Back to Journals » Nature and Science of Sleep » Volume 14
Gender Differences in Hippocampal/Parahippocampal Functional Connectivity Network in Patients Diagnosed with Chronic Insomnia Disorder
Authors Yang L, Yu S, Zhang L, Peng W, Hu Y, Feng F, Yang J ![]()
Received 26 December 2021
Accepted for publication 31 May 2022
Published 21 June 2022 Volume 2022:14 Pages 1175—1186
DOI https://doi.org/10.2147/NSS.S355922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Lili Yang,1,* Siyi Yu,1,2,* Leixiao Zhang,3 Wei Peng,1 Youping Hu,1 Fen Feng,4 Jie Yang1
1Department of Acupuncture & Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610075, People’s Republic of China; 2Acupuncture and Brain Science Research Center, Chengdu University of Traditional Chinese Medicine, Chengdu, 610075, People’s Republic of China; 3Department of Integrated Traditional and Western Medicine, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 4Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fen Feng, Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, No. 39 Shierqiao Road, Chengdu, Sichuan, 610072, People’s Republic of China, Email [email protected] Jie Yang, Department of Acupuncture & Tuina, Chengdu University of Traditional Chinese Medicine, No. 37 Shierqiao Road, Chengdu, Sichuan, 610075, People’s Republic of China, Email [email protected]
Background: Gender differences in hippocampal and parahippocampal gyrus (HIP/PHG) volumes have been reported in sleep disorders. Therefore, this study investigated the moderating effect of gender on the relationship between chronic insomnia disorder (CID) and the HIP/PHG functional connectivity (FC) network.
Methods: For this study, 110 patients diagnosed with CID (43 men and 67 women) and 60 matched good sleep control (GSC) (22 men and 38 women) were recruited. These participants underwent resting-state functional magnetic resonance imaging scans, after which a 2 × 2 (diagnosis × gender) analysis of variance was used to detect the main and interactive effect of insomnia and gender on their HIP/PHG FC networks.
Results: Although the main effect of insomnia on the HIP FC network was observed in the bilateral cerebellar tonsil, superior frontal gyrus, and the medial orbitofrontal cortex, effects on the PHG FC network were observed in the bilateral HIP and amygdala. In contrast, the main effect of gender on the HIP FC network was observed in the right cerebellum posterior lobe, the dorsolateral prefrontal cortex (DLPFC), and the supplemental motor area. Of note, the interactive effect of both insomnia and gender was observed in FCs between the right HIP and the dorsal anterior cingulate cortex, and then between the right PHG and DLPFC. Moreover, the FC between the right PHG and left DLPFC was positively associated with anxiety scores in the female patients with CID.
Conclusion: Our study identified that gender differences in brain connectivity existed between the HIP/PHG and executive control network in patients diagnosed with CID, these results will eventually extend our understanding of the important role that gender plays in the pathophysiology of CID.
Keywords: insomnia, gender difference, functional connectivity, hippocampus, parahippocampal gyrus
Introduction
Insomnia is a chief complaint that arises during clinical work, which is characterized by sleep dissatisfaction, in addition to difficulty initiating or maintaining sleep at night. It is accompanied by distress and impairments in daytime functioning.1,2 Studies have shown that insomnia disorder affects approximately 10–20% of the population, with approximately 50% progressing to the chronic course of the disease, ie, the chronic insomnia disorder (CID).3,4 In addition, during the coronavirus disease 2019 pandemic, the prevalence of insomnia doubled and tripled.5,6 Insomnia disorder incurs substantial health care and indirect costs because it poses a substantial risk toward developing mental disorders caused by impaired cognitive function.3,7,8 At present, the hyperarousal model is a final common pathway accounting for the pathophysiology of insomnia.1,9,10 However, no convergent brain alteration pattern across previous structural and functional neuroimaging studies was found.11–13 The main reason for this inconsistent finding is proposed to be because of the heterogeneous features of the patients with insomnia used in these studies.14,15 Thus, the investigation with different demographic information regarding CID would extend our understanding of the neuropathological of CID.
Gender differences in insomnia have been found and manifested in epidemiological, neurobiological, and psychological studies,16–18 with consistent results being observed during studies on epidemiology, which showed that insomnia was approximately 1.5 times more common in women than men.19 In women, but not in men, the risk ratio for developing insomnia also increased with age.19,20 A few studies have investigated the brain mechanism in relation to gender differences in patients with sleep disorders. In a functional neuroimaging study, Dai et al also observed that females with insomnia showed higher regional brain activities in the bilateral temporal gyrus and lower regional brain activities in the left limbic lobe.21 However, they did not explore the interactive effect of insomnia and gender on the brain regional activity. Based on our previous studies, we observed that gender did not affect the global functional connectivity (FC) density in patients with primary insomnia.22 Moreover, gender differences have been observed in the locus coeruleus functional network.23 However, till date, the neuropathological mechanism accounting for how gender differences affect insomnia has remained unclear.
The hippocampus and parahippocampus have been considered essential for sleep and emotion regulation,24,25 and showed gender differences in the circadian timing system.26,27 During previous neuroimaging studies of gender difference in insomnia, the most frequently reported brain region was the hippocampal and parahippocampal gyrus. Winkelman et al investigated the effects of gender and insomnia on the volume of the hippocampus, but no significant gender effect was observed, which was proposed to be because of the small sample size of this study.28 Alternatively, using surface-based structure analysis, Paul et al observed that the gender-specific regional hippocampal volume increased in patients with obstructive sleep apnea.16 Recently, Nicola et al also observed that an association existed between poor sleep quality and gray matter volume in the hippocampus and parahippocampal gyrus of women, but not in men, using a well-powered sample of healthy individuals (1074 young adults from the “Human Connectome Project”).18 Thus, investigating the potential modulating effect of gender on the hippocampal/parahippocampal function in patients with insomnia is essential to comprehensively understand insomnia-causing brain mechanisms.
The objective of this study was to explore the moderating effect of gender on the hippocampus/parahippocampal gyrus (HIP/PHG) functional network in patients with CID. Owing to the prominent role of HIP/PHG function in sleep processing, affective behaviors,24 and gender specificity,27 we hypothesized that interactive regions of insomnia and gender in the HIP/PHG functional network were identified and would be associated with mental symptoms (depression and anxiety) in patients with CID, especially in women.
Methods
Participants
The Institutional Review Board of the Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, China, approved this study (Ethics protocol number: 2018KL-041). Written informed consent was obtained from each subject before subjecting them to a magnetic resonance imaging (MRI) scan. The current study complies with the Declaration of Helsinki.
