Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Gender Differences in the Association Between Sarcopenia and Depressive Symptoms Among Community-Dwelling Older People in a Chinese Suburban Area
Authors Lu L, Mao L, Yang S, He X, Zhang Z, Chen N ![]()
Received 11 September 2023
Accepted for publication 23 November 2023
Published 4 December 2023 Volume 2023:16 Pages 3813—3824
DOI https://doi.org/10.2147/JMDH.S439785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Linqian Lu,1,2,* Lin Mao,3,* Shanshan Yang,3,* Xiangfeng He,1 Zhen Zhang,1 Nan Chen1
1Department of Rehabilitation, Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences, Shanghai, People’s Republic of China; 2The Second Affiliated Hospital of Zhejiang Chinese Medical University, Zhejiang, People’s Republic of China; 3Department of Rehabilitation, Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nan Chen, Department of Rehabilitation, Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences, Shanghai, 202150, People’s Republic of China, Email [email protected]
Introduction: Sarcopenia and depressive symptoms are common disorders in older people; however, there is lacking for studies focus on the association between sarcopenia and depressive symptoms by gender. Thus, we investigate gender differences in the association between sarcopenia and depressive symptoms.
Methods: 1119 participants aged ≥ 65 were included in our study. Sarcopenia was defined as no sarcopenia, possible sarcopenia, general sarcopenia, and severe sarcopenia by the Asian Working Group for Sarcopenia 2019 consensus. Depressive symptoms were assessed by the Geriatric Depression Scale-15. The logistic regression analysis was used to identify the association between sarcopenia and depressive symptoms.
Results: No sarcopenia and severe sarcopenia were significantly inversely and positively associated with depressive symptoms only in women. In men, low appendicular skeletal muscle mass index was significantly inversely associated with depressive symptoms. In women, low gait speed was significantly inversely associated with depressive symptoms, while poor 5-time chair stand test was significantly positively associated with depressive symptoms.
Conclusion: Our study found that sarcopenia and its diagnostic elements were significantly associated with depressive symptoms in men or women. Interventions for muscle mass and physical performance are necessary for sarcopenia to prevent the development of depressive symptoms timely.
Keywords: sarcopenia, depressive symptoms, gender difference, suburban area, older people
Introduction
Sarcopenia and depression are both prevalent disorders, especially among older people.1–3 Both sarcopenia and depression have significant adverse impacts on individuals and society, such as poor quality of life, severe psychological disorders, even mortality,4–7 and can also increase the medical burden on society.8,9 Low muscle mass, low muscle strength, and low physical performance are mostly used to define sarcopenia, according to the Asian Working Group for Sarcopenia 2019 (AWGS 2019) consensus.10 Self-reported scales are commonly used clinically to screen for depressive symptoms or through an interview with a psychiatrist to diagnose depression.5
Current evidence suggests that the relationship between sarcopenia and depression is not clear. Many studies have demonstrated that there is a significant association between sarcopenia and depression.11,12 Older people with sarcopenia are more likely to experience depressive symptoms. In a study by Gao et al, 769 out of 7706 older people were found to suffer from sarcopenia and 35.9% of sarcopenic people had depression.13 Additionally, older people with sarcopenia who have depressive symptoms are more likely to develop suicidal behaviour and increase the mortality of older people with sarcopenia.14 Multiple mechanisms of interaction between sarcopenia and depression have been identified, including inflammation, oxidative stress, neurotrophins, and lifestyle behaviors.11 However, some studies also demonstrated that there is no significant relationship between sarcopenia and depression.15,16
Currently, studies on the association between sarcopenia and depression among older people were mostly conducted in urban areas.17 For example, studies by Hayashi et al and Kim et al both found that sarcopenia was associated with depressive symptoms among older people in urban areas.18,19 However, there is considerable evidence of significant differences between older people in urban and suburban areas, such as sociodemographic (like occupation type and educational level),20 lifestyles (like physical activity [PA] level),21 and chronic diseases (like sarcopenia and mental disease).22,23 It has been proved that suburban older people are more likely to have sarcopenia than those urban older people in China.22 Therefore, more in-depth studies are required to clarify the relationship between sarcopenia and depression among older people in suburban areas of China.
Significant differences in physical and mental health have been found in older men and women, respectively.24 In terms of gender difference, men are more likely than women to have sarcopenia among community-dwelling older people.25 Furthermore, a gender difference in the prevalence of depression among Chinese residents was also found.26 Therefore, the relationship between sarcopenia and depression may be influenced by gender. However, no studies have directly explored the gender differences in the relationship between sarcopenia and depression. Sociodemographic characteristics (such as occupation types and educational level) and lifestyles (such as PA level) have been shown to have a strong relationship with sarcopenia.1 There are also significant gender differences in the relationship between the above aspects and depression.27 To facilitate the progression of healthy ageing, it is necessary to investigate gender differences in the relationship between sarcopenia and depression and to provide gender-specific early prevention and interventions for sarcopenia and depression in older people.
Thus, in this study, we aimed to: 1) identify gender differences in the prevalence of depressive symptoms in older people with different sarcopenic statuses; and 2) explore the relationship between sarcopenia and depressive symptoms by gender among older people in Chinese suburban areas.
Methods
Study Design and Ethical Consideration
Our study was performed in the community health service centers in the suburban area of Shanghai (the Chongming District), and all data were collected from April to December 2021. This study had achieved the approvement by the Ethical Committee of Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences in November 2020 (approval No. CMEC-2020-KT-42).
Study Participants
Older people were included if: 1) aged 65 years and above; 2) be able to live in their own house or live together with family in the community independently for a long time (at least one year); 3) willing to participate in and cooperate with various assessments. Older people were excluded if: 1) have physical disabilities (such as a hand, foot, or multiple limbs losing, visual and hearing impairments) and cognitive impairment (such as Alzheimer’s disease); 2) diagnosed or self-reported diseases (such as severe hypertension, diabetes, heart disease, stroke, hyperthyroidism, or hypothyroidism); 3) taking prescription drugs that may obviously affect body composition (such as systemic corticosteroids); 4) cannot communicate with researchers during the process of assessments.
We recruited participants from Chengqiao town and Sanxing town, which have 5 communities (n=5286) and 2 communities (n=2035), respectively. A total of 7 communities has similar demographic characteristics and health status. All residents ≥65 years old in 7 communities (n=7321) were invited to participate in our study, and eventually, a total of 1558 community-dwelling older people were willing to participate in our study. Before the assessments, informed consent was signed and obtained by each participant. Due to a lack of data on diagnosing sarcopenia, depressive symptoms, and other indicators that would have an impact on both sarcopenia and depressive symptoms, some participants dropped out of the assessments due to personal reasons such as time conflicts, and final data from 1119 participants (452 men and 667 women) were eventually analysed. Figure 1 shows the flowchart of our study.
