Back to Journals » Vascular Health and Risk Management » Volume 19
Genetic Variants in PHACTR1 & LPL Mediate Restenosis Risk in Coronary Artery Patients
Authors Al Hageh C ![]() , Chacar S
, Chacar S ![]() , Venkatachalam T, Gauguier D, Abchee A, Chammas E, Hamdan H
, Venkatachalam T, Gauguier D, Abchee A, Chammas E, Hamdan H ![]() , O'Sullivan S, Zalloua P, Nader M
, O'Sullivan S, Zalloua P, Nader M ![]()
Received 27 October 2022
Accepted for publication 25 December 2022
Published 16 February 2023 Volume 2023:19 Pages 83—92
DOI https://doi.org/10.2147/VHRM.S394695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Cynthia Al Hageh,1,* Stephanie Chacar,2,* Thenmozhi Venkatachalam,2 Dominique Gauguier,3,4 Antoine Abchee,5 Elie Chammas,6 Hamdan Hamdan,2 Siobhan O’Sullivan,1 Pierre Zalloua,1,7,8 Moni Nader2,7
1Department of Molecular Biology and Genetics, College of Medicine and Health Sciences, Khalifa University for Science and Technology, Abu Dhabi, United Arab Emirates; 2Department of Physiology and Immunology College of Medicine and Health Sciences, Khalifa University of Science and Technology, Abu Dhabi, UAE; 3McGill University and Genome Quebec Innovation Centre, Montreal, QC, H3A 0G1, Canada; 4Université Paris Cité, INSERM, Paris, France; 5Sheikh Shakhbout Medical City, Abu Dhabi, United Arab Emirates; 6School of Medicine, Lebanese University, Beirut, Lebanon; 7Biotechnology Center, Khalifa University for Science and Technology, Abu Dhabi, United Arab Emirates; 8Harvard T.H. Chan School of Public Health, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Pierre Zalloua; Moni Nader, College of Medicine and Health Sciences, Khalifa University for Science and Technology, PO Box 127788, Abu Dhabi, United Arab Emirates, Email [email protected]; [email protected]
Background and Objective: Coronary artery disease (CAD) is a major cause of death worldwide. Revascularization via stent placement or coronary artery bypass grafting (CABG) are standard treatments for CAD. Despite a high success rate, these approaches are associated with long-term failure due to restenosis. Risk factors associated with restenosis were investigated using a case-control association study design.
Methods: Five thousand two hundred and forty-two patients were enrolled in this study and were assigned as follows: Stenosis Group: 3570 patients with CAD > 50% without a prior stent or CABG (1394 genotyped), and Restenosis Group: 1672 patients with CAD > 50% and prior stent deployment or CABG (705 genotyped). Binomial regression models were applied to investigate the association of restenosis with diabetes, hypertension, and dyslipidemia. The genetic association with restenosis was conducted using PLINK 1.9.
Results: Dyslipidemia is a major risk factor (Odds Ratio (OR) = 2.14, P-value < 0.0001) for restenosis particularly among men (OR = 2.32, P < 0.0001), while type 2 diabetes (T2D) was associated with an increased risk of restenosis in women (OR = 1.36, P = 0.01). The rs9349379 (PHACTR1) and rs264 (LPL) were associated with an increased risk of restenosis in our patients. PHACTR1 variant was associated with increased risk of restenosis mainly in women and in diabetic patients, while the LPL variant was associated with increased risk of restenosis in men.
Conclusion: The rs9349379 in PHACTR1 gene is significantly associated with restenosis, this association is more pronounced in women and in diabetic patients. The rs264 in LPL gene was associated with increased risk of restenosis in male patients.
Keywords: PHACTR1, LPL, diabetes, restenosis
Introduction
Coronary artery disease (CAD) is a leading cause of mortality worldwide. Revascularization via coronary stent placed by percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) is a common treatment option for patients with CAD.1 There are more than 1,000,000 PCI and 400,000 CABG procedures performed yearly to treat CAD.2,3 Coronary stent implantation is widely used and reduces the early complications associated with balloon angioplasty.4,5 In addition, CABG is used to improve prognosis in patients with severe artery stenosis.6,7 Although most PCI and CABG procedures are successful, these therapies are also associated with complications that affect their long-term efficacy. These often result in the repeated reduction in the diameter of the coronary artery with ≥50% luminal narrowing, also known as restenosis.4,8 Within the span of ten years after CABG, a repeat revascularization is needed in approximately 13% of patients.9 In CABG, the coronary artery bypass is performed using an extract of the saphenous vein of the patient with stenosed coronary arteries. The restenosis rate for saphenous vein grafts (SVG), the most common graft, is projected to be close to 2% every year.1 While stents via either PCI or CABG remain the gold standard procedure to treat CAD, their long-term failure due to restenosis calls for deeper investigations to improve the outcome of these procedures.
