attributable to PM2. 5 in China, Japan and South Korea from 1990 to 2019: a comparative study based on Global Burden of Disease Study 2019. BMJ Open. 2024;14(2):e078887. doi:10.1136/bmjopen-2023-078887
21. Su X, Li H, Li F, et al. Trends in the Burden of COPD Attributable to Ambient PM2.5 Exposure in China 1990−2019: an Age-Period-Cohort Analysis. Risk Manag Healthc Policy. 2023;16:69–77. doi:10.2147/RMHP.S395278
22. GBD. 2021 diseases and injuries collaborators. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
23. GBD. 2021 risk factors collaborators. Lancet. 2024;403(10440):2162–2203. doi:10.1016/S0140-6736(24)00933-4
24. GBD. 2021 causes of death collaborators. Lancet. 2024;403(10440):2100–2132. doi:10.1016/S0140-6736(24)00367-2
25. Hankey BF, Ries LA, Kosary CL, et al. Partitioning linear trends in age-adjusted rates. Cancer Causes Control. 2000;11(1):31–35. doi:10.1023/a:1008953201688
26. Li HY, Gao TY, Fang W, et al. Global, regional and national burden of chronic obstructive pulmonary disease over a 30-year period: estimates from the 1990 to 2019 Global Burden of Disease Study. Respirology. 2023;28(1):29–36. doi:10.1111/resp.14349
27. Global Burden of Disease Collaborative Network. 2024. Global burden of disease study 2021(GBD 2021) socio-demographic index (SDI) 1950–2021. Seattle, United States of America: institute for health metrics and evaluation (IHME) https://ghdx.healthdata.org/record/global-burden-disease-study-2021-gbd-2021-socio-demographic-index-sdi-1950%E2%80%932021.
28. Chen J, Cui Y, Deng Y, et al. Global, regional, and national burden of cancers attributable to particulate matter pollution from 1990 to 2019 and projection to 2050: worsening or improving? J Hazard Mater. 2024;477:135319. doi:10.1016/j.jhazmat.2024.135319
29. World Heath Organization. 2022. Handbook on health inequality monitoring with a special focus on low- and middle-income countries. https://www.who.int/publications/i/item/9789241548632.
30. Bai Z, Wang H, Shen C, An J, Yang Z, Mo X. The global, regional, and national patterns of change in the burden of nonmalignant upper gastrointestinal diseases from 1990 to 2019 and the forecast for the next decade. Int J Surg. 2024;111(1):80–9.
31. Qin X, Chen L, Yuan X, et al. Projecting trends in the disease burden of adult edentulism in China between 2020 and 2030: a systematic study based on the global burden of disease. Front Public Health. 2024;12:1367138. doi:10.3389/fpubh.2024.1367138
32. Sørheim IC, Johannessen A, Gulsvik A, Bakke PS, Silverman EK, DeMeo DL. Gender differences in COPD: are women more susceptible to smoking effects than men? Thorax. 2010;65(6):480–485. doi:10.1136/thx.2009.122002
33. Grydeland TB, Dirksen A, Coxson HO, et al. Quantitative computed tomography: emphysema and airway wall thickness by sex, age and smoking. Eur Respir J. 2009;34(4):858–865. doi:10.1183/09031936.00167908
34. Zhang M, Liu S, Yang L, et al. Prevalence of Smoking and Knowledge About the Hazards of Smoking Among 170 000 Chinese Adults, 2013–2014. Nicotine Tob Res. 2019;21(12):1644–1651. doi:10.1093/ntr/ntz020
35. Liu Q, Pan L, Yang T, et al. Association between long-term exposure to ambient particulate matter and pulmonary function among men and women in typical areas of South and North China. Front Public Health. 2023;11:1170584. doi:10.3389/fpubh.2023.1170584
36. Kesavachandran CN, Bihari V, Pangtey BS, Kamal R, Singh A, Srivastava AK. Gender Disparity in Lung Function Abnormalities among a Population Exposed to Particulate Matter Concentration in Ambient Air in the National Capital Region, India. J Health Pollut. 2015;5(9):47–60. doi:10.5696/2156-9614-5-9.47
37. Harch EL, Garcia-Larsen I, Benmaamar V, et al. Association between biomass exposure and COPD occurrence in Fez, Morocco: results from the BOLD study. BMJ Open Respir Res. 2024;11(1):e002409. doi:10.1136/bmjresp-2024-002409
38. Sugiyama K, Tomata Y, Takemi Y, et al. [Awareness and health consciousness regarding the national health plan “Health Japan 21” (2nd edition) among the Japanese population in 2013 and 2014]. Nihon Koshu Eisei Zasshi. 2016;63(8):424–431. doi:10.11236/jph.63.8_424 Serbian
39. Pal A, Howarth TP, Rissel C, et al. COPD disease knowledge, self-awareness and reasons for hospital presentations among a predominately Indigenous Australian cohort: a study to explore preventable hospitalisation. BMJ Open Respir Res. 2022;9(1):e001295. doi:10.1136/bmjresp-2022-001295
