Back to Journals » International Journal of General Medicine » Volume 14
Global Correlations Between Chronic Inflammation and Violent Incidents: Potential Behavioral Consequences of Inflammatory Illnesses Across Socio-Demographic Levels
Authors Castle R ![]() , Bushell WC, Mills PJ, Williams MA, Chopra D, Rindfleisch JA
, Bushell WC, Mills PJ, Williams MA, Chopra D, Rindfleisch JA
Received 12 June 2021
Accepted for publication 1 September 2021
Published 12 October 2021 Volume 2021:14 Pages 6677—6691
DOI https://doi.org/10.2147/IJGM.S324367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ryan Castle,1 William C Bushell,2 Paul J Mills,3 Michelle A Williams,4 Deepak Chopra,5 James A Rindfleisch6
1Science Division, Whole Health Institute, Bentonville, AR, USA; 2Science Division, Whole Health Institute, New York, NY, USA; 3Herbert Wertheim School of Public Health and Human Longevity Science, Center of Excellence for Research and Training in Integrative Health, University of California San Diego, La Jolla, CA, USA; 4Harvard T.H. Chan School of Public Health, Department of Global Health and Population, Harvard University, Boston, MA, USA; 5Chopra Foundation, Carlsbad, CA, USA; 6Education Department, Whole Health School of Medicine and Health Sciences, Bentonville, AR, USA
Correspondence: Ryan Castle
Science Division, Whole Health Institute, 900 McClain Road, Bentonville, AR, 72712, USA
Tel +1 310 938 1390
Email [email protected]
Introduction: This review explores the potential correlation between conditions associated with chronic inflammation and measures of violence across five socioeconomic subgroups. The hypothesis being that since chronic inflammation is associated with increased aggression, an extreme version of which is violence, there should be a correlation between incidents of violence and diseases with one or more inflammatory factors, without an equivalent correlation with the contrast group. An extension of this reasoning would predict a higher correlation among lower socio-demographic index (SDI) populations as a result of fewer resources to prevent either inflammatory disease or violent crime.
Methods: In order to examine this potential correlation, an analysis was made comparing rates of change in incidence between violence, inflammatory conditions, and a contrast group disease of noninflammatory nature, as determined by Pearson’s correlation coefficient.
Results: In the low socio-demographic index, inflammatory conditions demonstrated 80% correlation with interpersonal violence, middle-low socio-demographic index inflammatory conditions demonstrated 60% correlation with interpersonal violence, middle socio-demographic index inflammatory conditions demonstrated 0% correlation with interpersonal violence, middle-high socio-demographic index inflammatory conditions demonstrated 60% correlation with interpersonal violence, and high socio-demographic index inflammatory conditions demonstrated 40% correlation with interpersonal violence.
Discussion: The majority of socio-demographic groups showed a significant correlation between rates of change in incidence of violence and inflammatory conditions. This correlation was not found with a similar frequency or strength in diseases not causally linked to inflammation. As predicted in the hypothesis, the highest correlations of inflammatory diseases with violence existed in the lower socio-demographic populations, supporting a link between inflammatory levels and incidences of violence.
Keywords: inflammation, aggression, chronic disease, incidence rates, inflammatory disease, violence, public health
Overview
Mechanism of Chronic Inflammation
A significant body of evidence suggests that acute and chronic inflammations underlie many noncommunicable diseases.1 Inflammation is critical to a healthy host’s defense against infection and injury, but when continually activated due to stressors it contributes to the pathophysiology of many chronic diseases. A persistent, low-level inflammatory response affects the innate immune system, adaptive immune system, and inflammatory mediators. The dynamic mechanisms of chronic inflammation can lead to tissue damage, oxidative stress, angiogenesis, and fibrosis in a variety of tissues, including the nervous system.2
Inflammation and Aggression
A recent area of research moves beyond psychosocial influences on inflammation and explores the inverse and/or cyclical relationship: to what degree chronic inflammation may increase or exaggerate anger and aggression, possibly contributing to a feedback loop of increasing inflammation and hostility.
Chronic activation of the body’s inflammatory system is associated with increases in hostility, aggression, and psychiatric symptoms.3 Although many of the symptoms include depression, anger and hostility are also prevalent.4 Strict application of DSM-IV criteria to increased inflammatory conditions reveals that most who developed symptoms displayed various types of mixed states, a state the DSM-V might consider “major depression with mixed features”.5 Irritability, impulsivity, and anger are symptomatic of both criteria for aggressive social behavior, while chronic inflammation is associated with increases in the likelihood and severity of anger and aggression.6–9 This analysis extrapolates from existing small-scale clinical research to search for correlational patterns at a societal level.
In order to determine a potential causal relationship between inflammation and hostility, researchers applied psychiatric control conditions for sudden changes in inflammatory condition. To achieve this criterion, human patients receiving drug treatments that affected their inflammatory systems were examined. Plasma levels of inflammatory markers were found to correlate with measures of aggression (and/or impulsivity) in healthy participants and psychiatric patients.10 Tests in humans for a causal relationship between inflammatory proteins and aggression were confirmed through CRP and IL-6, and the highest levels of chronic inflammation were associated with intermittent explosive disorder, a form of intense rage with a 2–3% prevalence rate in the United States.11
Several studies examined humans receiving the cytokine interferon (IFN)-alpha for cancer or chronic hepatitis C virus infection. Although depression has long been considered a major side effect of interferon treatment, IFN-alpha powerfully activates inflammation at a systemic level, and a causal relationship has been established between increases in IFN-alpha and increases in both depression and anger.12 Other studies into both humans and animals discovered increases and decreases in aggression in relation to the raising interleukin 1β (IL-1β) and IL-6, and the blocking of IL-1β activity, respectively.13,14 This further supports the concept that inflammatory levels are linked to mood and behavior, at least partially via the hypothalamus.15 Patients were also assessed on levels of the inflammatory marker CRP in plasma, finding elevations in inflammatory markers to be associated with increases in hostility and aggression.16,17 The pathophysiologic mechanisms are complex, but appear to involve decreased neurotrophic support, alterations in glutamate processing, and excitotoxicity that are consistent with neuropsychiatric disorders.18
The potential feedback loop of inflammation and aggression has serious implications. From a detrimental perspective, there is the danger that hostility and violence causes inflammation, which in turn may lead to increases in the severity of the hostility, which can cause yet more inflammation, etc. This cycle may trigger and perpetuate an increasingly aggressive, unhealthy population, a combination of factors that could potentially be correlated with incidents of violence.9 However, a more beneficial implication is that this cycle might be interrupted at both the inflammatory and behavioral levels.19 As referenced above, lower inflammatory levels were associated with decreased aggression, but several studies also confirmed that subjects who possessed strong social support systems did not appear to begin the inflammatory cycle in the first place.20,21 Interventions of either a medical or psychological nature could potentially be effective at interrupting a cycle that involves both.
Aggression and Violence
While a connection between inflammatory conditions and aggression has been repeatedly indicated under controlled conditions, the broader implications of these findings remain unresolved. The association of increased aggression with incidents of violence is considered strong, evidence indicating up to 71.2% of individuals with aggressive tendencies have engaged in interpersonal violence.22 To detect societal patterns, large datasets were acquired from the Global Burden of Disease (GBD) report, an ongoing longitudinal record of causes of death and disability across the world. The quantifiable societal markers of aggression are incidents of interpersonal violence and/or self-harm, which are factors closely monitored by various agencies and collated by the GBD study from 4466 reports.23 However, there has been no large-scale analysis of these incidents in relation to inflammatory disease patterns.
The relationship between violence and chronic inflammation is assumed to be mutually contributory, but given the long onset time of chronic inflammation incidents of violence are highly unlikely to begin an inflammatory cascade that results in chronic disease within the same year, though precise timeframes are currently unknown.24 Inversely, there is evidence preexisting chronic inflammation contributes to both physiological diseases and psychosocial problems.25 Therefore, this study assumes a correlation between violence and an inflammatory disease suggests a shared contributor in chronic inflammation, rather than the violent incident itself acting as the catalyst for chronic inflammation. The precise timeframe for inflammation to significantly contribute to behavior is unknown. A simplified model of this proposed set of interactions can be found in Figure 1.