Restenosis of the coronary arteries profoundly hinders the quality of life and is associated with increased health-care costs.10 Despite the tremendous advances in the field, understanding the etiology of restenosis is incomplete. There are several risk factors for stenosis including: age,11 dyslipidemia,12 hypertension,13 and history of restenosis14 and these have been also frequently reported as clinical risk factors for restenosis. Of interest, diabetes mellitus15 is one of the main risk factor for coronary artery restenosis considering its implications in a myriad of vasculopathies due to hyperglycemia-induced damaged endothelial function. Although the involvement of smooth muscle proliferation in restenosis remains a debatable matter, vascular smooth muscle cells (VSMCs) proliferation in patients with diabetes remains a main cause of restenosis.16 Further, hyperglycemia leads to endothelial dysfunction and increases the production of cytokines and growth factors, resulting in extensive neointima formation or thickening and subsequently restenosis.17 This is particularly observed in hypertensive patients. Hypertension has also been categorized amongst the risk factors of restenosis.13
The clinical incidence of in-stent restenosis (ISR) ranges from 20% to 35% narrowing after the placement of bare-metal stent (BMS).4 Inflammation and vascular remodeling are biological risk factors associated with coronary restenosis.18 These phenomena constitute the major limitations associated with angioplasty and stenting techniques, thus leading to restenosis.19,20 In general, restenosis occurs in response to the inflammatory process that takes place within the first 30 min after the deployment of the coronary artery stent at the site of occlusion which causes inflammatory and reparative processes. Restenosis results from the VSMCs and fibroblasts being exposed to circulating growth factors by the damaged endothelium, which promotes their uncontrolled proliferation.4 The mechanical damage brought on by the stent implant, the hypersensitivity reaction to stent material, the thrombogenicity of the stents and their ability to cause platelets adherence and inflammation, together with the neoatherosclerosis in the neointima, all induce ISR.8
Various allelic variants have been linked to a higher risk of ISR in the literature21 and, more importantly, population-targeted screening for SNPs is imperative to fill the gap associated in the demographic heterogeneity of these genetic variations and their putative associations.22–25 Vargas-Alarcón et al demonstrated that the CASP1 gene polymorphisms were associated with restenosis in Mexican mestizo patients.22 Further, Zholdybayeva et al demonstrated that genetic variants in FGB, CD14 and NOS3 genes were associated with restenosis in Kazakh population.24
Current knowledge about genetic predisposition to post-stent and post-CABG stenosis is still lacking in many populations. In this study, we investigated various risk factors for restenosis in a large group of CAD patients and control subjects in a Lebanese population. We further focused on the genetic basis of this pathology by investigating the association of previously identified 44 CAD susceptibility alleles with restenosis using a nested case-control study design.
Methodology
Study Population
The study was designed as a multi-center, nested case-control study for evaluating the risk factors of restenosis. All patients were recruited over the period of two years from three tertiary care hospitals in Lebanon between August 2007-June 2009.26 All patients underwent coronary catheterization by Judkins technique. The study procedure was approved by the International Review Board (IRB) at the Lebanese American University, and all participants provided written informed consent after they were given a description of the study. After consenting, subjects completed a questionnaire on their medical history, assisted by trained health workers. All protocols were performed according to the Helsinki Declaration of 1975.
Based on the coronary artery disease category, stent implantation and coronary artery bypass graft (CABG) surgery, the patients (5242 subjects) were categorized into two groups: Stenosis Group, where 3570 patients with CAD (>50% obstruction in any of the coronary arteries visualized) and without prior history of stent deployment or CABG; and Restenosis Group, where 1672 patients with CAD (>50% obstruction visualized in any of the coronary arteries visualized) and with prior history of stent deployment or CABG.
Data Collection and Clinical Assessment
Demographic and baseline clinical data for the participants were collected or were determined from patients’ charts at the time of enrolment. These data included: socio-demographic characteristics (sex, age, age of CAD onset, nationality, place of residence), clinical characteristics (T2D, cardiovascular disease, dyslipidemia, and hypertension), and anthropometric measurements: height (cm), weight (Kg) and BMI (kg/m2). In addition, patients’ smoking history and medication use were retrieved from the patient’s chart.
Patients were considered to have hypertension if they were taking antihypertensive drugs or had been so identified by their physician in their medical chart. Patients were considered diabetic if they were taking medication to reduce their blood sugar or if their physician had identified them as so in their medical chart. Patients were considered to have dyslipidemia if their physician diagnosed it in their medical chart or if they were given medication to treat dyslipidemia.
Furthermore, 20 mL of blood was collected during the angiography procedure by a health-care professional. Plasma and serum were separated and stored at −80°C until they were used for biochemistry analysis: fasting blood sugar (FBS), total cholesterol (mg/dL), triglycerides (mg/dL), high-density lipoprotein (HDL, mg/dL), low-density lipoprotein (LDL, mg/dL). Genomic DNA was extracted from the remaining blood samples using a standard phenol extraction method and subsequently used for genotyping.
Genotyping
DNA was extracted using the whole blood sample collected and subjected to genotyping using Illumina Human610-Quad BeadChip (Illumina, San Diego, CA, USA) and Illumina Human660W-Quad BeadChip (Illumina, San Diego, CA, USA), as described by Hager et al 2012.27 Among the study population, 1394 patients from Stenosis Group, and 705 patients from Stenosis Group had genotyped data available and were included in the genetic association using PLINK.28 Using PLINK, quality control (QC) was applied, and variants were filtered out. Sex checks were performed using PLINK and variants were excluded for having >5% missing genotyping rates and <1% MAF (minor allele frequency), and for failing HWE (Hardy-Weinberg Equilibrium) test (P > 0.05).
Statistical Analysis
All statistical analyses were processed by the R package (R version 4.1.2). Categorical variables were displayed as counts and percentages. Normally distributed continuous data were presented as mean ± standard deviation (SD). In the univariate analysis, continuous data were analyzed by one-way ANOVA while the categorical data were compared using the χ2 test. Differences with P-value <0.05 were considered statistically significant. Binomial logistic regression was applied to test the association between restenosis and the risk factors such as T2D, hypertension, dyslipidemia and low HDL (defined as HDL < 40 mg/dl, HDL < 40 in men and HDL < 50 in women29) after adjusting for age. In addition, the association of individual SNPs with the risk factors was tested in women and in men.
