Back to Journals » Infection and Drug Resistance » Volume 14
Genetic Diversity and Acquired Drug Resistance Mutations Detected by Deep Sequencing in Virologic Failures among Antiretroviral Treatment Experienced Human Immunodeficiency Virus-1 Patients in a Pastoralist Region of Ethiopia
Authors Tachbele E ![]() , Kyobe S
, Kyobe S ![]() , Katabazi FA, Kigozi E, Mwesigwa S
, Katabazi FA, Kigozi E, Mwesigwa S ![]() , Joloba M, Messele A
, Joloba M, Messele A ![]() , Amogne W
, Amogne W ![]() , Legesse M, Pieper R, Ameni G
, Legesse M, Pieper R, Ameni G ![]()
Received 2 September 2021
Accepted for publication 3 November 2021
Published 18 November 2021 Volume 2021:14 Pages 4833—4847
DOI https://doi.org/10.2147/IDR.S337485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Erdaw Tachbele, 1, 2 Samuel Kyobe, 3 Fred Ashaba Katabazi, 3 Edgar Kigozi, 3 Savannah Mwesigwa, 3 Moses Joloba, 3 Alebachew Messele, 1 Wondwossen Amogne, 2 Mengistu Legesse, 1 Rembert Pieper, 4 Gobena Ameni 1
1Aklilu Lemma Institute of Pathobiology, Addis Ababa University, Addis Ababa, Ethiopia; 2College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3College of Health Sciences, Makerere University, Kampala, Uganda; 4Janssen Biopharma, South San Francisco, CA, USA
Correspondence: Erdaw Tachbele Tel +251 911642880
Email [email protected]
Purpose: This study was conducted to investigate the drug resistance mutations and genetic diversity of HIV-1 in ART experienced patients in South Omo, Ethiopia.
Patients and Methods: A cross-sectional study conducted on 253 adult patients attending ART clinics for ≥ 6 months in South Omo. Samples with VL ≥ 1000 copies/mL were considered as virological failures (VF) and their reverse transcriptase gene codons 90– 234 were sequenced using Illumina MiSeq. MinVar was used for the identification of the subtypes and drug resistance mutations. Phylogenetic tree was constructed by neighbor-joining method using the maximum likelihood model.
Results: The median duration of ART was 51 months and 18.6% (47/253) of the patients exhibited VF. Of 47 viraemic patients, the genome of 41 were sequenced and subtype C was dominant (87.8%) followed by recombinant subtype BC (4.9%), M-09-CPX (4.9) and BF1 (2.4%). Of 41 genotyped subjects, 85.4% (35/41) had at least one ADR mutation. Eighty-one percent (33/41) of viraemic patients harbored NRTI resistance mutations, and 48.8% (20/41) were positive for NNRTI resistance mutations, with 43.9% dual resistance mutations. Among NRTI resistance mutations, M184V (73.2%), K219Q (63.4%) and T215 (56.1%) complex were the most mutated positions, while the most common NNRTI resistance mutations were K103N (24.4%), K101E, P225H and V108I 7.5% each. Active tuberculosis (aOR=13, 95% CI= 3.46– 29.69), immunological failure (aOR=3.61, 95% CI=1.26– 10.39), opportunistic infections (aOR=8.39, 95% CI= 1.75– 40.19), and poor adherence were significantly associated with virological failure, while rural residence (aOR 2.37; 95% CI: 1.62– 9.10, P= 0.05), immunological failures (aOR 2.37; 95% CI: 1.62– 9.10, P= 0.05) and high viral load (aOR 16; 95% CI: 5.35 51.59, P < 0.001) were predictors of ADR mutation among the ART experienced and viraemic study subjects.
Conclusion: The study revealed considerable prevalence of VF and ADR mutation with the associated risk indicators. Regular virological monitoring and drug resistance genotyping methods should be implemented for better ART treatment outcomes of the nation.
Keywords: HIV-1, genetic diversity, acquired drug resistance, ART experienced, South Omo, Ethiopia
Corrigendum for this paper has been published
Introduction
At the end of 2018, 19.5 million people living with HIV were accessing ART globally.1 However, virological failure and development of drug resistance are becoming a bottleneck for the success of ART program. A global study involving 36 countries and 1926 patients with treatment failure from 1998–2015 reported that 36.3% patients developed tenofovir resistance, where the highest (57%) was in sub-Saharan Africa. Of 700 individuals with tenofovir resistance, 578 (83%) had M184V/I mutation, 543 (78%) had major NNRTI resistance, and 457 (65%) had both.2
Since the first evidence of HIV infection in Ethiopia in 1984, AIDS has taken the lives of millions and left behind an estimated 744,100 orphans.3 At the end of 2016, the national HIV prevalence stabilized at 1.12%, and 715,500 people living with HIV/AIDS, with 27,288 AIDS related deaths, and 19,743 new infections in the year.4 Since free ART initiated in 2005 in Ethiopia, a total of 386,123 estimated adults living with HIV have been receiving ART with 73% coverage.5
Studies conducted in Ethiopia indicated that the prevalence of VF range from 5.3% to 18% among HIV/AIDS patients who were on ART for a median time of 6–24 months, while the dominant reported drug resistance mutations on RT gene were M184V, K103I, and no mutations reported on protease inhibitors associated gene.6–8 Another study conducted in Addis Ababa, reported 31% VF, and 70% ADR mutations among the viraemic patients, out of which 62% against NRTIs, 68% against NNRTIs, 61% against any NRTI and NNRTI double class mutations.9
Data on virological failures and drug resistance mutations among patients on ART in Ethiopia is scarce due to lack of routine laboratory monitoring of HIV VL and genotype tests.10 As the current study site borders to Kenya and South Sudan, and known world tourist destiny site, there is a concern that new HIV-1 variants may be introduced and intermixed from the neighboring and other countries.11,12
Furthermore, the available HIV drug resistance studies conducted in Ethiopia so far were based on the Standard Genotypic Resistance Testing (SGRT), that could not reliably detect clinically important low frequency (< 20%) drug resistance variant mutations of the virus quasispecies in a clinical sample.13–16 Currently, the emerging NGS platforms like Illumina MiSeq allow the detection of minority resistance mutation variants with 0.5–1% lower limit of detection while maintaining good accuracy.17–22
Therefore, this study was conducted to determine HIV-1 genetic diversity, rate of HIV-1 virological failure and ADR mutations using Illumina MiSeq in HIV-1 infected adults on ART for ≥ 6 months in South Omo, Ethiopia.
Patients and Methods
Study Area and Setting
This study was carried out in South Omo Zone of Southern Ethiopia bordering with Kenya in south and with South Sudan in southwest. The Zone is one of the least developed areas of the country with poor infrastructure, and inhabited by ethnically diversified population; possibly as many as 24 ethnic groups with unique cultural practices in the world, dominated by the ancient Nilotic pastoralist traditions.23 The Zone inhabited by 573,435, of which 43,203 were urban inhabitants, and 25,518 were pastoralists.24
Study Design and Setting
A cross-sectional study was conducted from January 2016 to December 2018 in patients attending ART clinic in four health centers and Jinka Zonal Hospital. Adult patients (age ≥18 years) who gave informed written consent and who had been on ART for 6 or more months and were still on ART at the time of enrolment were considered for the study. Sample size was determined using single population proportion formula assuming an HIV-1 VF prevalence of 21% after a median follow-up period of 12 months on ART in sub-Saharan setting,25 and 5% of margin of error.
