")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Giving Voice to People with Dementia and Perspectives Regarding a Dementia-Friendly Society: A Synthesis of Qualitative Studies
Authors Alteren J , Johannessen A , Lyberg AM, Magnussen IL
Received 24 November 2022
Accepted for publication 9 March 2023
Published 1 April 2023 Volume 2023:16 Pages 851—861
DOI https://doi.org/10.2147/JMDH.S398570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Johanne Alteren,1 Aud Johannessen,2,3 Anne Marit Lyberg,2 Inger-Lise Magnussen4
1Faculty of Health Sciences and Social Care, Molde University College, Molde, Norway; 2Faculty of Health and Social Sciences, University of South-Eastern Norway, Horten, Norway; 3Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 4Faculty of Nursing and Health Sciences, Nord University, Stokmarknes, Norway
Correspondence: Johanne Alteren, Tel +47 71 19 58 93, Fax +47 71 21 40 00, Email [email protected]
Introduction: The World Health Organization [WHO] and governments worldwide envision the development of dementia-friendly societies that are based on a person-centered culture. A limited number of studies have described the features of dementia-friendly societies based on the viewpoints of people with dementia.
Purpose: To synthesize qualitative empirical research that expands the knowledge of what people with dementia consider to be essential for daily living in a dementia-friendly society.
Methods: The authors searched phrases in the databases AgeLine, CINAHL, EMBASE, MedLine, PsycINFO, PubMed, ORIA, SveMed+, and Cochrane Library. Research articles that involved people with dementia and were conducted in Western countries, written in English, published in peer-reviewed academic journals using qualitative methods, and published within the past decade were included. The research included was critically and systematically appraised using the critical appraisal skills program checklist for qualitative research, and the findings were analyzed according to Graneheim and Lundman’s method of qualitative content analysis.
Results: Overall, 1122 records— 561 from 2019 and 561 from 2021—were identified through the search, and nine studies were included in the final synthesis. The studies included were from the United Kingdom (five studies), Australia (three studies), and New Zealand (one study). Through the analysis process, the following main theme emerged: giving voice to people with dementia, which summarizes the essence of what people with dementia believe is essential for daily living in a dementia-friendly society. The main theme covered two themes: a sense of being valued and a sense of being safeguarded, each of which contained subthemes.
Conclusion: To meet the WHO’s and the governments worldwide intention to develop dementia-friendly societies, further research should focus on the voices of people with dementia. By including those concerned, the political goals of a dementia-friendly society can be achieved.
Keywords: approachable society, user involvement, decision-making, systematic review, qualitative research, person-centered culture
Introduction
Globally, 55 million people are living with dementia.1–3 With an annual increase of approximately 10 million people, the figure will reach 152 million by 2050.4 In Norway, the number of people with dementia is expected to rise to 101,000 this year, which is approximately 2% of the population.5
Dementia is typically caused by progressive neurodegenerative disorders and results in a gradual decline in health conditions and functionality, which changes people’s living situations. Moreover, the condition causes a gradual cognitive decline.6,7 For people with dementia, caring for themselves, performing other daily activities, and moving independently becomes demanding. Dementia increases the difficulties experienced in maintaining work, social activities, and family commitments.8,9 Living with dementia can also cause isolation and loneliness,8 which can entail despair, shame, and loss of dignitiy.8,10,11
Living with dementia may test the subjective experience of one’s value as a human.12 To treat people with dementia in an accommodating and respectful way that strengthens the value humans provide each other is the core of person-centred care,12 the goal of which is to maintain an individual’s unique personality in personal and social relationships.12 This is the philosophy on which person-centered culture is based: amplifying the individual’s personhood rather than their diagnosis. Human beings exist by virtue of who they are.12 Measures based on knowledge and understanding individual needs, stories, and wishes of people with dementia promote this culture of care.13 However, research has indicated that many challenges exist in implementing person-centered dementia care in organizational cultures.14,15
Communities around the world strive to create more inclusive societies and supportive environments, both physical and social, without stigma or discrimination.4,16 Internationally, the terms dementia-friendly communities and dementia-friendly societies indicate a city, town, or village where people with dementia are understood, respected, and supported,17 as well as where they can contribute as active and valued citizens.18 Participation is a key concept in adopting a person-centered approach;4 however, if the voices of people with dementia are not heard, then one must raise the question of how much people with dementia stimulate and influence political decisions.19
Government policies in Western countries indicate that older people and people with dementia should continue living at home for as long as possible.3,7 Therefore, accessibility to social activities and various services is important not only for those with disabilities or dementia but also for others.3 To make society more approachable for the former, developments must be designed from the user’s perspective, resulting in an enhanced society for everyone.3 Previous scholars have reported that evaluations from health personnel regarding the needs of people with dementia are not necessarily consistent with their actual needs and preferences.20,21 Furthermore, it has been well documented that people with dementia can communicate their needs and lived experiences of having dementia.21,22
Therefore, people with dementia must be offered opportunities to express their thoughts, feelings, and perceptions of their needs and preferences,8,9,23,24 both in private and public spaces,8,25–27 so researchers and caregivers can gain valuable knowledge from their perspective.
