Back to Journals » Advances in Medical Education and Practice » Volume 17
Gender-Inclusive Pedagogy: Designing Effective Instructional Strategies for Male Nursing Students in Obstetric and Gynecological Nursing Education
Authors Liu Z ![]() , Liu L, Wang C, Zhong X, Zhou X, Shao Z, Ye Y
, Liu L, Wang C, Zhong X, Zhou X, Shao Z, Ye Y ![]() , Hu X
, Hu X ![]()
Received 17 May 2025
Accepted for publication 17 November 2025
Published 8 January 2026 Volume 2026:17 541147
DOI https://doi.org/10.2147/AMEP.S541147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Zhunzhun Liu,1,2 Lihui Liu,1 Can Wang,1 Xiaohui Zhong,1 Xiaoyi Zhou,3 Zhonglei Shao,4 Yun Ye,5 Xiang Hu6
1Nursing School, Wuxi Taihu University, Wuxi, Jiangsu Province, People’s Republic of China; 2Nursing Department, Rugao Boai Hospital, Nantong, Jiangsu Province, People’s Republic of China; 3School of Computer Science and Technology, Soochow University, Suzhou, Jiangsu Province, People’s Republic of China; 4The Scotland Academy, Wuxi Taihu University, Wuxi, Jiangsu Province, People’s Republic of China; 5Nursing Management Department, The First People’s Hospital of Changzhou, Changzhou, Jiangsu Province, People’s Republic of China; 6School of Education, Chongqing Normal University, Chongqing, Chongqing Province, People’s Republic of China
Correspondence: Zhunzhun Liu, Nursing Department, Rugao Boai Hospital, Nantong, People’s Republic of China, Email [email protected]
Background: Male nursing students face distinctive challenges in obstetrics and gynecology (OB-GYN) nursing education, influenced by social perceptions and the specialty’s gender dynamics.
Objective: This study aimed to develop effective instructional strategies addressing male students’ learning challenges in OB-GYN.
Methods: Using a mixed-method design (qualitative interviews, focus groups, expert workshops, Delphi survey), the prototype of instructional strategies was created based on design thinking and the Medical Research Council (MRC) framework. A non-randomized trial (n = 56) tested the 10-week intervention in a 2025 OB-GYN undergraduates’ course at Wuxi Taihu University, assessing academic performance, knowledge application/transfer (teacher-rated), and competency (self-reported).
Results: The experimental group demonstrated significantly better knowledge application/transfer skills (t = 2.206, P = 0.034) and higher overall competency levels (t = 2.207– 4.359, P < 0.05) compared to controls. Regression analysis confirmed the instructional strategies (β = 0.298, P < 0.001), academic performance (β = − 1.062, P = 0.001), and knowledge application skills (β = 1.674, P < 0.001) as significant predictors of self-reported competency, explaining 68.5% of variance.
Conclusion: The evidence-based instructional strategies effectively enhance practical skills and professional competencies in OB-GYN nursing education. While promising, further multi-center trials with larger samples are recommended to validate these findings and assess long-term impacts on professional development.
Keywords: teaching program, male nursing undergraduates, obstetrics and gynecology nursing, mixed-method approach, design thinking
Introduction
Obstetrics and Gynecology Nursing (OB-GYN) is a specialized discipline dedicated to the comprehensive care of women, addressing health needs across the lifespan from adolescence through menopause, encompassing prenatal, postpartum, and reproductive healthcare.1,2 In China, the foundation of modern OB-GYN nursing education was laid by pioneers like Dr. Mabel Poulter, who established the earliest nursing education program in Fuzhou in 1906 and opened the country’s first obstetric unit in 1911.3 Today, modern nursing calls on the sophisticated integration of knowledge through extensive formal training and certification.4 OB-GYN is a compulsory and core course for all nursing students in China and a mandatory component of the national licensing examination for registered nurse, applicable to all candidates of all genders.3,5
Despite this universal requirement, a significant demographic shift is underway. Data from the National Health Commission6 reveal a steady increase in the proportion of male nurses in China, growing from 2.6% (n = 4,445,047) in 2019 to 3.4% (n = 5,019,422) in 2021. However, deep-seated traditional expectations and social biases continue to frame OB-GYN as a female-dominated profession.7 This socio-cultural context creates a profound educational dilemma for male nursing students: they are required to master OB-GYN knowledge and skills, yet they often perceive limited future career prospects in this specialty. Consequently, male students frequently become passive observers rather than active participants in the OB-GYN classroom. Compared to their female counterparts, they report lower engagement, diminished professional identity, and greater psychological pressure,8 which collectively impedes the development of their overall nursing competency.9
In response, educators have explored various strategies to enhance students’ engagement and competency in nursing education programs,10 such as blending teaching and collectivist teaching.11 However, the application of these strategies within OB-GYN nursing education often lacks a coherent theoretical framework for their systematic selection and implementation.10,12 Many studies fail to detail the process of intervention construction, and crucially, students’ personal experiences13 and emotional journeys are often undervalued. This is particularly true for male students, whose unique perspectives and the potential for fostering etic-emic understanding (bridging both male/female and nurse/patient perspectives) remain largely untapped. Consequently, a clear research gap is underscored: the absence of a gender-inclusive pedagogical teaching model that is grounded in a robust theoretical framework, explicitly designed to address the psycho-social and professional needs of male nursing students in OB-GYN, and to leverage their unique position to improve care.
To address this gap, our study was guided by the Design Thinking process14 (Empathize, Define, Ideate, Prototype, Test) and the idea from Medical Research Council (MRC) framework15 for developing interventions (taking stakeholders into consideration while identifying challenges and strategies in ‘define and ideate” process). This combined approach ensured a user-centered and methodologically rigorous development of our educational intervention by using both qualitative and quantitative methods (mixed-method approach).