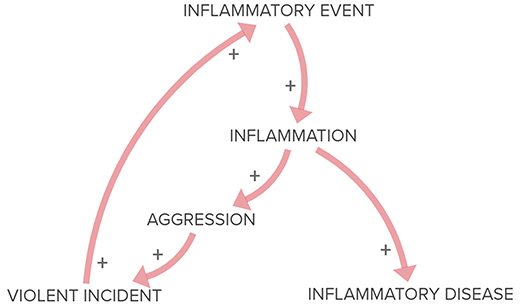 |
Figure 1 Model of proposed theory of inflammatory aggression and violence. Outlines relationships between Inflammatory Events, the chronic Inflammation the event incites, then the different manifestations of Inflammatory Disease and Aggression leading to Violent Incidents, which in turn produce their own Inflammatory Events. + = increase in effect or likelihood of the following stage. Length of connecting lines are not set to any scale and are intended to approximate relative time between stages. |
Without examining potential correlations between chronic inflammation and incidents of violence, it is difficult to either determine the degree to which inflammation influences violence or what an effective intervention for such incidents might be. This lack of knowledge impedes further research into psychosocial symptoms of inflammation and makes policy decisions on including violence within inflammation programs unlikely. Both risk excluding millions of incidents that could be influenced by chronic inflammation.
Hypothesis
As an initial examination of this possible relationship, a large-scale approach was taken to identify whether there are any significant correlations between inflammatory diseases and violent incidents. Metadata was extracted from the Global Burden of Disease (GBD) report, ranging from 1990 to 2017, spanning 285 countries and five categories in the socio-demographic index.26,27
The conditions examined include interpersonal violence and self-harm (not including states of war or foreign terrorism), inflammatory diseases including cardiovascular disease, COPD, inflammatory bowel disease (including diarrheal incidents), and a contrast group not causally linked to inflammation.
The hypothesis was that there would be a significant correlation between rates of change in conditions influenced by chronic inflammation and violent incidents, while there would be no close correlation between violent incidents and the contrast group non-inflammatory condition.
Methodology
Test Grouping
These will be the test groups associated with the presence of chronic inflammation, compared to incidents of interpersonal violence (IV) as a manifestation of aggression. Inflammatory conditions that might drastically limit the capability to inflict violence, such as advanced osteoarthritis, were excluded.
- Cardiovascular disease (CVD): the link between chronic inflammation and cardiovascular disease has been repeatedly established and is considered reliable.28,29 Evidence suggests correlations between cardiovascular disease and other inflammatory conditions.30
- Chronic obstructive pulmonary disease (COPD): the contributing factors and comorbidities of COPD are both linked to chronic inflammation.31
- Inflammatory bowel disease (IBD): A disease known to be predominantly caused by inflammation, though often underreported.32
