Back to Journals » International Journal of General Medicine » Volume 18
Gender-Specific Next-Generation Sequencing Reveals First Allelic Variation Patterns in Dementia Risk Among Bangladeshis: The CARED Study
Authors Ranjan R ![]() , Yusuf MA
, Yusuf MA ![]() , Uddin MN, Mamun MT, Mamun AA, Kawnayn G, Hakim M
, Uddin MN, Mamun MT, Mamun AA, Kawnayn G, Hakim M
Received 7 August 2025
Accepted for publication 4 October 2025
Published 9 October 2025 Volume 2025:18 Pages 6191—6199
DOI https://doi.org/10.2147/IJGM.S559162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Redoy Ranjan,1,2 Md Abdullah Yusuf,3 Mohammad Nur Uddin,4 Mim Tanzila Mamun,5 Alif Al Mamun,6,7 Ghulam Kawnayn,8 Maliha Hakim4
1Department of Biological Sciences, Royal Holloway University of London, London, UK; 2Department of Cardiac Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh; 3Department of Microbiology, National Institute of Neurosciences and Hospital, Dhaka, Bangladesh; 4Department of Neurology, National Institute of Neurosciences and Hospital, Dhaka, Bangladesh; 5Department of Medicine, Chottogram Army Medical College, Chottogram, Bangladesh; 6Department of Neuroscience, Macquarie University, Sydney, NSW, Australia; 7Department of Education, Southern Cross University, Sydney, Australia; 8Department of Neurology, Combined Military Hospital, Chottogram, Bangladesh
Correspondence: Maliha Hakim, Department of Neurology, National Institute of Neurosciences and Hospital, Dhaka, Bangladesh, Email [email protected]
Background: Alzheimer’s disease (AD) and related dementias exhibit significant gender disparities in prevalence and progression, yet the genetic underpinnings of these differences remain incompletely understood. We aimed to observe gender-specific allelic variation patterns in key dementia susceptibility genes among the Bangladeshi population.
Methods: The Community Awareness and Research on Early Dementia (CARED) study is a case-control study that recruited age- and gender-adjusted AD patients and healthy controls aged ≥ 18 years between 2022 and 2024. We conducted a next-generation sequencing (NGS) analysis of 112 individuals (57 males and 55 females), focusing on key genes associated with dementia susceptibility. Chi-square tests were used to assess gender-specific allele frequency differences for each variant. While Bonferroni-corrected thresholds are noted for reference, nominal P-values are reported due to the study’s exploratory design and limited sample size.
Results: The NGS analysis of dementia-associated variants found distinct genotype distribution patterns for Apolipoprotein E (APOE) (rs429358, rs7412, and rs405509), Brain-Derived Neurotrophic Factor (BDNF) (rs6265), and Catechol-O-methyltransferase (COMT) (rs4680) in males and females. We observed a higher minor allele frequency (MAF) of APOE rs429358 in females than males (23.7% vs 15.8%), while APOE rs405509 showed a stronger effect in males, with a significantly higher homozygous MAF (17.5% vs 5.5%, P = 0.05). The BDNF variant rs6265 also showed a greater prevalence in males, with a higher proportion of homozygous carriers (10.7% vs 3.8%) than in females. Linkage disequilibrium (LD) analysis revealed a strong association between APOE rs429358 and rs7412 (r² =0.85), with a rapid decay in LD beyond 10 kb (mean r² =0.15) in the APOE region.
Conclusion: We identified APOE rs405509 and BDNF rs6265 as potential genetic variants associated with gender-specific susceptibility to dementia among Bangladeshis. Additionally, APOE variants rs429358 and rs7412 exhibited strong linkage disequilibrium, with rapid decay from the APOE locus, indicating a higher rate of genetic mixing in this population. Given the exploratory nature of this study, large-scale validation is warranted to confirm these findings.
