Back to Journals » Nature and Science of Sleep » Volume 18

Gerontological Effects on Arousal Frequency, Autonomic Balance, and Slow-Wave Sleep During Pressure Adjustments of CPAP in OSA Patients
Authors Liu IJ, Liu WT ![]() , Chien R, Chen YY, Chen YL, Lin YC, Kuan YC
, Chien R, Chen YY, Chen YL, Lin YC, Kuan YC ![]() , Lee KY, Chen TT, Majumdar A, Kang JH
, Lee KY, Chen TT, Majumdar A, Kang JH ![]() , Lai W, Tsai CY
, Lai W, Tsai CY
Received 17 November 2025
Accepted for publication 18 February 2026
Published 11 March 2026 Volume 2026:18 578482
DOI https://doi.org/10.2147/NSS.S578482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
I-Jung Liu,1 Wen-Te Liu,2– 7 Rachel Chien,1 Ying-Ying Chen,1,8 Yen-Ling Chen,9 Yi-Chih Lin,6,10 Yi-Chun Kuan,6,11– 13 Kang-Yun Lee,2,3,14,15 Tzu-Tao Chen,2,3,14,15 Arnab Majumdar,16 Jiunn-Horng Kang,7,9,17,18 Wayne Lai,19,20 Cheng-Yu Tsai1,3,4,6,7,14,21
1Research Center of Sleep Medicine, College of Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 2Division of Pulmonary Medicine, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 3Division of Pulmonary Medicine, Department of Internal Medicine, Taipei Medical University-Shuang Ho Hospital, New Taipei, 23561, Taiwan; 4School of Respiratory Therapy, College of Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 5Advanced Technology Lab, Wistron Corporation, Taipei, 11469, Taiwan; 6Sleep Center, Taipei Medical University-Shuang Ho Hospital, New Taipei, 23561, Taiwan; 7TMU Research Center of Artificial Intelligence in Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 8Center for Artificial Intelligence and Advanced Robotics, National Taiwan University, Taipei, 106319, Taiwan; 9College of Biomedical Engineering, Taipei Medical University, Taipei, 11031, Taiwan; 10Department of Otolaryngology, Taipei Medical University-Shuang Ho Hospital, New Taipei, 23561, Taiwan; 11Department of Neurology, Taipei Medical University-Shuang Ho Hospital, New Taipei, 23561, Taiwan; 12Department of Neurology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 13Taipei Neuroscience Institute, Taipei Medical University, Taipei, 11031, Taiwan; 14TMU Research Center for Thoracic Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 15Graduate Institute of Clinical Medicine, College of Medicine, Taipei Medical University, Taipei, 11031, Taiwan; 16Department of Civil and Environmental Engineering, Imperial College London, London, SW7 2AZ, UK; 17Department of Physical Medicine and Rehabilitation, Taipei Medical University Hospital, Taipei, 11031, Taiwan; 18Graduate Institute of Nanomedicine and Medical Engineering, College of Biomedical Engineering, Taipei Medical University, Taipei, 11031, Taiwan; 19TranQ Medical and Technology Inc, Kelowna, BC V1Y 5A8, Canada; 20Division of Neurology, Department of Medicine, the University of British Columbia, Vancouver, BC V6T 2B5, Canada; 21School of Biomedical Engineering, College of Biomedical Engineering, Taipei Medical University, Taipei, 11031, Taiwan
Correspondence: Cheng-Yu Tsai, School of Biomedical Engineering, College of Biomedical Engineering, Taipei Medical University, 250 Wuxing Street, Taipei, 11031, Taiwan, Tel +886-2-2736-1661, Fax +886-2-2739-1143, Email [email protected]
Objective: Continuous positive airway pressure (CPAP) therapy is recognized as first-line treatment for obstructive sleep apnea (OSA), but tolerance to pressure adjustments may differ with age. In this study, we examined age-related differences in physiological and neurophysiological responses following CPAP pressure adjustment.
Methods: In this retrospective study, we analyzed baseline polysomnography (PSG) and CPAP titration data from 40 individuals, including 20 younger (< 65 years) and 20 older adults (≥ 65 years) matched at the group level. Time-specific analyses were conducted using 10-min windows following pressure adjustments. Group comparisons across predefined pressure categories of CPAP (4– 5, 6– 7, and ≥ 8 cmH2O) and age groups were performed using one-way analysis of variance (ANOVA) or Kruskal–Wallis tests, as appropriate, with post-hoc analyses. Single and multiple linear regression analyses were conducted to assess associations between CPAP pressure categories and physiological responses, using the 4– 5 cmH2O group as the reference and adjusting for prior pressure change history and sleep-stage distribution.
Results: Both age groups demonstrated improvements in sleep architecture and sleep disorder indices during CPAP titration. Among older individuals, analyses of 10-min periods following pressure adjustments showed a higher arousal frequency, increased elevated standard deviation (SD) of normal-to-normal (NN) intervals (SDNN) and low-frequency (LF)/high-frequency (HF) ratios, and reduced slow-wave peak-to-peak amplitudes and slopes compared to younger counterparts. Regression analyses further indicated associations between pressure categories, HRV features, and slow-wave characteristics in the elderly group.
Conclusion: These findings highlight potential age-related differences in short-term responses to pressure adjustments for CPAP. Future prospective studies are needed to validate and enhance the generalizability and robustness of these findings.
Keywords: continuous positive airway pressure titration, arousal event, slow-wave characteristic, heart rate variability, aging, sleep medicine
Introduction
Continuous positive airway pressure (CPAP) therapy is first-line treatment for moderate-to-severe obstructive sleep apnea (OSA).1 Its therapeutic effects in reducing respiratory events and improving sleep quality are well documented.2 However, adherence to CPAP remains a persistent challenge, particularly among older adults.3,4 Previous studies demonstrated that low CPAP compliance diminishes therapeutic efficacies and may exacerbate comorbidities such as cardiovascular,5 metabolic,6 and cognitive dysfunctions.7 These adverse consequences tend to be more pronounced in older individuals, who are generally more susceptible to physiological stress, multimorbidity, and impaired sleep regulation.8 Among the barriers to CPAP use, intolerance to pressure changes remains one of the most frequently reported issues, particularly among older adults who exhibit heightened sensitivity.9 These observations underscore the importance of examining age-related differences in sleep-related physiologic responses across different pressure settings for CPAP.
The standard protocol for determining optimal pressure for CPAP involves stepwise titration during sleep to eliminate respiratory events and oxygen desaturation.10 Clinically, according to American Academy of Sleep Medicine (AASM) guidelines for adults, the pressure of CPAP is increased by at least 1 cmH2O after three apneic events, four hypopneic events, or 5 min of continuous snoring, until reaching an optimal level. The optimal titration pressure is defined as the lowest pressure that reduces the respiratory disturbance index (RDI) to <5 events/h for at least 15 min, including supine rapid eye movement (REM) sleep without frequent arousals or awakenings.11 Although this strategy effectively stabilizes breathing in patients with OSA, higher pressure levels may also increase sleep fragmentation and the arousal frequency.12 These effects may be more pronounced in older adults, who often display age-related alterations in ventilatory control, including higher loop gain and increased upper airway collapsibility.13 A prior study suggested that elderly patients required lower pressure for CPAP titration, potentially reflecting a greater burden of comorbidities as well as changes in respiratory structure and function.14 Hence, while the standard titration effectively addresses respiratory events, understanding its broader implications for sleep physiology in older adults may provide additional insights within existing treatment frameworks.
Beyond sleep arousals, neural-related features, such as slow-wave activity and autonomic regulation, may also be affected by incrementally increased pressures in CPAP.15,16 Specifically, slow-wave activity, defined by electroencephalographic frequencies of 0.3–1.5 Hz, reflects synchronized cortical oscillations essential for memory consolidation and neural recovery.17 Alterations in slow-wave characteristics have been linked to reduced sleep quality, and effects on memory consolidation and cognitive decline.18,19 High pressures during CPAP can also augment sympathetic activation,20 stimulating mechanoreceptors and reflex pathways that destabilize ventilatory control and interfere with the occurrence of slow-wave sleep.21 Prolonged settings for high CPAP may further enhance sympathetic dominance,22 opposing the parasympathetic activity required for deep sleep. Such an autonomic imbalance can be reflected by the heart rate variability (HRV), an index representing the sympathetic-parasympathetic balance and its relationships to memory, emotion, and cardiovascular function.23,24 Previous studies suggested that excessive increases in pulmonary ventilation or airflow during high pressures for CPAP may disturb this autonomic balance.25,26 However, the underlying mechanisms linking pressures for CPAP to alterations in slow-wave activity and HRV have not yet been systematically investigated, particularly in the context of age-related physiological differences.