Therefore, this study aims to develop effective instructional strategies for OB-GYN education, specifically designed to create a more inclusive and effective OB-GYN learning environment for male nursing students, with the ultimate goal of enhancing their knowledge, skills, and overall competency. This aligns with the UNESCO Education 2030 Agenda and the United Nations’ Sustainable Development Goals (SDGs), particularly SDG 4 (Quality Education), and SDG 5 (Gender Equality), by advocating for inclusive, equitable, and quality education for all students, irrespective of gender. Furthermore, our intervention is designed in accordance with China’s “National Standards for Nursing Education”, which emphasizes competency-oriented education.12
Methods and Results
This study utilized a mixed-method design to develop and test a teaching program. To develop the teaching program, this part of the study followed the steps of the design thinking process and the idea of taking all stakeholders into consideration through intervention development. The final procedure included: understand and observe by students interview, define the point of view from teachers-focused group, ideate through expert workshop and Delphi survey, prototype, and test. A non-randomized controlled trial design was used to test male nursing students’ experience and comprehensive abilities after applying the newly designed teaching program. The study protocol was submitted to and approved by the Ethics Committee of Rugao Boai Hospital (2025-L02).
Students Interview
Methods
To understand male nursing undergraduates’ feelings, needs, and behaviors in OB-GYN learning, qualitative interviews were conducted. The purpose sampling approach was used to recruit participants from April to May 2024. The interviews were recorded and transcribed verbatim. Van Manen’s method of phenomenological hermeneutics was adopted to analyze the text. This part of the study was published.5
Results
This part of the study interviewed 10 male nursing undergraduates and identified three key themes: (1) negative future appraisal (unsatisfactory practical opportunities, unbearable psychological pressure, negative media coverage), (2) breaking out of information bubbles (learn real-world experience, discuss gender inclusivity), and (3) positive capacity-building (skills in empathy, critical thinking, and self-efficacy) among male students. In this part of the study, male nursing undergraduates expressed negative future appraisal, but experienced the growth and gain of personal skills in the learning process. An important finding is that male nursing undergraduates expressed the need to break out of the information bubbles engendered by traditional cultural notions.
Teachers-Focus Group
Methods
A focus group meeting (teachers who undertook the OB-GYN curriculum, including registered nurses from the affiliated hospitals and teachers from Wuxi Taihu University) was carried out in May 2024 to identify the challenges of teaching OB-GYN and develop solutions and goals. Participants were included if they: (1) undertook the OGN curriculum at least for one semester year; (2) had experience in teaching male nursing undergraduates. To capture the views of all teachers, individuals with varying teaching arrangements were selected, including those with little experience (under a two-semester year) and long-term experience. All interested individuals in Wuxi Taihu University meeting the inclusion criteria received prior written reports of qualitative interviews and information regarding the aim and content of the program.
A stepwise modeling process was conducted in the teachers-focus group, including: (1) Reviewing results and knowledge: Starting with a shared report of the qualitative interview results, the aim of the program, and the process of the workshop were introduced. (2) Identification of challenges of teaching OB-GYN: The aim of this stage was to identify further challenges from the perspective of the teachers. Participants were invited to identify challenges from their teaching experience or from the interview results. (3) Contextualization: The identification results were reintroduced to the group and synthesized with at least 50% agreement.
Results
In total, five teachers who undertook the curriculum participated in this meeting: 2 had both clinical and teaching experiences, and 3 had teaching experience. Course and results of the meeting: After reviewing reports of interview results, the Challenges thus were identified as follows (Supplementary Table 1): The most prioritized domain of CFIR (24 votes in total, 100%) was the inner setting (10 votes, 41.7%), followed by characteristics of individuals (5 votes, 20.8%), process (4 votes, 16.7%), intervention characteristics (3 votes, 12.5%), and outer setting (2 votes, 8.3%). Three leading challenges were: (1) Available resources (inner setting): 100% agreement (5 votes/5 voters). (2) Access to knowledge and information (inner setting): 60% agreement. (3) The need to build professional self-identity (characteristics of individuals: 60% agreement).
Expert Workshop
Methods
The expert workshop provided a platform for the collaborative design of intervention components and implementation strategies.16 To discuss and develop teaching improvement strategies, we aimed to involve all stakeholders in the workshop: clinical and research experts on nursing education, interviewees from steps 1 and 2, and other nursing male and female nursing students’ representatives were all invited to the workshop. The workshop was led by a senior researcher with extensive experience in workshops for developing interventions. Due to interviewees of Step 1 were in their internship in hospitals in different cities, the expert committee was conducted desperately with target groups. Firstly, 6 clinical and research experts on nursing education, 5 teachers in the teachers-focus group, other 7 nursing male and 7 female nursing student representatives participated in the workshop held in June 2024. Secondly, interviewees from Step 1 were invited to review the record of the first meeting and vote.
A revised stepwise process was adopted, including: (1) Reviewing results and knowledge: Starting with shared reports of the results of steps 1 and 2, the aim of the program, and the process of the workshop were introduced, followed by literature review of the topic. (2) Development of solutions and goals: To develop solutions and goals, creativity techniques, such as “brainstorming” writing,17 were used in the session. Brainstorming was organized, with the senior researcher as the moderator and recorder. The moderator clarified the discussion topics and disciplines, controlled the process during the meeting, and inspired guidance at the same time. All ideas are recorded on the blackboard for 30 minutes. Alternatively, the “reversal method” of brainstorming was used by identifying ways that could cause or worsen a problem. Then, these ideas were reversed to find solutions. (3) Contextualization: The moderator collected results and reintroduced the new insights whenever necessary. To identify potential implementation barriers and strategies, the Consolidated Framework of Implementation Research (CFIR)18 and the Expert Recommendation for Implementing Change (ERIC)19 were adapted and used in this process by deleting unnecessary constructs. Participants weighted and prioritized the constructs on the matching tool. The 7 strategies with the highest weights were selected and discussed by experts to specify the appropriation based on their experience. The final summary results were reintroduced to the workshop and synthesized into an initial intervention and an implementation plan with 80% agreement.
