Back to Journals » Journal of Inflammation Research » Volume 14
Genetic Polymorphisms in Genes Involved in the Type I Interferon System (IFIH1/MDA-5, TNFAIP3/A20, and STAT4): Association with SLE Risk in Egyptian Children and Adolescents
Authors Zedan MM ![]() , Attia ZR
, Attia ZR ![]() , Abd El Azeem RA, Mutawi TM, El Shehawy AS, Bakr A
, Abd El Azeem RA, Mutawi TM, El Shehawy AS, Bakr A
Received 12 March 2021
Accepted for publication 8 June 2021
Published 15 July 2021 Volume 2021:14 Pages 3349—3358
DOI https://doi.org/10.2147/JIR.S309008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monika Sharma
Mohamed M Zedan,1 Zeinab Rizk Attia,2 Rania A Abd El Azeem,2,3 Thuraya M Mutawi,2 Amora S El Shehawy,1 Ashraf Bakr1
1Department of Pediatrics, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 2Department of Laboratories, Immunology Lab, Mansoura University Children’s Hospital, Mansoura University, Mansoura, Egypt; 3Department of Clinical Laboratory Sciences, College of Medical Applied Sciences, University of Hafr Al Batin, Hafr Al Batin, Saudi Arabia
Correspondence: Zeinab Rizk Attia
Department of Laboratories, Immunology Lab, Mansoura University Children’s Hospital, Mansoura University, 60 Elgomhoria Street, Mansoura, 35516, Egypt
Tel +201098830190
Email [email protected]
Purpose: Systemic lupus erythematosus (SLE) is a multifactorial autoimmune inflammatory disease that is influenced by both genetic and environmental factors and associated with dysregulation of type I interferon (INF) response. This study aimed to investigate the effects of single nucleotide polymorphisms (SNPs) of the IFIH1, TNFAIP3, and STAT4 genes in the type I INF system on SLE risk in Egyptian children and adolescents.
Patients and Methods: We recruited 94 SLE individuals and 94 healthy subjects. SNPs of IFIH1 rs3747517 C/T, TNFAIP3 rs610604 G/T, and STAT4 rs7574865 G/T were evaluated using TaqMan™ SNP genotyping assay.
Results: Individuals with the TT, CT+TT genotypes, and T allele of rs3747517 in the IFIH1 gene were protective for SLE patients (OR = 0.429, 95% CI = 0.191– 0.962, P = 0.040), (OR = 0.685, 95% CI = 0.477– 0.984, P = 0.041), and (OR = 0.705, 95% CI = 0.527– 0.944, P = 0.019), respectively. Also, individuals with the TT, GT+TT genotypes, and T allele of rs7574865 in the STAT4 gene were associated with SLE risk (OR = 3.945, 95% CI = 1.303– 11.947, P = 0.015), (OR = 1.536, 95% CI = 1.058– 2.231, P = 0.024), and (OR = 1.522, 95% CI = 1.113– 2.082, P = 0.009), respectively. In the case of TNFAIP3 rs610604, no significant association of genotypes or alleles with SLE were detected, while the three SNPs did not show any significant association with the SLE clinical or laboratory features.
Conclusion: Our findings indicated that rs3747517 in IFIH1 was protective for SLE in Egyptian children and adolescents. Moreover, rs7574865 in STAT4 not rs610604 in TNFAIP3 was associated with SLE risk.
Keywords: systemic lupus erythematosus, type I interferon system, autoimmune disease, genetic polymorphism
Introduction
SLE is a multifactorial autoimmune disease involving genetic and environmental factors, which is characterized by pathogenic autoantibodies, chronic inflammation, and dysregulation in type I IFN pathway function.1,2 Type I interferons (IFNs) are innate immune response mediators that enhance the adaptive immune response by acting on dendritic cells, T and B cells, and natural killer cells in both direct and indirect ways.3 Genetic differences in the type I IFN pathway genes represented a common genetic factor of SLE.4
The interferon-induced Helicase C domain 1 (IFIH1, also known as melanoma differentiation-associated protein 5, MDA5) gene, is found on chromosome 2p24.3. The IFIH1 gene is a cytosolic RNA-responsive sensor that causes type I INF to progress by inducing INF regulatory factors 3,7 and the proinflammatory transcription factor nuclear factor-kB (NF-kB).5–7 Furthermore, NF-kB activation is a key factor in the pathogenesis of many inflammatory diseases.8 The tumor necrosis factor-alpha-induced protein 3 (TNFAIP3, also known as A20) gene, the ubiquitination enzyme, is located on the 6q23 chromosome. TNFAIP3 has emerged as a central negative regulator of the NF-kB signaling pathway and inflammation.9 The signal transducer and activator of transcription 4 (STAT4) gene have a key role in the activation of dendritic cells and macrophages, as well as the signal transductions within activated peripheral blood monocytes.10 It is located on the 2q32.3 chromosome.11
SNPs are the most common form of genetic variation in the human genome, and they can change the function of a gene if they are present.12 Polymorphisms in genes encoding proteins that are main components of the type I IFN pathway, such as IFIH1, TNFAIP3, and STAT4, have also been related to the risk of developing autoimmune disorders, including SLE.2 Here, we conducted the present study to clarify the hypothesis that SNPs in IFIH1, TNFAIP3, and STAT4 may affect the susceptibility of patients with SLE.