Specimen Collection Procedure
A standardized drug resistance survey data collection questionnaire was used to collect socio-demographic and clinical data. Upon written consent, 10 mL EDTA blood samples were collected for CD4+T-cell count, viral load assays and genotyping. Plasma was temporarily stored in multiple aliquots at −30°C at the study site and transported to Addis Ababa University and stored at −80°C, until shipped to Kampala, Uganda on dry ice for VL measurement and genotyping at Makerere University. CD4+ T cell counts were monitored at the time of ART initiation and every 6 months as part of the ART program. All tests were done anonymously linked with unique code.
CD4+ T Cell Counts, RNA Extraction and Viral Load Measurement
CD4+ T cell count was performed within 4–6 hours of blood collection using a FACS Caliber flow cytometer (FACScount Becton & Dickinson Immunocytometry, Oxford, UK) at the study site. HIV-1 genomic RNA was extracted from 140 µL of cryopreserved plasma using the QIAmp viral extraction kit (QIAGEN, Hilden, Germany) as per the manufacturer’s protocol. Viral load was estimated using QuantiTect Probe RT-PCR kit (QIAGEN, Hilden, Germany) following the manufacture’s protocol26 using the following primers and probes that targets the conserved portion of GAG and LTR genome of HIV-1 virus: Gag 183UF:CTA GCA GTGG CGCCGACAG, Gag187LR:CCATCTCTCTCCTTCTAGC CTCCGCTAGTCA, Probe Gag 187 PFAM–5ʹTCTCTC GACGCA G GACTC GCTTGCTG’3 –BHQ.
Amplicons Generation for Illumina MiSeq Sequencing
Two rounds of PCR were used to generate HIV DNA fragments spanning the HIV reverse transcriptase (RT) codons 90–234, as described previously following the manufacturer’s protocol.14 Briefly, first strand DNA was generated using KAPA HiFi HotStart ReadyMix PCR kit (Boston, USA) following an in vitro reverse transcriptase using TaKaRa PrimeScriptTM RT-PCR kit (Clontech Laboratories, Takara Bio Company). Using cDNA as a template, first round PCR was conducted using the following primers and cycling conditions: HIVRT3.1F: GAAGGGC ACACAGCCAGAAATTGCAG and HIVRT3.1R: GCTCCTACTATGGGTTCTTTCTCTAAC TGG. Using the first round PCR product as a template, second round PCR was done using internal sequence specific primer fused with Illumina Adaptors that adds the sequence to amplicon complementary to those on Illumina MiSeq flow cell as described elsewhere.14 ILRT2796F: TCGTCGGCAGCGTCAGATGTGTATAAGAGACAGAGAACTCAAGACTTCTGGA; ILRT3271R: GTCTCGTG GGCTCGGAGATGTGTATAAGAGACAGACTGTCCATTTATCAGGATC.
Cycling conditions for both PCRs were the same: 1) Initial denaturation at 95°C, 2min., 2) denaturation at 98°C, 30 sec., 3) annealing at 60°C, 30 sec, 4) extension at 72°C, 1 min (Step 2–4 for 35 cycles) and 5) final extension at 72°C, 10 min. Following amplification, 3µL of each 2nd round PCR product was analyzed on the QIAxcel Advanced, using the Fast analysis Cartridge. The expected amplicon is approximately 500bp, a short region spanning RT codon 90–234 was amplified in a nested second PCR with primers incorporating Illumina indexing adaptors (Lapointe et al 2015).
MiSeq Library Preparation and Sequencing
Multiplexing and Purification
Library preparation for MiSeq sequencing was done using a NextEra® XT DNA Sample Preparation and Index kit (Illumina, San Diego, CA, USA) as described elsewhere.14 Briefly, eight base pair-long NextEra XT multiplexing indices were added using low cycle PCR to both the 5ʹ and 3ʹ ends of each amplicon used as a unique identifier in pooling up to 96 samples for subsequent sequencing simultaneously. A total of 9 i7 and 30 i5 indices were used to prepare up to 114 samples in two plates following Illumina NextEra XT indexing procedure.27 Multiplexed MiSeq amplicons were purified using Agencourt AMPure® XP PCR purification systems (Beckman Coulter Company, Germany).
Library Quantification, Normalization, and Pooling
Library quantification was determined using Qubit® dsDNA HS (High Sensitivity) Assay kits using the Qubit® 2.0 Fluorometer. A final library with equimolar concentration of 4nM was prepared using Re-suspension Buffer, and 5 µL of diluted DNA was aliquoted from each library and then the two libraries were pooled with unique indices prior to MiSeq sequencing with a 2×300 cycles v3 reagent kit.
Denature and Dilute PhiX Control
In preparation for cluster generation and sequencing, pooled libraries were denatured using freshly diluted 0.2N NaOH with hybridization buffer, and then heat denatured before MiSeq sequencing. A 5% PhiX spike-in was added to serve as an internal control for these low diversity libraries according to Illumina recommendation.
MiSeq Data Processing
Sequences were de-multiplexed automatically on the MiSeq and two paired fastq files were generated for each sample representing the two paired-end reads. MiSeq short-read data in fastq format were imported and processed by freely available pipeline, MinVar, rapid and versatile tool for HIV-1 drug resistance genotyping by deep sequencing (Huber et al 2017). MiSeq consensus sequences spanning RT codons 90 to 234 were produced from the empirical raw nucleotide frequency distributions in the aligned and merged read data. The main output was a table with subtype and amino acid mutations with respect to HIV-1 consensus B, annotated according to the class of resistance defined in the Stanford HIVdb.28 Drug resistance associated mutations were grouped as NRTI, NNRTI and others.
Phylogenetic Analysis
All sequences were automatically aligned with reference sequences of all known HIV-1 group M (sub-) subtypes (A1, A2, B, C, D, F1, F2, G, H, J, and K) and circulating recombinant forms (CRFs) retrieved from the Los Alamos database using MUSCLE in MEGA 6 software.29 HIV-1 subtyping was determined using REGA version 3 of Stanford HIVdb.30 Phylogenetic tree was constructed by the neighbor-joining method using the Maximum Likelihood Model. The reliability of the tree was assessed by bootstrapping of 1000 replicates. Clustering of sequences with a bootstrap value of more than 70% was considered significant for subtyping. DNA polymorphism was analyzed using DnaSP software.
Variable Definitions
The major outcomes of interest in this study were virological Failure (VF), HIV-1 genetic diversity and ADR mutations. Detectable VL was defined as HIV-1 RNA levels ≥126 copies/mL and VF as HIV-1 RNA ≥1000 copies/mL. The prevalence of HIV-1 VF was determined as percentage of plasma samples with detectable viral load ≥1000 copies/mL. The prevalence of ADR was determined as percentage of samples with detectable resistance associated mutations as determined by the Stanford HIV drug resistance database divided by the total number of samples with VF that were successfully sequenced.
