Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 16
Global Patterns, Temporal Trends, and Potential Non-Infectious Risk Factors for Burkitt Lymphoma from 1990 to 2021
Authors Jin SK, Lyu JT, Feng ZY, Zhang SQ, Lu BY, Yan QF, Li J, Du J, Huang ZF
Received 27 July 2025
Accepted for publication 6 December 2025
Published 8 January 2026 Volume 2026:16 556459
DOI https://doi.org/10.2147/BLCTT.S556459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Shi-Kai Jin,1,* Jun-Ting Lyu,2,* Zi-Yu Feng,1 Shu-Qi Zhang,1 Bin-Yan Lu,1 Qin-Fu Yan,3 Jing Li,3 Jun Du,4 Zou-Fang Huang5
1Department of Clinical Medicine, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China; 2Department of Hematology, Zhuhai Hospital of Integrated Traditional Chinese and Western Medicine, Zhuhai, 519000, People’s Republic of China; 3Department of Clinical Medicine, School of the First Clinical Medicine, Gannan Medical University, Ganzhou, Jiangxi, 341000, People’s Republic of China; 4Department of Hematology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200127, People’s Republic of China; 5Department of Hematology, The Second Affiliated Hospital of Shenzhen University, The People’s Hospital of Baoan, Shenzhen, Guangdong 518101, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zou-Fang Huang, Department of Hematology, The Second Affiliated Hospital of Shenzhen University, The People’s Hospital of Baoan Shenzhen, Shenzhen, Guangdong, 518101, People’s Republic of China, Email [email protected] Jun Du, Department of Hematology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China, Email [email protected]
Background: The heterogeneity in the health burden and non-infectious risk factors of Burkitt lymphoma (BL) across sex, age, and geographic distribution remain inadequately understood.
Methods: Based on Global Burden of Disease study 2021, we estimate the health burden of BL from four metrics: incidence, mortality, prevalence, and disability-adjusted life years. Subgroups were stratified by age, sex, region, and socio-demographic index (SDI). Joinpoint regression was used to evaluate the average annual percentage change (AAPC) to quantify trends in the health burden. Predictions were performed using the Bayesian age-period-cohort model. Non-infectious risk factors were identified and analyzed utilizing summary exposure values (SEVs) to assess their impact on BL incidence and mortality.
Results: The estimated global incident number of BL was 19,073 (95% CI: 9651 to 32,509) in 2021, nearly threefold that of 1990. The health burden of BL was markedly higher in males than females, especially among individuals aged under 20 years. From 1990 to 2021, the most significant increasing trend in BL health burden was observed in Cabo Verde, while Georgia exhibited the most notable decline. From 2021 to 2040, the global age-standardized incidence and mortality rates were projected to decline by 14.7% and 24.7%, respectively. Conversely, the health burden on individuals aged 20 to 54 years was anticipated to rise through 2040. In our study, low bone mineral density was found to be linked with elevated risk for males aged over 54 years, while childhood sexual abuse exhibited a paramount positive association with BL risk for females, regardless of age. Notably, tobacco use, particularly secondhand smoking, were inversely associated with BL risk across all age groups and sexes.
Conclusion: Burkitt lymphoma demonstrated unique distribution patterns in terms of age, sex, and region. Further investigations into the heterogeneity of the risk factors for BL are essential for the development of more effective health policies and clinical practices.
Keywords: Burkitt lymphoma, global burden of disease, health burden, trend, risk factor
Introduction
Burkitt lymphoma (BL), a highly aggressive non-Hodgkin lymphoma (NHL), is derived from B cells and is genetically characterized by the translocation and dysregulation of the protooncogene MYC.1 The global health burden of BL demonstrates substantial disparities across sex, age, and geographical regions. This variability reflects a complex interplay of incompletely understood risk factors, inconsistent diagnostic approaches, and inequitable treatment access. Nevertheless, the diverse epidemiological landscape of BL has undergone significant and ongoing evolution, diverging from patterns documented in prior regional studies.2–4 A comprehensive assessment of those is urgently needed for updating.
BL was considered a multifactorial disease, involving dynamic interactions between infectious exposures and individual risk profiles. Plasmodium falciparum,5 Epstein-Barr virus (EBV), human immunodeficiency virus (HIV),6,7 and hepatitis virus8–10 were identified as the primary infectious risk factors for BL. While both the pathogen-specific promoting and inhibitory factors11–13 and their synergistic interactions in BL pathogenesis14 have been extensively investigated, non-infectious risk factors remain substantially understudied, with limited evidence supporting their associations. Emerging evidence from case-control studies has identified several categories of non-infectious risk factors associated with BL development: 1) Heredity and immunity: race,15 height,8 allergic history,8 a history of eczema,8 etc.; 2) Lifestyle: alcohol consumption,8 smoking,9 etc.; 3) Occupational exposures: cleaner,8 hair dyes,8 pesticides,16 etc.; 4) Metabolism: selenium,17 magnesium,18 etc. However, the existing analyses do not provide a comprehensive global overview of sex- and age-specific distributions in non-infectious risk factors, nor quantify the relative importance of risk factors for BL.
In this paper, we estimated the global patterns and temporal trends in health burden of BL and attached significance to its heterogeneity, with projections to 2040. We also identified potential non-infectious risk factors from a global view, aiming to offer new insights into the associations for BL in non-endemic settings and inform further researches.
Methods
Data Sources
Data on BL and associated risk factors were extracted from the updated Global Burden of Disease (GBD) 2021 Data Resources (https://ghdx.healthdata.org/gbd-2021). Therefore, ethical approval or consent was not required for participation in the study as all data were available in the public domain. This study followed the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) recommendations.19 Diagnoses adhere to the ICD-10 coding system where Burkitt lymphoma correspond to ICD-10 codes C83.7. In accordance with the established protocol, the numbers, percentages, and rates of incidence, mortality, prevalence, and disability-adjusted life years (DALYs) of BL between 1990 and 2021 were extracted, without any inclusion/exclusion criteria. The population with BL was stratified into different subgroups based on sex (males, females, and both sexes), age (five-year age groups and selected age groups: under 20 years, 20 to 54 years, and over 54 years), region (204 countries and territories, 7 GBD super regions, 21 GBD regions), and socio-demographic index (SDI) (Low SDI, Low-middle SDI, Middle SDI, High-middle SDI, and High SDI regions). The SDI, serving as an indicator of development, is calculated as the geometric mean of zero-to-one indices of the total fertility rate among youngsters aged less than 25 years, mean education for those aged 15 and above, and lag-distributed per-capita income.20 The methodologies of the overall 2021 GBD study and the estimations of disease burden were performed as described in previous studies.