In this study, we explored age-related differences in sleep disorder indices, slow-wave characteristics, and HRV features across pressure levels for CPAP titration. The dataset included 40 participants—20 younger and 20 older individuals—from northern Taiwan, comprising both baseline polysomnography (PSG) and CPAP titration recordings. Beyond conventional sleep parameters, we further examined slow-wave characteristics and HRV features under different pressure settings in each age group. We hypothesized that elderly individuals with OSA would exhibit more-frequent arousals, greater alterations in autonomic regulation, and reduced slow-wave sleep quality and quantity compared to younger individuals. The null hypothesis was that no age-related differences would be observed across pressure levels for CPAP. Findings of this study may enhance our understanding of physiological changes associated with pressure adjustments for CPAP in both younger and older individuals with OSA. These observations also highlight the importance of examining age-related differences in physiologic responses across different pressure settings for CPAP.
Materials and Methods
Ethical Statement
This study was approved by the Joint Institutional Review Board (IRB) of Taipei Medical University (approval no. TMU-N202508084, approval date: August 26, 2025), and was conducted in accordance with guidelines of the Declaration of Helsinki. Data collection, anonymization, analysis, and storage were performed in full compliance with the approved research protocol. Given the retrospective design and the absence of any risk to the rights or welfare of participants, the requirement for informed consent was waived by the IRB.
Study Design and Participant Enrollment
This retrospective study collected data from the Sleep Center of Taipei Medical University – Shuang Ho Hospital between June 2023 and December 2024. Participants were identified using a consecutive sampling approach from patients referred for a PSG examination and CPAP titration. Eligible individuals met the following inclusion criteria: (1) aged 20–85 years; (2) having completed both baseline PSG and CPAP titration within a 3-month interval; and (3) with no prior history of invasive treatment for OSA, such as otorhinolaryngological surgery. The requirement that baseline PSG and CPAP titration be completed within a 3-month interval was chosen to align with real-world scheduling practices for PSG examinations. This timeframe accounts for systemic constraints, such as limited laboratory availability and extensive patient waiting lists, while aiming to minimize potential changes in an individual’s health status and to ensure adequate sample retention. Baseline characteristics, including gender, age, body-mass index (BMI), neck circumference, and waist circumference, were obtained from electronic medical records. Sleep reports of both examinations and their corresponding physiological signal data were retrieved. The younger (< 65 years) and older (≥ 65 years) cohorts were balanced at the group level through matching for sex, BMI, and OSA severity to ensure comparability between the two cohorts.
Sleep Data Collection and Preprocessing
Overnight in-laboratory PSG was conducted using a ResMed Embla N7000 (ResMed, San Diego, CA, USA) and an Embla MPR (ResMed Global Supplier Alliance, Sydney, Australia) both before and during CPAP titration. Multiple physiological signals were recorded, including electromyography, electroencephalography (EEG), electrocardiography (EKG), respiratory patterns, and oxygen saturation. All recorded signals were analyzed and scored using RemLogic software (vers. 3.41, Embla, Thornton, CO, USA) by licensed technicians who attended monthly training sessions to ensure accuracy, aligning with the 2017 AASM manual.27 CPAP titration was performed following standardized stepwise titration protocols.11 Sleep parameters of interest included sleep architecture—wake, REM, and non-REM (NREM) stages—along with the arousal index (ArI), apnea-hypopnea index (AHI), and oxygen desaturation index (ODI). Additionally, apneic and hypopneic events were identified and expressed as total counts. Pressures of CPAP were categorized into three predefined groups (4–5, 6–7, and ≥ 8 cmH2O) to reflect common titration steps and variability in pressure adjustment settings (eg, increments of 1 or 2 cmH2O). This standardized categorization ensured sufficient observations within each pressure category to support robust statistical comparisons across both age groups. To evaluate acute physiological responses to pressure increments and align with the titration protocol—particularly given that some pressure adjustments occur rapidly during early titration stages—data were analyzed using standardized 10-min windows immediately following each pressure adjustment within the predefined categories. This approach enabled the assessment of temporal changes across different pressure levels.
Slow-Wave Detection and HRV Analysis
Slow-wave activity throughout the night was quantified from EEG signals using the YASA open-source Python toolbox (vers. 0.6.5; Python Software Foundation, Fredericksburg, VA, USA). Slow-wave detection was adapted from previously published methods with minor modifications.28 EEG signals from the F4 electrode channel were band-pass filtered between 0.3 and 1.5 Hz to isolate slow-wave activity, consistent with the reference approach. Candidate slow waves were identified as negative-positive deflections with a peak-to-peak (PTP) amplitude of ≥ 75 µV. In the present study, a minimum duration threshold of ≥ 0.5 s was additionally applied to standardize detection across recordings. Several slow-wave parameters were selected based on prior research linking these features to OSA–related neurophysiological alterations and sleep disruption.29 For each detected slow wave, the mean PTP amplitude, slope between the negative peak and the subsequent mid-crossing, wave duration, and total number of slow waves were automatically computed. The slow-wave index was defined as the average number of detected slow waves per minute of sleep.
HRV features were derived from EKG signals using the hrv-analysis open-source Python module (vers. 1.0.4; Python Software Foundation, Fredericksburg, VA, USA), with a sliding-window approach (60-s window with a 30-s stride) to capture short-term autonomic dynamics during a 10-min interval.30 This study selected heart rate variability (HRV) features that are commonly used markers of autonomic nervous system regulation, including both time- and frequency-domain metrics (Table S1). Time-domain features included the standard deviation (SD) of normal-to-normal (NN) intervals (SDNN), root mean square of successive differences (RMSSD), and the proportion of adjacent NN intervals that differ from each other by more than 50 ms (NN50) relative to total NNs (pNN50). Frequency-domain metrics included normalized low frequency (LF; nLF), normalized high frequency (HF; nHF), and the LF/HF ratio were determined. To reduce the influence of signal artifacts in EKG recordings, heart rate values below 40 beats per minute (bpm) or above 90 bpm were interpolated using median values.31 These thresholds were selected based on prior studies defining heart rates above 90 bpm as sinus tachycardia and below 40 bpm as bradycardia during sleep.32 Within short HRV analysis windows, such extreme values are more likely to reflect artifacts rather than stable physiological patterns; therefore, interpolation was applied to preserve HRV metric continuity.
Statistical Analysis
All statistical analyses were performed utilizing Python (vers. 3.13.5; Python Software Foundation). A two-tailed p value of < 0.05 was considered statistically significant for all statistical tests. Individual participants could contribute data multiple times—or not at all—to a given pressure category. In addition, analyses of HRV features and slow-wave characteristics required artifact-free signal segments, leading to the exclusion of some observations when valid data were unavailable. As a result, sample sizes varied across analyses due to differences in data availability.
The Shapiro–Wilk test was first applied to assess the normality of continuous variables. Depending on the data distribution, group comparisons were conducted using Student’s t-test for normally distributed variables or the Mann–Whitney U-test for non-normally distributed variables. For comparisons involving three groups, a one-way analysis of variance (ANOVA) with Tukey’s post-hoc test was performed for normally distributed data, while the Kruskal–Wallis test with Dunn’s post-hoc test was used for non-normally distributed variables. A Chi-squared test was used to evaluate differences in categorical variables. Using the 4–5 cmH2O group as a reference, simple linear regression models were employed to examine associations of predefined pressure categories of CPAP (6–7 and ≥ 8 cmH2O) with sleep disorder indices, HRV features, and slow-wave characteristics. Multiple linear regression models were further adjusted for the prior pressure change history and sleep-stage distribution (ie, wake, REM, and NREM durations). A post-hoc power analysis was conducted for overall pressure-group comparisons using Cohen’s f and an F-test-based approach with a two-sided significance level of α=0.05. Results are summarized in Supplementary Materials, Tables S2 and S3.
Results
Baseline Demographics and Sleep Parameters Before CPAP Titration
Table 1 presents comparisons of demographic information and sleep parameters recorded during baseline PSG examinations between the elderly and young groups. The mean age of the elderly group (72.00 ± 5.27 years) was significantly higher than that of the young group (38.60 ± 7.35 years, p < 0.01). Other demographic variables, including gender, BMI, neck circumference, and waist circumference were comparable between the two groups. Regarding sleep architecture, the elderly group exhibited a significantly longer wake after sleep onset (WASO; 90.1 ± 42.20 vs 68.39 ± 59.26 min) and a higher proportion of wake stage relative to total sleep time (21.72% ± 14.38% vs 14.22% ± 17.46%, both p < 0.05) compared to the young group. Conversely, no significant differences were found in sleep efficiency, the ODI, AHI, or ArI between the two groups.