Worldwide, we still do not meet the World Health Organization’s [WHO] goal of a dementia-friendly society that aligns with person-centered care based on knowledge from people with dementia.4,16 Previous research has indicated that few studies involve the perspectives of people with dementia. To gain and develop knowledge about existing research regarding those concerned, the aim of this systematic review is to synthesize the qualitative empirical research that describes what people with dementia experience as essential for daily living in a dementia-friendly society.
Materials and Methods
Design
A systematic review method28 of qualitative evidence was performed to expand the knowledge of what people with dementia consider essential for daily living in a dementia-friendly society.
Search Strategy and Data Sources
The search strategy was designed in collaboration with a subject-specialist librarian.29 One example of a systematic search is this: the search terms dementia and cognitive impairment were employed in various combinations with daily living in diverse environments, and experiences both separately and combined with functions such as AND as well as OR, using the framework established by Fineout-Overholt and Johnston.30 Several possible combinations are portrayed in Table 1. Additionally, these search terms were employed as phrases to make appropriate demarcations that produced exact records regarding what people with dementia consider essential for daily living in a dementia-friendly society. For example, a phrase search could be “Title (TI) dementia friendly society OR TI dementia friendly communities OR TI dementia village OR TI dementia friendly OR TI physical environment OR TI psychosocial environment”. In a phrase search, the title (TI) groups the terms and maintains the order so that dementia is not searched in one place in an article, friendly in another part of the article and society in a third part. To connect the various search terms, the authors narrowed the terms by conducting systematic searches in titles and abstracts: systematic data and hand searches were conducted in July 2019. An updated exploration was repeated in May 2021 using the same search strategy and databases.
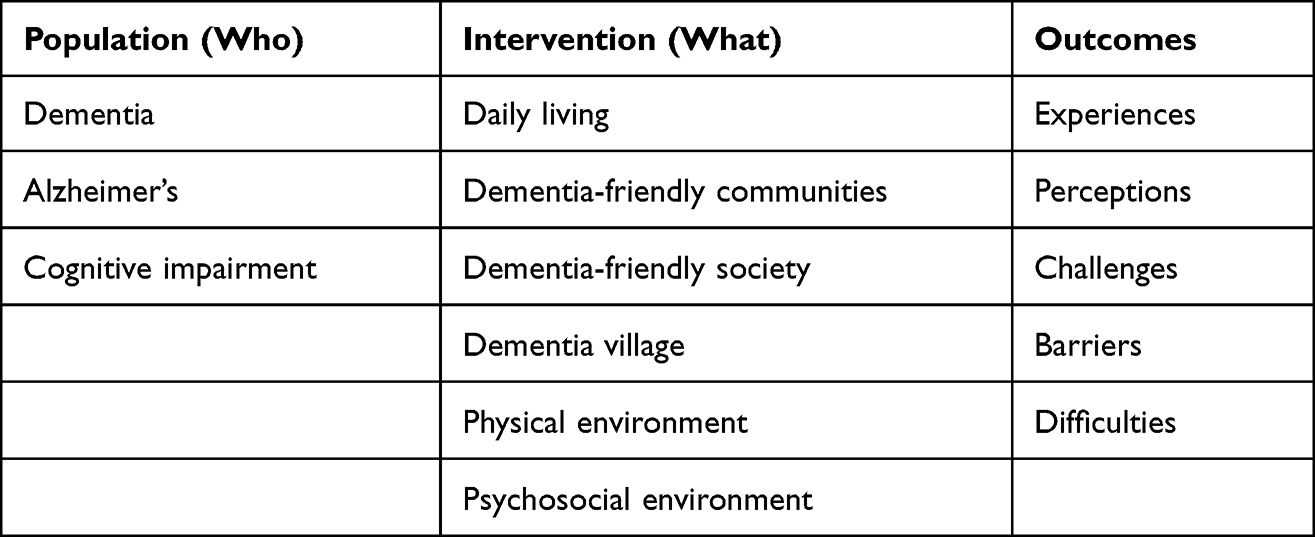 |
Table 1 Search Terms in Various Combinations |
The search with these combinations was conducted using AgeLine, CINAHL, EMBASE, MedLine, PsycINFO, PubMed, ORIA, SveMed+, and Cochrane Library, Appendix 1. SveMed+ was discontinued in late 2019 and thus was not included in the 2021 search. The search strategy followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) reporting guidelines.31 The article selection process is illustrated in Figure 1; nine studies were included in the qualitative synthesis.