Statistical Analysis
The average annual percentage change (AAPC) and its corresponding 95% confidence interval (CI) were calculated by joinpoint regression to quantify the temporal trends in the health burden of BL, using the Joinpoint regression program (version 5.3.0), accessible through the Surveillance Research Program of the US National Cancer Institute.21 Monte Carlo permutation method was used to test significance. An upward trend in ASRs was defined as the corresponding AAPC value and its 95% CI above zero, and vice versa. An interval that overlaps between 95% CI of AAPC and zero indicates a stable trend, suggesting no significant increase or decrease.
To quantify the age-related factors contributing to the changes in the DALYs of BL over time within different global demographic contexts, we employed Dus Gupta’s decomposition analysis by expressing the disease burden as the product of four factors: (1) population growth, (2) population aging, (3) variations in prevalence rate by age, and (4) disease severity, which corresponds to the four terms outlined in the following equation:

where a represents the 5-year age group of the adult population, d represents BL, and y represents year.22 We quantified the additive contribution of these four factors to the total percentage change in BL DALYs from 1990 to 2021 across the 7 GBD super regions and 21 GBD regions.
All rates are reported per 100,000 person-years. The computation of age-standardized rates was based on the GBD world population standard. Each estimate was followed by a 95% CI. All statistical analyses in this study were conducted utilizing R program (version 4.4.1). A two-sided P value of less than 0.05 was considered statistically significant.
Estimate Projections
The Bayesian age-period-cohort (BAPC) model is a sophisticated statistical approach used in the prediction to decompose and forecast the impacts of age, period, and cohort effects on the health burden of diseases. Utilizing the BAPC model, we predicted trends in the health burdens of BL until 2040, stratified by sex and age subgroups, based on forecasted population estimates.23
Risk Factors Analysis
The summary exposure value (SEV) is a measure of a population’s exposure to a risk factor that takes into account the extent of exposure by risk level and the severity of that risk’s contribution to disease burden with a scale of 0% to 100%. We extracted SEVs for 66 non-infectious risk factors in 204 countries and territories from the GBD database stratified by sex and age. Regions with missing values were excluded from the subgroup analysis. Potential factors were preliminarily identified through univariate analysis and Spearman correlation analysis (P <0.05). Subsequently, further identification was via LASSO regression analysis with a variance inflation factor threshold of less than 4. Finally, the relationships between risk factors and health burden, including incidence and mortality, for BL were assessed using multivariate linear regression analysis stratified by sex and age. The incidence and mortality data of BL as well as SEVs for risk factors underwent logarithmic transformation. Regression coefficient, also known as beta coefficient (β), and its corresponding 95% CI was derived from multivariate regression. The β estimates represent the degree of change in the ASRs of incidence or mortality for BL per unit increase in the prevalence of the risk factors. Furthermore, standardized beta coefficient (βstd) was calculated with adjusted scales of data to compare the relative importance between the different risk factors.
Results
Health Burden and Its Heterogeneity of Burkitt Lymphoma, in 2021
In 2021, the estimated global incident number of BL was 19,073 (95% CI: 9651 to 32,509), nearly threefold that of 1990. The estimated global mortality was 6526 (95% CI: 3955 to 9035), representing a 70% rise over the past three decades. The global age-standardized incidence rate (ASIR) was 0.24 (95% CI: 0.21 to 0.40), age-standardized mortality rate (ASMR) was 0.07 (95% CI: 0.05 to 0.09), age-standardized prevalence rate (ASPR) was 1.57 (95% CI: 0.84 to 2.55), and age-standardized DALY rate (ASDR) was 5.30 (95% CI: 3.29 to 6.89) per 100,000 person-years (Figures 1 and S1,Table S2). Compared to 1990, ASIR and ASPR had significant percentage increases, while ASMR and ASDR showed no significant changes (Tables S1 and S2).
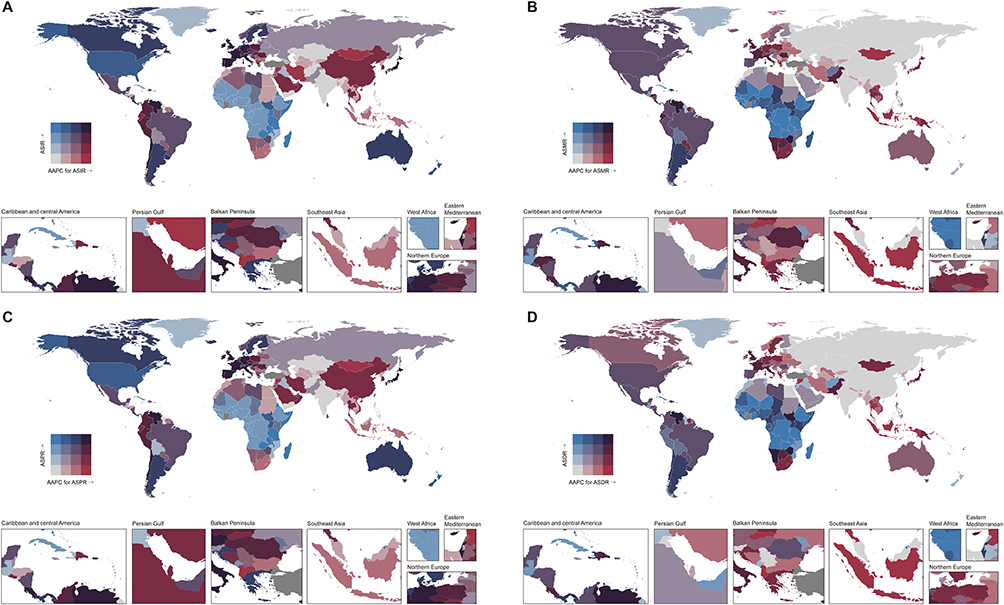 |
Figure 1 Quartiles of age-standardized rates of incidence (A), mortality (B), prevalence (C), and DALYs (D) for Burkitt lymphoma in 2021 and corresponding average annual percentage changes from 1990 to 2021, both sexes. Abbreviations: ASR, age-standardized incidence/mortality/prevalence/DALY rate; AAPC, average annual percentage change. |
Globally, with the exception of Oceania, there was a consistent pattern where males experienced a greater health burden from BL in 2021 than females. This is evident in the global male-to-female (M/F) ratios: 2.0 for ASIR, 1.8 for ASMR, 1.9 for ASPR, and 2.1 for ASDR (Figures 2 and S1). Furthermore, this pattern was more pronounced among individuals aged under 20 years with higher global M/F ratios across all ASRs, except in South Asia.