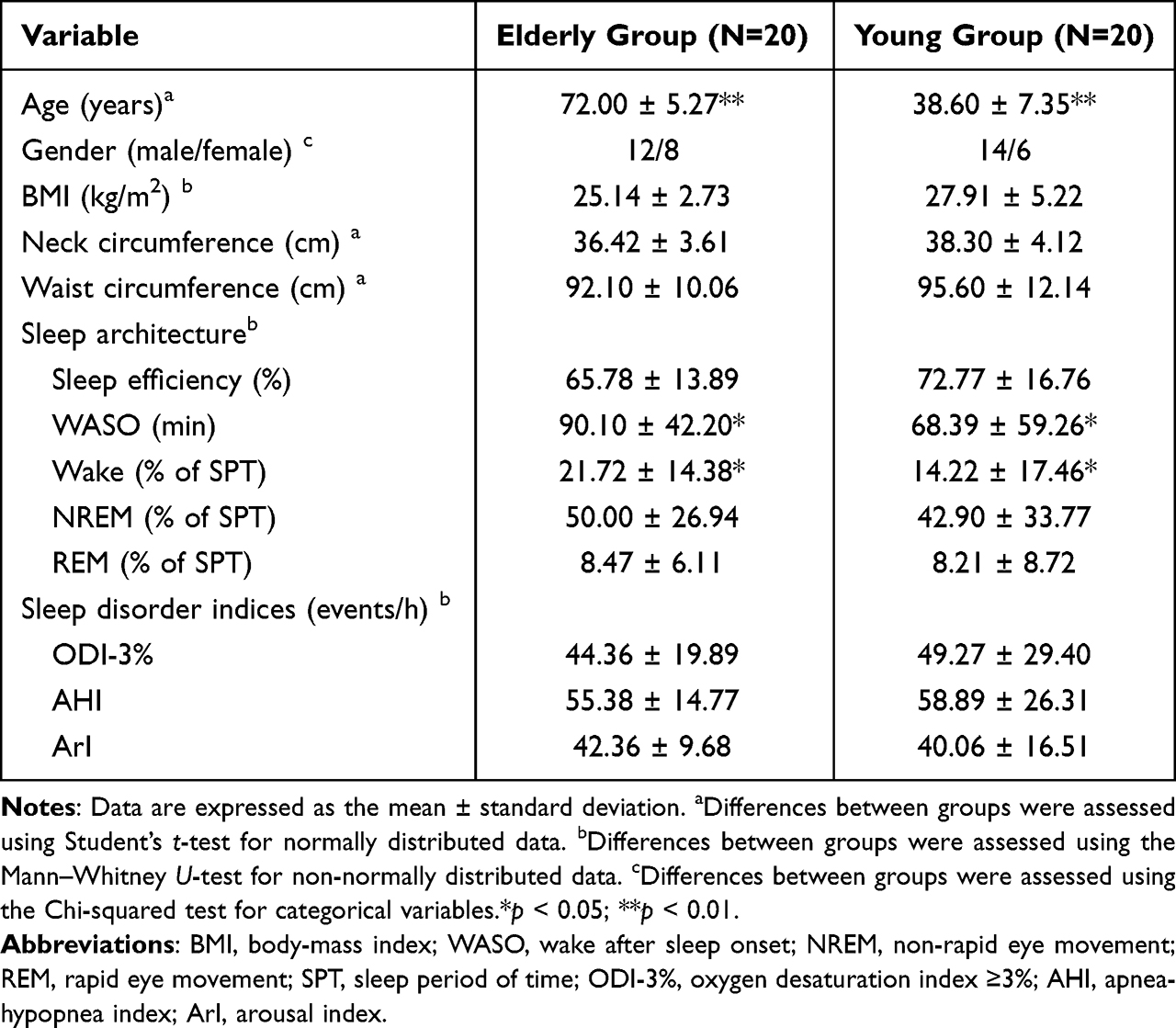 |
Table 1 Comparisons of Baseline Demographics and Sleep Parameters During Baseline PSG (N=40) |
Sleep Parameters Between CPAP Titration and PSG
Comparisons of sleep parameters between the CPAP titration and baseline PSG examinations are demonstrated in Table 2. The mean optimal pressure of CPAP was 9.75 ± 3.86 cmH2O in the elderly group and 8.65 ± 3.70 cmH2O in the young group. In the elderly group, the proportion of the NREM stage relative to total sleep time (77.66% ± 11.62%) was significantly higher during CPAP titration than during the PSG test (50.00% ± 26.94%, p < 0.01). However, no significant differences were found in the sleep efficiency, wake ratio, or REM ratio between the two sessions. In terms of sleep disorder indices, ODI values were significantly lower during CPAP titration (7.62 ± 6.55 events/h) compared to the PSG examination (44.36 ± 19.89 events/h, p < 0.01). Similar improvements were observed for the AHI (7.36 ± 5.80 vs 55.38 ± 14.77 events/h) and ArI (21.67 ± 10.62 vs 42.36 ± 9.68 events/h, both p < 0.01).
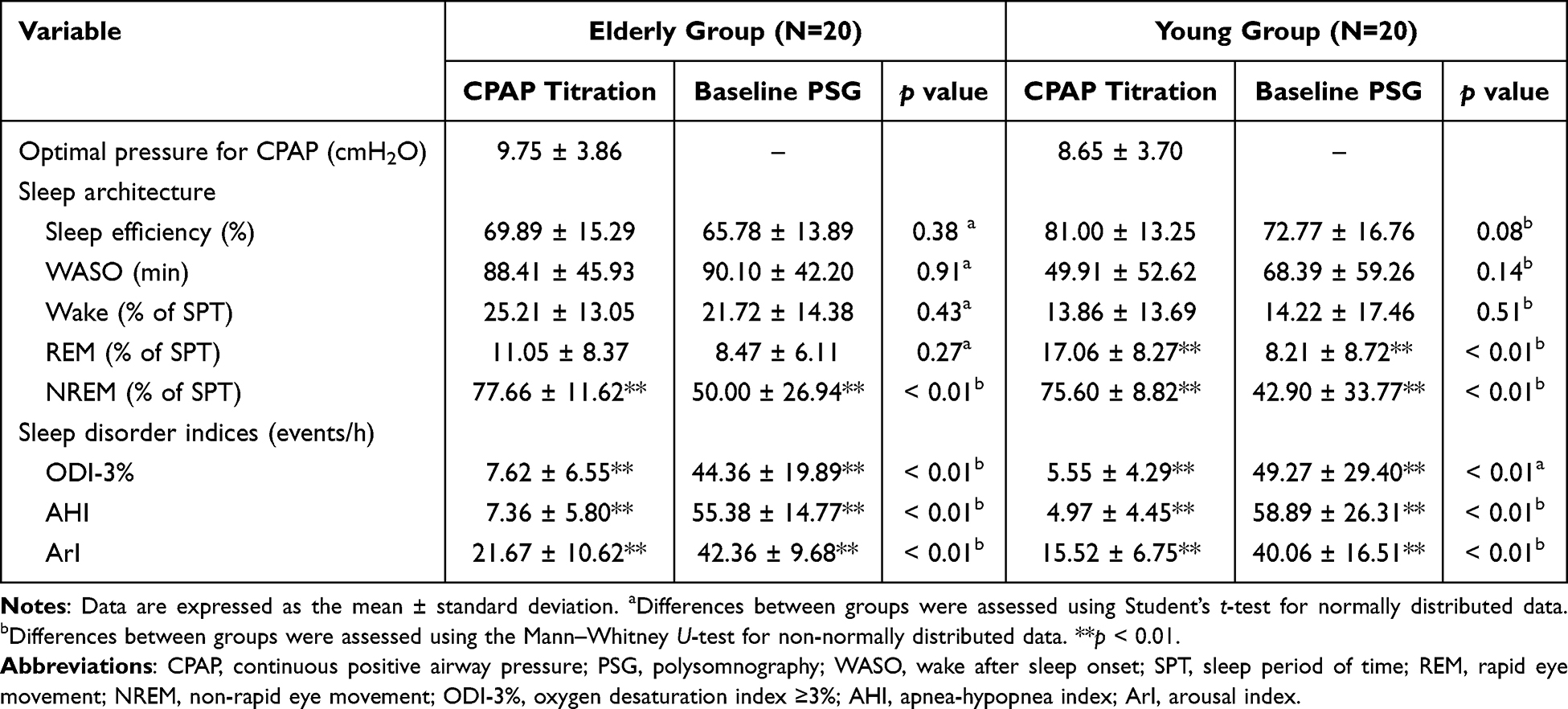 |
Table 2 Comparisons of Sleep Parameters Between CPAP Titration and Baseline PSG (N=40) |
The young group exhibited a significantly higher NREM ratio during CPAP titration (75.60% ± 8.82%) than during the PSG test (42.90% ± 33.77%, p < 0.01). The proportion of the REM stage relative to total sleep time was also significantly higher during CPAP titration (17.06% ± 8.27%) compared to the PSG examination (8.21% ± 8.72%, p < 0.01). Conversely, ODI values were significantly reduced during CPAP titration (5.55% ± 4.29%) than during PSG (49.27% ± 29.40%, p < 0.01). Both AHI and ArI values were also significantly lower during CPAP titration compared to PSG (both p < 0.01).
