Back to Journals » Risk Management and Healthcare Policy » Volume 14
Generic Logic Model for Coronavirus Disease-2019 Responses Based on the South Korean Experience
Authors Chun H ![]() , Yoon K
, Yoon K ![]() , Kim H, Cheon E, Ha J, Tak S, Cho S
, Kim H, Cheon E, Ha J, Tak S, Cho S ![]()
Received 3 September 2021
Accepted for publication 18 November 2021
Published 25 November 2021 Volume 2021:14 Pages 4765—4774
DOI https://doi.org/10.2147/RMHP.S336425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Hae-ryoung Chun,1 Kyuhyun Yoon,2 Hana Kim,1 Eunsil Cheon,1 Jaeyoung Ha,1 Sangwoo Tak,2 Sung-il Cho1
1Graduate School of Public Health, Seoul National University, Seoul, 08826, Republic of Korea; 2Institute of Health & Environment, Seoul National University, Seoul, 08826, Republic of Korea
Correspondence: Sung-il Cho
Graduate School of Public Health, Seoul National University, 1 Gwanak-ro, Gwanak-gu, Seoul, 08826, Republic of Korea
Email [email protected]
Background: As the global coronavirus disease-2019 (COVID-19) pandemic continues, many countries have implemented public health policies, such as lockdowns and physical distancing measures, to prevent its spread. South Korea’s response to COVID-19, which prevented an increase in confirmed cases and increased resilience, has been considered very effective.
Purpose: To analyze Korea’s response to COVID-19 in 2020 and develop a logic model to evaluate performance effectiveness in follow-up studies.
Methods: By content analysis of Korea Disease Control and Prevention Agency (KDCA) press releases, we defined the problems and identified the causes of the health and social effects of the COVID-19 outbreak. Next, we created a problem tree and developed a logic model that comprised inputs, activities, outputs, outcomes, and impacts. Finally, we held expert consultations to obtain expert opinions regarding the logic model and to ensure the model’s validity.
Results: South Korea’s COVID-19 response policy mitigated the social and health impacts. The 2020 COVID-19 responses had four outcomes (identifying cases on time, preventing transmission of coronavirus infection, effective treatment of COVID-19 cases, protecting public resilience and well-being) and 12 outputs; South Korea conducted 32 activities.
Conclusion: The results can be a practical reference for managing problems faced in other countries. Korean policy may be of interest in the future for international decision-makers in charge of policy enforcement and those who may be called on to respond to new infectious diseases.
Keywords: COVID-19 pandemic, public health policy, logical framework
Introduction
On January 30, 2020, the World Health Organization (WHO) declared coronavirus disease-2019 (COVID-19), a disease of the respiratory tract characterized by a severe acute respiratory syndrome,1 to be a public health emergency of international concern.2 As of December 31, 2020, a total of 82,357,480 cases of COVID-19 was reported, causing 1,802,390 deaths.3 Because of the pandemic, various standards and measures to control the spread of the disease have been adopted worldwide. Many countries have implemented lockdowns and physical distancing measures to prevent the spread of COVID-19, while also working to protect mental health from the effects of the resulting economic crisis.4 This is because the mental health of older adults5 and young people6 is particularly threatened by physical distancing, school closures, and job loss; they are experiencing economic and organizational difficulties7 related to COVID-19. Many countries are attempting to manage mental health problems by providing online counseling and psychological support services;8 online platforms are also actively used in medical services9 for people in need of mental health services and subsidies. In addition, the importance of crisis communication is clear10 in response to growing public fear and distrust in the early stages of COVID-19, particularly concerning fake news and infodemics.11,12 It is important to prevent the spread of COVID-19 and to protect well-being.
