Back to Journals » Psychology Research and Behavior Management » Volume 16
Gender Differences in Facial Emotion Recognition Among Adolescents Depression with Non-Suicidal Self-Injury
Authors He K ![]() , Ji S, Sun L, Yang T, Chen L
, Ji S, Sun L, Yang T, Chen L ![]() , Liu H, Wang K
, Liu H, Wang K
Received 27 April 2023
Accepted for publication 12 August 2023
Published 1 September 2023 Volume 2023:16 Pages 3531—3539
DOI https://doi.org/10.2147/PRBM.S418966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Kongliang He,1– 3 Sifan Ji,3 Lingmin Sun,3 Tingting Yang,2 Lu Chen,2 Huanzhong Liu,4 Kai Wang1,3
1Department of Neurology, the First Affiliated Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China; 2Psychological Counseling Department, Hefei Fourth People’s Hospital, Hefei, 230022, People’s Republic of China; 3School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, 230022, People’s Republic of China; 4Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, 230022, People’s Republic of China
Correspondence: Huanzhong Liu; Kai Wang, Email [email protected]; [email protected]
Objective: Despite the perception that healthy female are superior at emotional identification, it remains unclear whether gender-specific differences exist in adolescent depression and whether such specific differences in emotional recognition are associated with the most salient feature of adolescent depression---non-suicidal self-injury (NSSI).
Methods: In this study, 1428 adolescents (1136 females and 292 males) with depression and NSSI were examined using the Facial Emotion Recognition Task, Patient Health Questionnaire-9 (PHQ-9), and Functional Assessment of Self-mutilation questionnaire (FASM). This study was grouped by gender. Data were analyzed using the descriptive statistics, independent sample t-test, chi-square test, non-parametric test (Mann–Whitney U-test), Spearman correlation and Multiple linear regression analysis.
Results: Depressed females reported a significantly greater frequency of self-injurious behaviour and more severe depressive symptoms than males. Face emotion recognition was also significantly more accurate in females and was positively correlated with levels of self-injury and depression, whereas no such correlations were found in males. Among depressed adolescents, face emotion recognition is better in females and is associated with self-injurious behaviour.
Conclusion: This study found that the greater susceptibility to depression and NSSI among adolescent females may stem in part from superior recognition and sensitivity to the negative emotions of others.
Keywords: emotion recognition, non-suicidal self-injury, adolescent depression, gender
Introduction
Non-suicidal self-injury (NSSI) is defined as injury to body tissue that is direct, repetitive, and socially unacceptable, but without suicidal intention.1 Such behaviour typically occurs in early and mid-adolescence and is frequent in adolescents with depression. Surveys have reported a global lifetime NSSI prevalence of 13%–17%, while the estimated prevalence among Chinese adolescents appears higher at 27.4%.2 Further, the incidence of self-injury may also differ between females and males.3–5 Research has shown that the gender difference on self-injury may vary from age to age, with gender differences being greater in adolescents.6,7 However, several other studies show an equal prevalence of NSSI across males and females in Adolescents.4,8 Therefore, those findings of gender differences in self-injury symptoms still remain controversial, and there may be specific factors for gender differences in adolescent depression.
It is generally found that NSSI is associated with emotional regulation.9 Adolescents with self-injury disorders often encounter difficulties in emotional regulation which relies on emotional recognition as the latter may be a precursor to the former.10,11 Specifically, facial emotional perception is a crucial component to maintain adequate social function. Failure to accurately recognize emotional facial expressions will ultimately compromise the ability to use appropriate emotional regulation, which increases the risk of self-injury.12 Moreover, the qualitative stress theory posits that NSSI behaviour results from an interaction between adverse environmental factors and individual susceptibility.2 People who are better able to recognize negative emotions tend to develop a greater individual susceptibility to negative emotions and depression,13 aggravating the risk of self-injurious behaviors. Thus, emotion recognition is a possible risk factor for self-injury.