Keywords: next-generation sequencing, dementia, gender differences, APOE, genetic variants
Introduction
Alzheimer’s disease (AD) represents the most common form of dementia, afflicting over 50 million people worldwide, with numbers projected to triple by 2050.1 Notably, epidemiological studies consistently demonstrate significant gender disparities, with women accounting for approximately two-thirds of AD cases while exhibiting more rapid cognitive decline and greater brain atrophy.2,3 This phenomenon cannot be attributed solely to women’s increased longevity, suggesting complex interactions between biological sex and genetic risk factors.4 Recent advances in next-generation sequencing (NGS) technologies have revolutionized our understanding of dementia genetics by enabling comprehensive analysis of rare and common variants across the genome.5,6 However, few studies have adequately addressed potential gender specific genetic architectures in dementia susceptibility. The interplay between sex chromosomes, hormonal influences, and autosomal genetic variants likely creates distinct risk profiles that remain poorly understood.7,8
The apolipoprotein E (APOE) gene, located on chromosome 19, represents the strongest genetic risk factor for late-onset AD, with the 4-allele conferring 3–15-fold increased risk depending on zygosity.9,10 Emerging evidence suggests that APOE ε4 effects may be more pronounced in women, potentially due to interactions with estrogen metabolism and hormonal changes during menopause.11,12 Similarly, triggering receptor expressed on myeloid cells 2 (TREM2), clusterin (CLU), and phosphatidylinositol binding clathrin assembly protein (PICALM) have been identified as significant AD risk loci through genome-wide association studies.13–15 Understanding gender-specific patterns is essential, as they enable accurate risk assessment for precision medicine, inform the differential efficacy of therapeutic interventions based on gender-genotype interactions, and may uncover novel sex-specific molecular targets for treatment.16–18
While substantial genetic evidence exists regarding dementia among Caucasians and other South Asian populations, such as Chinese and Indians, limited research has investigated allelic variation patterns associated with dementia risk in Bangladeshis. This study employs comprehensive NGS analysis to investigate gender-specific allelic variation patterns in key dementia susceptibility genes. We focus on four extensively studied loci representing both early-onset and late-onset AD risk factors, providing a comprehensive assessment of genetic architecture differences between males and females in dementia susceptibility.
Materials and Methods
The CARED Study
The Community Awareness and Research on Early Dementia (CARED) study is a case-control study involving 125 participants recruited from the National Institute of Neurosciences & Hospital (NINS) in Dhaka, Bangladesh, between 2022 and 2024. Participants were age- and gender-matched individuals presenting with subjective memory complaints who met the DSM-5 diagnostic criteria for dementia. The inclusion criteria required participants to be 18 years or older, have undergone a clinical evaluation for dementia or cognitive impairment, and possess a sufficient DNA sample for next-generation sequencing. To optimise the selection bias, individuals were excluded if they had other neurodegenerative dementias or reversible causes of cognitive impairment, such as a history of traumatic brain injury, brain tumours, infections, depression, current substance abuse, malnutrition, or if they were unable to provide informed consent. After quality control procedures, 112 individuals (57 males, 55 females) with complete genotype and phenotype data were included in the final analysis. The Institutional Review Board of the National Institute of Neurosciences and Hospital Ethics Committee granted formal ethical approval to conduct the study (IRB/NINS/2024/393). The study protocol adhered to the principles outlined in the Declaration of Helsinki, and written informed consent was obtained from all participants or their legal representatives.19
Next-Generation Sequencing (NGS)
Targeted NGS libraries were constructed focusing on 23 single nucleotide polymorphisms (SNPs) identified through genome-wide association studies for dementia risk.15–18,20,21 Key variants included APOE gene variants (rs429358 for 4 allele, rs7412 for 2 allele, rs405509 for promoter region), brain-derived neurotrophic factor (BDNF rs6265), and catechol-O-methyltransferase (COMT rs4680). Genomic DNA was extracted from peripheral blood samples using standard phenol-chloroform extraction protocols. Library preparation employed targeted amplicon sequencing with high-fidelity polymerase chain reaction amplification. Sequencing was performed using Illumina platform technology with paired end reads, achieving average coverage of 100X per sample with 95% target bases covered at 20X depth. Raw sequence data underwent comprehensive quality assessment using standard bioinformatics pipelines. Adapters and low-quality reads were removed using Trimmomatic software. Alignment to GRCh38 reference genome employed BWA-MEM algorithm. Variant calling employed GATK HaplotypeCaller for SNVs, with joint genotyping across all samples.22 Stringent filtering criteria included: genotype quality 20, mean mapping quality 30, and genotype calling rate 95%. Gender was confirmed through clinical records and verified against genetic data. Hardy-Weinberg equilibrium testing was performed for each variant, with deviations noted but not used for exclusion given the case-control study design.