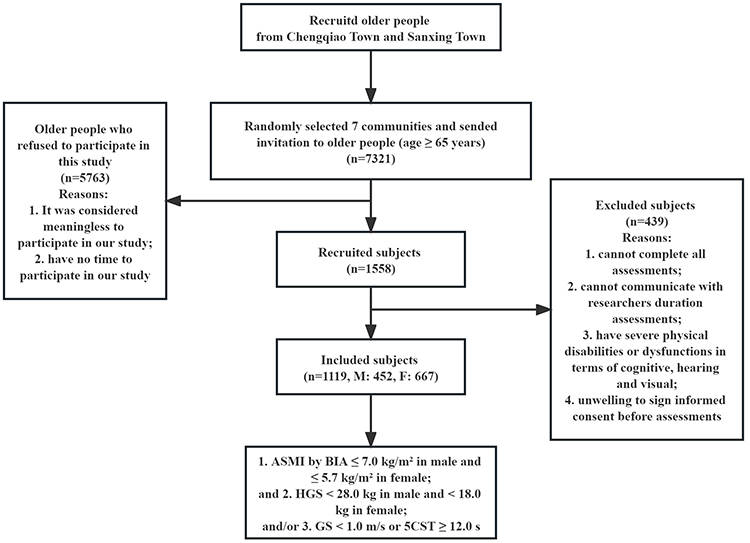 |
Figure 1 The flowchart of study. |
Assessment of Sarcopenia
In our study, participants with low muscle mass, decreased muscle strength and/or physical performance were identified as having sarcopenia, according to the AWGS 2019 consensus.28 Muscle mass was measured by the bioelectrical impedance analysis (BIA) (Inbody 720, Korea), and appendicular skeletal muscle mass index (ASMI) ≤ 7.0 kg/m2 in men and ≤ 5.7 kg/m2 in women was defined as low muscle mass. Muscle strength was measured by the hand dynamometer (Jamar Plus+ Digital Hand Dynamometer; IL, USA), and handgrip strength (HGS) < 28.0 kg in men and < 18.0 kg in women were defined as decreased muscle strength. Physical performance [6-meter walking test (6MWT) or 5-time chair stand test (5CST)] was used to assess the gait speed (GS) or the time of 5CST. And GS < 1.0 m/s measured by the 6MWT or the time of 5CST ≥ 12.0 s was defined as low physical performance. All assessments were performed in the community health service centers by assessors.
Assessment of Depressive Symptoms
The Geriatric Depression Scale-15 (GDS-15) is a tool for the screening of depressive symptoms in older people.29 It contains 15 items and each requires only a yes/no answer. The total score of this scale ranges from 0 to 15 points, and in our study, a score of < 5 was defined as having no depressive symptoms and a score of ≥ 5 was defined as having depressive symptoms.30,31 The assessment was performed in the community health service centers by asking participants and filling in scales by the assessors.
Assessment of Confounders
Clinical characteristics include age, gender, anthropometric, sociodemographic, and lifestyle. Anthropometric characteristic assessments include height, weight, body mass index (BMI), and percent of body fat (PBF). BMI was calculated by height and weight (BMI=height in meters/weight in kilograms2), and PBF was also assessed by BIA. Sociodemographic characteristics include income monthly, farming, educational level, and residence mode. Lifestyles include smoking, drinking, nutritional status, PA level, and sleep duration. Smoking and drinking status were both categorized as non-, current- and former- smoking/drinking. Nutrition status was assessed using the Mini Nutritional Assessment.32 Educational level was categorized into the following three levels: low (including those with no education and only with primary education), moderate (including those with junior and/or senior secondary education) and high (including those with high school education and above). PA was assessed by the short-form International Physical Activity Questionnaire in Chinese language (SF-IPAQ),33 and the level of PA was classified into the following three categories: high, moderate, and low, which are according to the criteria of SF-IPAQ. All assessments were performed in community health service centers by asking participants and filling in scales by the assessors.
Statistical Analyses
All statistical analyses were performed using the IBM SPSS Statistics version 24.0 (SPSS, Inc., USA). Continuous data were presented as mean ± standard deviation meanwhile categorical data were presented as numbers and percentages. Baseline characteristics of participants between different sarcopenia statuses were analysed by one-way analysis of variance test for analyzing continuous variable data, while Pearson’s chi-square test for the comparison of categorical variable data. Logistic regression analysis was used to explore the association between possible/confirmed sarcopenia and its diagnostic elements and depressive symptoms. The regression analysis was performed with the forward: LR method as the variable screening method. The dependent variable was the risk value for having depressive symptoms (subjects without depressive symptoms were coded as 0, while subjects with depressive symptoms were coded as 1), while the independent variables were age, BMI, PBF, sociodemographic (income monthly, farming, educational level, and residence mode), and lifestyles (smoking status, drinking status, nutritional status, physical activity level, and sleep duration). Of all independent variables, only age, BMI, PBF, and income monthly were continuous variables, while the rest were categorical variables. The odds ratio and 95% confidence intervals were recorded as analysed results. P-value < 0.05 is statistically significant.
Results
Characteristics of Participants with Different Sarcopenia Statuses
Among 1119 participants, 90 participants have depressive symptoms and 1029 participants did not have depressive symptoms. Among those 90 participants with depression symptoms, only 37 have no sarcopenia, while 25 have possible sarcopenia, 11 have general sarcopenia, and 17 have severe sarcopenia (p<0.001). The mean age was 71.80 ± 5.32 years old, with 40.4% were men and 59.6% were women. The mean ASMI was 6.81 ± 1.04 kg/m2, mean HGS was 27.93 ± 9.63 kg, mean GS was 0.85 ± 0.19 m/s, and mean 5CST time was 9.24 ± 3.19 s. The details of the characteristics of participants are shown in Table 1.
