Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Gender Differences in the First-Year Antipsychotic Treatment for Chinese First-Episode Schizophrenia
Authors Pu C, Huang B ![]() , Zhou T, Cheng Z, Wang Y, Shi C, Yu X
, Zhou T, Cheng Z, Wang Y, Shi C, Yu X ![]()
Received 11 September 2020
Accepted for publication 4 December 2020
Published 17 December 2020 Volume 2020:16 Pages 3145—3152
DOI https://doi.org/10.2147/NDT.S280719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Chengcheng Pu,1,* Bingjie Huang,1,* Tianhang Zhou,1 Zhang Cheng,1 Yi Wang,2 Chuan Shi,1 Xin Yu1
1Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, People’s Republic of China; 2Neuropsychology and Applied Cognitive Neuroscience Laboratory, CAS Key Laboratory of Mental Health, Institute of Psychology, Chinese Academy of Sciences, Department of Psychology, University of Chinese Academy of Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Yu; Chuan Shi
Peking University Sixth Hospital, 51 Huayuan North Road, Beijing 100089, People’s Republic of China
Email [email protected]; [email protected]
Objective: To investigate the gender differences in the efficacy and side effects of three frequently used antipsychotic medicines (risperidone, olanzapine, aripiprazole) for patients with first-episode schizophrenia during the first year of treatment.
Methods: A total of 569 patients with first-episode schizophrenia were randomly assigned to risperidone, olanzapine, and aripiprazole groups. All patients were treated according to their actual clinical needs. Clinical efficacies were assessed by the Positive and Negative Symptom Scale (PANSS) and side effects were assessed by the Udvalg for Kliniske Undersogelser Side-Effect scale (UKU). All assessments were completed at baseline and at 1, 2, 3, 6, 9, and 12 months.
Results: Males had higher baseline PANSS total scores and PANSS negative and general pathological scores. No significant interactions were found between treatment time and gender in psychopathology improvements in all three groups. In the end of the first year, female patients receiving risperidone reported more dermatological symptoms (rashes) than males, female patients receiving olanzapine reported more autonomic side effects and dermatological symptoms than males, and female patients receiving aripiprazole reported more psychotic side effects than males.
Conclusion: Gender differences exhibited in response to antipsychotic treatments for Chinese patients with first-episode schizophrenia. After the first year of antipsychotic treatment, drug-related side effects were more likely presented in female patients than male patients.
Keywords: first-episode schizophrenia, gender difference, antipsychotic treatment, treatment response, side effects
Introduction
Gender differences generally present in schizophrenia, including but not limited to clinical characteristics, treatment responses, and the global functioning.1 Female patients seem to have less hospitalization time, fewer functional impairments, and better social support than male patients.2 Evidence suggested that female schizophrenic patients may have a more favorable clinical prognosis.3,4 However, gender differences in response to antipsychotic treatments have not been systematically investigated, especially in Chinese schizophrenic patients.
Generally, males have faster gastrointestinal absorptions, lower fat contents, and higher activity of metabolic enzymes than females. Thus, males need higher doses of antipsychotic drugs to reach stable blood concentration, which increases their risk of drug-related side effects.5 However, female schizophrenic patients have been observed to report more side effects, eg weight gain, sexual dysfunction, and arrhythmia than men.6 Clinical studies and animal studies suggested an antidopaminergic effect of estrogens,7,8 which accounted for some of the better responses to antipsychotics in females. In addition, gender differences were reported in responses to different types of antipsychotic drugs. Female patients receiving clozapine displayed significantly better prognosis than male patients, while olanzapine-related gender differences were only observed in quality of life. No gender differences have been found in patients receiving risperidone.9
Gender differences in the treatment of first-episode schizophrenia (FES) have been reported based on the European First Episode Schizophrenia Trial,3 while few studies from Asia or developing countries have been reported. We designed a one-year prospective cohort study to examine the efficacy and side effects of three frequently used antipsychotics (olanzapine, risperidone, aripiprazole) in Chinese Han FES patients. The aims of this study were to prospectively investigate gender differences in responses to antipsychotics and drug-related side effects. We hypothesized that female FES patients have better responses to antipsychotic drugs, while may present more drug-related side effects.
Methods
Study Design
This was a one-year prospective study. The specific study design and patient disposition were published elsewhere.10 All participants were aged 18~45 years and met the diagnostic criteria for schizophrenia according to the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorder-IV Axis I Disorder (SCID). All participants had not been exposed to continuous antipsychotic treatments longer than four weeks. All participants and their legal guardians provided written informed consent before any assessments. This study was approved by the ethics committees of Peking University Institute of Mental Health and was registered as an International Standard Randomized Controlled Trial (No. NCT01057849).