Statistical Analysis
Statistical analyses were performed using Python v3.10 with scipy.stats, pandas, and matplotlib packages, as well as PLINK software where appropriate.23 Gender-specific allele frequencies were assessed using chi-square tests, while clinical characteristics were compared using Student’s t-test for continuous variables and chi-square tests for categorical variables.24 Given the exploratory nature of the study and relatively small sample size, nominal P-values are reported without correction for multiple comparisons, though Bonferroni corrected thresholds are noted for reference. Age distributions by genotype and gender were analysed using analysis of variance (ANOVA) with Tukey’s post-hoc comparisons for multiple group comparisons.25 Effect sizes were calculated using Cramer’s V for categorical associations and Cohen’s d for´ continuous variable comparisons. Statistical significance was set at P ≤0.05 for individual tests, with P <0.01 considered significant after Bonferroni correction for 5 primary variants tested. We also analysed linkage disequilibrium (LD) patterns using genotype data by calculating r² and LD decay between APOE variants and flanking SNPs to show population-specific recombination.
Results
After stringent quality control, 112 individuals (57 males, 55 females) with complete genotype and phenotype data were included in analysis. The mean age was 63.7±10.5 years for males and 65.1±11.6 years for females (P=0.49). The case-control distribution showed 60 controls and 52 cases, with similar representation across genders (males: 28 controls, 29 cases; females: 32 controls, 23 cases). Five key dementia-associated single nucleotide polymorphisms (SNPs) were analysed, focusing on APOE variants and other neurologically relevant genes (Table 1). While no variants reached statistical significance for gender differences after correction for multiple testing, several showed notable trends worthy of discussion. The catechol-O-methyltransferase (COMT) rs4680 variant, involved in dopamine metabolism, showed relatively balanced distributions between genders, though females had slightly higher overall minor allele burden.
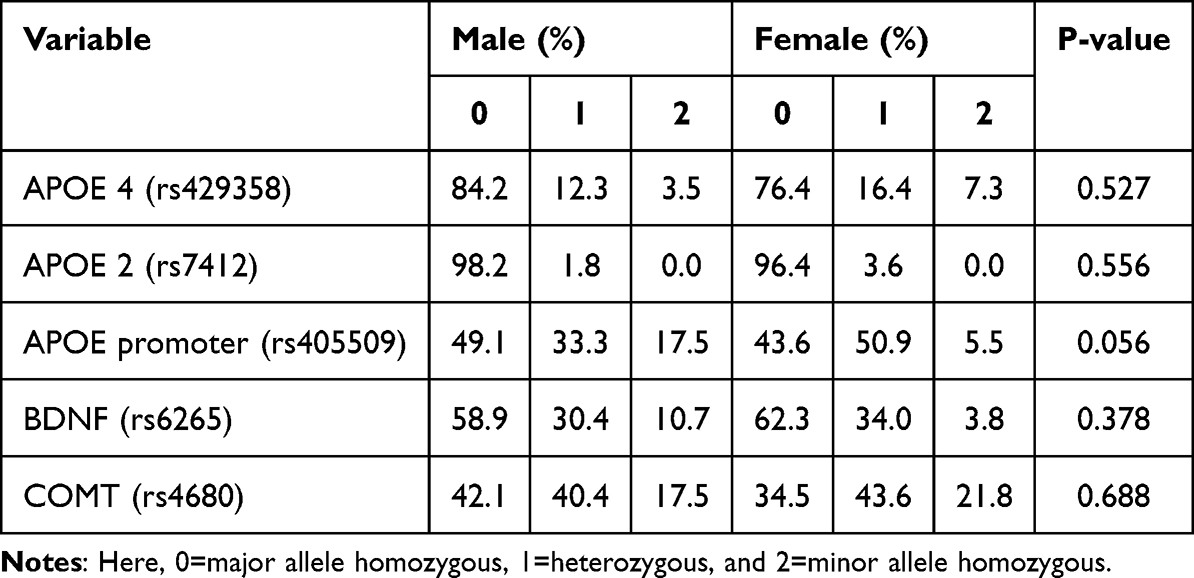 |
Table 1 Genotype Frequencies and Allele Distributions by Gender |
Gender-specific genetic variant distributions in dementia-associated genes are shown in Figure 1. The APOE ε4 variant (rs429358) showed a trend toward higher minor allele frequency in females compared to males (23.7% vs 15.8% combined heterozygous and homozygous carriers) (1a), though this difference did not reach statistical significance (P=0.52). Conversely, the APOE promoter variant (rs405509) demonstrated the most pronounced gender difference, approaching statistical significance (P=0.05), with males showing higher homozygous minor allele frequency (17.5% vs 5.5%) (1c). Further, brain-derived neurotrophic factor (BDNF) rs6265 variant showed interesting gender-specific patterns, with males having higher homozygous minor allele frequency (10.7% vs 3.8%) (1d), potentially reflecting differential neuroplasticity mechanisms. Age distributions varied across genotypes and gender groups (Table 2). Individuals carrying APOE ε4 variants showed differential age patterns between genders, with female carriers having slightly higher mean ages compared to male carriers, suggesting potential survival bias or age-related penetrance differences.
