Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Gender Divergence in COPD Phenotypes and Narrowing Urban–Rural Diagnostic Gaps: A Surveillance Study in Chongqing, China, 2020–2024
Authors Tan Q ![]() , Gao Y, Lv X, Jiao Y, Lian J, Ding X
, Gao Y, Lv X, Jiao Y, Lian J, Ding X
Received 25 February 2026
Accepted for publication 9 May 2026
Published 25 May 2026 Volume 2026:21 550948
DOI https://doi.org/10.2147/COPD.S550948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Qiang Tan,* Yang Gao,* Xiaoyan Lv, Yan Jiao, Jian Lian, Xianbin Ding
Institute of Chronic and Non‑communicable Disease Control and Prevention, Chongqing Center for Disease Control and Prevention, Chongqing, 400042, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianbin Ding, Institute of Chronic and Non-Communicable Disease Control and Prevention, Chongqing Center for Disease Control and Prevention, No. 187, Tongxing North Road, Liangjiang District, Chongqing, 400707, People’s Republic of China, Email [email protected] Jian Lian, Institute of Chronic and Non-communicable Disease Control and Prevention, Chongqing Center for Disease Control and Prevention, No. 187, Tongxing North Road, Beibei District, Chongqing, 400707, People’s Republic of China, Email [email protected]
Purpose: To analyze epidemiological trends of COPD, chronic bronchitis, and emphysema in Chongqing, China (2020– 2024), and assess spirometry-confirmed diagnosis rates.
Patients and Methods: Data were obtained from the Chongqing Chronic Disease Surveillance System (CCDSS), including 975,421 incident cases and 1,244,978 prevalent cases among residents aged ≥ 15 years, and 239,086 deaths from all age groups. Age‑standardized rates were calculated using the 2000 Chinese census population. Type 1 (spirometry‑confirmed) COPD diagnosis rate was analyzed by urban–rural residence.
Results: Age-standardized prevalence per 100,000 increased for COPD (732.06 to 1,424.54), emphysema (182.51 to 536.71), and chronic bronchitis (309.48 to 1,021.75). COPD and emphysema were male-predominant; chronic bronchitis became female-predominant after 2023. Rural burden was consistently higher. Type 1 diagnosis rate rose sharply from 6.96% (2022) to 26.04% (2024), with urban-rural gap narrowing to 0.77 percentage points.
Conclusion: The rising prevalence mainly reflects improved case ascertainment. Female‑predominant chronic bronchitis highlights the need for sex‑specific public health strategies. The rapid increase in spirometry‑confirmed diagnosis and near‑elimination of urban–rural disparity demonstrate a successful model for diagnostic standardization in primary care.
Keywords: chronic obstructive pulmonary disease, epidemiology, surveillance, gender differences, urban-rural disparity, spirometry, Chongqing
Introduction
Chronic Obstructive Pulmonary Disease (COPD) represents a monumental challenge to global public health, currently ranking as the third leading cause of death worldwide and contributing significantly to the global burden of disability-adjusted life years (DALYs).1 This burden is disproportionately concentrated in low- and middle-income countries (LMICs), with China shouldering approximately one-third of the global economic and health toll associated with COPD.2–4 The persistently high prevalence and mortality are driven by complex and interacting factors, including rapid population aging, high rates of active and passive smoking, and sustained exposure to environmental particulate matter (PM) and household air pollution (HAP).1,5 These persistent and widespread risk factors necessitate highly resilient and data-driven public health strategies globally.6
Effective control of Chronic Respiratory Diseases (CRDs) requires an integrated understanding of the entire disease spectrum.7 According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2024 strategy, COPD is defined by persistent airflow limitation, typically confirmed by post-bronchodilator spirometry (FEV1/FVC <0.7).8 In this study, we report COPD, emphysema, and chronic bronchitis as hierarchical categories based on diagnostic severity (COPD > emphysema > chronic bronchitis). This approach provides mutually exclusive estimates for public health surveillance while recognizing their pathological continuum.9 Despite this recognition, a major scientific gap persists globally: while traditional cross-sectional population surveys provide valuable snapshots of symptom-based prevalence, they are inherently limited by high cost, low spatial-temporal resolution, and considerable time lag.10 Consequently, there remains a critical dearth of high-fidelity, real-time epidemiological data, particularly concerning true disease incidence, mortality dynamics, and the efficacy of standardized diagnostic practices (like spirometry confirmation) in real-world settings.6,10
The need for high-resolution, continuous data is particularly acute in Chongqing, a region heavily burdened by chronic respiratory diseases.2,11 As a core city in this region, Chongqing is situated in the upper reaches of the Yangtze River, with a total area of 82,400 square kilometers. Its topography is predominantly mountainous, characterized by widespread karst landscapes, significant relief variations, and diverse landform types. According to the sixth national population census of China, Chongqing has a permanent population of 28.84 million. It is a composite municipality that integrates substantial industrial and agricultural sectors, as well as extensive urban and rural areas. With jurisdiction over 38 districts and counties (26 districts, 8 counties, and 4 autonomous counties), Chongqing is representative of both southwestern China and its characteristic mountainous environments.12 Although the data in this study are derived exclusively from Chongqing, the city is representative of the broader Southwest China region in terms of its socioeconomic and geographic characteristics. Large-scale epidemiological studies in China have reported that the prevalence of COPD among adults aged 40 and above in Chongqing is 18.7%.13 This figure not only exceeds the national average of 13.7%14 but is also higher than rates reported for Beijing (17.1%),15 Shanghai (11.5%),16 Tianjin (9.4%),17 and Guizhou (10.7%)18 during a comparable period. Given this significant disease burden, the demand for granular, temporally continuous data is especially pronounced. However, traditional sampling-based methods are fundamentally limited in their capacity to capture the fine-scale spatiotemporal heterogeneity and dynamic evolution of the disease burden. Consequently, they are inadequate for reliably estimating true incidence rates or effectively monitoring the quality of clinical care.10,19 To overcome this methodological deficiency and provide continuous, high-fidelity data, Chongqing established the Chronic Disease Surveillance System (CCDSS). This system, which has been in place since 2017, represents a unique, mandatory, city-wide platform for the comprehensive reporting of morbidity and case data for COPD, chronic bronchitis, and emphysema among all residents aged ≥15 years, along with mortality data across all age groups.20
The CCDSS significantly advances the field by offering a continuous and robust alternative to intermittent surveys. Its strength lies in a sophisticated, multi-level quality control (QC) system that ensures data integrity. This QC process includes a dual-track reporting mechanism (physician input via structured electronic medical records and three-tier audits by the local Centers for Disease Control and Prevention), real-time anomaly detection, and crucial cross-verification of mortality data with public safety and civil affairs records. By the study endpoint, this system had accumulated information on over 1.2 million prevalent cases. This infrastructure allows for the reliable estimation of key longitudinal epidemiological indicators, such as true annual incidence and mortality, which are often poorly captured or lagged in other national datasets.5 Furthermore, it provides the essential denominator for assessing the quality of care, specifically by tracking the proportion of spirometry-confirmed (Type 1) COPD diagnoses. The ability to conduct such analyses is critical for designing regionally tailored intervention strategies suitable for Chongqing’s unique demographic and environmental profile.20
Utilizing the comprehensive data from the CCDSS spanning January 1, 2020, to December 31, 2024, this study provides a systematic and detailed epidemiological analysis of COPD, chronic bronchitis, and emphysema among Chongqing residents aged ≥ 15 years. Specifically, we aim to: (1) precisely calculate and analyze the age-standardized incidence, prevalence, and mortality rates for all three conditions, examining the temporal dynamics over the study period; (2) investigate key demographic heterogeneities, particularly focusing on age-specific burdens and evidence for sex-specific phenotypes, such as the differential patterns observed between emphysema and chronic bronchitis; and (3) assess the effectiveness and equity of regional public health policies by tracking the trend and urban-rural disparity of the spirometry-confirmed (Type 1) COPD diagnosis rate. By leveraging this unique, high-fidelity monitoring platform, this research fills a critical gap in real-time, comprehensive CRD epidemiological data for Chongqing, providing robust evidence to inform region-specific prevention guidelines and contributing a model for standardized chronic disease surveillance in complex, high-burden environments globally.