SouthKorea’s response to COVID-19, which prevented an increase in confirmed cases and improved resilience, has been considered very effective. The South Korean government implemented diagnostic tests, epidemiological investigations, contact tracing and follow-up, and isolated treatment.13 As a result of such an effective response, the excess death rate due to COVID-19 in Korea has not deviated significantly from the mortality trend in the last 3 years.14 In particular, Korea’s Disaster Emergency Support Subsidy,15 which positively affected low-income households, and psychological counseling reduced the negative social effects of COVID-19. In addition, the KDCA has made efforts to deliver accurate information to the public by identifying incorrect information related to COVID-19.16 Also, South Korea’s economy has contracted only slightly (−1%), and is likely to be the smallest GDP slump among the Organization for Economic Co-operation and Development countries in the pandemic year.17 Compared with the same month in 2019, the overall suicide mortality decreased in 2020, except for increases of 0.6% in February, 1.8% in June, and 0.7% in August.18
Due to the characteristics of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the inability to diagnose and treat promptly could negatively impact physical health and well-being. A logic model intuitively represents the elements and processes necessary to respond to COVID-19; it enables advance determination of countermeasures to be taken. The logic model can structure the main strategies to achieve the effect and the policy implementation process19 in a single table. Moreover, it shows which conditions lead to specific outcomes and can assist in evaluating the effectiveness of policies.20,21 A logic model visualizes the inputs, activities, outputs, and outcomes required to achieve an effect. Most research on policy evaluation focuses on the relationship between the independent and dependent variables, leaving various factors affecting policy unaccounted for, thus preventing explanation of the transition from intervention to outcome. The logic model describes the policy process openly by setting out and analyzing the policy components.22 The logic model is a framework developed for monitoring and evaluating performance. Before making a logic model, problem analysis using a problem tree, solution, or objectives analysis should be done. Problem trees can determine the root causes of the main problem, identify the overall picture of problems,23 and suggest solutions.24 We analyzed South Korea’s COVID-19 response in 2020 and developed a logic model to evaluate its performance effect in subsequent studies.
Materials and Methods
Content Analysis for Problem Definition
The data sources in this study were the “Seoul COVID-19 Report,” published by the Seoul Metropolitan Government, and daily press releases by KDCA from January 3rd to December 31st, 2020; data were collected between October 2020 and December 2020. To identify the categories of response activities, a content analysis was conducted in three steps—preparation, organization, and reporting.25 In the preparation phase, we reviewed the source documents and established the unit of analysis as the keywords of sentences that described the response activities. In the organization phase, we identified a total of 409 activities from the source documents and extracted the keywords from those activities. Next, we grouped the keywords into 20 categories. In the reporting phase, we labeled the categories according to the problems encountered, as indicated by the keywords. The relationships among problem categories were assessed and a problem tree was formulated.
From Problem Tree to Logic Model
Creation of the Problem Tree
A problem tree and logic model were developed based on the problem context and categories of activities. A problem tree is a conceptual map that functions via content analysis and problem categorization.25 This is the result of overlapping between the content reporting and problem analysis phases. The problem tree that shows the relationships of the problems is shown in Figure 1.
Development of the Logic Model
The categories were mapped to the six topics described above. The key policy classification items were listed according to test, tracing, treatment, physical distancing, communication, and resilience categories, identified by reference to the policy classification items of the Seoul COVID-19 Report. After brainstorming sessions with researchers, the categories were grouped into four significant outcomes according to purpose: identifying cases in a timely manner, preventing transmission of coronavirus infection, effective treatment of COVID-19 cases, and protecting public resilience and well-being. One main impact was selected by grouping these outcomes. In Supplementary Table 1, the activities implemented in Korea are in the left column; inputs needed to implement those activities are in the right column. In addition, we present WHO’s indicators to monitor healthcare capacity and utilization for decision-making regarding COVID-19.26 The other outcome indicators refer to the Monitoring and Evaluation Framework Report of the WHO.27
Expert Consultation
We held expert consultations to obtain expert opinions concerning the logic model and to ensure its validity. We formed an expert group that consisted of one infectious disease expert, one health policy analyst, one international development cooperation expert, and five global health experts. The consultation committee had one online meeting and four offline meetings to review the contents and flow of the logic model, as well as the configuration of indicators.