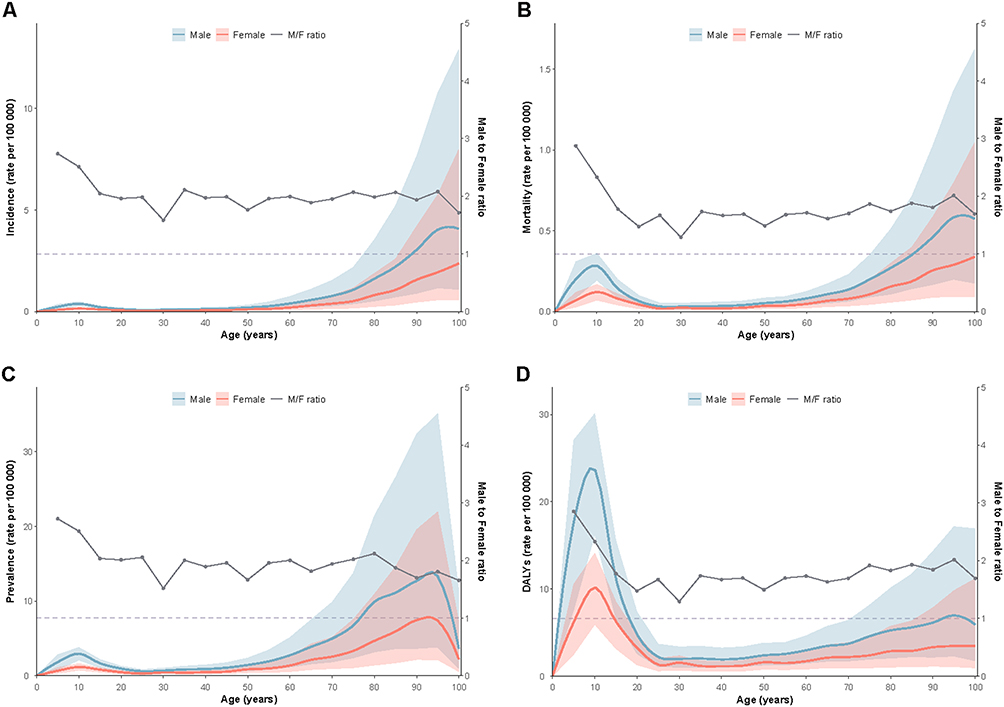 |
Figure 2 Global sex- and age-specific distributions in incidence (A), mortality (B), prevalence (C), and DALY (D) rates for Burkitt lymphoma, per 100,000 person-years, in 2021. |
The age distribution of the BL health burden typically followed a unimodal or bimodal pattern, with peak values observed in cases aged under 20 years and/or those aged over 80 years (Figures 2 and S1). For ASDR alone, the main peak occurred in the age group under 20 years at the global level. Across the SDI strata, the peak within the age group under 20 years receded as the SDI values increased, regardless of the disease measure.
In 2021, the highest ASIR and ASPR for BL were both reported in Andorra (ASIR = 1.43, 95% CI: 0.46 to 3.14; ASPR = 9.61, 95% CI: 3.21 to 20.63), while the highest ASMR and ASDR were both reported in Uganda (ASMR = 0.86, 95% CI: 0.41 to 1.38; ASDR = 52.60, 95% CI: 28.06 to 78.86). In terms of SDI strata, there were positive correlations between ASIR and SDI (rho = 0.239, P <0.001) and between ASPR and SDI (rho = 0.216, P =0.002). However, inverse correlations were found between ASMR and SDI (rho = −0.387, P <0.001) and between ASDR and SDI (rho = −0.438, P <0.001) (Figure 3).
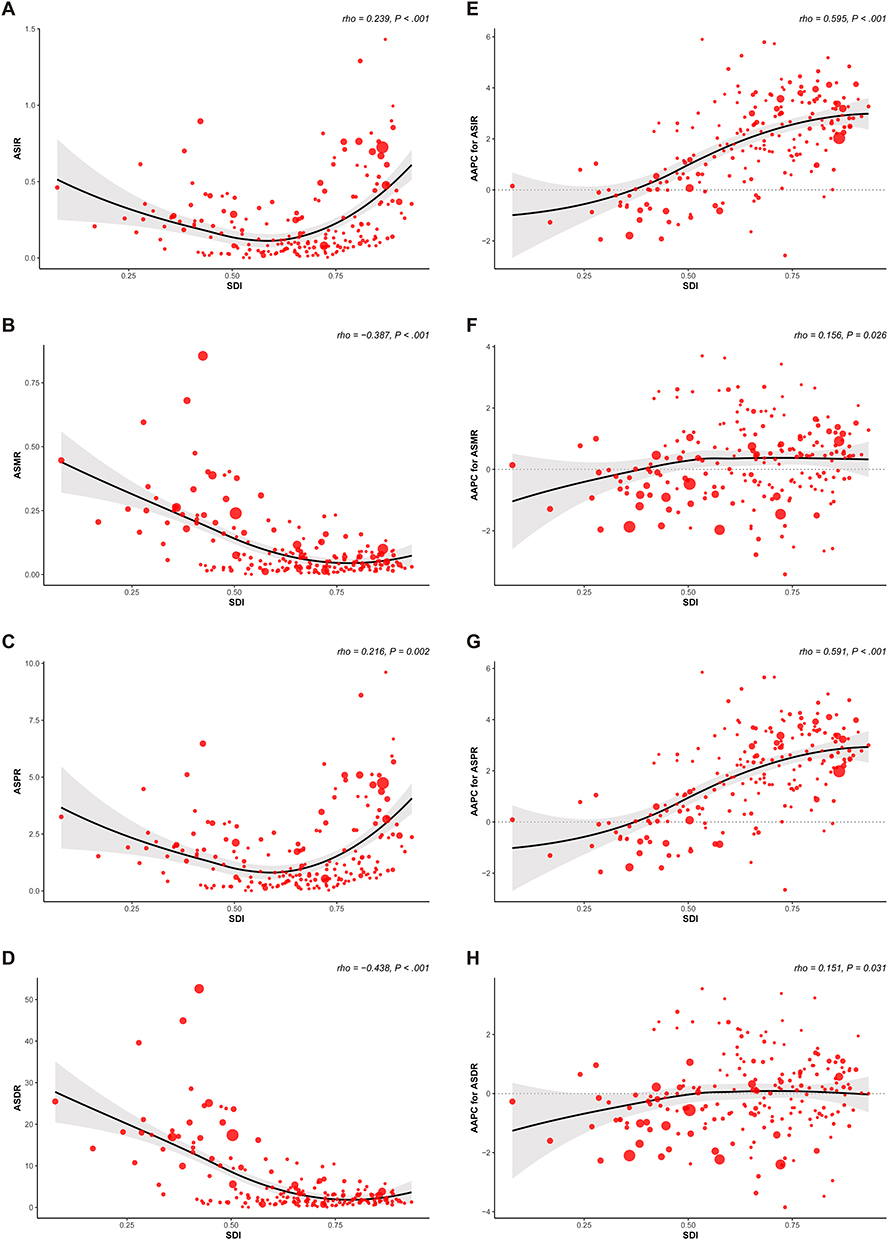 |
Figure 3 The correlations between SDI and ASR of incidence (A), mortality (B), prevalence (C), and DALYs (D) in 2021, and between SDI and AAPC for ASIR (E), ASMR (F), ASPR (G), and ASDR (H) from 1990 to 2021. The circles represent 204 countries and territories. The size of circle represents the number of Burkitt lymphoma patients in 1990 (E-H) and 2021 (A–D). The rho indices Spearman correlation coefficient. Abbreviations: ASR, age-standardized incidence/mortality/prevalence/DALY rate; AAPC, average annual percentage change; SDI, socio-demographic index. |
Temporal Health Burden Trends of Burkitt Lymphoma, 1990–2021
From 1990 to 2021, there was an upward trend in the global health burden of BL among all ASRs (Tables S1 and S2). Among the 204 countries and territories, Cabo Verde exhibited the most pronounced increasing trend (AAPC for ASIR = 5.90, 95% CI: 5.36 to 6.45; AAPC for ASMR = 3.70, 95% CI: 3.18 to 4.22; AAPC for ASPR = 5.85, 95% CI: 5.31 to 6.40; AAPC for ASDR = 3.55, 95% CI: 2.97 to 4.14), whereas Georgia showed the most significant decreasing trend across all health measures (AAPC for ASIR = −2.57, 95% CI: −3.95 to −1.17; AAPC for ASMR = −3.42, 95% CI: −4.82 to −2.00; AAPC for ASPR = −2.65, 95% CI: −4.06 to −1.22; AAPC for ASDR = −3.85, 95% CI: −5.34 to −2.32).