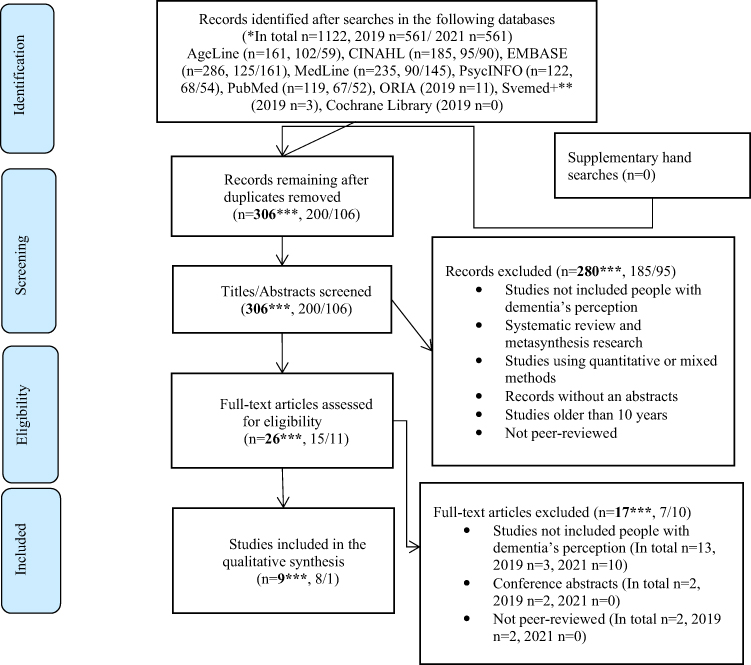 |
Figure 1 PRISMA diagram of the article selection process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. 31 *In total and number of searches in 2019 and 2021. **In the SveMed+ database, Norwegian, Swedish, Danish, and Finnish languages were used in the search. ***In total representing 2019 and 2021. |
Study Selection
Research articles that involved people with dementia and were conducted in Western countries, written in English, and published in peer-reviewed academic journals using qualitative methods within the past decade were included. This time frame was chosen due to the recent increased focus on dementia-friendly societies.4 Overall, 1122 records—561 in 2019 and 561 in 2021—were identified through the search. After duplicates were removed (n = 816; n = 361, 2019; n = 455, 2021), each of the four researchers independently conducted title and abstract screenings (n = 306; n = 200, 2019; n = 106, 2021) and examined the remaining full texts (n = 26; n = 15, 2019; n = 11, 2021), for eligibility based on the aforementioned inclusion criteria. The review and any disagreements regarding study selection were discussed; a consensus was reached to verify eligibility before undertaking full-text reviews. Only three studies exclusively included the perspectives of people with dementia; consequently, the authors employed findings that could be directly linked to the perspectives of people with dementia, which were extracted from studies whose participants included families, relatives, volunteers, health personnel, and professionals associated with people who have dementia. The full-text articles were examined for further review and selection, and the four researchers compared their individual assessments. The nine studies included in the qualitative synthesis were critically and systematically appraised using the critical appraisal skills program (CASP) checklist for qualitative research.32 The CASP was chosen to assess three issues that included 10 questions regarding the quality of the research articles. The three issues are as follows: Are the results of the study valid? What are the results? Will the results help locally? All studies fulfilled the criteria of the three issues.
Analysis
An inductive, interpretive approach33 was employed in which the included studies were processed and analyzed according to Graneheim and Lundman’s34 method of qualitative content analysis. Furthermore, this research adhered to their published work regarding this procedure.35,36 An open-minded approach was adopted to identify meaningful subjects and extend an interpretive level of understanding concerning the views of people with dementia. To determine themes for the analysis, the authors extracted the findings that could be clearly related to people with dementia, which comprised statements and views. The authors read the studies’ findings to obtain an initial overview and then jointly reflected upon the content. Remembering the aim of the study, we divided the text into classifications meaning and then condensed the meanings. An example of a condensed meaning, as presented in Table 2, is as follows: Family is the most important thing. I am married to a person who I love very much, and I have no problem with the setup. In the current analysis, these descriptions reflect the text and the manifest content. The authors then compared and grouped the various collections of meanings based on their differences and similarities. The research texts included were more concentrated than those of an interview; consequently, further condensation was challenging. Therefore, the authors subsequently observed the units of meaning as a whole and abstracted them into subthemes, such as belonging to others. The subthemes represent an interpretation of the underlying meaning based on latent content that was distant from the text, but close to the view of people with dementia. During the analysis, two recurring themes were developed: a sense of being valued and a sense of being safeguarded, each of which contained subthemes. Finally, the main theme was developed: giving voice to people with dementia.
 |
Table 2 Examples from the Content Analysis: From Categories of Meaning to the Main Theme Giving Voice to People with Dementia |
This process was not linear, as it involved discussions between the authors and moving throughout different parts of the texts. The limited disagreements that occurred were resolved by reaching a consensus, which can be linked to the trustworthiness concept presented by Elo et al.37 The goal of this process was to achieve a reasonable explanation of the meaning underlying the nine articles,34,35 however, the authors experienced challenges in ensuring a consistent focus on the views of people with dementia.