- Diarrheal diseases (DD): symptom of irritation, Crohn’s disease, and other gastrointestinal illnesses linked to inflammation and which often display inflammatory markers.33
- Incidents of self-harm (SH): Research has found evidence correlating chronic inflammation with extreme depressive states, measured in this case by incidents of self-harm.5,34
The conditions for a contrast group consist of a common disease whose incidence is not directly increased by preexisting inflammatory levels that is internationally recognized and tracked across the majority of the world.23
- Tuberculosis (TB): Prevalent around the world and possessing dynamic variables for infection, tuberculosis’ complex etiology and lack of clear causal relationship from chronic inflammation make it a viable contrast group to test correlation.35 Though TB eventually produces inflammatory responses, it is an infectious disease whose communicability and virulence have not been directly associated with preexisting inflammation levels. Further, the early stages of the disease are marked by inflammatory-suppressive mediators from Mycobacterium tuberculosis, making inflammation an unlikely contributing factor.36
In order to account for variances in violence and disease relative to poverty, all compared records are divided into five socio-demographic index groupings: Low, Low-Middle, Middle, High-Middle, and High. The socio-demographic index (SDI) is a summary measure of a region’s socio-demographic development. It is based on average income per person, educational attainment, and total fertility rate. This is crucial due to the differing levels of healthcare available relative to socioeconomic position. Correlation is considered plausible when the majority of SDI groups demonstrate a statistically significant pattern in common between a given inflammatory condition and violence, AND this correlation differs significantly from the majority of the SDI groups of the contrast group.
Correlation
The primary method for establishing correlation is comparing records of incidence rates for each inflammatory condition from 1990 to 2017, as reported by the Global Burden of Disease Collaborative Network, composed of data from 786 global regions.26 Rates of change are the preferred metrics, given that they lend themselves to identifying patterns irrespective of starting positions. Rates of change were calculated for each annual period, based on comparisons with the prior year’s incidence rates of the given condition or contrast group. Therefore, the effective range of the data spans from 1991 to 2017. Average incidence values will be compared to each condition and the contrast group. In order to capture changing trends rather than lingering effects of previous health crises, a focus was placed on changes in incidence rates per 10,000, rather than on overall prevalence rates.