Association analyses with restenosis of 44 SNPs previously associated with CAD or T2D were performed using PLINK 1.9 (www.cog-genomics.org/plink/1.9/) in R language. These SNPs were specifically selected for this nested case-control study to investigate their association with restenosis. Odds ratios (OR) were adjusted for age and/or sex and were reported, OR greater than 1 implies that the mutant allele is associated with increased risk of restenosis. Allele frequencies among Restenosis and Stenosis Groups were reported. In addition, associations between the SNPs and restenosis were assessed among men and women. The Hardy-Weinberg Equilibrium (HWE) was tested using the χ2 test, the distribution of alleles was considered in agreement with HWE when P-value is more than 0.05.
Results
Impact of CAD Risk Factors on Restenosis
A total of 1672 restenosis patients (1296 men and 376 women) and 3570 stenosis patients (2559 men and 1010 women) were included in this study. The mean age in patients of Restenosis Group was 63.862 years (±10.326) while that of patients in Stenosis Group was 62.455 (±11.153) years (Table 1). LDL, HDL, and total cholesterol levels were found to be significantly lower (P-value <0.05) in Restenosis Group. Higher prevalence of T2D (38.3%), dyslipidemia (64.9%) and hypertension (69.7%) were observed in Restenosis Group (Table 1).
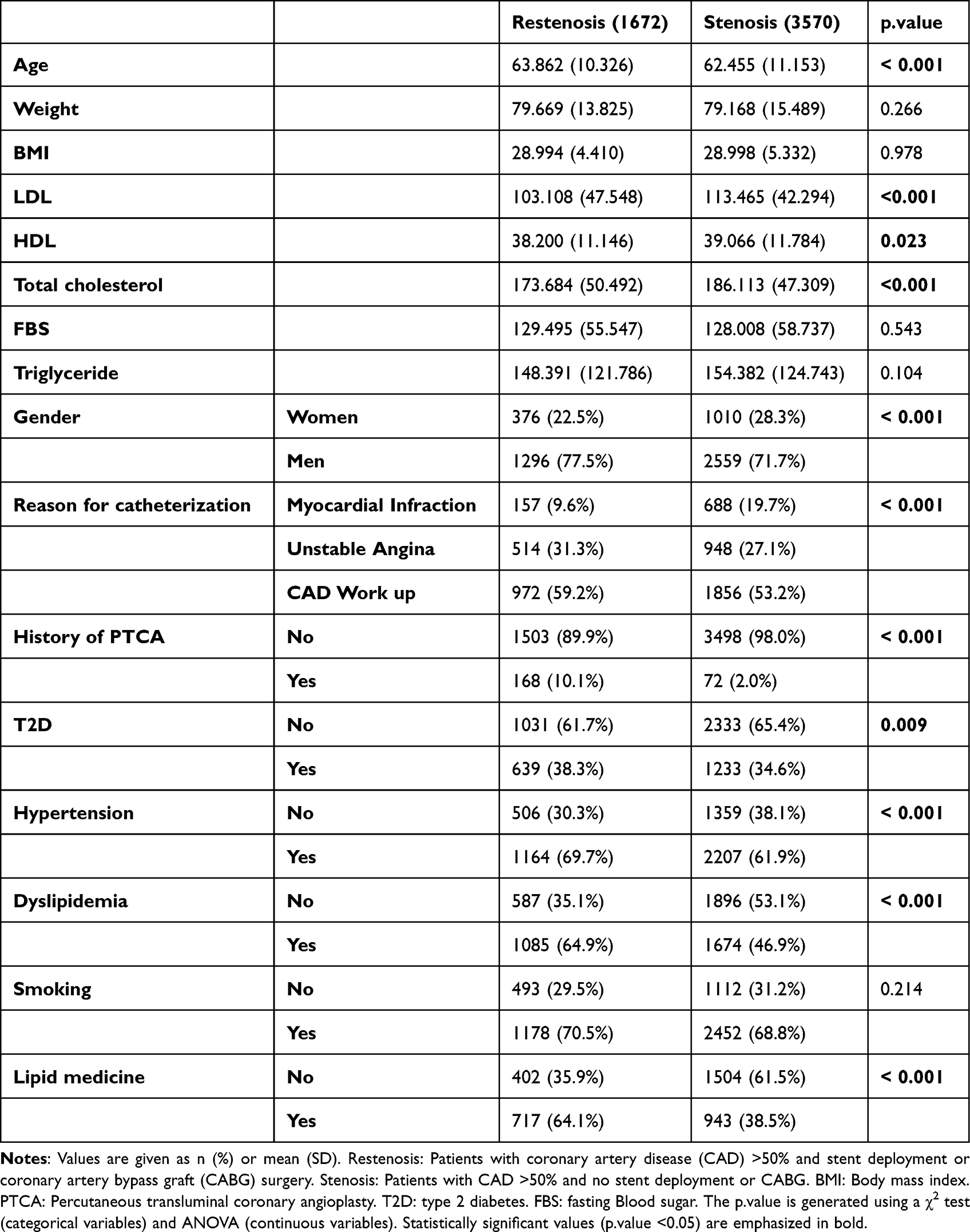 |
Table 1 Demographic, Clinical Characteristics of the 5242 Subjects Segregated Between Restenosis and Stenosis Patients of the Study Population |
Restenosis male patients (Table 2) were younger (63.016±10.319 years) when compared to women (66.784±9.819 years). In women, higher prevalence of T2D, hypertension and dyslipidemia among restenosis patients was observed when compared with men (46.5% vs 35.9%, 83.5% vs 65.7% and 69.1 vs. 63.7%, respectively). The mean value of LDL cholesterol in men with restenosis was 103.411±45.995 mg/dL and that of men with stenosis was 113.419±42.355 (P < 0.001). The mean value of LDL in women with restenosis was 101.985±52.971 while in women with stenosis was 113.619±42.173. Total cholesterol was significantly lower in men and women with restenosis when compared to men and women with stenosis (P < 0.001).