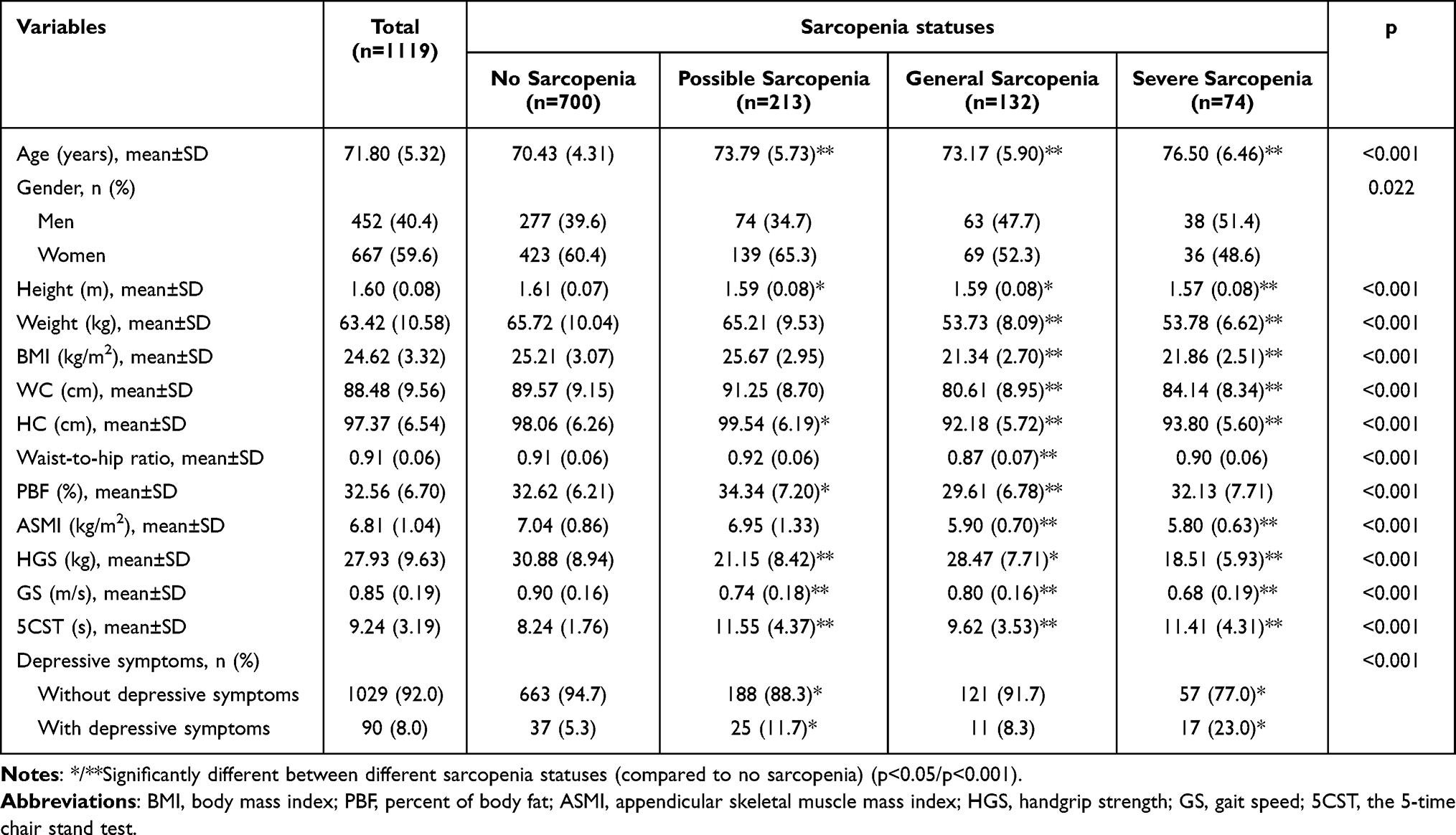 |
Table 1 Characteristics of Participants with Different Sarcopenia Statuses |
Characteristics of Participants in Men and Women
Table 2 shows the characteristics of participants in older men and women. Compared to older men, more older women in our study have depressive symptoms (M: 5.1% vs W: 10.0%, p=0.003). 55.9% of older women and 35.2% of older men are farmers (p<0.001). More older women are at low educational level than older men (M: 41.8% vs W: 56.4%, p<0.001). There are 16.8% of older women living alone. In terms of spouse status, 25.6% of older women are widowed, while 16.4% of older men are widowed (p<0.001). For smoking and drinking status, older men are significantly more than older women (both p<0.001).
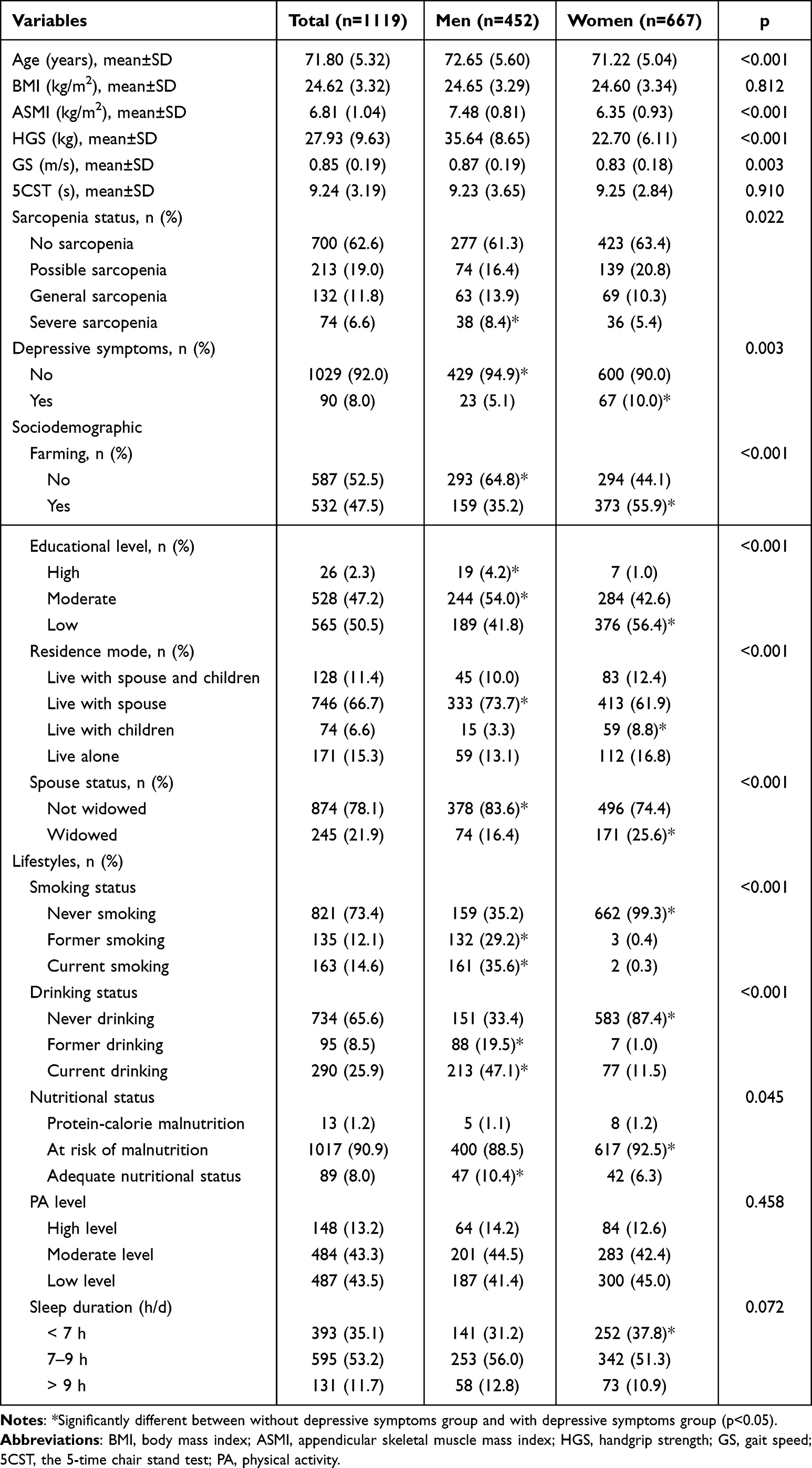 |
Table 2 Characteristics of Participants in Men and Women |
Prevalence of Depressive Symptoms in Different Sarcopenia Statuses in Older Men and Women
Among older people with possible sarcopenia, the prevalence of depressive symptoms was 5.41% and 15.11% in men and women. In general sarcopenia participants, the prevalence of depressive symptoms in men and women was 9.52% and 7.25%, respectively. There are 18.42% and 27.78% participants with depressive symptoms in older people with severe sarcopenia, and there are significant differences between the two. Figure 2 shows the prevalence of depressive symptoms in different sarcopenia statuses in men and women, respectively.