Overall, there was no significant difference in the health burden percentage changes between males and females. However, for those aged under 5 years, females exhibited a significantly lower percentage increase in mortality and DALYs compared to males, and even showed a decreasing trend in incidence and prevalence (Figure S2). Globally, the greatest percentage increases of mortality and DALYs were observed in individuals under 20 years old, while the highest increase of incidence and prevalence occurred in those over 54 years old (Figure S2).
Across the SDI strata, there were positive correlations between the SDI and AAPCs for ASIR (rho = 0.595, P <0.001), ASMR (rho = 0.156, P = 0.026), ASPR (rho = 0.591, P <0.001), and ASDR (rho = 0.151, P = 0.031) (Figure 3). Low SDI regions exhibited significant declining trends in all ASRs from 1990 to 2021, whereas other SDI regions showed rising trends in ASIR and ASPR (Tables S1 and S2). Notably, there were downward trends in the ASDR of Middle SDI regions and in the ASMR and ASDR of High-middle SDI regions.
Factors Influencing DALY Changes, 1990–2021
Decomposition analysis by region revealed the contributions of the four factors to the aggregate percentage changes in BL DALYs from 1990 to 2021 (Figure 4 and Table S3). Population growth was the most substantial contributor in Low SDI regions, sub-Saharan Africa, and Oceania, accounting for an increase exceeding 100%. Positive contributions attributable to population aging were observed only in High SDI regions and High-income regions. Age-specific prevalence rate variations dominated the DALY changes among regions with medium to high SDI values, notably in Centre Europe, High-income regions, and Southern sub-Saharan Africa. Across all GBD regions, the impact of disease severity was uniformly negative, albeit to varying degrees, but minimal in Low SDI regions.
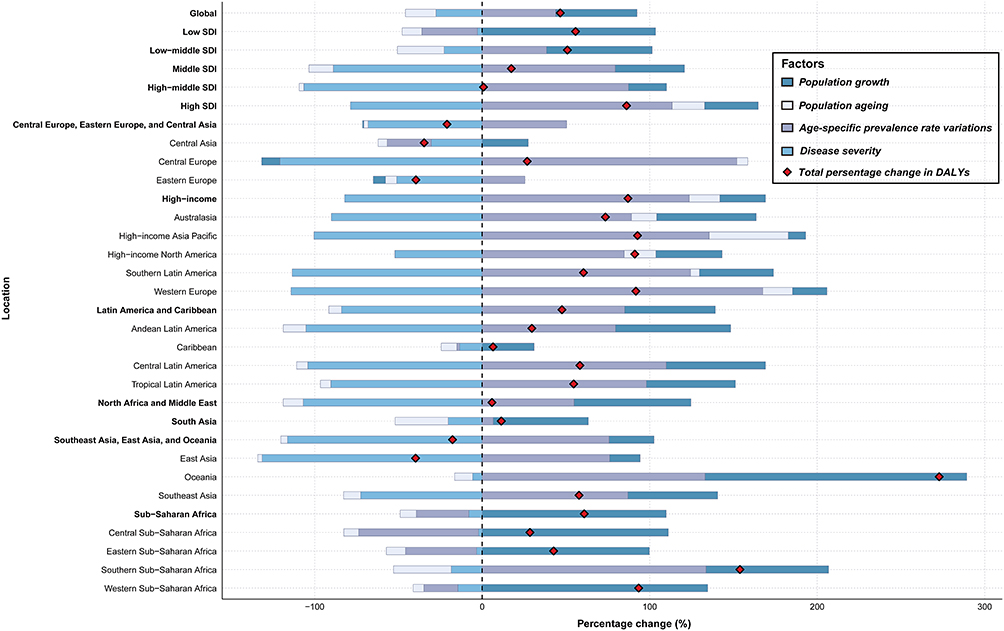 |
Figure 4 Contributions of population growth, population aging, age-specific prevalence rate variations, and disease severity to the percentage changes of Burkitt lymphoma DALYs, 1990–2021. |
Health Burden Projections of Burkitt Lymphoma, 2021–2040
At the global level, from 2021 to 2040, ASRs of incidence, mortality, prevalence, and DALYs for BL all tended to decrease, and no notable gender differences were observed (Figure S3). Among the GBD super regions, Southeast Asia, East Asia, and Oceania, and South Asia were predicted to bear greater health burdens on BL, while the burdens for other regions were expected to be alleviated (Figure S4). The most marked increase in ASIR was predicted to occur in Southeast Asia, East Asia, and Oceania (AAPC = 3.92%, 95% CI: 3.91% to 3.94%, P <0.001). Furthermore, sub-Saharan Africa was expected to exhibit the most evident downward trends across all health burden rates.
