Back to Journals » Journal of Inflammation Research » Volume 19
Glasgow Prognostic Score Predicts Hepatic Recompensation in Decompensated Primary Biliary Cholangitis: A Multicenter Cohort Study
Authors Huang M, Dai A, Gao L, Wu C, Zou W, Duan D, Niu J, Tang Y, Yang J, Lei H ![]()
Received 20 February 2026
Accepted for publication 25 April 2026
Published 4 June 2026 Volume 2026:19 601389
DOI https://doi.org/10.2147/JIR.S601389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Fatih Türker
Man Huang,1,2,* An Dai,3,* Liufei Gao,4,* Changhui Wu,5 Wen Zou,6 De Duan,7 Junkun Niu,8 Yuan Tang,9 Jinhui Yang,10 Hongtao Lei1
1School of Public Health & School of Basic Medical Sciences, Kunming Medical University, Kunming, Yunnan, 650500, People’s Republic of China; 2Shangluo Vocational and Technical College, Shangluo, Shaanxi, 726000, People’s Republic of China; 3The People’s Hospital of Xishuangbanna Dai Nationality Autonomous Prefecture, Xishuangbanna, Yunnan, 666100, People’s Republic of China; 4Hospital Office, The Second People’s Hospital of Qujing, Qujing, Yunnan, 655000, People’s Republic of China; 5Department of Infectious Diseases and Liver Diseases, Yunnan Second People’s Hospital, Kunming, Yunnan, 650101, People’s Republic of China; 6Department of Gastroenterology, Yuxi People’s Hospital, Yuxi, Yunnan, 653100, People’s Republic of China; 7Department of Gastroenterology, Dali Prefecture People’s Hospital, Dali, Yunnan, 671099, People’s Republic of China; 8Department of Gastroenterology, The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650032, People’s Republic of China; 9Department of Gastroenterology, Qujing City Central Hospital, Qujing, Yunnan, 655000, People’s Republic of China; 10Department of Gastroenterology, The Second Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, 650101, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan Tang, Department of Gastroenterology, Qujing City Central Hospital, No. 1, Yuanlin Road, Nanning Subdistrict, Qilin District, Qujing, Yunnan, 655000, People’s Republic of China, Email [email protected] Hongtao Lei, School of Public Health, Kunming Medical University, No. 1168, Yu Hua Street, Chenggong District, Kunming, Yunnan, 650500, People’s Republic of China, Email [email protected]
Background: Chronic liver disease progression is closely linked to systemic inflammatory responses and nutritional status. This study aimed to evaluate the prognostic value of the Glasgow Prognostic Score (GPS) system for predicting recompensation in patients with decompensated primary biliary cholangitis (PBC).
Methods: This multicenter, retrospective cohort study enrolled patients with decompensated PBC admitted to seven hospitals between January 2014 and December 2023. The GPS, mGPS, and hs-mGPS were determined according to baseline CRP, hs-CRP, and ALB levels. The primary endpoint was the achievement of recompensation during follow-up (defined as biochemical response to UDCA, resolution of decompensating events, and stable improvement in liver function per Baveno VII criteria).
Results: Of the 504 patients with decompensated PBC analyzed, the median age was 62 years (IQR: 53– 69) and 81.5% (n=411) were women. Over a median follow-up of 31 months (IQR: 14– 56), recompensation occurred in 136 patients (27.0%). Kaplan-Meier analysis confirmed that higher GPS, mGPS, and hs-mGPS scores were associated with lower 5-year recompensation rates (all P < 0.0001). Cox regression analysis revealed that in the fully adjusted model, GPS (HR: 0.311, 95% CI: 0.219– 0.444), mGPS (HR: 0.302, 95% CI: 0.188– 0.487), and hs-mGPS (HR: 0.351, 95% CI: 0.248– 0.496) were all independent predictors for recompensation. Time-dependent ROC analysis showed that the AUCs for predicting recompensation were 0.888 for GPS, 0.795 for mGPS, and 0.871 for hs-mGPS, indicating the best predictive performance for GPS. Sensitivity and subgroup analyses confirmed the robustness of these findings.
Conclusion: The GPS and its variants reliably predict recompensation in decompensated PBC, with the GPS showing superior accuracy. These tools can stratify risk and inform early intervention strategies.
Keywords: primary biliary cholangitis, decompensated cirrhosis, Glasgow Prognostic Score, predictive value
Introduction
Primary biliary cholangitis (PBC) is a chronic autoimmune-mediated liver disease characterized by the progressive, non-suppurative inflammatory destruction of the small intrahepatic bile ducts.1 Ursodeoxycholic acid (UDCA) is the current standard first-line pharmacotherapy for this condition.2 Recent studies indicate that a subset of patients with decompensated PBC can achieve a fundamental reversal of their disease status—termed “recompensation”—following UDCA therapy, which is considered a key treatment goal.3 Therefore, the early identification of patients with recompensation potential is crucial for formulating aggressive, individualized treatment plans and improving long-term outcomes.