Data and Methods
Data Source
Data Access Statement
The data used in this study were obtained from the CCDSS, a mandatory, city-wide surveillance platform established and maintained by the Chongqing Center for Disease Control and Prevention (Chongqing CDC). As this is a governmental public health surveillance system, data access was granted through official administrative approval within the Chongqing CDC. The research team, composed of staff members from the Institute of Chronic and Non-communicable Disease Control and Prevention at Chongqing CDC, accessed the data as part of their routine public health surveillance duties and research authorization. The study protocol, including data access procedures, was approved by the Ethical Review Committee of Chongqing Center for Disease Control and Prevention (Approval Number: KY-2025-004-1). Due to institutional policies and privacy regulations governing this governmental surveillance data, the underlying individual-level data are not available for external distribution.
Patient Population
Data on the incidence and prevalence of COPD, chronic bronchitis, and emphysema were obtained from the chronic respiratory disease surveillance module of the CCDSS. Collected variables included date of death (occurring within the study period), sex, date of initial diagnosis, date of medical visits (up to December 31, 2024), diagnostic methods, and residential address. Target diseases were defined according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes: chronic bronchitis (J40–J42), emphysema (J43), and COPD (J44). Incident cases meeting the inclusion criteria were extracted from the system, comprising 975,421 cases (male: 604,369; female: 371,052). Prevalent cases as of December 31, 2024 (the study endpoint) totaled 1,244,978 (male: 774,206; female: 470,772). Population composition data for each district/county were derived from demographic statistics published by the respective district/county statistical authorities.
Hierarchical Classification of Chronic Respiratory Diseases
In the CCDSS, patients are assigned to mutually exclusive disease categories based on ICD-10 codes and a hierarchical severity principle: COPD (J44) > emphysema (J43) > chronic bronchitis (J40–J42). This approach avoids double-counting and ensures robust population-level surveillance. Importantly, J44 reflects physician-recorded clinical COPD diagnoses, which may or may not be confirmed by spirometry (the Type 1 diagnosis rate quantifies this gap). J43 and J40–J42 represent patients diagnosed with emphysema or chronic bronchitis without a concurrent COPD diagnosis; these individuals may or may not have airflow limitation but are kept separate to avoid artificially inflating COPD prevalence and to enable unbiased assessment of real-world diagnostic practices. Thus, while we fully recognize the underlying pathological continuum, our classification is methodologically appropriate for evaluating population diagnostic quality and disease burden in routine surveillance settings.
COPD Mortality Data
Data on mortality related to COPD, emphysema, and chronic bronchitis were obtained from the mortality surveillance module of the Chongqing Chronic Disease Surveillance System (CCDSS), which is based on official death certificates completed across all districts of Chongqing. Extracted variables included age at death, sex, residential area, date of death, and the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD‑10) code for the underlying cause of death. Death cases were included if the underlying cause was coded to chronic bronchitis (J40–J42), emphysema (J43), or COPD (J44). Cases in which these conditions were listed only as secondary or contributing causes (not the underlying cause) were excluded from analysis. A total of 239,086 deaths meeting this criterion were analyzed, including 140,904 males and 98,182 females.
Data Cleaning and Case Verification
Duplicate records were identified and removed using unique individual identification information. Extreme outliers in demographic characteristics and diagnostic dates were verified against original medical records for correction or exclusion. Incident cases were defined as patients with a first-time diagnosis of COPD, emphysema, or chronic bronchitis during 2020–2024, and were cross-checked against historical CCDSS records to confirm no prior diagnosis of these diseases before the study period. Prevalent cases were defined as individuals who were alive and had a confirmed diagnosis of any target disease as of December 31 each year from 2020 to 2024, including those diagnosed prior to the study period. Mortality cases referred to all-age deaths during 2020–2024 with the underlying cause of death coded as any of the three target diseases.
Quality Control
CCDSS utilizes a rigorous, multi-tier quality control framework to ensure data accuracy and completeness, as detailed in our prior methodological publication.20 In brief, data were collected via a dual-track reporting mechanism integrating structured electronic medical records and automated extraction of core diagnostic variables. A three-level audit, real-time anomaly detection, and cross-verification of mortality data with public security and civil affairs databases were implemented. Annual monitoring of data completeness and underreporting was conducted to sustain high-quality surveillance.
Statistical Analysis
All analyses were conducted using R version 4.5.1, with packages including dplyr for data cleaning, epiR for calculating standardized rates, and ggplot2 for visualizations. Age-standardized rates (prevalence, incidence, and mortality) were computed using the direct standardization method, with data from the 2000 Chinese population census as the standard population to adjust for differences in age structure across years.
The Type 1 (spirometry‑confirmed) COPD diagnosis rate was defined as the proportion of clinically diagnosed COPD cases (ICD‑10 J44) confirmed by spirometry according to GOLD 2024 criteria (post‑bronchodilator FEV1/FVC < 0.7). Spirometry status was obtained directly from a dedicated structured field in electronic medical records, not inferred from ICD‑10 coding. The ICD‑10 code J44 was used only to define the denominator (all clinical COPD cases), while the numerator reflected actual spirometry test results.
Residential addresses were classified as urban or rural based on economic development level. Urban areas included 11 districts: Yuzhong, Jiulongpo, Shapingba, Jiangbei, Yubei, Banan, Nan’an, Beibei, Dadukou, High-Tech Zone, and Liangjiang New Area. All other areas were defined as rural.
Because this study is based on complete population surveillance data covering all eligible residents of Chongqing rather than a sample survey, the reported rates represent true population parameters without sampling error. Therefore, we present absolute rate changes and rate differences to describe temporal trends and demographic disparities, and we do not perform hypothesis tests (eg., p-values). Under complete population coverage, even minor annual fluctuations would yield statistically significant p-values that lack meaningful public health interpretation, making absolute measures more informative for surveillance purposes.
Results
Prevalence of COPD, Emphysema, and Chronic Bronchitis
The age-standardized prevalence rates of COPD, emphysema, and chronic bronchitis in Chongqing from 2020 to 2024 are presented in Figure 1. All three diseases exhibited a consistent upward trend over the five-year period. COPD had the highest overall prevalence, increasing from 732.06 per 100,000 population in 2020 to 1,424.54 in 2024. Emphysema and chronic bronchitis also showed significant increases, with prevalence rates rising from 182.51 to 536.71 and from 309.48 to 1,021.75 per 100,000, respectively.
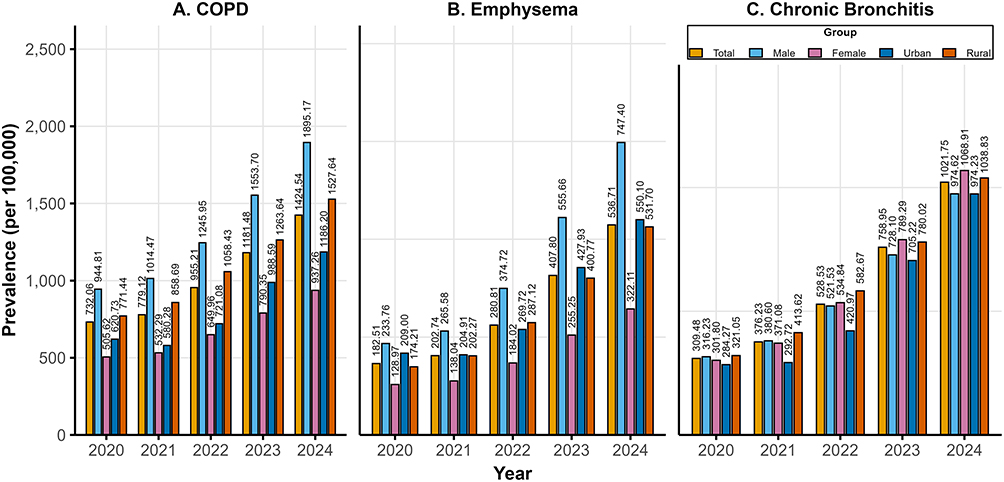 |
Figure 1 Trends in Age-Standardized Prevalence of COPD, Emphysema, and Chronic Bronchitis from 2020 to 2024 in Chongqing, Stratified by Gender and Urban-Rural Residence. (A: COPD; B: Emphysema; C: Chronic Bronchitis). |
Gender-specific analysis revealed a marked male predominance in COPD and emphysema. For instance, in 2024, the male prevalence of COPD (1,895.17 per 100,000) was approximately twice that of females (937.26 per 100,000), while emphysema showed a similar pattern (747.40 vs. 322.11 per 100,000). Chronic bronchitis exhibited a more balanced gender distribution, with female prevalence surpassing male prevalence in 2023 (789.29 vs. 728.10 per 100,000) and 2024 (1,068.91 vs. 974.62 per 100,000).