Patients and Methods
Patients
This research included 94 Egyptian pediatric and adolescent participants (82 females and 12 males with an average age of 13.7 years) and 94 controls (80 females and 14 males with the mean age of 13.5 years). All patients with SLE were diagnosed using the American College of Rheumatology (ACR) guidelines from 1997.13 Systemic lupus erythematosus Disease Activity Index (SLEDAI) was measured by the Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) damage index (SDI).14 Renal biopsy grades of SLE patients with nephritis according to the International Society of Nephrology/Renal Pathology Society (ISN/RPS) 2003 classification of lupus nephritis, as well as SLE demographic data and clinical features, were obtained from medical records filled in the Medical Archive Service and Health Information (Figures 1 and 2). All participants were enrolled between May 2018 and August 2020 from the Outpatient Clinic of pediatric nephrology (Mansoura University Children’s Hospital, Faculty of Medicine, Egypt). Each control was a healthy individual, did not suffer from any systemic disease, and had no family relation with SLE patients. The protocol was approved by the Institutional Research Board (IRB) of the Faculty of Medicine (Mansoura University, Egypt), and written informed parental consent, and child assent from participants was obtained. The study was conducted at the Laboratory according to the guidelines of the Declaration of Helsinki.
 |
Figure 1 Renal biopsy classes (stage I, II, III, IV and V) in lupus nephritis cases. |
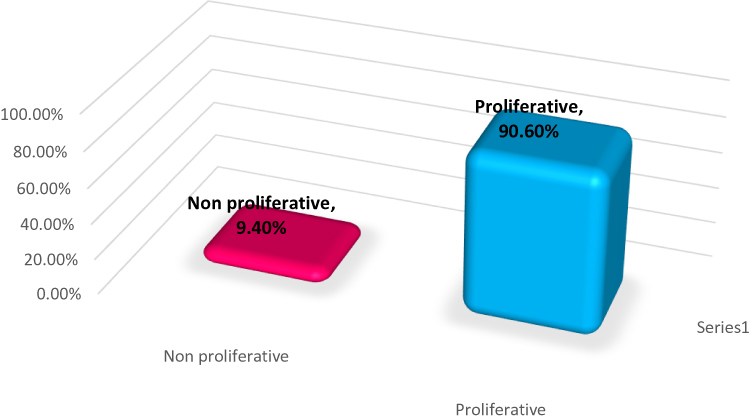 |
Figure 2 Proliferative and non- proliferative renal biopsies in lupus nephritis cases. |
Routine Laboratory Tests
We determined serum Anti-Nuclear Antibodies (ANA) by using enzyme-linked immunosorbent assay (ELISA) technique (Euroimmun, Germany) and Anti-ds-DNA by ELISA technique (INOVA Diagnostic, USA). We assessed serum complement levels (C3 and C4) with a turbidimetric assay (DIALAB GmbH, Austria). Estimation of Calcium and creatinine by using computerized DIALAB, Austria, and Phosphorous using SPINREACT, Spain. Assays had been accomplished according to the manufacturer’s instructions.
DNA Isolation and Genotyping
Genomic DNA was extracted from the peripheral blood using QIAamp DNA Blood Kit (Qiagen, Germany). Genotyping of the IFIH1 (ID: C__25984418_10 for rs3747517 C/T), TNFAIP3 (ID: C____884105_20 for rs610604 G/T) and STAT4 (ID: C__29882391_10 for rs7574865 G/T) variants were performed using the TaqMan® genotyping assays (Thermo Fisher Scientific Inc., Waltham, MA, USA). PCR reaction was conducted on Artus Rotor-Gene Qiagen fast real-time PCR System (Applied Biosystems, software 2.1.0).
Statistical Analysis
The Statistical Package for Social Science (IBM Corp., 2017) was used to analyze the data. Version 25.0 of IBM SPSS Statistics for Windows (Armonk, NY: IBM Corp.). The statistical significance of the difference in parametric data between the two groups was determined using the Student’s T-test. Kruskal Wallis test was used for differences between nonparametric numerical data among three groups. The relationship between qualitative variables was determined using the Chi-square test or Fisher’s exact test. The Goodness-of-Fit test was used to determine deviations from Hardy–Weinberg equilibrium expectancy. Moreover, Logistic regression analysis was used for the prediction of risk factors, using generalized linear models. P-values less than 0.05 were considered significant.