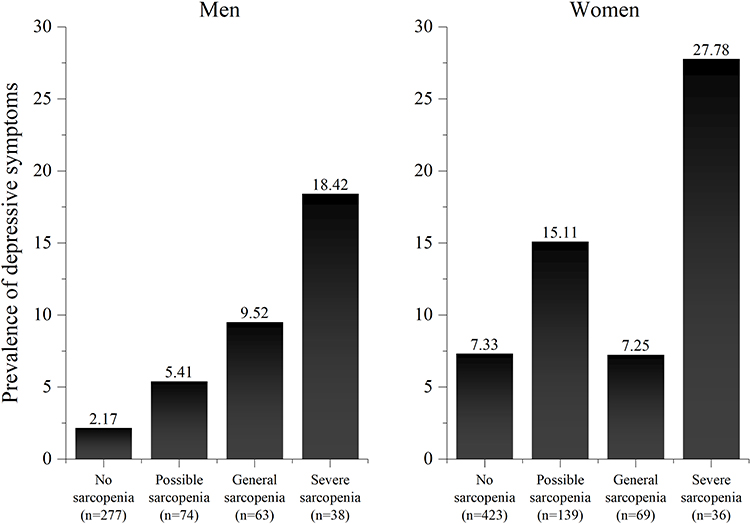 |
Figure 2 The prevalence of depressive symptoms in different sarcopenia status in men and women. |
Association Between Different Sarcopenia Statuses and Its Diagnostic Elements and Depressive Symptoms
We investigated the association between different sarcopenia statuses and depressive symptoms in older people using logistic regression analysis, and Table 3 shows the logistic regression analysis results of the association between different sarcopenia statuses and depressive symptoms in men and women, respectively. There was a significant association between no sarcopenia and depressive symptoms only in women, even after adjusting for confounders in all models [OR=0.516, 95% CI: 0.290–0.917 (p=0.024)]. And severe sarcopenia was also significantly associated with depressive symptoms only in women even after adjusting for confounders in all models [OR=2.802, 95% CI: 1.151–6.820 (p=0.023)]. Table 4 shows the logistic regression analysis results of the association between the diagnostic elements of sarcopenia and depressive symptoms in men and women, respectively. Only low ASMI was significantly associated with depressive symptoms in men, even after adjusting for confounders [OR=0.308, 95% CI: 0.129–0.737 (p=0.008)]; Low GS and poor 5CST were significantly associated with depressive symptoms in women, even after adjusting for confounders [OR=0.020, 95% CI: 0.004–0.117 (p<0.001)] [OR=1.172, 95% CI: 1.079–1.273 (p<0.001)].