Urban-rural disparity analysis indicated that age-standardized prevalence rates for all three diseases were consistently higher in rural areas than in urban areas. For COPD, the prevalence was 771.44 per 100,000 in rural areas versus 620.73 per 100,000 in urban areas in 2020; by 2024, it had risen to 1,527.64 and 1,186.20 per 100,000, respectively, with rural areas remaining higher. Similar trends were observed for emphysema and chronic bronchitis, suggesting a greater disease burden in rural regions.
As detailed in Table 1 (chronic bronchitis), Table 2 (emphysema) and Table 3 (COPD), age-specific prevalence analysis highlighted a steep increase with advancing age for all diseases. Prevalence remained low in the 15–19 age group (eg., COPD ranged from 3.29 to 13.53 per 100,000) but rose sharply in older demographics. Individuals aged ≥60 years showed exponential increases. For example, COPD prevalence reached 4,633.24 per 100,000 in those aged 60–64 in 2024, peaking at 14,714.32 per 100,000 in the ≥85 age group. Emphysema and chronic bronchitis followed similar trajectories, with the highest burdens observed in the oldest age groups.
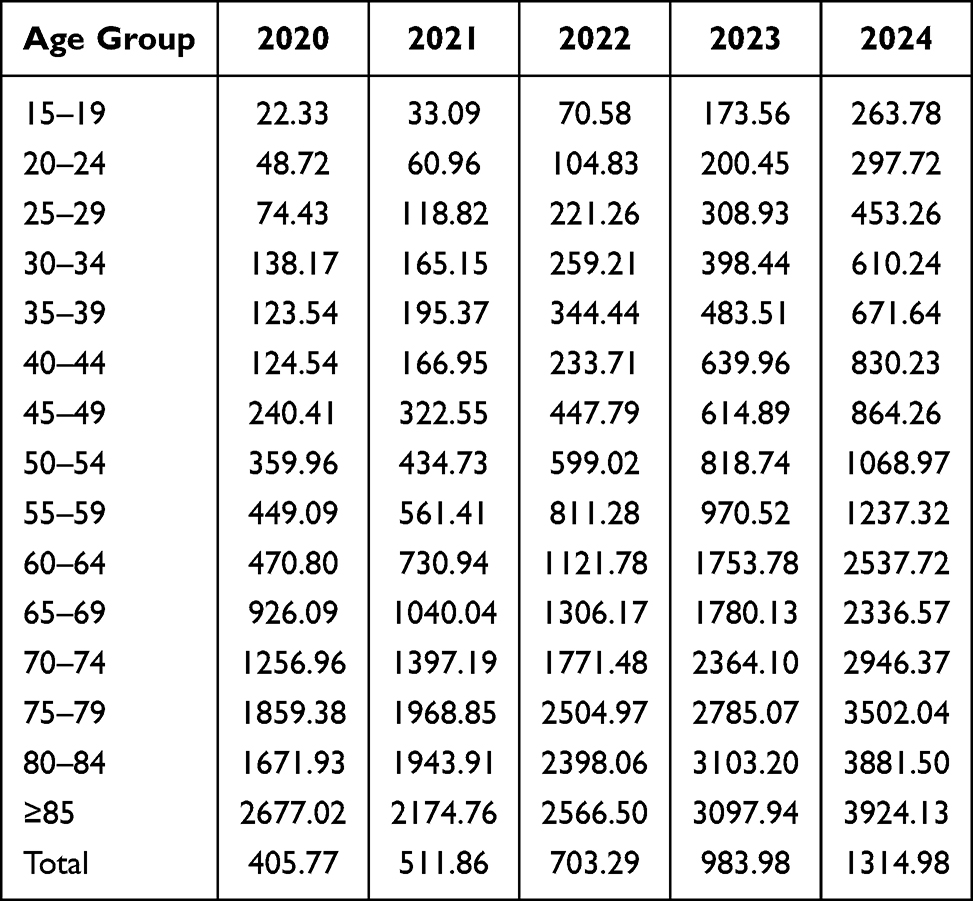 |
Table 1 Prevalence Rates of Chronic Bronchitis (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
 |
Table 2 Prevalence Rates of Emphysema (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
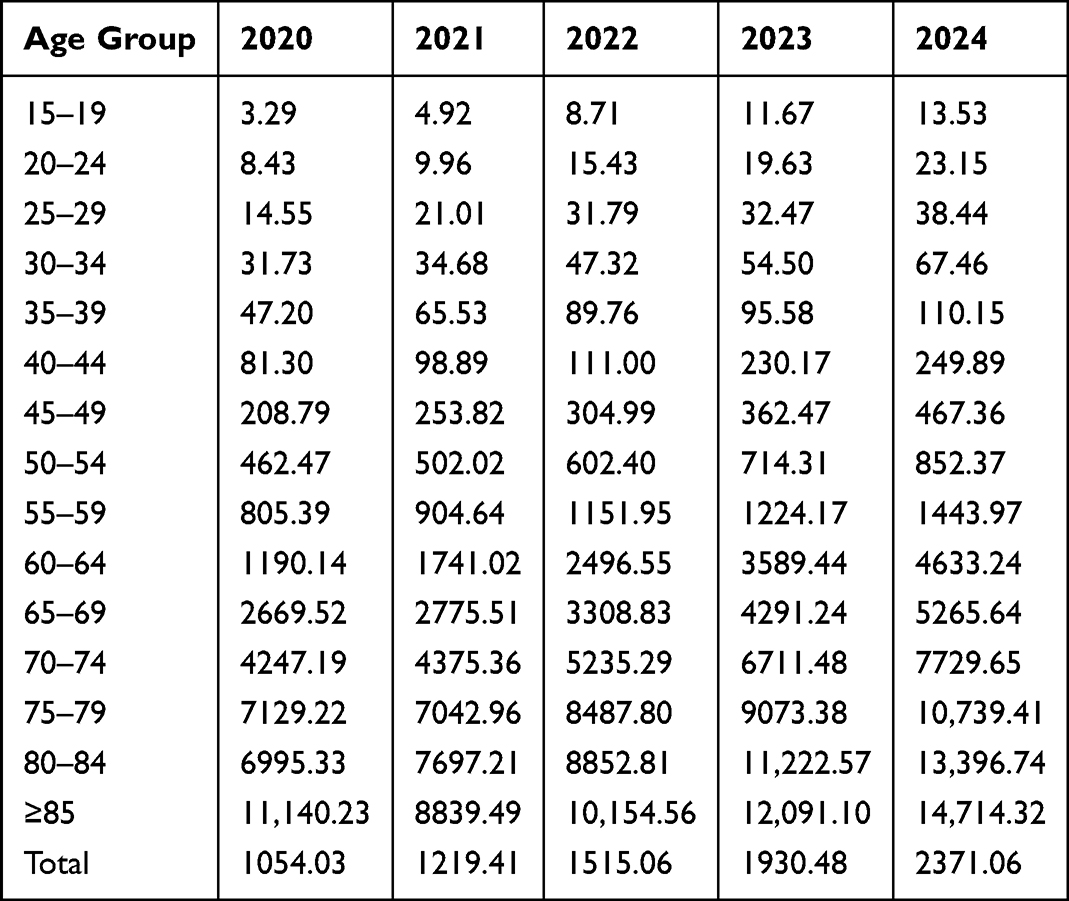 |
Table 3 Prevalence Rates of COPD (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
Incidence of COPD, Emphysema, and Chronic Bronchitis
The age-standardized incidence rates are shown in Figure 2, with varying temporal patterns across diseases. COPD incidence fluctuated, peaking at 350.52 per 100,000 person-years in 2020, dropping to a low of 147.84 in 2021, and subsequently recovering to 231.04 in 2024. Emphysema showed a similar pattern, with the highest incidence in 2020 (178.14 per 100,000) and the lowest in 2021 (47.89 per 100,000). In contrast, chronic bronchitis incidence demonstrated a steady increase from 142.22 per 100,000 in 2020 to 265.35 in 2024.