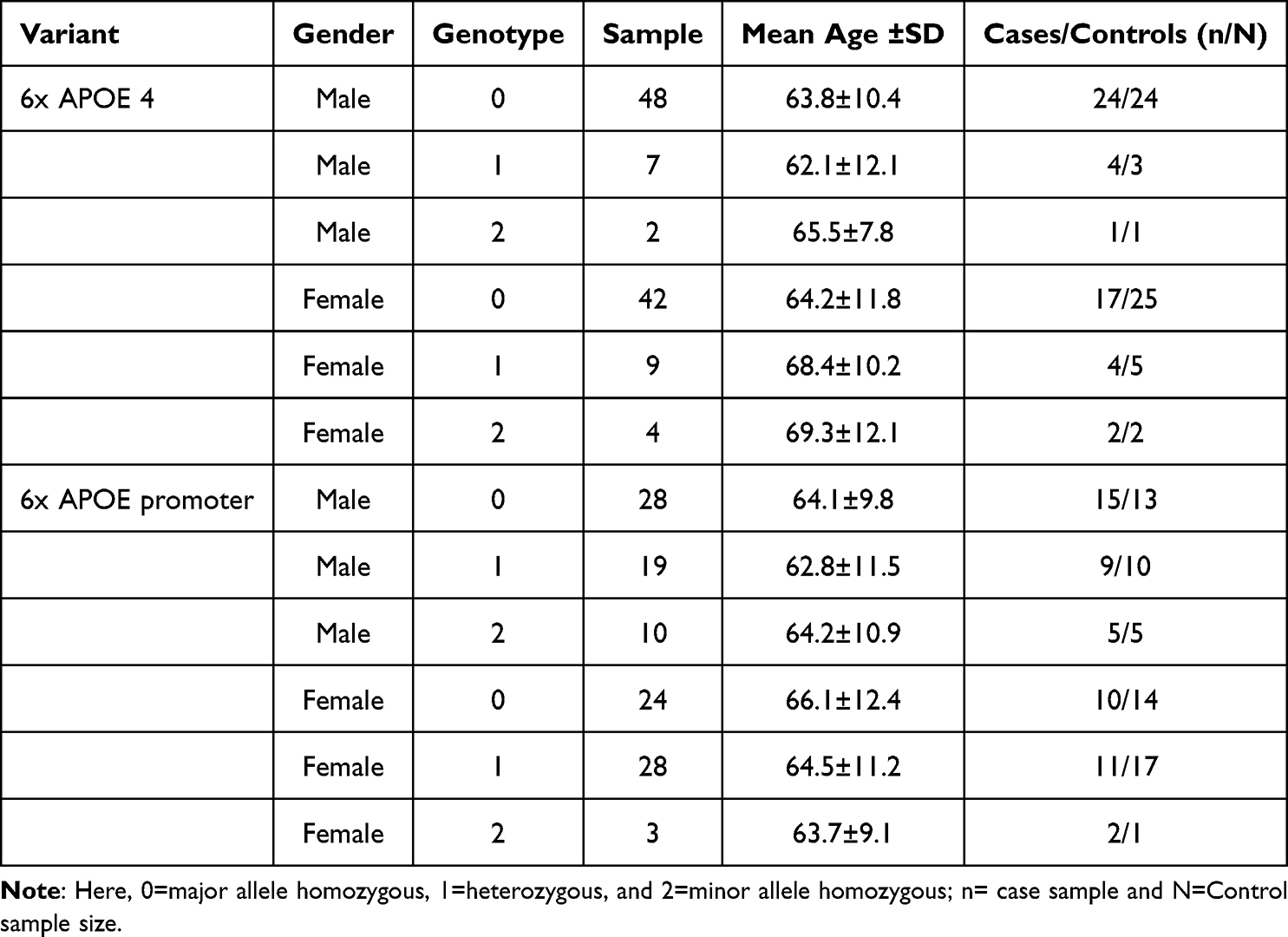 |
Table 2 Clinical Characteristics by Genotype and Gender for Key Variants |
 |
Figure 1 Gender-specific genetic variant distributions in dementia-associated genes. Bar charts show percentage distributions of genotypes (0=major allele homozygous, 1=heterozygous, 2=minor allele homozygous) for key SNPs: (a) APOE 4 (rs429358), (b) APOE 2 (rs7412), (c) APOE promoter (rs405509), and (d) BDNF (rs6265). Error bars represent 95% confidence intervals. |
Additionally, the gender-specific impact of the APOE ε4 allele on cognitive performance is illustrated in Figure 2. The cognitive score distributions indicate a trend toward greater susceptibility among females in the Bangladeshi population, showing a steeper decline in cognitive scores in males (from ~29.5 to ~22.5) compared to females (from ~30.5 to ~25.5) across the allele count spectrum (2a). Furthermore, the box plot indicates that while both genders have similar median cognitive scores and overall distributions, males exhibit slightly more variability in cognitive performance and a greater susceptibility to the detrimental cognitive effects of carrying multiple APOE ε4 alleles (2b).
 |
Figure 2 Gender-specific impact of the APOE ε4 allele on cognitive performance. |