Based on the Stanford HIV drug resistance database, mutation levels were classified as high resistant (H), intermediate (I), low (L), potential low (PL), and susceptible (S). In this study, a read frequency of 5% and 20% was considered as a minor variant, and a read frequency >20% was classified as a major variant. All Food and Drug Administration (FDA) approved first line ARVs were considered for analysis that were covered in the sequenced region (codon 90–234) of RT gene.31
Data Analysis
Descriptive statistics were employed to describe socio-demographic, clinical characteristics, HIV-1 VF and different types of drug resistant mutations among the study subjects. Continuous data were presented using mean and medians, and categorical data were presented as frequencies and percentages. To determine the independent predictor variables of ADR mutations among the study subjects, bivariate and multivariate logistic regression analysis were conducted. Crude and adjusted odd ratios (OR), 95% confidence intervals (CI) and p-values <0.05 were considered significantly associated. Data analysis was performed using SPSS for Windows, Version 23.0. Chicago, SPSS Inc.
Ethics Approval and Consent to Participate
Institutional permission to conduct the study was obtained from Aklilu Lemma Institute of Pathobiology Institution Review Board, Addis Ababa University. In addition, written consent was received from each study participant. We confirm that the revised manuscript of this study was conducted in accordance with the Declaration of Helsinki.
Results
Baseline Characteristics of the Study Participants
A total of 253 adults on first line ART for a median duration of 51 (IQR: 49–61) months were recruited from January 2016–December 2018. Majority of them were females (60.5%), mean age was 33.5 years ([95% CI: 32.5–34.5/]) and 70% the study subjects were taking tenofovir (TDF) based ART, while 30% were on Zidovudine (AZT) based regimen during the study period. Majority (71.9%) of them started ART in WHO III/IV stage, with the median base line CD4 count of 239 (95% CI: 204–284.5) and IQR of 228 (95% CI: 208–268). About 40% (102/253) of the participants reported poor ART adherence. Majority (94%) of study subjects had base line CD4 cell counts ≤ 350 cells/µL at the start of the study (Table 1). Based on the fall of follow up CD4 count to baseline, severe immunological failure was observed in 11.5% (27/235) of the subjects and it was significantly associated with older age and malnutrition in the bivariate analysis (OR= 5.9, 95% CI: 1.7–20.1, P.= 0.005) and (OR= 3.1, 95% CI:1.22–8.10, P=0.02) respectively (data not shown).
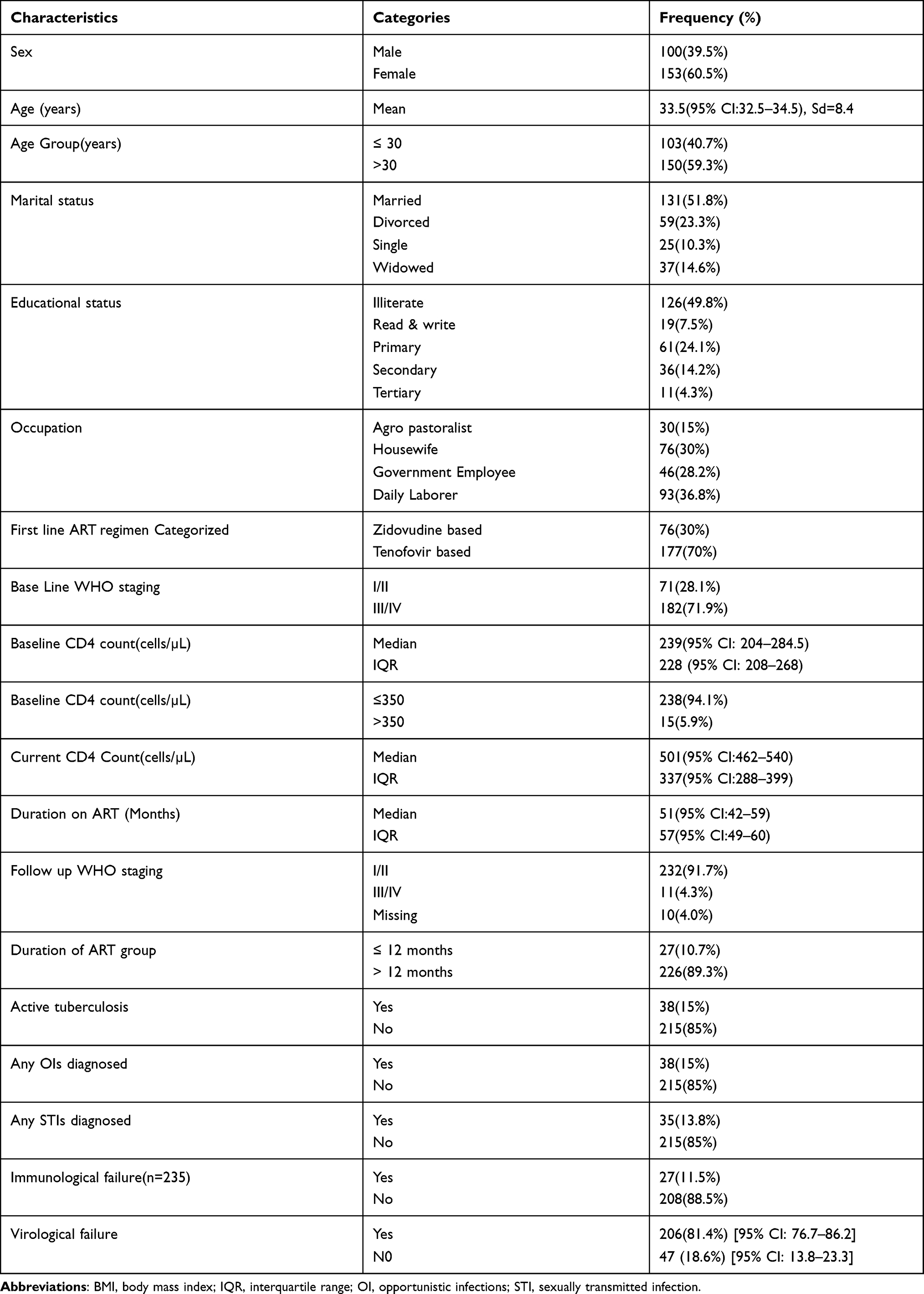 |
Table 1 Socio-Demographic and Clinical Characteristics of the Study Subjects Among First Line ART Experienced Patients at South Omo, Ethiopia (n=253) |
Phylogenetic Analysis of HIV-1 Sequences of RT Gene from ART Experienced Patients
From a total of 253 ART experienced study subjects, 47 (18.6%) showed VF (≥1000 copies/mL), of which 41 isolates were successfully sequenced on MiSeq platform using partial reverse transcriptase (RT) gene covering codons 90–234. Sequencing was successfully completed with cluster density of 1043/mm2, 82.5% of clusters passing filters, and 79.6% base with Q scores of ≥30, and mean depth coverage of 70,000X (760–110,000X).