Sleep and Autonomic Responses Within 10 min After Pressure Modifications of CPAP
Each participant contributed 3.85 ± 1.76 windows (range: 1–6 windows/participant) in the young group and 4.45 ± 1.61 windows (range: 1–6 windows/participant) in the elderly group, depending on the number of pressure adjustments within predefined pressure categories during titration. Table 3 summarize changes in sleep disorder indices, HRV features, and slow-wave characteristics within a 10-min interval following pressure adjustments of CPAP among elderly participants across different pressure categories. The trends of arousal events and slow-wave characteristics across pressure categories are illustrated in Figure 1. Arousal events were significantly lower under pressures of 4–5 cmH2O (2.11 ± 2.93) compared to pressures of 6–7 cmH2O (4.10 ± 2.96) and ≥ 8 cmH2O (4.46 ± 2.82, both p < 0.01). Although hypopneic events showed an increasing trend with higher pressure levels, no significant differences were observed among the three groups. Similarly, SDNN values were significantly lower under the 4–5 cmH2O condition (59.32 ± 45.41 ms) than under 6–7 cmH2O (65.64 ± 47.77 ms) and ≥ 8 cmH2O (71.98 ± 57.09 ms, both p < 0.05). The RMSSD exhibited a slight upward trend with increasing pressure but did not significantly differ across the pressure groups. As for slow-wave characteristics, elderly participants demonstrated significantly greater mean PTP and slope values under pressures of 4–5 cmH2O (126.30 ± 28.45 µV; 452.73 ± 138.69 µV/s) than under pressures ≥ 8 cmH2O (104.02 ± 18.61 µV; 306.43 ± 85.25 µV/s, both p < 0.05). Conversely, the mean slow-wave duration was significantly shorter at pressures of 4–5 cmH2O (1.24 ± 0.15 s) compared to 6–7 cmH2O (1.37 ± 0.25 s) and ≥ 8 cmH2O (1.48 ± 0.29 s, both p < 0.05). No significant differences were found in the slow-wave index among the three pressure groups. Subgroup analyses comparing initial and optimal CPAP pressures in the elderly group are presented in Table S4.
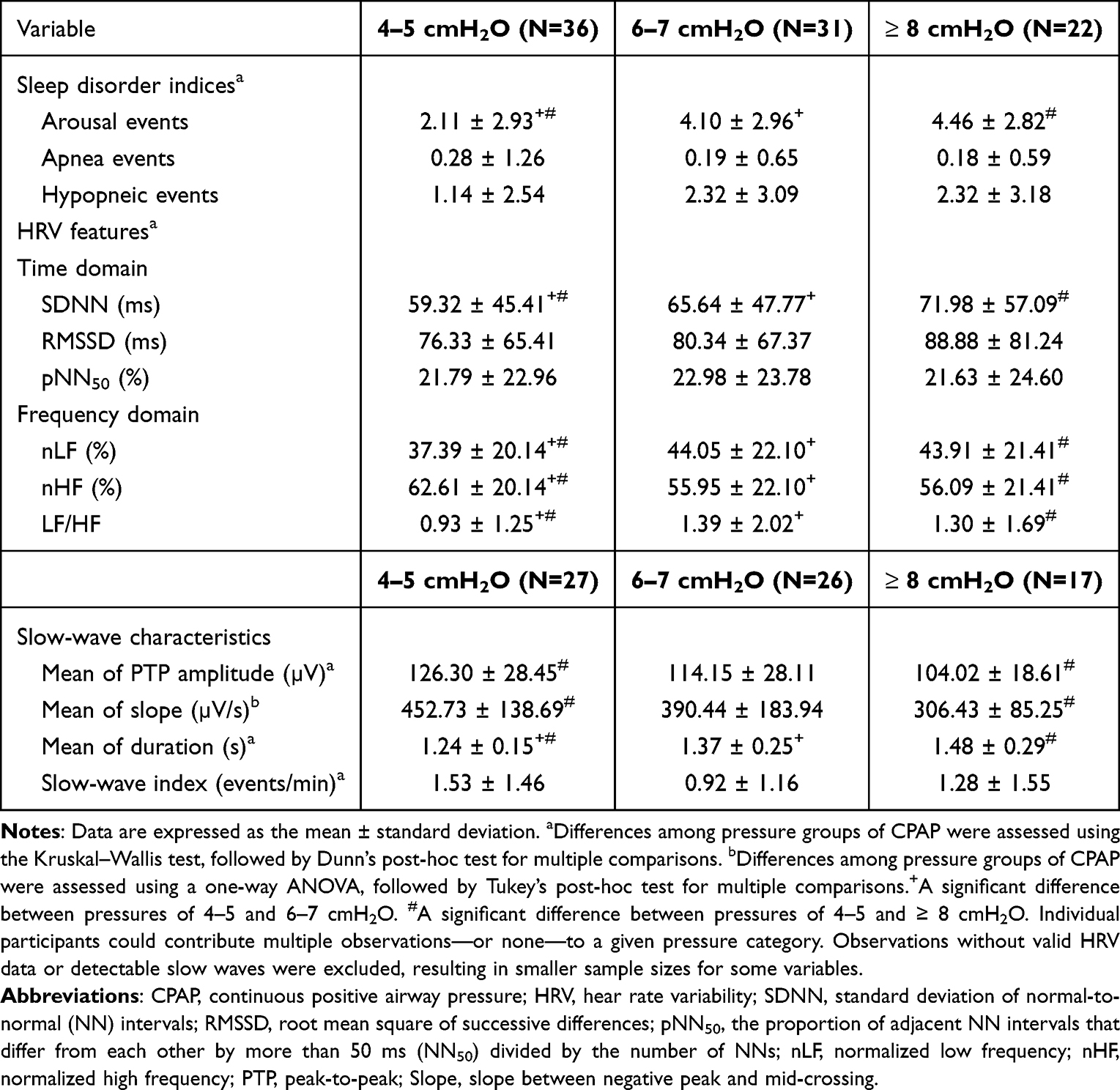 |
Table 3 Physiological and Neurophysiological Changes Within 10 min After Pressure Adjustment During CPAP Among Elderly Individuals Across Different Pressure Categories (cmH2O) |
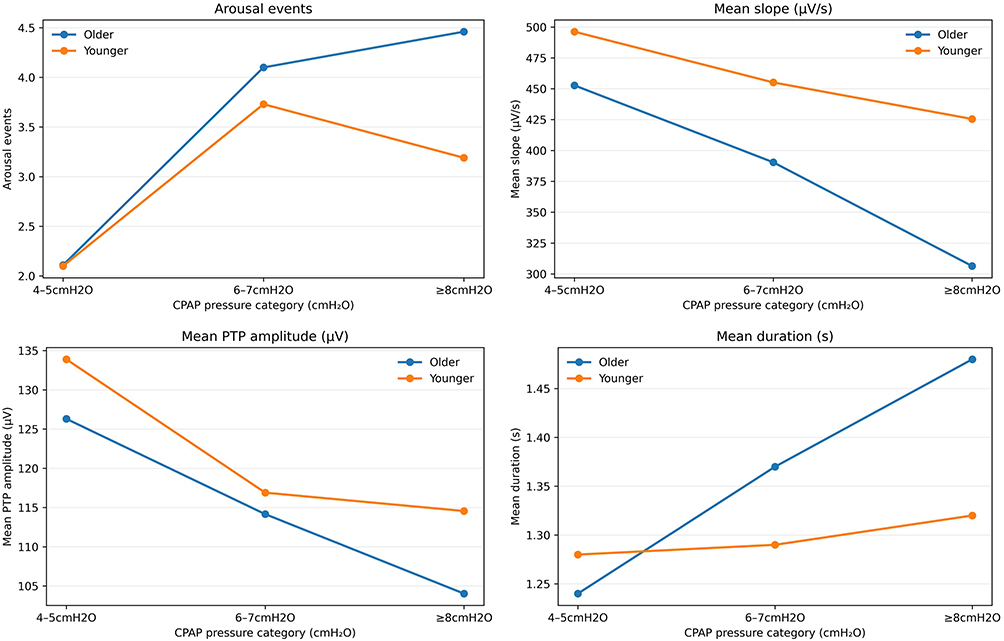 |
Figure 1 Trends in Arousal Events and Slow-wave Characteristics Across Pressure Categories of CPAP. Changes in total arousal events and slow-wave metrics (PTP amplitude, slope, duration, and slow-wave index) across three predefined pressure categories (4–5, 6–7, and ≥ 8 cmH2O). The blue line represents the elderly group, while the orange line represents the younger group. Abbreviations: CPAP, continuous positive airway pressure; PTP, peak-to-peak; Slope, slope between the negative peak and mid-crossing. |
Young participants exhibited different trends in physiological and neurophysiological variables after pressure adjustments of CPAP across different pressure groups (Table 4). Corresponding trends in HRV features across pressure categories are illustrated in Figure 2. No significant differences were observed in sleep disorder indices among the three groups. However, time-domain HRV features—SDNN (57.59 ± 37.38 ms), RMSSD (65.27 ± 52.04 ms), and pNN50 (18.02% ± 15.53%)—were significantly higher at pressures of 4–5 cmH2O compared to 6–7 cmH2O and ≥ 8 cmH2O (all p < 0.05). In the frequency domain, the nLF was lower at pressures of 4–5 cmH2O (44.15% ± 22.78%) and 6–7 cmH2O (43.53% ± 22.25%) compared to ≥ 8 cmH2O (47.93% ± 21.07%, both p < 0.05). In contrast, the nHF was higher at pressures of 4–5 cmH2O (55.85% ± 22.78%) and 6–7 cmH2O (56.47% ± 22.25%) than at ≥ 8 cmH2O (52.07% ± 21.07%, both p < 0.05). The LF/HF ratio was highest at 4–5 cmH2O compared to the other two pressure levels (both p < 0.05). Among slow-wave characteristic, the mean PTP amplitude was higher at pressures of 4–5 cmH2O (133.89 ± 26.27µV) compared to 6–7 cmH2O and ≥ 8 cmH2O (both p < 0.05).