One hundred and ten patients with CID (43 men and 67 women) were recruited based on the criteria of the International Classification of Sleep Disorders-Third Edition.2 The inclusion criteria for patients were as follows: (1) They should be between 18 and 65 years old; (2) they should be right-handed; (3) they should have experienced at least 3 months of difficulty falling asleep, maintaining sleep, or early awakening; (4) they should have a Pittsburgh sleep quality index score (PSQI) above seven (PSQI > 7);29 and (5) they should be willing to stop taking medications or receiving any other treatment 2 weeks before beginning the intervention. Alternatively, the exclusion criteria were as follows: (1) Patients with any severe condition of cardiovascular, cerebrovascular, liver, kidney, and hematopoietic systems; (2) those whose secondary insomnia was caused through drugs, cervical spondylosis, or other diseases; (3) those having a history of serious organic disease or severe mental disease secondary to depression or generalized anxiety; (4) those with abnormal findings, such as infarction or focal lesion, on conventional brain MRIs; (5) pregnant, preparing for pregnancy or lactating women; and (6) those with MRI contraindications.
Meanwhile, 60 good sleep controls (GSCs, 22 men and 38 women) who matched with the gender, age, and education of the CID group were recruited as healthy controls. All control participants met the same exclusion criteria that were applied to the patient group.
Four CID and five GSC participants were excluded owing to excessive head motion artifacts and/or incomplete echo-planar imaging images after normalized data artificial checking was conducted. Finally, the remaining 55 GSC and 106 CID patients were included in the final analysis. Demographic characteristics and clinical features of patients included in each group for the final analysis are summarized in Table 1.
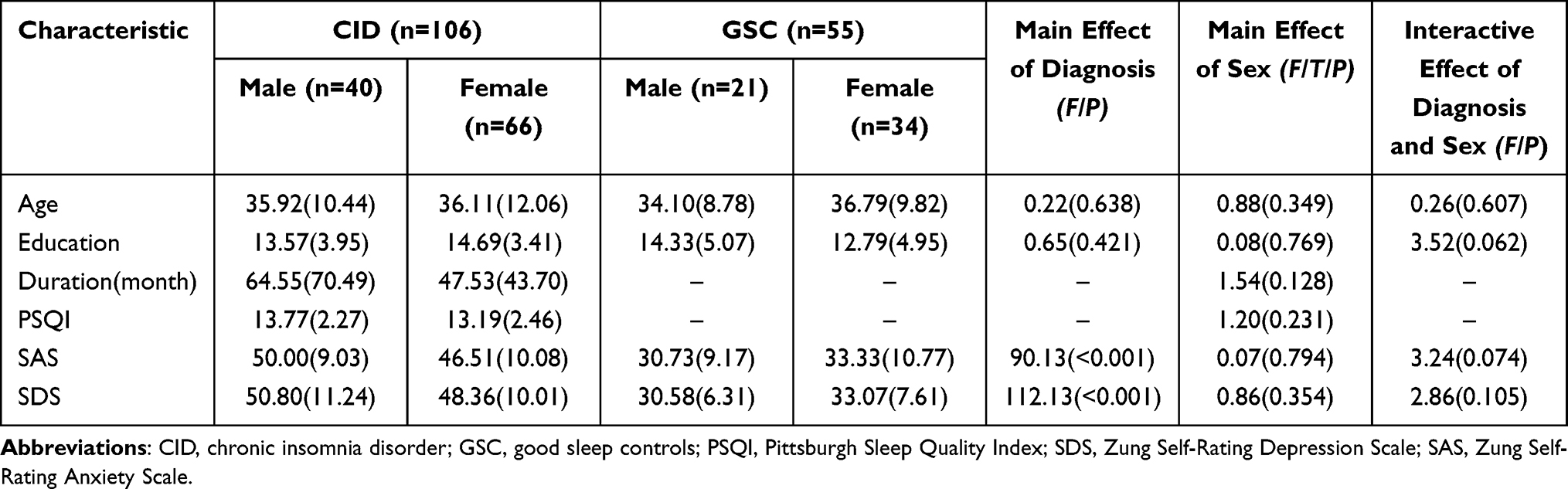 |
Table 1 Demographic and Clinical Traits for All Participants |
Clinical Assessments
Before MRI scanning, participants completed questionnaires that inquired about their PSQI, which is a seven-item inventory designed to assess the severity of insomnia symptoms, in addition to their Zung Self-Rating Anxiety Scale (SAS) and Zung Self-Rating Depression Scale (SDS) results, which were used to assess symptoms of anxiety and depression.30,31
MRI Data Acquisition and Preprocessing
MRI data were acquired using a 3.0 T MRI scanner (GE Healthcare Discovery MR750). Scans were conducted in the afternoon (14:00–18:00) at the University of Electronic Science and Technology of China. Afterward, structural images were acquired using a high-resolution 3D T1-weighted brain volume MRI sequence as follows: repetition time (TR)/echo time (TE) = 5.988/1.972 ms, slice thickness = 1 mm, slice number = 154, and field of view (FOV) = 256 × 256 mm. Subsequently, axial functional images were also obtained using a gradient-echo T2*-weighted echo-planar imaging sequence. Scanning parameters were as follows: TR/TE = 2000/30 ms, flip angle = 90°, slice number = 35, matrix size = 3.75 × 3.75, FOV = 64 × 64 mm, and slice thickness = 4 mm. With these parameters, 240 volumes were acquired in approximately 10 min. All participants in our study were instructed not to consume caffeine, alcohol, or any other psychoactive substance 48 h before the day on which the fMRI scan was to be conducted. Scanner noise and head motion were also reduced using earplugs and foam padding. All subjects were asked to close their eyes, lie quietly without falling asleep, not to think about anything, and avoid any head movement during the scan.
Subsequently, the original fMRI data obtained were pre-processed using the statistical parametric mapping package (SPM12, http://www.fil.ion.ucl.ac.uk/spm) and Data Processing Assistant for Resting-State fMRI (DPARSF) toolbox (http://www.restfmri.net) implemented in MATLAB v.8.0 (MathWorks Inc., Sherborn, MA, USA).32 Volumes of the first five time points were removed for everyone to reduce noise interference. Then, the following procedures were conducted: slice-timing adjustment, head motion correction adjustment, normalization of images with a T1 template in the Montreal Neurological Institute template space (resampling voxel size = 3 × 3 × 3 mm3), isotropic Gaussian kernel smoothing (full width at half maximum (FWHM) = 6 mm), in addition to detrending and filtering (0.01–0.1 Hz). Subjects with a head motion >2.5° of rotation or 2.5 mm of translation in any direction were excluded. Several sources of spurious variances were removed through linear regression, which included six head motion parameters and average signals from the white matter, cerebrospinal fluid, and the whole brain.