Comparisons will be calculated using the Pearson correlation coefficient, a method used to determine the potential relationship between two datasets.37 The correlation coefficient ranges from −1 to 1. A value of 1 implies that a linear equation describes the relationship between X and Y perfectly, with all data points lying on a line for which Y increases as X increases. A value of −1 implies that all data points lie on a line for which Y decreases as X increases. A value of 0 implies that there is no linear correlation between the variables.38
The primary confounding variable that has a relationship to both the dependent variable (violent incidents) and the independent variable (inflammatory diseases) is poverty. Poverty could make both untreated, non-communicable diseases more prevalent and violent crime more pervasive. If associations between inflammatory diseases and violence are evident solely in lower SDI groups, then it is possible that the confounding variable has not been controlled for.
Results
Incidence Data by SDI Group
Tables 1–5 reflect the rates of change in incidence levels for various illnesses between the year listed and the preceding year. This focus on rates of change is intended to isolate shifting patterns rather than simple similarities in aggregate numbers. Illnesses that shift in similar patterns during similar timeframes can reasonably said to be correlated.
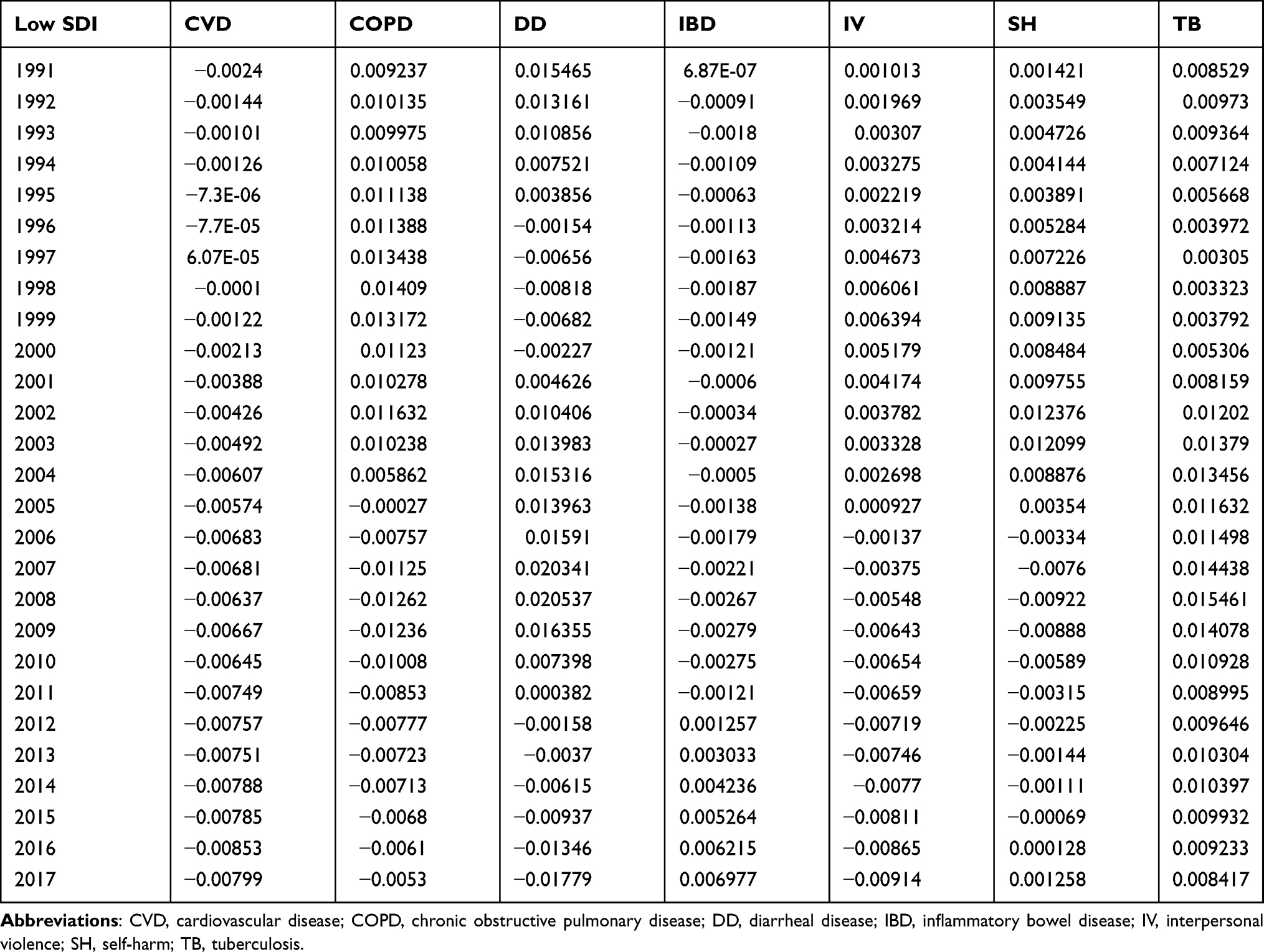 |
Table 1 Chart of the Rates of Change for Conditions and Contrast Group from 1991 to 2016 for Results in the Low Socio-Demographic Index |
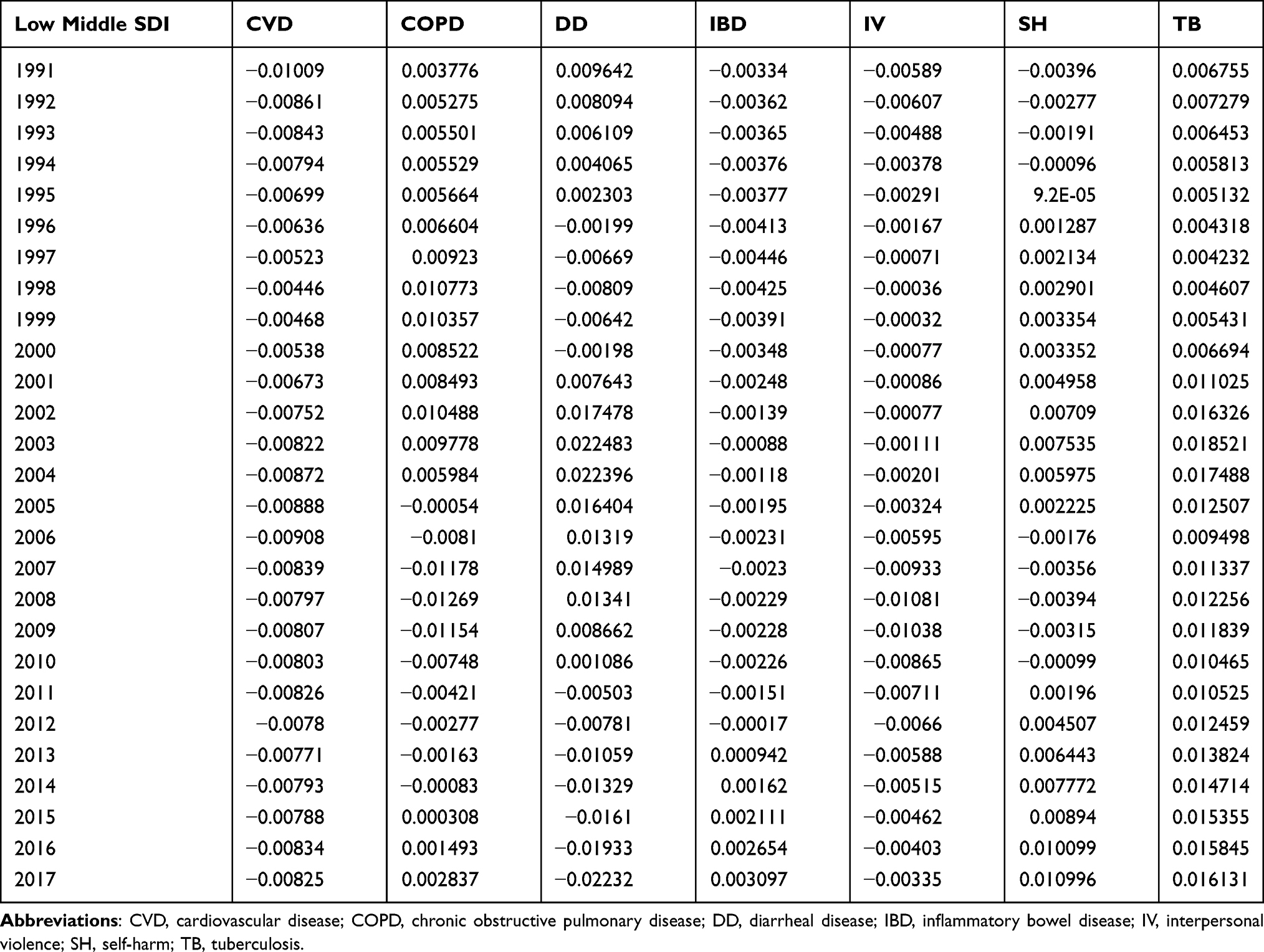 |
Table 2 Chart of the Rates of Change for Conditions and Contrast Group from 1991 to 2016 for Results in the Low-Middle Socio-Demographic Index |
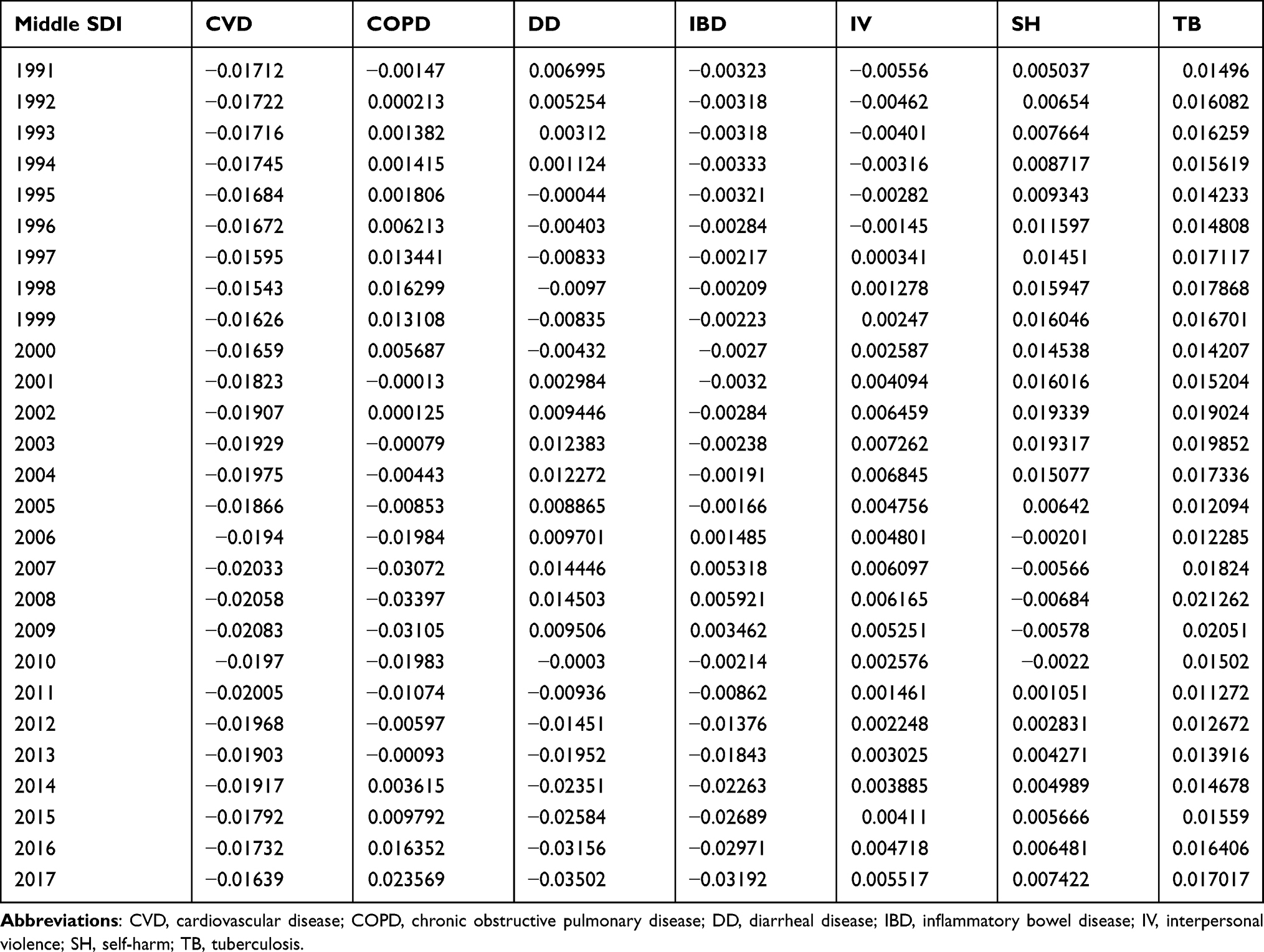 |
Table 3 Chart of the Rates of Change for Conditions and Contrast Group from 1991 to 2016 for Results in the Middle Socio-Demographic Index |
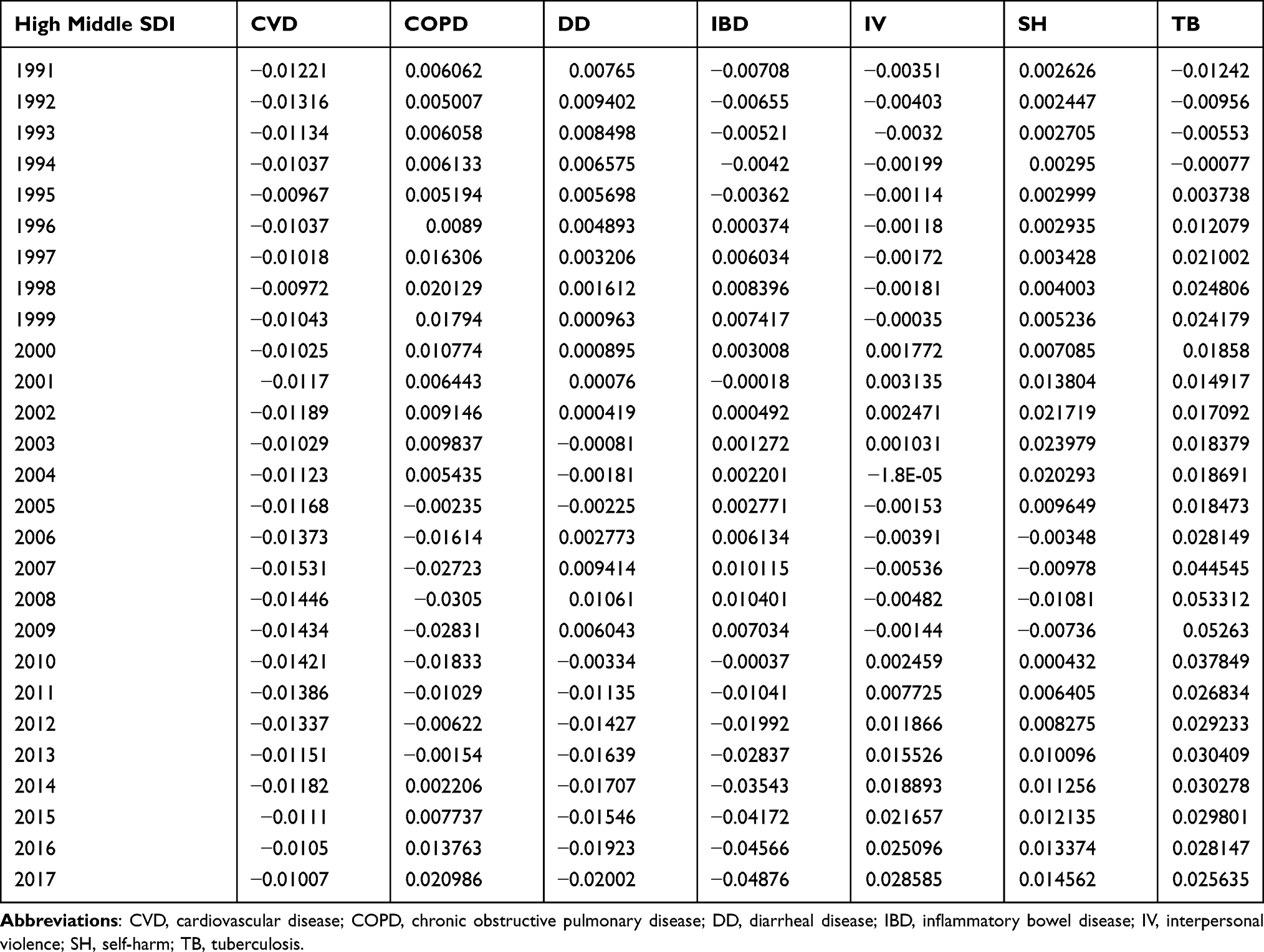 |
Table 4 Chart of the Rates of Change for Conditions and Contrast Group from 1991 to 2016 for Results in the Middle-High Socio-Demographic Index |
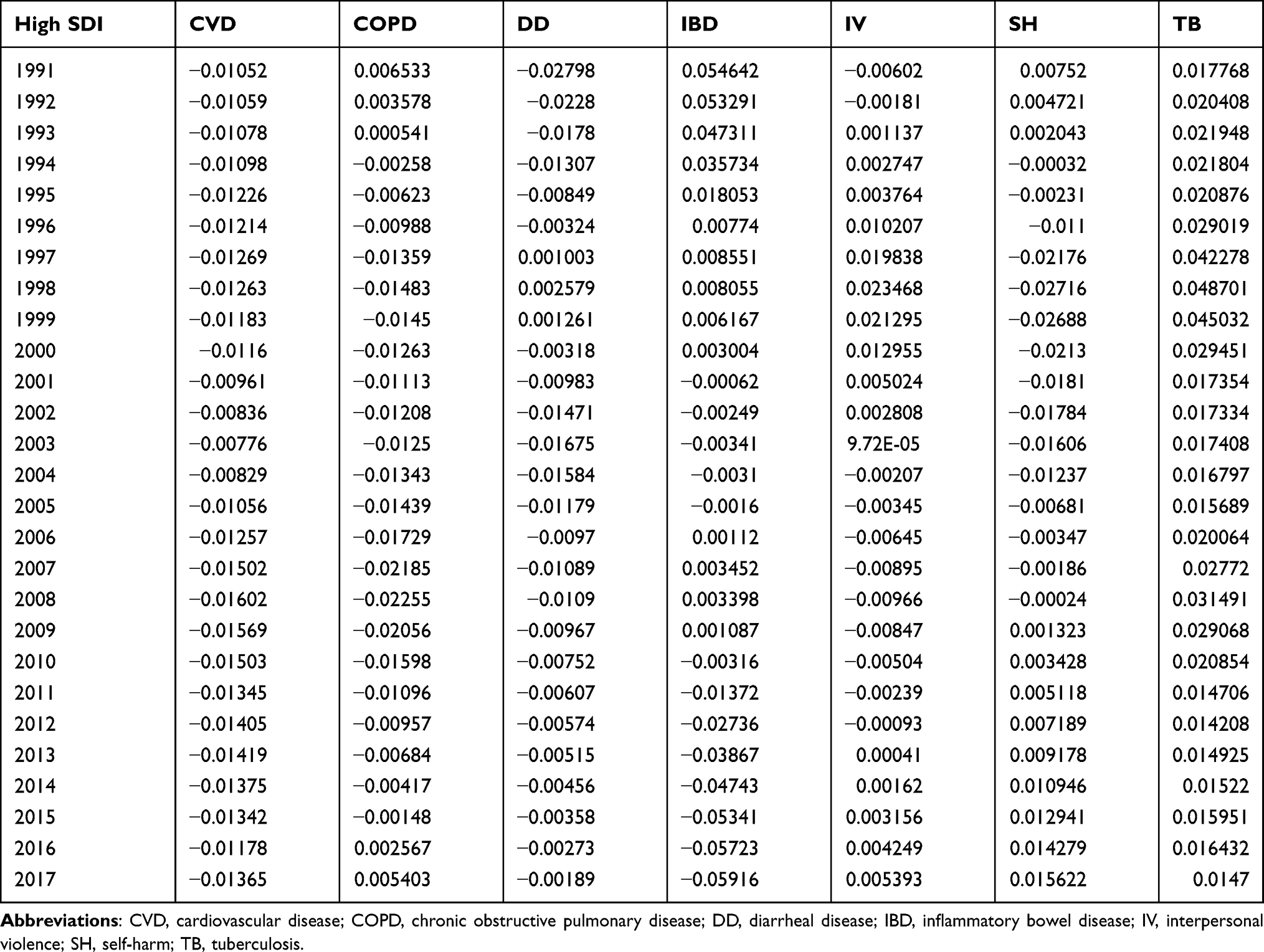 |
Table 5 Chart of the Rates of Change for Conditions and Contrast Group from 1991 to 2016 for Results in the High Socio-Demographic Index |
Correlation Data by SDI Group
After being divided into 5 SDI groups, average incidence rate of change (RoC) values were compared to each condition and the contrast group using the Pearson correlation coefficient (Tables 6–10). This tracks how closely changes in one value are reflected in another value, suggesting a correlation between the two. As noted above, a value of 1 implies that a linear equation describes the relationship between X and Y perfectly, with all data points lying on a line for which Y increases as X increases. A value of −1 implies that all data points lie on a line for which Y decreases as X increases. A value of 0 implies that there is no linear correlation between the variables. The results were then charted and graphed (Figures 2–6).