HIV-1 subtypes were analyzed for the 41 MiSeq sequenced isolates based on 500kb sequences of RT gene. Figure 1 shows the genetic diversity of HIV-1 samples from ART experienced patients in South Omo, Ethiopia. HIV-1 subtype C was the dominant, 87.8% (36/41), followed by inter-subtype recombinants strains BC (4.9%), M-09-CPX (4.9%), and BF1 (2.4%) were found. DNA polymorphism analyses indicated that HIV-1 isolates exhibited high haplotype (h>0.99) and nucleotide (π >0.08) diversity.
 |
Figure 1 Phylogenetic tree of 41 HIV samples collected from South Omo Zone, Ethiopia. cDNA was prepared from HIV-1 genomic RNA, and a region spanning codons 90–234 of HIV reverse transcriptase was PCR amplified and sequenced on the Illumina MiSeq platform. A neighbor-joining tree30,32 constructed from the consensus sequences is depicted as a circular cladogram. Clinical samples are coded by a prefix OMO, indicating the name of the study site followed by two digit numbers. HIV-1 subtype consensus sequences (n=25) spanning RT codons 90 to 234 were included and represent subtypes A1, A2, B, C, D, F1, F2, G, and H, as well as recombinant viruses AE, AG, AB, BC, CD, BF, BG (retrieved from http://www.hiv.lanl.gov) and reference amplicon. HIV-1 RT sequences were primarily subtypes C. There were a total of 476 positions in the final dataset. Evolutionary analyses were conducted in MEGA627. |
 |
Figure 2 ADR mutation frequency at 5%and 20% detection sensitivity thresholds, as determined by MiSeq sequencing. |
 |
Figure 3 Predicted ARV drug responses of 35 patients with ADR mutations. Drug responses were based on the Stanford HIVdb. The y-axis indicates the number of sequences with ADR while the x-axis indicates the different ARV druelsg classes that were affected by the ADR mutations. Abbreviations: ADR, acquired drug resistance; NRTIs, nucleoside reverse transcriptase; NNRTI, nonnucleoside reverse transcriptase inhibitors; ABC, abacavir; AZT, zidovudine; DDI, didanosine; 3TC, lamivudine; D4T, stavudine; TDF, tenofovir; NVP, nevirapine; EFV, efavirenz; ETR, etravirine RPV, rilpivirine. |
Prevalence of Acquired Drug Resistance Mutations (ADR)
Out of 41 genotyped isolates, 85.4% (35/41) had at least one ADR mutations on RT gene, while 14.6% (6/41) viraemic samples did not have any detectable resistance mutations, or had very low frequency (2–4%) drug resistance mutants. Among study subjects who harbored at least one DRM, 60% (14/35) were taking tenofovir (TDF) based regimen, while 40% (11/35) were on zidovudine (AZT). With regard to NNRTI class, 21 (60%) were taking efavirenz-containing ART regimen, while 14 (40%) were on nevirapine combined regimen. However, there was no significant associations between regimen type and development of drug resistance mutations among both drug class combinations.
Out of the 41 viraemic subjects 33 (80.5%) harbored NRTI resistance mutations, and 20 (48.8%) were found to have NNRTI resistance mutations, while 13 (31.7%) harbored other resistance mutations like V90A, K101Q and K103R. Both NRTI and NNRTI resistance mutations were simultaneously detected among 18 (43.9%) viraemic patients (Table 2).
 |
Table 2 HIV-1 Drug Resistance Conferring Mutations in the RT Gene Among First Line ART Experienced Adults with ADR Mutations, South Omo, Ethiopia, 2017 (N=41) |
Among NRTI resistance mutations, M184V (73.2%), and K219Q, (63.4%) were the most common resistance mutations detected from viraemic subjects, respectively. Among the drug resistance harboring subjects, 23 (56.1%) were found to have T215 complex which is Thymidine Analog–associated Mutations (TAMs) that are known to affect all NRTIs currently approved by the US FDA other than emtricitabine and lamivudine (Figure 2). In addition, multi-NRTI resistance mutation, Q151M was detected among 5 (12.2%) of the study subjects, which affects all NRTIs currently approved by the US FDA except tenofovir33 (Table 2).
Of the 41 viraemic specimens genotyped, the major NNRTI resistance-associated mutations detected were: K103N (24.4%), P225H (7.3%), K101E (7.3%), V108I (7.3%), V90I (4.9%), V106M/A (9.8%), H221Y (4.9%), E138G/A (4.9%), and Y181C (4.9%). Among the NNRTI associated mutations, Y188D was detected in all viraemic patients at low frequency (2–4%), which is not common in earlier reports. All NNRTI resistance associated mutations were found as major variants (>20% detection level; Figure 2 and Figure 3).
We examined risk factors associated with HIV-1 ADR mutations among first line ART experienced patients (Table 3). In bivariate analysis, resident type, occupation, immunological failure, follow up CD4+ T cell count, missed ART pills within the last week, and VL were found to be associated with ADR mutations. However, in multivariate model analysis only residence type, immunological status and VL at the time of sampling were found to be independent predictors of acquired drug resistance mutation among the ART experienced and viraemic study subjects. Accordingly, study subjects that resided in rural areas were three times more likely to develop ADR (aOR 2.37; 95% CI: 1.62–9.10, P= 0.05) than urban dwellers. Similarly, study subjects that showed immunological failure during ART (aOR 2.37; 95% CI: 1.62–9.10, P= 0.05) had a higher prevalence of ADR, compared to those with immunological recovery. Likewise, participants with higher VL (≥3.7 log copies/mL) had a higher prevalence of ADR, in comparison to those with lower viral loads (< 3.7log copies/mL (aOR 16; 95% CI: 5.35 51.59, P <0.001)) (Table 3).