Results
Demographic Manifestations of the Study Population
Demographics and basic information for SLE patients and controls are summarized in Table 1, Figure 3.
 |
Table 1 Demographic, Clinical and Laboratory Characteristics of SLE (Systemic Lupus Erythematosus) Patients and Healthy Control Subjects |
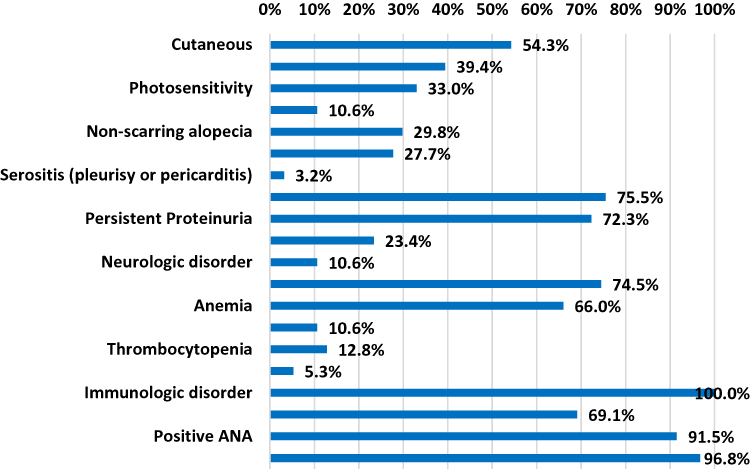 |
Figure 3 SLE features. Abbreviations: SLE, systemic lupus erythematosus; ANA, anti-nuclear antibodies. |
Association of IFIH1 rs3747517 C/T, TNFAIP3 rs610604 G/T, and STAT4 rs7574865 G/T Polymorphisms with the Risk of SLE
Full genotypes and alleles data were corresponded to Hardy-Weinberg equilibrium (HWE) in patients and controls; Table 2. The IFIH1 rs3747517 “TT”, “CT+TT” genotypes and “T” allele were significantly lowered in patient group compared with control subjects {(OR = 0.429, 95% CI = 0.191–0.962, P = 0.040), (OR = 0.685, 95% CI = 0.477–0.984, P = 0.041) and (OR = 0.705, 95% CI = 0.527–0.944, P = 0.019)}, respectively; Table 2. However, no significant evidence was detected in “CT” genotype (P=0.108); Table 2.
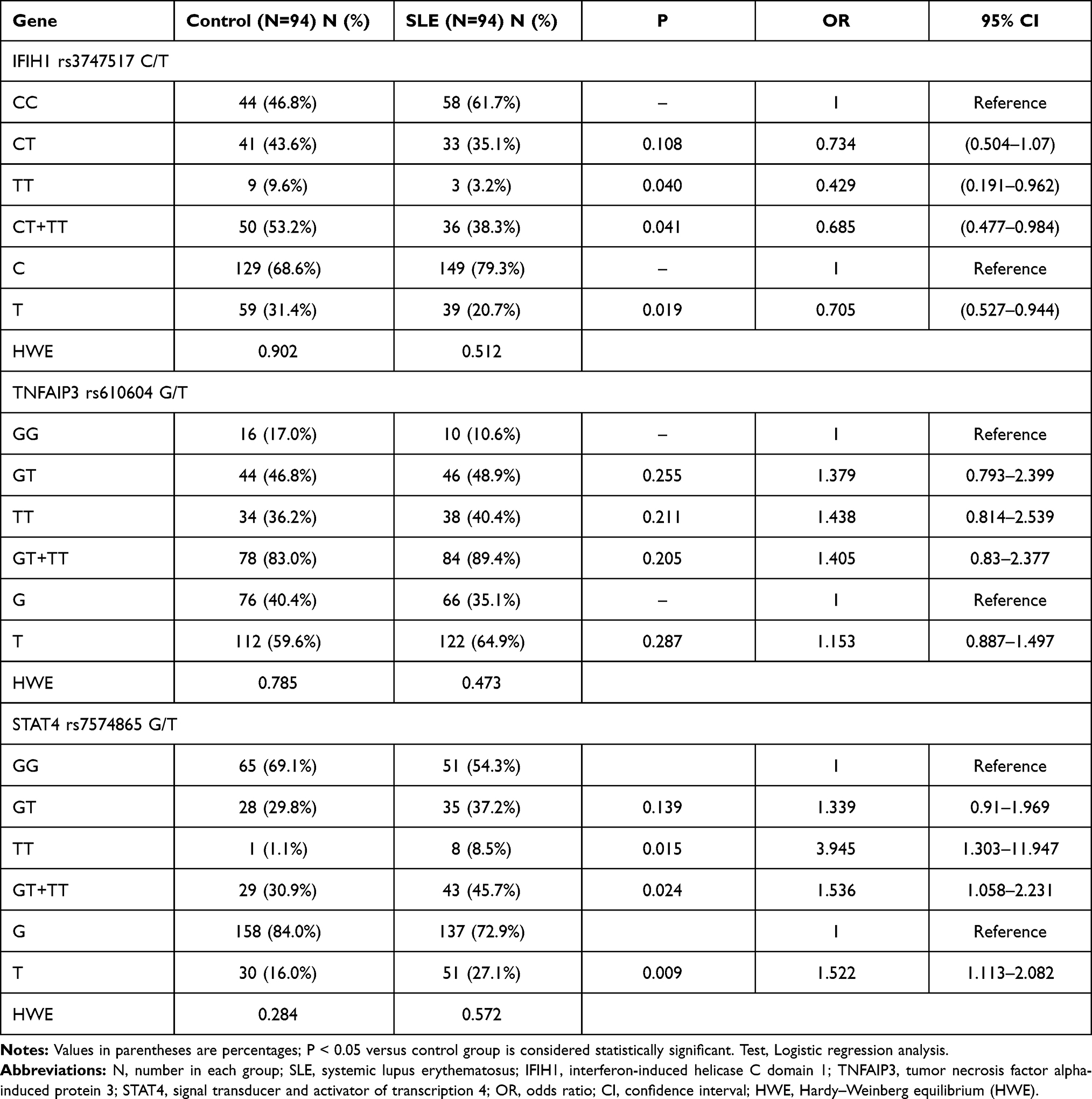 |
Table 2 Distribution of IFIH1, TNFAIP3 and STAT4 Genotype and Allele Frequencies in the Studied SLE (Systemic Lupus Erythematosus) Patients and Healthy Control Subjects |
As shown in Table 2, no significant difference in TNFAIP3 rs610604 genotype and allele distributions were found between patients and controls (P>0.05). We also determined no association of rs610604 SNP with SLE under the combined model (“GT+TT”, P= 0.205).