Course and Results of the Workshop
The workshop carefully reviewed and elaborated the final findings to avoid an appropriate impact on decisions in this process. The most weighted constructs of CFIR domains were transformed into ERIC strategies. Figure 1 detailed the selected 7 ERIC strategies; these strategies were further developed into implementation strategies by the workshop. We further defined an implementation plan (a preliminary implementation blueprint).
 |
Figure 1 Study Design. |
Delphi Survey
Methods
The research team reviewed and discussed the intervention and implementation plan. To validate and refine this plan, a Delphi survey20 was conducted. The survey was developed based on the findings from the prior steps, ensuring its content validity was grounded in expert input and literature. A panel of 20 representatives were invited to participate, including professors from the workshop (n = 11), additional external experts from diverse backgrounds (two in education, one in management, and two in a healthcare setting), two male nursing students, and two female nursing students.
The Delphi process was conducted as follows: Experts were invited via Email and provided with the survey instrument. They were asked to rate the importance of each item using a 5-point Likert scale (1 = Very Unimportant to 5 = Extremely Important) and to provide qualitative comments in open-ended fields after each item. The consensus criteria were pre-defined as a selection rate (percentage of experts rating an item 4 or 5) >80% and a full score rate (percentage of experts rating an item 5) >50%. The expert active coefficient (response rate) for the first round was 95% (19/20), indicating a high level of engagement. The degree of consensus among experts was quantitatively assessed using Kendall’s coefficient of concordance (W).
Results
There was strong agreement on the first round of the survey (selection rate = 90%–100%, full score rate = 60–100%). Statistical analysis revealed a high and significant level of consensus (Kendall’s W = 0.72, p < 0.05). As the pre-defined consensus criteria were met for all items and a strong concordance was achieved, no second round was required, and no major changes to the core intervention plan were made based on the quantitative ratings.
The qualitative findings from the open-ended questions provided valuable implementation insights. These findings directly influenced the final development of the program by highlighting key logistical considerations. For example, experts suggested that the presentation should be integrated into already established lectures or training sessions. It was also recommended that comprehensive training for teachers was necessary, which we could integrate with regular group meetings for lesson preparation. Researchers incorporated these suggestions to finalize the formal intervention and implementation plan.
Prototype
A program modeling was developed by the research team to represent the common understanding of the process (why and how the program works) of the intervention. Considering nursing is an interdisciplinary field, C-POTE (Concept group, Problem chain, Objective layer, Task cluster, and Evidence set) model21,22 which is designed from STEAM and adapted well to Chinese culture, is the best fit to implement the education projects. With the notion that teaching is a dialogue, putting students in the center of the learning process and an educational concept of interdisciplinary integration, the conversational framework was integrated with the C-POTE model, which emphasizes interactions between teachers, learners, peers, and the learning environment at both the conceptual and practice level within target culture background. The program model will serve as the theoretical basis for our further feasibility study.
A revised model was developed based on conversational framework23 and Zhan’s C-POTE model.22 The principle of the intervention of the C-POTE pyramid model specifically needs students and teachers to interactively participate in each 5 stages: (1) Teachers select OB-GYN disease module with related medical terms, and students clarify the subject and integrate knowledge through concept learning. (2) Generate problem chains around multiple concepts; teachers introduce OB-GYN cases and present problems, and students explore the rules by clarifying the questions. (3) The teacher informs students of the objectives to help students’ understanding; students rearrange tasks into groups. (4) By decomposing tasks in the form of task clusters, teachers provide support and help for students to encourage students learning, knowledge transferring, and application. (5) Teachers collect evidence to give feedback to students, and students present their own or their group’s work for further revision and reflection through feedback from classmates and teachers. The conversation framework among students, peers, and teachers is the key principle throughout the whole five stages. The specific implementation blueprint of instructional strategies for OB-GYN education is shown in Figure 2.