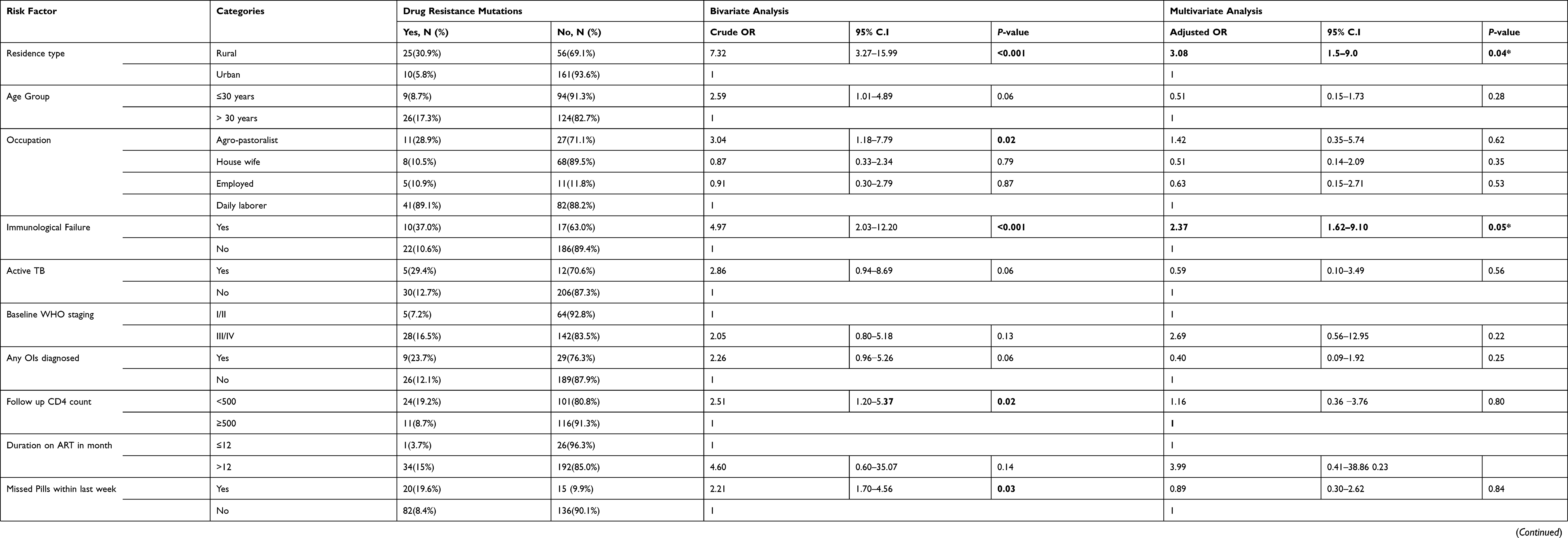 |
Table 3 Logistic Regression Analysis Describing Associations of HIV-1 Drug Resistance Mutations Among First Line ART Experienced Patients in South Omo, Ethiopia (n=253) |
Discussion
In this study, we investigated HIV-1 genetic diversity and acquired drug resistance mutations among 253 adults on first-line antiretroviral treatment for ≥ 6 months in South Omo, Ethiopia.
Detection of a significant number of HIV-1 subtype C in the current study in Ethiopia is in agreement with the previous studies that unanimously reported the HIV-1 epidemic in Ethiopia is dominated by subtype C viruses with two co-circulating sub-clusters named C and C’ that were identified since 2000.34–37 It is well established fact that the dominant circulating HIV-1 subtype in East Africa is subtype C with different geographical clusters identified as East African HIV-1 subtype C, and Ethiopian unique subtype C’ lineage.35,37 However, 8.5% HIV-1 isolates from in Djibouti patients were identified as subtype B,38 and two isolates (1%) from Addis Ababa were detected as subtype B.9
The identification recombinant HIV-1 subtype BC, BF1 and M-09-cpx in the current study might indicate the introduction of new subtypes as a result of high tourist flow and population movement between the bordering countries in the study area. However, this finding should be interpreted with precaution since we sequenced a very short RT region used for drug resistance mutation analysis that may not be suitable for HIV subtyping. As a result, future studies that involve long and conserved region of the virus will be required to proof that we had non-C subtypes in Ethiopia.
Eighty five percent (35/41) of the genotyped study subjects had at least one RTI-associated drug resistance mutations, is similar to the South African study where 84% viraemic samples had one or more ADR mutations,39 and comparable to the pooled ADR mutation prevalence of 70.7% reported by WHO at the end of 201,1 where resistance to NNRTI had the highest observed rate (61%), followed by NRTI (55%). Similarly 70% prevalence of ADR mutation in Addis Ababa was reported by Abegaz in 2011.9
In contrast, more than 80% of NRTI resistance mutation described in this study is much higher than 55.3% reported from West Africa, while 48.8% NNRTI associated resistance mutation prevalence is comparable to 57% NNRTI prevalence reported from other East African Countries.10,40 The disparity may emanate from the genotyping methods used. Most previous studies used the conventional Sanger based genotyping tests to identify HIV drug resistance associated mutations that could miss the lower abundance variants, unlike the current study which applied NGS platforms that could detect low frequency mutations.
Similar to our study, 83% for reverse transcriptase inhibitors (RTIs) drug resistance mutations among viraemic patients was reported from Rwanda.41 Moreover, another study from Spain, indicated 76.9% NRTI drug resistance mutations and 36.5% NNRTI associated mutations among ART experience patients.42 Similar to our report, a decade review from India identified drug resistance mutation prevalence of 78.4% to any RTIs, 68.8% to NRTI, and 73.13% to NNRTI among first line ART experienced adults.43 The most recent WHO report also indicated that NNRTI resistance ranged from 47% to 90% among people with viral failure on first-line NNRTI containing regimens, which are the backbone of the WHO first line ART regimen.1
Mathematical modeling on global trend on drug resistance pattern suggesting that NNRTI resistance mutations harboring individuals were found to be more likely to acquire new HIVDR mutations and experience death, this in turn may be a challenge to achieve the global targets to end AIDS as a public health threat by 2030.1
In this study, majority (60%) participants who had ADR mutations were on tenofovir (TDF), while the remaining 40% were on Zidovudine (AZT) based regimen. However, regimen type did not show any association with viral failure and drug resistance mutations. A recent global research conducted in an attempt to find a point of care genotypic resistance test to detect HIV-1 drug resistance mutations revealed that the most common major DRMs were M184V (91.5%) and the TAMs complex 34.5%,44 which is comparable to the prevalence of major NRTIs in the present study. Moreover, this is in line with another study conducted in Northern India that reported 89.8% NRTI and NNRTI ADR mutations among virological failures with M184V, T215Y were the most frequent NRTI associated mutations and K103N, G190A, Y181C from NNRTI associated ones.45
In consistent with this study, quite a number of global and regional genetic analyses of HIV-1 have unanimously reported that the most globally prevalent NRTI resistance mutations is M184V followed by thymidine analog-associated mutations (TAM) including M41L, D67N, K70R, L210W, T215Y/F and K219Q/E, and, the most prevalent NNRTI was K103N.10,33,40,46–48 Similarly, WHO 2017 drug resistance mutations revealed that the most commonly observed NRTI‑associated resistance mutations were at codons 184, and the most commonly observed NNRTI-associated mutations were at positions 103, 181 and 190 globally.1
In this study, all NNRTI resistance mutations were found at a higher frequencies and no minor mutations were detected. The most frequent NNRTI resistance mutation detected were K103N (24.4%), followed by K101E, V108I and P225H found at 7.3% prevalence each. Interestingly, the finding identified all the four RT gene positions (K103N, Y181C, G190A and V106M) recommended for point of care genotypic test for DRMs in low and middle income countries.44
In the current study the most abundantly identified resistance mutations were M184V, K103N and TAMs which are known to be the key resistance mutation types among ART naïve and experienced subjects.49 It is known that M184V causes high level resistance to 3TC and FTC and low level resistance to ddI and ABC, however, it increases susceptibility to TDF, AZT and d4T susceptibility and decreases viral replication fitness, and it also appears to delay or prevent emergence of TAMs.50 TAMs were first reported among patients receiving AZT monotherapy.51–53 The presence of TAMs in this study may be a warning sign for clinicians in charge of the AIDS patients to closely monitor their clients, as TAMs are known to reduce all NRTIs susceptibility currently approved by the US FDA other than emtricitabine and lamivudine.33,54 K103N is a non-polymorphic mutation selected in patients receiving NVP and EFV,55 which is known to reduce NVP and EFV susceptibility by about 50 and 20-fold, respectively.56
Hence, the high prevalence of M184V and K103N in the present study may be challenging to control HIV viraemia among ART experienced patients, as these mutations almost affect all FDA approved first line regimen commonly used in Ethiopia.