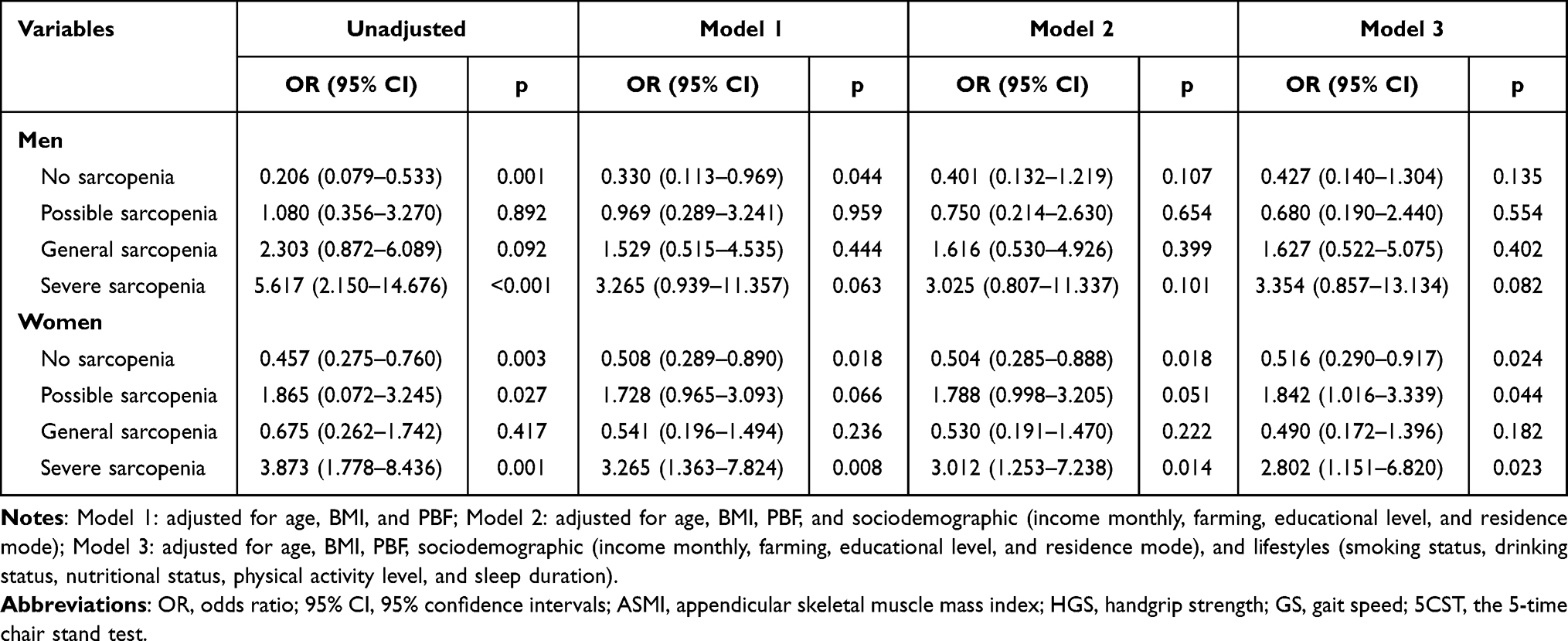 |
Table 3 Association Between Different Sarcopenia Statuses and Depressive Symptoms in Men and Women |
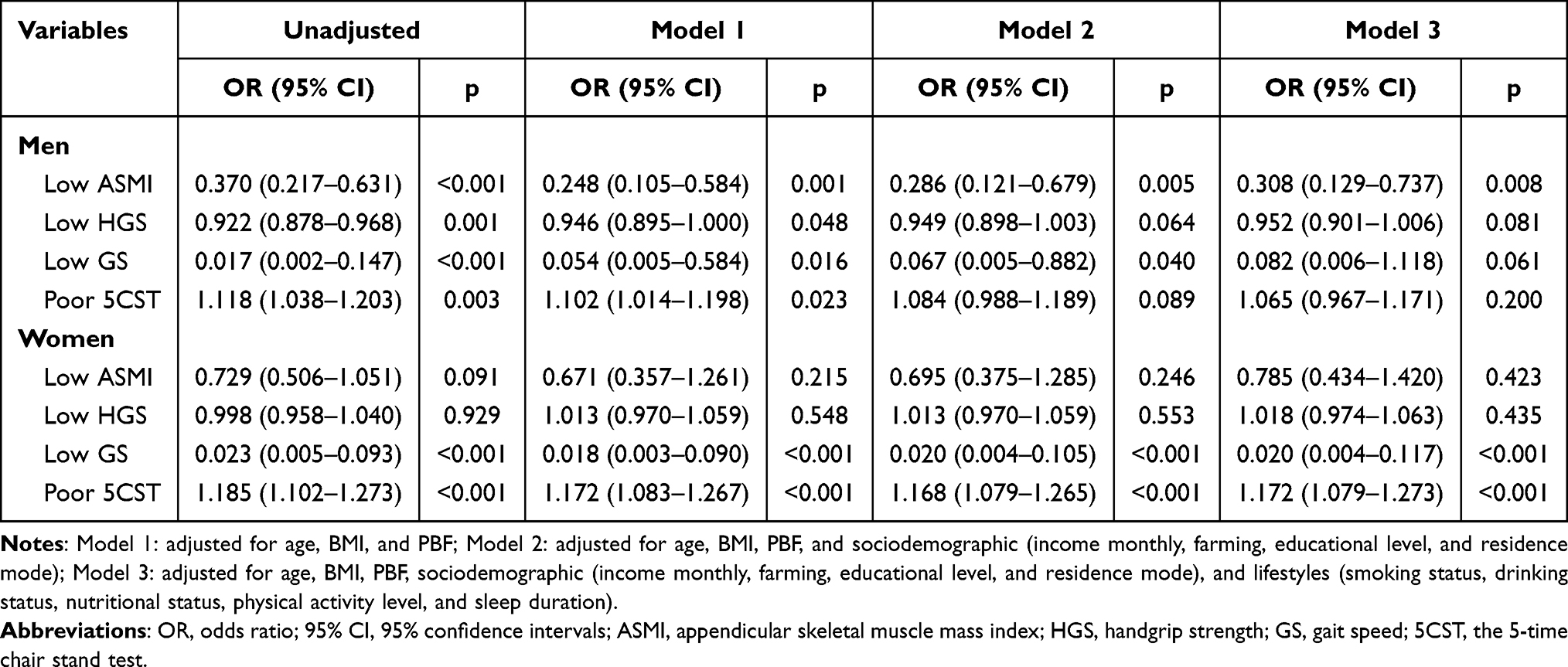 |
Table 4 Association Between the Diagnostic Elements of Sarcopenia and Depressive Symptoms in Men and Women |
Discussion
To our knowledge, this is the first study to investigate the relationship between different sarcopenia statuses and its diagnostic elements and depressive symptoms by gender among older people in a suburban area of Shanghai, China. The findings of this study were that women were much more likely than men to have depressed symptoms when they had severe sarcopenia, and at the same time, women without sarcopenia were less likely to suffer from depressive symptoms than men. After adjusting for confounders, there has a significant difference in the association between no sarcopenia and severe sarcopenia and depressive symptoms in women rather than men; In terms of the diagnostic elements of sarcopenia, low muscle mass (ASMI) was significantly associated with depressive symptoms only in men, while poor physical performance (including low GS and poor 5CST) was significantly associated with depressive symptoms only in women even after adjusting for confounders. However, there was no significant relationship between low muscle strength (HGS) and depressive symptoms in either men or women.