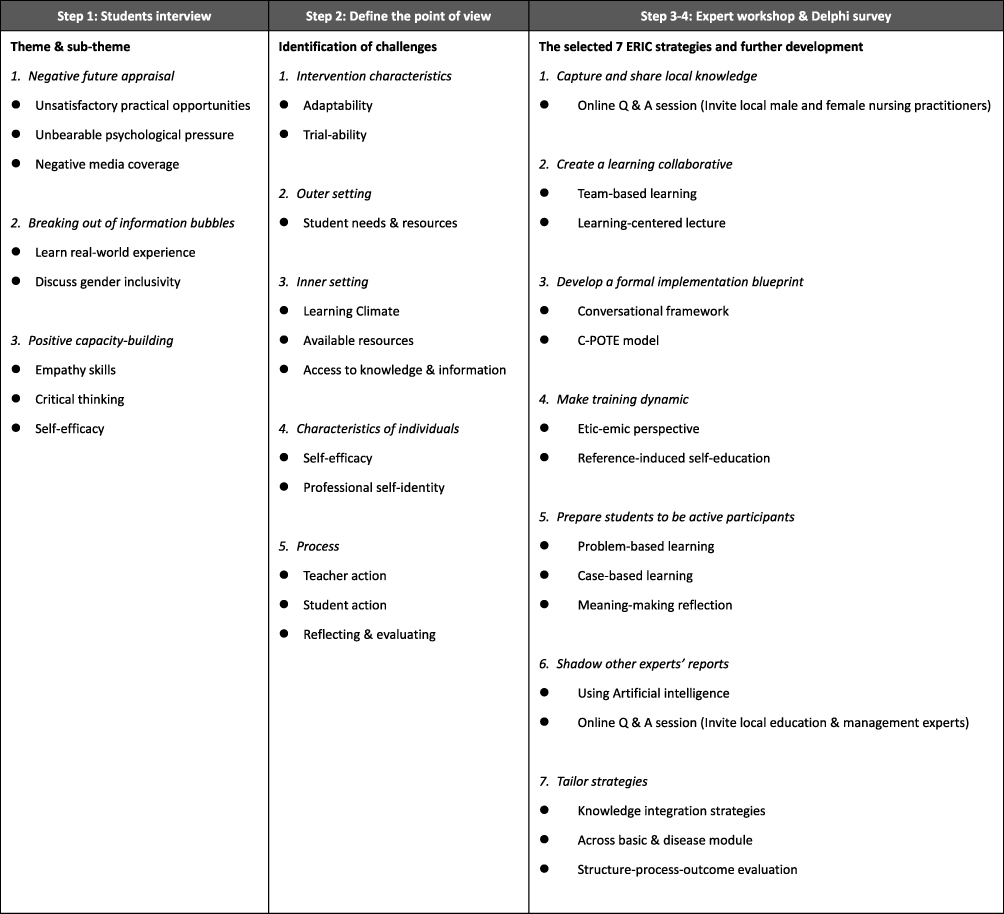 |
Figure 2 Results of Step 1, 2, 3 and 4. |
Preliminary Test of the Instructional Strategies for OB-GYN Education
Sample and Setting
This part of the study was conducted between March to May 2025 (10 weeks) in nursing school, Wuxi Taihu University. By offering electric poster with contacting information, male participants who met the following criteria were invited for the study and offered the informed consent: (1) enrolled in a full-time Bachelor of Nursing program, following a standardized curriculum that included comprehensive training in general nursing (eg, Medical-Surgical, Obstetrics and Gynecology, Pediatrics Nursing) and foundational medical courses, (2) currently studying or have studied OB-GYN in the nursing school setting, (3) finished foundational medical courses and Medical-Surgical nursing courses, not yet graduated, and (4) have experience in clinical observation (clerkship) but no internship experience. To avoid the influence of teaching style on the participants’ learning experience of OB-GYN, we recruited male students taught by the same teacher on both theoretical courses and clinical practice session, and grouped into the experimental group and control group.
The Experimental Group
Apart from the teaching tasks as the control group, the classes where male students (n = 28) were from were arranged to one flipper class (one study hour) 6 weeks later. The OB-GYN instruction framework in experimental group was designed based on C-POTE model, see Figure 3.
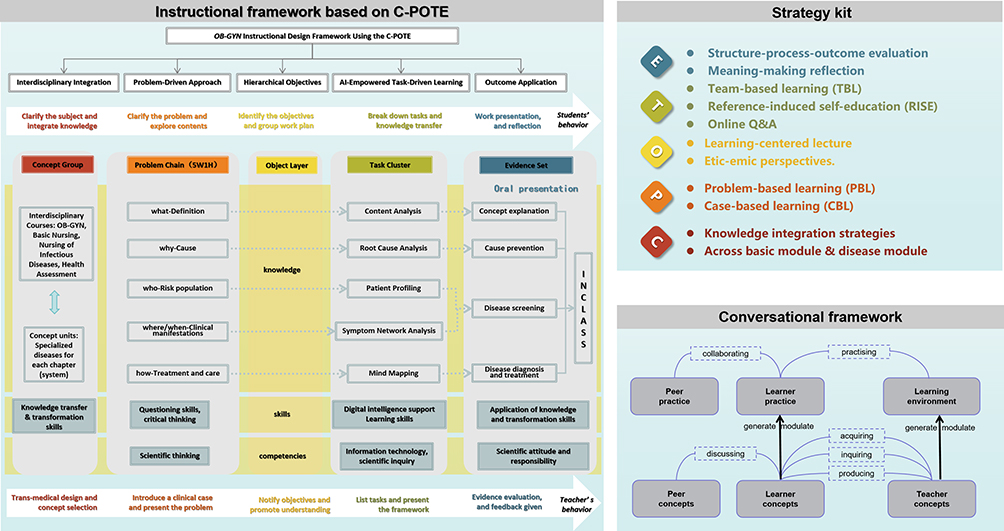 |
Figure 3 Result of Step 5: The instructional strategies for OB-GYN education. |
(1) Concept group: The OB-GYN disease module “Sexually Transmitted Diseases (STD) in Women” was chosen as it contained integrate knowledge of OB-GYN, Basic Nursing, Nursing of Infectious Diseases, Health Assessment by using mind mapping strategy.
(2) Problem chain: The teacher presented two cases (a pregnant woman diagnosed with STD and an STD patient planning a pregnancy), students were encouraged using the 5W1H Method to build problem chain. Problem-based learning (PBL) and case-based learning (CBL) strategies were recommended to be implemented.
(3) Objective layer: To achieve knowledge, skills, and competencies, the teacher invited local practitioners to share clinical experience and experts to share management and self-education skills in a learning-centered online lecture, and introduce etic-emic (both male and female or both nurse and patient) perspectives, around 1 hour before task-cluster using Tencent Meeting.
(4) Task Cluster: The ChaoXing (Superstar) Learning Platform was utilized as an educational management system wherein instructors upload and curate pedagogical resources, including Team-Based Learning (TBL) modules, reference-induced self-education (RISE), and discipline-specific literature. Students accessed these resources through authenticated logins, engaging in self-directed learning activities and participating in synchronous or asynchronous online Q&A forums to facilitate academic inquiry and knowledge consolidation.
(5) Evidence set: After the in-class presentation by students, the teacher gave structure-process-outcome evaluation. Students were invited to fill questionnaires and meaning-making reflection interview.
Control Group
The students (n = 28) in this group received the PBL teaching model consisted of 48 hours of theoretical courses and 24 hours of clinical practice session with the rest of their classmates. There were 5 routine theoretical assignments, 6 practical training reports, 1 skill-based practical examination and 1 group homework with portfolio, and standardized final examination. They were invited to one discussion session to share experience of learning OB-GYN (one study hour) 6 weeks later, nothing was recorded.