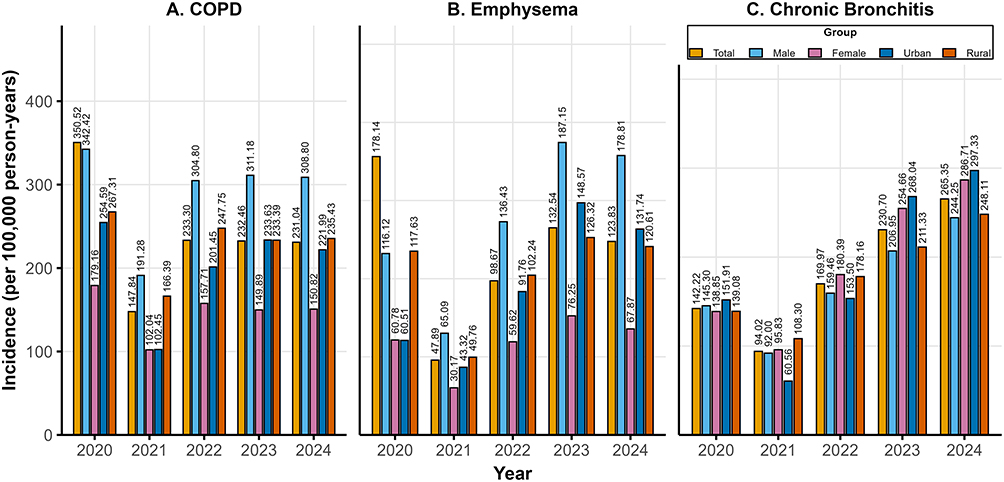 |
Figure 2 Trends in Age-Standardized Incidence of COPD, Emphysema, and Chronic Bronchitis from 2020 to 2024 in Chongqing, Stratified by Gender and Urban-Rural Residence. (A: COPD; B: Emphysema; C: Chronic Bronchitis). |
Gender analysis indicated a consistent male predominance in the incidence of all diseases. However, the gender gap was narrower for chronic bronchitis, with female incidence exceeding male incidence in 2023 and 2024. Urban-rural differences in incidence were more complex. For COPD, incidence was higher in urban areas in 2020 but was surpassed by rural areas from 2021 onwards. Emphysema incidence was significantly higher in rural areas in 2020, with the gap narrowing subsequently. Chronic bronchitis incidence was generally higher in urban areas for most years.
Age-specific incidence rates, detailed in Table 4 (chronic bronchitis), Table 5 (emphysema) and Table 6 (COPD), revealed a steep increase with age for all conditions. Individuals aged ≥60 years showed exponential rises. In 2024, COPD incidence reached 747.25 per 100,000 in the 60–64 age group and peaked at 6,050.21 per 100,000 in those aged ≥85.
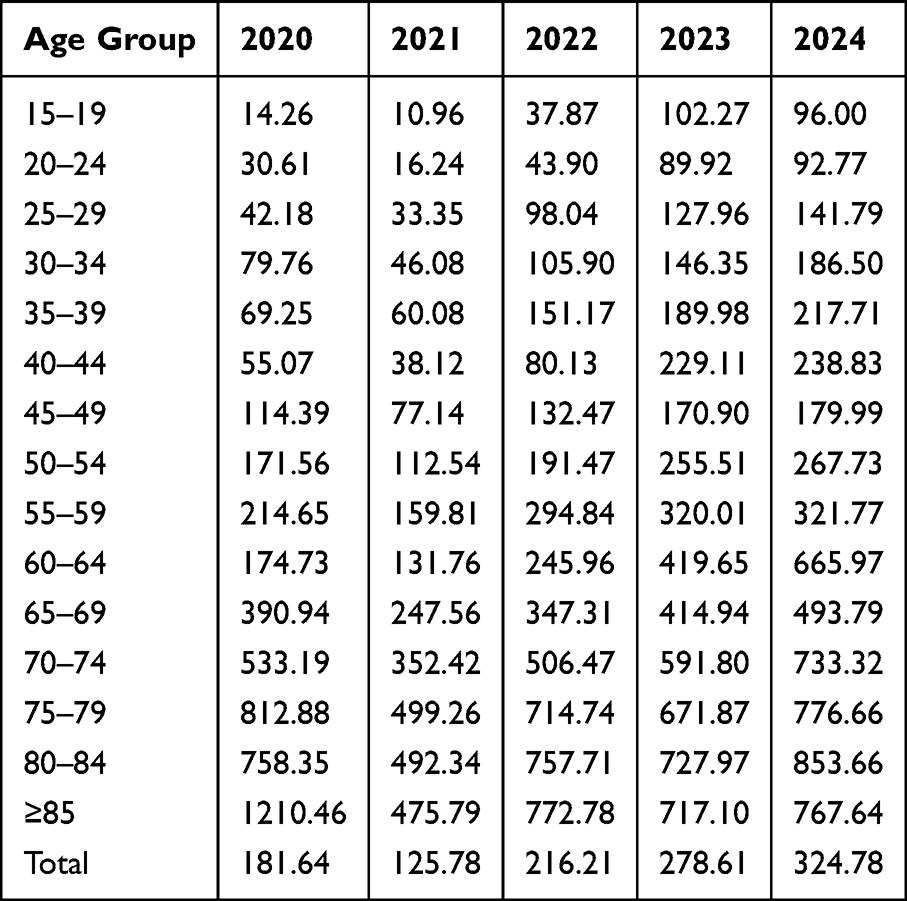 |
Table 4 Incidence Rates of Chronic Bronchitis (Per 100,000 Person-Years), by Age Group and Year, Chongqing, 2020–2024 |
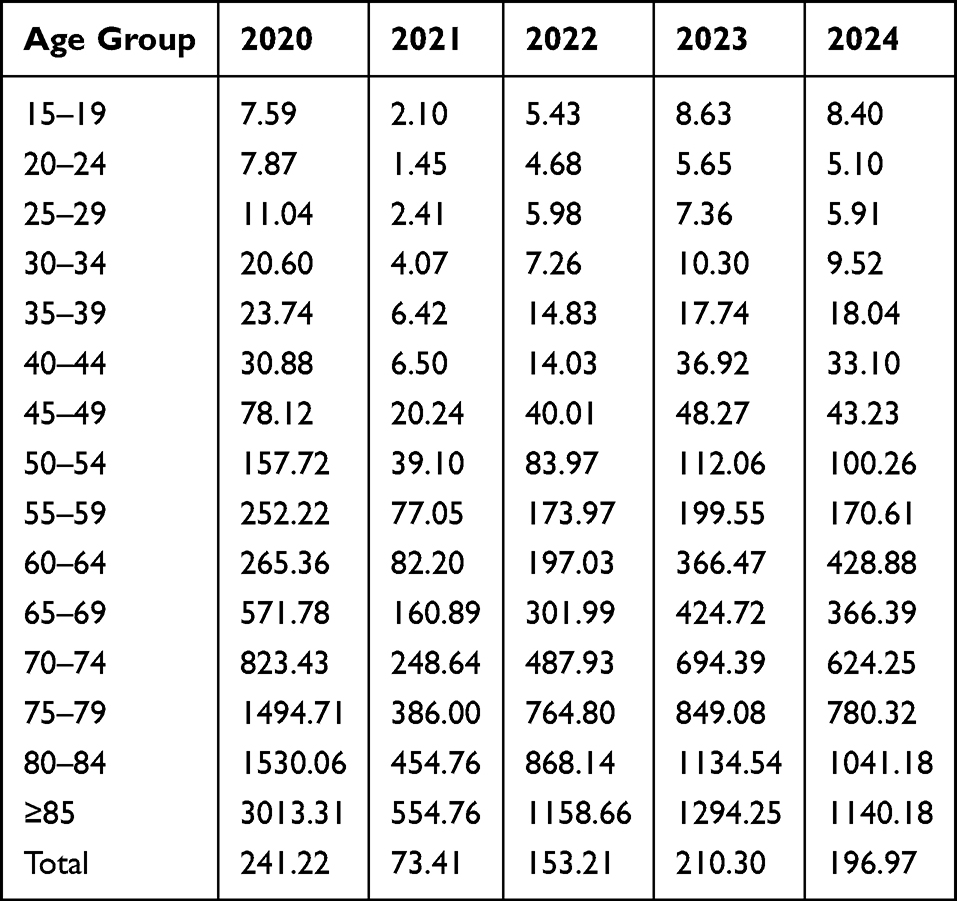 |
Table 5 Incidence Rates of Emphysema (Per 100,000 Person-Years), by Age Group and Year, Chongqing, 2020–2024 |
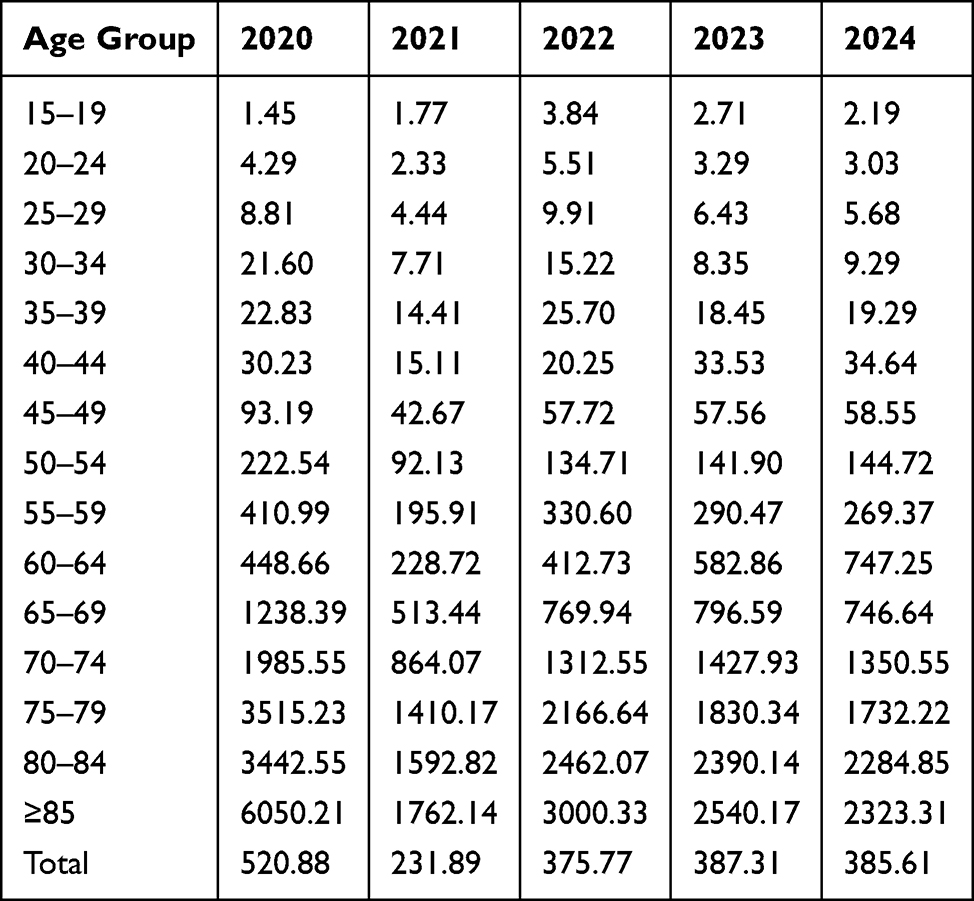 |
Table 6 Incidence Rates of COPD (Per 100,000 Person-Years), by Age Group and Year, Chongqing, 2020–2024 |
Mortality Caused by COPD, Emphysema, and Chronic Bronchitis