Treatment
Participants were randomly assigned to a risperidone (3–6mg/day), olanzapine (10–25mg/day), or aripiprazole (15–30mg/day) group. Participants who showed little benefit from the first group were permitted to a medication alteration process (selection restricted to olanzapine, risperidone, and aripiprazole), which was only allowed in the first four weeks. Drug choices were made based on patients’ actual needs and psychiatrists’ clinical experiences. Oral benzhexol (2–6mg/day), promethazine (25–75mg/day), or lorazepam (0.5–1.5mg/day) were allowed to be prescribed if necessary.
Assessment
Clinical efficacy was assessed by the Positive and Negative Symptom Scale (PANSS). It is a 30-item structured scale which can be divided into the positive syndrome subscale (PPANSS), the negative syndrome subscale (NPANSS), and the general syndrome subscale (GPANSS).11 Side effects were measured by Udvalg for Kliniske Undersogelser Side-Effect Scale (UKU), which assessed psychotic side effects, neurological side effects, autonomic side effects, and other side effects (eg, dermatological symptoms, sexual functions).12 Social functioning was assessed by Personal and Social Performance Scale (PSP).13 All assessments were conducted by trained psychiatrists at baseline and after 1, 2, 3, 6, 9, and 12 months’ treatments. All interviewers attended a 1-week training workshop prior to the study and reached a qualified consistency (intraclass correlation coefficients or kappa values higher than 0.75).