Data Collection and Procedures
A structured and timed data collection process was implemented for both the experimental and control groups to ensure consistency and comparability. Sociodemographic data included age and gender. For the Knowledge Layer: Data on academic performance (scores from assignments, reports, and exams) were collected continuously throughout the semester and aggregated after the final examination for both groups. For the Skills Layer: In the experimental group, skills layer data (flipped classroom performance and portfolio assessment) were collected immediately following the completion of related module. For the control group, the portfolio assessment scores were collected at the same point in the curriculum. For the Competency Layer: The primary outcome measure, the Chinese version of the Competency Inventory for Nursing Students (CINS),9 was administered as a self-report questionnaire to all participants (both experimental and control groups) in a single session by the end of the 10th week of the OB-GYN course.
To ensure the validity and reliability of the intervention implementation: The lead researcher conducted a standardized training session for the teacher (senior faculty members with over 5 years of experience in OB-GYN nursing education) involved in experimental, using a detailed lesson plan to ensure consistency. Both the experimental and control groups followed a predefined teaching protocol specific to their group assignment, minimizing cross-contamination of teaching methods. Where feasible, the teachers assessing the skills layer outcomes (eg, portfolios) were not informed of the group assignment of the students to reduce bias. The clinical scenario discussions were primarily managed for all students through the Online Q&A forum on the Tencent Meeting platform. As this was a standard and equally available resource for both the experimental and control groups, it was not specified as a differentiated part of the intervention.
Assessments and Analysis
The evaluation system incorporated three hierarchical domains:
- The Knowledge Layer examinations assess lower-order cognitive skills like “Remembering” (eg, recalling facts) and “Understanding” (eg, explaining concepts) (total 100 scoring/assessment): Final course grades are computed through a weighted composite of 5 routine theoretical assignments (10% total weight), 6 practical training reports (10%), skill-based practical examinations (20%), and standardized final examination (60%).
- The Skills Layer evaluations, including flipped classroom performance (50%) and portfolio assessments (50%), are designed to measure “Applying”, “Analyzing”, and “Evaluating” by having students use knowledge in new situations, deconstruct cases, and make judgments. For the control group, the peer-reviewed portfolio assessment accounts for 100%, total 100 scoring/assessment.
- The Competency Layer, assessed through reflective self-analyses, the Chinese version of 43-item CINS consisted of 6 dimensions: ethics and accountability (15 items), general clinical skills (7 items), lifelong learning (6 items), clinical biomedical science (5 items), caring (6 items), and critical thinking and reasoning (4 items).9 Each item is rated on a 7-point Likert scale, total score ranges from 43 to 301, the higher score reveals greater competency. The reliability of Chinese CINS had a Cronbach’s α value >0.80,9 which was confirmed in our study sample (Cronbach’s α = 0.90). Its construct validity has also been well-established.9
Statistical analysis: Statistical analyses were performed using SPSS version 26.0. Continuous data are presented as mean ± standard deviation. The independent samples t-test was employed to compare the scores between the two groups. To assess the joint influence of the instructional strategies for OB-GYN education and teacher-rated knowledge and skill layer performance on self-reported competency, a linear regression model was fitted. A two-tailed p-value of <0.05 was considered statistically significant.
Results
(1) Sample characteristics
The mean age of the experimental group was 21.143 ± 0.756 years, while that of the control group was 21.071 ± 0.716 years. No statistically significant difference was observed between the two groups (t (54) = 0.363, p > 0.05).
(2) Differences between the experimental group and the control group on three hierarchical domains
Evaluation results between the experimental group and the control group on three hierarchical domains were presented in Table 1. No statistically significant difference in knowledge layer was observed between the experimental group (M = 73.714, SD = 8.48) and the control group (M = 70.321, SD = 3.840), t = 1.929, P = 0.061. Statistically significant difference in skill layer was observed between the experimental group (M = 75.143, SD = 11.034) and the control group (M = 70.286, SD = 3.740), t = 2.206, P = 0.034. An independent-samples t-test demonstrated that participants in experimental group reported significantly higher competency levels (total score level and dimensional level) compared to the control group, t = 2.207–4.359, P < 0.05.
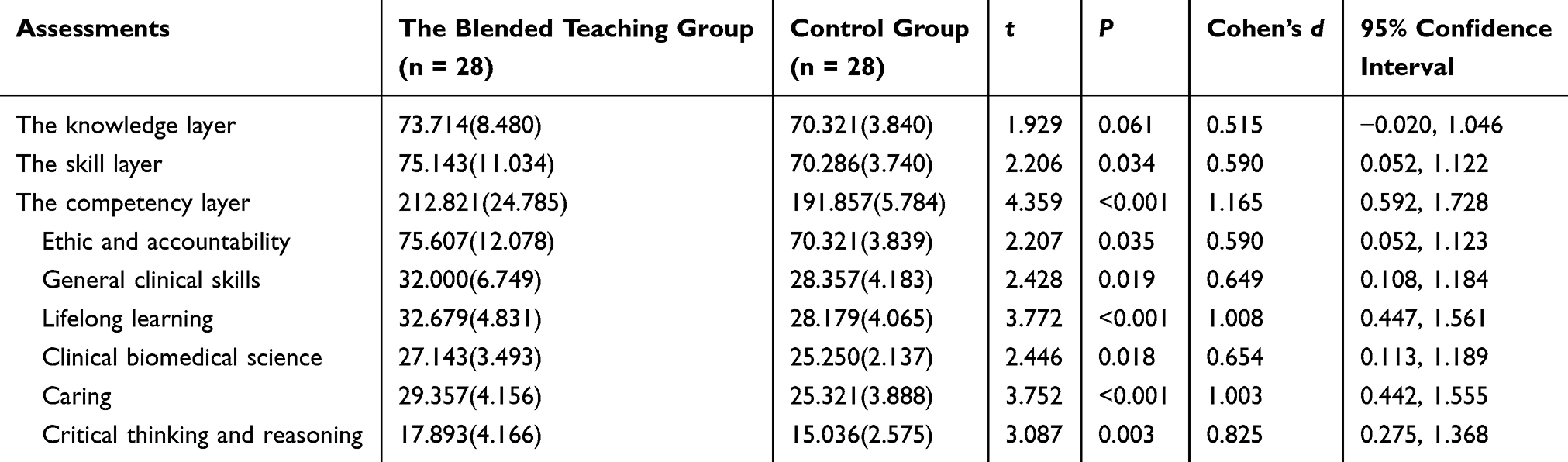 |
Table 1 Comparisons of Domains Between the Blended Teaching Group and the Control Group, Mean (Standard Deviation) |
(3) The effect of instructional strategies for OB-GYN education, teacher-rated knowledge and skill layer performance on self-reported competency
The regression model (Table 2) revealed that instructional strategies for OB-GYN education (β = 0.298, t = 3.757, P < 0.001), teacher-rated academic performance (the knowledge layer) (β = −1.062, t = −3.479, P = 0.001), and teacher-rated knowledge application and transfer skill performance (the skill layer) (β = 1.674, t = 5.431, P < 0.001) were significant predictors of self-reported competency. The overall model explained 68.5% of the variance in cardiovascular risk (R2 = 0.685, F = 40.881, P < 0.001). Additional analysis on dimensional competency showed that instructional strategies for OB-GYN education were significant predictors of self-reported lifelong learning (β = 0.437, t = 3.420, P = 0.001), clinical biomedical science (β = 0.319, t = 2.359, P = 0.022), caring (β = 0.423, t = 3.414, P = 0.001), and critical thinking and reasoning (β = 0.283, t = 2.254, P = 0.028).