As presented in Figure 3, among the age-standardized mortality rates for the three diseases, COPD exhibited the highest mortality. The rate fluctuated from 28.76 per 100,000 in 2020, declined to a nadir of 16.82 in 2023, and rebounded to 22.53 in 2024. Emphysema and chronic bronchitis showed lower but generally increasing mortality: emphysema rose from 4.28 to 6.19 per 100,000, while chronic bronchitis fluctuated between 8.17 and 11.17 per 100,000.
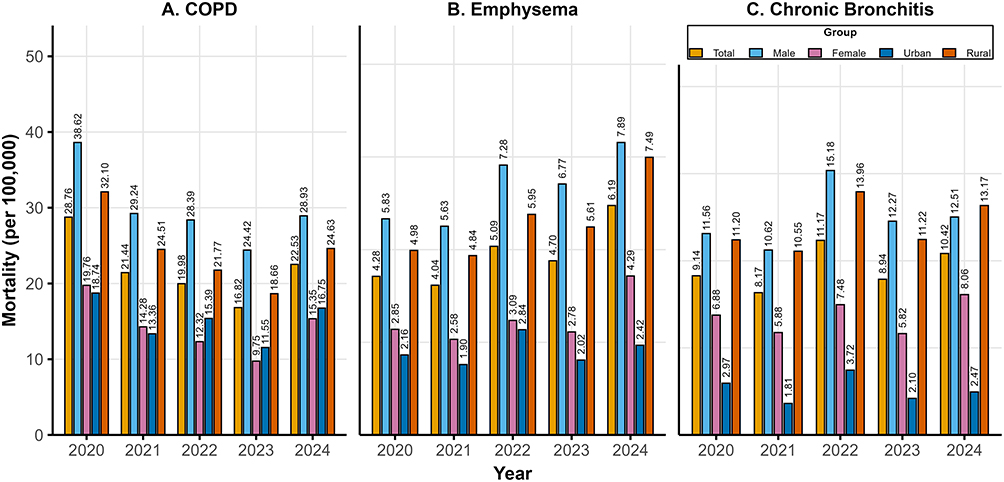 |
Figure 3 Trends in Age-Standardized Mortality of COPD, Emphysema, and Chronic Bronchitis from 2020 to 2024 in Chongqing, Stratified by Gender and Urban-Rural Residence. (A: COPD; B: Emphysema; C: Chronic Bronchitis). |
Gender analysis consistently showed higher mortality among males, although the gap was narrower for chronic bronchitis. Rural areas consistently demonstrated higher age-standardized mortality rates than urban areas for all three diseases, although the disparities narrowed over time.
Age-specific mortality rates in Table 7 (chronic bronchitis), Table 8 (emphysema) and Table 9 (COPD) revealed a steep age gradient. Mortality was negligible in individuals younger than 30 years but escalated exponentially with age. Those aged ≥80 years had the highest mortality: COPD mortality reached 1,351.12 per 100,000 in 2020, declining to 711.61 per 100,000 in 2024.
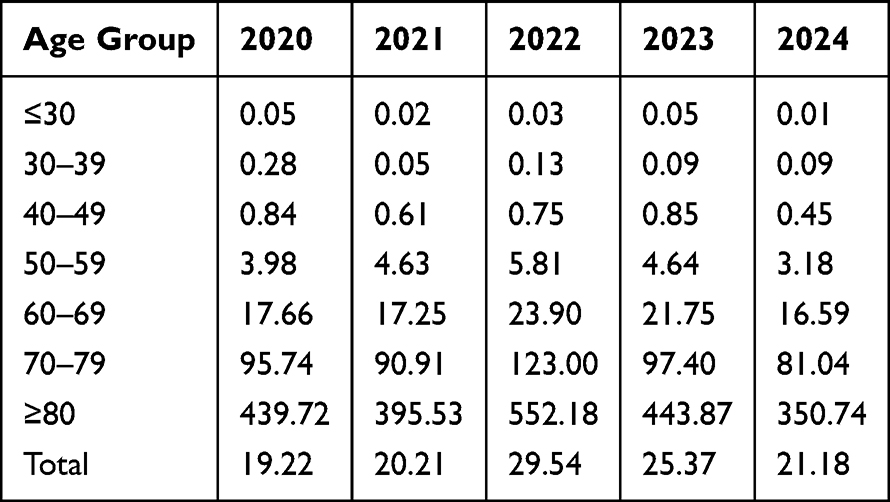 |
Table 7 Mortality Rates of Chronic Bronchitis (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
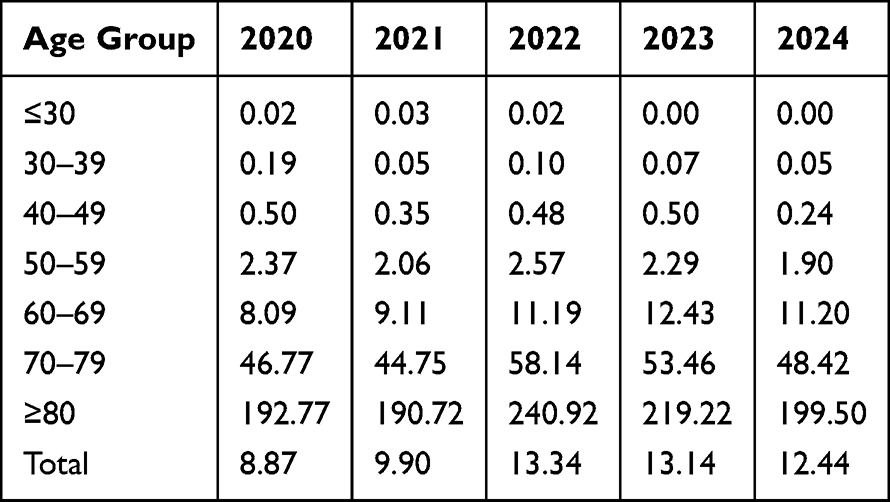 |
Table 8 Mortality Rates of Emphysema (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
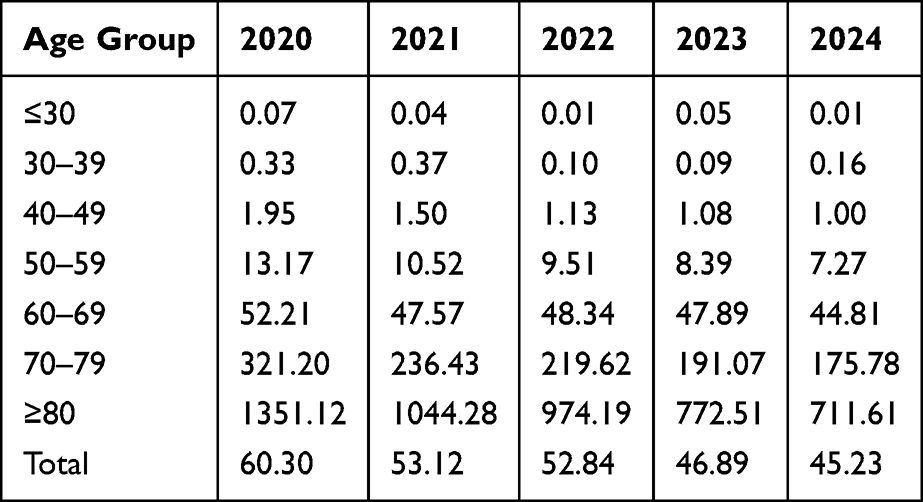 |
Table 9 Mortality Rates of COPD (Per 100,000 Population), by Age Group and Year, Chongqing, 2020–2024 |
The Type 1 Diagnosis Rate of COPD
Figure 4 illustrates the Type 1 diagnosis rate of COPD (defined by the GOLD 2024 criteria as post-bronchodilator FEV1/FVC <0.7) stratified by urban-rural residence. The overall diagnosis rate showed a U-shaped trend, decreasing from 11.66% in 2020 to a nadir of 6.96% in 2022, followed by a sharp rise to 26.04% in 2024.