Seed-Based FC Analysis
The bilateral hippocampus and parahippocampal gyrus were selected using the WFU-Pick Atlas software (http://www.ansir.wfubmc.edu). The seed-based FC analysis was then performed using a DPARSF toolbox. Briefly, by extracting the residual blood oxygenation level-dependent time series from each seed and correlating that with the time series of all other voxels in the brain, first-level correlation maps were produced. Afterward, the Pearson’s correlation coefficients (FC values) that were obtained were further normalized to Z scores using Fisher’s transformation.
Statistical Analysis
Demographic and Clinical Data Analysis
The 2 × 2 (diagnosis × gender) ANOVA was used to compare the demographic and clinical data, such as age, education, duration of disease, PSQI, SAS, and SDS, using the Statistical Package for the Social Sciences software version 24.0 (SPSS, Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
Neuroimaging Data Analysis
Voxel-wise comparisons of FC mappings (bilateral HIP and PHG, separately) were conducted using a 2 × 2 (Diagnosis × gender) analysis of covariance, with age and years of education as nuisance covariates. The main effect of diagnosis, gender, and the interactive effect of diagnosis × gender was explored on the left/right HIP/PHG FC network, separately. The threshold was set at P < 0.005 for voxel-wise and P < 0.05 cluster-level for whole gray matter false discovery rate corrections.
Correlation Analysis
To investigate the behavioral significance of affected brain functions on the interaction between diagnosis and gender, mean FC signals were extracted from various brain regions. A partial correlation analysis was then conducted to examine relationships between FCs and PSQI scores (in addition to SAS and SDS scores and duration of disease) in men and women diagnosed with CID. The evaluation was conducted separately after controlling for the effects of age, education, and duration of disease (not in the correlation analyses between FCs and duration). As a preliminary and relatively small sample study, the results of partial correlation analyses were not corrected by any multiple comparison correction approaches.
Results
Demographics and Clinical Characteristics
Results from the comparison of demographic and clinical characteristics are displayed in Table 1 and Table S1. As shown, no significant main and interactive effect of diagnosis and gender on age and education was noted (all P > 0.05). However, SAS and SDS scores were higher in patients with CID than in the GSC group (P < 0.001). No group difference was observed in the duration of disease, PSQI, SAS, and SDS parameters between men and women in the CID group (P > 0.05). No significant interactive effects of diagnosis and gender were observed on SAS and SDS scores (P > 0.05).