Data Analysis
Independent sample t-tests were used to analyze gender differences in psychopathological changes. Repeated ANOVA was performed for the three antipsychotic groups to determine gender differences in the treatment effects and drug-related side effects. Due to differences in the number of follow-up visits, the tracking time point was used as the internal variable, and gender was used as the subject variable in the repeated ANOVA. All p-values were two-tailed and at a significance level of ≤0.05.
Results
Baseline Clinical Characteristics and Patient Disposition
A total of 569 patients (289 males and 280 females) were enrolled and randomly assigned to risperidone group (100 males and 90 females), olanzapine group (89 males and 96 females), and aripiprazole group (100 males and 94 females). Proportions of patients assigned to individual antipsychotics were not different between females and males. Females were older than males in the whole sample (p<0.01) and in the risperidone group (p=0.04). Initial NPANSS, GPANSS, and total PANSS scores were significantly higher in males than females (Table 1).
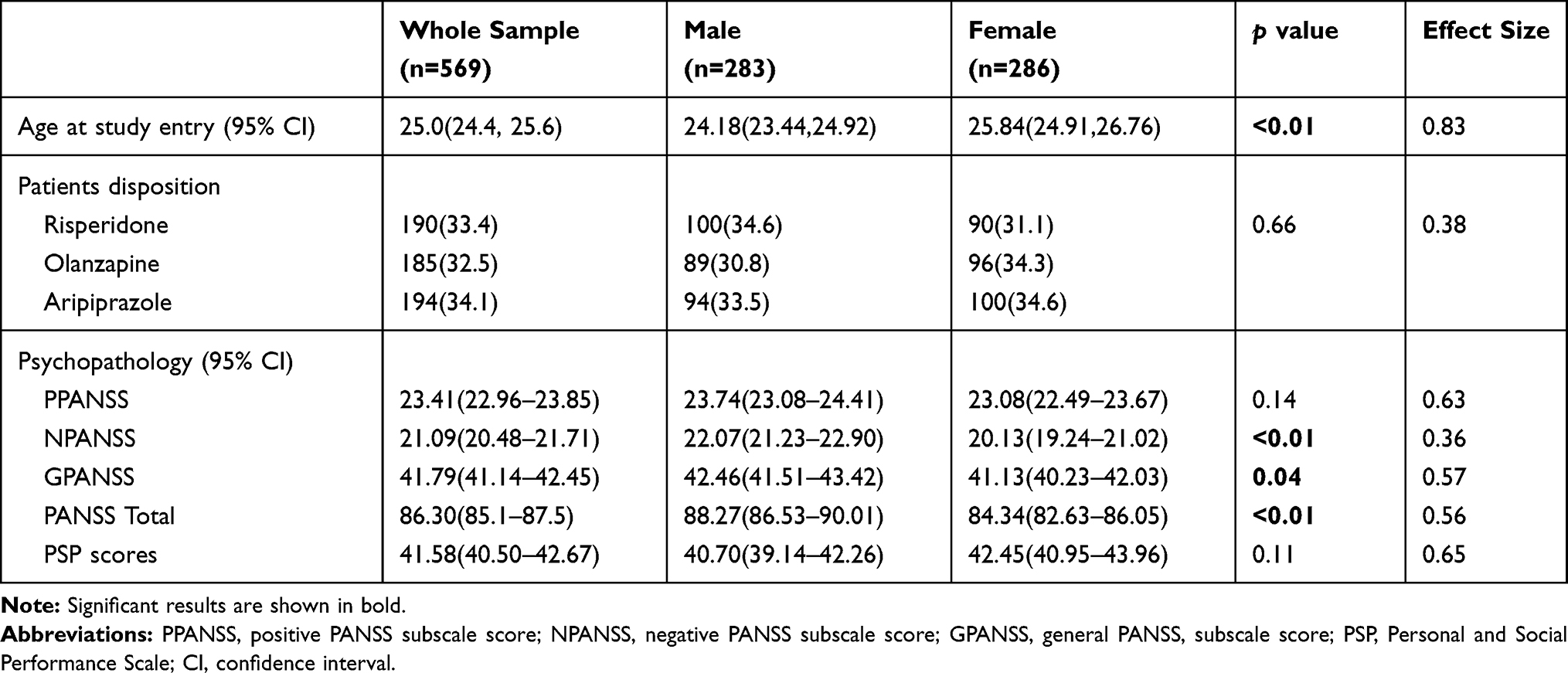 |
Table 1 Baseline Clinical Characteristics of All First-Episode Schizophrenia Patients |
Gender Differences in Psychopathology and Functioning Change in the Initial Year of Antipsychotic Treatment