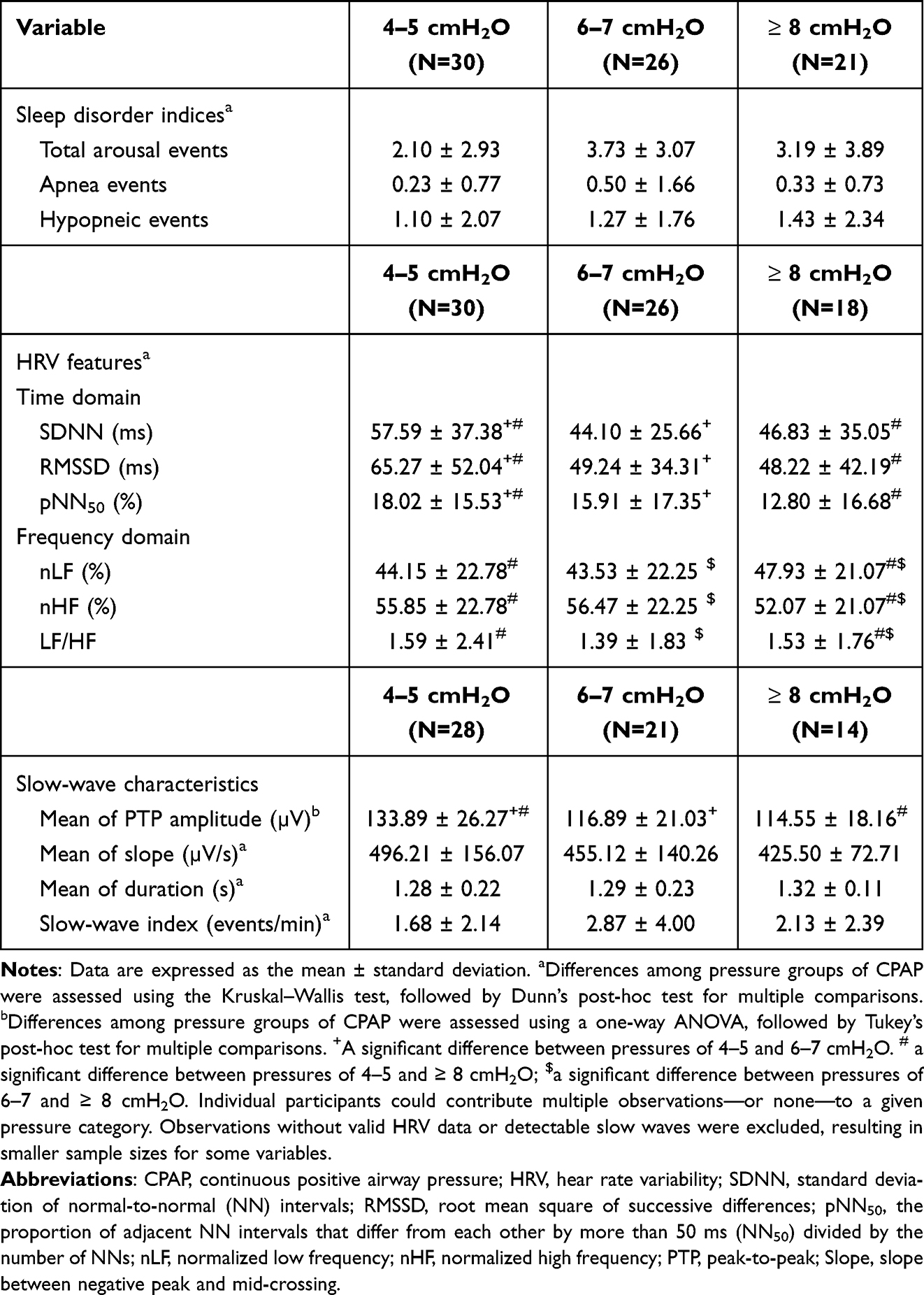 |
Table 4 Physiological and Neurophysiological Changes Within 10 min After Pressure Adjustment for CPAP Among Young Individuals Across Different Pressure Categories (cmH2O) |
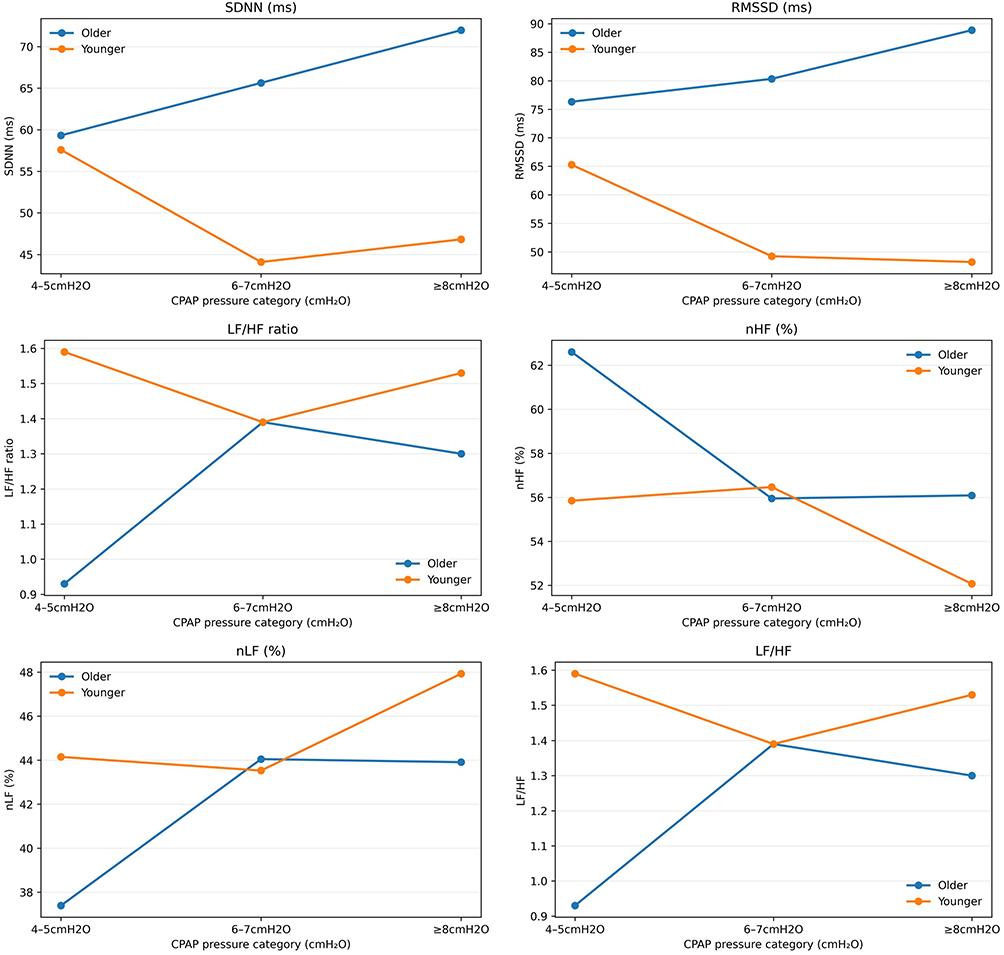 |
Figure 2 Trends in HRV Features Across Pressure Categories of CPAP. Changes in HRV features, including the time-domain and frequency domain, across three predefined pressure categories (4–5, 6–7, and ≥ 8 cmH2O). The blue line represents the elderly group, while the orange line represents the younger group. Abbreviations: HRV, hear rate variability; CPAP, continuous positive airway pressure; SDNN, standard deviation of normal-to-normal (NN) intervals; RMSSD, root mean square of successive differences; pNN50, the proportion of adjacent NN intervals that differ from each other by more than 50 ms (NN50) divided by the number of NNs; nLF, normalized low frequency; nHF, normalized high frequency. |
Associations Between Pressure Increments in CPAP and Physiological Responses
Table 5 presents associations between pressures categories of CPAP and sleep disorder indices, HRV features, and slow-wave characteristics in the elderly group. Compared to the reference group (4–5 cmH2O), pressures of 6–7 cmH2O were associated with a higher number of arousal events (β = 1.89, 95% CI: 0.46–3.32, p < 0.05), while pressures of ≥ 8 cmH2O showed a stronger association (β = 2.54, 95% CI: 0.96–4.11, p < 0.01). Similarly, both 6–7 cmH2O (β = 6.33, 95% CI: 0.98–11.68, p < 0.05) and ≥ 8 cmH2O (β = 12.66, 95% CI: 6.80–18.53, p < 0.01) were associated with higher SDNN values relative to the reference group. In the frequency domain, higher pressure categories of CPAP were associated with increased nLF (β = 6.51–6.65, both p < 0.01) and decreased nHF. The LF/HF ratio was also associated with pressures of 6–7 cmH2O (β = 0.46, 95% CI: 0.28–0.64, p < 0.01) and ≥ 8 cmH2O (β = 0.37, 95% CI: 0.17–0.57, p < 0.01), compared to the 4–5 cmH2O group. Regarding slow-wave characteristics, pressures of ≥ 8 cmH2O were associated with lower mean PTP amplitudes (β = −22.29, 95% CI: −38.54–-6.03, p < 0.01) and reduced mean slopes (β = −146.30, 95% CI: −237.59–-55.00, p < 0.01), relative to the reference group. Additionally, a longer mean slow-wave duration was associated with pressures of 6–7 cmH2O (β = 0.13, 95% CI: 0.01–0.26) and ≥ 8 cmH2O (β = 0.24, 95% CI: 0.10–0.38, both p < 0.01). Multiple linear regression analyses adjusting for prior pressure change history and sleep-stage distribution are presented in Table S5.