The Model for End-Stage Liver Disease (MELD) score, which incorporates bilirubin, INR, and creatinine, is a well-established tool for predicting mortality in patients with advanced liver disease and is widely used for organ allocation in liver transplantation. However, MELD primarily reflects synthetic and excretory liver function and renal impairment, without directly capturing systemic inflammation or nutritional status—key drivers of the decompensation-recompensation continuum.4 In contrast, the Glasgow Prognostic Score (GPS) system, which assesses systemic inflammation and nutritional status based on serum albumin, C-reactive protein (CRP), and high-sensitivity CRP (hs-CRP) levels, may offer complementary prognostic information by targeting the “inflammation-nutrition” axis. PBC is intrinsically an autoimmune-mediated cholestatic liver disease, in which persistent bile duct injury and cholestasis trigger sustained systemic inflammation and progressive nutritional deterioration, making the “inflammation-nutrition” axis particularly relevant for disease monitoring and prognosis. The Glasgow Prognostic Score (GPS) system assesses systemic inflammation and nutritional status based on serum albumin (ALB), C-reactive protein (CRP), and high-sensitivity CRP (hs-CRP) levels.5 Originally developed for prognostic evaluation in malignancies,6 its use has increasingly extended to hepatology.7,8 Systemic inflammation is known to be crucial in cirrhosis progression and the decompensation/recompensation continuum.9,10 However, the predictive capacity of the GPS system for recompensation in decompensated PBC patients remains poorly defined.
To address this, we conducted a multicenter retrospective cohort study to determine the predictive value of baseline GPS, mGPS, and hs-mGPS scores for recompensation in decompensated PBC. This study seeks to provide empirical evidence to guide early risk stratification and management optimization.
Methods
Study Population
This was a multicenter retrospective cohort study. Between January 2014 and December 2023, a total of 735 patients with decompensated PBC were enrolled from seven participating hospitals, and their clinical data were retrospectively reviewed. The last follow-up date was December 31, 2024. Patient distribution across the centers was as follows (Figure 1): The Second Affiliated Hospital of Kunming Medical University (n=473), The First Affiliated Hospital of Kunming Medical University (n=129), Qujing First People’s Hospital (n=33), The Affiliated Hospital of Yunnan University (n=40), Qujing Second People’s Hospital (n=23), Yuxi People’s Hospital (n=22), and Dali Prefecture People’s Hospital (n=15). This study was conducted after obtaining approval from the Ethics Committee of Kunming Medical University (Approval No.: KMMU2025MEC155) and adhered strictly to the ethical tenets of the Declaration of Helsinki.
 |
Figure 1 Flowchart of participant selection. |
Inclusion Criteria
PBC was diagnosed according to the established guidelines from the European Association for the Study of the Liver (EASL)11,12 and the British Society of Gastroenterology/UK-PBC.13 Decompensation was characterized by the occurrence of at least one decompensating event, such as ascites, hepatic encephalopathy, or variceal hemorrhage.14
Exclusion Criteria
1) Concomitant other major liver diseases, including viral hepatitis, alcoholic liver disease, or autoimmune hepatitis-PBC overlap syndrome; 2) Comorbid malignancies or active infections; 3) Lack of standardized ursodeoxycholic acid therapy for over 12 months; 4) Previous use of corticosteroids, immunosuppressants, or albumin preparations; 5) Incomplete clinical follow-up data.For the three key variables required for GPS calculation (CRP, hs-CRP, and albumin), patients with any missing values for these parameters were excluded from the analysis. All other clinical variables in the included patients had no missing data.
GPS, mGPS, and Hs-mGPS Scores
We derived the original GPS, mGPS, and hs-mGPS from baseline CRP, hs-CRP, and ALB levels. The specific cutoff values and criteria for score assignment are provided in Table 1.5
 |
Table 1 Scoring Criteria for the GPS, mGPS, and Hs-mGPS |
Outcomes
The primary outcome was defined as the achievement of recompensation within the follow-up period. Recompensation was defined per the Baveno VII consensus15 and EASL clinical practice guidelines,11,12 requiring the simultaneous fulfillment of all three of the following criteria: a) Successful Etiological Treatment: Response to ursodeoxycholic acid, defined as achieving an alkaline phosphatase level under 1.67 times the upper limit of normal following 12 months of treatment. b) Resolution of Decompensating Events: Control of ascites (disappearance after diuretic withdrawal), absence of hepatic encephalopathy recurrence after discontinuing lactulose/rifaximin, and no variceal hemorrhage recurrence for at least 12 months. c) Consistent and stable improvement in liver function (ALB > 35 g/L, INR < 1.50, TBIL < 34 μmol/L).
Treatment Protocol
All patients received ursodeoxycholic acid (UDCA) at a standardized dose of 13–15 mg·kg−1·d−1 for at least 12 months, consistent with international guidelines.13 Patients with documented poor adherence (based on medical and pharmacy record review) were excluded from the study. All included patients were UDCA-naïve at baseline. The decision to initiate second-line therapies was made by treating physicians according to clinical judgment of inadequate response to UDCA, following guideline-directed care.
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 and R version 4.5.1. Continuous variables exhibiting skewed distributions are summarized as median with interquartile range (IQR), and between-group comparisons were made using the Mann–Whitney U-test. Categorical variables are presented as numbers (percentages), with comparisons conducted via the Chi-square test or Fisher’s exact test, as appropriate. Recompensation rates were estimated using both the Kaplan-Meier method and the cumulative incidence function (CIF) accounting for death as a competing event, and inter-group differences were compared with the Log rank test. Cox regression (treating death as censored) and Fine-Gray competing-risk regression (treating death as a competing event) were performed and compared. Collinearity was evaluated by tolerance and variance inflation factor (VIF) (Table S1). Time-dependent area under the curve (AUC) for predicting recompensation was evaluated, with internal validation conducted using bootstrap resampling. We used the follow-up time from baseline (date of diagnosis of decompensation) to the occurrence of the event (recompensation) or censoring. Specifically, we employed the cumulative case/dynamic control approach for time-dependent ROC curves and evaluated the discriminative ability of the model at a fixed prediction horizon of 60 months (5 years), Corresponding areas under the curve (AUC) with 95% confidence intervals (CI) were calculated, and the DeLong test was applied for AUC comparisons across models. The robustness of key findings was assessed in subgroup analyses—stratified by MELD scores (<10 vs ≥10)—and in a sensitivity analysis that excluded patients with concomitant hypertension, arteriosclerosis, or diabetes to minimize potential confounding from medications used to manage these conditions. A two-sided P-value < 0.05 was considered statistically significant for all tests.