In our study, 4 (9.8%) study subjects harbored Q151M, multi NRTI resistance mutation, which is known to cause high level resistance to AZT, D4T, DDI, ABC and low level resistance to 3TC, FTC, TDF.57,58 The detection of Q151 complex in the present study might be a big challenge to manage and control HIV/AIDs patients among the ART users in the country, this in turn calls for vigilant monitoring of drug resistance in the area.
Contrary to most earlier reports,59 Y188D was detected in low frequency (2–4%) among all the genotyped viraemic samples in this study as NNRTI associated mutation. This might require further investigation to confirm its significance as NNRTI associated resistance mutation in the study area in particular, and in Ethiopia in general.
In our study, residence type, immunological status and viral load of the study participants were found to be independent predictors of acquired drug resistance mutation in multivariate logistic analysis. In this study, unlike several research findings, age was not significantly associated with drug resistance mutations in multivariate analysis.60
Higher viral load (> 3.7 log copies/mL) showed strong correlation with acquired drug resistance mutations in this study. It is well established fact that high viral load had strong correlation with acquired drug resistance mutation.60–62 Hence, World Health Organization recommendation of switching to second line ART after 2 consecutive viral loads of ≥5000 copies/mL, appeared to be the most appropriate strategy.63 Although immunological failure seems inferior to confirm development of drug resistance, it has been found to be associated with both virological failure and drug resistance mutations.63
In the current study, rural patients were significantly more likely to have higher rates of NRTI and NNRTI resistance mutations, compared to the urban dwellers (aOR 2.37; 95% CI: 1.62–9.10, P= 0.05). This is similar to a recent study conducted in South Africa comparing urban and rural HIV treatment programs, reported that the rural group were more likely to have high rate of drug resistance mutations (88.8%, vs 64.1%) than the urban inhabitants.64 According to the authors, the prevalence of acquired drug resistance mutations in adults with first-line therapy failure differed between the urban and rural sites. Several reasons might be suggested to this differential prevalence of drug resistance mutation between the urban and rural groups. The current study site is one of the poorest area in road access and other infrastructures, hence, rural dwellers faces transportation problem to access the health facilities, and higher stigma than the urban inhabitants.
Conclusion and Recommendation
The degree of HIV-1 virological failure (18.6%) and acquired drug resistance mutations acquired drug resistance (85.4%) detected from the current study conducted in South Omo, Ethiopia, were similar with global reports found from other resource limited countries. High virological failure was observed among participants diagnosed with opportunistic infections, active tuberculosis, immunological failures and poor treatment adherence. Similarly, rural residents, having a high viral load and immunological failures were more prone to develop acquired drug resistance HIV-1 mutants. Hence, special attention should be given to those who developed opportunistic infections including active tuberculosis, poor treatment adherence, and immunologically failed individuals for better ARV treatment outcomes. In addition, ART service providers should give special attention to the rural residents and with viral load of ≥ 5000 copies per mL. We would also recommend that, at the very least, viral load measurements and genotypic drug resistance testing should be in place to inform the timely switch to second line treatment in case of virological failures. This will improve the quality of HIV/AIDS care and treatment program in Ethiopia. This study also highlights the utility of high-throughput sequencing in a relatively low resource limited settings for deep HIV genotyping and analysis of drug resistance mutation.
Abbreviations
AIDS, Acquired immune deficiency syndrome; DRMs, drug-resistance mutations; ADR, Acquired Drug Resistance; ART, Antiretroviral Therapy; cDNA, complementary DNA; NRTI, Nucleoside Reverse Transcriptase Inhibitor; NNRTI, Non-Nucleoside Reverse Transcriptase Inhibitor; RT, Reverse Transcriptase; RT-PCR, Real Time Polymerase Chain Reaction; CRF, Circulating Recombinant Form.
Data Sharing Statement
The nucleotide sequences discussed in this study were deposited into National Centre for Biotechnology Information (NCBI) GenBank under accession numbers MG570974-MG571084.
Consent for Publication
Not applicable, as the manuscript does not contain data from any individual person.
Acknowledgments
We are very grateful to all study participants and health professionals working in South Omo, Ethiopia. We also acknowledged Addis Ababa University and National Institute of Health/H3Africa are for sponsoring the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was obtained from National Institute of Health (NIH), under H3Africa program (grant no: U01HG007472-01). The funding body did not have any role in the design of the study, collection, analysis or interpretation of the data.
Disclosure
Rembert Pieper is an employee of Janssen Biopharma. The authors declare that they have no other potential conflicts of interest for this work.
References
1. World Health Organization. HIV Drug Resistance Report 2019. Geneva, Switzerland: World Health Organization; 2019. 2019 (WHO/CDS/ HIV/19.21). Licence: CC BY-NC-SA 3.0 IGO.
2. Gupta RK, Shafer RW, Ndembi N. Global epidemiology of drug resistance after failure of WHO recommended first-line regimens for adult HIV-1 infection: a multicentre retrospective cohort study. Lancet Infect Dis. 2016;16(5):565–575. doi:10.1016/S1473-3099(15)00536-8
3. EFMH. National Guidelines for Comprehensive HIV Prevention, Care and Treatment. Addis Ababa, Ethiopia: Federal Ministry of Health(FMOH); 2014.
4. EPHI. HIV Related Estimates and Projections for Ethiopia–2017. Addis Ababa, Ethiopia: Ethiopian Public Health Institute; 2017.
5. Barnabas G, Sibhatu M, Berhane Y. Antiretroviral therapy program in Ethiopia benefits from virology treatment monitoring. Ethiop J Health Sci. 2017;27(1):1–2. doi:10.4314/ejhs.v27i1.1S
6. Abdissa A, Yilma D, Fonager J, et al. Drug resistance in HIV patients with virological failure or slow virological response to antiretroviral therapy in Ethiopia. BMC Infect Dis. 2014;14:181. doi:10.1186/1471-2334-14-181
7. Mulu A, Liebert UG, Maier M. Virological efficacy and immunological recovery among Ethiopian HIV-1 infected adults and children. BMC Infect Dis. 2014;14:28. doi:10.1186/1471-2334-14-28
8. Mulu A, Maier M, Liebert UG. Low incidence of HIV-1C acquired drug resistance 10 years after roll-out of antiretroviral therapy in Ethiopia: a prospective cohort study. PLoS One. 2015;10(10):e0141318. doi:10.1371/journal.pone.0141318
9. Abegaz W. Genomic characterization of HIV-1 isolates from Ethiopian patients: baseline studies on antiretroviral drug resistance and sub-type variations. A Thesis Submitted to the school of Graduate Studies of the Addis Ababa University in Partial Fulfillment of the Requirement for the Degree of Doctor of Philosophy in Medical Microbiology, Addis Ababa, Ethiopia. 2011.