Main Effects of Diagnosis on the HIP/PHG FC Network
The main effect of diagnosis was observed in both the HIP and PHG FC networks (Figures 1 and S1; Tables 2 and 3). For the left HIP FC network, patients with CID showed a higher HIP FC in the bilateral cerebellar tonsil, bilateral superior frontal gyrus (SFG), and left HIP/PHG in comparison with GSC subjects. However, a decreased HIP FC was observed in the bilateral medial orbitofrontal cortex (mOFC). For the right HIP FC network, an increased FC was observed in the right HIP/PHG and amygdala, with no decrease in FC in the right HIP FC network. However, for the bilateral PHG FC network, a significantly increased FC was observed in the bilateral HIP/PHG/amygdala, which was located in the amygdala–hippocampus complex, with no decrease in FC in the bilateral PHG FC network.
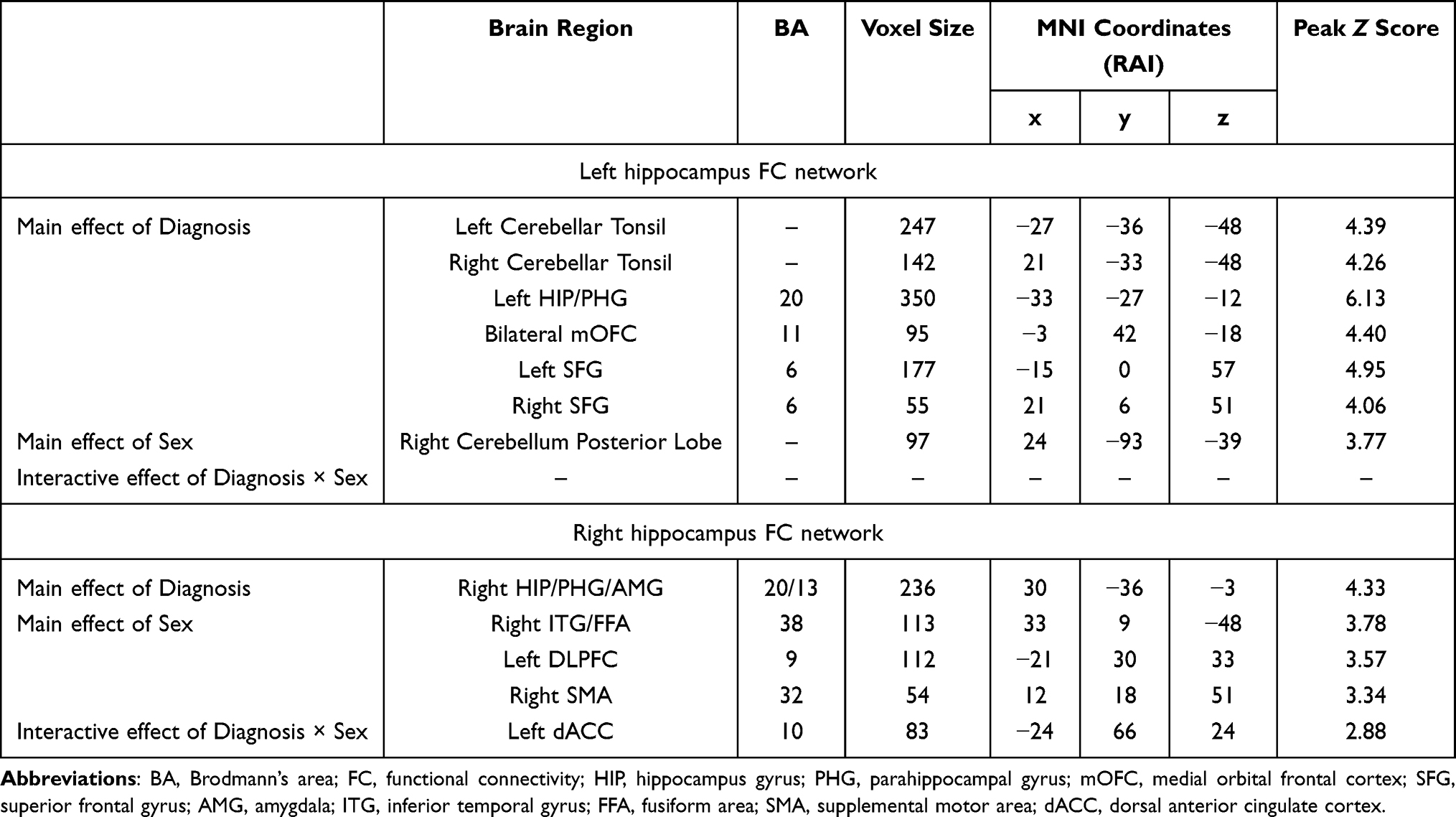 |
Table 2 Brain Areas with Significant Diagnosis, Sex and Diagnosis × Sex Effects on the Hippocampus Functional Connectivity Network |
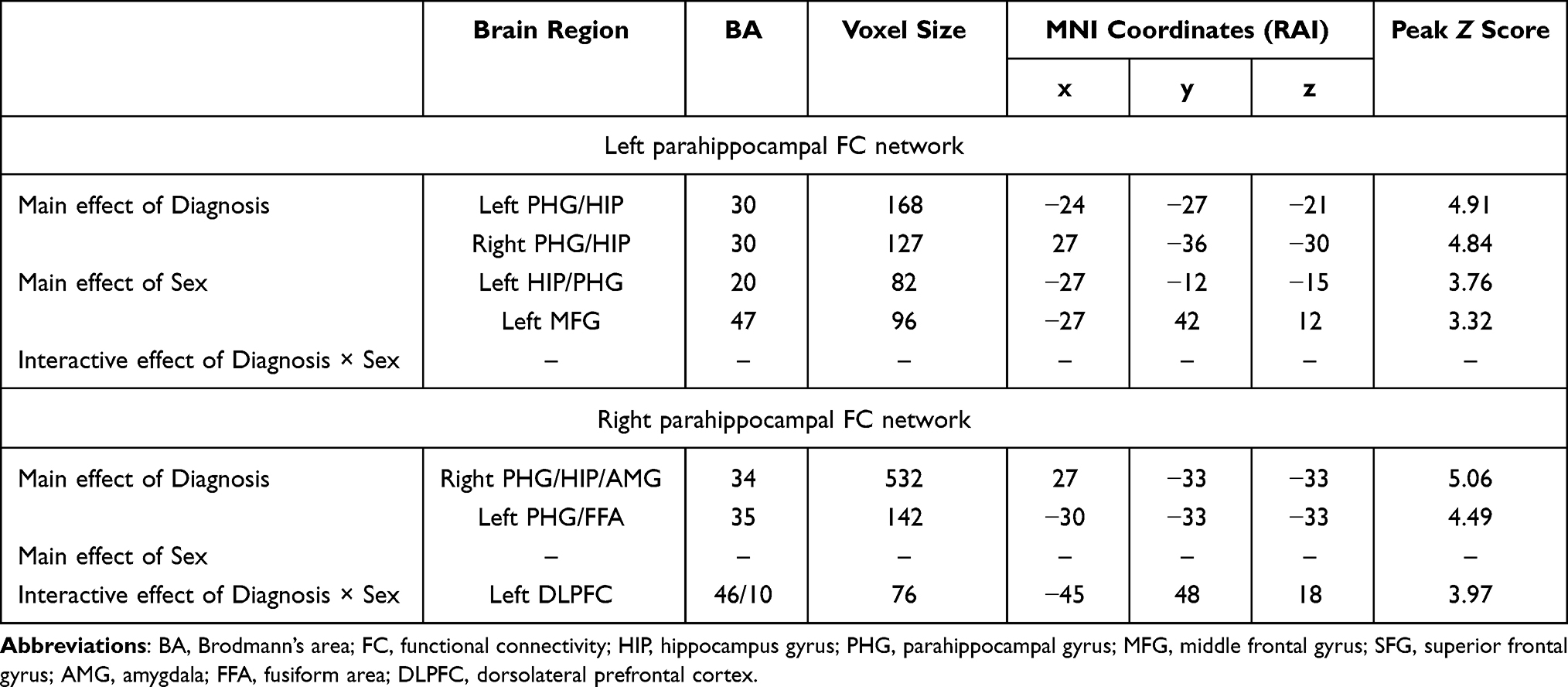 |
Table 3 Brain Areas with Significant Diagnosis, Sex and Diagnosis × Sex Effects on the Parahippocampal Functional Connectivity Network |
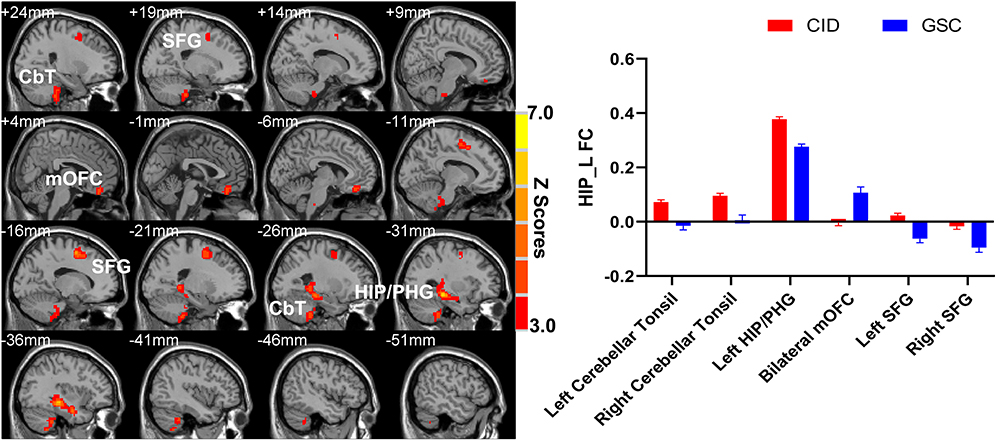 |
Figure 1 The main effect of diagnosis on the left hippocampus functional connectivity network. Abbreviations: CID, chronic insomnia disorder; GSC, good sleep control; HIP, hippocampus; FC, functional connectivity; Cbt, cerebellar tonsil; PHG, parahippocampal gyrus; mOFC, medial orbitofrontal cortex; SFG, superior frontal gyrus. |
Main Effects of Gender on the HIP/PHG FC Network
For the left HIP FC network, the main effect of gender was observed in the right cerebellum posterior lobe, with men showing a higher HIP FC than women (Figure 2A and B). Alternatively, for the right HIP FC network, women showed a lower HIP-negative FC in the left dorsolateral prefrontal cortex (DLPFC) and right supplemental motor area (SMA). However, they showed a lower HIP-positive FC in the right inferior temporal gyrus (ITG)/fusiform area (FFA) than men (Figure 2C and D). For the left PHG FC network, women showed a lower FC in left HIP/PHG than men. However, they showed a higher FC in the left middle frontal gyrus (MFG) than men (Figure S2). Nevertheless, no significant gender effect on the right PHG FC network was observed (Tables 2 and 3).