 |
Table 2 Clinical Presentation of Restenosis and Stenosis Patients of the Study Population Stratified by Gender |
Results of the regression analysis showed that, after adjustment for age, restenosis was positively associated with dyslipidemia (OR = 2.14, P < 0.0001), and hypertension (OR = 1.36, P < 0.0001), low HDL (OR = 1.2, P = 0.01) and T2D (OR = 1.16, P = 0.01) (Figure 1). Dyslipidemia was the strongest risk factor. The association between dyslipidemia and restenosis was stronger in men with an OR = 2.32 (P < 0.0001) when compared with all patients (OR = 2.14) and with women (OR = 1.95). T2D was significantly associated with an increased risk of restenosis in women (OR = 1.36, P = 0.01) but not in men (P > 0.05). In addition, no significant association between low HDL and restenosis was found when analyzed separately in men and women. Among restenosis patients, women patients with T2D were younger (P = 0.029), had higher levels of FBS (P < 0.001) and triglyceride (P < 0.001), while lower levels of HDL (P < 0.001) than non-diabetic women (Supplementary Table 1). In addition, among restenosis patients, hyperlipidemic men (Supplementary Table 2) were significantly younger (P < 0.001) and had higher BMI (P = 0.002) and triglyceride (P < 0.001) levels than non-hyperlipidemic men.
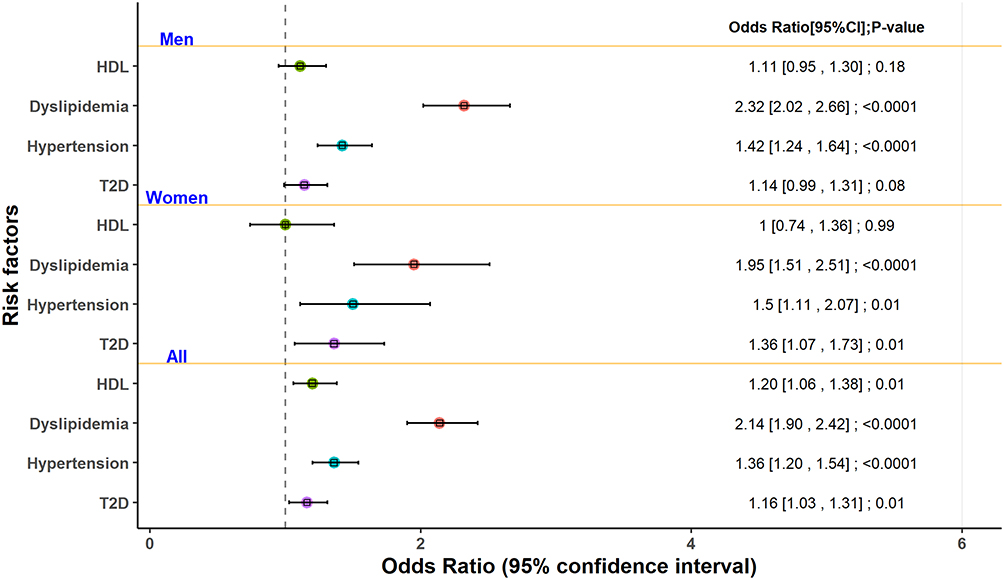 |
Figure 1 Forest plot of the logistic regression with restenosis as an outcome and different risk factors as predictor variables stratified by gender. Restenosis: patients with CAD >50% obstruction and history of percutaneous stent deployment. Odds ratios are adjusted for age. HDL (defined as HDL < 40 mg/dl, HDL < 40 in men and HDL < 50 in women). Abbreviations: CI, Confidence Interval; T2D, Type 2 diabetes. |
Allelic Association of the SNPs with CAD Restenosis in the Study Cohort
All significantly associated SNPs were found to be in HWE (P > 0.05). The allelic frequencies of the 44 tested SNPs are shown in Supplementary Table 3. Two SNPs (rs9349379*G and rs264*A) were found to be significantly associated with restenosis after adjustment for age and sex. These SNPs reside in two different genes namely, PHACTR1, and LPL (Figure 2).