Results
Problem Tree
In South Korea from January to March, problems (lack of equipment related to preventing the spread of infectious diseases and difficulty in management, shortage of human resources and facilities for quarantine, difficulties in implementing and managing physical distancing measures, delayed diagnosis, quarantine difficulty) presented in the problem tree (Figure 1, bottom) occurred. Each of these problems was likely to result in unclear case identification, the uncontrolled transmission of coronavirus infections, ineffective treatment of COVID-19 cases, and a decrease in public resilience and well-being. Ultimately, COVID-19 could have health and social effects. Epidemiological investigation and contact tracing were quickly implemented in South Korea because systems and technologies were established. By a revision of the Act on the Prevention and Management of Infectious Diseases, personal information was available for epidemiological investigation in the event of an epidemic. However, because this problem can potentially be encountered abroad, we presented it in the problem tree. In South Korea, even in the early stages of the COVID-19 pandemic, epidemiological investigations and contact tracing were efficient, enabling isolation and management of suspected patients, thereby suppressing the spread of the disease.28
 |
Figure 1 Problem tree. Notes: *Although this tracing problem can potentially occur in other countries, South Korea did not have problems after the early days of the COVID-19 pandemic. |
Results of the Logic Model
We drew the logic model (Table 1) to present the inputs, activities, output, outcome, and impact mechanisms. By classifying 2020 response policies into four outcomes (Identifying cases in a timely manner, preventing transmission of coronavirus infection, effective treatment of COVID-19 cases, protecting public resilience and well-being), we identified factors that contributed to minimizing the harmful physical and social effects of COVID-19. The outputs (two to four per outcome) are listed in Table 1. Activities carried out to achieve the outcomes, as well as the 12 outputs, are listed in Table 1. Only the input types are listed in Table 1; the details of the input required for the activity are provided in Supplementary Table 1. Input consists of resources and a system. Resources include human resources, equipment related to preventing infectious diseases, budget, and infrastructure (Supplementary Table 1). Items classified by the system are preconditions for input and activity, including legal and technical aspects.
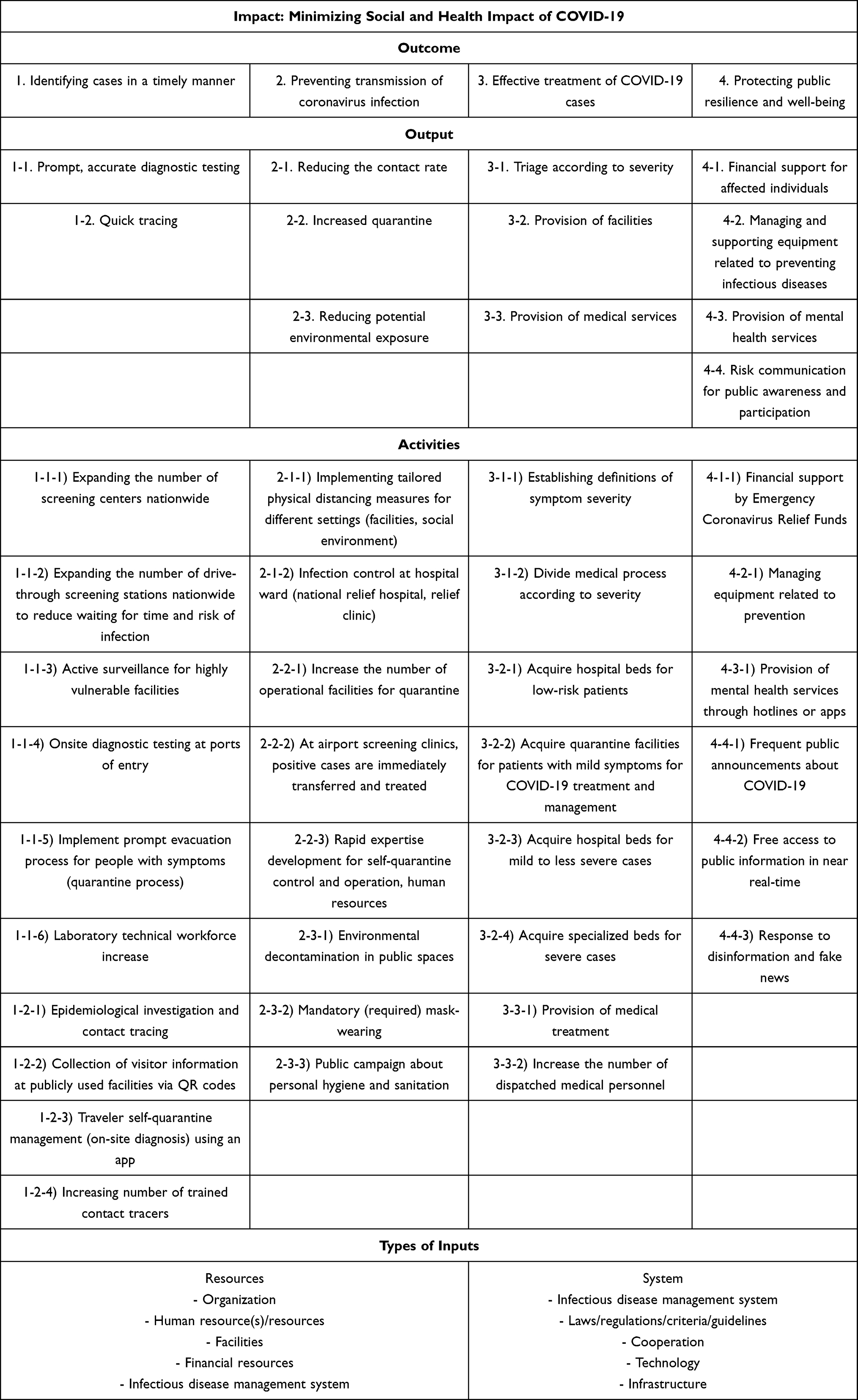 |
Table 1 Logic Model for COVID-19 Responses: Impact, Outcome, Output, and Activities Based on the National Experience of South Korea |
Activities Performed to Achieve the First Outcome (Identifying Cases in a Timely Manner)
Prompt, accurate diagnostic testing (1–1 output) and quick tracing (1–2 output) are needed to identify cases in a timely manner (first outcome). The activities in Korea were as follows. First, we expanded the number of screening centers nationwide ((1-1-1) activities) and drive-through screening centers to reduce the waiting time (1-1-2) activities) and risk of infection. In addition, we actively monitored vulnerable facilities ((1-1-3) activities) and conducted on-site diagnostic tests at ports of entry ((1-1-4) activities). We implemented an immediate evacuation process for people with symptoms ((1-1-5) activities) and increased the laboratory technical workforce (1-1-6) activities). We performed an epidemiological investigation and contact tracing ((1-2-1) activities) and collected visitor information ((1-2-2) activities) to improve contact tracing (1–2 output). In addition, we managed traveler self-quarantine using an app (1-2-3) activities) and increased the number of trained contact tracers ((1-2-4) activities).