Two hundred and six patients (75 from risperidone group, 59 from olanzapine group, and 72 from aripiprazole) fully completed the first-year antipsychotic treatment and all assessments. After first month treatment, a significant improvement in PPANSS was seen in males than females (p=0.03). After nine months of treatment, significant improvement was seen in males than females in NPANSS (p=0.03) – see Table 2.
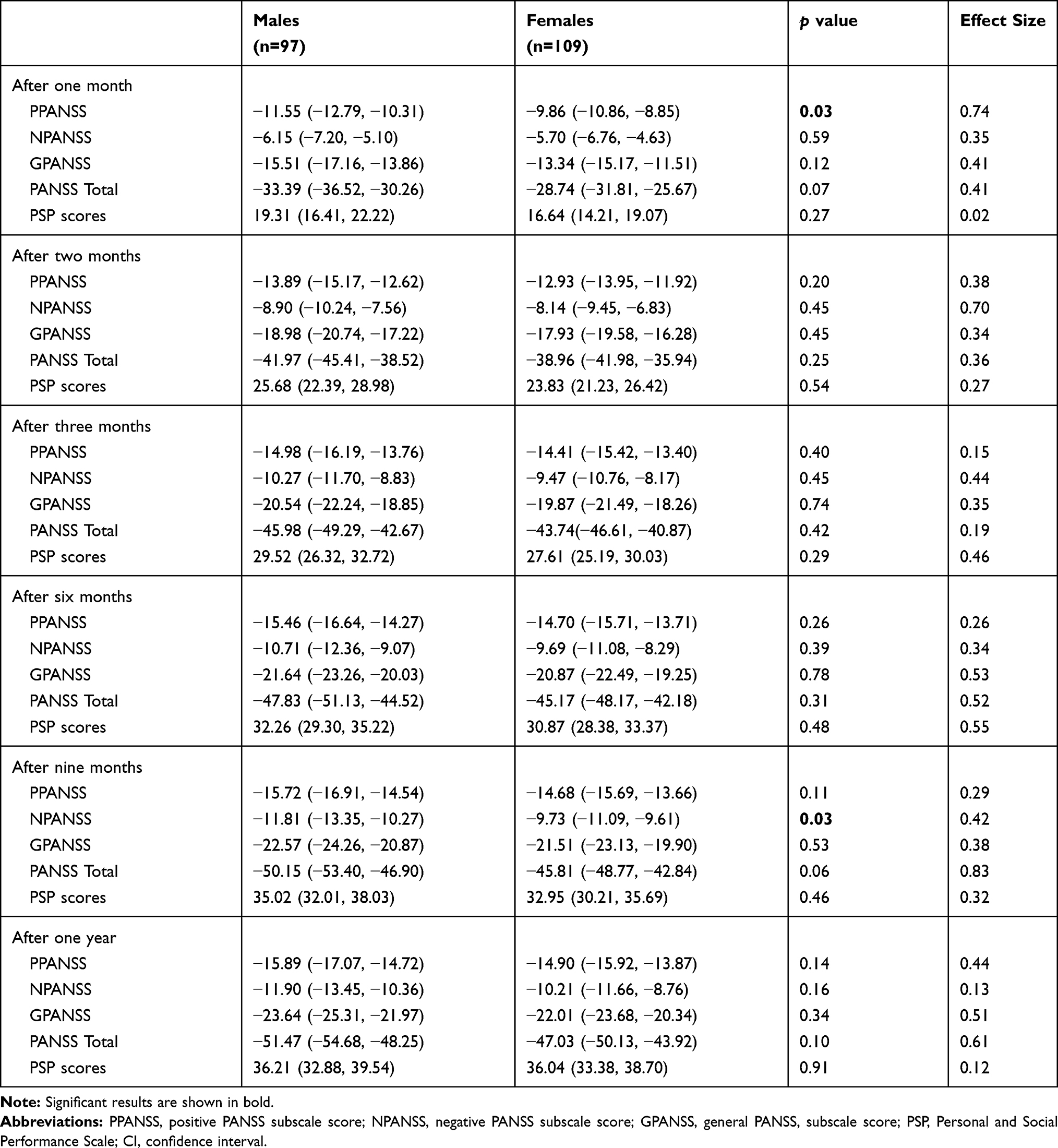 |
Table 2 PANSS and PSP Score Changes from Baseline (95% CI) – Comparison of Males and Females |
Gender Difference in Response to Specific Antipsychotics and Drug-Related Side Effects in the Initial Year of Treatment
In the end of the first year treatment, drug doses were not significantly different between males and females (risperidone: 3.29±1.42mg for male and 3.15±1.38mg for female; olanzapine: 10 (5,15) mg for male and 15 (10,20) mg for female; aripiprazole: 16.85±5.03mg for male and 15.48±6.84mg for female, all p>0.05). After one-year treatment, patients-reported side effects were not significantly different among three antipsychotic groups. No significant interactions were found between treatment time and gender in psychopathology improvements (PANSS total scores and all PANSS subscale scores) in all three antipsychotic groups (Table 3, Figures 1–3). In the end of the first year, female patients receiving