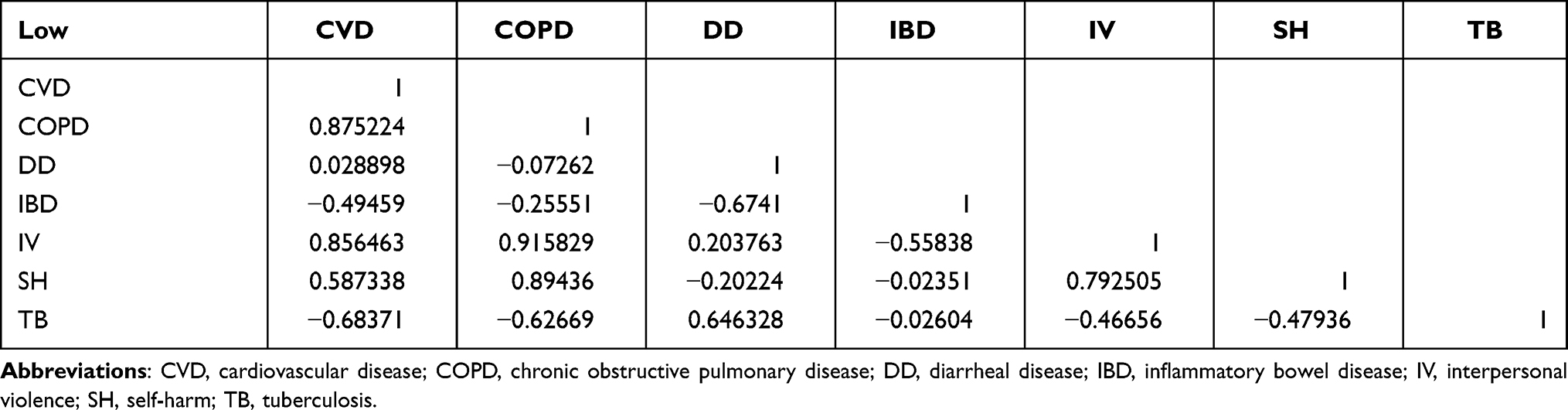 |
Table 6 Pearson Correlation Values Within the Low Socio-Demographic Index |
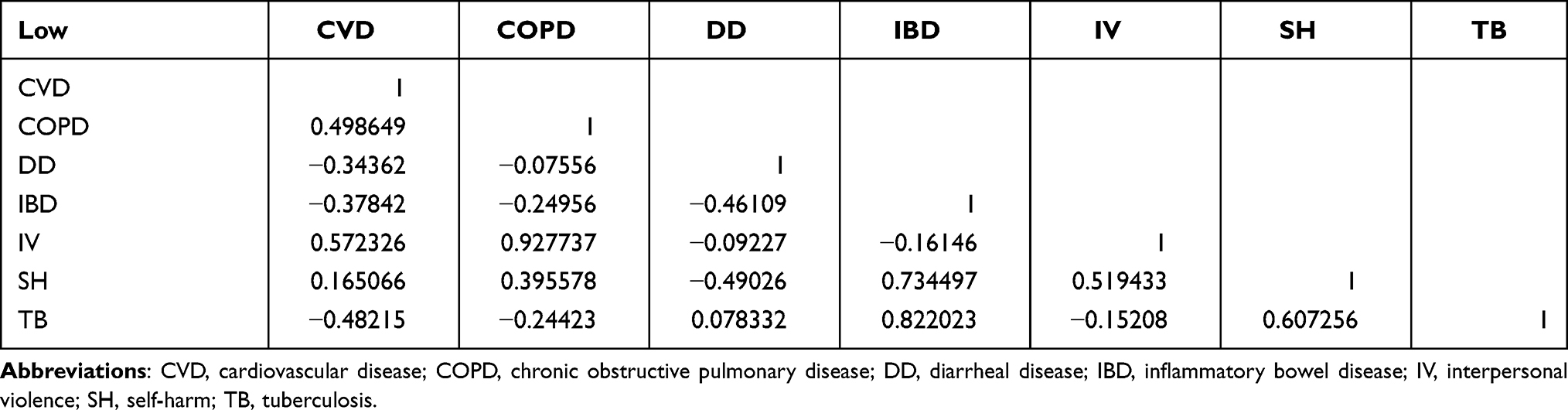 |
Table 7 Pearson Correlation Values Within the Middle-Low Socio-Demographic Index |
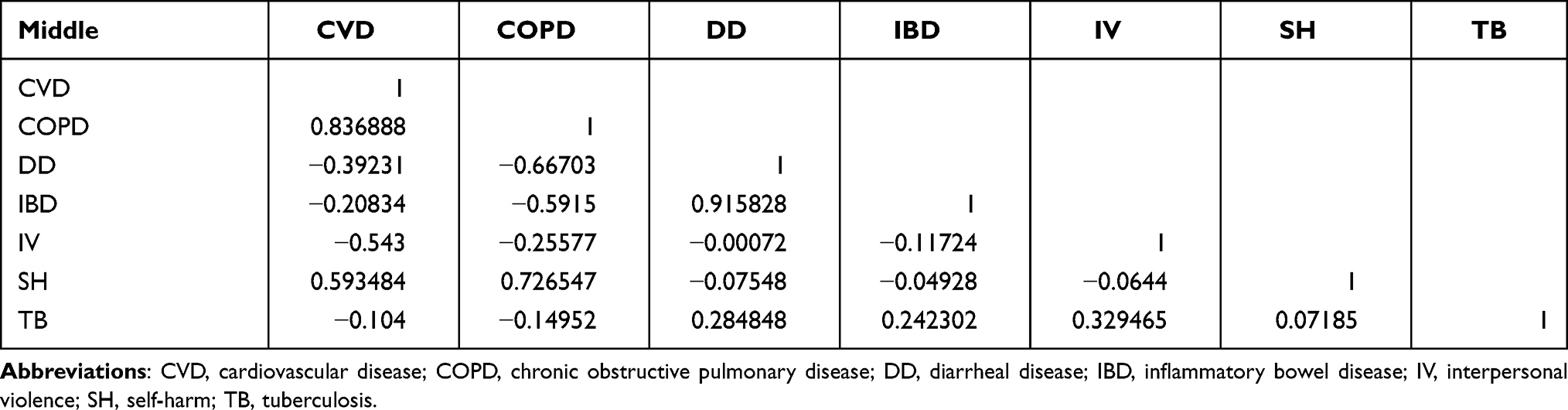 |
Table 8 Pearson Correlation Values Within the Middle Socio-Demographic Index |
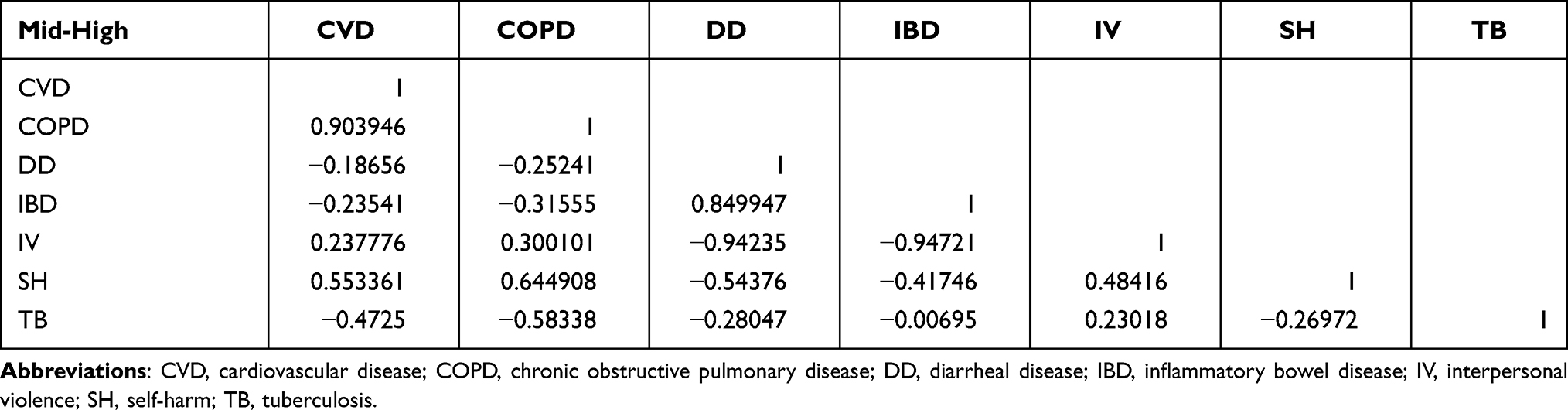 |
Table 9 Pearson Correlation Values Within the Middle-High Socio-Demographic Index |
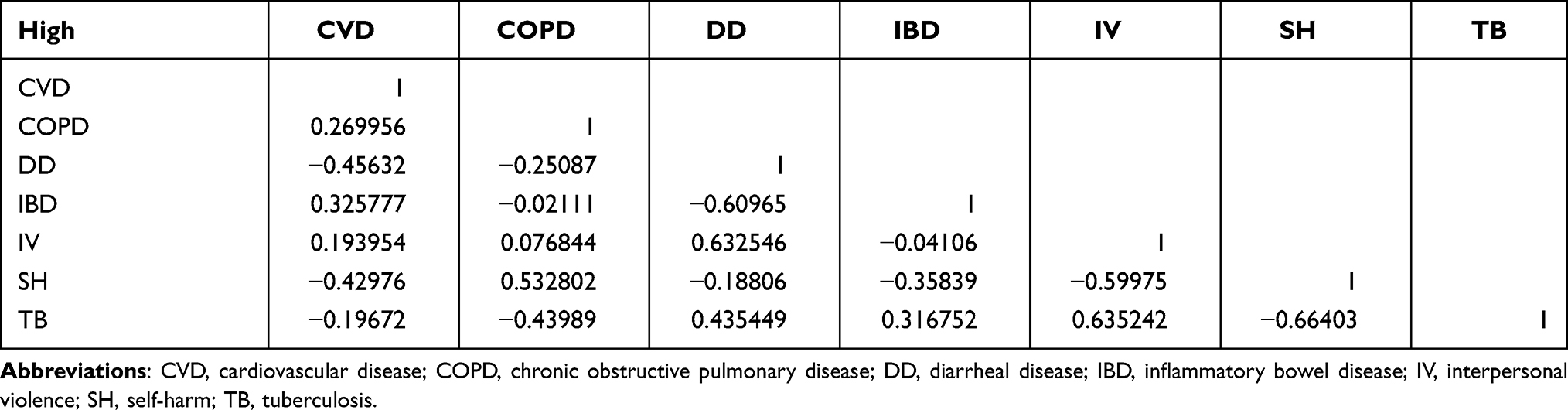 |
Table 10 Pearson Correlation Values Within the High Socio-Demographic Index |
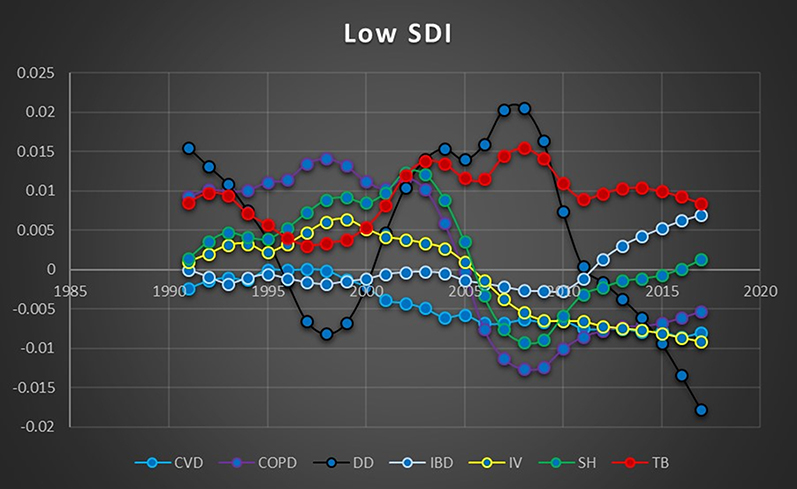 |
Figure 2 Pearson correlation graph within the Low socio-demographic index. Abbreviations: CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; DD, diarrheal disease; IBD, inflammatory bowel disease; IV, interpersonal violence; SH, self-harm; TB, tuberculosis. |
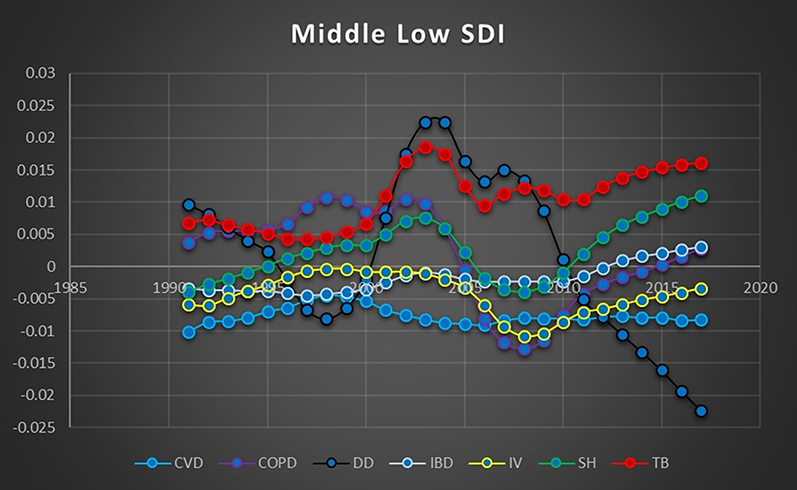 |
Figure 3 Pearson correlation graph within the Middle-Low socio-demographic index. Abbreviations: CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; DD, diarrheal disease; IBD, inflammatory bowel disease; IV, interpersonal violence; SH, self-harm; TB, tuberculosis. |
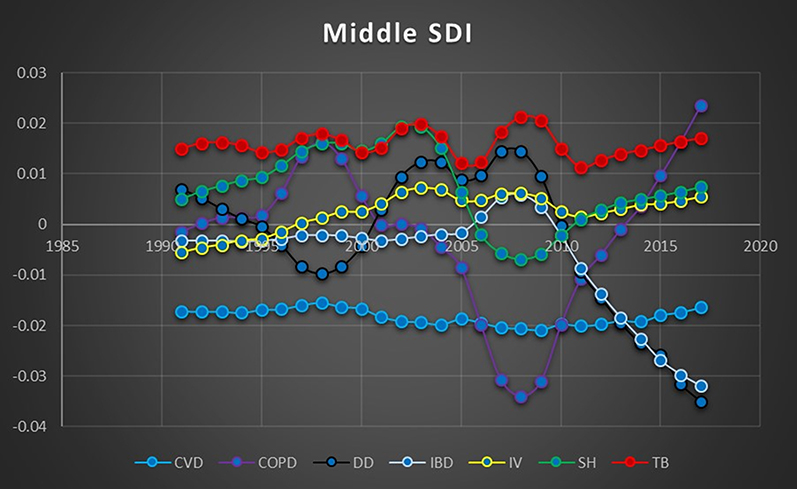 |
Figure 4 Pearson correlation graph within the Middle socio-demographic index. Abbreviations: CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; DD, diarrheal disease; IBD, inflammatory bowel disease; IV, interpersonal violence; SH, self-harm; TB, tuberculosis. |
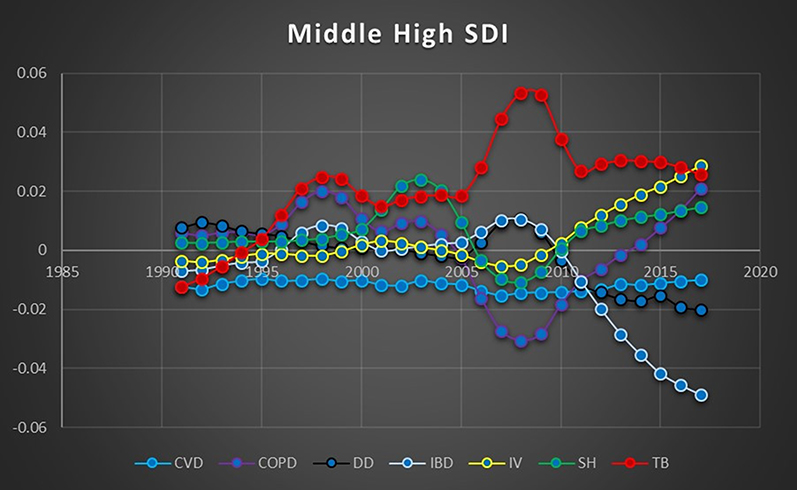 |
Figure 5 Pearson correlation graph within the Middle-High socio-demographic index. Abbreviations: CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; DD, diarrheal disease; IBD, inflammatory bowel disease; IV, interpersonal violence; SH, self-harm; TB, tuberculosis. |
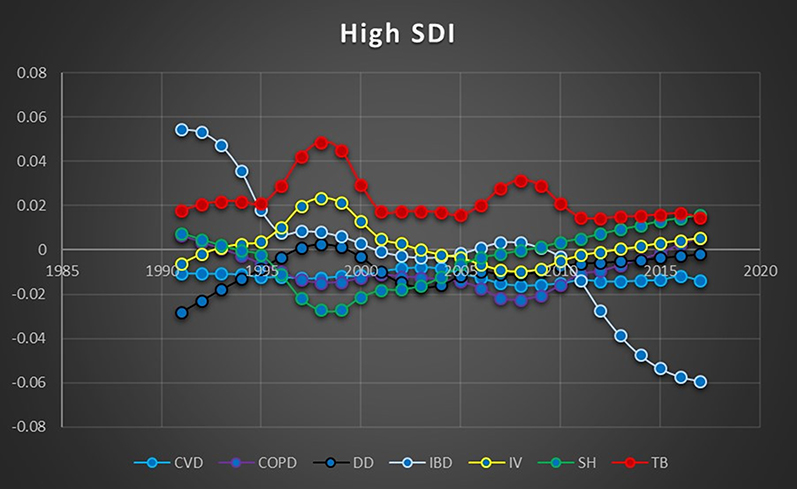 |
Figure 6 Pearson correlation graph within the High socio-demographic index. Abbreviations: CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; DD, diarrheal disease; IBD, inflammatory bowel disease; IV, interpersonal violence; SH, self-harm; TB, tuberculosis. |
Analysis
The results of the correlational calculations were examined for connections between inflammatory conditions and interpersonal violence. The categorization was performed in accordance with common Pearson coefficient guidelines.35
- Inverse: −0.1 to −1
- Negligible: −0.09 to 0.09
- Weak: 0.1 to 0.3
- Medium: 0.3 to 0.5
- Strong: 0.5 to 1
In the low socio-demographic index inflammatory conditions were correlated with interpersonal violence 80% of the time, detailed as follows:
- 60% of inflammatory conditions showed a strong correlation with interpersonal violence.
- 0% of inflammatory conditions showed a medium correlation with interpersonal violence.
- 20% of inflammatory conditions showed a weak correlation with interpersonal violence.
- 0% of inflammatory conditions showed negligible correlation.
- 20% of inflammatory conditions showed an inverse association with interpersonal violence.
- The contrast group showed an inverse association with interpersonal violence.
In the middle-low socio-demographic index inflammatory conditions were correlated with interpersonal violence 60% of the time, detailed as follows:
- 60% of inflammatory conditions showed a strong correlation with interpersonal violence.