The frequencies of the “TT”, “GT+TT” genotypes and “T” allele of rs7574865 in STAT4 gene were significantly increased in SLE cases compared with control group {(OR= 3.945; 95% CI, 1. 303–11.947, p=0.015), (OR= 1.536; 95% CI, 1.058–2.231, p= 0.024) and (OR= 1.522; 95% CI, 1.113–2.082, p = 0.009)}, respectively; Table 2.
Association of IFIH1 rs3747517, TNFAIP3 rs610604, and STAT4 rs7574865 SNPs with Clinical and Laboratory Features in SLE Cases
Regression analysis showed no potential genetic association between the IFIH1, TNFAIP3, and STAT4 with clinical and laboratory features (P> 0.05; Table 3). However, Genotypes “CT+TT” in IFIH1 were significantly associated with the lower of SLE severity in univariate analyses and multivariate analysis {(OR =0.685, 95% CI: 0.477–0.984, P=0.041) and (OR =0.638, 95% CI: 0.440–0.924, P=0.018)}, respectively; Table 4}. Furthermore, STAT4 “GT+TT” genotype was significantly associated with the risk of SLE in univariate and multivariate analysis {(OR =1.536, 95% CI: 1.058–2.231 P=0.024) and (OR =1.644, 95% CI: 1.122–2.408, P=0.011)}, respectively; Table 4). While no significant association was detected in the case of genotype “GT+TT” in TNFAIP3 (P=0.205; Table 4).
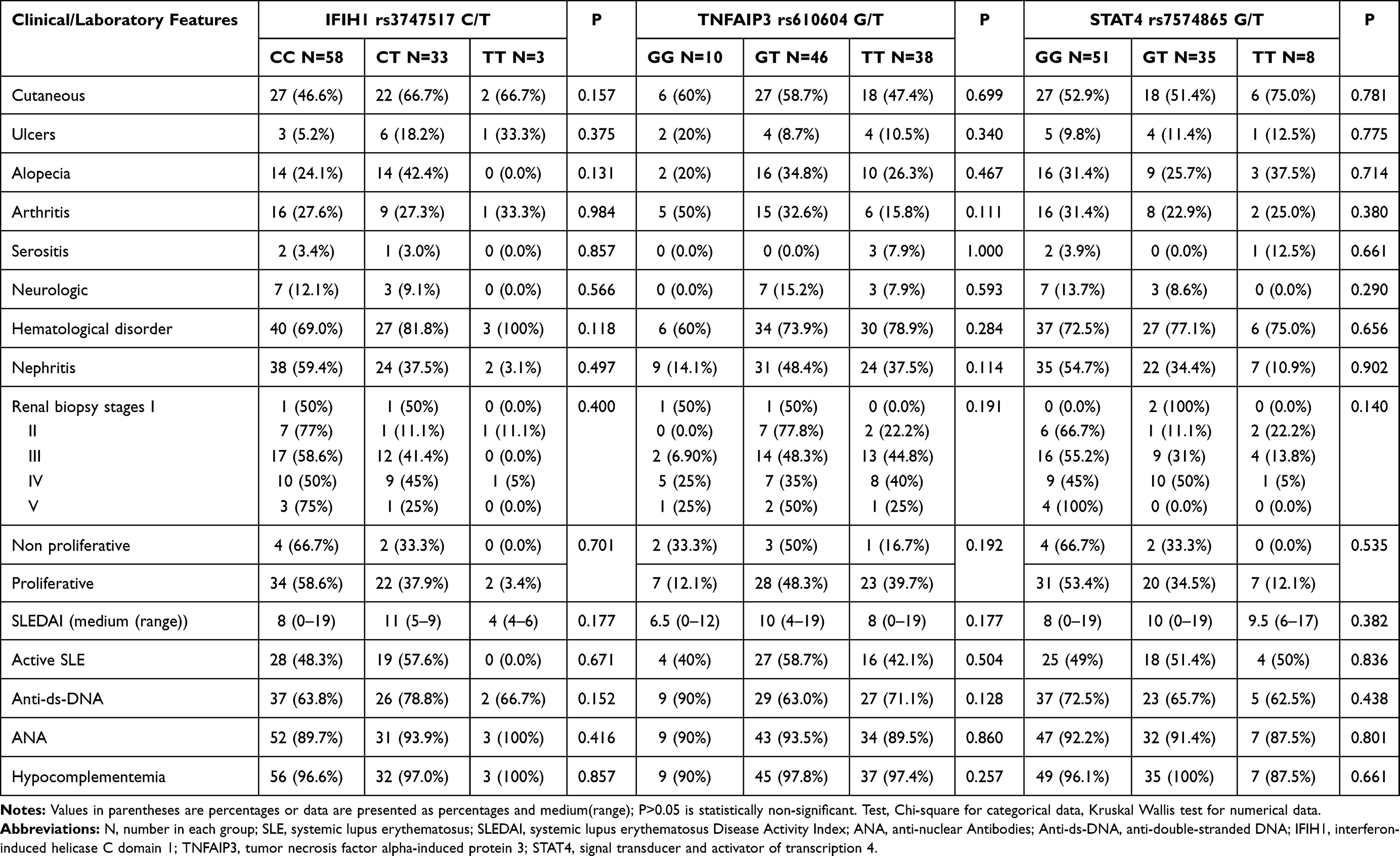 |
Table 3 Association of IFIH1 rs3747517 C/T, TNFAIP3 rs610604 G/T and STAT4 rs7574865 G/T Genotypes with SLE Clinical or Laboratory Features |
 |
Table 4 Regression Analysis for Prediction of SLE Susceptibility |
Discussion
SLE is a multifaceted autoimmune inflammatory disorder with several clinical features including immunologic defects, blood cell abnormalities, arthritis, kidney disorder, and skin disease.15–17 Similarly, immunological, hematological, renal, and cutaneous disorders were predominated in SLE cases in our research. In the present study, we investigated the association between IFIH1 rs3747517, TNFAIP3 rs610604, and STAT4 rs7574865 SNPs and SLE in Egyptian pediatric and adolescents. Type I IFNs play a key role in the pathogenesis and severity of autoimmune diseases including, SLE.7 So, any genetic variations in type I IFN system genes such as IFIH1, TNFAIP3, and STAT4 were found to be a common SLE genetic factor.4 Previous studies have related to the IFIH1, TNFAIP3, and STAT4 polymorphisms with a variety of inflammatory and autoimmune disorders such as multiple sclerosis, type 1 diabetes, psoriasis, inflammatory diseases, and SLE.18–23
IFIH1 is found in various immune system cells and is involved in autoimmune disorders such as SLE.24 IFIH1 increased IFN production by activation of NF-kB, IFN-regulatory factors 3 and 7.5,6 For the first time, we confirmed that IFIH1 rs3747517 plays a beneficial role in Egyptian children and adolescents with SLE. Our results indicated that SLE patients carrying IFIH1 “TT”, “CT+TT” genotypes, and “T” allele have a potential effect on lowering the risk of SLE. Therefore, we suggested that a protective role of the IFIH1 rs3747517 gene in SLE cases. Similarly, the IFIH1 rs3747517 polymorphism was found to be protective against SLE by Wang et al (P= 0.025).25 A haplotype analysis with IFIH1 rs78456138 and rs3747517 revealed a protective effect against SLE development in the same study.25 However, “CT” and “CC+CT/TT” genotypes at IFIH1 