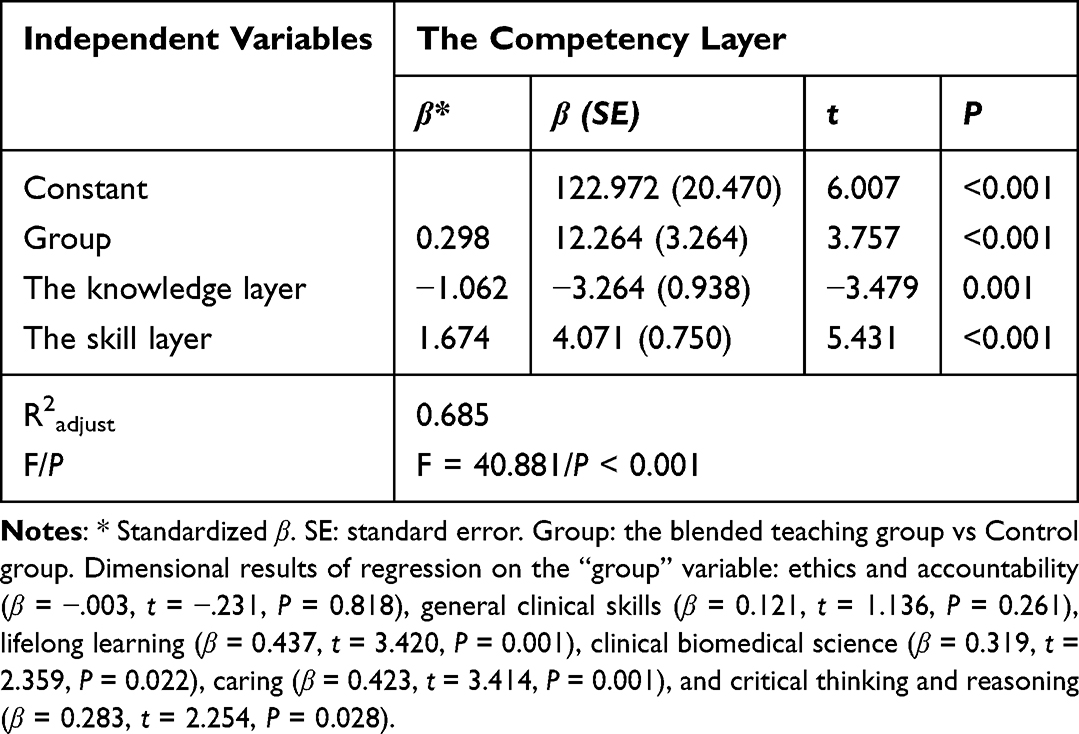 |
Table 2 Regression Results of Competency Inventory for Nursing Students |
Discussion
This paper aimed to develop an effective instructional strategy that addresses the unique learning challenges faced by male nursing students, following the design thinking steps and recommendations in the MRC framework.15 We hypothesized that a collaborative, theory-informed intervention designed with stakeholders (students, teachers, and experts) would yield a feasible and contextually relevant teaching model. Qualitative interviews were carried out to understand the students’ experiences of learning OB-GYN. Subsequently, the teachers-focus group was engaged to identify the challenges of teaching. Efforts were made to include all stakeholders in the workshop followed by a Delphi survey to design the intervention and implementation strategies in response to the challenges identified by teachers and students’ experiences. The regression analysis provides a more sophisticated understanding of what drives competency development. The model’s high explanatory power (R2 = 0.685) underscores the multifactorial nature of competency.
Design thinking14 is a human-centered approach with a set of cognitive, strategic, and practical procedures, which helped put those recommendations into practice to a great extent. Studies have benefited from the recommendations of MRC, building effective intervention models and solving clinical problems by taking stakeholders’ voice into consideration. Based on this idea and design thinking process, the OB-GYN instructional strategies were developed.15 Based on the results of the qualitative interviews with male students and challenges identified by the teachers-focus group, design thinking’s “ideate” and “prototype” steps enabled the co-creation of the C-POTE model with stakeholders. For example, the “Problem Chain” component directly reflects teachers’ challenges and students’ expressed need for clearer clinical reasoning pathways. This alignment shows how both frameworks supported a logical, participatory, and iterative development process.