Activities Performed to Achieve the Second Outcome (Preventing Transmission)
To prevent the transmission of SARS-CoV2 infection (second outcome), we should reduce the contact rate (2–1 output), increase quarantine (2–2 output), and reduce potential environmental exposure (2–3 output). To this end, the activities in Korea were as follows. Physical distancing ((2-1-1) activities) in different settings (facilities, social environment) and sufficient operational facilities for quarantine ((2-2-1) activities) are needed to prevent further virus transmission. In addition, mask-wearing ((2-3-2) activities) should be mandated, and environmental decontamination should be implemented in public spaces ((2-3-3) activities).
Activities Performed to Achieve the Third Outcome (Effective Treatment of COVID-19 Cases)
For effective treatment (third outcome), triage according to severity (3–1 output) must be in place, facilities must be in place (3–2 output), and medical services (3–3 output) must be available. We established definitions of symptom severity ((3-1-1) activities) and divided medical processes based on severity ((3-1-2) activities). In addition, we acquired sufficient patient beds according to severity ((3-2-1), 2), 3) activities). Also, we increased the number of dispatched medical personnel ((3-3-2) activities).
Activities Performed to Achieve the Fourth Outcome (Enhancing Public Resilience and Well-Being)
To protect public resilience and well-being (fourth outcome), financial (4–1 output) support by Emergency Coronavirus Relief Funds and mental services (4–3 output) were provided, accurate information and knowledge related to COVID-19 was reported, and communication with citizens was conducted (4–4 output). In addition, Korea managed equipment related to preventing infectious diseases (4–2 output). We made frequent public announcements about COVID-19 ((4-4-1) activities) and made it accessible in near-real-time ((4-4-2) activities). In addition, accurate information was delivered by the response to fake news ((4-4-3) activities).
Logic Model for South Korea’s COVID-19 Responses: Indicators
We presented objective indicators that can be used to analyze policy effectiveness (Table 2). To evaluate confirmed cases, there is a need to know the time from exposure to confirmation, as well as the positivity rate. As an indicator of coronavirus transmission, the number of new confirmed cases per week must be determined, along with the decrease in movement according to the level of physical distancing. To evaluate the effectiveness of treatment of COVID-19 cases, the total number of COVID-19 admissions and discharges must be recorded, along with determination of mortality and excess mortality. Mechanisms must be in place to collect community feedback for assessment of public resilience and protection of well-being; this information must be provided to the community. Additionally, sufficient economic growth is needed to ensure adequate financial support for affected individuals.