10. Ssemwanga D, Lihana RW, Ugoji C, et al. Update on HIV-1 acquired and transmitted drug resistance in Africa. AIDS Rev. 2015;17(1):3–20.
11. Lo Presti A, Farcomeni S, Fontanelli Sulekova L, et al. Characterization of HIV-1 subtypes among south Sudanese patients. AIDS Res Hum Retroviruses. 2019;35(10):968–971. doi:10.1089/aid.2019.0133
12. Giovanetti M, Ciccozzi M, Parolin C, Borsetti A. Molecular epidemiology of HIV-1 in African countries: a comprehensive overview. Pathogens. 2020;9(12):1072. doi:10.3390/pathogens9121072
13. Parikha UM, McCormicka K, Zylb GV, Mellorsa JW. Future technologies for monitoring HIV drug resistance and cure. Curr Opin HIV AIDS. 2017;12:182–189. doi:10.1097/COH.0000000000000344
14. Lapointe HR, Dong W, Lee GQ, et al. HIV drug resistance testing by high-multiplex “wide” sequencing on the miseq instrument. Antimicrob Agents Chemother. 2015;59(11):6824–6833. doi:10.1128/AAC.01490-15
15. Simen B, Simons JF, Hullsiek K, et al. Low-abundance drug-resistant viral variants in chronically HIV-infected, antiretroviral treatment-naive patients significantly impact treatment outcomes. J Infect Dis. 2009;199:693–701. doi:10.1086/596736
16. Lataillade M, Chiarella J, Yang R, et al. Prevalence and clinical significance of HIV drug resistance mutations by ultra-deep sequencing in antiretroviral-naive subjects in the CASTLE study. PLoS One. 2010;5:e10952. doi:10.1371/journal.pone.0010952
17. Huber M, Metzner KJ, Geissberger FD, et al. MinVar: a rapid and versatile tool for HIV-1 drug resistance genotyping by deep sequencing. J Virol Methods. 2017;240:7–13. doi:10.1016/j.jviromet.2016.11.008
18. Mohamed S, Penaranda G, Gonzalez D, et al. Comparison of ultra-deep versus Sanger sequencing detection of minority mutations on the HIV-1 drug resistance interpretations after virological failure. AIDS. 2014;28(9):1315–1324. doi:10.1097/QAD.0000000000000267
19. Ode H, Matsuda M, Matsuoka K, et al. Quasispecies analyses of the HIV-1 near-full-length genome with illumina MiSeq. Front Microbiol. 2015;6:1258. doi:10.3389/fmicb.2015.01258
20. Thys K, Verhasselt P, Reumers J, Verbist M, Maes B, Aerssens J. Performance assessment of the Illumina massively parallel sequencing platform for deep sequencing analysis of viral minority variants. J Virol Methods. 2015;221:29–39. doi:10.1016/j.jviromet.2015.04.022
21. Verbist B, Clement L, Reumers J, et al. ViVaMBC: estimating viral sequence variation in complex populations from illumina deep-sequencing data using model-based clustering. BMC Bioinf. 2015;16(1). doi:10.1186/s12859-015-0458-7
22. Ram D, Leshkowitz D, Gonzalez D, Forer R, Levy I, Chowers M. Evaluation of GS Junior and MiSeq next-generation sequencing technologies as an alternative to Trugene population sequencing in the clinical HIV laboratory. J Virol Methods. 2015;212(212):12–16. doi:10.1016/j.jviromet.2014.11.003
23. UNDP-EUE. Preliminary examination of major factors affecting subsistence economy of South Omo Zone and Konso special wereda in South-western Ethiopia” UNDP-EUE Report, May 1996. 1996.
24. CSA. Ethiopia-population and housing census of 2007. Central statistics agency -Ministry of Finance and Economic Development 2007; ETH_PHC-v01_M, Addis Ababa, Ethiopia; 2007.
25. Barth RE, van der Loeff MF, Schuurman R, Hoepelman AI, Wensing AM. Virological follow-up of adult patients in antiretroviral treatment programmes in sub-Saharan Africa: a systematic review. Lancet Infect Dis. 2010;10(3):155–166. doi:10.1016/S1473-3099(09)70328-7
26. QIAGEN. QIAamp® viral RNA mini handbook for purification of viral RNA from plasma, serum, cell-free body fluids, and cell-culture supernatants. 2014.
27. Kozich JJ, Westcott SL, Baxter NT, Highlander SK, Schloss PD. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Appl Environ Microbiol. 2013;79:5112–5120. doi:10.1128/AEM.01043-13
28. Liu T, Shafer R. Web resources for HIV type 1 genotypic-resistance test interpretation. Clin Infect Dis. 2006;42(11):1608–1618. doi:10.1086/503914
29. Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: molecular evolutionary genetics analysis version 6.0. Mol Biol Evol. 2013;30(12):2725–2729. doi:10.1093/molbev/mst197
30. Rhee S, Gonzales M, Kantor R, Betts B, Ravela J, Shafer R. Human immunodeficiency virus reverse transcriptase and protease sequence database. Nucleic Acids Res. 2003;31:298–303. doi:10.1093/nar/gkg100
31. Barennes H, Guillet S, Limsreng S, et al. Virological failure and HIV-1 drug resistance mutations among naive and antiretroviral pre-treated patients entering the ESTHER program of Calmette Hospital in Cambodia. PLoS One. 2014;9(8):e105736. doi:10.1371/journal.pone.0105736
32. Saitou N, Nei M. The neighbor-joining method: a new method for reconstructing phylogenetic trees. Mol Biol Evol. 1987;4:406–425.
33. Wensing AM, Calvez V, Gunthard HF, et al. 2017 update of the drug resistance mutations in HIV-1. Top Antivir Med. 2017;24(4):132–133.
34. Abebe A, Kuiken C, Goudsmit J, et al. HIV type 1 subtype C in Addis Ababa, Ethiopia. AIDS Res Hum Retroviruses. 1997;13:1071–1075. doi:10.1089/aid.1997.13.1071
35. Amogne W, Bontell I, Grossmann S, et al. Phylogenetic analysis of Ethiopian HIV-1 subtype C near full-length genomes reveals high intrasubtype diversity and a strong geographical cluster. AIDS Res Hum Retroviruses. 2016;32(5):471–474. doi:10.1089/aid.2015.0380
36. Mulu A, Lange T, Liebert U, Maier M. Clade homogeneity and Pol gene polymorphisms in chronically HIV-1 infected antiretroviral treatment naive patients after the roll out of ART in Ethiopia. BMC Infect Dis. 2014;1(158):1–9.
37. Tully D, Wood C. Chronology and evolution of the HIV-1 subtype C epidemic in Ethiopia. AIDS. 2010;24(10):1577–1582. doi:10.1097/QAD.0b013e32833999e1
38. Abar A, Jlizi A, Darar H, et al. Human immunodeficiency virus type 1 in Djibouti. Arch Inst Pasteur Tunis. 2012;89(1):33–37.