- 0% of inflammatory conditions showed a medium correlation with interpersonal violence.
- 0% of inflammatory conditions showed a weak correlation with interpersonal violence.
- 20% of inflammatory conditions showed negligible correlation.
- 20% of inflammatory conditions showed an inverse association with interpersonal violence.
- The contrast group showed an inverse association with interpersonal violence.
In the middle socio-demographic index inflammatory conditions were correlated with interpersonal violence 0% of the time, detailed as follows:
- 0% of inflammatory conditions showed a strong correlation with interpersonal violence.
- 0% of inflammatory conditions showed a medium correlation with interpersonal violence.
- 0% of inflammatory conditions showed a weak correlation with interpersonal violence.
- 40% of inflammatory conditions showed negligible correlation.
- 60% of inflammatory conditions showed an inverse association with interpersonal violence.
- The contrast group showed a medium correlation with interpersonal violence.
In the middle-high socio-demographic index inflammatory conditions were correlated with interpersonal violence 60% of the time, detailed as follows:
- 0% of inflammatory conditions showed a strong correlation with interpersonal violence.
- 40% of inflammatory conditions showed a medium correlation with interpersonal violence.
- 20% of inflammatory conditions showed a weak correlation with interpersonal violence.
- 0% of inflammatory conditions showed negligible correlation.
- 40% of inflammatory conditions showed an inverse association with interpersonal violence.
- The contrast group showed a medium correlation with interpersonal violence.
In the high socio-demographic index inflammatory conditions were correlated with interpersonal violence 40% of the time, detailed as follows:
- 20% of inflammatory conditions showed a strong correlation with interpersonal violence.
- 0% of inflammatory conditions showed a medium correlation with interpersonal violence.
- 20% of inflammatory conditions showed a weak correlation with interpersonal violence.
- 40% of inflammatory conditions showed negligible correlation.
- 20% of inflammatory conditions showed an inverse association with interpersonal violence.
- The contrast group showed a strong correlation with interpersonal violence.
Discussion
The Low SDI group showed the strongest association between violence and inflammatory conditions, and also tends to have the lowest quality healthcare. This suggests that untreated, unchecked inflammatory conditions might lead to a higher level of aggression and violent incidents. The correlation rate gradually declined as socio-demographic status improved, further supporting the idea that effective inflammatory intervention might interrupt the cycle of inflammatory cascades and increasing aggression. It is likely that the stronger societal infrastructures of higher SDI groups also decrease the rate of violence, but it is unclear how this impacts the correlations found with inflammatory conditions.