Results
Baseline Characteristics of the Study Population
Following the predefined screening protocol (Figure 1), a total of 504 patients with decompensated PBC were included for the analysis of baseline characteristics.The median age of the patients was 62 years (IQR: 53–69), with 411 (81.5%) being female. The median BMI was 21.64 (IQR: 19.6–23.42). As shown in Table 2, compared to the non-recompensation group, patients who achieved recompensation had significantly lower baseline levels of total bilirubin, ALT, AST, ALP, CRP, lower MELD scores, and a lower GP210 positivity rate, but higher BMI and albumin levels (all comparisons P < 0.05). Additionally, significant differences were observed between the two groups in GPS, mGPS, and hs-mGPS scores (P < 0.001).
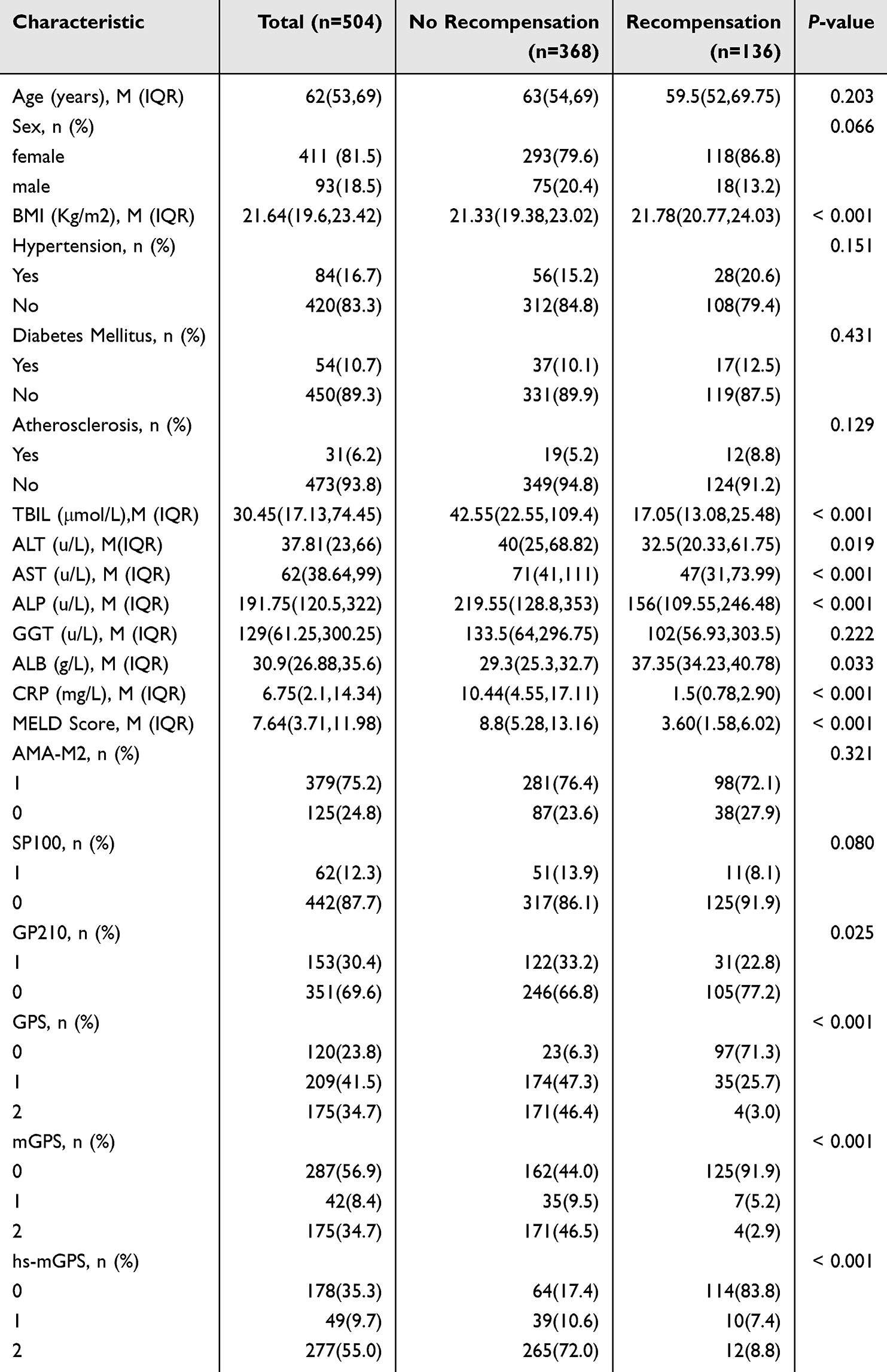 |
Table 2 Comparison of Baseline Clinical Characteristics |
Association Between Glasgow Prognostic Scores and Recompensation
Kaplan-Meier survival analysis revealed that elevation in GPS, mGPS, and hs-mGPS scores corresponded to significantly lower 5-year cumulative recompensation rates. (all trend P < 0.0001, Figure 2). Specifically, the 5-year recompensation rate exhibited a stepwise decline with increasing GPS scores, measuring 53.9%, 22.2%, and 3.9% for scores of 0, 1, and 2, respectively; for those with corresponding mGPS scores, the rates were 39.8%, 17.0%, and 3.9%; and for those with corresponding hs-mGPS scores, the rates were 49.4%, 17.2%, and 7.6%. In the presence of competing events, the 5-year recompensation rate estimated by CIF was slightly lower than that estimated by KM, but the absolute difference was small (≤4.3%), and the decreasing trend with increasing GPS scores remained unchanged (Table S2).