Results
The included studies were from the United Kingdom (five),40–42,44,45 Australia (three),38,43,46 and New Zealand (one).39 The private and public spaces denoted the context: the former included private rooms and associated physical areas as well as outdoor spaces where people with dementia lived, such as their house, apartment, or care housing; the latter signified the community, health and social services, and leisure spaces, such as museums, parks, and swimming pools. The publication period of the nine articles was from 2014 to 2021 (Table 3).
 |
Table 3 Description of the Nine Qualitative Studies That Include People with Dementia |
The main theme, giving voice to people with dementia included the two recurring themes: a sense of being valued and a sense of being safeguarded.
A Sense of Being Valued
The first theme was illuminated through the following three subthemes: belonging to others, supportive and customized activities, and facilitating the development of buildings and community spaces.
Belonging to Others
People with dementia expressed that being able to live in society and engage in their social life stimulated their feeling of belonging.38–40 Being part of a social community was highlighted as important; people with dementia reported that their self-confidence increased when they experienced acceptance.39,41,42 Furthermore, social support provided by organizations and volunteers was valued by individuals with dementia39,40 and opportunities for meeting and engaging with other people reduced feelings of isolation.41 During these social events, people with dementia began new relationships and developed informal social support networks.41
Independence, autonomy, flexibility, freedom to socialize, and deciding how to live were significant for people with dementia to experience belonging with respect to others and society, as these factors provided a highly valued sense of normality and control.38 The feeling of having personal space and power over this space symbolized others’ respect for the possessions and privacy of people who have dementia.38 In residential care facilities, individuals with dementia often shared a room with another person, which prevented private family conversations.43
Supportive and Customized Activities
Although people with dementia desired to access and participate in meaningful leisure activities, challenges were created by impaired health, stigma, and inadequate support.38,39,41,42 However, if support was available, then people with dementia wanted to engage in new activities.39 Partaking in activity groups, such as art classes, nature walks, church visits, or coffee chats in another environment, allowed people with dementia to feel content in daily life.38,39,41 For example, when people with dementia were able to participate in a swimming activity, they experienced empowerment and joy,41 and events involving songs and poetry provided engagement in a dignified manner. Moreover, people with dementia reacquired their dignity by exercising at a gym that offered an opportunity to continue life as it had been before dementia.40,41 Loss of previous skills created grief and sadness; however, people with dementia enjoyed personalized activities that were adapted to their state of health.38,40
Tailor-made events were appreciated,38 such as artists who conducted weekly home visits and delivered cultural activities based on the interests and engagement of isolated people who had mild and moderate dementia.44 Having a social arena in which people with dementia could contribute and be together in various activities created meaningful moments.44 People with dementia reflected on the value of these activities and their current sense of isolation. Furthermore, people with dementia emphasized the importance of being heard in society.
Facilitating the Development of Buildings and Community Spaces
People with dementia reported challenges in navigating public areas and expressed the importance of seriously considering these challenges to reduce confusion and disorientation.39,42,43,45 The experiences regarding disorientation were influenced by the location of apartments for people with dementia in care housing in relation to communal spaces as well as by the accessibility and the specific route to community areas.