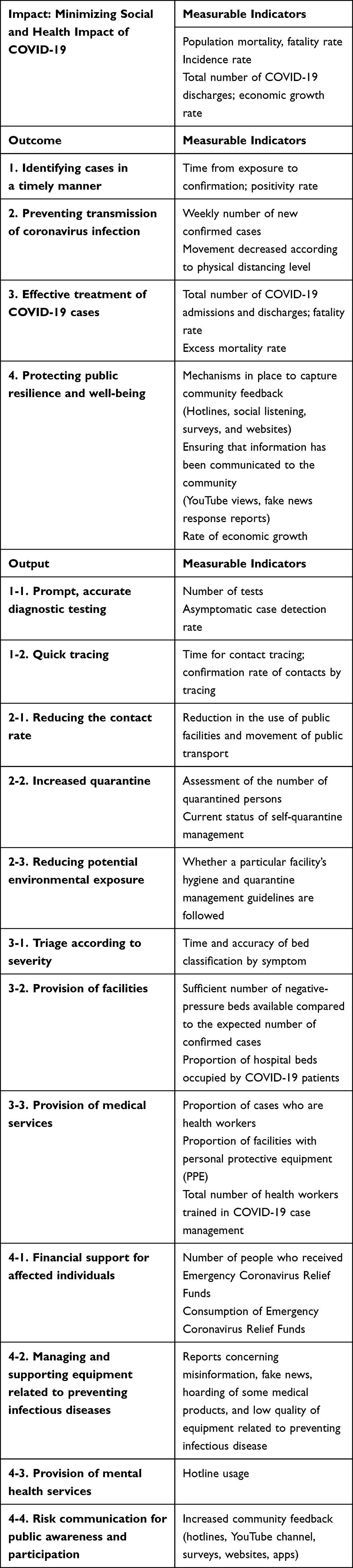 |
Table 2 Logic Model for COVID-19 Responses: Indicators Based on the National Experience of South Korea |
Discussion
In the logic model, we presented the 3T, physical distancing, and resilience policy in response to COVID-19. In addition, we analyzed the problems caused by the COVID-19 epidemic using a problem tree. Previous studies introduced 3T (testing, tracing, treatment) and physical distancing in the epidemic phase;13 they explained that policies could prevent negative social effects.29 Unlike previous studies13,29 that introduced detailed situations and responses on a small scale, the present report discusses the activities performed on a large scale in response to COVID-19 and the input that should be prepared first.
Preemptive testing for vulnerable high-risk groups (such as religious gatherings, senior care facilities, and correctional facilities)30 and on-site diagnostic testing at ports of entry31 were conducted on a large scale in a short time. The tests increased the positivity rate and prevented the early spread of COVID-19. In addition, we quickly identified cases by introducing new testing methods with reduced contact, such as drive-through and walk-through, and a temporary screening center where anyone who wanted to be tested could be tested. In addition, with the introduction of quick response code-based entry logs in publicly used facilities, the number of contact-traced cases increased significantly.32
Maintenance of personal hygiene, reduced time away from home, and avoidance of large gatherings strengthens physical distancing.33 As the epidemic became severe, the physical distancing level increased, and subway use in Seoul decreased.34 In addition, the transmission of COVID-19 infection was prevented by mandatory face masks in public facilities, along with prevention and control measures.35 Effective treatment was implemented by classifying patients,36 assigning beds, securing available beds according to symptoms, and securing personnel and supplies.37 As a result, the excess mortality rate did not significantly change, compared with 2019.38
Compared with 2019, sales rose after payments to all citizens from the first COVID-19 relief fund, thus contributing to the economic crisis in 2020.39 Most of the COVID-19 relief fund was used within the expiration date and was used for living expenses. In an online poll of COVID-19-related news, the COVID-19 relief fund ranked second and was regarded as a practically helpful economic policy.