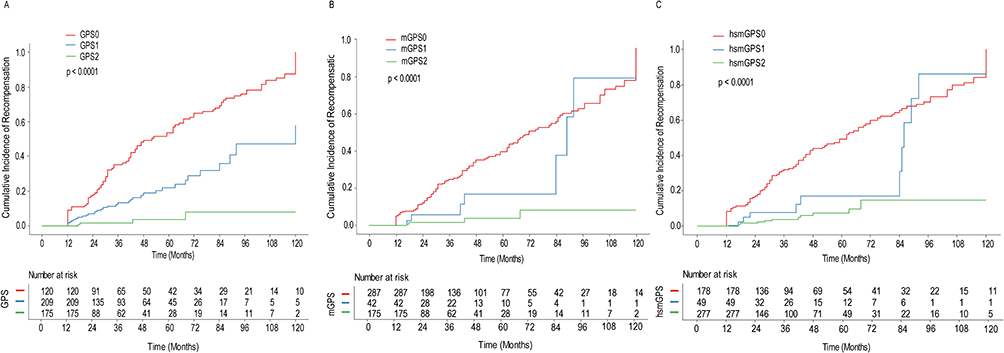 |
Figure 2 Kaplan-Meier curves for re-compensation in patients with decompensated PBC, stratified by the Glasgow Prognostic Score system: (A) GPS, (B) mGPS, (C) hs-mGPS. |
In the fully adjusted model (Table 3), compared with a score of 0, higher scores of GPS, mGPS, and hs-mGPS were independently associated with a reduced risk of recompensation, with adjusted hazard ratios (95% CIs) as follows: GPS 1, 0.383 (0.249–0.590) and GPS 2, 0.054 (0.017–0.168); mGPS 1, 0.393 (0.176–0.878) and mGPS 2, 0.075 (0.024–0.235); hs-mGPS 1, 0.413 (0.203–0.841) and hs-mGPS 2, 0.117 (0.057–0.243). The sHRs from Fine-Gray regression were directionally consistent with those from Cox regression (all P < 0.001), confirming the robust independent predictive value of the Glasgow Prognostic Score system (Table S3).
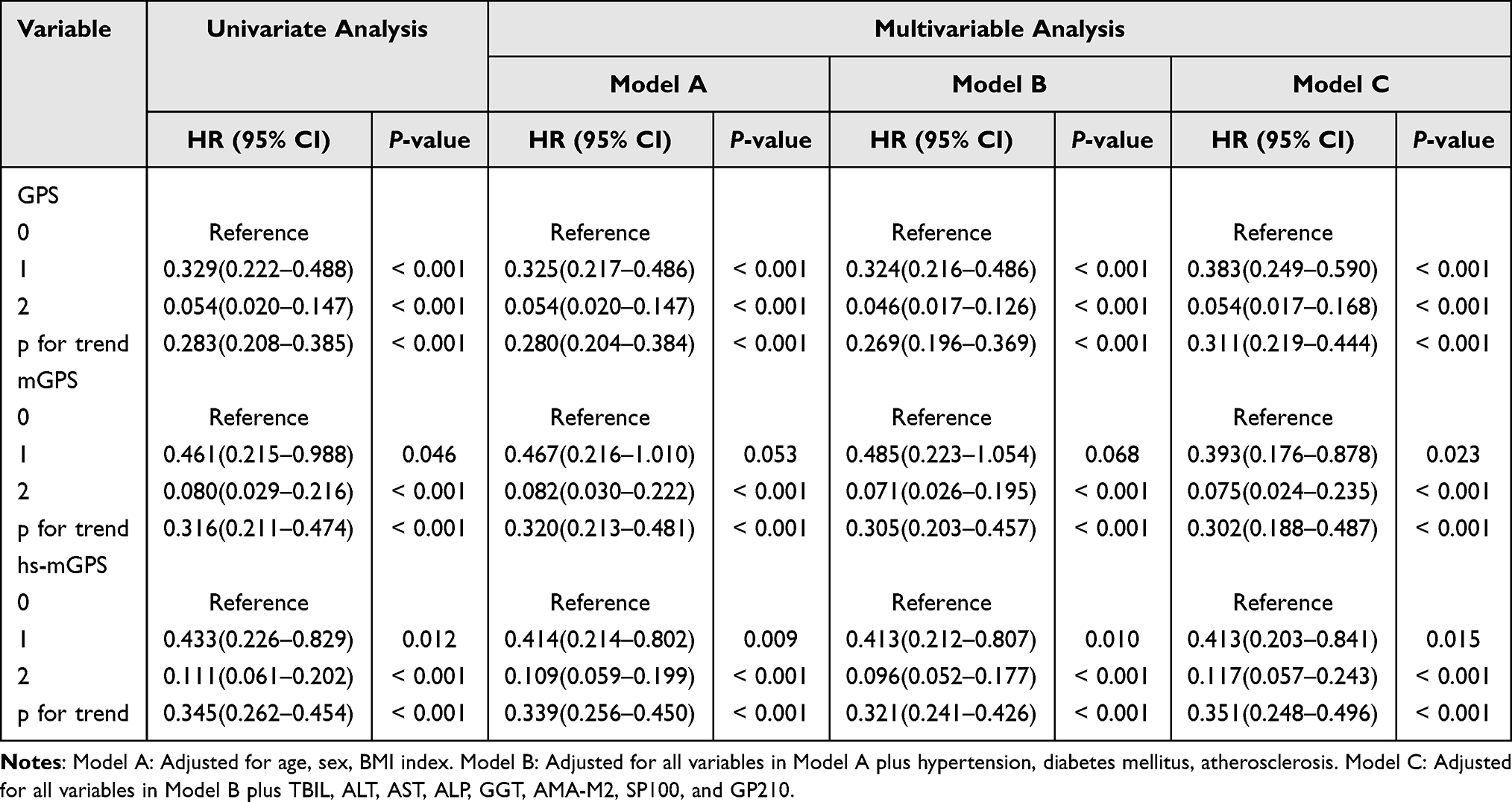 |
Table 3 Univariable and Multivariable Cox Regression Analyses of the Association Between Glasgow Prognostic Scores and Recompensation |
Trend Analysis
Trend analysis confirmed a significant inverse dose–response relationship between increasing scores of each system and the risk of recompensation, with HRs (95% CIs) of 0.311 (0.219–0.444) for GPS, 0.302 (0.188–0.487) for mGPS, and 0.351 (0.248–0.496) for hs-mGPS (all P < 0.05; Table 3).