risperidone reported more dermatological symptoms (rashes), female patients receiving olanzapine reported more autonomic side effects and dermatological symptoms, and female patients receiving aripiprazole reported more psychotic side effects than males (Table 3).
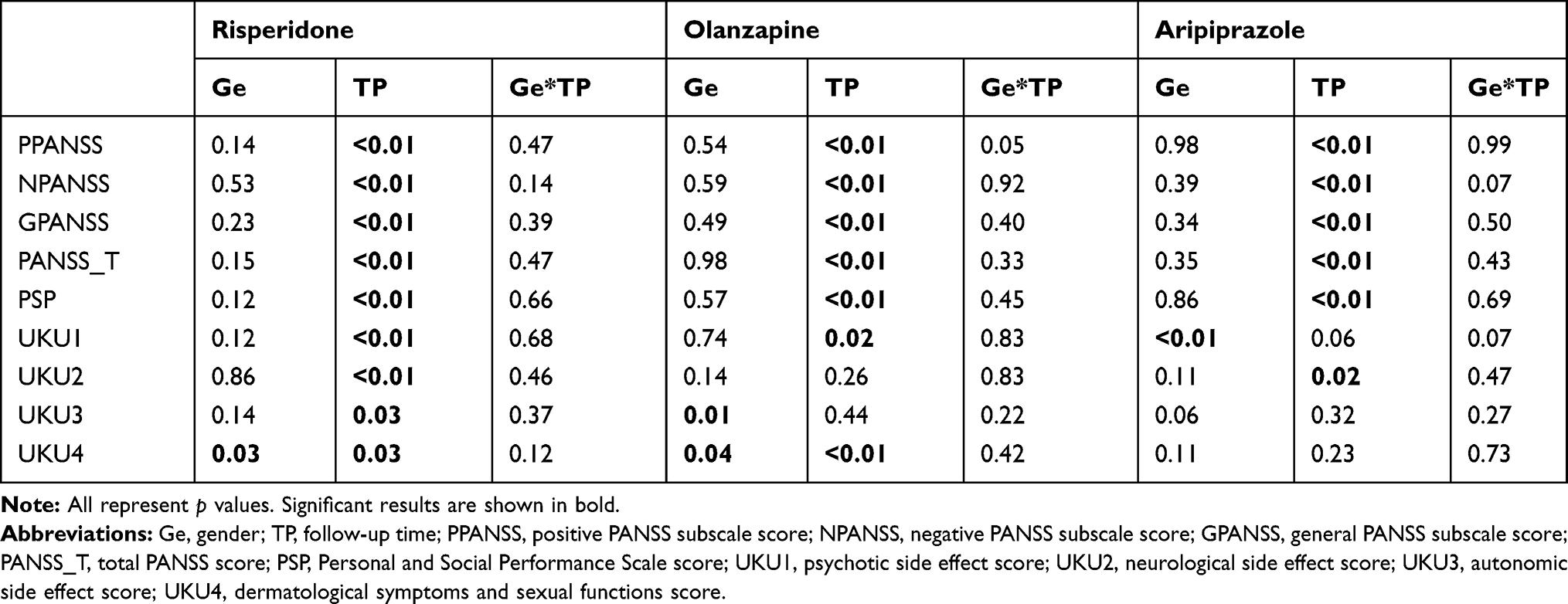 |
Table 3 Interaction Between Gender and Treatment Time in Psychopathology Improvement, Functioning Improvement, and Drug-Related Side Effects |
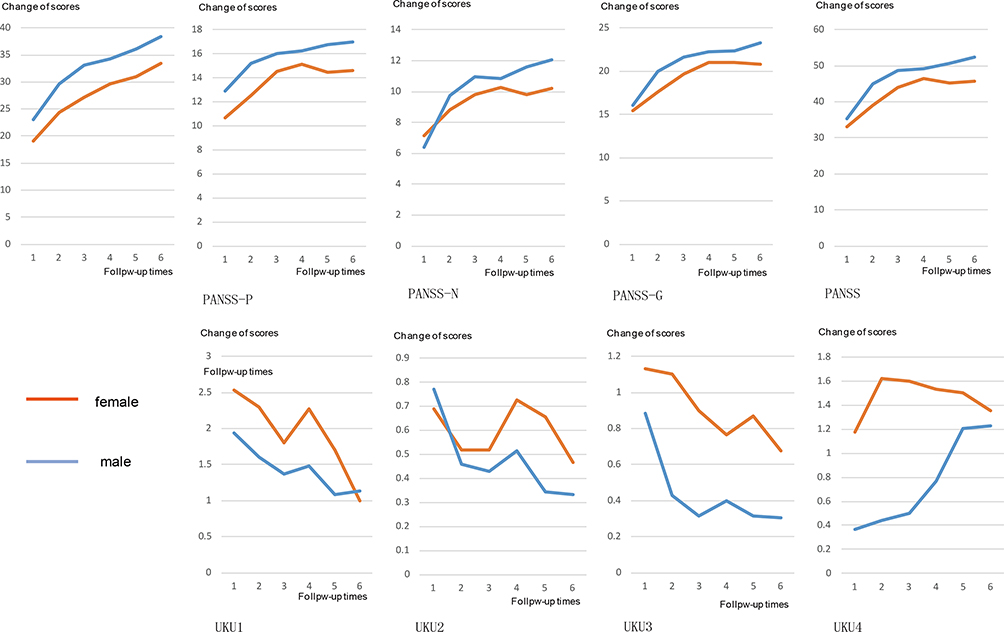 |
Figure 1 Symptoms and side effects changes after one-year risperidone treatment in first-episode schizophrenia - comparison of males and females. Abbreviations: PANSS_P, positive PANSS subscale score; PANSS_N, negative PANSS subscale score; PANSS_G, general PANSS subscale score; PANSS_T, total PANSS score; PSP, Personal and social performance scale score; UKU1, psychic side effect score; UKU2, neurological side effect score; UKU3, autonomic side effect score; UKU4, dermatological symptoms and sexual functions score. |
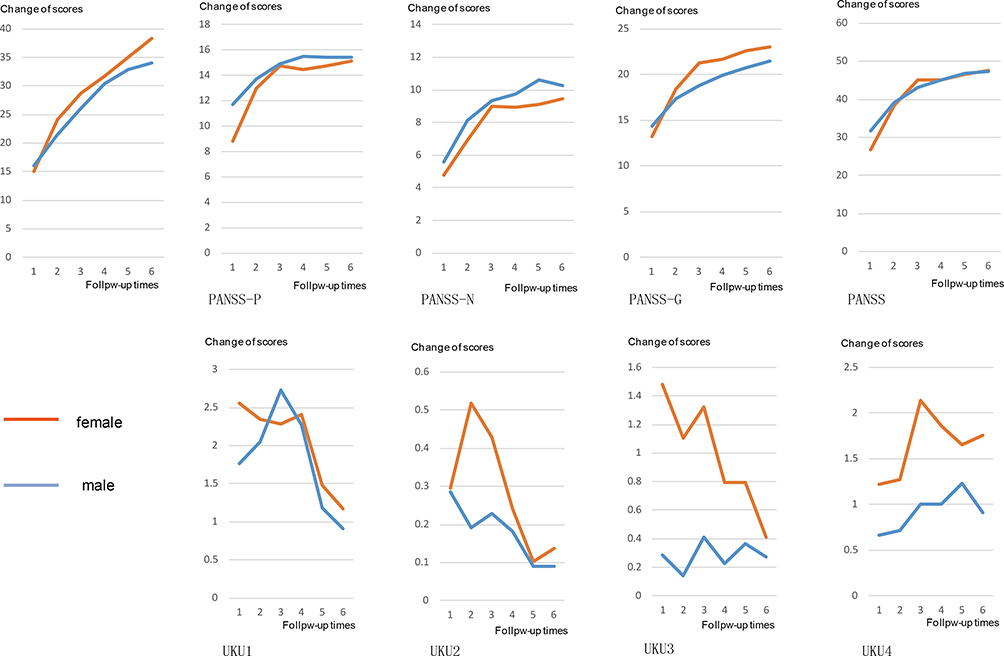 |
Figure 2 Symptoms and side effects changes after one-year olanzapine treatment in first-episode schizophrenia - comparison of males and females. Abbreviations: PANSS_P, positive PANSS subscale score; PANSS_N, negative PANSS subscale score; PANSS_G, general PANSS subscale score; PANSS_T, total PANSS score; PSP, Personal and social performance scale score; UKU1, psychic side effect score; UKU2, neurological side effect score; UKU3, autonomic side effect score; UKU4, dermatological symptoms and sexual functions score. |