Individuals with dementia highlighted their right to be involved and heard in planning and facilitating the development of buildings and community spaces. Moreover, people with dementia considered this essential to the ability to partake in activities and live independently.39,42–45 In a retirement development, people with dementia demonstrated the need to minimize the distance between apartments and communal areas; additionally, people with dementia noted that designers should incorporate photographs, louvered windows, table flowers, apartment numbers, distinctive corridors, signs that indicate stairs and elevator floors, and landmarks along routes to communal areas.45
After earthquakes occurred in Christchurch, New Zealand, people with dementia were involved in planning and facilitating community spaces to allow simpler navigation, thus enhancing their lives.39 People with dementia provided information regarding the community’s need for clear signage that would enable them to travel independently as well as a visible police presence, limited traffic in residential areas with additional cul-de-sac streets, and traffic-light-controlled pedestrian crossings on busy roads rather than the zebra-striped crosswalks or pedestrian islands.39 Attractions such as museums and galleries that offered amenities including disability-friendly cafés, restrooms, and parking spaces were popular among individuals with dementia.42 Those places where it was feasible to combine a meal with an activity, a social event, and an opportunity to rest were preferred. Outdoor and open spaces offering people with dementia freedom to walk were considered relaxing.39,42
In another research study included in the review, people with dementia were involved in discussing the environment and design features of a new hospital.43 They argued against the plan to have less personal space and two-bed rooms while encouraging access to the outdoors, gardens, and nature. People with dementia highlighted the need for fresh air and well-lit spaces as well as a less institutional and more homelike feeling. Taking ownership of the space allowed people with dementia to experience satisfaction and a sense of freedom in the environment.43
A Sense of Being Safeguarded
The second theme was highlighted through the following two subthemes: trustworthy housing that supports predictable living and health services based on knowledge and empathy.
Trustworthy Housing That Supports Predictable Living
The experiences of people with dementia who lived at home and in safe environments were essential for housing that supports predictable living.40,45 A natural, pleasant environment; friendly, supportive networks; and accessible formal dementia services within the community contributed to such experiences.40 Rural environments were viewed positively, as they offered people with dementia a sense of peace and connection with nature as well as safe surroundings within which they felt comfortable navigating.40 People with dementia were acquainted with one another; this was experienced as a safe and visible network that constituted a culture of caring.40
The purpose of care housing is to enable people with dementia to live together in safe surroundings with some additional assistance.45 Although care housing enabled people with dementia to live collectively, many regarded such a move with uncertainty and loss of affiliation. People with dementia were familiar with their local community where they had family and friends and knew their neighbors. Furthermore, people with dementia experienced disorientation in new surroundings.45 With increased familiarity, people with dementia became more comfortable and safer in the surroundings, upon which general function improved.40,45 For those with dementia who chose to move to care housing, it was important that the facility suited their needs.45 People with dementia who found the buildings and surroundings confusing refrained from leaving their apartment, which could cause isolation and loss of participation in social community.45
Health Services Based on Knowledge and Empathy
Care provision from health services and people with dementia caring for each other were expressed as significant parts of a health facility that is based on knowledge and empathy.38,41,44,46 The support received by people with dementia was often considered limited or absent in formal care services.40 People with dementia stated that health care personnel should be better qualified in the early recognition and diagnosis of dementia. Furthermore, health care personnel should be able to provide individual support based on each patient’s diagnosis.39,46 The prejudice against dementia can impact the approach and treatment provided in hospitals.46
Knowledge about the building conditions includes information about the modifications needed for people with dementia to discover and access the services necessary to care for personal health and daily routines, such as washing clothes.38 Moreover, people with dementia must be able to use the city’s facilities provided by medical doctors, hair stylists, and grocery shops.38,45 This knowledge is important in developing a health service wherein people with dementia can live safely in their homes. Additionally, information regarding homelike physical environments, wherein people with dementia have access to private outdoor spaces with trees and flowers, is also considered essential for people with dementia to experience health services that are based on knowledge and empathy.38
Discussion
Including people with dementia in society and requesting their involvement in decision-making are essential for life in a dementia-friendly society. People with dementia must be able to live independently while being valued and safeguarded in private and public spaces, which requires that such spaces must be developed and facilitated based on the needs indicated by the definition of a dementia-friendly society.3,7,17 People with dementia are citizens with voices that should be protected and acknowledged in the private and public issues concerning dementia care.7,8,21,24 Involving people with dementia in the development and improvement of health, social, and leisure services has been emphasized over recent years, although people with dementia have been less involved in these processes.47 This study’s findings describe societies in which the inclusion of people with dementia varies. Societal inclusion implies involvement in creative critical dialogue with professionals and others who develop health and welfare systems.15,17,48 In which users’ experiences are solicited by recruiting service consumers to improve outcomes for people with dementia.49
The studies included in the current research explain the experiences of people with dementia in a dementia-friendly society. However, the studies do not address the extent to which their experiences are considered. People with dementia provided input regarding two-bed rooms in the design of a new hospital.43 These participants stated that the service and care received were more important than the building itself. Nevertheless, the outcome was two-bed rooms and less personal space, which limited the potential of having an independent and safe life. This exemplifies plans that are created without considering individuals who have dementia and their relevant needs. During service-led user involvement processes, the lived experiences of the users often become objectified,50 indicating that such initiatives are action-oriented and instrumental; people with dementia are relevant only to the extent of being actively incorporated into discourse.