Subgroup and Sensitivity Analyses
Subgroup analysis stratified by MELD score is presented in Table 4. Among patients with MELD <10, higher scores on the GPS (HR 0.298, 95% CI 0.199–0.447), mGPS (0.285, 0.164–0.494), and hs-mGPS (0.363, 0.244–0.540) remained independent predictors of recompensation. However, in the MELD ≥10 subgroup, only GPS (HR 0.141, 95% CI 0.034–0.588) and hs-mGPS (HR 0.275, 95% CI 0.110–0.684) were significantly associated with recompensation, whereas the association for mGPS was not significant (HR 0.256, 95% CI 0.062–1.066, P = 0.061).
 |
Table 4 Association Between Glasgow Prognostic Scores and Recompensation, Stratified by MELD Score |
A sensitivity analysis excluding patients with hypertension, arteriosclerosis, or diabetes yielded consistent results (Table 5). In the adjusted model, higher scores on all three systems maintained a significant inverse association with recompensation (all P < 0.001), with HRs (95% CIs) of 0.269 (0.168–0.428) for GPS, 0.309 (0.160–0.599) for mGPS, and 0.423 (0.274–0.652) for hs-mGPS.
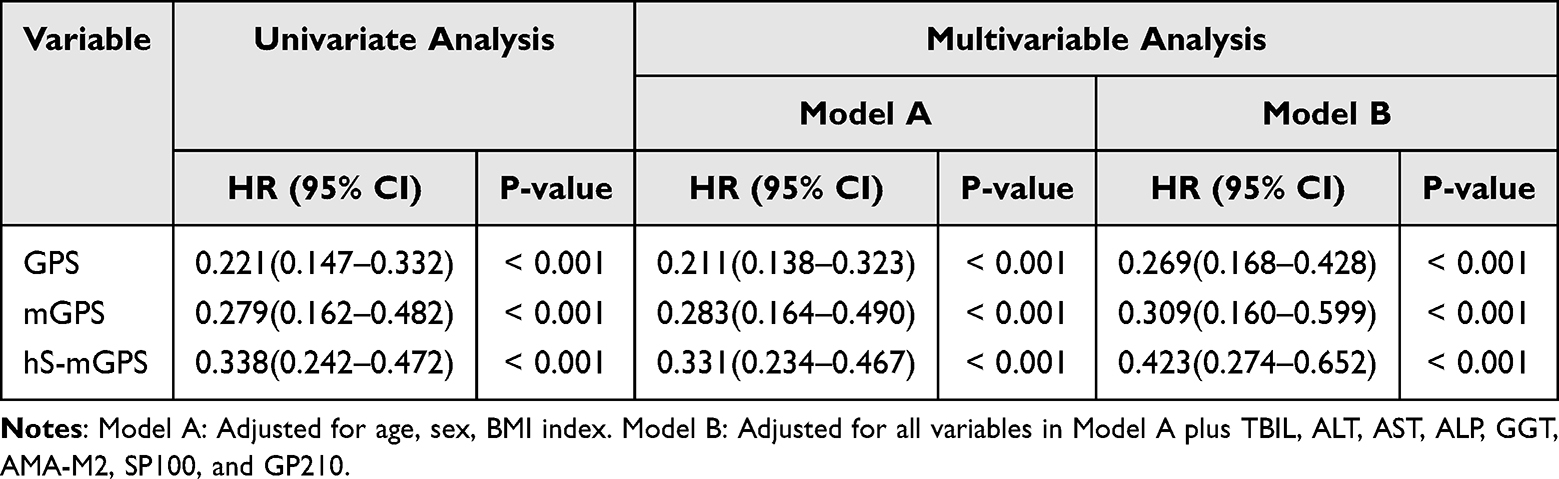 |
Table 5 Association Between Glasgow Prognostic Scores and Recompensation in the Sensitivity Analysis After Excluding Patients with Hypertension, Atherosclerosis, or Diabetes Mellitus |
Although most patients were from a single center, a mixed-effects Cox model with hospital as random intercept confirmed that the prognostic value of the GPS system was not driven by center-specific bias (results consistent with the primary analysis) (Table S4). A analysis censoring patients at initiation of second-line therapies yielded results consistent with the primary analysis, confirming that the prognostic value of the GPS is robust and independent of subsequent second-line therapy decisions (Table S5).