39. Etta EM, Mavhandu L, Manhaeve C, et al. High level of HIV-1 drug resistance mutations in patients with unsuppressed viral loads in rural northern South Africa. AIDS Res Ther. 2017;14(1):36. doi:10.1186/s12981-017-0161-z
40. Stadeli K, Richman D. Rates of emergence of HIV drug resistance in resource-limited settings: a systematic review. Antivir Ther. 2013;18(1):115–123. doi:10.3851/IMP2437
41. Ndahimana J, Riedel D, Mwumvaneza M, et al. Drug resistance mutations after the first 12 months on antiretroviral therapy and determinants of virological failure in Rwanda. Trop Med Int Health. 2016;21(7):928–935. doi:10.1111/tmi.12717
42. de Mulder M, Yebra G, Navas A, de Jose M, Gurbindo M, Gonzalez-Tome M. High drug resistance prevalence among verticallyHIV-infected patients transferred from pediatric care to adult units in Spain. PLoS One. 2012;7(12):e52155. doi:10.1371/journal.pone.0052155
43. Karadea S, Chaturbhuja D, Senb S, et al. HIV drug resistance following a decade of the free antiretroviral therapy programme in India: a review. Int J Infect Dis. 2018;66:33–41. doi:10.1016/j.ijid.2017.10.020
44. Rhee SY, Jordan MR, Raizes E, et al. HIV-1 drug resistance mutations: potential applications for point-of-care genotypic resistance testing. PLoS One. 2015;10(12):e0145772. doi:10.1371/journal.pone.0145772
45. Sinha R, Shekhar H, Ahmed N, et al. Prevalence of HIV drug resistance mutation in the Northern Indian population after failure of the first line antiretroviral therapy. Curr HIV Res. 2012;10(6):532–538.
46. Hamers RL, Sigaloff KC, Wensing AM, et al. Patterns of HIV-1 drug resistance after first-line antiretroviral therapy (ART) failure in 6 sub-Saharan African countries: implications for second-line ART strategies. Clin Infect Dis. 2012;54(11):1660–1669. doi:10.1093/cid/cis254
47. Ibe S, Sugiura W. Clinical significance of HIV reverse-transcriptase inhibitor-resistance mutations. Future Microbiol. 2011;6(3):295–315. doi:10.2217/fmb.11.7
48. Sharma A, Singh T, Devi KR, Singh L. Prevalence of drug resistance associated mutations among the anti retroviral therapy exposed HIV-1 infected individuals in Manipur, Northeast India. Curr HIV Res. 2016;14(4):360–370. doi:10.2174/1570162X14666160401131426
49. Metznera K, Raucha P, Braunc P, et al. Prevalence of key resistance mutations K65R, K103N, and M184V as minority HIV-1 variants in chronically HIV-1 infected, treatment-naïve patients. J Clin Virol. 2011;50:156–161. doi:10.1016/j.jcv.2010.10.001
50. Kuritzkes DR, Quinn JB, Benoit SL. Drug resistance and virologic response in NUCA 3001, a randomized trial of lamivudine (3TC) versus zidovudine (ZDV) versus ZDV plus 3TC in previously untreated patients. AIDS. 1996;10(9):975–981. doi:10.1097/00002030-199610090-00007
51. Larder BA, Kemp SD. Multiple mutations in HIV-1 reverse transcriptase confer high-level resistance to zidovudine (AZT). Science. 1989;246(4934):1155–1158. doi:10.1126/science.2479983
52. Kellam P, Boucher CA, Larder BA. Fifth mutation in human immunodeficiency virus type 1 reverse transcriptase contributes to the development of high-level resistance to zidovudine. Proc Natl Acad Sci U S A. 1992;89(5):1934–1938. doi:10.1073/pnas.89.5.1934
53. Harrigan PR, Kinghorn I, Bloor S, et al. Significance of amino acid variation at human immunodeficiency virus type 1 reverse transcriptase residue 210 for zidovudine susceptibility.. J Virol. 1996;70(9):5930–5934. doi:10.1128/jvi.70.9.5930-5934.1996
54. Whitcomb JM, Parkin NT, Chappey C, Hellman NS, Petropoulos CJ. Broad nucleoside reverse-transcriptase inhibitor cross-resistance in human immunodeficiency virus type 1 clinical isolates.. J Infect Dis. 2003;188(7):992–1000. doi:10.1086/378281
55. Bacheler L, Anton E, Kudish P, et al. Human immunodeficiency virus type 1 mutations selected in patients failing efavirenz combination therapy. Antimicrob Agents Chemother. 2000;44(9):2475–2484. doi:10.1128/AAC.44.9.2475-2484.2000
56. Zhang Z, Xu W, Koh Y, et al. A novel nonnucleoside analogue that inhibits human immunodeficiency virus type 1 isolates resistant to current nonnucleoside reverse transcriptase inhibitors. Antimicrob Agents Chemother. 2007;51(2):429–437. doi:10.1128/AAC.01032-06
57. Melikian G, Rhee S, Taylor J, et al. Standardized comparison of the relative impacts of HIV-1 reverse transcriptase (RT) mutations on nucleoside RT inhibitor susceptibility. Antimicrob Agents Chemother. 2012;56(5):2305–2313. doi:10.1128/AAC.05487-11
58. Margot N, Johnson A, Miller M, Callebaut C. Characterization of HIV-1 resistance to tenofovir alafenamide in vitro. Antimicrob Agents Chemother. 2015;59(10):5917–5924. doi:10.1128/AAC.01151-15
59. Mascolini M, Richman D, Larder B, Mellors J, Boucher CA. Clinical implications of resistance to antiretrovirals: new resistance technologies and interpretations. Antivir Ther. 2008;13:319–334.
60. Hassan AS, Nabwera HM, Mwaringa SM, et al. HIV-1 virologic failure and acquired drug resistance among first-line antiretroviral experienced adults at a rural HIV clinic in coastal Kenya: a cross-sectional study. AIDS Res Ther. 2014;11(1):9. doi:10.1186/1742-6405-11-9
61. Goldman JD, Cantrell RA, Mulenga LB. Simple adherence assessments to predict virologic failure among HIV-infected adults with discordant immunologic and clinical responses to antiretroviral therapy. AIDS Res Hum Retroviruses. 2008;24(8):1031–1035. doi:10.1089/aid.2008.0035
62. Assoumou L, Descamps D, Yerly S. Prevalence of HIV-1 drug resistance in treated patients with viral load >50 copies/mL in 2009: a French nationwide study.. J Antimicrob Chemother. 2013;66(6):1400–1405. doi:10.1093/jac/dkt033
63. Boulle C, Kouanfack C, Laborde-Balen G. Prediction of HIV drug resistance based on virologic, immunologic, clinical, and /or adherence criteria in the stratall ANRS 12110/ESTHER trial in Cameroon. Clin Infect Dis. 2013;57(4):604–607. doi:10.1093/cid/cit323
64. Rossouw TM, Nieuwoudt M, Manasa J, et al. HIV drug resistance levels in adults failing first-line antiretroviral therapy in an urban and a rural setting in South Africa. HIV Med. 2017;18(2):104–114. doi:10.1111/hiv.12400
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.