Depression is a very common disorder in the progression of ageing with a high prevalence rate of 27.10% in China,13 especially in women than men.26 In our study, we found that the proportion of women with depressive symptoms was significantly higher than that of men among older people with severe sarcopenia. The gender differences in the prevalence of depressive symptoms among severe sarcopenia may be due to the following reasons. First, women go through menopause as aging and the function of endocrine and metabolic changes significantly, and there is a greater sex hormone change in women (such as the decline of oestrogen level).34,35 Sarcopenia is associated with a lack of sex hormones (such as oestroge) which decrease with aging, that has a negative impact on satellite cell function.36 It has been proved that women with low oestrogen level are more susceptible to depression.35 Thus, it is a reason for more women than men with sarcopenia suffer from depressive symptoms. Second, significant psychological changes occur in women after puberty, peripartal period, and menopause (such as the development of neuroticism and post-traumatic stress disorder), as well as the changing role of women in life, lead to pessimistic thoughts about life and family, which may trigger depressive symptoms.5,37,38 The average life expectancy of women is higher than that of men,39 it is possible that older women are more likely than older men to experience widowhood. Our study also found that significantly more women than men experience widowhood (M: 16.4% vs W: 25.6%, p<0.001). Additionally, it has been demonstrated that experiencing widowhood was closely associated with depression.40 In addition to spouses, children also have a significant impact on women’s psychological state. Our study was conducted in a suburban area of China, which is characterized by many older people and most of their children choose to work outside the home, leading to an increasing number of older women living alone. Our study also did find that more women than men live alone (M: 13.1% vs W: 16.8%, p<0.001). It has been shown that living alone in older people significantly increases the risk of depressive symptoms.41 However, no studies have been conducted to explore gender differences in the psychology of older people with sarcopenia. We suggest that future studies should explore the difference between depressive symptoms and depression by gender among sarcopenic older people.
There are conflicting results from previous studies on the association between diagnostic elements of sarcopenia and depressive symptoms. Szlejf et al and Kim et al demonstrated that muscle mass was significantly and not significantly associated with depressive symptoms among older people (including men and women), respectively.19,42 However, these studies did not explore gender differences in the relationship between muscle mass and depressive symptoms. In our study, we found a significant negative association between muscle mass and depressive symptoms only in men. Compared to older women, older men in our study had more poor lifestyles, such as smoking, drinking, and excessive sleep duration, and these poor behaviors can accelerate age-related muscle mass loss, thereby exacerbating the severity of sarcopenia.43,44 At the same time, these poor behaviors may reduce the expression of factors related to neuronal plasticity (such as brain-derived neurotrophic factor, which is one of the biomarkers of depression),45 thus trigger to the development of mental disorders (such as depression).46–48 We, therefore, propose to reduce the development of depressive symptoms in older people by educating them about the negative effects of poor lifestyles in their daily lives and providing early interventions to prevent sarcopenia. In contrast, our study did not find a significant relationship between muscle mass and depressive symptoms in women. This may be related to gender differences in the mechanisms of muscle mass loss in sarcopenia. The development of sarcopenia is associated with a chronic low-inflammatory state,49 which in turn leads to an increase in the concentration of substances secreted by the hypothalamus and the hippocampus that may predispose to certain mental diseases (such as depression).5,11 And studies have shown that sex hormones in women (such as oestrogens) can protect skeletal muscle by reducing the inflammatory effects. Therefore, this may explain the absence of a significant relationship between muscle mass and depressive symptoms in women.
There is a significant relationship between physical performance and depressive symptoms found only in women. In our study, there were more farmers in older women than men. Heavy and repetitive agricultural activities can cause farmers to maintain inappropriate postures and overuse body functions for long periods of time, causing fatigue to themselves.50 Long-time agricultural activities make older people have no enough relax time for muscle recovery, which leads to musculoskeletal dysfunction and avoid them from PA.50 These situations may cause low PA level in older women, and our study also found that more older women are at low PA level than older men. However, it has been proved that maintaining a high PA level was associated with better lower limb function (including GS and the number of chair stands) among postmenopausal women.51 Thus, older women in our study may keep more poor lower limb function than men, which led to a poor lower limb strength for standing up from chairs. Indeed, physical inactivity increases the risk of depressive symptoms.52 Thus, it may be the reason for that a significant relationship between physical performance and depressive symptoms may only be found in older women in our study. Furthermore, pesticides exposure from agricultural activities may also be a cause of depression. Pesticides have been shown to make alterations in neurotransmitter levels, which are associated with various psychological dysfunctions (such as depression, anxiety, and suicidal ideation).53 Sufficient evidence suggests that exercise can be effective in improving muscle mass and physical performance among older people.54,55 Therefore, implementing exercise interventions to improve muscle mass and physical performance in older men and women, respectively, can be effective in the early prevention of depressive symptoms and increase the likelihood of healthy aging in older people.
Our study has strengths to this study. First, as there are significant differences between men and women in terms of sociodemographic and lifestyle, these differences can affect the association between sarcopenia and depressive symptoms. However, most current studies ignored the impact of gender on the relationship between sarcopenia and depressive symptoms. Thus, we investigated not only the relationship between sarcopenia and depression but also the relationship between the diagnostic elements of sarcopenia and depressive symptoms by gender, and provided a valid theoretical basis for the future implementation of early prevention and intervention for sex-specific older people. Second, previous studies were mostly conducted in urban areas, but studies in suburban areas are lacking. This is the first study to explore the association between sarcopenia and depressive symptoms in suburban area of Shanghai, China, and addresses the insufficient number of studies conducted in suburban areas.
Several limitations of the study should be considered. First, GDS-15, as a self-report scale, is commonly used to screen older people with depressive symptoms and is not used to diagnose depression. The participants’ response may cause recall bias that may have an influence on the prevalence of depressive symptoms. Second, our study used a cross-sectional design that cannot establish causality between sarcopenia and depressive symptoms. Thus, we recommend that future studies be performed using other types of designs (such as a longitudinal design) to explore the causal relationship between sarcopenia and depressive symptoms.
Conclusion
Our study indicated that compared to those with no sarcopenia, the prevalence of depressive symptoms in participants with possible sarcopenia and severe sarcopenia were significantly higher. Only in women, no sarcopenia and severe sarcopenia were both significantly associated with depressive symptoms even after adjusting for confounders. Low muscle mass was significantly associated with depressive symptoms only in men, while low physical performance was significantly associated with depressive symptoms only in women even after adjusting for confounders. Thus, intervention strategies focusing on muscle mass and physical performance may be included in the comprehensive management of depression.
Abbreviation
AWGS 2019, the Asian Working Group for Sarcopenia 2019; PA, physical activity; BIA, the bioelectrical impedance analysis; ASMI, appendicular skeletal muscle mass index; HGS, handgrip strength; 6MWT, the 6-meter walking test; 5CST, the 5-time chair stand test; GS, gait speed; GDS-15, the Geriatric Depression Scale-15; BMI, body mass index; PBF, percent of body fat.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The current study had achieved the approvement by the Ethical Committee of Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences in November 2020 (approval No. CMEC-2020-KT-42). Informed consent was signed and obtained by each participant and/or their legal guardian(s), for being willing to participate in this study and consented to the use of the study data for publication in an online open access publication. We confirm that all methods were performed in accordance with relevant guidelines and regulations. This study complied with the Declaration of Helsinki.