Predictive Performance of Glasgow Prognostic Scores
Time-dependent ROC analysis was performed to evaluate the predictive performance of each score for recompensation (Figure 3). The AUCs were 0.888 (95% CI: 0.855–0.921) for GPS, 0.795 (0.756–0.835) for mGPS, and 0.871 (0.838–0.904) for hs-mGPS (all P < 0.001). Subsequent model comparison using the DeLong test revealed that both GPS and hs-mGPS demonstrated significantly superior predictive performance compared to mGPS (P < 0.05), whereas no significant difference was found between GPS and hs-mGPS. We performed time-dependent ROC analysis with a 60-month prediction horizon and validated the AUC estimates using 1000 bootstrap resampling iterations, confirming the robustness of the predictive model without overfitting (Table S6).
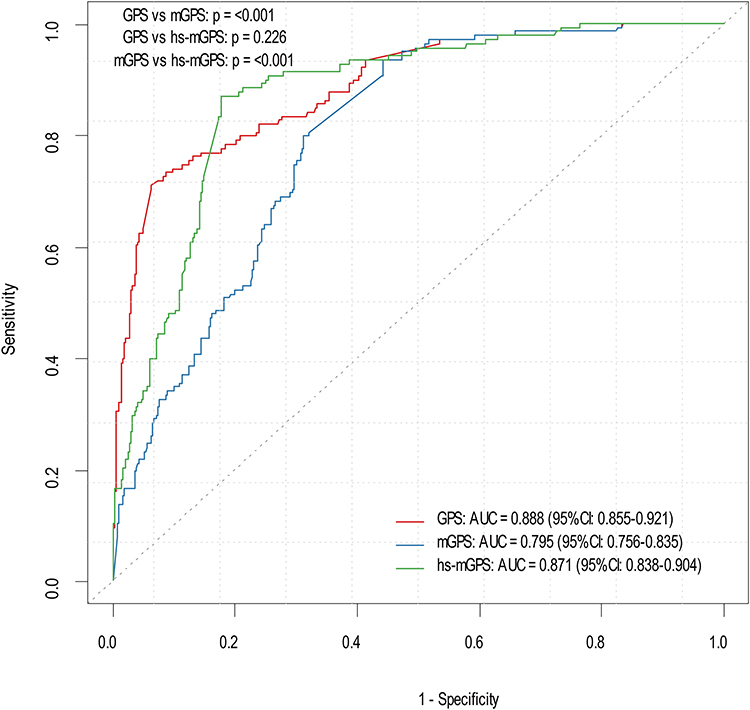 |
Figure 3 Time-dependent ROC curves for predicting re-compensation using the GPS, mGPS, and hs-mGPS. |
Discussion
This study is the first to systematically evaluate the predictive value of the GPS system for recompensation in patients with decompensated PBC, based on a large multicenter cohort from Southwest China. The main findings are that GPS, mGPS, and hs-mGPS scores are all independent predictors of recompensation, with GPS demonstrating the best predictive performance. Thus, this work lays a foundation for improved risk stratification and personalized management in patients with decompensated PBC. Sensitivity and subgroup analyses further validated the robustness of these conclusions.
This study validates that the Glasgow Prognostic Score system—originally derived in oncology to assess the nutrition-inflammation axis via albumin and C-reactive protein16,17—also predicts the likelihood of recompensation in PBC, with higher scores indicating a lower probability. Multiple lines of evidence support this finding. Cash et al reported significantly elevated CRP levels in PBC patients.18 Mendelian randomization studies further confirmed CRP as a risk factor for PBC.19 Elevated CRP is also associated with cirrhosis progression and increased mortality risk,20 and holds prognostic value in acute liver failure with sepsis.21 In PBC patients, hypoalbuminemia is strongly associated with an unfavorable prognosis.22,23 The underlying mechanism may stem from a vicious cycle of sustained inflammatory injury and progressive nutritional depletion during PBC progression.24 Within the context of the autoimmune bile duct injury characteristic of PBC, elevated CRP levels signify a persistent systemic inflammatory state. This state may exacerbate liver fibrogenesis by impairing regulatory T-cell function and promoting the activation of pro-inflammatory Th1/Th17 cells, which in turn activate hepatic stellate cells.25 Concurrently, inflammatory cytokines promote the hepatic synthesis of acute-phase proteins while inhibiting albumin production.26 Hypoalbuminemia not only directly reflects decreased liver synthetic function but is also often accompanied by malnutrition, which weakens the intestinal mucosal barrier and increases the risk of bacterial translocation.27 These mechanisms collectively drive immune dysfunction and the progression of liver fibrosis, ultimately leading the disease into its decompensated phase.
The predictive power of the GPS stems from its ability to capture the “inflammation-nutrition” vicious cycle comprehensively. By simultaneously capturing both inflammatory and nutritional dimensions, the GPS creates a composite index more informative than any single marker, effectively identifying patients in the adverse dual-risk state of “high inflammation and low nutrition.” This integrative advantage is reflected in its superior predictive performance, as demonstrated by a time-dependent ROC analysis yielding an optimal AUC of 0.888 for GPS. This difference primarily arises from the distinct ways the three scores handle the weighting of albumin. The mGPS and hs-mGPS adjust the score based on low albumin only when CRP or hs-CRP is elevated; thus, they may fail to identify patients with normal CRP but significantly reduced albumin. In chronic liver diseases like PBC, low albumin is often related to malabsorption due to cholestasis, chronic decline in liver synthetic function, and malnutrition.28 The GPS, by incorporating both CRP and ALB, can more sensitively identify patients with “low-grade inflammation but high malnutrition risk,” thereby achieving a more comprehensive and precise stratification of recompensation risk. Therefore, in the clinical management of PBC, using the original GPS may provide more accurate prognostic information than its modified versions.