By age, the age groups under 20 years and over 54 years were expected to experience a considerable declining trend in all health burden rates per 100,000 person-years (Figure S5 and Table S4). Notably, females under 20 years of age were predicted to show a more significant declining trend than males across all health burden rates. However, cases aged 20 to 54 years were predicted to suffer from increased health burden during the next two decades.
Potential Non-Infectious Risk Factors for Burkitt Lymphoma, in 2021
Risk Factor-Incidence Correlations in Burkitt Lymphoma
At the global level in 2021, the ASIR of BL for males exhibited a positive association with high consumption of processed meat (β = 0.21, βstd = 0.11, P =0.047) (Figures 5 and S7A). Conversely, it was negatively associated with high exposure to smoking (β = −1.13, βstd = −0.49, P <0.001), iron deficiency (β = −0.48, βstd = −0.46, P <0.001), and kidney dysfunction (β = −1.19, βstd = −0.24, P <0.001). Furthermore, a positive correlation was observed between the ASIR of BL for females and high exposure to childhood sexual abuse (β = 0.52, βstd = 0.28, P <0.001), while high exposure to unsafe sanitation (β = −0.19, βstd = −0.26, P <0.001), kidney dysfunction (β = −1.33, βstd = −0.28, P <0.001), and secondhand smoke (β = −0.78, βstd = −0.31, P <0.001) was associated with a lower risk.
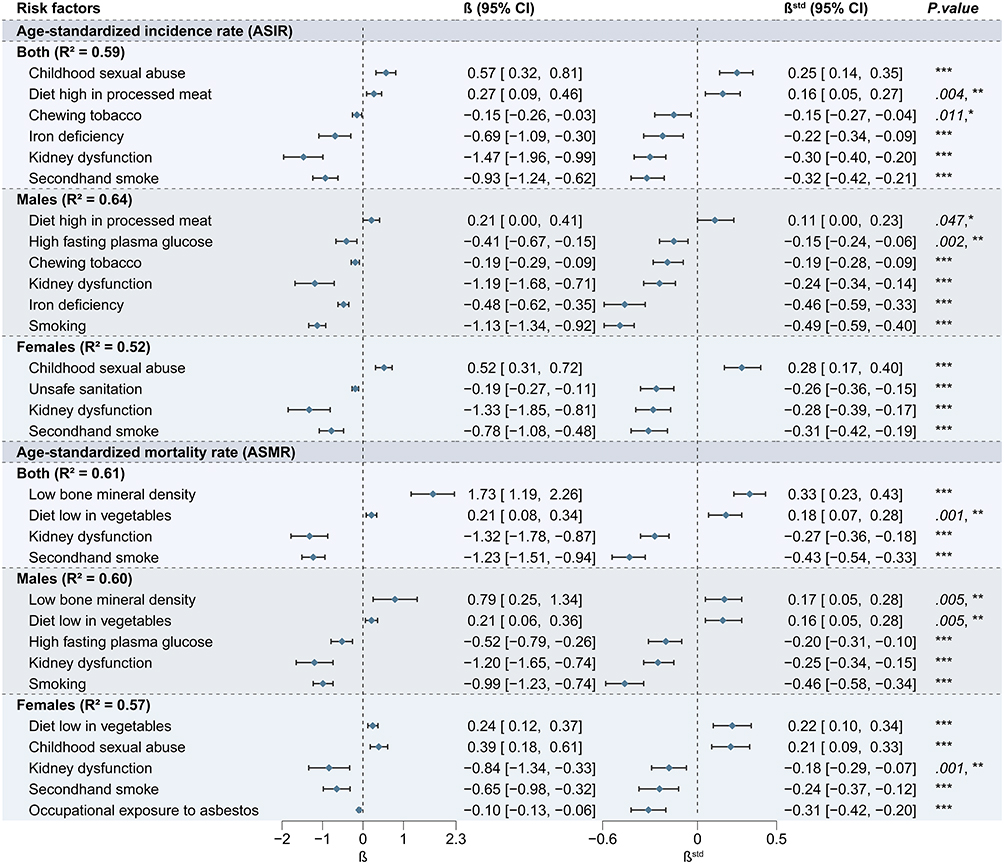 |
Figure 5 Potential non-infectious risk factors for global incidence and mortality of Burkitt lymphoma by sex in 2021. Abbreviations: β, regression coefficient; βstd, standardized regression coefficient. Note: *P <0.05, **P <0.01, ***P <0.001. |
In the age-specific analysis, a high intake of sugar-sweetened beverages emerged as a prominent risk factor for individuals aged 20 to 54 years (β = 0.26, βstd = 0.21, P <0.001) and those over 54 years (β = 0.62, βstd = 0.25, P <0.001) (Figures S6 and S7B–D). Among individuals over 54 years old, low bone mineral density (β = 2.86, βstd = 0.45, P <0.001) was identified as an additional and more pronounced risk factor, particularly for males, whereas iron deficiency (β = −1.04, βstd = −0.67, P <0.001) was the most significantly inversely associated factor in this age group. Notably, high exposure to childhood sexual abuse was the most significant risk factor for BL incidence among females under 20 years and over 54 years. Secondhand smoke (β = −1.27, βstd = −0.47, P <0.001) was the primary factor contributing to low BL incidence in both sexes for individuals under 20 years, while kidney dysfunction (β = −1.63, βstd = −0.39, P <0.001) played a similar role in those aged 20 to 54 years, and iron deficiency (β = −1.04, βstd = −0.67, P <0.001) for those over 54 years.