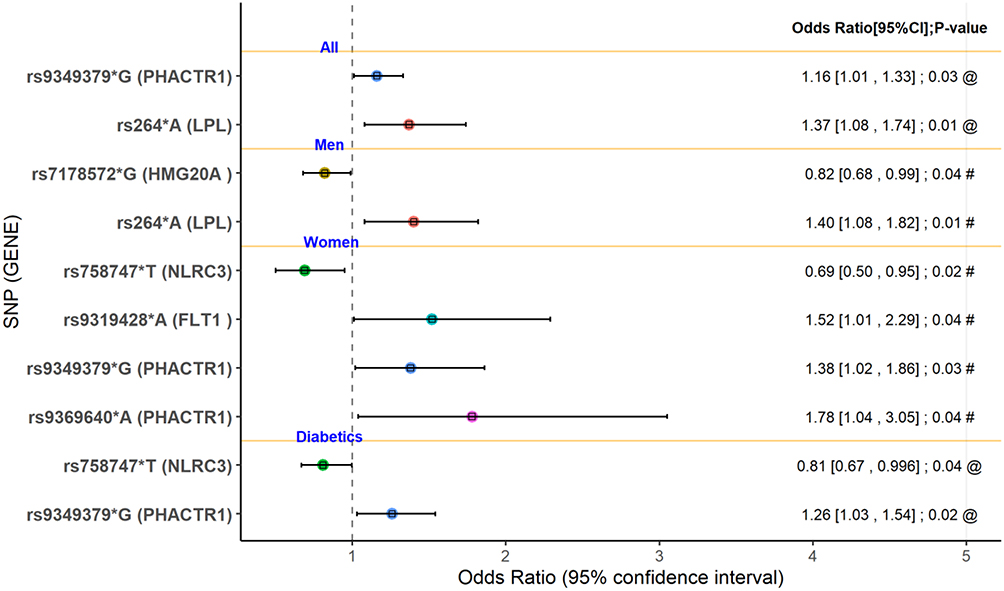 |
Figure 2 Forest plot of the logistic regression with restenosis as an outcome and SNPs that have been associated with CAD and T2D as predictor variables according to gender and diabetes. Restenosis: patients with CAD >50% obstruction and history of percutaneous stent deployment. @: adjusted for age and sex. #: adjusted for age. Abbreviations: CI, Confidence Interval; SNPs, single nucleotide polymorphisms; HMG20A, high mobility group 20A. LPL; lipoprotein lipase. NLRC3, NLR family CARD domain containing 3. FLT1; fms related receptor tyrosine kinase 1; PHACTR1, phosphatase and actin regulator 1. |
The derived allele frequency of rs9349379 A>G was 43% in restenosis patients compared to 40% in stenosis patients (Supplementary Table 3). This variant was significantly and positively associated with restenosis with an OR = 1.16 (P = 0.03) (Figure 2 and Supplementary Table 3). This variant was more frequent among diabetic patients with restenosis with an allele frequency of 45% than among diabetic patients with stenosis 40% (OR = 1.26, P = 0.02) (Supplementary Table 3). In addition, the association between rs9349379*G and restenosis was stronger among women (OR = 1.38, P = 0.03) when compared with all patients with an allele frequency of 51% in women with restenosis and 43% in women with stenosis (Supplementary Table 3). In addition to rs9349379*G, rs9369640 (C>A) which is also located in PHACTR1 was found to be associated with increased risk of restenosis in women (OR = 1.78, P = 0.04). rs9319428 (G>A) located in FLT1 was associated with an increased risk of restenosis in women (OR = 1.52, P = 0.04) and rs758747 (C>T) located in NLRC3 was associated with a reduced risk of restenosis in women (OR = 0.69, P = 0.02). This last SNP was also found associated with a reduced risk of restenosis among diabetic patients (OR = 0.81, P = 0.04).
The rs264 G>A was associated with an increased risk of restenosis (OR = 1.37, P = 0.01) (Figure 2) and in particular among men (OR = 1.40, P = 0.01). The derived allele frequency of rs264 G>A was 15% in the Restenosis Group compared to 11% in Stenosis Group. The allele frequencies for both groups were also similar in men (Supplementary Table 3). Despite having similar allele frequencies among diabetics, this allele was not associated with restenosis in diabetic patients. In addition, this derived allele was not significantly associated with restenosis among women. In addition to LPL, we found rs7178572 (A>G) located in HMG20A to be negatively associated with restenosis in men (OR = 0.82, P = 0.04) (Figure 2).
Discussion
We report a significant association between restenosis and dyslipidemia, hypertension, and T2D in a Lebanese population of CAD patients, with T2D being significantly more pronounced in women. We also show that the genetic loci rs9349379 (PHACTR1) in women and in diabetic patients and rs264 (LPL) in men are significantly associated with restenosis in our study population.
Our results showing that dyslipidemia is a risk factor for restenosis are in line with other reports indicating that this risk is particularly increased in men.12 High levels of oxidized LDL in the intima trigger the release of mitogens from platelets, macrophages, and endothelial cells. This process stimulates smooth muscle cell migration and proliferation which subsequently results in neointima formation.30 Patients with low rates of normal systolic/diastolic blood pressure exhibited higher restenosis than controls.31,32 The restenosis in hypertensive patients may be due to combinatory effects of the injured endothelium along with inflammation that promote plaque formation and narrowing of blood vessels.33–35
Similarly, diabetes has been demonstrated to contribute to CAD and to restenosis.36 In this study, we found that T2D was strongly associated with restenosis in women. This observation is in line with a previous study by Trabattoni et al reporting that diabetic women were more susceptible for restenosis after coronary stent implantation.37 A greater degree of neointimal hyperplasia promoting the development of restenosis with the inflammatory response is associated with hyperglycemia.18 Further, the small vessel diameter in women constitutes a risk factor for angiographic restenosis.37 Together, these factors underscore the pronounced restenosis risk in diabetic women. In addition, it has been reported that a reduced plasma level of adiponectin, the adipocyte-derived hormone, triggers neointimal thickening in diabetic patients and can lead to restenosis.38,39 In normal conditions, adiponectin exerts cardiovascular protective effects and the levels of this protein are higher among women compared to men.40 However, decreased plasma levels of adiponectin have been reported in patients with T2D, and particularly in CAD subjects.38 This argument could also explain the increased risk for restenosis in diabetic women. Further investigation is warranted to confirm the role of adiponectin in restenosis especially in women.
Our genetic investigation showed that two polymorphisms rs9349379*G (PHACTR1) in women and in diabetic patients and rs264*A (LPL) in men were found to be significantly and positively associated with restenosis. The rs9349379 A>G is located in PHACTR1 on chromosome 6 and encodes phosphatase and actin regulator protein 1. PHACTR1 has been linked to endothelial dysfunction, vascular calcification, apoptosis, and angiogenesis.41–44 It has been shown that disruption of the PHACTR1 pathway induces the production of pro-inflammatory and pro-atherogenic biomarkers41 and mediates endothelial inflammation and dysfunction.45 Thus, when associated with diabetes and small vessel diameter, often the case in women, mutations in the PHACTR1 gene are likely to exacerbate inflammation, endothelial dysfunction, and atherosclerosis. The rs264 G>A polymorphism was also found to be associated with restenosis. The rs264 is located at the lipoprotein lipase (LPL) gene on chromosome 8, which encodes lipoprotein lipase. LPL plays an important role in lipid metabolism as it facilitates intravascular lipolysis of triglycerides in lipoprotein.46 Thus, it has been shown to possess antiatherogenic activity.47 The LPL knockout mice exhibit dyslipidemia, reduced HDL clearance and neonatal death.48 Therefore, mutation of LPL gene may result in a defective LPL enzyme which could impair normal lipid metabolism. This causes blood lipid accumulation and increases the risk of lipid deposition in intima, with subsequent neointimal formation as well as restenosis.