It is important for people with dementia to be invited and actively integrated into discussions of experiences and needs in new constructions.21 When people with dementia participate in decisions and discussions about personal beliefs and values, society characterizes person-centered practices and culture.4,12,16 In the aforementioned building cases, various interest organizations, such as Alzheimer’s Society, represented people with dementia, a diverse group that essentially has various requirements. Regardless, all people with dementia require holistic, collaborative services that meet health and social care needs and reflect the necessity of retaining social inclusion.47 Additionally, interested organizations may represent other needs that conflict with those of people with dementia.
Furthermore, challenges occur when decisions and facilitation in private and public spaces safeguard groups as a whole rather than individuals. Generally, when verdicts are made and several organizations are involved, final decisions might not align with the needs of people with dementia. Decisions may mirror the common interests of the organizations involved. Additionally, the trade unions safeguard employees’ working conditions and requirements. For example, in new hospital construction,43 the hospital must provide an effective environment for staff that might compete with the requirements of people with dementia.51 Therefore, an appropriate balance must be attained. Often, a tailor-made solution for the individual needs of people with dementia is required.51
In decision-making processes, interested organizations can be challenged when safeguarding the group’s interests. As mentioned, people with dementia are diverse individuals; although some experiences may be shared inside and outside the group, each person has specific concerns and needs. Consequently, private and public spaces may be ineffectively dementia-friendly, such as a museum in which the restrooms are readily available but finding parking is difficult.42 The degree of involvement by people with dementia in generating alternatives as well as planning and evaluating results is significantly related to satisfaction.52 When people with dementia are allowed to participate in decisions and discussions about their beliefs and values, society is characterized by person-centered practice and culture.12,13 This aligns with international guidelines that emphasize the importance of reducing both physical and social barriers to achieve a dementia-friendly society.4,7,16
Strengths and Limitations
This study provides knowledge from the perspective of people with dementia rather than the public and private services that are central to facilitating such a society. Only three studies were found that exclusively included the perspectives of people with dementia. Mixed-participant groups with participation from people with dementia, caregivers, and professionals offered varied results and conclusions. The challenge may be to separate the voices of people with dementia from those of other participants, as supporting relatives may have answered on their behalf. Nine studies were included, which may be a limitation because findings were based only on qualitative studies. By excluding mixed-methods studies, some relevant qualitative data may have been omitted, especially if the quantitative findings were relatively small. The descriptions and PRISMA diagram in the methods section ensured transparency and contributed to the credibility and validity of the results.34 A subject-specialist librarian contributed to the quality assurance of the search process. Additionally, the discussion within the author group regarding the method, analysis, and results strengthened the research validity. The included studies were published in English and in peer-reviewed academic journals, which may have excluded potentially relevant results in other languages and thereby affected the results and conclusion. In the analysis process, the authors reflected and abstracted new themes from the perspectives of people with dementia. This study highlighted the complexity and the significance of dementia-friendly societies and opportunities for people with dementia to live independently and securely.
Conclusion
Having an independent safe life with societal inclusion, both in private and public spaces, is important for people with dementia who live in a dementia-friendly society. To achieve the WHO’s policy goals and care for the needs of people with dementia, society must include them more carefully, ask appropriate questions of the relevant people, and listen to their answers. A society that hears people with dementia and supports their involvement in community and social life is an important part of a dementia-friendly and person-centered culture. To achieve the WHO’s goal, further research should focus on the voices of people with dementia. The consequences of a lack of research regarding people with dementia affect the level of knowledge required to meet the WHO and governmental goals of developing dementia-friendly societies.
Ethics Statement
This review did not need ethical approval.
Acknowledgment
The authors would like to thank the subject-specialist librarian, Vigdis Knutsen, at the National Advisory Unit on Ageing and Health for her valuable contribution in designing and conducting the search strategy.
Author Contributions
All authors made significant contributions to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, or interpretation. JA drafted and revised the article. All authors critically reviewed the article. All authors provided final approval of the version to be published, agreed on the journal to which the article was submitted, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Dementia. Available from: Dementia(who.int).
2. Zhu XC, Tan L, Wang HF, et al. Rate of early onset Alzheimer’s disease: a systematic review and meta-analysis. [Erratum appears in Annals of Translation Medicine 2016 May: 4(9):E4;PMID: 27275503]. Ann Transl Med. 2015;3(3):38. doi:10.3978/j.issn.2305-5839.2015.01.19
3. Norwegian Ministry of Health and Care Services (NMHCS). Action plan. Oslo: Dementia plan 2025; 2020. Available from: DementiaPlan2025-regjeringen.no.
4. World Health Organization (WHO). Towards a Dementia-Inclusive Society: WHO Toolkit for Dementia-Friendly Initiatives (Dfis). Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO; 2021.