Risk Factor-Mortality Correlations in Burkitt Lymphoma
At the global level in 2021, high ASMRs in males with BL were associated with low bone mineral density (β = 0.79, βstd = 0.17, P =0.005) and a low consumption of vegetables (β = 0.21, βstd = 0.16, P =0.005) (Figures 5 and S7A). However, there were inverse correlations between ASMR and a high prevalence of high fasting plasma glucose (β = −0.52, βstd = −0.20, P <0.001), kidney dysfunction (β = −1.20, βstd = −0.25, P <0.001), and smoking (β = −0.99, βstd = −0.46, P <0.001). For females with BL, there was a positive association between ASMR and low consumption of vegetables (β = 0.24, βstd = 0.22, P <0.001), as well as childhood sexual abuse (β = 0.39, βstd = 0.21, P <0.001). Nevertheless, kidney dysfunction (β = −0.84, βstd = −0.18, P =0.001), secondhand smoke (β = −0.65, βstd = −0.24, P <0.001), and occupational exposure to asbestos (β = −0.10, βstd = −0.31, P <0.001) were inversely associated with mortality risk.
Among cases under 20 years of age, no access to handwashing facilities (β = 0.60, βstd = 0.52, P <0.001) was the most prominent risk factor for BL mortality in both sexes (Figures S6 and S7B–D). In terms of the group aged 20 to 54 years, the mortality of BL was considered positively related to low bone mineral density (β = 1.18, βstd = 0.24, P <0.001), whereas no statistical significance was detected by sex. A low consumption of vegetables led to elevated mortality of BL for the group aged 20 to 54 years (β = 0.27, βstd = 0.24, P <0.001) and the group over 54 years (β = 0.24, βstd = 0.21, P <0.001), irrespective of sex. Besides, low bone mineral density (β = 1.74, βstd = 0.40, P <0.001) and high alcohol use (β = 0.28, βstd = 0.20, P <0.001) were additional risk factors for males over 54 years. Childhood sexual abuse remained a significant risk factor for BL mortality among females across all age groups. Of particular concern, tobacco use, which includes smoking, secondhand smoke, and chewing tobacco, was inversely associated with mortality across all age groups and sexes, except for males over 54 years, where iron deficiency was of greater significance.
Discussion
Based on the GBD 2021 database, we presented markedly distinct distribution patterns of BL in terms of health burden by sex, age, and region. The highest burdens on incidence and prevalence were observed in High-income regions, while the highest ASMR and ASDR were observed in sub-Saharan Africa, highlighting critical focus areas for future interventions. Our analysis confirmed a consistent global pattern of a marked male predominance in the health burden of BL. This disparity was most pronounced among individuals under the age of 20. Projections from 2021 to 2040 indicate a stark contrast: a declining global BL burden alongside a significant increase in the 20–54-year-old population. Breaking from previous regional surveys, our study is the first to utilize the GBD database for a comprehensive global assessment of potential non-infectious BL risk factors, demonstrating their sex- and age-specific heterogeneity.
In our study of potential BL-related non-infectious risk factors, lack of access to handwashing facilities significantly increases the risk of infections like EBV and malaria, which in turn correlates with higher mortality rates of BL among cases under 20 years of age. Low bone mineral density was linked to elevated incidence and mortality rates in males aged over 54 years. The correlation could be attributed to vitamin D insufficiency, which was prevalent in the elderly24 and malaria infections.25,26 Previous studies reported that a low level of vitamin D led to reduced production of vitamin D dependent antimicrobial peptide cathelicidin by lymphoma associated macrophages, suppressing selective antitumor activity against BL.27–29 Although a diet high in sugar-sweetened beverages was associated with increased incidence of BL among individuals aged over 20 years, this correlation was not statistically significant when analyzed across the entire population. A high-vegetable diet has been reported to be associated with a reduction in the risk of several B-cell NHL subtypes, such as diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma.30–32 However, BL was not classified or discussed in these studies, warranting further investigation. Childhood sexual abuse played a paramount role in the elevated incidence and mortality of BL for females, regardless of age, which remains insufficient direct evidence. According to previous studies, childhood maltreatment is associated with heightened HPA-axis activity and inflammation, which may compromise the acquired immune response to chronic or latent infections and induce latent herpesvirus reactivation, including EBV.33–35 This suggests potential mechanisms connecting female physiological and psychological health to the pathogenesis of BL. Occupational or daily life exposure to potential chemicals, such as hair dyes, pesticides, benzene, and trichloroethylene, played a vital role in the risk of NHL.8,16 Our findings suggested that occupational exposure to asbestos was strongly correlated with the incidence of BL among males over 54 years of age in the simple regression analysis (rho = 0.521, P <0.001). However, this correlation, while indicative, did not achieve statistical significance in the multivariate regression analysis, which agreed with the results of several studies on NHL without setting BL apart and thus entailed further investigation.36 Population-wide results that were not confirmed in the subgroups were thought to result from Simpson’s paradox,37 requiring more detailed and precise grouping by combination with age, sex, and region.