rs3747517 were linked to an increased risk of SLE in the Chinese Han population.7 On the other hand, Van Eyck et al found no association between the IFIH1 rs3747517 polymorphism and SLE susceptibility in Brazil in a previous study.18 Moreover, ethnic differences in the allele distributions of rs3747517 have been observed among European, Asian, and African individuals.7 Also, we failed to detect any significant association between polymorphism of rs3747517 in IFIH1 and other clinical or laboratory investigations of SLE, Table 3. Our results reinforced a previous study that found no association between the IFIH1 rs3747517 SNP and positive anti-dsDNA in SLE patients.7
The A20 encoded by TNFAIP3 has emerged as a key negative regulator of nuclear factor-KB-mediated inflammatory signaling.8 Multiple SNPs in the promoter; intronic regions, and coding exons of the TNFAIP3 gene have been discovered, and they may play a role in inflammatory and autoimmune diseases including SLE.8,26 To date, only a few studies in the literature investigated the TNFAIP3 rs610604 polymorphism in SLE. Our study found the frequencies of genotype and allele in rs610604 were higher in SLE patients than the healthy control group but no statistically significant differences between the two studied groups as cleared in Table 2. This observation confirmed no association between examined rs610604 SNP in TNFAIP3 and SLE risk in Egyptian populations. In agreement with a previous study reported by Lodolce et al, genetic polymorphism in TNFAIP3 rs610604 was not linked to SLE susceptibility in African American SLE patients.27
STAT proteins are involved in the signaling of many cytokines, hormones, and growth factors that regulate key cellular processes such as survival, proliferation, and differentiation, and are needed for IFN-dependent gene expression.28 In this study, we assessed the role of the STAT4 rs7574865 variant in SLE susceptibility. It is well documented that STAT4 can be activated by type I IFNs and STAT4 genetic variants have been linked to the development of SLE in several populations.28,29 The STAT4 gene’s SNP rs7574865 in the third intron30 is one of the most commonly studied polymorphisms31 and has been linked to the severity of SLE, with conflicting results.32 In the present study, it was found that in the Egyptian pediatric and adolescents, STAT4 rs7574865 G/T genotype displayed an increased risk of SLE and this result confirmed an association of the polymorphism with SLE. We found individuals with TT, GT+TT genotypes, and T allele were significant positive risk and severe factors for SLE. Although GT genotype is more frequent in SLE patients than in controls, no significance was detected (P>0.05; Table 2). Our genetic data agree with the meta-analysis performed by Wang et al, which revealed that STAT4 rs7574865 G/T SNP is linked to the severity of SLE in Argentinians, Colombians, Mexicans, Japanese, Chinese, and Iranians.32 Our findings confirm and extend the results of the previous study in Egyptian cohorts with adult-onset SLE.33 On the other hand, the study performed by Zervou et al found that there was no significant association in Turkish cohorts.34 This may be attributed to disparities between racial and ethnic groups.