The regression analysis reveals a nuanced competency development pattern. While strong skill layer performance positively predicted self-reported competency (β = 1.674, P < 0.001), the C-POTE instructional strategy itself demonstrated significant independent effects (β = 0.298, P < 0.001), suggesting its overall design fosters competency beyond discrete skill acquisition. Crucially, knowledge layer performance showed a negative relationship with competency (β = −1.062, P = 0.001), potentially indicating that traditional knowledge assessment methods may not align with developing holistic professional identity in innovative learning environments.24 The strategy specifically enhanced lifelong learning, caring, and critical thinking competencies. These findings suggest the intervention successfully promotes higher-order capabilities, with the knowledge coefficient highlighting a shift toward authentic competency-based education rather than representing an intervention weakness.
The involvement of male nursing students, which has so far been neglected, was the central base of the development of the intervention of this study. The age range, 20–23 years old, is typical for third-year undergraduate nursing students in China, as this cohort is simultaneously enrolled in core theoretical courses and their initial clinical practicums, making them the ideal population for studying the integration of theory and practice in OB-GYN nursing. While male nursing students experience negative future appraisal due to social bias, they are still open to breaking information cocoons and building positive capabilities. Studies found that male nursing students who continue to work and overcome difficulties were motivated by positive sense of belonging.25
Nursing education in schools is the first place to assist a student to think, act, and feel like a nurse. “To change the culture of nursing through intentionally forming and fostering the professional identity of the nursing discipline.” is the mission of the International Society for Professional Identity (ISPIN). However, limited by the environment and resources, it is difficult to fully foster a professional identity in nursing in school.26,27 Social biases that are deeply ingrained for a long time should be removed, or at least become loose in class. More knowledge and experience beyond books are needed, especially from the career models of the same gender identity.28,29 Yet our study extends this discourse by introducing the etic-emic perspective and male role models’ experience as practical strategies for identity formation. Unlike previous works that primarily focused on improving technical skills, our model explicitly values personal experience and aims to foster an inclusive classroom culture—addressing a gap noted in recent psychology and educational reviews.30 The etic-emic approach would facilitate the implementation of other strategies, eg, CBL and PBL.
Strengths and Limitations
This study has several strengths: (1) Interventions and implementation strategies were developed by using well-established recommendations for complex intervention construction. (2) This study adopted the multi-method approach fully considering views of groups from students, teachers, and experts, as well as individual etic-emic perspectives. These multi-dimensional perspectives enable in-depth discussions involving different individuals with different settings, which facilitates choosing appropriate implementation strategies. (3) The conversational framework23 was the only one incorporated in the final development of the intervention, as this study intended to use it to engage learners, understand their needs, and provide recommendations to enhance their learning experience. To date, few studies reported similar detailed intervention and implementation processes combining theoretical framework, practical guide, and involvement of stakeholders. This study provides the framework for future studies to develop teaching interventions and implementation strategies.
Limitations should be taken into consideration. Teachers and students involved in this study were from Wuxi Taihu University, although they were from different areas in China, they were not representatives for all students and teachers in China. Considering that the subsequent implementation study sample also comes from the same school, this limitation of this study ensures the feasibility of the implementation. The small sample size also reduces statistical power and the ability to detect small effect sizes. Geographical and cultural constraints mean that findings are influenced by local teaching practices and student demographics. We also acknowledge the potential for performance and detection bias. Future studies should include multi-center collaborations and larger samples to enhance representativeness and statistical robustness. Cross-cultural replications and the use of international competency benchmarks in future research are also encouraged.
Conclusions
This study successfully developed and preliminarily validated the instructional strategies for OB-GYN nursing education, through a systematic process guided by the Design Thinking. The findings demonstrate that the model effectively enhances students’ clinical skills and competencies-particularly in lifelong learning, caring, and critical thinking-while maintaining OB-GYN knowledge acquisition. The identified dissonance between traditional knowledge assessment and competency development underscores the model’s role in shifting the educational paradigm towards more authentic, competency-based learning. Future research should implement a controlled trial to rigorously evaluate the intervention’s effectiveness and investigate its long-term impact on professional identity formation in larger, more diverse student populations.
Data Sharing Statement
To protect participant anonymity, not all qualitative data was shared. Only relevant, de-identified quotes were included after obtaining consent for publication. Data is available from corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in compliance with the ethical principles outlined in the Declaration of Helsinki (http://www.wma.net/en/30publications/10policies/b3/index.html). The study protocol was submitted to and approved by the Ethics Committee of Rugao Boai Hospital (2025-L02).
Oral informed consent was acceptable and approved by the Ethics Committee of Rugao Boai Hospital, the oral informed consent for qualitative interview was obtained and recorded from all participants prior to their participation in the study.5 The formal written consent to participate the non-randomized controlled trial was collected at the beginning of the trial. Participants were informed about the purpose of the study, the procedures involved, and their right to withdraw at any time without any consequences.
Acknowledgments
We would like to express my sincere gratitude to Melissa S.Y. Thong for her valuable suggestions on the methodology and her meticulous polishing of the language in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Wuxi Taihu University initiation funding (No.2025THQD018), the National College Students’ Innovation and Entrepreneurship Training Program (grant number: 2024135710052), and the specific project on “Digital Transformation and Modernization Practice in Higher Education” (grant number: 2024CXJG167, 2025JSETKT040). The funders did not have any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Royce CS, Everett EN, Craig LB, et al. To the Point: advising students applying to Obstetrics and Gynecology residency in 2020 and beyond. Am J Obstet Gynecol. 2021;224(2):148–13. doi:10.1016/j.ajog.2020.10.006
2. Erenel A Ş, Yaman Sözbir Ş, Uzun Aksoy M, et al. Effect of scenario-based simulation training on the obstetrics and gynecology nursing clinical practicum. J Nurs Res. 2021;29(2):e142. doi:10.1097/jnr.0000000000000417
3. X Y, X Z, Z J. The nursing education system in the People’s Republic of China: evolution, structure and reform. Int Nurs Rev. 2000;47(4):207–217. doi:10.1046/j.1466-7657.2000.00027.x
4. Slattery MJ, Logan BL, Mudge B, Secore K, von Reyn LJ, Maue RA. An undergraduate research fellowship program to prepare nursing students for future workforce roles. J Prof Nurs. 2016;32(6):412–420. doi:10.1016/j.profnurs.2016.03.008
5. Wang CTM, Hu X, Liu Z. Male nursing undergraduates’ experience of learning Obstetrics and Gynecology Nursing: a qualitative study. Adv Med Educ Pract. 2025;16:1141–1150. doi:10.2147/AMEP.S528192
6. National H, Commission, of, the, People’s, Republic, of, China. China Health Statistics Yearbook 2023. Beijing Peking Union Medical College Press; 2024.