From a practical clinical perspective, our finding that hs-mGPS did not significantly outperform the original GPS (AUC: 0.871 vs 0.888, P > 0.05) carries an important message. High-sensitivity CRP assays, while offering greater precision at low CRP concentrations, are more expensive and not universally available in all clinical laboratories, particularly in resource-limited settings. The comparable predictive performance of the standard GPS, which uses conventional CRP testing, suggests that the additional cost and complexity of hs-CRP are not necessary for risk stratification of recompensation in decompensated PBC. This finding supports the widespread clinical translatability of the GPS, as it can be calculated using routine, inexpensive laboratory tests available in most healthcare facilities. We propose that the GPS be calculated using routinely available baseline levels of CRP and albumin in patients with an initial diagnosis of decompensated PBC. This scoring system effectively stratifies the probability of recompensation: higher GPS values are associated with a lower likelihood of achieving recompensation, thereby enabling early intervention in high-risk individuals. Whether longitudinal dynamic monitoring of GPS offers additional prognostic value beyond that of baseline assessment remains an open question. Future prospective studies are warranted to investigate whether serial GPS measurements can capture treatment response and inform adaptive management strategies.
The principal strengths of this investigation lie in its multicenter design, substantial sample size, and extended median follow-up duration. However, the following limitations should be acknowledged. First, 231 of 735 patients (31.4%) were excluded, including 136 due to incomplete follow-up data, which may introduce selection bias. Second, the strict Baveno VII recompensation criteria may theoretically underestimate clinical improvement in some patients, and future studies should consider this issue. Third, due to the limitations inherent in the retrospective study design, graded severity of decompensation events could not be assessed. Furthermore, we acknowledge that the incremental predictive value of the GPS beyond established prognostic models such as MELD was not evaluated in this study; future dedicated analyses are planned to perform comparative model assessments and determine whether GPS improves discrimination for recompensation beyond these scores.
In conclusion, our findings establish the utility of the Glasgow Prognostic Score system in predicting recompensation in decompensated primary biliary cholangitis, with the original GPS showing the highest predictive accuracy. Relying on routinely available blood markers, this tool is clinically feasible and readily translatable, supporting earlier risk stratification and personalized care for this patient population.
Data Sharing Statement
The dataset is available from the corresponding authors upon reasonable request.
Ethic Statement
This retrospective study was approved by the Institutional Review Board (IRB) of Kunming Medical University (Approval No: KMMU2025MEC155), which waived the requirement for informed consent. All patient data were anonymized.
Author Contributions
Man Huang: Conceptualization, Methodology, Formal analysis, Writing – original draft; An Dai: Conceptualization, Methodology, Writing – review & editing; Liufei Gao: Conceptualization, Methodology, Writing – review & editing; Changhui Wu: Data curation, Writing – review & editing; Wen Zou: Data curation, Writing – review & editing; De Duan: Data curation, Writing – review & editing; Junkun Niu: Data curation, Writing – review & editing; Jinhui Yang: Data curation, Methodology, Writing – review & editing; Yuan Tang: Conceptualization, Methodology, Writing – review & editing; Hongtao Lei: Conceptualization, Methodology, Formal analysis, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Laboratory of Integrated Care for Geriatric Chronic Diseases (Kunming Medical University, School of Nursing), Yunnan Provincial Education Department (Grant No. 2024HTHLYB02), Scientific Research Foundation of the Education Department of Yunnan Province (Grant No. 2025J0329). Yunnan Fundamental Research Kunming Medical University Projects (Grant No. 202501AC070216).
Disclosure
The authors declare no competing interests.
References
1. Levy C, Manns M, Hirschfield G. New Treatment Paradigms in Primary Biliary Cholangitis. Clinical gastroenterology and hepatology: the official clinical practice. J Am Gastroenterol Assoc. 2023;21(8):2076–11.