It is notable that the Middle SDI group is distinct from the other groups due to the fact that it does not exhibit any of the patterns seen in the others. The reasons behind this are unclear, but it may be that the heterogeneous nature of income and quality of life within Middle SDI groups lends itself to such uneven levels of public health that meaningful patterns are difficult to isolate. Other research involving noncommunicable diseases and SDI groups suggests economic development, industrial outsourcing, social mobility, and unequal environmental conditions create unpredictable conditions.39 Given this potential phenomenon, it is not clear if this group should be considered as an outlier; if it were, then the average correlation rate between inflammatory conditions and violence would be significantly higher.
Conclusions
The majority of socio-demographic groups showed a significant correlation between rates of change in incidence of violence and inflammatory conditions. This correlation was not found with a similar frequency or strength in the contrast group. Given that chronic inflammation is linked to aggressive episodes, there is evidence that persistent inflammation is a contributing factor to interpersonal violence. The long onset time of chronic inflammation makes the inverse causality highly unlikely, at least within the same year. The fact that correlation persisted across nearly every socio-demographic group suggests the confounder has been effectively controlled for and the association between inflammatory diseases and violence reflects an actual relationship. Based on these results it is reasonable to conclude that the hypothesis is plausible.
Implications
The potential significance of these relationships could extend beyond adding another layer to the complexity of biopsychosocial behavior. A connection between inflammatory illnesses and aggression and/or violence lends further evidence to the overlap between public health and public safety. The burden of chronic disease could be viewed as a matter involving multiple sectors of society, possibly influencing resource allocations and informing systemic social reforms.
The correlations themselves have possible significance. The strong correlation between violence and self-harm supports the research indication inflammation contributes to both aggression and depression. Leveraging these influences could have multiple benefits. If increased inflammation contributes to increased violence, it follows that decreased inflammation might lead to decreased violence, which could also decrease rates of self-harm and suicide.
In addition to being valuable for development of health policies concerning psychosocial medicine, these findings improve understanding of the full scope of “mind-body” dynamics, both in health and sickness. Extrapolating broad patterns in societal behavior from small-scale inflammation studies supports leveraging clinical inflammation research for public health purposes. Further research in this field is warranted, preferably with more detailed RCT studies.
Limitations
The relationships established in this study are correlational but have not yet been established as causal. Various points of ambiguity in the study warrant deeper investigation and clarification. There are multiple factors tied to inflammatory status beyond chronic illness, especially diet and obesity. There are likewise multiple factors tied to incidents of violence beyond inflammatory influences, such as poverty, geography, corruption, and local conflict. Although certain inflammatory diseases such as osteoarthritis were excluded due to limiting factors relating to violence, further studies should examine illnesses like these to assess other behavioral and quality of life metrics that may be impacted.