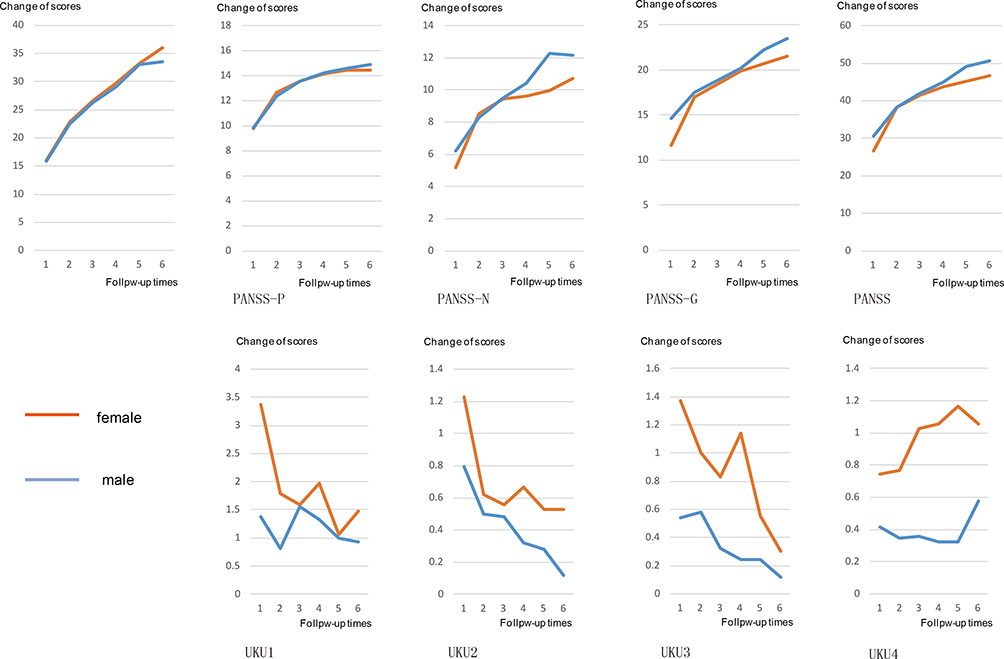 |
Figure 3 Symptoms and side effects changes after one-year aripiprazole treatment in first-episode schizophrenia - comparison of males and females. Abbreviations: PANSS_P, positive PANSS subscale score; PANSS_N, negative PANSS subscale score; PANSS_G, general PANSS subscale score; PANSS_T, total PANSS score; PSP, Personal and social performance scale score; UKU1, psychic side effect score; UKU2, neurological side effect score; UKU3, autonomic side effect score; UKU4, dermatological symptoms and sexual functions score. |
Discussion
This was one of the largest cohort studies to investigate gender differences in responses to antipsychotics in Chinese FES patients. We evaluated gender differences in responses to three frequently used second-generation antipsychotics and drug-related side effects during the initial year of treatment. Though males seemed to have robust improvements in positive symptoms after one-month treatment and negative symptoms after nine months of treatment, we failed to find interaction between gender and treatment time in terms of the improvement of psychopathology. Female patients reported more drug-related side effects than male patients in all antipsychotic groups.