In addition to these two genes, a polymorphism in FLT1 (rs9319428*A), encoding a member of vascular endothelial growth factor (VEGF) receptor family, was associated with an increased risk of restenosis in women. FLT1 deficient mice exhibit impaired neovascularization49 and inhibition of FLT1 reduces inflammation and neointimal formation in hypercholesterolemic mice.50 This implication in atherosclerosis could partially explain our findings. Additional work is needed to determine whether the FLT1 polymorphism amplifies or attenuates the role of FLT1 in vascular injury remains.
The following two SNPs, rs7178572 (HMG20A), and rs758747 (NLRC3) were found to be negatively associated with restenosis in our study patients. The HMG20A polymorphism was previously found to be associated with increased risk of T2D.51 The HMG20A gene encodes high mobility group protein 20A. Recently, a role for HMG20A in adipogenesis was established. HMG20A silencing promoted adipogenic differentiation of porcine myogenic stromal vascular fraction (SVF) cells and C3H10T1/2 cells and thus it negatively regulates adipogenesis, hence not likely to promote diabetes.52 Yet, the pathophysiological consequence of the rs7178572 SNP associated with adipogenesis is still unknown. The SNP rs758747 (C>T) located in NLR family CARD domain containing 3 (NLRC3) gene was also found to be negatively associated with restenosis in diabetic women. Several studies revealed an association between obesity and the rs758747 T allele.53 Furthermore, NLRC3 deficiency promotes cutaneous wound healing due to the inhibition of p53 signaling.54 As p53 is also involved in vascular remodeling and atherosclerosis,55 thus we speculate that NLRC3 alteration could have reversed the expression and phosphorylation of p53 that is usually observed in advanced atherosclerotic plaques56 and therefore reduced restenosis susceptibility. Further studies are needed to explore this relationship.
Female patients who had prior stents and who have elevated FBS tend to require recurrent stent deployment at a significantly younger age than women with low FBS, and this is further increased in the presence PHACTR1 polymorphisms. For men who had prior stents and who have higher lipid levels, they tend to require recurrent stent deployment and this risk increases in the presence LPL polymorphisms. These findings highlight the importance of targeted and personalized management of restenosis and can be used to tailor patient’s management based on genetic and other metabolic determinants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Agrawal H, Teleb M, Lahsaei S, Carbajal L, Montanez R, Carrozza JP. Routine angiographic follow-up after coronary artery disease revascularization: is seeing believing? Curr Cardiol Rep. 2018;20(3):17. doi:10.1007/s11886-018-0957-z
2. Bachar BJ, Manna B. Coronary Artery Bypass Graft. Treasure Island (FL): StatPearls Publishing; 2022.
3. Smith SC, Dove JT, Jacobs AK, et al. ACC/AHA Guidelines for Percutaneous Coronary Intervention (Revision of the 1993 PTCA Guidelines)—Executive Summary. Circulation. 2001;103(24):3019–3041. doi:10.1161/01.CIR.103.24.3019
4. Pleva L, Kukla P, Hlinomaz O. Treatment of coronary in-stent restenosis: a systematic review. J Geriatr Cardiol. 2018;15(2):173–184. doi:10.11909/j.issn.1671-5411.2018.02.007
5. Kim MS, Dean LS. In-Stent Restenosis. Cardiovasc Ther. 2011;29(3):190–198. doi:10.1111/j.1755-5922.2010.00155.x
6. Beerkens FJ, Claessen BE, Mahan M, et al. Contemporary coronary artery bypass graft surgery and subsequent percutaneous revascularization. Nat Rev Cardiol. 2022;19(3):195–208. doi:10.1038/s41569-021-00612-6
7. Alexander JH, Smith PK. Coronary-artery bypass grafting. N Engl J Med. 2016;374(20):1954–1964. doi:10.1056/NEJMra1406944
8. Gori T. Restenosis after coronary stent implantation: cellular mechanisms and potential of endothelial progenitor cells (a short guide for the interventional cardiologist). Cells. 2022;11(13):2094. doi:10.3390/cells11132094
9. Xenogiannis I, Zenati M, Bhatt DL, et al. Saphenous vein graft failure: from pathophysiology to prevention and treatment strategies. Circulation. 2021;144(9):728–745. doi:10.1161/CIRCULATIONAHA.120.052163
10. Douglas JS, Holmes DR, Kereiakes DJ, et al. Coronary stent restenosis in patients treated with cilostazol. Circulation. 2005;112(18):2826–2832. doi:10.1161/CIRCULATIONAHA.104.530097
11. Weintraub WS, Kosinski AS, Brown CL 3rd, King SB 3rd:. Can restenosis after coronary angioplasty be predicted from clinical variables? J Am Coll Cardiol. 1993;21(1):6–14. doi:10.1016/0735-1097(93)90711-9
12. Vertes M, Nguyen DT, Szekely G, Berczi Á, Dosa E. Middle and Distal Common Carotid Artery Stenting: long-Term Patency Rates and Risk Factors for In-Stent Restenosis. Cardiovasc Intervent Radiol. 2020;43(8):1134–1142. doi:10.1007/s00270-020-02522-5
13. Agema WR, et al. Current PTCA practice and clinical outcomes in The Netherlands: the real world in the pre-drug-eluting stent era. Eur Heart J. 2004;25(13):1163–1170. doi:10.1016/j.ehj.2004.05.006