Future studies are needed to isolate these influences to determine the existence and effect size of any causal relationship.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hunter P. The inflammation theory of disease: the growing realization that chronic inflammation is crucial in many diseases opens new avenues for treatment. EMBO Rep. 2012;13(11):968–970. doi:10.1038/embor.2012.142
2. Libby P. Inflammatory mechanisms: the molecular basis of inflammation and disease. Nutr Rev. 2007;65(12 Pt 2):S140–146. doi:10.1301/nr.2007.dec.S140-S146
3. Raison CL, Borisov AS, Woolwine BJ, Massung B, Vogt G, Miller AH. Interferon-alpha effects on diurnal hypothalamic-pituitary-adrenal axis activity: relationship with proinflammatory cytokines and behavior. Mol Psychiatry. 2010;15(5):535–547. doi:10.1038/mp.2008.58
4. Kraus MR, Schafer A, Faller H, Csef H, Scheurlen M. Psychiatric symptoms in patients with chronic hepatitis C receiving interferon alfa-2b therapy. J Clin Psychiatry. 2003;64(6):708–714. doi:10.4088/JCP.v64n0614
5. Constant A, Castera L, Dantzer R, et al. Mood alterations during interferon-alfa therapy in patients with chronic hepatitis C: evidence for an overlap between manic/hypomanic and depressive symptoms. J Clin Psychiatry. 2005;66(8):1050–1057. doi:10.4088/JCP.v66n0814
6. Zalcman SS, Siegel A. The neurobiology of aggression and rage: role of cytokines. Brain Behav Immun. 2006;20(6):507–514. doi:10.1016/j.bbi.2006.05.002
7. Graham JE, Robles TF, Kiecolt-Glaser JK, Malarkey WB, Bissell MG, Glaser R. Hostility and pain are related to inflammation in older adults. Brain Behav Immun. 2006;20(4):389–400. doi:10.1016/j.bbi.2005.11.002
8. Coccaro EF. Association of C-reactive protein elevation with trait aggression and hostility in personality disordered subjects: a pilot study. J Psychiatr Res. 2006;40(5):460–465. doi:10.1016/j.jpsychires.2005.04.005
9. Marsland AL, Prather AA, Petersen KL, Cohen S, Manuck SB. Antagonistic characteristics are positively associated with inflammatory markers independently of trait negative emotionality. Brain Behav Immun. 2008;22(5):753–761. doi:10.1016/j.bbi.2007.11.008
10. Coccaro EF, Lee R, Coussons-Read M. Elevated plasma inflammatory markers in individuals with intermittent explosive disorder and correlation with aggression in humans. JAMA Psychiatry. 2014;71(2):158–165. doi:10.1001/jamapsychiatry.2013.3297
11. Coccaro EF, Lee RJ, Kavoussi RJ. A double-blind, randomized, placebo-controlled trial of fluoxetine in patients with intermittent explosive disorder. J Clin Psychiatry. 2009;70(5):653–662. doi:10.4088/JCP.08m04150
12. Raison CL, Borisov AS, Woolwine BJ, Massung B, Vogt G, Miller AH. Interferon-alpha effects on diurnal hypothalamic-pituitary-adrenal axis activity: relationship with proinflammatory cytokines and behavior. Mol Psychiatry. 2010;15(5):535–547. doi:10.1038/mp.2008.58
13. Bhatt S, Bhatt R, Zalcman SS, Siegel A. Role of IL-1 beta and 5-HT2 receptors in midbrain periaqueductal gray (PAG) in potentiating defensive rage behavior in cat. Brain Behav Immun. 2008;22(2):224–233. doi:10.1016/j.bbi.2007.07.011
14. Patel A, Siegel A, Zalcman SS. Lack of aggression and anxiolytic-like behavior in TNF receptor (TNF-R1 and TNF-R2) deficient mice. Brain Behav Immun. 2010;24(8):1276–1280. doi:10.1016/j.bbi.2010.05.005
15. Pesce M, Speranza L, Franceschelli S, et al. Biological role of interleukin-1beta in defensive-aggressive behaviour. J Biol Regul Homeost Agents. 2011;25(3):323–329.
16. Suarez EC. Joint effect of hostility and severity of depressive symptoms on plasma interleukin-6 concentration. Psychosom Med. 2003;65(4):523–527. doi:10.1097/01.PSY.0000062530.94551.EA
17. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805–1812. doi:10.1172/JCI200318921
18. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741. doi:10.1016/j.biopsych.2008.11.029
19. Boylan JM, Ryff CD. Varieties of anger and the inverse link between education and inflammation: toward an integrative framework. Psychosom Med. 2013;75(6):566–574. doi:10.1097/PSY.0b013e31829683bd
20. Rakovec-Felser Z. The biopsychosocial model of treatment the patients with inflammatory chronic bowel disease. Coll Antropol. 2011;35(2):453–461.
21. Gross R, Groer M, Thomas SP. Relationship of trait anger and anger expression to C-reactive protein in postmenopausal women. Health Care Women Int. 2014;35(5):580–595. doi:10.1080/07399332.2013.862798
22. Kessler RC, Coccaro EF, Fava M, Jaeger S, Jin R, Walters E. The prevalence and correlates of DSM-IV intermittent explosive disorder in the national comorbidity survey replication. Arch Gen Psychiatry. 2006;63(6):669–678. doi:10.1001/archpsyc.63.6.669
23. Global burden of disease study 2016 (GBD 2016) data input sources tool. GHDx. Available from: http://ghdx.healthdata.org/gbd-2016/data-input-sources?components=3&causes=724.
24. Alexandra CH, Nowakowski KY, Sumerau JE. Mediation analysis of relationships between chronic inflammation and quality of life in older adults. Health Qual Life Outcomes. 2016;14(1):46. doi:10.1186/s12955-016-0452-4
25. Alexandra CH. Chronic inflammation and quality of life in older adults: a cross-sectional study using biomarkers to predict emotional and relational outcomes. Health Qual Life Outcomes. 2014;12(1):141. doi:10.1186/s12955-014-0141-0
26. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2016 (GBD 2016) Socio-Demographic Index (SDI) 1970–2016. Seattle, United States: Institute for Health Metrics and Evaluation (IHME); 2017.
27. Kassebaum NJ, Arora M, Barber RM, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–1658. doi:10.1016/S0140-6736(16)31460-X
28. Golia E, Limongelli G, Natale F. Inflammation and cardiovascular disease: from pathogenesis to therapeutic target. Curr Atheroscler Rep. 2014;16(9):435. doi:10.1007/s11883-014-0435-z
29. Raggi P, Genest J, Giles JT. Role of inflammation in the pathogenesis of atherosclerosis and therapeutic interventions. Atherosclerosis. 2018;276:98–108. doi:10.1016/j.atherosclerosis.2018.07.014
30. Natalie E. Heart under attack: cardiac manifestations of inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(11):2322–6. doi:10.1093/ibd/izy157
31. Cavaillès A, Brinchault-Rabin G, Dixmier A. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. doi:10.1183/09059180.00008612
32. Zhang Y-Z, Yong-Yu L. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 2014;20(1):91–99. doi:10.3748/wjg.v20.i1.91
33. Paweł W, Paradowski L. Stool patterns and symptoms of disordered anorectal function in patients with inflammatory bowel diseases. Adv Clin Exp Med. 2018;27(6):813–818. doi:10.17219/acem/68986
34. Hawton K, Casañas I Comabella C, Haw C, Saunders K. Risk factors for suicide in individuals with depression: a systematic review. J Affect Disord. 2013;147(1–3):17–28. doi:10.1016/j.jad.2013.01.004
35. Dubovsky H. A historical basis for modern concepts of the pathogenesis of tuberculosis. S Afr Med J. 1975;49(27):1105–1110.
36. Sasindran SJ, Torrelles JB. Mycobacterium tuberculosis infection and inflammation: what is beneficial for the host and for the bacterium? Front Microbiol. 2011;2:2. doi:10.3389/fmicb.2011.00002
37. Pearson product-moment correlation - when you should run this test, the range of values the coefficient can take and how to measure strength of association. Available from: https://statistics.laerd.com/statistical-guides/pearson-correlation-coefficient-statistical-guide.php.
38. Weisstein EW. Statistical correlation. Available from: https://mathworld.wolfram.com/StatisticalCorrelation.html.
39. Wang Z, Hu L, Li J, Wei L, Zhang J, Zhou J. Magnitude, temporal trends and inequality in global burden of tracheal, bronchus and lung cancer: findings from the Global Burden of Disease Study 2017. BMJ Glob Health. 2020;5(10):e002788. doi:10.1136/bmjgh-2020-002788
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.