40. IQAir. 2024. IQAir Map. https://www.iqair.cn/cn/earth.
41. IQAir. 2024. Historic air quality data (2017-2023). https://www.iqair.com/ca/world-most-polluted-countries.
42. World Health Organization.WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide. Geneva: World Health Organization; 2021. PMID: 34662007.
43. Gkiouleka A, Huijts T, Beckfield J, Bambra C. Understanding the micro and macro politics of health: inequalities, intersectionality & institutions - A research agenda. Soc Sci Med. 2018;200:92–98. doi:10.1016/j.socscimed.2018.01.025
44. Pleasants RA, Riley IL, Mannino DM. Defining and targeting health disparities in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2016;11:2475–2496. doi:10.2147/COPD.S79077
45. Sansgiry SS, Bhansali A, Serna O, et al. Effect of coverage gap on healthcare utilization among Medicare beneficiaries with chronic obstructive pulmonary disorder. Curr Med Res Opin. 2019;35(2):321–328. doi:10.1080/03007995.2018.1495622
46. Heng W, Yin S, Min J, et al. A smart mask for exhaled breath condensate harvesting and analysis. Science. 2024;385(6712):954–961. doi:10.1126/science.adn6471
47. Dai H, Liu Y, Wang J, et al. Large-scale spatiotemporal deep learning predicting urban residential indoor PM2.5 concentration. Environ Int. 2023;182:108343. doi:10.1016/j.envint.2023.108343
48. Aguilera R, Luo N, Basu R, et al. A novel ensemble-based statistical approach to estimate daily wildfire-specific PM2.5 in California (2006–2020). Environ Int. 2023;171:107719. doi:10.1016/j.envint.2022.107719
49. Li X, Zhou HP, Zhou ZJ, et al. Artificial intelligence-powered remote monitoring of patients with chronic obstructive pulmonary disease. Chin Med J. 2021;134(13):1546–1548. doi:10.1097/CM9.0000000000001529
50. Yim SHL, Li Y, Huang T, et al. Global health impacts of ambient fine particulate pollution associated with climate variability. Environ Int. 2024;186:108587. doi:10.1016/j.envint.2024.108587
51. Romanello M, Walawender M, Hsu SC, et al. The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action. Lancet. 2024;404(10465):1847–1896. doi:10.1016/S0140-6736(24)01822-1
52. Yang H, Huang X, Westervelt DM, Horowitz L, wei P. Socio-demographic factors shaping the future global health burden from air pollution. Nat Sustainability. 2023;6(1):58–68. doi:10.1038/s41893-022-00976-8
53. GBD. 2021 demographics collaborators. Lancet. 2024;403(10440):1989–2056. doi:10.1016/S0140-6736(24)00476-8
54. Alupo P, Baluku J, Bongomin F, et al. Overcoming challenges of managing chronic obstructive pulmonary disease in low-and middle-income countries. Expert Rev Respir Med. 2024;16:1–10.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.