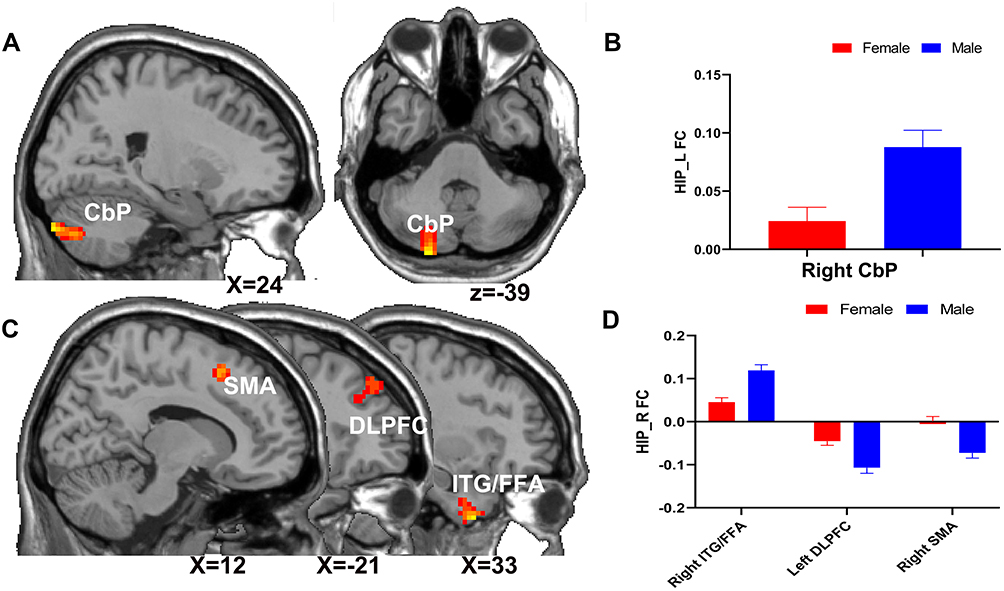 |
Figure 2 The main effect of gender on the hippocampus functional network. The main effect of gender on the left hippocampus functional network (located on the right CbP) (A and B); the main effect of gender on the right hippocampus functional network (located on the left DLPFC, right SMA, ITG, and FFA) (C and D). Abbreviations: CbP, cerebellar posterior lobe; DLPFC, dorsolateral prefrontal cortex; FFA, fusiform area; ITG, inferior temporal gyrus; SMA, supplemental motor area. |
Interactive Effects of Diagnosis and Gender on the HIP/PHG FC Network
An interactive effect of diagnosis and gender was observed on the right HIP and PHG FC networks (Figure 3 and Tables 2 and 3). The interaction was located in the left dorsal anterior cingulate cortex (dACC) at the right HIP FC network and in the left DLPFC at the right PHG FC network. As shown in Figure 3, women presented a lower negative FC between HIP/PHG and dACC/DLPFC than men in the GSC group. However, FCs were increased in women and decreased in men at the stage of CID.
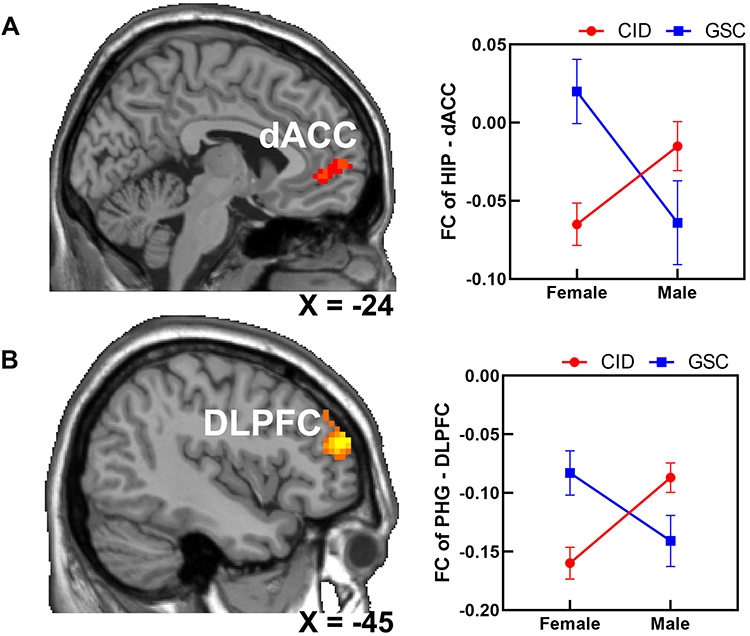 |
Figure 3 The interactive effect of diagnosis × gender on the right hippocampus functional connectivity network (A) and right parahippocampal gyrus functional connectivity network (B). Abbreviations: CID, chronic insomnia disorder; dACC, dorsal anterior cingulate cortex; DLPFC, dorsolateral prefrontal cortex; FC, functional connectivity; GSC, good sleep control; HIP, hippocampus; PHG, parahippocampal gyrus. |
Clinical Significance of the Interactive HIP/PHG FC Network
Partial correlation analysis results revealed that FC between the right PHG and left DLPFC was positively associated with SAS scores in women with CID (R = 0.27, P = 0.03) (Figure 4). The association was not significant to other regions and clinical features (P > 0.05).
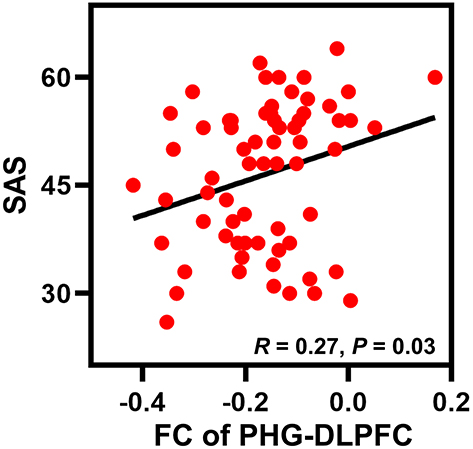 |
Figure 4 The functional connectivity between the right PHG and left DLPFC was positively associated with anxiety symptoms in women diagnosed with CID. Abbreviations: CID, chronic insomnia disorder; DLPFC, dorsolateral prefrontal cortex; FC, functional connectivity; PHG, parahippocampal gyrus; SAS, Zung Self-Rating Anxiety Scale. |
Discussion
This study explored the gender-specific effects of insomnia on the HIP/PHG function network. Based on our literature search, this study is the first to demonstrate gender-specific patterns of HIP/PHG function among individuals with and without insomnia. First, this study confirmed an association between insomnia and altered HIP/PHG function, which was in agreement with the findings of previous studies. Second, the full factorial model, using gender and insomnia factors, yielded an interaction between gender and diagnosis in FC of the right HIP-dACC and right PHG-DLPFC. Moreover, the correlation analysis corroborated the fact that a higher FC between the right PHG and DLPFC was associated with higher anxiety symptoms in women with CID. These results support our hypothesis that gender has a moderating effect on the HIP/PHG function in insomnia disorders. Taken together, our findings further indicate the importance of gender in the pathophysiology of CID.