Evidence have reported gender differences of symptom presence among schizophrenic patients, with more negative and disorganization symptoms presented in males and more affective and atypical positive symptoms presented in females.14,15 Our results confirmed that males displayed more serious negative, and general symptoms than females, but failed to find gender difference in positive symptoms. The Schizophrenia Outpatient Health Outcomes (SOHO) study and European First Episode Schizophrenia Trial have reported females responded better and more quickly to antipsychotics.3,9 Our results did not find gender differences in response to antipsychotic treatments. Inconsistent results may be related to differences in selected antipsychotic medications. Although gender could be a predictor for antipsychotic efficacy, it may not be fit for all antipsychotic medications. The most significant gender differences were observed in typical antipsychotics and clozapine, while the efficacy of atypical antipsychotics seemed to not relate to gender.9
Another explanation could be the high drop-off rate of our study, which is also an important limitation of this study. Cheng et al found that 47.1% of patients had discontinued using antipsychotics at the 52-week follow-up, and reported treatment interruption was associated with gender.16 We found that more females completed the first year of antipsychotic treatment than males, though the difference was not statistically significant. We failed to follow up the drop-offs and could not give more detailed results. Thus, we suggested that gender differences in response to specific treatments should be studied in expanded sample size.
Previous studies have reported that 50–75% higher rates of drug-related side effects occurred in females than in males,17 which is consistent with our results. Multiple factors may contribute to the gender differences in response to antipsychotic treatments, including the generally higher proportion of body fat in females and the differences in the metabolic pathways of drugs between genders.18,19 Additionally, self-reported side effects were more common in female patients,20 which have been observed in both Western and Asian countries.21 Especially in Chinese culture, females are more concerned about their bodies, while men are more likely to ignore their feelings, which may also affect their self-reported side effects.
There are several limitations to this study. First, nearly half of the participants failed to complete the first year of treatment and were not included in final analysis, which may cause significant bias to our results. Second, though we measured drug-related side effects by UKU scale, reliable objective measures, such as prolactin and other plasma monitoring, were absent in this study. Self-reported side effects may also bias our results towards more side effects in females.
Conclusion
Gender differences exhibited in response to antipsychotic treatments for Chinese patients with first-episode schizophrenia. In the first year of treatment with risperidone, olanzapine, and aripiprazole, side effects were more likely presented in female patients than male patients. Gender should be taken into account in choosing appropriate antipsychotic treatment for patients. Gender differences are of importance and should be systematically investigated, which may improve treatment outcomes and reduce side-effects, and contribute significantly to the development of precision treatment.
Data Sharing Statement
Data are available upon reasonable request. Data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
This study was supported by National Key R&D Program of China (2018YFC1314200), the Capital’s Funds for Health Improvement and Research (CFH, No.2018-4-4116), the Key Program of Beijing Science and Technology Commission (D171100007017002, D121100005012004), the National Key Project of Scientific and Technical Supporting Programs funded by Ministry of Science and Technology of China (no. 2007BAI17B04). Chengcheng Pu and Bingjie Huang are co-first authors for this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Ochoa S, Usall J, Cobo J, Labad X, Kulkarni J. Gender differences in schizophrenia and first-episode psychosis: a comprehensive literature review. Schizophr Res Treatment. 2012;2012:916198.
2. Leung A, Chue P. Sex differences in schizophrenia, a review of the literature. Acta Psychiatr Scand Suppl. 2000;401:3–38.