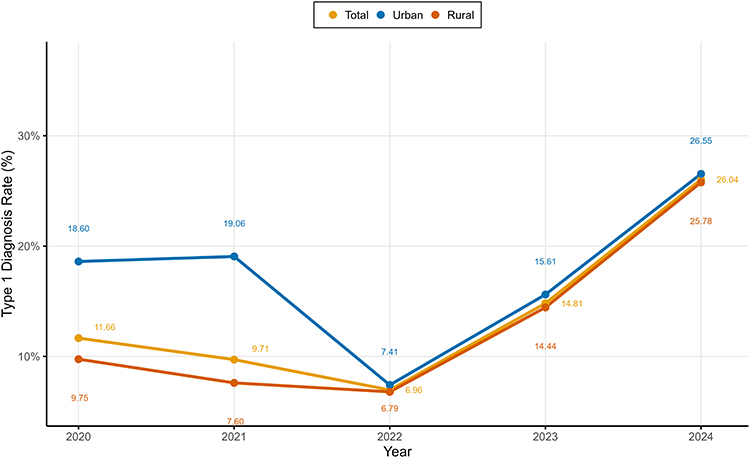 |
Figure 4 Trends in Type 1 Diagnosis Rate of COPD from 2020 to 2024 in Chongqing, Stratified by Urban-Rural Residence. |
Urban areas consistently had higher diagnosis rates than rural areas, though the gap narrowed substantially over time. In 2020, the urban diagnosis rate (18.60%) was nearly double that of rural areas (9.75%). By 2024, this difference had shrunk to 0.77 percentage points (26.55% vs. 25.78%). The most notable increase occurred between 2023 and 2024, where rates surged in both settings, likely reflecting improved diagnostic access or heightened clinical awareness in the post-pandemic period.
Discussion
This multi-dimensional epidemiological analysis of COPD, emphysema, and chronic bronchitis among residents aged ≥15 years in Chongqing from 2020 to 2024 reveals distinct trends in disease burden, shaped by diagnostic practices, demographic factors, and the unique context of the pandemic period. Previous studies have documented the high prevalence of COPD in China, with a disproportionately heavy burden concentrated in resource-limited western regions.2 National population surveys have identified tobacco smoking, ambient air pollution, undernutrition, and early-life respiratory events as major predisposing factors for COPD.14,21 Our findings from Chongqing are consistent with these prior reports, demonstrating a substantial and rising burden of COPD and emphysema, especially among elderly individuals and male residents.2,14
However, this study provides novel evidence by leveraging a 5-year continuous chronic disease surveillance platform to simultaneously track longitudinal trends in incidence, prevalence, mortality, and spirometry-confirmed (Type 1) diagnosis rates. Most notably, we characterized a distinct female-predominant chronic bronchitis phenotype and documented a sharply narrowed urban–rural diagnostic gap, indicating that expanded access to spirometry in primary care has driven more equitable and standardized COPD detection.22 Our findings, derived from a surveillance system with multi-level quality control, highlight four key observations: a substantial rise in age-standardized prevalence for all three conditions; a shift toward female predominance in chronic bronchitis prevalence and mortality in later years; notable short-term fluctuations in incidence and mortality rates; and a rapid increase in spirometry-confirmed COPD diagnoses alongside a marked reduction in the urban-rural diagnostic gap. The following discussion interprets these findings in the context of recent epidemiological literature, explores potential underlying mechanisms, and considers their public health implications.
The observed near-doubling of COPD age-standardized prevalence in Chongqing stands in contrast to the declining trends in age-standardized incidence and mortality rates for COPD reported in China by the Global Burden of Disease studies.23 This local increase likely reflects enhanced detection rather than worsening population health. Instead, it is more plausibly attributed to enhanced case ascertainment—an “unmasking effect”—facilitated by improvements in the local surveillance and quality control system.24 The steep rise in prevalence among the oldest age groups (≥60 years), reaching 14,714.32 per 100,000 in those aged ≥85 years in 2024, supports this interpretation, as it reflects the cumulative identification of prevalent cases. Even so, the high absolute disease burden underscores that regions in Western China continue to experience a disproportionate share of chronic respiratory disease, likely associated with persistent environmental and occupational risk factors.2,25 Although COPD is rare among individuals aged 15–19 years, such cases are biologically plausible and likely reflect early-life developmental vulnerabilities rather than conventional adult-onset disease. Low birth weight, preterm birth, severe childhood respiratory infections, and early exposure to household biomass fuel or ambient air pollution can restrict maximal lung growth and reduce peak lung function, thereby increasing the risk of airflow obstruction in adolescence or young adulthood. Therefore, COPD in this age group should be recognized as a marker of early-life respiratory insult and cumulative lung damage, rather than an inconsistency with the typical age distribution of COPD.21
The fluctuations in incidence and mortality observed between 2020 and 2024 must be viewed within the context of the COVID-19 pandemic. The sharp decline in COPD incidence in 2021 is consistent with international reports and likely stems from delayed healthcare-seeking for non-acute respiratory symptoms during periods of stringent public health restrictions.26 The rise in spirometry-confirmed COPD diagnosis rates did not coincide with an increase in incidence, as these two metrics reflect distinct processes: incidence denotes new-onset disease, whereas diagnosis rate represents the proportion of cases validated by spirometry. The observed increase in diagnosis rate is better explained by improved access to spirometry, enhanced primary care screening, and more standardized case documentation, rather than a true surge in new cases. Post-pandemic recovery of outpatient services and expanded community-based screening further facilitated the detection of previously undiagnosed prevalent cases, elevating diagnosis rates without a corresponding short-term rise in incidence.22,27 The subsequent mortality nadir in 2023 is a notable finding. The widespread implementation of non-pharmaceutical interventions (NPIs) to control SARS-CoV-2 transmission also suppressed the circulation of other respiratory viruses, which are primary triggers for severe acute exacerbations of COPD (AECOPD). This reduction in exacerbations may have temporarily lowered COPD-related mortality.28 The rebound in mortality in 2024 suggests a reversal of this effect following the relaxation of NPIs. Additionally, the potential for misclassification bias, where COPD deaths were attributed to COVID-19 during peak pandemic periods, may have artificially depressed recorded non-COVID respiratory mortality in earlier years.29
A prominent finding of this study is the divergent gender patterns among the three diseases. While COPD and emphysema showed a clear male predominance, consistent with historically higher smoking rates among Chinese men, chronic bronchitis exhibited a distinct profile. Female prevalence and mortality from chronic bronchitis exceeded male rates in 2023 and 2024. This aligns with emerging evidence of sex-specific phenotypes in chronic respiratory diseases, where chronic bronchitis and small airways disease are more frequently reported in women, whereas emphysema is strongly linked to male smoking history.30 Biological susceptibility may play a role, with women demonstrating a greater risk of COPD development per unit of tobacco exposure.31 Critically, exposure to household air pollution (HAP)—a significant risk factor in historically rural settings like Chongqing—disproportionately affects women and is associated with an airway-predominant (chronic bronchitis) phenotype rather than emphysema, offering a plausible explanation for the observed female burden.32 Furthermore, the higher prevalence of cardiovascular and metabolic comorbidities among women with COPD may contribute to the complex management and fluctuating mortality seen in this group.33
The rapid increase in the Type 1 (spirometry-confirmed) COPD diagnosis rate, from 6.96% in 2022 to 26.04% in 2024, represents a significant development. This trend coincides with national efforts to strengthen primary care and expand diagnostic capacity.34 Prior national data indicated that only 5.9% of diagnosed COPD patients had received spirometry confirmation, underscoring a previously massive diagnostic gap.35,36 The current increase likely reflects the successful deployment of resources such as portable spirometers and targeted training at the primary care level.22 Most notably, the near-elimination of the urban-rural gap in diagnosis—with only a 0.77-percentage-point difference in 2024—provides compelling evidence that these system-level investments are effectively reaching rural populations, promoting diagnostic equity where disparities have traditionally been wide.24 The narrowing urban–rural diagnostic gap is likely attributable to the strengthened primary care chronic disease management system in China. In recent years, the National Basic Public Health Service has promoted standardized chronic disease management, and the widespread use of portable spirometers in primary and community health facilities has lowered the threshold for spirometry testing in rural areas. For mountainous and geographically/administratively complex regions such as Chongqing, local poverty alleviation and primary care capacity-building policies have further improved rural diagnostic access. These changes suggest that the narrowing gap reflects improved accessibility and case ascertainment, rather than a synchronous short-term decline in the actual disease risk in rural areas.22,27,37