Main Effects of Diagnosis on the HIP/PHG Functional Network
Abnormal hippocampal functions observed in insomnia have been reported in many previous studies. However, results have been inconsistent.33–36 Li et al reported an increased FC between the left HIP and left SFG in patients with insomnia, which was similar to the findings of this study.37 A decreased thalamic connectivity at the PHG and HIP has also been observed across wakefulness and sleep stages in patients with insomnia.38 In this study, an altered HIP/PHG FC was observed in the bilateral cerebellum, SFG, mOFC, and amygdala–hippocampus complex in patients with insomnia. Notably, the cerebellum has recently been considered to be involved in the sleep–wake cycle and consolidation of memories, with a malfunction in the cerebellum being proposed to affect sleep patterns.39 Furthermore, the increased FC between the HIP and the cerebellum is proposed to be indicated as a maladaptive mechanism during insomnia in memory consolidation. The FC of SFG and the HIP are reportedly negative in good sleepers, which indicates a control function of the frontal cortex to the HIP.40 However, for insomniacs, FC was decreased or inverted to positive, which also manifested in the abnormal control function observed in patients with CID. Alternatively, the mOFC is the core cortical region for reward and anticipation processing,41 with a decreased connectivity being observed between mOFC and HIP, which indicates an abnormal reward processing in patients with CID.15 Additionally, an increased HIP/PHG FC was widely observed within the amygdala, HIP, and PHG in patients with CID, which is proposed to account for the overloaded and maladaptive function noticed during the processing of emotion and cognition in these regions. Taken together, the present and previous results indicated that the HIP/PHG in patients with CID is dysfunctional; however, these inconsistent results suggest that future studies should focus on the heterogeneity of patients with CID.
Main Effects of Gender on the HIP/PHG Functional Network
Effects of gender differences in structural and functional features of the HIP and PHG have been manifested in both mice and human studies.27,42–45 However, much less is known about the effects of gender differences on the intrinsic FC in HIP/PHG using resting-state fMRI data. A recent task-based fMRI revealed gender differences in hippocampal connectivity during spatial memory processing.44 Moreover, Helpman et al investigated the gender-specific brain FC pattern during posttraumatic stress disorders. They observed a stronger FC between HIP and the precuneus in men than in women.46 In this study, gender differences were observed in the HIP FC network in the posterior cerebellum, DLPFC, SMA, and ITG/FFA, whereas gender differences in the PHG network were observed in the HIP/PHG and MFG. These brain regions have been considered during the processing of cognitive control (DLPFC), control of action (SMA),47 and face perception (FFA),48 which also present gender differences in their function. Thus, our findings extended the knowledge on gender differences in brain function.
Interaction Effects of Insomnia and Gender on the HIP/PHG Functional Network
The effect of insomnia-by-gender was located in the FC between the HIP/PHG and dACC/DLPFC, which are core hubs in the cognitive control network.49 Specifically, the FC between HIP and dACC was higher in men with insomnia compared with men without insomnia, whereas in women, the effect was inverse. A similar moderating effect of gender was observed in the left DLPFC in the PHG functional network. Based on the structural connectivity analysis, Tunç et al found that men showed a higher structural connectivity, which was associated with a motor and executive function subnetwork, than females.50 Previous task-based fMRI studies have also revealed gender differences during response inhibition processing. As observed, men showed higher functional connectivity than women in the anterior cingulate cortex, parahippocampal gyrus, and thalamus during successful inhibition.51,52 Another task-based fMRI revealed that the left ACC and DLPFC showed different activity patterns between men and women during a verbal fluency task.53 Moreover, gender-specific activation patterns were also shown in the DLPFC, hippocampus, and PHG during other high-level cognitive processes such as planning and problem solutions.54 The gender effect on sleep, including the gender steroid (estrogen) on sleep modulation and neuroendocrine in sleep circuitry systems, has received more attention as well.55 These findings therefore indicate that men and women with insomnia employed different FC patterns between the HIP/PHG and executive control network, which supported different HIP-frontal connectivity mechanisms during insomnia development.
Clinical Associations Within the Interactive HIP/PHG FC Network
Gender differences have been observed in cases of insomnia’s comorbidity with depression and anxiety.56 Besides, the relationship between insomnia and mental illnesses, such as depression and anxiety, is bidirectional.57,58 The present study could not find any interaction between the diagnosis and gender or depression and anxiety, which can be attributed to the small sample size. For the clinical association analysis, we observed that a stronger connectivity in PHG-DLPFC was associated with higher anxiety symptoms in women with insomnia but not in men with insomnia. Notably, the FC of PHG-DLPFC was negative in women without insomnia because the DLPFC is the core region for cognitive control.49 This negative FC is proposed to negatively regulate the sleep control pathway. However, in women with insomnia, the negative connectivity was increased and associated with more anxiety symptoms. These findings indicate a maladaptive frontal function in women with insomnia, which also helps to extend our understanding of higher insomnia’s comorbidity with anxiety in women.
Limitations
This study had several limitations worth mentioning. First, this preliminary study selected the whole HIP and PHG as regions of interest to explore the HIP/PHG function. However, future studies should investigate the gender modulating effect on the HIP/PHG substructure function in patients with insomnia disorders.59 Second, genetic factors were not investigated in this study. Although it was noted that patients with insomnia had alterations in the APOE genotype in the hippocampus in a previous study,60 future studies can explore genetic and gender interactions on the brain function in patients with CID. Third, because insomnia is a heterogeneous disorder, such as CID combined with or without mental symptoms,14,61 and different medication histories for the same may exist, this study provided subgroup analysis using a small sample size. Therefore, subtypes with mental symptoms should also be detected in future studies. Finally, the results obtained did not explain causal relationships between insomnia and brain function because of the cross-sectional design type of this study. Thus, future studies should also conduct research along this line.