Acknowledgments
We would like to thank the Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences, China, and the Xinhua Hospital of Shanghai Jiaotong University School of Medicine, China, for their study support. We would also like to acknowledge all the participants for their time and contribution to this work.
Linqian Lu, Lin Mao, and Shanshan Yang contributed equally to this work and share first authorship.
Funding
This work was supported by the project of the National Natural Science Foundation of China “Mechanism of the Regulation of Skeletal Muscle Cell AMPK Pathway by Intestinal P.merdae in the Progression of Sarcopenia” (No.82102651), and the Center for Whole Population Whole Lifecycle Cohort Clinical Research (22MC2022001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
2. Wang LT, Huang WC, Hung YC, Park JH. Association between depressive symptoms and risk of sarcopenia in Taiwanese older adults. J Nutr Health Aging. 2021;25(6):790–794. doi:10.1007/s12603-021-1631-5
3. Wang H, Hai S, Liu Y, et al. Association between depressive symptoms and sarcopenia in older Chinese community-dwelling individuals. Clin Interv Aging. 2018;13:1605–1611. doi:10.2147/CIA.S173146
4. Stenvinkel P, Carrero JJ, von Walden F, Ikizler TA, Nader GA. Muscle wasting in end-stage renal disease promulgates premature death: established, emerging and potential novel treatment strategies. Nephrol Dial Transplant. 2016;31(7):1070–1077. doi:10.1093/ndt/gfv122
5. Alexopoulos GS. Depression in the elderly. Lancet. 2005;365(9475):1961–1970. doi:10.1016/S0140-6736(05)66665-2
6. Smith K. Mental health: a world of depression. Nature. 2014;515(7526):181.
7. Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. 2018;212(5):279–286. doi:10.1192/bjp.2018.27
8. Beaudart C, Rizzoli R, Bruyère O, Reginster J-Y, Biver E. Sarcopenia: burden and challenges for public health. Arch Public Health. 2014;72(1):45. doi:10.1186/2049-3258-72-45
9. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res. 2020;126:134–140. doi:10.1016/j.jpsychires.2019.08.002
10. Chen L-K, Liu L-K, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
11. Li Z, Tong X, Ma Y, Bao T, Yue J. Prevalence of depression in patients with sarcopenia and correlation between the two diseases: systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2022;13(1):128–144. doi:10.1002/jcsm.12908
12. Chang K-V, Hsu T-H, W-T W, Huang K-C, Han D-S. Is sarcopenia associated with depression? A systematic review and meta-analysis of observational studies. Age Ageing. 2017;46(5):738–746. doi:10.1093/ageing/afx094
13. Gao K, W-Z M, Huck S, et al. Association between sarcopenia and depressive symptoms in Chinese older adults: evidence from the china health and retirement longitudinal study. Front Med Lausanne. 2021;8:755705. doi:10.3389/fmed.2021.755705
14. Fan X, Yuan J, Wei Y, et al. Association between suicide risk severity and sarcopenia in non-elderly Chinese inpatients with major depressive disorder. BMC Psychiatry. 2020;20(1):345. doi:10.1186/s12888-020-02763-1
15. Zhang HY, Chong MC, Tan MP, Chua YP, Zhang JH. The association between depressive symptoms and sarcopenia among community-dwelling older adults: a cross-sectional study. J Multidiscip Healthc. 2022;15:837–846. doi:10.2147/JMDH.S355680
16. Byeon C-H, Kang K-Y, Kang S-H, Kim H-K, Bae E-J. Sarcopenia is not associated with depression in Korean adults: results from the 2010–2011 Korean national health and nutrition examination survey. Korean J Fam Med. 2016;37(1):37–43. doi:10.4082/kjfm.2016.37.1.37
17. Ma C. The prevalence of depressive symptoms and associated factors in countryside-dwelling older Chinese patients with hypertension. J Clin Nurs. 2018;27(15–16):2933–2941. doi:10.1111/jocn.14349
18. Hayashi T, Umegaki H, Makino T, Cheng XW, Shimada H, Kuzuya M. Association between sarcopenia and depressive mood in urban-dwelling older adults: a cross-sectional study. Geriatr Gerontol Int. 2019;19(6):508–512. doi:10.1111/ggi.13650
19. Kim NH, Kim HS, Eun CR, et al. Depression is associated with sarcopenia, not central obesity, in elderly Korean men. J Am Geriatr Soc. 2011;59(11):2062–2068. doi:10.1111/j.1532-5415.2011.03664.x
20. Hao L, Liang Y. The spatial and career mobility of China’s Urban and Rural labor force. Manag Organ Rev. 2016;12(1):135–158. doi:10.1017/mor.2015.35
21. Deluga A, Kosicka B, Dobrowolska B, et al. Lifestyle of the elderly living in rural and urban areas measured by the FANTASTIC Life Inventory. Ann Agric Environ Med. 2018;25(3):562–567. doi:10.26444/aaem/86459
22. Gao L, Jiang J, Yang M, Hao Q, Luo L, Dong B. Prevalence of sarcopenia and associated factors in Chinese community-dwelling elderly: comparison between Rural and Urban Areas. J Am Med Dir Assoc. 2015;16(11):1003.e1–e6. doi:10.1016/j.jamda.2015.07.020
23. Tian T, Chen Y, Zhu J, Liu P. Effect of air pollution and rural-urban difference on mental health of the Elderly in China. Iran J Public Health. 2015;44(8):1084–1094.
24. Kiely KM, Brady B, Byles J. Gender, mental health and ageing. Maturitas. 2019;129:76–84. doi:10.1016/j.maturitas.2019.09.004
25. Chen Z, Li W-Y, Ho M, Chau P-H. The prevalence of sarcopenia in Chinese older adults: meta-analysis and meta-regression. Nutrients. 2021;13:5.
26. Lu J, Xu X, Huang Y, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2021;8(11):981–990. doi:10.1016/S2215-0366(21)00251-0
27. Lim EJ. Sex differences in factors affecting depressive symptoms in older people in the prefrailty phase. Int J Environ Res Public Health. 2020;17(12):4207. doi:10.3390/ijerph17124207
28. Chen LK, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. Am Med Direct Asso. 2020;21(3):300–307. doi:10.1016/j.jamda.2019.12.012
29. Tang D. Application of Short form geriatric depression scale (GDS-15) in Chinese elderly. Chin J Clin Psychol. 2013;21(03):402–405.