3. Ceskova E, Prikryl R, Libiger J, Svancara J, Jarkovsky J. Gender differences in the treatment of first-episode schizophrenia: results from the European first episode schizophrenia trial. Schizophr Res. 2015;169(1–3):303–307. doi:10.1016/j.schres.2015.10.013
4. Seeman MV. Does gender influence outcome in schizophrenia? Psychiatr Q. 2019;90(1):173–184. doi:10.1007/s11126-018-9619-y
5. Lange B, Mueller JK, Leweke FM, Bumb JM. How gender affects the pharmacotherapeutic approach to treating psychosis - a systematic review. Expert Opin Pharmacother. 2017;18(4):351–362. doi:10.1080/14656566.2017.1288722
6. Nakagawa K, Kajiwara A. Female sex as a risk factor for adverse drug reactions. Japan J Clin Med. 2015;73(4):581–585.
7. Canuso CM, Pandina G. Gender and schizophrenia. Psychopharmacol Bull. 2007;40(4):178–190.
8. Groleger U, Novak-Grubic V. Gender, psychosis and psychotropic drugs: differences and similarities. Psychiatr Danub. 2010;22(2):338–342.
9. Usall J, Suarez D, Haro JM, Group SS. Gender differences in response to antipsychotic treatment in outpatients with schizophrenia. Psychiatry Res. 2007;153(3):225–231. doi:10.1016/j.psychres.2006.09.016
10. Han X, Yuan YB, Yu X, et al. The Chinese first-episode schizophrenia trial: background and study design. East Asian Arch Psychiatry. 2014;24(4):169–173.
11. Si T, Yang J, Shu L, et al. Reliability and validity of the Chinese version of the positive and negative syndrome scale. Chin Ment Health J. 2004;(01):45–47.
12. Chen K-P, Lung F-W. Reliability and validity of the short version of udvalg for kliniske undersogelser in antipsychotic treatment. Psychiatr Q. 2017;88(4):787–796. doi:10.1007/s11126-017-9494-y
13. Si T, Shu L, Tian C, et al. Reliability and validity of the Chinese version of the personal and social performance scale in patients with schizophrenia. Chin Ment Health J. 2009;23(11):790–794.
14. Thorup A, Petersen L, Jeppesen P, et al. Gender differences in young adults with first-episode schizophrenia spectrum disorders at baseline in the Danish OPUS study. J Nerv Ment Dis. 2007;195(5):396–405. doi:10.1097/01.nmd.0000253784.59708.dd
15. Morgan VA, Castle DJ, Jablensky AV. Do women express and experience psychosis differently from men? Epidemiological evidence from the Australian National Study of Low Prevalence (Psychotic) Disorders. Aust N Z J Psychiatry. 2008;42(1):74–82. doi:10.1080/00048670701732699
16. Cheng Z, Yuan Y, Han X, et al. Rates and predictors of one-year antipsychotic treatment discontinuation in first-episode schizophrenia: results from an open-label, randomized, “real world” clinical trial. Psychiatry Res. 2019;273:631–640. doi:10.1016/j.psychres.2019.01.068
17. Patel TK, Patel PB. Incidence of adverse drug reactions in indian hospitals: a systematic review of prospective studies. Curr Drug Saf. 2016;11(2):128–136. doi:10.2174/1574886310666150921104523
18. Damoiseaux VA, Proost JH, Jiawan VC, Melgert BN. Sex differences in the pharmacokinetics of antidepressants: influence of female sex hormones and oral contraceptives. Clin Pharmacokinet. 2014;53(6):509–519.
19. Zhang Y, Kim MJ, Bertino JS, Nafziger AN, Sellers EM. Use of omeprazole as a CYP3A probe drug: effect of sex and menstrual cycle phase on CYP3A activity in healthy Caucasian adults. J Clin Pharmacol. 2006;46(3):345–352. doi:10.1177/0091270005284389
20. Haack S, Seeringer A, Thürmann PA, Becker T, Kirchheiner J. Sex-specific differences in side effects of psychotropic drugs: genes or gender? Pharmacogenomics. 2009;10(9):1511–1526. doi:10.2217/pgs.09.102
21. Lucca J, Madhan R, Ram D. Gender differences in the occurrences and pattern of adverse drug reactions in psychiatric patients: a prospective observational study. Trop J Med Res. 2017;20:84. doi:10.4103/1119-0388.198134
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.