Our study benefits from the use of systematic surveillance data collected under a robust quality control framework. However, several limitations inherent to such data should be acknowledged. First, despite the marked increase, the 2024 Type 1 diagnosis rate of 26.04% indicates that a substantial proportion of managed COPD cases still lack spirometric confirmation by GOLD standards. Second, while the data capture outcomes effectively, they lack detailed individual-level exposure histories (eg., precise smoking pack-years, duration of biomass fuel exposure), which limits our ability to establish causal inferences for the observed trends. Third, mortality ascertainment may be underestimated because we only included deaths where COPD, chronic bronchitis, or emphysema was documented as the underlying cause of death. Deaths coded as pneumonia, respiratory failure, or other acute respiratory conditions—even when COPD was listed as a secondary or contributing diagnosis—were not captured. Similarly, deaths attributed to cardiovascular or other comorbidities, which are highly prevalent in patients with COPD, may also have been missed. This limitation may lead to underestimation of COPD-related mortality and should be taken into account when interpreting the observed mortality trends. Finally, although the impact of the pandemic period is evident, more sophisticated analytical approaches would be required to precisely quantify its temporary effects versus long-term epidemiological changes.
The findings from this study offer several directions for public health policy and research. The demonstrated model for expanding spirometry access and achieving diagnostic parity between urban and rural settings should be considered for adaptation in other regions. The identified high disease burden among the elderly and the distinct phenotype of chronic bronchitis among women call for more tailored, risk-factor-specific interventions that extend beyond tobacco control campaigns aimed primarily at men. Enhancing early detection will require bridging the communication gap between patients’ lived experience of symptoms and clinical diagnostic criteria, potentially through the use of plain-language educational tools. Future initiatives should focus on embedding spirometry quality assurance into routine primary care. Concurrently, prospective studies linked to surveillance data are needed to better characterize the female-predominant chronic bronchitis phenotype.38 Adopting a syndemic framework that addresses the co-occurrence of chronic respiratory, cardiovascular, and metabolic diseases could guide more integrated care models.39 Leveraging the existing data platform for spatio-temporal analyses with environmental exposure data represents a promising avenue for future research into disease drivers and prevention.
Conclusion
This 5-year surveillance study in Chongqing (2020–2024) demonstrates a rising prevalence of COPD, emphysema, and chronic bronchitis, mainly driven by improved case ascertainment. A clear gender divergence was found: chronic bronchitis became female-predominant, whereas COPD and emphysema remained male-dominant, supporting sex-specific public health strategies. The COVID-19 pandemic contributed to short-term fluctuations in incidence and mortality. Notably, the spirometry-confirmed COPD diagnosis rate increased sharply to 26.04%, with the urban-rural diagnostic gap nearly eliminated, validating a successful primary care diagnostic standardization model. Future interventions should prioritize diagnostic equity and targeted strategies for the female-predominant chronic bronchitis phenotype to reduce the chronic respiratory disease burden.
Data Sharing Statement
All relevant data are presented in the article. In accordance with institutional policies and approvals governing this research, the underlying data are not available for external distribution.
Ethics Approval and Consent to Participate
This study was approved by the Ethical Review Committee of Chongqing Center for Disease Control and Prevention (Approval Number: KY-2025-004-1). The data used in this study were obtained from the CCDSS, which is maintained by Chongqing CDC. As employees of the Institute of Chronic and Non-communicable Disease Control and Prevention at Chongqing CDC, the authors had authorized access to these data for research purposes in accordance with institutional policies and data governance protocols. The study was conducted in strict accordance with relevant guidelines and regulations. As this research involved the analysis of de-identified secondary surveillance data, the requirement for individual informed consent was waived by the ethics committee.
Acknowledgments
We extend our sincere thanks to all healthcare and public health staff in Chongqing who participated in the collection, verification, and reporting of case data for COPD, chronic bronchitis, and emphysema. Their meticulous and rigorous work laid a solid foundation for this study. We also acknowledge the technical support team responsible for upgrading the reporting system and implementing intelligent validation features during the data coverage period of this research. Their contributions provided strong support for enhancing data quality.
Funding
This research was supported by the Chongqing Natural Science Foundation (Project Number: CSTB2025NSCQ-GPX1058).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang Z, Lin J, Liang L, et al. Global, regional, and national burden of chronic obstructive pulmonary disease and its attributable risk factors from 1990 to 2021: an analysis for the Global Burden of Disease Study 2021. Respir Res. 2025;26(1):2. doi:10.1186/s12931-024-03051-2
2. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the Global Burden of Disease Study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
3. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–15. doi:10.1016/S2214-109X(23)00217-6
4. Yao L, Cao J, Cheng S, et al. Inequalities in disease burden and care quality of chronic obstructive pulmonary disease, 1990-2021: findings from the Global Burden of Disease Study 2021. J Glob Health. 2024;14:04213. doi:10.7189/jogh.14.04213
5. Jiang Y, Yan F, Kan H, Zhou M, Yin P, Chen R. Burden of chronic obstructive pulmonary disease attributable to ambient ozone pollution across China and its provinces, 1990-2021: an analysis for the Global Burden of Disease Study 2021. Chin Med J. 2024;137(24):3126–3135. doi:10.1097/CM9.0000000000003415
6. May SM, Li JT. Burden of chronic obstructive pulmonary disease: healthcare costs and beyond. Allergy Asthma Proc. 2015;36(1):4–10. doi:10.2500/aap.2015.36.3812
7. Agusti A, Vogelmeier CF. GOLD 2024: a brief overview of key changes. J Bras Pneumol. 2023;49(6):e20230369. doi:10.36416/1806-3756/e20230369
8. Singh D, Stockley R, Anzueto A, et al. GOLD Science committee recommendations for the use of pre- and post-bronchodilator spirometry for the diagnosis of COPD. Eur Respir J. 2025;65(2). doi:10.1183/13993003.01603-2024
9. Rossi A, Zanardi E. E pluribus plurima: multidimensional indices and clinical phenotypes in COPD. Respir Res. 2011;12:152. doi:10.1186/1465-9921-12-152
10. Salvi SS, Manap R, Beasley R. Understanding the true burden of COPD: the epidemiological challenges. Prim Care Respir J. 2012;21(3):249–251. doi:10.4104/pcrj.2012.00082
11. Ding XB, Liu Y, Jiao Y, et al. Mortality and trends of chronic respiratory diseases in people aged 70 years and below in Chongqing, 2012-2020. Chin J Prev Control Chronic Dis. 2022;30(11):821–824+830. doi:10.16386/j.cjpccd.issn.1004-6194.2022.11.005
12. Gou A, Tan G, Ding X, et al. Urban-rural difference in the lagged effects of PM2.5 and PM10 on COPD mortality in Chongqing, China. BMC Public Health. 2023;23(1):1270. doi:10.1186/s12889-023-16113-9
13. Ding XB, Tan Q, Xu J, et al. Changes in disease burden of chronic obstructive pulmonary disease among people aged ≥40 years in Chongqing. Pract Prev Med. 2024;31(10):1158–1162. doi:10.3969/j.issn.1006-3110.2024.10.002
14. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
15. Han XY, Wei YQ, Dong Z. Prevalence and knowledge of chronic obstructive pulmonary disease among people aged 40 years and above in Beijing, 2014. Chin J Health Educ. 2021;37(2):130–134. doi:10.16168/j.cnki.issn.1002-9982.2021.02.008
16. Cheng MZ, Li L, Hou DN, et al. Analysis on prevalence and risk factors of chronic obstructive pulmonary disease among adults in Shanghai. Shanghai Med J. 2020;43(11):651–658. doi:10.19842/j.cnki.issn.0253-9934.2020.11.002
17. Chen BY, Shan SX, Chen Z, et al. Epidemiological survey of chronic obstructive pulmonary disease in rural areas of Tianjin. Chin J Gen Pract. 2006;5(10):596–598. doi:10.3760/cma.j.issn.1671-7368.2006.10.007
18. Huang L. Prevalence and influencing factors of chronic obstructive pulmonary disease among residents aged 40 years and above in Guizhou Province [dissertation]. Guiyang: Guizhou University; 2023. doi:10.27045/d.cnki.ggyyc.2022.000139.