14. Kastrati A, Schomig A, Elezi S, Schuuhlen H, Wilhelm M, Dirschinger J. Interlesion Dependence of the Risk for Restenosis in Patients With Coronary Stent Placement in Multiple Lesions. Circulation. 1998;97(24):2396–2401. doi:10.1161/01.cir.97.24.2396
15. Gilbert J, Raboud J, Zinman B. Meta-analysis of the effect of diabetes on restenosis rates among patients receiving coronary angioplasty stenting. Diabetes Care. 2004;27(4):990–994. doi:10.2337/diacare.27.4.990
16. Smith SA, Newby N, Bond B. Ending Restenosis: inhibition of Vascular Smooth Muscle Cell Proliferation by cAMP. Cells. 2019;8(11):11. doi:10.3390/cells8111447
17. Jukema JW, Verschuren JJW, Ahmed TAN, Quax PHA. Restenosis after PCI. Part 1: pathophysiology and risk factors. Nat Rev Cardiol. 2012;9(1):53–62. doi:10.1038/nrcardio.2011.132
18. Kornowski R, Hong MK, Tio FO, Bramwell O, Wu H, Leon MB. In-stent restenosis: contributions of inflammatory responses and arterial injury to neointimal hyperplasia. J Am Coll Cardiol. 1998;31(1):224–230. doi:10.1016/s0735-1097(97)00450-6
19. Dangas G, Kuepper F. Cardiology patient page. Restenosis: repeat narrowing of a coronary artery: prevention and treatment. Circulation. 2002;105(22):2586–2587. doi:10.1161/01.cir.0000019122.00032.df
20. Xu X, Liu X, Yu L, Ma J, Yu S, Ni M. Impact of intracoronary nicorandil before stent deployment in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Exp Ther Med. 2020;19(1):137–146. doi:10.3892/etm.2019.8219
21. Verschuren JJW, Trompet S, Postmus I, et al. Systematic testing of literature reported genetic variation associated with coronary restenosis: results of the GENDER Study. PLoS One. 2012;7(8):e42401. doi:10.1371/journal.pone.0042401
22. Vargas-Alarcón G, Ramírez-Bello J, Peña-Duque MA, Martínez-Ríos MA, Delgadillo-Rodríguez H, Fragoso JM. CASP1 Gene Polymorphisms and BAT1-NFKBIL-LTA-CASP1 Gene–Gene Interactions Are Associated with Restenosis after Coronary Stenting. Biomolecules. 2022;12(6):765. doi:10.3390/biom12060765
23. Liu Y-W, Huang M-S, Hsu L-W, et al. Genetic risk model for in-stent restenosis of second-and third-generation drug-eluting stents. iScience. 2021;24(9):103082. doi:10.1016/j.isci.2021.103082
24. Zholdybayeva EV, Talzhanov YA, Aitkulova AM, et al. Genetic risk factors for restenosis after percutaneous coronary intervention in Kazakh population. Hum Genomics. 2016;10(1):15. doi:10.1186/s40246-016-0077-z
25. Verschuren JJW, Trompet S, Sampietro ML, et al. Pathway analysis using genome-wide association study data for coronary restenosis – a potential role for the PARVB gene. PLoS One. 2013;8(8):e70676. doi:10.1371/journal.pone.0070676
26. Youhanna S, Platt DE, Rebeiz A, et al. Parental consanguinity and family history of coronary artery disease strongly predict early stenosis. Atherosclerosis. 2010;212(2):559–563. doi:10.1016/j.atherosclerosis.2010.07.013
27. Hager J, Kamatani Y, Cazier J-B, et al. Genome-wide association study in a Lebanese cohort confirms PHACTR1 as a major determinant of coronary artery stenosis. PLoS One. 2012;7(6):e38663. doi:10.1371/journal.pone.0038663
28. Wakim V, Abi Khalil E, Salloum AK, Khazen G, Ghassibe-Sabbagh M, Zalloua PA. New susceptibility alleles associated with severe coronary artery stenosis in the Lebanese population. BMC Med Genomics. 2021;14(1):90. doi:10.1186/s12920-021-00942-x
29. Rader DJ, deGoma EM. Approach to the Patient with Extremely Low HDL-Cholesterol. J Clin Endocrinol Metab. 2012;97(10):3399–3407. doi:10.1210/jc.2012-2185
30. Mertens A, Holvoet P. Oxidized LDL and HDL: antagonists in atherothrombosis. FASEB J. 2001;15(12):2073–2084. doi:10.1096/fj.01-0273rev
31. Tocci G, Barbato E, Coluccia R, et al. Blood pressure levels at the time of percutaneous coronary revascularization and risk of coronary in-stent restenosis. Am J Hypertens. 2016;29(4):509–518. doi:10.1093/ajh/hpv131
32. Tocci G, Modestino A, Coluccia R, et al. Coronary intrastent restenosis and blood pressure levels: retrospective analysis of a large cohort of patients with coronary single vessel disease: 1c.06. J Hypertens. 2010;28:e8. doi:10.1097/01.hjh.0000378255.81414.b5
33. Brandes RP. Endothelial dysfunction and hypertension. Hypertension. 2014;64(5):924–928. doi:10.1161/HYPERTENSIONAHA.114.03575
34. Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation. 2001;104(3):365–372. doi:10.1161/01.CIR.104.3.365
35. Ross R, Epstein FH. Atherosclerosis — an inflammatory disease. N Eng J Med. 1999;340(2):115–126. doi:10.1056/nejm199901143400207
36. Lexis CPH, Rahel BM, Meeder JG, Zijlstra F, van derHorst IC. van der Horst ICC: the role of glucose lowering agents on restenosis after percutaneous coronary intervention in patients with diabetes mellitus. Cardiovasc Diabetol. 2009;8(1):41. doi:10.1186/1475-2840-8-41
37. Trabattoni D, Fabbiocchi F, Montorsi P, et al. Angiographic patterns of in-stent restenosis in men and women. Ital Heart J. 2005;6(2):138–142.