7. Meister T, Foessleitner P, Breuer G, et al. The impact of gender on the self-confidence of practical and surgical skills among OBGYN residents: a trinational survey. Arch Gynecol Obstet. 2024;309(1432–0711 (Electronic):2669–2679. doi:10.1007/s00404-023-07202-6
8. He Z, Yao J, De Ala MB, Zhang X. The work experience of male nursing teachers in Chinese universities: a phenomenological study. Front Psychol. 2023;14:1256934. doi:10.3389/fpsyg.2023.1256934
9. Hsu LL, Hsieh SI. Development and psychometric evaluation of the competency inventory for nursing students: a learning outcome perspective. Nurse Education Today. 2013;33(5):492–497. doi:10.1016/j.nedt.2012.05.028
10. Iduye D, Vukic A, Waldron I, et al. Educators’ strategies for engaging diverse students in undergraduate nursing education programs: a scoping review protocol. JBI Evidence Synth. 2021;19(5):1178–1185. doi:10.11124/JBIES-20-00039
11. Siemens G, Conole G. Connectivism: design and delivery of social networked learning. Int Rev Res Open Distance Learn. 2011;12(3):1.
12. An-Li J. Interpretation of the National Standards for Nursing Teaching Quality: educational Plan. Chin J Nurs Educ. 2019;16(1):12–15.
13. Rezakhani Moghaddam H, Aghamohammadi V, Jafari MA-O, Absalan M, Nasiri KA-O. Challenges faced by nursing students to work with nursing personnel: a qualitative study. Adv Med Educ Pract. 2020;11(1179–7258 (Print):313–319. doi:10.2147/AMEP.S246901
14. Plattner H, Meinel C, Weinberg U. Design Thinking. Springer; 2009.
15. Wallner M, Mayer H, Adlbrecht L, et al. Theory-based evaluation and programme theories in nursing: a discussion on the occasion of the updated Medical Research Council (MRC) Framework. Int J Nurs Stud. 2023;140:104451. doi:10.1016/j.ijnurstu.2023.104451
16. Denninger N-E, Brefka S, Skudlik S, et al. Development of a complex intervention to prevent delirium in older hospitalized patients by optimizing discharge and transfer processes and involving caregivers: a multi-method study. Int J Nurs Stud. 2024;150:104645. doi:10.1016/j.ijnurstu.2023.104645
17. Litcanu M, Prostean O, Oros C, Mnerie AV. Brain-writing vs. Brainstorming case study for power engineering education. Procedia Soc Behav Sci. 2015;191:387–390. doi:10.1016/j.sbspro.2015.04.452
18. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:1–15. doi:10.1186/1748-5908-4-50
19. Powell BJ, Waltz TJ, Chinman MJ, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10:1–14. doi:10.1186/s13012-015-0209-1
20. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–1015. doi:10.1046/j.1365-2648.2000.t01-1-01567.x
21. Zhan ZLK, Lin Z, Zhong B, Mai Z, Li W. Interdisciplinary education for cultural inheritance (C-STEAM): 6C model and its typical case. Mod Distance Educ Res. 2020a;32(2):29–38.
22. Zhan Z, He W, Cheng S, Lu J, Han Y, Han Y. K12 teacher-student interaction patterns in the smart classrooms. Int J Innovation Learning. 2021b;29(3):267–286. doi:10.1504/IJIL.2021.114511
23. Laurillard D. Rethinking University Teaching: A Conversational Framework for the Effective Use of Learning Technologies. Routledge; 2013.
24. Hammoud MM, Stansfield Rb Fau - Katz NT, Katz Nt Fau - Dugoff L, et al. The effect of the obstetrics and gynecology clerkship on students’ interest in a career in obstetrics and gynecology. Am J Obstet Gynecol. 2006;195(1097–6868 (Electronic)):1422–1466. doi:10.1016/j.ajog.2006.07.044
25. Dos Santos LM. Male nursing practitioners and nursing educators: the relationship between childhood experience, social stigma, and social bias. Int J Environ Res Public Health. 2020;17(14):4959. doi:10.3390/ijerph17144959
26. Hsieh B. The importance of orientation: implications of professional identity on classroom practice and for professional learning. Teachers Teaching. 2015;21(2):178–190. doi:10.1080/13540602.2014.928133
27. Nagle L. An Exploration of the Factors Impacting on Pre-Professional Identity Formation During Legitimate Peripheral Participation Within Nursing Clinical Placement. University of Limerick; 2021.
28. Dinella LM, Fulcher M, Weisgram ES. Sex-typed personality traits and gender identity as predictors of young adults’ career interests. Arch Sex Behav. 2014;43:493–504. doi:10.1007/s10508-013-0234-6
29. Ndou NP, Moloko-Phiri SS. Four-year diploma male students’ experiences in a profession traditionally perceived as a female domain at a selected public college of nursing in Limpopo, South Africa. Curationis. 2018;41(1):1–6. doi:10.4102/curationis.v41i1.1932
30. Helfrich H. Beyond the dilemma of cross-cultural psychology: resolving the tension between etic and emic approaches. Culture Psychol. 1999;5(2):131–153. doi:10.1177/1354067X9952002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Chinese Male Nursing Undergraduates’ Experience of Learning Obstetrics and Gynecology Nursing: A Qualitative Study
Wang C, Liu Z, Thong MSY, Hu X
Advances in Medical Education and Practice 2025, 16:1141-1150
Published Date: 30 June 2025