5. Gjora L, Strand BH, Bergh S, et al. Current and future prevalence estimates of mild cognitive impairment, dementia, and its subtypes in a population-based sample of people 70 years and older in Norway: the HUNT study. J Alzheimers Dis. 2021;79(3):1213–1226. doi:10.3233/jad-201275
6. Koedam EL, Pijnenburg YA, Deeg DJ, et al. Early-onset dementia is associated with higher mortality. Dement Geriatr Cogn Disord. 2008;26(2):147–152. doi:10.1159/000149585
7. World Health Organization (WHO). Dementia: a public health priority. World Health Organization; 2012. Available from: Dementia:apublichealthpriority(who.int).
8. Johannessen A, Engedal K, Haugen PK, Dourado MCN, Thorsen K. “To be, or not to be”: experiencing deterioration among people with young-onset dementia living alone. Int J Qual Stud Health Well-Being. 2018;13(1):1490620. doi:10.1080/17482631.2018.1490620
9. Spreadbury JH, Kipps C. Measuring younger onset dementia: what the qualitative literature reveals about the ‘lived experience’ for patients and caregivers. Dementia. 2019;18(2):579–598. doi:10.1177/1471301216684401
10. Tranvåg O, Petersen KA, Nåden DJD. Crucial dimensions constituting dignity experience in persons living with dementia. Dementia. 2016;15(4):578–595. doi:10.1177/1471301214529783
11. Norberg A. Identitetsverdighet hos personer med demens [Identity dignity in people with dementia]. Demens Alderspsykiatri. 2016;20(4):26–29. Norwegian.
12. Kitwood T. Dementia Reconsidered: The Person Still Comes First. Brooker D, ed. London: Open University Press; 2019.
13. Fazio S, Pace D, Finner J, Kallmyer B. The fundamentals of person-centered care for individuals with dementia. Gerontologist. 2018;58:10–19. doi:10.1093/geront/gnx122
14. Kirkley C, Bamford C, Poole M, Arksey H, Hughes J, Bond J. The impact of organisational culture on the delivery of person-centered care in services providing respite care and short breaks for people with dementia. Health Soc Care Community. 2011;19(4):438–448. doi:10.1111/j.1365-2524.2011.00998.x
15. Hrybyk RL, Frankowski AC, Nemec M, Peeples AD. “It’s a lot!” The universal worker model and dementia care in assisted living. Geriatr Nurs. 2021;42(1):233–239. doi:10.1016/j.gerinurse.2020.08.006
16. World Health Organization (WHO). Global Action Plan on the Public Health Response to Dementia. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO; 2017.
17. Alzheimer Society. What is a dementia-friendly society? 2022. Available from: https://www.alzheimers.org.uk/get-involved/dementia-friendly-communities/what-dementia-friendly-community.
18. Herbert CA, Scales K. Dementia friendly initiatives: a state of the science review. Dementia. 2017;18(5):1858–1895. doi:10.1177/1471301217731433
19. Martin A, O’Connor S, Jackson C. A scoping review of gaps and priorities in dementia care in Europe. Dementia. 2020;19(7):2135–2151. doi:10.1177/1471301218816250
20. Chemali Z, Schamber S, Tarbi EC, Acar D, Avila-Urizar M. Diagnosing early onset dementia and then what? A frustrating system of aftercare resources. Int J Gen Med. 2012;5:81. doi:10.2147/IJGM.S26523
21. Frank C, Forbes RF. A patient’s experience in dementia care: using the “lived experience” to improve care. Can Fam Physician. 2017;63(1):22–26.
22. Hunderi RIA, Hunder O. The Road into the Land of Mist. Tønsberg: Ageing and Health; 2009.
23. Svanström R, Sundler AJ. Gradually losing one’s foothold – a fragmented existence when living alone with dementia. Dementia. 2015;14(2):145–163. doi:10.1177/1471301213494510
24. Johannessen A, Engedal K, Haugen PK, Dourado MCN, Thorsen K. Coping with transitions in life: a four-year longitudinal narrative study of single younger people with dementia. J Multidiscip Healthc. 2019;12:479–492. doi:10.2147/jmdh.S208424
25. Magnussen I-L, Alteren J, Bondas T. Appreciative inquiry in a Norwegian nursing home: a unifying and maturing process to forward new knowledge and new practice. Int J Qual Stud Health Well-Being. 2019;14(1). doi:10.1080/17482631.2018.1559437
26. Magnussen I-L, Bondas T, Alteren J. The significance of a sensory garden in the formation of “the room of closeness” – an action research in a nursing home (Sansehagens betydning for dannelsen av «nærhetsrommet» - aksjonsforskning i sykehjem). Klin Sygepleje. 2017;31(2):96–113. doi:10.18261/issn.1903-2285-2017-02-03
27. Brooke J, Cronin C, Stiell M, Ojo O. The intersection of culture in the provision of dementia care: a systematic review. J Clin Nurs. 2018;27(17–18):3241–3253. doi:10.1111/jocn.13999
28. Polit DF, Beck CT. Nursing Research. Generating and Assessing Evidence for Nursing Practice.
29. Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0; 2011. Available from: http://handbook.cochrane.org/.