Citizen satisfaction is associated with public trust in government in South Korea.40 Citizen opinions concerning public policy build support for government policy-making41 and improve government performance.42 Fake news and disinformation about the effectiveness of prevention and treatment of COVID-19 were actively discouraged and prevented.43 The Seoul Metropolitan Government’s YouTube daily briefing functioned as an essential channel for communicating important changes in the prevention and control situation or policy. Citizens were provided with psychological support and could receive welfare services such as emergency support and treatment cost support.44
An indicator of the effectiveness of South Korean COVID-19 response interventions is presented in Table 1. The logic model developed by the United States Centers for Disease Control and Prevention45 focuses on community mitigation but lacks detailed input. The COVID-19 response logic model developed by the WHO46 focuses on the African region. The Strategic Response Plan pillars function as objectives and support the monitoring and evaluation of planned COVID19 response activities. In the Strategic Response Plan report, there is no evaluation indicator for the economic crisis.46
A logic model can be used as a tool to disseminate findings to academic communities and policymakers, as well as funders. This paper shows that the logic model can help people overcome problems by providing a conceptual framework for checking and identifying inputs and activities that must be performed preemptively. It may be challenging to apply Korea’s COVID-19 response logic model to other countries. However, it would enable the identification of inputs necessary for constructive activities. Already-implemented projects were rearranged within the logic model structure; they showed activities and goals in stages. There was not enough time to develop the logic model before implementing the response policy because an immediate and rapid response was needed upon the emergence of COVID-19. We collected information related to the response implemented in 2020 using Gray Documents and press releases by government agencies. Research and development of preventive and therapeutic interventions in response to COVID-19 has been crucial. However, this study did not incorporate the research and development perspective. Scientific research during the pandemic can arise from urgent needs that may challenge conventional guidelines,47 although such research must be conducted safely and in compliance with the Declaration of Helsinki.48 Sufficient discussion and assessment of the role of research and development in the COVID-19 pandemic response should be reflected in future studies involving logic models.
Implications
The COVID-19 pandemic has a marked impact on the economy, society, culture, legislation, mental health, and finance.49 Cooperation with fields other than health is a prerequisite for successful policy implementation. As demonstrated by the logic model, a pandemic response requires comprehensive collaboration of multiple sectors in public health, sociocultural, economic, and legal areas. Our logic model provides potential indicators for the monitoring and evaluation of pandemic responses. Policy effects can only result from combinations of essential activities in proper balance. Furthermore, securing adequate input—the fundamental component of the logic model—with sufficient resources and enabling systems may be the most crucial and pressing need.
Because the context and situation differ among countries, the components included in the logic model can be modified and improved according to the context. For example, as shown in the problem tree, Korea did not experience considerable difficulty in the initial epidemiological investigation because information technology related to the contact-tracing system was established. In some other countries, despite their minimal resources, insufficient healthcare, and weak surveillance system, social media platforms facilitated effective risk communication and public education.50
Conclusion
This study evaluated Korea’s COVID-19 response policy using a logic model consisting of input, activities, output, outcome, and impact. Korea’s active response to COVID-19 in 2020 mitigated the social and health effects of COVID-19 through timely identification, preventing transmission of coronavirus infection, effective treatment, and protecting resilience and well-being. Because we presented indicators that could evaluate future responses to pandemic-prone acute respiratory infections such as COVID-19, this logic model enables activities through numerous inputs; it shows that various activities produce outputs and outcomes. In addition, collaboration for policy implementation is occurring in various fields, including public health. Other countries are expected to implement this logic model for COVID-19 responses according to their particular situations by building inputs and systems. In addition, if policy evaluation using a logic model is implemented, more rapid measures will presumably be taken when responding to new infectious diseases.
Acknowledgment
We are thankful to the advisory committee members for consultation.
Funding
This work was supported by the National Research Foundation of Korea (BK21 Center for Integrative Response to Health Disasters, Graduate School of Public Health, Seoul National University) (No. 4199990514025).
Disclosure
The authors declare that they have no competing interests.
References
1. Berlin I, Thomas D, Le Faou AL, Cornuz J. COVID-19 and smoking. Nicotine Tob Res. 2020;22(9):1650–1652. doi:10.1093/ntr/ntaa059
2. World Health Organization. COVID 19 Public Health Emergency of International Concern (PHEIC). Global research and innovation forum: towards a research roadmap; 2020.