30. Low S, Goh KS, Ng TP, et al. The prevalence of sarcopenic obesity and its association with cognitive performance in type 2 diabetes in Singapore. Clin Nutr. 2020;39(7):2274–2281. doi:10.1016/j.clnu.2019.10.019
31. Ng TP, Feng L, Yap KB, Lee TS, Tan CH, Winblad B. Long-term metformin usage and cognitive function among older adults with diabetes. J Alzheimers Dis. 2014;41(1):61–68. doi:10.3233/JAD-131901
32. Cereda E. Mini nutritional assessment. Curr Opin Clin Nutr Metab Care. 2012;15(1):29–41. doi:10.1097/MCO.0b013e32834d7647
33. Qu N, Li K. Study on the reliability and validity of international physical activity questionnaire (Chinese Vision, IPAQ). Chin J Epidemiol. 2004;25(3):265–268.
34. Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry. 2017;4(2):146–158. doi:10.1016/S2215-0366(16)30263-2
35. Albert KM, Newhouse PA. Estrogen, Stress, and Depression: cognitive and Biological Interactions. Annu Rev Clin Psychol. 2019;15:399–423. doi:10.1146/annurev-clinpsy-050718-095557
36. La Colla A, Pronsato L, Milanesi L, Vasconsuelo A. 17β-Estradiol and testosterone in sarcopenia: role of satellite cells. Ageing Res Rev. 2015;24(Pt B):166–177. doi:10.1016/j.arr.2015.07.011
37. Howard LM, Molyneaux E, Dennis C-L, Rochat T, Stein A, Milgrom J. Non-psychotic mental disorders in the perinatal period. Lancet. 2014;384(9956):1775–1788. doi:10.1016/S0140-6736(14)61276-9
38. Seng JS, Rauch SAM, Resnick H, et al. Exploring posttraumatic stress disorder symptom profile among pregnant women. J Psychosom Obstet Gynaecol. 2010;31(3):176–187. doi:10.3109/0167482X.2010.486453
39. National Bureau of Statistics of China. The average life expectancy of men in China; 2022. Available from: http://data.stats.gov.cn/easyquery.htm?cn=C01&zb=A0304&sj=2018.
40. Xu J, Wu Z, Schimmele CM, Li S. Widowhood and depression: a longitudinal study of older persons in rural China. Aging Ment Health. 2020;24(6):914–922. doi:10.1080/13607863.2019.1571016
41. Stahl ST, Beach SR, Musa D, Schulz R. Living alone and depression: the modifying role of the perceived neighborhood environment. Aging Ment Health. 2017;21(10):1065–1071. doi:10.1080/13607863.2016.1191060
42. Szlejf C, Suemoto CK, Brunoni AR, et al. Depression is associated with sarcopenia due to low muscle strength: results from the ELSA-Brasil study. J Am Med Dir Assoc. 2019;20(12):1641–1646. doi:10.1016/j.jamda.2018.09.020
43. Johansson J, Morseth B, Scott D, Strand BH, Hopstock LA, Grimsgaard S. Moderate-to-vigorous physical activity modifies the relationship between sedentary time and sarcopenia: the Tromsø Study 2015–2016. J Cachexia, Sarcopenia Muscle. 2021;12(4):955–963. doi:10.1002/jcsm.12718
44. Lucassen EA, de Mutsert R, le Cessie S, et al. Poor sleep quality and later sleep timing are risk factors for osteopenia and sarcopenia in middle-aged men and women: the NEO study. PLoS One. 2017;12(5):e0176685. doi:10.1371/journal.pone.0176685
45. Salinas-Rodríguez A, Palazuelos-González R, Rivera-Almaraz A, Manrique-Espinoza B. Longitudinal association of sarcopenia and mild cognitive impairment among older Mexican adults. J Cachexia, Sarcopenia Muscle. 2021;12(6):1848–1859. doi:10.1002/jcsm.12787
46. Achttien R, van Lieshout J, Wensing M, van der Sanden MN, Staal JB. Symptoms of depression are associated with physical inactivity but not modified by gender or the presence of a cardiovascular disease; a cross-sectional study. BMC Cardiovasc Disord. 2019;19(1):95. doi:10.1186/s12872-019-1065-8
47. Pengpid S, Peltzer K. High sedentary behavior is associated with depression among Rural South Africans. Int J Environ Res Public Health. 2019;16(8):1413. doi:10.3390/ijerph16081413
48. Kim S, Choi J-Y, Moon S, Park D-H, Kwak H-B, Kang J-H. Roles of myokines in exercise-induced improvement of neuropsychiatric function. Pflugers Arch. 2019;471(3):491–505. doi:10.1007/s00424-019-02253-8
49. Bano G, Trevisan C, Carraro S, et al. Inflammation and sarcopenia: a systematic review and meta-analysis. Maturitas. 2017;96:10–15. doi:10.1016/j.maturitas.2016.11.006
50. Kang F, He Z, Feng B, Qu W, Zhang B, Wang Z. Prevalence and risk factors for MSDs in vegetable greenhouse farmers: a cross-sectional survey from Shandong rural area, China. Med Lav. 2021;112(5):377–386.
51. Laddu DR, Wertheim BC, Garcia DO, et al. Associations between self-reported physical activity and physical performance measures over time in postmenopausal women: the women’s health initiative. J Am Geriatr Soc. 2017;65(10):2176–2181. doi:10.1111/jgs.14991
52. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–539.
53. Kori RK, Mandrah K, Hasan W, Patel DK, Roy SK, Yadav RS. Identification of markers of depression and neurotoxicity in pesticide exposed agriculture workers. J Biochem Mol Toxicol. 2020;34(6):e22477. doi:10.1002/jbt.22477
54. Escriche-Escuder A, Fuentes-Abolafio IJ, Roldán-Jiménez C, Cuesta-Vargas AI. Effects of exercise on muscle mass, strength, and physical performance in older adults with sarcopenia: a systematic review and meta-analysis according to the EWGSOP criteria. Exp Gerontol. 2021;151:111420. doi:10.1016/j.exger.2021.111420
55. Deutz NEP, Bauer JM, Barazzoni R, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin Nutrit. 2014;33(6):929–936. doi:10.1016/j.clnu.2014.04.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.