30. Fineout-Overholt E, Johnston L. Teaching EBP: asking searchable, answerable clinical questions. Worldviews Evid Based Nurs. 2005;2(3):157–160. doi:10.1111/j.1741-6787.2005.00032.x
31. Page MJ, McKenzie JE, Bossuyt PM, et al. PRISMA 2020 statement: and updated guideline for repporting systematic review. BMJ. 2021;372:n71. doi:10.1136/bmj.n.71
32. Critical Appraisal Skills Programme (CASP); 2018. Available from: 2CASP-Qualitative-Checklist-2018_fillable_form.pdf(b-cdn.net).
33. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.
34. Graneheim UH, Lundman BM. Qualitative content analysis in nursing research: concepts, procedure, and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
35. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualtiative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
36. Lindgren BM, Lundman B, Graneheim UH. Abstraction and interpretation during the qualitative content analysis process. Int J Nurs Stud. 2020;108:103632. doi:10.1016/j.ijnurstu.2020.103632
37. Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative content analysis: a focus on trustwortiness. SAGE Open. 2014;1–10. doi:10.1177/2158244014522633
38. Milte R, Shulver W, Killington M, Bradley C, Ratcliffe J, Crotty M. Quality in residential care from the perspective of people living with dementia: the importance of peoplehood. Arch Gerontol Geriatr. 2016;63:9–17. doi:10.1016/j.archger.2015.11.007
39. Smith K, Gee S, Sharrock T, Croucher M. Developing a dementia-friendly Christchurch: perspectives of people with dementia. Australas J Ageing. 2016;35(3):188–192. doi:10.1111/ajag.12287
40. Hicks B, Innes A, Nyman SR. Experiences of rural life among community-dwelling older men with dementia and their implications for social inclusion. Dementia. 2021;20(2):444–463. doi:10.1177/1471301219887586
41. Hobden T, Swallow M, Beer C, Dening T. Swimming for dementia: an exploratory qualitative study: innovative practice. Dementia. 2019;18(2):776–784. doi:10.1177/1471301218768372
42. Innes A, Page SJ, Cutler C. Barriers to leisure participation for people with dementia and their carers: an exploratory analysis of carer and people with dementia’s experiences. Dementia. 2016;15(6):1643–1665. doi:10.1177/1471301215570346
43. Digby R, Bloomer MJ. People with dementia and the hospital environment: the view of patients and family carers. Int J Older People Nurs. 2014;9(1):34–43. doi:10.1111/opn.12014
44. Eades M, Lord K, Cooper C. “Festival in a Box”: development and qualitative evaluation of an outreach programme to engage socially isolated people with dementia. Dementia. 2018;17(7):896–908. doi:10.1177/1471301216658158
45. O’Malley M, Innes A, Muir S, Wiener JM. “All the corridors are the same”: a qualitative study of the orientation experiences and design preferences of UK older adult living in a communal retirement development. Ageing Soc. 2018;38(9):1791–1816. doi:10.1017/S0144686X17000277
46. Challen R, Low LF, McEntee MF. Dementia patient care in the diagnostic medical imaging department. Radiography. 2018;24:33–42. doi:10.1016/j.radi.2018.05.012
47. Minogue V. The role of service users and carers in helping to develop and improve services for people with dementia. In: Curran S, Wattis J, editors. Practical Management of Dementia: A Multi-Professional Approach.
48. Cowden S, Singh G. The “User”: friend, foe or fetish? A critical exploration of user involvement in health and social care. Crit Soc Policy. 2007;27(1):5–23. doi:10.1177/0261018307072205
49. Fudge N, Wolfe CDA, McKevitt C. Assessing the promise of user involvement in health service development: ethnographic study. BMJ. 2008;336(7639):313–317. doi:10.1136/bmj.39456.552257.BE
50. Hodge S. Participation, discourse and power: a case study in service user involvement. Crit Soc Policy. 2005;25(2):164–179. doi:10.1177/0261018305051324
51. Fisher LH, Edwards DJ, Pärn EA, Aigbavboa CO. Building design for people with dementia: a case study of a UK care home. Facilities. 2018;36(7/8):349–368. doi:10.1108/F-06-2017-0062
52. Black JS, Gregersen B. Participative decision-making: an integration of multiple dimensions. Human Relation. 1997;50(7):859–878. doi:10.1177/001872679705000705
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.