38. Hotta K, Funahashi T, Arita Y, et al. Plasma concentrations of a novel, adipose-specific protein, adiponectin, in type 2 diabetic patients. Arterioscler Thromb Vasc Biol. 2000;20(6):1595–1599. doi:10.1161/01.atv.20.6.1595
39. Li TD, Zeng ZH. Adiponectin as a potential therapeutic target for the treatment of restenosis. Biomed Pharmacother. 2018;101:798–804. doi:10.1016/j.biopha.2018.03.003
40. Diez JJ, Iglesias P. The role of the novel adipocyte-derived hormone adiponectin in human disease. Eur J Endocrinol. 2003;148(3):293–300. doi:10.1530/eje.0.1480293
41. Jarray R, Pavoni S, Borriello L, et al. Disruption of phactr-1 pathway triggers pro-inflammatory and pro-atherogenic factors: new insights in atherosclerosis development. Biochimie. 2015;118:151–161. doi:10.1016/j.biochi.2015.09.008
42. Aherrahrou R, Aherrahrou Z, Schunkert H, Erdmann J. Coronary artery disease associated gene Phactr1 modulates severity of vascular calcification in vitro. Biochem Biophys Res Commun. 2017;491(2):396–402. doi:10.1016/j.bbrc.2017.07.090
43. Jarray R, Allain B, Borriello L, et al. Depletion of the novel protein PHACTR-1 from human endothelial cells abolishes tube formation and induces cell death receptor apoptosis. Biochimie. 2011;93(10):1668–1675. doi:10.1016/j.biochi.2011.07.010
44. Allain B, Jarray R, Borriello L, Leforban B, Dufour S. Neuropilin-1 regulates a new VEGF-induced gene, Phactr-1, which controls tubulogenesis and modulates lamellipodial dynamics in human endothelial cells. Cell Signal. 2012;24(1):214–223. doi:10.1016/j.cellsig.2011.09.003
45. Ma X, Su M, He Q, et al. PHACTR1, a coronary artery disease risk gene, mediates endothelial dysfunction. Front Immunol. 2022;13:958677. doi:10.3389/fimmu.2022.958677
46. Liu C, Li L, Guo D, et al. Lipoprotein lipase transporter GPIHBP1 and triglyceride-rich lipoprotein metabolism. Clinica Chimica Acta. 2018;487:33–40. doi:10.1016/j.cca.2018.09.020
47. Shimada M, Ishibashi S, Inaba T, et al. Suppression of diet-induced atherosclerosis in low density lipoprotein receptor knockout mice overexpressing lipoprotein lipase. Proc Natl Acad Sci U S A. 1996;93(14):7242–7246. doi:10.1073/pnas.93.14.7242
48. Weinstock PH, Bisgaier CL, Aalto-Setälä K, et al. Severe hypertriglyceridemia, reduced high density lipoprotein, and neonatal death in lipoprotein lipase knockout mice. Mild hypertriglyceridemia with impaired very low density lipoprotein clearance in heterozygotes. J Clin Invest. 1995;96(6):2555–2568. doi:10.1172/jci118319
49. Thirunavukkarasu M, Juhasz B, Zhan L, et al. VEGFR1 (Flt-1±) gene knockout leads to the disruption of VEGF-mediated signaling through the nitric oxide/heme oxygenase pathway in ischemic preconditioned myocardium. Free Radic Biol Med. 2007;42(10):1487–1495. doi:10.1016/j.freeradbiomed.2007.02.011
50. Zhao Q, Egashira K. Essential role of vascular endothelial growth factor and Flt-1 signals in neointimal formation after periadventitial injury. Arterioscler Thromb Vasc Biol. 2004;24(12):2284–2289. doi:10.1161/01.ATV.0000147161.42956.80
51. Huang T, Wang L, Bai M, et al. Influence of IGF2BP2, HMG20A, and HNF1B genetic polymorphisms on the susceptibility to Type 2 diabetes mellitus in Chinese Han population. Biosci Rep. 2020;40(5). doi:10.1042/BSR20193955
52. Li R, Meng S, Ji M, et al. HMG20A inhibit adipogenesis by transcriptional and epigenetic regulation of MEF2C expression. Int J Mol Sci. 2022;23(18). doi:10.3390/ijms231810559
53. Mikhailova SV, Ivanoshchuk DE. Innate-immunity genes in obesity. J Pers Med. 2021;11(11). doi:10.3390/jpm11111201
54. Qin Y, Wu K, Zhang Z, et al. NLRC3 deficiency promotes cutaneous wound healing due to the inhibition of p53 signaling. Biochim Biophys Acta Mol Basis Dis. 2022;1868(11):166518. doi:10.1016/j.bbadis.2022.166518
55. Chan GH, Chan E, Kwok CT, Leung GP, Lee SM, Seto SW. The role of p53 in the alternation of vascular functions. Front Pharmacol. 2022;13:981152. doi:10.3389/fphar.2022.981152
56. Gorgoulis VG, Pratsinis H, Zacharatos P, et al. p53-dependent ICAM-1 overexpression in senescent human cells identified in atherosclerotic lesions. Lab Invest. 2005;85(4):502–511. doi:10.1038/labinvest.3700241
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.