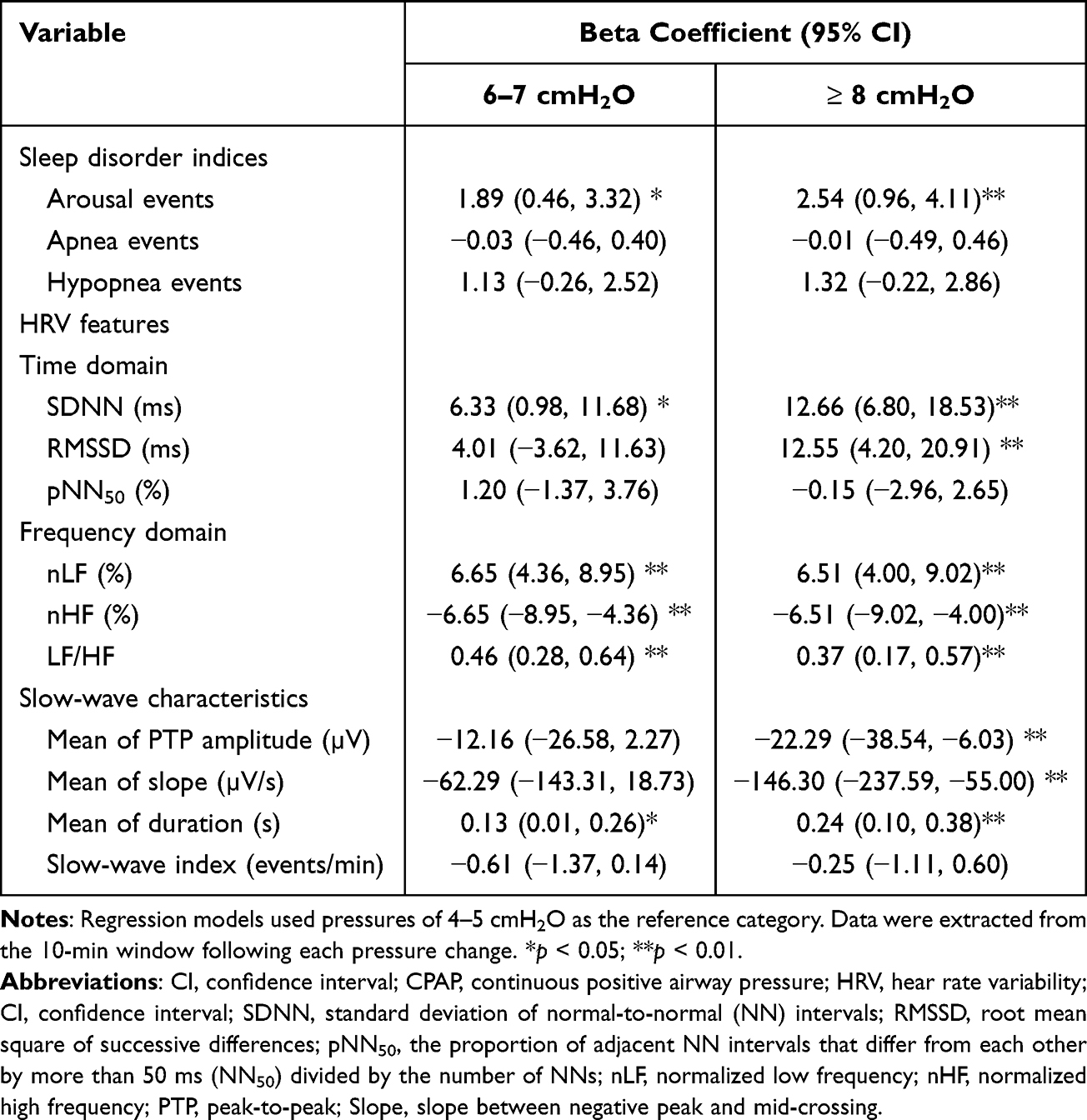 |
Table 5 Single Linear Regression Analysis of Incremental CPAP Pressure Categories with Sleep Disorder Indices, HRV Features, and Slow-Wave Characteristics Among Elderly Individuals (N=20) |
Discussion
Results revealed different physiological responses to incremental increases in pressure levels for CPAP between the young and elderly group, despite comparable baseline demographics. Both age groups showed significant improvements in sleep architecture and sleep disorder indices during CPAP titration. However, incremental increases in pressure during CPAP were accompanied by significantly higher arousal events, elevated SDNN, nLF, and LF/HF ratio values, and reduced PTP amplitude and slope in the elderly group. Regression analyses further revealed that higher pressure levels were associated with an increased arousal frequency, enhanced sympathetic activation, and diminished slow-wave sleep quality among older participants. Notably, these physiological alterations were also found under the optimal pressure settings.
The two age groups demonstrated comparable gender distributions, BMI values, and OSA severity levels, except that the elderly group had a significantly longer WASO duration and a higher proportion of wake relative to total sleep time. These findings are consistent with a previous study reporting that older adults with OSA tend to experience prolonged wake periods during sleep.33 Age-related physiological changes in sleep regulation—such as increased unintentional napping, cognitive decline, and sleep fragmentation—may partially account for this observation.34 In addition, the higher prevalence of central sleep apnea in older adults, which is often accompanied by frequent awakenings, may further contribute to the extended WASO duration observed in this age group.35 Regarding differences between sleep parameters recorded during CPAP titration and the baseline PSG, both groups exhibited a significantly higher proportion of the NREM stage relative to total sleep time during CPAP titration. Moreover, significant improvements were observed in sleep disorder indices, including the ODI, AHI, and ArI, across both age groups. These findings align with previous reports demonstrating the therapeutic efficacy of CPAP in alleviating OSA-related manifestations.36,37 However, despite the well-established benefits of CPAP therapy, the physiological and neurophysiological outcomes of incremental pressure adjustments remain insufficiently explored.
Different patterns of sleep disorder indices, HRV features, and slow-wave characteristics were observed between the young and elderly groups within the 10-min intervals following pressure adjustments of CPAP. Notably, a significant increase in arousal events with higher pressure settings was exclusively observed in the elderly group. This finding suggests that older adults may exhibit heightened sensitivity to pressure fluctuations during CPAP titration, potentially related to age-associated alterations in ventilatory control and upper airway mechanics.38 Conversely, hypopneic events showed a non-significant upward trend across pressure categories in the elderly group, diverging from the general expectation that higher pressures reduce such events. Despite a small effect size and statistical power, this discrepancy may be related to transient respiratory instability occurring within the 10-min period following pressure adjustments, as older adults may require more time to achieve physiological adaptation. The absence of this pattern in younger participants further highlights age-related differences in short-term adaptive responses. Such transient instability may partly explain why elderly individuals required higher optimal pressures for CPAP than younger counterparts, despite comparable baseline OSA severities. Further investigation is warranted to validate and expand these findings.
Consistently, an upward trend in the LF/HF ratio was observed in the elderly group across higher pressure categories of CPAP, while the young group showed the highest LF/HF at lower pressure levels (4–5 cmH2O). These results may reflect a transient autonomic imbalance occurring during the short period following pressure adjustments. In particular, the elevated LF/HF observed within the 10-min analysis window may have been influenced by arousal-related variability, sleep fragmentation, or rapid fluctuations in cardiorespiratory coupling immediately after the pressure increment.39 Notably, changes in HRV features showed age-specific patterns. SDNN and RMSSD did not exhibit consistent parallel changes with the LF/HF ratio, suggesting that the observed variability measures may reflect mixed influences of arousal frequency, altered sleep continuity, and short-term autonomic instability. This paradoxical pattern likely reveals a compensatory parasympathetic rebound following arousal-related sympathetic surges.40 Among older adults, age-related reductions in the baroreflex sensitivity and ventilatory stability may exacerbate an alternating pattern of sympathetic activation and parasympathetic recovery following pressure adjustments.41 Regarding slow-wave characteristics, older individuals exhibited reductions in the mean PTP amplitude and slope, accompanied by a prolonged mean duration. While CPAP treatment is traditionally known to restore reduced slow-wave amplitudes in OSA patients to levels comparable to healthy controls,42 the discrepancies observed in our cohort may be attributed to the short-term observation window immediately after pressure adjustments that disrupted cortical synchronization. In addition, age-related changes in the cortical structure and reduced slow-wave generation may increase susceptibility to such transient disturbances.43 In younger individuals, concurrent reductions in the PTP amplitude and HRV features across higher pressure categories of CPAP may similarly reflect short-term arousal-related autonomic and cortical responses following pressure adjustments, rather than sustained sympathetic dominance. Consistent patterns were also observed when comparing the 10-min intervals following pressure adjustments of CPAP between the initial and optimal titration pressures among the elderly group. Additionally, in the elderly group, higher pressure levels (≥ 8 cmH2O) during CPAP were significantly associated with increased arousal events, augmented sympathetic activity, and attenuated slow-wave characteristics relative to 4–5 cmH2O. These findings highlight that pressure adjustments may be associated with concurrent changes in the arousal frequency, autonomic regulation, and slow-wave characteristics, particularly in older adults. Therefore, physiological responses related to autonomic and cortical stability—such as the arousal frequency, HRV features, and slow-wave activity—may provide a complementary context to respiratory indices during CPAP titration.