Although, our study demonstrated that the STAT4 rs7574865 associate with the SLE risk, but we did not confirm any association between rs7574865 polymorphism and SLE clinical or laboratory parameters; Table 3. Similarly, Mirkazemi et al3 and Yin et al35 found no connection between the same SNP in the STAT4 gene and clinical manifestations of SLE in their studies. Our results were contradicted with Yang et al, the STAT4 rs7574865 variant was linked to positive anti-dsDNA antibodies36 and Kadota et al, the rs7574865 T allele in the STAT4 gene was linked to cutaneous manifestation such as malar rash in SLE patients.37 Furthermore, the rs3747517 “CT+TT” genotype was linked to SLE protection, while the rs7574865 “GT+TT” genotype was associated with disease risk in both univariate and multivariate tests; Table 4. SNPs in IFIH1 and STAT4 were considered to be independent predictors of SLE in our present study. These discrepancies between our genetic data and previous studies may be explained by both genetic and environmental influences, attributed to race/ethnic diversity, disease duration as well as variations in sample size and studied age.
Our research has a few limitations. Since the sample size of the patients examined was so small, large sample studies are needed. Besides, the patients enrolled in this study were all from the Egyptian Delta area. We were unable to obtain cases from other regions to include in our study to investigate the effect of people’s residence on their outcomes. Also, we only look at one genetic variation per gene. To understand the function of these genes in the severity of SLE, further research into more variants in the IFIH1, TNFAIP3, and STAT4 genes is needed.
Conclusion
SLE is triggered by a complex interaction of genetic and environmental factors, which is well understood. The IFIH1 rs3747517 polymorphism was found to have a protective effect in Egyptian children and adolescents with SLE in our research. Also, STAT4 rs7574865, not TNFAIP3 rs610604 SNPs, was linked to SLE risk. Furthermore, our study found no evidence of a correlation between the three SNPs studied and any of the clinical or laboratory features of SLE. However, further research is required to validate our findings.
Abbreviations
SLE, systemic lupus erythematosus; INF, interferon; SNPs, single nucleotide polymorphisms; IFIH1, interferon-induced Helicase C domain 1; TNFAIP3, tumor necrosis factor alpha-induced protein 3; STAT4, signal transducer and activator of transcription 4; MDA5, melanoma differentiation-associated protein 5; NF-kB, transcription factor nuclear factor-kB; SLICC/ACR, Systemic Lupus International Collaborating Clinics/American College of Rheumatology; SLEDAI, systemic lupus erythematosus Disease Activity Index; IRB, Institutional Research Board; ISN/RPS, International Society of Nephrology/Renal Pathology Society; ANA, Anti-Nuclear Antibodies; Anti-ds-DNA, Anti-double stranded DNA; ELISA, enzyme-linked immunosorbent assay; C3 & C4, complement components 3 and 4.