Facial expressions play an important functional social role in human existence, and at least six basic emotions have been found to be universally recognizable.14 The basic emotions include happiness, sadness, fear, surprise, and disgust anger.Significant gender differences exist in emotional processing, which is mainly reflected in the superior emotional recognition, emotional memory and susceptibility to negative emotions of women. A large number of early behavioral studies have demonstrated that females are able to recognize emotions more accurately and quickly as well as are more sensitive to emotions.15,16 It has been suggested that such emotional processing characteristics of females are closely related to their susceptibility to mood disorders such as depression and anxiety. For instance, repeated rumination on negative emotional events and inhibitory control of negative emotions are often leading sources of depressive disorders.17 Moreover, gender differences in emotional processing may contribute to the observed discrepancies in depressive episode prevalence and pattern between adolescent females and males.18 Thus, from the perspective of emotional processing, females at adolescent stage are at higher risk of depression, tending to suffer from more acute symptoms.
Several studies have reported a significant correlation between mood recognition disorder (misunderstanding the emotions of others) and depression, especially among adolescents,19 possibly because adolescents may be more susceptible to the harmful physical and psychological effects of interpersonal stressors such as loss and rejection, which, in turn, are major predictors of depression.20 Previous studies on emotional recognition deficits in adolescents with depression have yielded inconsistent results. One such study reported that adolescents with depression tend to misidentify happy and sad facial expressions as anger,21 while another concluded that depressed adolescents are able to quickly identify negative emotions such as sadness but not positive emotions such as happiness,22 and yet another concluded that depressed adolescents identify anger and fear more rapidly than non-depressed adolescents.23 Alternatively, other studies have found no abnormalities to recognize facial emotions among adolescents with depression.24,25
These inconsistencies may result at least in part from gender differences in emotional processing26(in addition to differences in study design, research methods, and other uncontrollable factors). Indeed, females of all ages are able to recognize emotions more accurately and quickly than males.27 Females are also more vulnerable to the physical and psychological effects of negative emotional events.28 Superior recognition of negative emotions from facial expression may increase the susceptibility to own negative emotions through emotional contagion, potentially resulting in depression.29,30 A few recent studies have found greater accuracy in the identification of negative emotions among depressed patients,31,32 it has been reported that emotion recognition is related to the severity of depressive symptoms. Specifically, patients with major depression tend to show more accurate recognition of negative emotions,11,33 suggesting that they are more likely to develop negative emotions in response to the negative emotions of others. Noteworthy, females are not only at higher risk of major depression, but also exhibit a greater incidence and severity of self-injurious behavior.7 Whereas, there are few studies on gender differences in the emotion recognition of depression in adolescents.
Consequently, the aim of the current study is to investigate gender differences in facial emotion recognition among adolescents with depression and self-injury, and to assess the association between facial emotion recognition capacity and self-injury in males and females. We hypothesized that females with depression and self-injurious behavior would be better able to recognize negative emotions than male adolescents with these same symptoms and that face emotion recognition would be more strongly correlated with self-injurious behavior among females.
Methods
Participants
Adolescents with depression were recruited from the outpatient clinics of 10 large tertiary hospitals across China from January to December 2020. A total of 2159 depressed adolescents between 12 and 18 years of age participated in this study, of whom 1428 (1136 females and 292 males) exhibited NSSI (Table 1). Inclusion criteria were as follows: (1) meeting the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), diagnostic criteria for Major Depressive Disorder or depressive episodes in bipolar disorder (outpatient depressive status meeting the criteria for depressive episodes); (2) 12–18 years of age (3) six years or more of formal education; (4) right-handed; (5) patients and guardians willing to participate and provide informed written consent. Exclusion criteria were as follows: (1) severe physical, infectious, or immune system diseases; (2) traumatic brain injury, epilepsy, or other known severe neurological or organic brain diseases; (3) schizophrenia, other severe mental disorders, or mental retardation. The study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Medical Ethics Committee of Hefei Fourth People’s Hospital. Written informed consent was provided by all participants and guardians prior to enrolment.