This study has several strengths. To our knowledge, it is the first to examine the effects of incremental pressure changes during CPAP on physiological and neurophysiological outcomes, including sleep disorder indices, HRV features, and slow-wave characteristics. Also, the inclusion of both younger and older participants with comparable demographics strengthened the reliability of the observed age-dependent responses to pressure adjustments during CPAP. Additionally, time-specific analyses offered insights into temporal interactions of incremental pressure levels of CPAP with sleep regulation, autonomic function, and cortical activity. These observations suggest that age-related differences may influence adaptation to pressure changes. Specifically, older adults may benefit from more-gradual pressure increments or extended stabilization intervals between adjustments to facilitate physiological adaptation. Future prospective studies are warranted to validate these hypotheses and determine whether age-specific titration strategies can improve sleep stability and treatment tolerance without compromising therapeutic efficacy. Furthermore, exploring the role of oral appliances in the therapeutic pathway may provide valuable insights into managing age-related differences in treatment tolerance.44
Several limitations should be acknowledged. Despite IRB approval and the inclusion of multiple physiological parameters, the retrospective, single-center design and relatively small sample size limit the generalizability and ability to make causal inferences. In addition, the absence of randomized or interventional clinical trial data precludes definitive conclusions regarding treatment effects. Accordingly, this study should be interpreted as exploratory and hypothesis-generating. Pressures of CPAP were grouped into three predefined categories that were consistently applied across age groups to ensure sufficient observations within each category and facilitate comparability. However, this standardized categorization might not fully capture individual-level optimal pressure ranges and may limit generalizability to other populations. Future studies involving larger and more-diverse cohorts, as well as alternative pressure categorizations or individualized pressure modeling approaches, are warranted. Next, although time-specific analyses were used to characterize short-term physiological responses following pressure adjustments, multiple observations per individuals across different pressure categories were included. This may have introduced within-subject dependency that was not fully accounted for in the current analytical framework, thereby constraining the robustness of causal inferences. Future prospective studies employing longitudinal or mixed-effects modeling approaches are needed to validate and extend these findings. In addition, although the sleep stage distribution within the analysis windows and prior pressure adjustment history were accounted for in the multiple regression analyses, factors such as medication use and comorbid conditions may also contribute to inter-individual variability and warrant further examination. While a standardized fixed-amplitude threshold was applied for slow-wave identification to ensure analytical consistency across individuals, age-related attenuation of EEG amplitudes may influence slow-wave detection. In addition, while preprocessing of EKG signals was implemented to reduce transient artifacts, this approach may have attenuated true extreme values. Thus, findings related to slow-wave characteristics and HRV features should be interpreted as relative differences across pressure categories rather than absolute measures of cortical slow-wave generation and autonomic activity. Future research incorporating age-specific or individualized detection criteria are warranted to validate and improve the robustness of the results. Finally, the 3-month interval and the10-min analysis window reflected routine clinical workflows but may inherently introduce bias related to unmeasured physiological changes. Future prospective studies are needed to investigate longer-term physiological effects of sustained CPAP pressure exposure.
Conclusions
This study examined temporal physiological and neurophysiological responses to pressure adjustments during CPAP in younger and older individuals. In the elderly group, increased arousal events and an elevated LF/HF ratio were linked to relatively high pressure levels, along with a lower slow-wave PTP amplitude and slope. Regression analyses further indicated associations between pressure categories and alterations in autonomic regulation and changes in restorative sleep characteristics among elderly individuals. These findings suggest the potential value in incorporating age-related considerations into CPAP titration to support therapeutic efficacy while reducing sleep instability in elderly patients. Future prospective studies are needed to validate age-specific titration strategies and to enhance the generalizability and robustness of these findings.
Abbreviations
AASM, American Academy of Sleep Medicine; AHI, apnea-hypopnea index; ArI, arousal Index; AUROC, area under the receiver operating characteristic curve; BMI, body-mass index; BPM, beats per minute; CI, confidence interval; CPAP, continuous positive airway pressure; EEG, electroencephalography; EKG, electrocardiography; HF, high frequency; HRV, heart rate variability; IRB, Institutional Review Board; LF, low frequency; nHF, normalized high frequency; nLF, normalized low frequency; NREM, non-rapid eye movement; ODI-3%, oxygen desaturation index ≥3%; OSA, obstructive sleep apnea; pNN50, the proportion of adjacent NN intervals that differ from each other by more than 50 ms (NN50) divided by numbers of NNs; PSG, polysomnography; PTP, peak-to-peak; RDI, respiratory disturbance index; REM, rapid eye movement; RMSSD, root mean square of successive differences; SDNN, standard deviation (SD) of normal-to-normal (NN) intervals; WASO, wake after sleep onset.
Data Sharing Statement
All data were retrospectively collected from the Sleep Center of Taipei Medical University–Shuang Ho Hospital between June 2023 and December 2024. The dataset is not publicly available due to the inclusion of personal information. Requests for data access or related documents can be directed to the corresponding author.
Acknowledgments
The authors express their gratitude to all participants for their contributions to this research. Appreciation is also extended to technicians at the Sleep Center of Taipei Medical University–Shuang Ho Hospital for their assistance in data collection.
Author Contributions
I-Jung Liu: conceptualization, methodology, data curation, formal analysis, writing-original draft.
Wen-Te Liu: data curation, conceptualization, methodology, validation, supervision, resources, project administration, investigation, writing – review & editing, writing – original draft.
Rachel Chien: data curation, formal analysis, methodology, project administration.
Ying-Ying Chen: data curation, formal analysis, writing – review and editing.
Yen-Ling Chen: data curation, project administration, writing – review and editing.
Yi-Chih Lin: project supervision, data curation, formal analysis.
Wayne Lai: project supervision, resources, conceptualization, methodology, writing – review & editing, funding acquisition.
Yi-Chun Kuan: project supervision, visualization, investigation, conceptualization, resources.
Kang-Yun Lee: conceptualization, validation, supervision.
Tzu-Tao Chen: validation, data curation, methodology.
Arnab Majumdar: visualization, conceptualization, supervision, writing – review & editing.
Jiunn-Horng Kang: conceptualization, methodology, funding acquisition, writing – review & editing, project administration, supervision.
Cheng-Yu Tsai: data curation, validation, funding acquisition, supervision, writing – original draft.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the National Science and Technology Council of Taiwan (grant nos.: NSTC 112-2634-F002-003 and NSTC 113-2222-E-038-003) and Taipei Medical University (grant no.: TMU A-114-049). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no potential conflicts of interest with respect to this research, authorship, and/or publication of this article.