3. World Health Organization. WHO Coronavirus (COVID-19) dashboard. Available from: https://covid19.who.int/.
4. Abbas J. Crisis management, transnational healthcare challenges and opportunities: the intersection of COVID-19 pandemic and global mental health. Res Globalization. 2021;3:100037. doi:10.1016/j.resglo.2021.100037
5. Shuja KH, Aqeel M, Khan EA, Abbas J. Letter to highlight the effects of isolation on elderly during COVID‐19 outbreak. Int J Geriatr Psychiatry. 2020;35(12):1477–1478. doi:10.1002/gps.5423
6. Aqeel M, Abbas J, Shuja KH, et al. The influence of illness perception, anxiety and depression disorders on students mental health during COVID-19 outbreak in Pakistan: a web-based cross-sectional survey. Int J Hum Rights Healthc. 2021. doi:10.1108/IJHRH-10-2020-0095
7. Azizi MR, Atlasi R, Ziapour A, Abbas J, Naemi R. Innovative human resource management strategies during the COVID-19 pandemic: a systematic narrative review approach. Heliyon. 2021;7(6):e07233. doi:10.1016/j.heliyon.2021.e07233
8. Maqsood A, Abbas J, Rehman G, Mubeen R. The paradigm shift for educational system continuance in the advent of COVID-19 pandemic: mental health challenges and reflections. Curr Opin Behav Sci. 2021;2:100011. doi:10.1016/j.crbeha.2020.100011
9. NeJhaddadgar N, Ziapour A, Zakkipour G, Abbas J, Abolfathi M, Shabani M. Effectiveness of telephone-based screening and triage during COVID-19 outbreak in the promoted primary healthcare system: a case study in Ardabil province, Iran. J Public Health. 2020;1–6. doi:10.1007/s10389-020-01407-8
10. Su Z, Wen J, Abbas J, et al. A race for a better understanding of COVID-19 vaccine non-adopters. Brain Behav Immun Health. 2020;9:100159.
11. Su Z, McDonnell D, Wen J, et al. Mental health consequences of COVID-19 media coverage: the need for effective crisis communication practices. Global Health. 2021;17(1):1–8. doi:10.1186/s12992-020-00654-4
12. Tasnim S, Hossain MM, Mazumder H. Impact of rumors and misinformation on COVID-19 in social media. J Prev Med Public Health. 2020;53(3):171–174. doi:10.3961/jpmph.20.094
13. Kang J, Jang YY, Kim J, et al. South Korea’s responses to stop the COVID-19 pandemic. Am J Infect Control. 2020;48(9):1080–1086. doi:10.1016/j.ajic.2020.06.003
14. Statistics Research Institue. KOSTAT Statistics Plus Vol.12 2020.12. winter; 2020.
15. Nam Jae-Hyun LR-H. The influence of COVID-19 economic impact payment on household consumption in South Korea - Focusing on comparison by income classes. Korean J Soc Welf Policy. 2021;48(1):63–95.
16. Song Y, Ko L, Jang SH. The South Korean government’s response to combat COVID-19 misinformation: analysis of “Fact and Issue Check” on the Korea centers for disease control and prevention website. Asia Pac J Public Health. 2021;10105395211014705. doi:10.1177/10105395211014705
17. Lee D, Choi B. Policies and innovations to battle Covid-19–A case study of South Korea. Health Policy Technol. 2020;9(4):587–597. doi:10.1016/j.hlpt.2020.08.010
18. Korean Statistical Information Service. Specific cause of death (intentional self-harm) and the number of deaths by gender/month. 2021.09. Available from: https://kosis.kr/eng/statisticsList/. Acccessed September 30, 2021.
19. Westmoreland H, Lopez E, Rosenberg H. How to develop a logic model for districtwide family engagement strategies. Harvard Family Research Project; 2009:10.
20. Chen HT. Theory-Driven Evaluations. Sage publications; 1990.
21. Renger R, Titcomb A. A three-step approach to teaching logic models. Am J Eval. 2002;23(4):493–503. doi:10.1177/109821400202300409
22. Dyehouse M, Bennett D, Harbor J, Childress A, Dark M. A comparison of linear and systems thinking approaches for program evaluation illustrated using the Indiana Interdisciplinary GK-12. Eval Program Plann. 2009;32(3):187–196. doi:10.1016/j.evalprogplan.2009.03.001
23. USAID. USAID Applying Science to Strengthen and Improve Systems (ASSIST) project; 2020.
24. ESCAP/UNDP/ADB. Achieving the health millennium development goals in Asia and the Pacific; 2007.
25. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
26. World Health Organization. Indicators to monitor health-care capacity and utilization for decision-making on COVID-19; 2020
27. World Health Organization. COVID‑19 Strategic Preparedness and Response (SPRP): monitoring and Evaluation Framework; 2020.