2. Trivella J, John BV, Levy C. Primary biliary cholangitis: epidemiology, prognosis, and treatment. Hepatol Commun. 2023;7(6). doi:10.1097/HC9.0000000000000179
3. Hofer BS, Burghart L, Halilbasic E, et al. Evaluation of potential hepatic recompensation criteria in patients with PBC and decompensated cirrhosis. Aliment Pharmacol Ther. 2024;59(8):962–972. doi:10.1111/apt.17908
4. Moore O, Ma WS, Read S, George J, Ahlenstiel G. The unwell patient with advanced chronic liver disease: when to use each score? BMC Med. 2025;23(1):413. doi:10.1186/s12916-025-04185-w
5. Li J, Yan K, Zhu P, et al. Prognostic value of Glasgow Prognostic Score and its modified scores on 5-year outcome in patients with coronary heart disease undergoing percutaneous coronary intervention. Heliyon. 2024;10(18):e37317. doi:10.1016/j.heliyon.2024.e37317
6. Chang PH, Wang CH, Chen EY, et al. Glasgow prognostic score after concurrent chemoradiotherapy is a prognostic factor in advanced head and neck cancer. Chin J Cancer Res. 2017;29(3):172–178. doi:10.21147/j.issn.1000-9604.2017.03.02
7. Luo B, Zhang Y, Zhu X, et al. Prognostic impact of the high-sensitivity modified glasgow prognostic score on patients undergoing radical surgery for hepatocellular carcinoma: authorship. Langenbecks Arch Surg. 2024;409(1):223. doi:10.1007/s00423-024-03423-8
8. Chen Y, Ruan GT, Shi JY, et al. The combination of hand grip strength and modified Glasgow prognostic score predicts clinical outcomes in patients with liver cancer. Front Nutr. 2023;10:1062117. doi:10.3389/fnut.2023.1062117
9. Taru V, Szabo G, Mehal W, Reiberger T. Inflammasomes in chronic liver disease: hepatic injury, fibrosis progression and systemic inflammation. J Hepatol. 2024;81(5):895–910. doi:10.1016/j.jhep.2024.06.016
10. Engelmann C, Clària J, Szabo G, Bosch J, Bernardi M. Pathophysiology of decompensated cirrhosis: portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction. J Hepatol. 2021;75(Suppl 1):S49–s66. doi:10.1016/j.jhep.2021.01.002
11. Hirschfield GM, Beuers U, Corpechot C. EASL Clinical Practice Guidelines: the diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017;67(1):145–172. doi:10.1016/j.jhep.2017.03.022
12. Moreau R, Tonon M, Krag A. EASL Clinical Practice Guidelines on acute-on-chronic liver failure. J Hepatol. 2023;79(2):461–491. doi:10.1016/j.jhep.2023.04.021
13. Hirschfield GM, Dyson JK, Alexander GJM, et al. The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines. Gut. 2018;67(9):1568–1594. doi:10.1136/gutjnl-2017-315259
14. Ferstl P, Trebicka J. Acute Decompensation and Acute-on-Chronic Liver Failure. Clin Liver Dis. 2021;25(2):419–430. doi:10.1016/j.cld.2021.01.009
15. Tonon M, Gagliardi R, Pompili E, et al. Validation and expansion of Baveno VII recompensation criteria in patients with cirrhosis and curable liver disease. J Hepatol. 2025;83(4):888–898. doi:10.1016/j.jhep.2025.04.018
16. Di Rosa M, Sabbatinelli J, Giuliani A, et al. Inflammation scores based on C-reactive protein and albumin predict mortality in hospitalized older patients independent of the admission diagnosis. Immun Ageing. 2024;21(1):67. doi:10.1186/s12979-024-00471-y
17. Takamori S, Takada K, Shimokawa M, et al. Clinical utility of pretreatment Glasgow prognostic score in non-small-cell lung cancer patients treated with immune checkpoint inhibitors. Lung Cancer. 2021;152:27–33. doi:10.1016/j.lungcan.2020.11.026
18. Cash WJ, McCance DR, Young IS, et al. Primary biliary cirrhosis is associated with oxidative stress and endothelial dysfunction but not increased cardiovascular risk. Hepatol Res. 2010;40(11):1098–1106. doi:10.1111/j.1872-034X.2010.00717.x
19. Gao W, Peng C, Wang Z, Li Y, Liu M. Genetic association and causal relationship between multiple modifiable risk factors and autoimmune liver disease: a two-sample mendelian randomization study. J Transl Med. 2024;22(1):425. doi:10.1186/s12967-024-05247-y
20. Turco L, Garcia-Tsao G, Magnani I, et al. Cardiopulmonary hemodynamics and C-reactive protein as prognostic indicators in compensated and decompensated cirrhosis. J Hepatol. 2018;68(5):949–958. doi:10.1016/j.jhep.2017.12.027
21. Wang D, Wang X, Mu J, et al. Prognostic indicators and outcome in patients with acute liver failure, sepsis and with and without shock: a retrospective cohort study. Annals of Medicine. 2025;57(1):2438833. doi:10.1080/07853890.2024.2438833
22. Yao TT, Qian JD, Wang GQ. Efficacy of ursodeoxycholic acid combined with prednisolone and immunosuppressant triple therapy in the treatment of refractory primary biliary cholangitis. Medicina Clinica. 2020;155(4):165–170. doi:10.1016/j.medcli.2020.03.013
23. Li Y, Liu B, Li X. High C-reactive protein-to-albumin ratio levels are associated with osteoporosis in patients with primary biliary cholangitis. Front Endocrinol. 2024;15:1415488. doi:10.3389/fendo.2024.1415488
24. Chen R, Sun Y, Hu Y, Tai W. Innate immunity of bile and cholangiocytes in primary biliary cholangitis. Front Immunol. 2025;16:1655287. doi:10.3389/fimmu.2025.1655287
25. Simbrunner B, Villesen IF, Königshofer P, et al. Systemic inflammation is linked to liver fibrogenesis in patients with advanced chronic liver disease. Liver Int. 2022;42(11):2501–2512. doi:10.1111/liv.15365
26. Wiedermann CJ. Hypoalbuminemia as surrogate and culprit of infections. Int J Mol Sci. 2021;22(9):4496. doi:10.3390/ijms22094496
27. Giordano DM, Pinto C, Maroni L, Benedetti A, Marzioni M. Inflammation and the gut-liver axis in the pathophysiology of cholangiopathies. Int J Mol Sci. 2018;19(10):3003. doi:10.3390/ijms19103003
28. Jagdish RK, Maras JS, Sarin SK. Albumin in advanced liver diseases: the good and bad of a drug! Hepatology. 2021;74(5):2848–2862. doi:10.1002/hep.31836
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.