Conclusion
This study demonstrated that the gender differences in brain connectivity existed between the HIP/PHG and executive control network in patients diagnosed with CID. These results extend our understanding of the important role played by gender in the pathophysiology of CID.
Funding
The National Natural Science Foundation of China (82004488), the Sichuan Provincial Science and Technology Department project in China (2021YJ0176, 2018JY0249), the China Postdoctoral Science Foundation Funded Project (2019M663454) and Chengdu University of Traditional Chinese Medicine Xinglin Scholar Discipline Talent Research and Improvement Plan (BSH2019011).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Riemann D, Nissen C, Palagini L, Otte A, Perlis ML, Spiegelhalder K. The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol. 2015;14(5):547–558. doi:10.1016/S1474-4422(15)00021-6
2. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
3. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1(1):15026. doi:10.1038/nrdp.2015.26
4. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
5. Kokou-Kpolou CK, Megalakaki O, Laimou D, Kousouri M. Insomnia during COVID-19 pandemic and lockdown: prevalence, severity, and associated risk factors in French population. Psychiatry Res. 2020;290:113128. doi:10.1016/j.psychres.2020.113128
6. Shi L, Lu ZA, Que JY, et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3(7):e2014053. doi:10.1001/jamanetworkopen.2020.14053
7. Staner L. Comorbidity of insomnia and depression. Sleep Med Rev. 2010;14(1):35–46.
8. Leger D, Bayon V. Societal costs of insomnia. Sleep Med Rev. 2010;14(6):379–389. doi:10.1016/j.smrv.2010.01.003
9. Riemann D, Spiegelhalder K, Feige B, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev. 2010;14(1):19–31. doi:10.1016/j.smrv.2009.04.002
10. Nofzinger EA, Buysse DJ, Germain A, Price JC, Miewald JM, Kupfer DJ. Functional neuroimaging evidence for hyperarousal in insomnia. Am J Psychiatr. 2004;161(11):2126–2128. doi:10.1176/appi.ajp.161.11.2126
11. Kay DB, Buysse DJ. Hyperarousal and beyond: new insights to the pathophysiology of insomnia disorder through functional neuroimaging studies. Brain Sci. 2017;7(12):23. doi:10.3390/brainsci7030023
12. Liu H, Shi H, Pan P. Brain structural and functional alterations in insomnia disorder: more “homogeneous” research is needed. Sleep Med Rev. 2018;42:234–235. doi:10.1016/j.smrv.2018.08.005
13. Tahmasian M, Noori K, Samea F, et al. A lack of consistent brain alterations in insomnia disorder: an activation likelihood estimation meta-analysis. Sleep Med Rev. 2018;42:111–118. doi:10.1016/j.smrv.2018.07.004
14. Yu S, Shen Z, Lai R, et al. The orbitofrontal cortex gray matter is associated with the interaction between insomnia and depression. Front Psychiatry. 2018;9:651. doi:10.3389/fpsyt.2018.00651
15. Gong L, Yu S, Xu R, et al. The abnormal reward network associated with insomnia severity and depression in chronic insomnia disorder. Brain Imaging Behav. 2021;15(2):1033–1042. doi:10.1007/s11682-020-00310-w
16. Macey PM, Prasad JP, Ogren JA, et al. Sex-specific hippocampus volume changes in obstructive sleep apnea. NeuroImage Clin. 2018;20:305–317. doi:10.1016/j.nicl.2018.07.027
17. Suh S, Cho N, Zhang J. Sex differences in insomnia: from epidemiology and etiology to intervention. Curr Psychiatry Rep. 2018;20(9):69. doi:10.1007/s11920-018-0940-9
18. Neumann N, Lotze M, Domin M. Sex-specific association of poor sleep quality with gray matter volume. Sleep. 2020;43(9). doi:10.1093/sleep/zsaa035
19. Zhang B, Wing YK. Sex differences in insomnia: a meta-analysis. Sleep. 2006;29(1):85–93. doi:10.1093/sleep/29.1.85
20. Carrier J, Semba K, Deurveilher S, et al. Sex differences in age-related changes in the sleep-wake cycle. Front Neuroendocrinol. 2017;47:66–85. doi:10.1016/j.yfrne.2017.07.004
21. Dai XJ, Nie X, Liu X, et al. Gender differences in regional brain activity in patients with chronic primary insomnia: evidence from a resting-state fMRI study. J Clin Sleep Med. 2016;12(3):363–374. doi:10.5664/jcsm.5586
22. Yu S, Guo B, Shen Z, et al. The imbalanced anterior and posterior default mode network in the primary insomnia. J Psychiatr Res. 2018;103:97–103. doi:10.1016/j.jpsychires.2018.05.013
23. Gong L, Shi M, Wang J, et al. The abnormal functional connectivity in the locus coeruleus-norepinephrine system associated with anxiety symptom in chronic insomnia disorder. Front Neurosci. 2021;15:522. doi:10.3389/fnins.2021.678465
24. Vecsey CG, Baillie GS, Jaganath D, et al. Sleep deprivation impairs cAMP signalling in the hippocampus. Nature. 2009;461(7267):1122–1125. doi:10.1038/nature08488
25. Havekes R, Abel T. The tired hippocampus: the molecular impact of sleep deprivation on hippocampal function. Curr Opin Neurobiol. 2017;44:13–19. doi:10.1016/j.conb.2017.02.005
26. Bailey M, Silver R. Sex differences in circadian timing systems: implications for disease. Front Neuroendocrinol. 2014;35(1):111–139. doi:10.1016/j.yfrne.2013.11.003
27. Hu Y, Wu DL, Luo CX, et al. Hippocampal nitric oxide contributes to sex difference in affective behaviors. Proc Natl Acad Sci U S A. 2012;109(35):14224–14229. doi:10.1073/pnas.1207461109
28. Winkelman JW, Benson KL, Buxton OM, et al. Lack of hippocampal volume differences in primary insomnia and good sleeper controls: an MRI volumetric study at 3 Tesla. Sleep Med. 2010;11(6):576–582. doi:10.1016/j.sleep.2010.03.009
29. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
30. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
31. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515. doi:10.1001/archpsyc.1965.01730060026004
32. Yan CG, Wang XD, Zuo XN, Zang YF. DPABI: data processing & analysis for (resting-state) brain imaging. Neuroinformatics. 2016;14(3):339–351. doi:10.1007/s12021-016-9299-4
33. Leerssen J, Wassing R, Ramautar JR, et al. Increased hippocampal-prefrontal functional connectivity in insomnia. Neurobiol Learn Mem. 2019;160:144–150. doi:10.1016/j.nlm.2018.02.006
34. Ma X, Jiang G, Tian J, et al. Convergent and divergent functional connectivity alterations of hippocampal subregions between short-term and chronic insomnia disorder. Brain Imaging Behav. 2021;15(2):986–995. doi:10.1007/s11682-020-00306-6
35. Regen W, Kyle SD, Nissen C, et al. Objective sleep disturbances are associated with greater waking resting-state connectivity between the retrosplenial cortex/hippocampus and various nodes of the default mode network. J Psychiatr Neurosci. 2016;41(5):295. doi:10.1503/jpn.140290
36. Gong L, Xu R, Liu D, et al. Abnormal functional connectivity density in patients with major depressive disorder with comorbid insomnia. J Affect Disord. 2020;266(4):417–423.