Data Sharing Statement
All data detected or analyzed during this current study are involved in this published work.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Research Board (IRB) of the Faculty of Medicine of Mansoura University. Written informed parental consent, and child assent from participants was obtained before any research procedures were conducted. This study was carried out under the guidelines of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu M, Gao W, Wu L, et al. Functional variants of TNFAIP3 are associated with systemic lupus erythematosus in a cohort of Chinese Han population. Hum Immunol. 2019;80(2):140–145. PMID: 30529365. doi:10.1016/j.humimm.2018.11.008
2. Ceccarelli F, Agmon-Levin N, Perricone C. Genetic factors of autoimmune diseases. J Immunol Res. 2017;2017:2789242. PMID: 29270439. PMCID: PMC5706077. doi:10.1155/2017/2789242
3. Mirkazemi S, Akbarian M, Jamshidi AR, et al. Association of STAT4 rs7574865 with susceptibility to systemic lupus erythematosus in Iranian population. Inflammation. 2013;36(6):1548–1552. PMID: 23912645. doi:10.1007/s10753-013-9698-8
4. Ghodke-Puranik Y, Niewold TB. Genetics of the type I interferon pathway in systemic lupus erythematosus 2013. Int J Clin Rheumtol. 2013;8(6):657–669. PMID: 24416080. PMCID: PMC3885171. doi:10.2217/ijr.13.58
5. Yin Q, Wu LC, Zheng L, et al. Comprehensive assessment of the association between genes on JAKSTAT pathway (IFIH1, TYK2, IL-10) and systemic lupus erythematosus: a meta-analysis. Arch Dermatol Res. 2018;310(9):711–728. PMID: 30171347. doi:10.1007/s00403-018-1858-0
6. Smyth DJ, Cooper JD, Bailey R, et al. A genome-wide association study of nonsynonymous SNPs identifies a type 1 diabetes locus in the interferon-induced helicase (IFIH1) region. Nat Genet. 2006;38(6):617–619. PMID: 16699517. doi:10.1038/ng1800
7. Zhang J, Liu X, Yanming M, et al. Autoimmune disease-associated IFIH1 single nucleotide polymorphism related with IL-18 serum levels in Chinese systemic lupus erythematosus patients. Sci Rep. 2018;8(1):9442. PMID: 29930297. PMCID: PMC6013496. doi:10.1038/s41598-018-27782-7
8. Momtazi G, Lambrecht BN, Naranjo JR, Schock BC. Regulators of A20 (TNFAIP3) - new drug-able targets in inflammation. Am J Physiol Lung Cell Mol Physiol. 2019;316(3):L456–L469. PMID: 30543305. doi:10.1152/ajplung.00335.2018
9. Gupta V, Kumar S, Pratap A, et al. Association of ITGAM, TNFSF4, TNFAIP3, and STAT4 gene polymorphisms with risk of systemic lupus erythematosus in a North Indian population. Lupus. 2018;27(12):1973–1979. PMID: 30041578. doi:10.1177/0961203318786432
10. Chaouali M, Fernandes V, Ghazouani E, Pereira L, Kochkar R. Association of STAT4, TGFβ1, SH2B3 and PTPN22 polymorphisms with autoimmune hepatitis. Exp Mol Pathol. 2018;105(3):279–284. PMID: 30291855. doi:10.1016/j.yexmp.2018.10.001
11. Kaplan MH. STAT4: a critical regulator of inflammation in vivo. Immunol Res. 2005;31(3):231–242. PMID: 15888914. doi:10.1385/IR:31:3:231
12. Chambliss JM, Ansar M, Kelley JP, Spratt H, Garofalo RP, Casola A. A polymorphism in the catalase gene promoter confers protection against severe RSV Bronchiolitis. Viruses. 2020;12(1):57. PMID: 31947722. PMCID: PMC7019864. doi:10.3390/v12010057
13. Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;64(8):2677–2686. PMID: 22553077. PMCID: PMC3409311. doi:10.1002/art.34473
14. Petri M, Kim MY, Kalunian KC, et al. Combined oral contraceptives in women with systemic lupus erythematosus. N Engl J Med. 2005;353(24):2550–2558. PMID: 16354891. doi:10.1056/NEJMoa051135
15. Zhang CX, Wang HY, Yin L, Mao YY, Zhou W. Immunometabolism in the pathogenesis of systemic lupus erythematosus. J Transl Autoimmun. 2020;3:100046. PMID: 32743527.PMCID: PMC7388408. doi:10.1016/j.jtauto.2020.100046
16. Bashal F. Hematological disorders in patients with systemic lupus erythematosus. Open Rheumatol J. 2013;7(1):87–95. PMID: 24198852. PMCID: PMC3816272. doi:10.2174/1874312901307010087
17. Qu C, Zhang J, Zhang X, Du J, Su B, Li H. Value of combined detection of antinuclear antibody, anti-double-stranded DNA antibody and C3, C4 complements in the clinical diagnosis of systemic lupus erythematosus. Exp Ther Med. 2019;17(2):1390–1394. PMID: 30680018. PMCID: PMC6327606. doi:10.3892/etm.2018.7072
18. Van Eyck L, De Som L, Pombal D, et al. Brief report: IFIH1 mutation causes systemic lupus erythematosus with selective IgA deficiency. Arthritis Rheumatol. 2015;67:1592–1597. PMID: 25777993. doi:10.1002/art.39110
19. Graham DSC, Morris DL, Bhangale TR, et al. Association of NCF2, IKZF1, IRF8, IFIH1, and TYK2 with systemic lupus erythematosus. PLoS Genet. 2011;7(10):e1002341. PMID: 22046141.PMCID: PMC3203198. doi:10.1371/journal.pgen.100231