References
1. Cao MT, Sternbach JM, Guilleminault C. Continuous positive airway pressure therapy in obstuctive sleep apnea: benefits and alternatives. Exp Rev Respiratory Med. 2017;11(4):259–15. doi:10.1080/17476348.2017.1305893
2. Loredo JS, Ancoli-Israel S, Kim E-J, et al. Effect of continuous positive airway pressure versus supplemental oxygen on sleep quality in obstructive sleep apnea: a Placebo-CPAP−Controlled Study. Sleep. 2006;29(4):564–571. doi:10.1093/sleep/29.4.564
3. Joskin A, Bruyneel M. Challenges in obstructive sleep apnea management in elderly patients. J Clin Med. 2024;13(24):7718. doi:10.3390/jcm13247718
4. Martinez-Garcia MA, Valero-Sánchez I, Reyes-Nuñez N, et al. Continuous positive airway pressure adherence declines with age in elderly obstructive sleep apnoea patients. ERJ Open Res. 2019;5(1):00178–2018. doi:10.1183/23120541.00178-2018
5. Dorkova Z, Petrasova D, Molcanyiova A, et al. Effects of continuous positive airway pressure on cardiovascular risk profile in patients with severe obstructive sleep apnea and metabolic syndrome. Chest. 2008;134(4):686–692. doi:10.1378/chest.08-0556
6. Lv M, Mao J, Wang S, et al. Effect of continuous positive airway pressure on cardiometabolic risk factors in patients with obstructive sleep apnea: a systematic review and meta-analysis. Respir Med. 2024;235:107852. doi:10.1016/j.rmed.2024.107852
7. Richards KC, Gooneratne N, Dicicco B, et al. CPAP adherence may slow 1-year cognitive decline in older adults with mild cognitive impairment and apnea. J Am Geriatr Soc. 2019;67(3):558–564. doi:10.1111/jgs.15758
8. Idalino SCC, Canever JB, Cândido LM, et al. Association between sleep problems and multimorbidity patterns in older adults. BMC Public Health. 2023;23(1):978. doi:10.1186/s12889-023-15965-5
9. Campos-Rodriguez F, Martinez-Garcia MA, Reyes-Nuñez N, et al. Long-term continuous positive airway pressure compliance in females with obstructive sleep apnoea. Eur Respir J. 2013;42(5):1255–1262. doi:10.1183/09031936.00165812
10. Berry RB, Chediak A, Brown LK, et al. Best clinical practices for the sleep center adjustment of noninvasive positive pressure ventilation (NPPV) in stable chronic alveolar hypoventilation syndromes. J Clin Sleep Med. 2010;6(5):491–509. doi:10.5664/jcsm.27941
11. Kushida CA, Chediak A, Berry RB, et al. Clinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apnea. J Clin Sleep Med. 2008;4(2):157–171. doi:10.5664/jcsm.27133
12. Nakazaki C, Noda A, Yasuda Y, et al. Continuous positive airway pressure intolerance associated with elevated nasal resistance is possible mechanism of complex sleep apnea syndrome. Sleep Breathing. 2012;16(3):747–752. doi:10.1007/s11325-011-0570-5
13. Hang L-W, Tsai YC, Finnsson E, et al. Sex-specific age-related worsening of pathological endotypic traits in patients with obstructive sleep apnea. Sleep. 2024;48(1):zsae185.
14. Weaver TE, Chasens ER. Continuous positive airway pressure treatment for sleep apnea in older adults. Sleep Med Rev. 2007;11(2):99–111. doi:10.1016/j.smrv.2006.08.001
15. Shin JH, Song MJ, Kim JH. Acute effect of positive airway pressure on heart rate variability in obstructive sleep apnea. J Clin Med. 2023;12(24):7606. doi:10.3390/jcm12247606
16. Sun Y, Lei F, Luo L, et al. Effects of a single night of continuous positive airway pressure on spontaneous brain activity in severe obstructive sleep apnea. Sci Rep. 2023;13(1):8950. doi:10.1038/s41598-023-36206-0
17. Mölle M, Born J. Chapter 7 - slow oscillations orchestrating fast oscillations and memory consolidation. In: Van Someren EJW, editor. Progress in Brain Research. Elsevier;2011:93–110.
18. Lee YF, Gerashchenko D, Timofeev I, et al. Slow wave sleep is a promising intervention target for alzheimer’s disease. Front Neurosci. 2020;14:705. doi:10.3389/fnins.2020.00705
19. Mander BA, Rao V, Lu B, et al. Prefrontal atrophy, disrupted NREM slow waves and impaired hippocampal-dependent memory in aging. Nat Neurosci. 2013;16(3):357–364. doi:10.1038/nn.3324
20. Reis MS, Sampaio LMM, Lacerda D, et al. Acute effects of different levels of continuous positive airway pressure on cardiac autonomic modulation in chronic heart failure and chronic obstructive pulmonary disease. Arch Med Sci. 2010;6(5):719–727. doi:10.5114/aoms.2010.17087
21. Dijk DJ. Slow-wave sleep, diabetes, and the sympathetic nervous system. Proc Natl Acad Sci U S A. 2008;105(4):1107–1108. doi:10.1073/pnas.0711635105
22. Grzęda-Hałon M, Poręba M, Gut G, et al. The effect of CPAP therapy on heart rate variability in patients with obstructive sleep apnea. Sleep Biol Rhythms. 2023;21(2):143–154. doi:10.1007/s41105-022-00424-2
23. Forte G, Favieri F, Casagrande M. Heart rate variability and cognitive function: a systematic review. Front Neurosci. 2019;13:710. doi:10.3389/fnins.2019.00710
24. Galin S, Keren H. The predictive potential of heart rate variability for depression. Neuroscience. 2024;546:88–103. doi:10.1016/j.neuroscience.2024.03.013
25. Pantoni CBF, Mendes RG, Di Thommazo L, et al. Acute application of bilevel positive airway pressure influences the cardiac autonomic nervous system. Clinics. 2009;64(11):1085–1092. doi:10.1590/S1807-59322009001100008
26. Spiesshoefer J, Becker S, Tuleta I, et al. Impact of simulated hyperventilation and periodic breathing on sympatho-vagal balance and hemodynamics in patients with and without heart failure. Respiration. 2019;98(6):482–494. doi:10.1159/000502155
27. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (version 2.4). Am Academy Sleep Med. 2017;13(5):665–666.
28. Kuan Y-C, Lin H-W, Yang -C-C, et al. Slow-wave sleep, oxygen desaturation, and memory consolidation in sleep-disturbed individuals. Int J Clin Health Psychol. 2025;25(2):100574. doi:10.1016/j.ijchp.2025.100574
29. Tsai C-Y, Su C-L, Huang H-T, et al. Mediating role of obstructive sleep apnea in altering slow-wave activity and elevating Alzheimer’s disease risk: pilot study from a northern Taiwan cohort. Sleep Health. 2025;11(1):80–90. doi:10.1016/j.sleh.2024.08.012
30. Zhang H, Zhu M, Zheng Y, et al. Toward capturing momentary changes of heart rate variability by a dynamic analysis method. PLoS One. 2015;10(7):e0133148. doi:10.1371/journal.pone.0133148
31. Kuo CF, Lin Y-C, Chen Z-Y, et al. From reactive to proactive: machine learning models for continuous positive airway pressure adjustments using heart rate variability and oximetry-related parameters. Digit Health. 2025;11:20552076251339273. doi:10.1177/20552076251339273
32. Caples SM, Rosen CL, Shen WK, et al. The scoring of cardiac events during sleep. J Clin Sleep Med. 2007;3(2):147–154. doi:10.5664/jcsm.26816
33. El-Helbawy RH, Kasemy ZA, Eid HA. Effect of obstructive sleep apnea syndrome on sleep architecture: comparative study between geriatrics and middle-aged adult patients. Egy J Chest Dis and Tuberculosis. 2023;72(4):559–564. doi:10.4103/ecdt.ecdt_1_23
34. Norman D, Loredo JS. Obstructive sleep apnea in older adults. Clin Geriatric Med. 2008;24(1):151–165. doi:10.1016/j.cger.2007.08.006
35. Randerath W, Baillieul S, Tamisier R. Central sleep apnoea: not just one phenotype. Eur Respir Rev. 2024;33(171):230141. doi:10.1183/16000617.0141-2023
36. McDaid C, Durée KH, Griffin SC, et al. A systematic review of continuous positive airway pressure for obstructive sleep apnoea–hypopnoea syndrome. Sleep Med Rev. 2009;13(6):427–436. doi:10.1016/j.smrv.2009.02.004
37. Giles TL, Lasserson TJ, Smith BH, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;2006(1). doi:10.1002/14651858.CD001106.pub3.
38. Edwards BA, Wellman A, Sands SA, et al. Obstructive sleep apnea in older adults is a distinctly different physiological phenotype. Sleep. 2014;37(7):1227–1236. doi:10.5665/sleep.3844
39. Hietakoste S, Armañac-Julián P, Karhu T, et al. Acute cardiorespiratory coupling impairment in worsening sleep apnea-related intermittent hypoxemia. IEEE Trans Biomed Eng. 2023;71(1):326–333. doi:10.1109/TBME.2023.3300079
40. Trinder J, Kleiman J, Carrington M, et al. Autonomic activity during human sleep as a function of time and sleep stage. J Sleep Res. 2001;10(4):253–264. doi:10.1046/j.1365-2869.2001.00263.x
41. Monahan KD. Effect of aging on baroreflex function in humans. Am J Physiol Regul Integr Comp Physiol. 2007;293(1):R3–R12. doi:10.1152/ajpregu.00031.2007
42. Li Y, Li Q, Zou X, et al. Effects of CPAP treatment on electroencephalographic activity in patients with obstructive sleep apnea syndrome during deep sleep: preliminary findings of a cross-sectional study. Chron Respir Dis. 2023;20:14799731231215094. doi:10.1177/14799731231215094
43. Dubé J, Lafortune M, Bedetti C, et al. Cortical thinning explains changes in sleep slow waves during adulthood. J Neurosci. 2015;35(20):7795. doi:10.1523/JNEUROSCI.3956-14.2015
44. Segù M, Cosi A, Santagostini A, et al. Efficacy of a trial oral appliance in OSAS management: a new protocol to recognize responder/nonresponder patients. Int J Dent. 2021;2021:8811700. doi:10.1155/2021/8811700
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.