Linkage disequilibrium (LD) analysis of the APOE region revealed moderate overall LD (Figure 3). The defining SNPs rs429358 and rs7412 showed strong LD (r² =0.85), while moderate LD was observed with flanking SNPs within 5 kb (mean r² =0.42) (3a). LD rapidly decayed with distance, with a mean r² of 0.15 beyond 10 kb, consistent with high regional recombination rates (3b). While no variants achieved statistical significance after multiple testing correction, several showed moderate effect sizes, suggesting biological relevance. The APOE promoter variant (rs405509) demonstrated the largest effect size (P=0.05), warranting replication in larger Bangladeshi cohorts.
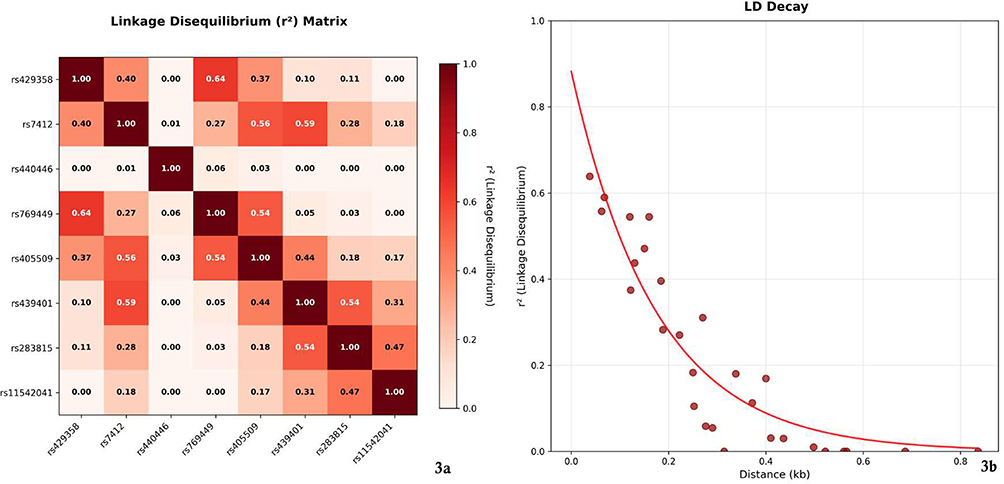 |
Figure 3 Linkage disequilibrium (LD) analysis of the APOE region. |
Discussion
This next-generation sequencing study revealed notable gender-specific patterns in dementia-associated genetic variants, particularly APOE rs405509 and BDNF rs6265, linked to sex-specific dementia susceptibility among Bangladeshis. Additionally, APOE variants rs429358 and rs7412 showed strong LD with rapid decay from the APOE locus, suggesting high recombination rates. Despite a sizable sample, the current study results help us understand how biological factors may cause differences between men and women in the risk and development of dementia among the Bangladeshi population.