Although BL has not been considered to be a smoking-related malignancy,8 recent investigations suggest otherwise. In our analysis, tobacco use, particularly secondhand smoking, emerged as the leading risk factor inversely associated with the incidence and mortality rates of BL across all age groups and sexes. This result was in accord with a nested case-control study in the UK, which showed a decreased risk of BL in those who were former smokers (OR = 0.47, 95% CI: 0.29 to 0.76; P = 0.002) and current smokers (OR = 0.24, 95% CI: 0.12 to 0.46; P < 0.0001), particularly for those aged over 20 years old.9 However, there was insufficient molecular biology evidence backing up. Kidney dysfunction was also one of the most common risk factors inversely associated with BL risk, observed significantly only within the age group of 20 to 54 years in this study. However, there was insufficient evidence to support this correlation. Iron deficiency was an additional negative risk factor contributing to the health burden of BL, mainly affecting both males and females over the age of 54 years. Although there was insufficient evidence to establish a definitive correlation between BL and iron deficiency, it has been reported that CYB561A3, a gene exhibiting ferrireductase activity and leading to iron starvation when knocked out, was essential for the proliferation of EBV+ BL cells but not lymphoblastoid cell lines, which underscored the significance and specificity of iron metabolism in BL.38
This study has several inherent limitations. First, owing to lagging cancer reporting mechanisms and classification systems in some developing countries and territories, the health burden of BL might be underestimated. Second, infectious risk factors for BL, such as EBV infection, malaria, and HIV/AIDS, were not included in this analysis, primarily because of data deficiencies in many countries. In particular, most cases of EBV infection are asymptomatic infections without serosurveys. There is no universally accepted, standardized metric to accurately and uniformly measure the burden of EBV infection across the globe. These gaps inevitably introduced limitations to the statistical power of our analysis. In addition, genome association studies have revealed a correlation between BL and non-infectious diseases such as sickle cell disease, offering clues to the exploration of risk factors at a genetic level.11,39 Third, not all of the aforementioned risk factors could be reasonably explained or reconciled with the outcomes of case-control studies, which warrants further exploration. Besides, it’s worth stating that the results of the risk factor association analysis might not be applicable at an individual level. Fourth, the analysis of BL subtypes could not be performed owing to data constraints, even though heterogeneity in the distribution, temporal trends, and risk factors of subtypes could indeed make sense.
Conclusions
In conclusion, this study demonstrates distinct age, sex, and geographical distributions and temporal patterns in the health burden of Burkitt lymphoma from 1990 to 2021. Projections from 2021 to 2040 indicate a critical shift towards a growing proportion of adult cases, highlighting the need for an age-based hierarchical management strategy. Our analysis identifies several novel modifiable risk factors for Burkitt lymphoma, such as low bone mineral density, as actionable targets for future preventive strategies aimed at reducing the disease burden. Moreover, further investigation into the risk factors for Burkitt lymphoma is indeed meaningful via multicenter, randomized controlled studies. Preventive measures, early diagnosis, and precision treatment for Burkitt lymphoma warrant global promotion and tailored adjustments based on the national medical situation.
Abbreviations
BL, Burkitt lymphoma; DALY, disability-adjusted life year; SDI, socio-demographic index; ASR, age-standardized incidence/mortality/prevalence/DALY rate; AAPC, average annual percentage change; SEV, summary exposure value; β, beta coefficient; βstd, standardized beta coefficient; NHL, non-Hodgkin lymphoma; EBV, Epstein-Barr virus; HIV, human immunodeficiency virus; GBD, Global Burden of Disease; CI, confidence interval; BAPC, Bayesian age-period-cohort; M/F ratio, male-to-female ratio.
Data Sharing Statement
All data reported in this paper are publicly available from the Institute of Health Metrics and Evaluation (http://www.healthdata.org/; http://ghdx.healthdata.org/gbd-results-tool).
Ethics Approval and Consent to Participate
Our study is available to be exempt from ethical approval based on national legislation guidelines. More details are on item 1 and item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China.
Acknowledgments
We highly appreciate the work by the GBD 2021 collaborators.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Science and Technology Program of Health and Family Planning Commission of Jiangxi Province (202210918) and the Science and Technology Department of Jiangxi Province (20223BCG74003).
Disclosure
The authors have declared that no competing interests exist.
References
1. Crombie J, Lacasce A. The treatment of Burkitt lymphoma in adults. Blood. 2021;137(6):743–12. doi:10.1182/blood.2019004099
2. Mbulaiteye SM, Anderson WF, Bhatia K, Rosenberg PS, Linet MS, Devesa SS. Trimodal age-specific incidence patterns for Burkitt lymphoma in the United States, 1973-2005. Int J Cancer. 2010;126(7):1732–1739. doi:10.1002/ijc.24934
3. Mbulaiteye SM, Devesa SS. Burkitt Lymphoma incidence in five continents. Hemato. 2022;3(3):434–453. doi:10.3390/hemato3030030
4. Aka P, Kawira E, Masalu N, et al. Incidence and trends in Burkitt lymphoma in northern Tanzania from 2000 to 2009. Pediatr Blood Cancer. 2012;59(7):1234–1238. doi:10.1002/pbc.24194
5. Broen K, Dickens J, Trangucci R, et al. Burkitt lymphoma risk shows geographic and temporal associations with Plasmodium falciparum infections in Uganda, Tanzania, and Kenya. Proc Natl Acad Sci U S A. 2023;120(2):e2211055120. doi:10.1073/pnas.2211055120
6. Ziegler JL, Drew WL, Miner RC, et al. Outbreak of Burkitt’s-like lymphoma in homosexual men. Lancet. 1982;2(8299):631–633. doi:10.1016/s0140-6736(82)92740-4
7. Guech-Ongey M, Simard EP, Anderson WF, et al. AIDS-related Burkitt lymphoma in the United States: what do age and CD4 lymphocyte patterns tell us about etiology and/or biology? Blood. 2010;116(25):5600–5604. doi:10.1182/blood-2010-03-275917