28. Park Y, Huh IS, Lee J, et al. Application of testing-tracing-treatment strategy in response to the COVID-19 outbreak in Seoul, Korea. J Korean Med Sci. 2020;35(45). doi:10.3346/jkms.2020.35.e396.
29. Lim B, Kyoungseo Hong E, Mou J, Cheong I. COVID-19 in Korea: success based on past failure. Asian Econ Pap. 2021;20(2):41–62.
30. Our World in Data. The share of COVID-19 tests that are positive. Available from: https://ourworldindata.org/grapher/positive-rate-daily-smoothed?tab=chart&country=~KOR.
31. Ministry of Health and Welfare. COVID-19 site inspection of overseas immigration (12.17); 2020.
32. Korea Disease Control and Prevention Agency. COVID-19 central disaster and safety countermeasure headquarters regular briefing (11.6.Fri). Available from: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=4013&contSeq=4013&board_id=&gubun=#.
33. Hwang YS, Jo HS. Associations between compliance with non-pharmaceutical interventions and social-distancing policies in Korea during the COVID-19 pandemic. J Prev Med Public Health. 2021;54(4):230. doi:10.3961/jpmph.21.139
34. Park J. Changes in subway ridership in response to COVID-19 in Seoul, South Korea: implications for social distancing. Cureus. 2020;12(4):e7668.
35. Issac A, Stephen S, Jacob J, et al. The pandemic league of COVID-19: Korea versus the United States, with lessons for the entire world. J Prev Med Public Health. 2020;53(4):228. doi:10.3961/jpmph.20.166
36. Kwon YS, Park SH, Kim HJ, et al. Screening clinic for coronavirus disease 2019 to prevent intrahospital spread in Daegu, Korea: a single-center report. J Korean Med Sci. 2020;35(26):e246. doi:10.3346/jkms.2020.35.e246.
37. Planning and Administration Office SPaAO, City Planning Division, Organization Division, Evaluation Division. Seoul COVID-19 Report; 2020.
38. Shin MS, Sim B, Jang WM, Lee JY. Estimation of excess all-cause mortality during COVID-19 pandemic in Korea. J Korean Med Sci. 2021;36(39):e280. doi:10.3346/jkms.2021.36.e280
39. Asian Development Bank. Assessment of COVID-19 response in the Republic of Korea; 2021.
40. Kim S. Public trust in government in Japan and South Korea: Does the rise of critical citizens matter? Public Adm Rev. 2010;70(5):801–810. doi:10.1111/j.1540-6210.2010.02207.x
41. Kweit MG, Kweit RW. Citizen participation and citizen evaluation in disaster recovery. Am Rev Public Adm. 2004;34(4):354–373. doi:10.1177/0275074004268573
42. Neshkova MI, Guo H. Public participation and organizational performance: evidence from state agencies. J Public Adm Res Theory. 2012;22(2):267–288. doi:10.1093/jopart/mur038
43. Choi YS, Ko JY. Operating a national hotline in Korea during the COVID-19 pandemic. Osong Public Health Res Perspect. 2020;11(6):380. doi:10.24171/j.phrp.2020.11.6.06
44. Hyun J, You S, Sohn S, et al. Psychosocial support during the COVID-19 outbreak in Korea: activities of multidisciplinary mental health professionals. J Korean Med Sci. 2020;35(22):e211. doi:10.3346/jkms.2020.35.e211.
45. Centers for Disease Control and Prevention. An approach for monitoring and evaluating community mitigation strategies for COVID-19; 2020.
46. World Health Organization. Monitoring and evaluation framework for the Covid-19 response in the WHO African region; 2020.
47. Su Z, McDonnell D, Cheshmehzangi A, Abbas J, Li X, Cai Y. The promise and perils of Unit 731 data to advance COVID-19 research. BMJ Glob Health. 2021;6(5):e004772. doi:10.1136/bmjgh-2020-004772
48. General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81(3):14–18.
49. Yoosefi Lebni J, Abbas J, Moradi F, et al. How the COVID-19 pandemic effected economic, social, political, and cultural factors: a lesson from Iran. Int J Soc Psychiatry. 2021;67(3):298–300. doi:10.1177/0020764020939984
50. Abbas J, Wang D, Su Z, Ziapour A. The role of social media in the advent of COVID-19 pandemic: crisis management, mental health challenges and implications. Risk Manag Healthc Policy. 2021;14:1917. doi:10.2147/RMHP.S284313
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.