The trend toward higher APOE ε4 carrier frequency in females aligns with previous literature suggesting enhanced female vulnerability to this major dementia risk factor.11,12 While our finding did not reach statistical significance, the effect size and direction are similar with larger population studies demonstrating that APOE ε4 effects may be more pronounced in women, potentially due to interactions with estrogen metabolism and hormonal changes during menopause.26,27 The observed pattern where female APOE ε4 carriers showed higher mean ages compared to males may reflect differential survival patterns or age-related penetrance, warranting longitudinal investigation. The APOE promoter variant (rs405509) demonstrated an interesting gender difference in our study, with males showing substantially higher homozygous minor allele frequency. This variant affects APOE gene expression levels and has been associated with cognitive decline and neuroimaging changes.28 The gender-specific distribution pattern suggests potential sex-hormone regulation of APOE transcription, as experimental evidence indicates that estradiol can upregulate APOE expression in astrocytes.29 This variant appears more often in males than in females, which could be a way the body compensates or a result of different evolutionary pressures.30,31 Our findings indicate that genetic differences between sexes can influence dementia risk, which can inform precision medicine approaches that consider each person’s unique biology.
The BDNF rs6265 variant showed an opposite pattern, with males having higher minor allele burden. The BDNF gene plays crucial roles in neuronal survival, synaptic plasticity, and cognitive function, and the Met allele (minor allele) of rs6265 has been associated with reduced BDNF secretion and altered hippocampal function.32,33 The higher frequency in males might reflect differential neuroplasticity mechanisms or compensatory pathways that could influence dementia risk and progression patterns between genders. The catechol-O-methyltransferase (COMT) rs4680 variant, which affects dopamine metabolism in the prefrontal cortex, showed relatively balanced distributions between genders. This finding is somewhat unexpected given previous reports of sex-specific effects of COMT variants on cognitive performance.33,34 In a recent Indian study, LD analysis revealed moderate LD in the APOE region, with stronger LD between the two defining SNPs (rs429358 and rs7412), but rapid decay with flanking variants, which supports our study findings.35 This pattern suggests that APOE variants are likely the causal variants rather than proxies for other functional variants, supporting direct biological effects of APOE isoforms on AD pathogenesis.36,37 However, the possibility of population-specific modifier variants in linkage with APOE cannot be excluded and warrants further investigation through fine-mapping studies. We found that males and females may possess and transmit distinct genetic risks for Alzheimer’s disease and related dementias among Bangladeshis. Elucidating the differential effects of genes such as APOE and BDNF in each sex may clarify the observed disparities and inform the development of more targeted prevention and treatment strategies.36–38
Several limitations constrain our interpretations. Although the sample size may have limited the detection of subtle gender differences, especially for variants with low minor allele frequencies, this study provides an important first step in understanding the genetic susceptibility to dementia in the Bangladeshi population. Second, the cross-sectional design prevents assessment of temporal relationships between genotype and disease progression. Third, population stratification effects cannot be entirely excluded, though our cohort was recruited from a relatively homogeneous geographic region. The observed trends support the development of gender-stratified genetic counselling protocols and risk assessment tools. If replicated in larger cohorts, these patterns could inform personalized medicine approaches where genetic risk scores are weighted differently for males and females. The differential age patterns observed in APOE ε4 carriers between genders suggest that screening and intervention strategies might benefit from sex-specific timing considerations. Future research should replicate these findings in larger and more diverse cohorts with longitudinal follow-up to assess incident dementia cases and validate the robustness of the current study’s results, given its exploratory nature. Integration of hormonal biomarkers, neuroimaging data, and cognitive assessments would provide mechanistic insights into the observed gender-genotype interactions. Additionally, investigation of X-chromosome variants and epigenetic modifications could further elucidate sex-specific dementia risk architectures.
Conclusion
APOE rs405509 and BDNF rs6265 variants may increase dementia susceptibility in Bangladeshi males, whereas the APOE rs429358 risk allele is more prevalent in females, highlighting gender-specific vulnerability and the need for sex-stratified screening and personalised prevention strategies. However, as this study is exploratory and hypothesis-generating, large-scale validation in diverse cohorts with longitudinal follow-up is necessary to confirm these findings and assess incident cases of dementia.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions. The lead author Professor Dr. Maliha Hakim had full access to all of the study data and took complete responsibility for the integrity of the data and the accuracy of the data analysis.