8. Mbulaiteye SM, Morton LM, Sampson JN, et al. Medical history, lifestyle, family history, and occupational risk factors for sporadic Burkitt lymphoma/leukemia: the interlymph non-hodgkin lymphoma subtypes project. JNCI Monographs. 2014;2014(48):106–114. doi:10.1093/jncimonographs/lgu003
9. Karimi P, Birmann BM, Anderson LA, et al. Risk factors for Burkitt lymphoma: a nested case-control study in the UK clinical practice research datalink. Br J Haematol. 2018;181(4):505–514. doi:10.1111/bjh.15229
10. Baker FS, Wang J, Florez-Vargas O, et al. IFNL4 genotypes and risk of childhood Burkitt lymphoma in east Africa. J Interferon Cytokine Res. 2023;43(9):394–402. doi:10.1089/jir.2023.0014
11. Hong HG, Gouveia MH, Ogwang MD, et al. Sickle cell allele HBB-rs334(T) is associated with decreased risk of childhood Burkitt lymphoma in East Africa. Am J Hematol. 2024;99(1):113–123. doi:10.1002/ajh.27149
12. López C, Burkhardt B, Chan JKC, et al. Burkitt lymphoma. Nat Rev Dis Primers. 2022;8(1):78. doi:10.1038/s41572-022-00404-3
13. Schmit N, Kaur J, Aglago EK. Mosquito bed net use and burkitt lymphoma incidence in Sub-Saharan Africa: a systematic review and meta-analysis. JAMA Netw Open. 2024;7(4):e247351. doi:10.1001/jamanetworkopen.2024.7351
14. Aguilar R, Casabonne D, O’Callaghan-Gordo C, et al. Assessment of the combined effect of epstein-barr virus and plasmodium falciparum infections on endemic Burkitt lymphoma using a multiplex serological approach. Front Immunol. 2017;8:1284. doi:10.3389/fimmu.2017.01284
15. Mishra A, Mishra A, Taylor MA, Sharma D, Kubesh M. Poor disease-specific survival in black pediatric patients diagnosed with Burkitt lymphoma: an analysis of the surveillance, epidemiology, and end results database. Pediatr Blood Cancer. 2024;71(10):e31204. doi:10.1002/pbc.31204
16. Francisco LFV, da Silva RN, Oliveira MA, et al. Occupational exposures and risks of non-hodgkin lymphoma: a meta-analysis. Cancers. 2023;15(9):2600. doi:10.3390/cancers15092600
17. Sumba PO, Kabiru EW, Namuyenga E, et al. Microgeographic variations in Burkitt’s lymphoma incidence correlate with differences in malnutrition, malaria and Epstein-Barr virus. Br J Cancer. 2010;103(11):1736–1741. doi:10.1038/sj.bjc.6605947
18. Ravell J, Otim I, Nabalende H, et al. Plasma magnesium is inversely associated with Epstein-Barr virus load in peripheral blood and Burkitt lymphoma in Uganda. Cancer Epidemiol. 2018;52:70–74. doi:10.1016/j.canep.2017.12.004
19. Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet. 2016;388(10062):e19–e23. doi:10.1016/s0140-6736(16)30388-9
20. Ong KL, Stafford LK, McLaughlin SA, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. The Lancet. 2023;402(10397):203–234. doi:10.1016/s0140-6736(23)01301-6
21. Kim H-J, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. doi:10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z
22. Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL. Measuring population ageing: an analysis of the global burden of disease study 2017. Lancet Public Health. 2019;4(3):e159–e167. doi:10.1016/s2468-2667(19)30019-2
23. Vollset SE, Goren E, Yuan CW, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the global burden of disease study. Lancet. 2020;396(10258):1285–1306. doi:10.1016/s0140-6736(20)30677-2
24. Li J, Jia H, Liu Z, Xu K. Global, regional and national trends in the burden of low bone mineral density from 1990 to 2030: a Bayesian age-period-cohort modeling study. Bone. 2024;189:117253. doi:10.1016/j.bone.2024.117253
25. Setto JM, Libonati RMF, Ventura A, et al. Association between vitamin D serum levels and clinical, laboratory, and parasitological parameters in patients with malaria from an endemic area of the Amazon. Rev Soc Bras Med Trop. 2022;55:e00772021. doi:10.1590/0037-8682-0077-2021
26. Cusick SE, Opoka RO, Lund TC, John CC, Polgreen LE. Vitamin D insufficiency is common in Ugandan children and is associated with severe malaria. PLoS One. 2014;9(12):e113185. doi:10.1371/journal.pone.0113185
27. Bruns H, Büttner M, Fabri M, et al. Vitamin D-dependent induction of cathelicidin in human macrophages results in cytotoxicity against high-grade B cell lymphoma. Sci Transl Med. 2015;7(282):282ra47. doi:10.1126/scitranslmed.aaa3230
28. Bruns H, Fabri M, Maurberger A, et al. M1 macrophages eliminate lymphoma cells through the vitamin D dependent antimicrobial peptide cathelicidin. Blood. 2011;118(21):1098. doi:10.1182/blood.V118.21.1098.1098
29. Bruns H, Mougiakakos D, Fabri M, et al. Vitamin D triggers killing of burkitt lymphoma cells by human macrophages. Blood. 2012;120(21):1035. doi:10.1182/blood.V120.21.1035.1035
30. Chiu BCH, Kwon S, Evens AM, Surawicz T, Smith SM, Weisenburger DD. Dietary intake of fruit and vegetables and risk of non-Hodgkin lymphoma. Cancer Causes Control. 2011;22(8):1183–1195. doi:10.1007/s10552-011-9797-5
31. Bradbury KE, Appleby PN, Key TJ. Fruit, vegetable, and fiber intake in relation to cancer risk: findings from the European Prospective Investigation into Cancer and Nutrition (EPIC). Am J Clin Nutr. 2014;100(Suppl 1):394s–8s. doi:10.3945/ajcn.113.071357
32. Birmann BM, Bertrand K, Rosner B, Ardisson Korat A. Fruit and vegetable consumption and risk of non-hodgkin lymphoma. Blood. 2019;134(Supplement_1):4127. doi:10.1182/blood-2019-128518
33. Shirtcliff EA, Coe CL, Pollak SD. Early childhood stress is associated with elevated antibody levels to herpes simplex virus type 1. Proc Nat Acad Sci. 2009;106(8):2963–2967. doi:10.1073/pnas.0806660106
34. Danese A, McEwen BS. Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiol Behav. 2012;106(1):29–39. doi:10.1016/j.physbeh.2011.08.019
35. Chen MA, LeRoy AS, Majd M, et al. Immune and epigenetic pathways linking childhood adversity and health across the lifespan. review. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.788351
36. Seidler A, Becker N, Nieters A, et al. Asbestos exposure and malignant lymphoma: a multicenter case-control study in Germany and Italy. Int Arch Occup Environ Health. 2010;83(5):563–570. doi:10.1007/s00420-009-0502-x
37. Tu YK, Gunnell D, Gilthorpe MS. Simpson’s paradox, lord’s paradox, and suppression effects are the same phenomenon--the reversal paradox. Emerg Themes Epidemiol. 2008;5:2. doi:10.1186/1742-7622-5-2
38. Wang Z, Guo R, Trudeau SJ, et al. CYB561A3 is the key lysosomal iron reductase required for Burkitt B-cell growth and survival. Blood. 2021;138(22):2216–2230. doi:10.1182/blood.2021011079
39. Legason ID, Pfeiffer RM, Udquim KI, et al. Evaluating the causal link between malaria infection and endemic Burkitt lymphoma in northern uganda: a mendelian randomization study. EBioMedicine. 2017;25:58–65. doi:10.1016/j.ebiom.2017.09.037
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.