20. Ciccacci C, Latini A, Perricone C, et al. TNFAIP3 gene polymorphisms in three common autoimmune diseases: systemic lupus erythematosus, rheumatoid arthritis, and primary Sjogren syndrome-association with disease susceptibility and clinical phenotypes in Italian patients. J Immunol Res. 2019;2019:6728694. PMID: 31534975. PMCID: PMC6732636. doi:10.1155/2019/6728694
21. Zamani MR, Salmaninejad A, Akbari Asbagh F, Masoud A, Rezaei N. STAT4 single nucleotide gene polymorphisms and susceptibility to endometriosis-related infertility. Eur J Obstet Gynecol Reprod Biol. 2016;203:20–24. PMID: 27235632. doi:10.1016/j.ejogrb.2016.05.003
22. Hinks A, Cobb J, Marion MC, et al. Dense genotyping of immune-related disease regions identifies 14 new susceptibility loci for juvenile idiopathic arthritis. Nat Genet. 2013;45:664–669. PMID: 23603761. PMCID: PMC3673707. doi:10.1038/ng.2614
23. Tong G, Zhang X, Tong W, Liu Y. Association between polymorphism in STAT4 gene and risk of rheumatoid arthritis: a meta-analysis. Hum Immunol. 2013;74(5):586–592. PMID: 23295549. doi:10.1016/j.humimm.2012.11.033
24. De Azevedo Silva J, Lima SC, Addobbati C, et al. Association of interferon-induced helicase C domain (IFIH1) gene polymorphisms with systemic lupus erythematosus and a relevant updated meta-analysis. Genet Mol Res. 2016;15(4). PMID: 27813554. doi:10.4238/gmr15048008
25. Wang C, Ahlford A, Laxman N, et al. Contribution of IKBKE and IFIH1 gene variants to SLE susceptibility. Genes Immun. 2013;14(4):217–222. PMID: 23535865. doi:10.1038/gene.2013.9
26. Duncan CJA, Dinnigan E, Theobald R, et al. Early-onset autoimmune disease due to a heterozygous loss-of-function mutation in TNFAIP3 (A20). Ann Rheum Dis. 2018;77(5):783–786. PMID: 28659290. PMCID: PMC5909743. doi:10.1136/annrheumdis-2016-210944
27. Lodolce JP, Kolodziej LE, Rhee L, et al. African-derived genetic polymorphisms in TNFAIP3 mediate risk for autoimmunity. J Immunol. 2010;184(12):7001–7009. PMID: 20483768. PMCID: PMC3307531. doi:10.4049/jimmunol.1000324
28. Goropevšek A, Holcar M, Avčin T. The role of STAT signaling pathways in the pathogenesis of systemic lupus erythematosus. Clin Rev Allergy Immunol. 2017;52(2):164–181. PMID: 27216430. doi:10.1007/s12016-016-8550-y
29. Remmers EF, Plenge RM, Lee AT, et al. STAT4 and the risk of rheumatoid arthritis and systemic lupus erythematosus. N Engl J Med. 2007;357(10):977–986. PMID: 17804842. PMCID: PMC2630215. doi:10.1056/NEJMoa073003
30. Gorji AE, Roudbari Z, Alizadeh A, Sadeghi B. Investigation of systemic lupus erythematosus (SLE) with integrating transcriptomics and genome-wide association information. Gene. 2019;706:181–187. PMID: 31082500. doi:10.1016/j.gene.2019.05.004
31. de Azevêdo Silva J, Tavares NAC, Santos MMS, et al. Meta-analysis of STAT4 and IFIH1 polymorphisms in type 1 diabetes mellitus patients with autoimmune polyglandular syndrome type III. Genet Mol Res. 2015;14(4):17730–17738. PMID: 26782418. doi:10.4238/2015.December.21.46
32. Wang JM, Xu WD, Huang AF. Association of STAT4 gene Rs7574865, Rs10168266 polymorphisms, and systemic lupus erythematosus susceptibility: a meta-analysis. Immunol Invest. 2021;50(2–3):2–3. PMID: 32429712. doi:10.1080/08820139.2020.1752712
33. El-Saadany HM, Amer WH, Khalil HS, Gaber RA, Elshweikh SA. Association of STAT4 polymorphism with susceptibility and severity of rheumatoid arthritis and systemic lupus erythematosus in Egyptian patients. Egypt Rheumatol. 2016;38(1):21–27. doi:10.1016/j.ejr.2015.04.003
34. Zervou MI, Vazgiourakis VM, Yilmaz N, et al. TRAF1/C5, e NOS, C1q, but not STAT4 and PTPN22 gene polymorphisms are associated with genetic susceptibility to systemic lupus erythematosus in Turkey. Hum Immunol. 2011;72(12):1210–1213. PMID: 21968398. doi:10.1016/j.humimm.2011.09.003
35. Yin S, Yi Z, Xu L, et al. Variation in STAT4 is associated with systemic lupus erythematosus in Chinese Northern Han population. Chin Med J. 2010;123(22):3173–3177. PMID: 21163111. doi:10.3760/cma.j.issn.0366-6999.2010.22.001
36. Yang W, Ng P, Zhao M, et al. Population differences in SLE susceptibility genes: STAT4 and BLK, but not PXK, are associated with systemic lupus erythematosus in Hong Kong Chinese. Genes Immun. 2009;10(3):219–226. PMID: 19225526. doi:10.1038/gene.2009.1
37. Kadota K, Mori M, Yanagimachi M, et al. Analysis of gender differences in genetic risk: association of TNFAIP3 polymorphism with male childhood-onset systemic lupus erythematosus in the Japanese population. PLoS One. 2013;8(8):e72551. PMID: 24023622. PMCID: PMC3758304. doi:10.1371/journal.pone.0072551
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.