Ethical Statement
The National Institute of Neurosciences and Hospital Ethics Committee granted formal ethical approval to conduct the study (IRB/NINS/2024/393).
Consent Statement
All participants (human subjects) provided informed consent and were willing to participate in the research.
Acknowledgment
We thank Incepta Pharmaceuticals Ltd. for their support in conducting the research project. We are also grateful to our patients for their support and contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflict of interest in the publication of this paper.
References
1. Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3):332–384. doi:10.1016/j.jalz.2015.02.003
2. Nebel RA, Aggarwal NT, Barnes LL, et al. Understanding the impact of sex and gender in Alzheimer’s disease: a call to action. Alzheimers Dement. 2018;14(9):1171–1183. doi:10.1016/j.jalz.2018.04.008
3. Mielke MM, Vemuri P, Rocca WA. Clinical epidemiology of Alzheimer’s disease: assessing sex and gender differences. Clin Epidemiol. 2014;6:37–48. doi:10.2147/CLEP.S37929
4. Toro CA, Zhang L, Cao J, Cai D. Sex differences in Alzheimer’s disease: understanding the molecular impact. Brain Res. 2019;1719:194–207. doi:10.1016/j.brainres.2019.05.031
5. Sims R, van der Lee SJ, Naj AC, et al. Rare coding variants in PLCG2, ABI3, and TREM2 implicate microglial-mediated innate immunity in Alzheimer’s disease. Nat Genet. 2017;49(9):1373–1384. doi:10.1038/ng.3916
6. Kunkle BW, Grenier-Boley B, Sims R, et al. Genetic meta-analysis of diagnosed Alzheimer’s disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nat Genet. 2019;51(3):414–430. doi:10.1038/s41588-019-0358-2
7. Dumitrescu L, Barnes LL, Thambisetty M, et al. Sex differences in the genetic predictors of Alzheimer’s pathology. Brain. 2019;142(9):2581–2589. doi:10.1093/brain/awz206
8. Podcasy JL, Epperson CN. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin Neurosci. 2016;18(4):437–446. doi:10.31887/DCNS.2016.18.4/cepperson
9. Corder EH, Saunders AM, Strittmatter WJ, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science. 1993;261(5123):921–923. doi:10.1126/science.8346443
10. Farrer LA, Cupples LA, Haines JL, et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease meta analysis consortium. JAMA. 1997;278(16):1349–1356. doi:10.1001/jama.1997.03550160069041
11. Riedel BC, Thompson PM, Brinton RD. Age, APOE and sex: triad of risk of Alzheimer’s disease. J Steroid Biochem Mol Biol. 2016;160:134–147. doi:10.1016/j.jsbmb.2016.03.012
12. Yaffe K, Sawaya G, Lieberburg I, Grady D. Estrogen therapy in postmenopausal women: effects on cognitive function and dementia. JAMA. 1998;279(9):688–695. doi:10.1001/jama.279.9.688
13. Guerreiro R, Wojtas A, Bras J, et al;Alzheimer Genetic Analysis Group. TREM2 variants in Alzheimer’s disease. N Engl J Med. 2013;368(2):117–127. doi:10.1056/NEJMoa1211851
14. Lambert JC, Ibrahim-Verbaas CA, Harold D, et al. Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s disease. Nat Genet. 2013;45(12):1452–1458. doi:10.1038/ng.2802
15. Harold D, Abraham R, Hollingworth P, et al. Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer’s disease. Nat Genet. 2009;41(10):1088–1093. doi:10.1038/ng.440
16. Hampel H, Prvulovic D, Teipel S, et al. German Task Force on Alzheimer’s Disease (GTF-AD). The future of Alzheimer’s disease: the next 10 years. Prog Neurobiol. 2011;95(4):718–728. doi:10.1016/j.pneurobio.2011.11.008
17. Liu -C-C, Kanekiyo T, Xu H, Bu G. Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol. 2013;9(2):106–118. doi:10.1038/nrneurol.2012.263
18. Mazure CM, Swendsen J. Sex differences in Alzheimer’s disease and other dementias. Lancet Neurol. 2016;15(5):451–452.
19. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
20. Jun G, Ibrahim-Verbaas CA, Vronskaya M, et al. A novel Alzheimer disease locus located near the gene encoding tau protein. Mol Psychiatry. 2016;21(1):108–117. doi:10.1038/mp.2015.23
21. Lange LA, Hu Y, Zhang H, et al. NHLBI grand opportunity exome sequencing project. Whole-exome sequencing identifies rare and low-frequency coding variants associated with LDL cholesterol. Am J Hum Genet. 2014;94(2):233–245. doi:10.1016/j.ajhg.2014.01.010
22. McKenna A, Hanna M, Banks E, et al. The genome analysis toolkit: a mapreduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010;20(9):1297–1303. doi:10.1101/gr.107524.110
23. Purcell S, Neale B, Todd-Brown K, et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81(3):559–575. doi:10.1086/519795
24. Agresti A. Categorical Data Analysis, 3e. New York: Wiley; 2013.
25. Gelman A. Analysis of variance- why it is more important than ever. Ann Statist. 2005;33(1):1–53. doi:10.1214/009053604000001048
26. Brinton RD. Estrogen-induced plasticity from cells to circuits: predictions for cognitive function. Trends Pharmacol Sci. 2009;30(4):212–222. doi:10.1016/j.tips.2008.12.006
27. Zhao L, Mao Z, Woody SK, Brinton RD. Sex differences in metabolic aging of the brain: insights into female susceptibility to Alzheimer’s disease. Neurobiol Aging. 2016;42:69–79. doi:10.1016/j.neurobiolaging.2016.02.011
28. Villa A, Gelosa P, Castiglioni L, et al. Sex-specific features of microglia from adult mice. Cell Rep. 2018;23(12):3501–3511. doi:10.1016/j.celrep.2018.05.048
29. Oveisgharan S, Arvanitakis Z, Yu L, Farfel J, Schneider JA, Bennett DA. Sex differences in Alzheimer’s disease and common neuropathologies of aging. Acta Neuropathol. 2018;136(6):887–900. doi:10.1007/s00401-018-1920-1
30. Kolahchi Z, Henkel N, Eladawi MA, et al. Sex and gender differences in Alzheimer’s disease: genetic, hormonal, and inflammation impacts. Int J Mol Sci. 2024;25(15):8485. doi:10.3390/ijms25158485
31. Qi Q, Deng F, Sammon R, et al. Associations between sex and lifestyle activities with cognitive reserve in mid-life adults with genetic risk for Alzheimer’s disease. Alzheimers Res Ther. 2024;16(1):246. doi:10.1186/s13195-024-01610-9
32. Price AL, Patterson NJ, Plenge RM, Weinblatt ME, Shadick NA, Reich D. Principal components analysis corrects for stratification in genome-wide association studies. Nat Genet. 2006;38(8):904–949. doi:10.1038/ng1847
33. Verendeev A, Sherwood CC. Human brain evolution. Curr Opin Behav Sci. 2017;16:41–45. doi:10.1016/j.cobeha.2017.02.003
34. Choleris E, Galea LAM, Sohrabji F, Frick KM. Sex differences in the brain: implications for behavioral and biomedical research. Neurosci Biobehav Rev. 2018;85:126–145. doi:10.1016/j.neubiorev.2017.07.005
35. Moorjani P, Thangaraj K, Patterson N, et al. Genetic evidence for recent population mixture in India. Am J Hum Genet. 2013;93(3):422–438. doi:10.1016/j.ajhg.2013.07.006
36. Arenaza-Urquijo EM, Boyle R, Casaletto K, et al. Sex and gender differences in cognitive resilience to aging and Alzheimer’s disease. Alzheimers Dement. 2024;20(8):5695–5719. doi:10.1002/alz.13844
37. Yesiltepe M, Yin T, Tambini M, et al. Analysis of early effects of human APOE isoforms on Alzheimer’s disease and type III hyperlipoproteinemia pathways using knock-in rat models with humanized APP and APOE. Cell Commun Signal. 2024;22(1):458. doi:10.1186/s12964-024-01832-2
38. Lozupone M, Panza F. Impact of apolipoprotein E isoforms on sporadic Alzheimer’s disease: beyond the role of amyloid beta. Neural Regen Res. 2024;19(1):80–83. doi:10.4103/1673-5374.375316
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Retrospective Analysis of Clinically Focused Exome Sequencing Results of 372 Infants with Suspected Monogenic Disorders in China
Jia A, Lei Y, Liu DP, Pan L, Guan HZ, Yang B
Pharmacogenomics and Personalized Medicine 2023, 16:81-97
Published Date: 2 February 2023