37. Li C, Dong M, Yin Y, Hua K, Fu S, Jiang G. Abnormal whole-brain functional connectivity in patients with primary insomnia. Neuropsychiatr Dis Treat. 2017;13:427–435. doi:10.2147/NDT.S128811
38. Zou G, Li Y, Liu J, et al. Altered thalamic connectivity in insomnia disorder during wakefulness and sleep. Hum Brain Mapp. 2021;42(1):259–270. doi:10.1002/hbm.25221
39. Canto CB, Onuki Y, Bruinsma B, van der Werf YD, De Zeeuw CI. The sleeping cerebellum. Trends Neurosci. 2017;40(5):309–323. doi:10.1016/j.tins.2017.03.001
40. Li W, Qin W, Liu H, et al. Subregions of the human superior frontal gyrus and their connections. Neuroimage. 2013;78:46–58. doi:10.1016/j.neuroimage.2013.04.011
41. Kringelbach ML. The human orbitofrontal cortex: linking reward to hedonic experience. Nat Rev Neurosci. 2005;6(9):691–702. doi:10.1038/nrn1747
42. Shors TJ, Chua C, Falduto J. Sex differences and opposite effects of stress on dendritic spine density in the male versus female hippocampus. J Neurosci. 2001;21(16):6292–6297. doi:10.1523/JNEUROSCI.21-16-06292.2001
43. van Eijk L, Hansell NK, Strike LT, et al. Region-specific sex differences in the hippocampus. NeuroImage. 2020;215:116781. doi:10.1016/j.neuroimage.2020.116781
44. Spets DS, Fritch HA, Slotnick SD. Sex differences in hippocampal connectivity during spatial long‐term memory. Hippocampus. 2021;31:669–676. doi:10.1002/hipo.23319
45. Lotze M, Domin M, Gerlach FH, et al. Novel findings from 2838 adult brains on sex differences in gray matter brain volume. Sci Rep. 2019;9(1):1–7. doi:10.1038/s41598-018-38239-2
46. Helpman L, Zhu X, Zilcha-Mano S, et al. Reversed patterns of resting state functional connectivity for females vs. males in posttraumatic stress disorder. Neurobiol Stress. 2021;15:100389. doi:10.1016/j.ynstr.2021.100389
47. Nachev P, Wydell H, O’Neill K, Husain M, Kennard C. The role of the pre-supplementary motor area in the control of action. Neuroimage. 2007;36(3):T155–163. doi:10.1016/j.neuroimage.2007.03.034
48. Kanwisher N, Yovel G. The fusiform face area: a cortical region specialized for the perception of faces. Philos Trans R Soc Lond B Biol Sci. 2006;361(1476):2109–2128. doi:10.1098/rstb.2006.1934
49. Vincent JL, Kahn I, Snyder AZ, Raichle ME, Buckner RL. Evidence for a frontoparietal control system revealed by intrinsic functional connectivity. J Neurophysiol. 2008;100(6):3328–3342. doi:10.1152/jn.90355.2008
50. Tunç B, Solmaz B, Parker D, et al. Establishing a link between sex-related differences in the structural connectome and behaviour. Philos Trans R Soc Lond B Biol Sci. 2016;371(1688):20150111. doi:10.1098/rstb.2015.0111
51. Li CS, Huang C, Constable RT, Sinha R. Imaging response inhibition in a stop-signal task: neural correlates independent of signal monitoring and post-response processing. J Neurosci. 2006;26(1):186–192. doi:10.1523/JNEUROSCI.3741-05.2006
52. Li CS, Huang C, Constable RT, Sinha R. Gender differences in the neural correlates of response inhibition during a stop signal task. Neuroimage. 2006;32(4):1918–1929. doi:10.1016/j.neuroimage.2006.05.017
53. Gauthier CT, Duyme M, Zanca M, Capron C. Sex and performance level effects on brain activation during a verbal fluency task: a functional magnetic resonance imaging study. Cortex. 2009;45(2):164–176. doi:10.1016/j.cortex.2007.09.006
54. Unterrainer JM, Ruff CC, Rahm B, et al. The influence of sex differences and individual task performance on brain activation during planning. NeuroImage. 2005;24(2):586–590. doi:10.1016/j.neuroimage.2004.09.020
55. Mong JA, Cusmano DM. Sex differences in sleep: impact of biological sex and sex steroids. Philos Trans R Soc Lond B Biol Sci. 2016;371(1688):20150110. doi:10.1098/rstb.2015.0110
56. Morin CM, Bjorvatn B, Chung F, et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: an international collaborative study. Sleep Med. 2021;87:38–45. doi:10.1016/j.sleep.2021.07.035
57. Jansson-Fröjmark M, Lindblom K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J Psychosom Res. 2008;64(4):443–449. doi:10.1016/j.jpsychores.2007.10.016
58. Alvaro PK, Roberts RM, Harris JK. The independent relationships between insomnia, depression, subtypes of anxiety, and chronotype during adolescence. Sleep Med. 2014;15(8):934–941. doi:10.1016/j.sleep.2014.03.019
59. Joo EY, Kim H, Suh S, Hong SB. Hippocampal substructural vulnerability to sleep disturbance and cognitive impairment in patients with chronic primary insomnia: magnetic resonance imaging morphometry. Sleep. 2014;37(7):1189–1198. doi:10.5665/sleep.3836
60. Grau-Rivera O, Operto G, Falcón C, et al. Association between insomnia and cognitive performance, gray matter volume, and white matter microstructure in cognitively unimpaired adults. Alzheimers Res Ther. 2020;12(1):4. doi:10.1186/s13195-019-0547-3
61. Taylor DJ, Lichstein KL, Durrence HH, Reidel BW, Bush AJ. Epidemiology of insomnia, depression, and anxiety. Sleep. 2005;28(11):1457–1464. doi:10.1093/sleep/28.11.1457
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.