19. Victor JC, To T, Wilton A, Guan J, Ho MH, Gershon AS. The feasibility of COPD surveillance in Ontario: a population study. Healthc Q. 2011;14(4):25–29. doi:10.12927/hcq.2011.22647
20. Tang R, Zhang HD, Ding XB, Xia YY, Jiang L. Construction and application of a regional chronic disease surveillance and management information platform based on medical big data. J Med Inform. 2025;46(6):86–92. doi:10.3969/j.issn.1673-6036.2025.06.014
21. Han MK, Martinez FJ. Host, gender, and early-life factors as risks for chronic obstructive pulmonary disease. Clin Chest Med. 2020;41(3):329–337. doi:10.1016/j.ccm.2020.06.009
22. Xiao S, Wu F, Wang Z, et al. Validity of a portable spirometer in the communities of China. BMC Pulm Med. 2022;22(1):80. doi:10.1186/s12890-022-01872-9
23. Dong F, Su R, Ren Y, Yang T. Burden of chronic obstructive pulmonary disease and risk factors in China from 1990 to 2021: analysis of global burden of disease 2021. Chin Med J Pulm Crit Care Med. 2025;3(2):132–140. doi:10.1016/j.pccm.2025.05.004
24. Pan Z, Dickens AP, Chi C, et al. Accuracy and cost-effectiveness of different screening strategies for identifying undiagnosed COPD among primary care patients (≥40 years) in China: a cross-sectional screening test accuracy study: findings from the Breathe Well group. BMJ Open. 2021;11(9):e051811. doi:10.1136/bmjopen-2021-051811
25. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8
26. Poucineau J, Khlat M, Lapidus N, et al. Impact of the COVID-19 pandemic on COPD patient mortality: a Nationwide Study in France. Int J Public Health. 2024;69:1606617. doi:10.3389/ijph.2024.1606617
27. Zhou J, Li X, Wang X, Yu N, Wang W. Accuracy of portable spirometers in the diagnosis of chronic obstructive pulmonary disease A meta-analysis. NPJ Prim Care Respir Med. 2022;32(1):15. doi:10.1038/s41533-022-00275-x
28. Ho T, Shahzad A, Jones A, Raghavan N, Loeb M, Johnston N. Examining the effect of the COVID-19 pandemic on community virus prevalence and healthcare utilisation reveals that peaks in asthma, COPD and respiratory tract infection occur with the re-emergence of rhino/enterovirus. Thorax. 2023;78(12):1248–1253. doi:10.1136/thorax-2022-219957
29. Fedeli U, Casotto V, Barbiellini Amidei C, Vianello A, Guarnieri G. COPD-Related mortality before and after mass COVID-19 vaccination in Northern Italy. Vaccines. 2023;11(8). doi:10.3390/vaccines11081392
30. Rossi A, Butorac-Petanjek B, Chilosi M, et al. Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research - a consensus document from six scientific societies. Int J Chron Obstruct Pulmon Dis. 2017;12:2593–2610. doi:10.2147/COPD.S132236
31. Sørheim IC, Johannessen A, Gulsvik A, Bakke PS, Silverman EK, DeMeo DL. Gender differences in COPD: are women more susceptible to smoking effects than men. Thorax. 2010;65(6):480–485. doi:10.1136/thx.2009.122002
32. Han MK. Chronic obstructive pulmonary disease in women: a biologically focused review with a systematic search strategy. Int J Chron Obstruct Pulmon Dis. 2020;15:711–721. doi:10.2147/COPD.S237228
33. Sodhi A, Pisani M, Glassberg MK, Bourjeily G, D’Ambrosio C. Sex and gender in lung disease and sleep disorders: a state-of-the-art review. Chest. 2022;162(3):647–658. doi:10.1016/j.chest.2022.03.006
34. Ozoh OB, Ayo-Olagunju T, Mortimer K. Meeting unmet needs in chronic obstructive pulmonary disease diagnosis and treatment in low- and middle-income countries. Am J Respir Crit Care Med. 2023;208(4):352–354. doi:10.1164/rccm.202307-1167ED
35. Yang T, Cai B, Cao B, et al. Severity distribution and treatment of chronic obstructive pulmonary disease in China: baseline results of an observational study. Respir Res. 2022;23(1):106. doi:10.1186/s12931-022-02021-w
36. Lu XL, Cong S, Fan J, et al. Analysis on pulmonary function test rate and its influencing factors among patients with chronic obstructive pulmonary disease aged 40 years and above in China, 2014–2015. Chin J Epidemiol. 2020;41(5):672–677. doi:10.3760/cma.j.cn112338-20200122-00054
37. Yang T, Wu J, Chi C. Investing in primary care to reduce the burden of chronic obstructive pulmonary disease. China CDC Wkly. 2025;7(47):1473–1476. doi:10.46234/ccdcw2025.246
38. Li J. Guidelines for Chinese medicine rehabilitation of chronic obstructive pulmonary disease. World J Tradit Chin Med. 2020;6(3):295–306. doi:10.4103/wjtcm.wjtcm_44_20
39. Ozdemir T, Yıldız M, Arı M, et al. Gender-based differences in COPD patients with type 2 respiratory failure-impact on clinical practice. Medicina. 2025;61(4). doi:10.3390/medicina61040587
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology and Survival of Kaposi’s Sarcoma by Race in the United States: A Surveillance, Epidemiology, and End Results Database Analysis
Ragi SD, Moseley I, Ouellette S, Rao B
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1681-1685
Published Date: 18 August 2022
The Pharmacokinetics, Safety and Tolerability of Aclidinium Bromide 400 μg Administered by Inhalation as Single and Multiple (Twice Daily) Doses in Healthy Chinese Participants
Li W, Daoud SZ, Trivedi R, Lukka PB, Jimenez E, Molins E, Stewart C, Bharali P, Garcia-Gil E
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2725-2735
Published Date: 27 November 2023
Prevalence and Risk Factors of Chronic Obstructive Pulmonary Disease Among Users of Primary Health Care Facilities in Morocco
Al wachami N, Arraji M, Iderdar Y, Mourajid Y, Boumendil K, Bouchachi FZ, Jaouhar S, Guennouni M, Laamiri F, Elkhoudri N, Bandadi L, Louerdi ML, Hilali A, Chahboune M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:375-387
Published Date: 5 February 2024
Dynamic Risk Status of OSA and Its Association with COPD Incidence and Progression to Oxygen Therapy: Insights from a US National Cohort

Wang Y, Luo J, Huang R, Xiao Y
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:753-766
Published Date: 21 March 2025
Reliability of Pulmonary Function Tests in Patients with Chronic Obstructive Pulmonary Disease
Arslan F, Şen E, Şirin B, Köktürk N, Ulubay G, Aydogan Eroglu S, Gemicioglu B, Sönmez Ö, Şerifoğlu İ, Dilektasli AG, Öztürk Şahin B, Doğan İ, Gürhan N, Günen H, Ensen N
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:554115
Published Date: 21 January 2026