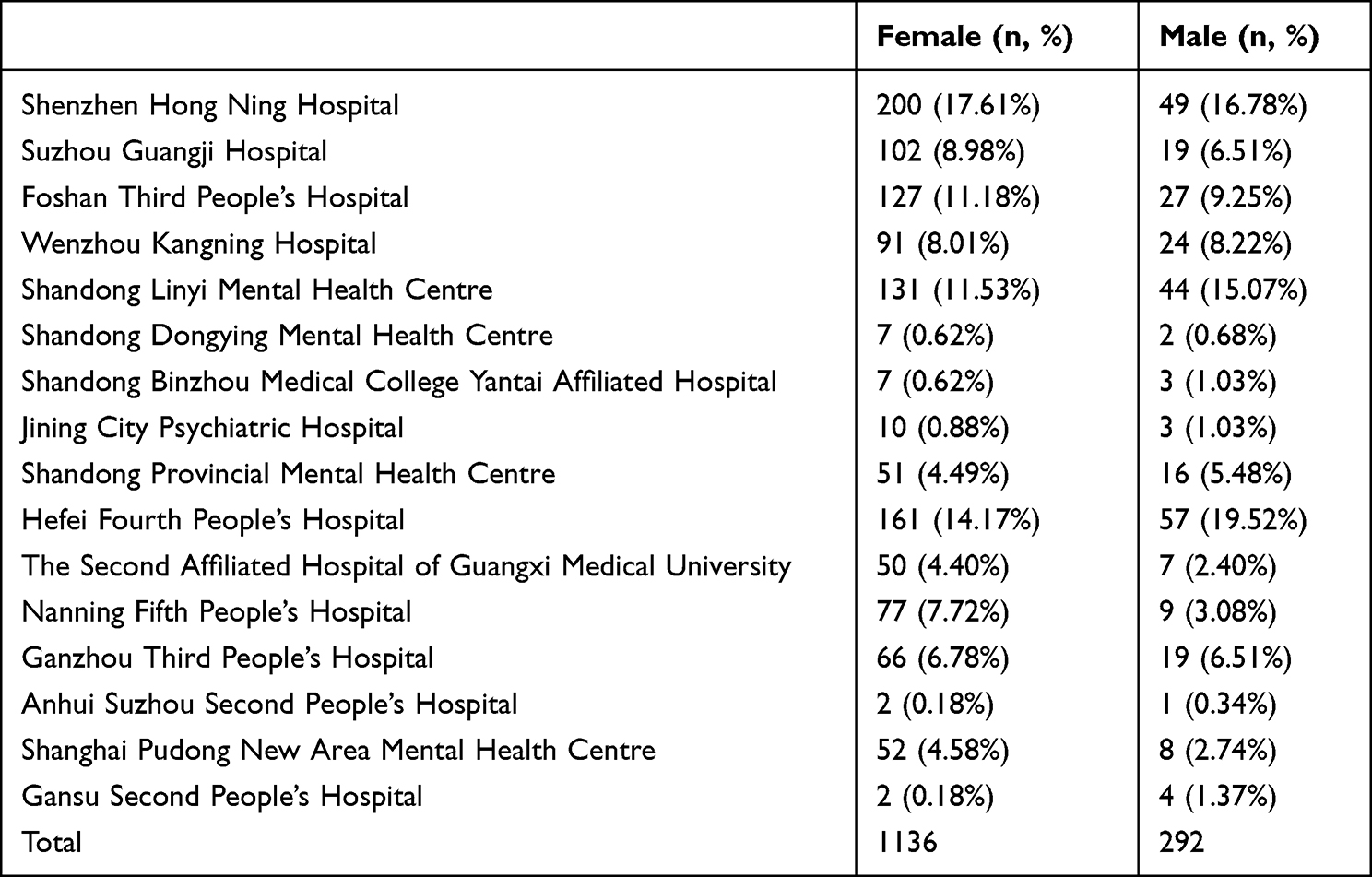 |
Table 1 Institutional Origins and Gender Ratios of Participants |
Measures
Functional Assessment of Self-Mutilation (FASM)
The FASM has demonstrated good reliability and validity for assessing self-injury in Chinese adolescents with depression, with Cronbach’ s alpha coefficient = 0.991.34 This self-report questionnaire assesses 11 common self-injurious behaviour in the past 12 months.34 If these self-injurious behaviour were expressed, subjects were asked to report the 1 under the corresponding questions. If no self-injurious behaviour was committed, they will fill in 0 under the corresponding questions. The higher the score is, the more serious the self-harming behaviors are.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a simple and efficient self-assessment tool for depression developed for the DSM-IV. It consists of nine items with four options for each answer. The total maximum score is 27, and higher scores indicate a greater likelihood of depression. The PHQ-9 has good internal consistency, with a Cronbach’ s alpha coefficient between 0.8 and 0.9,35 and good reliability and validity.36 It can be used for screening of primary community populations and specific populations to assist physicians in rapidly identifying depressed patients.
Facial Emotion Recognition Task
The emotion recognition task used in this project was adapted from a previous study,37 and developed by Huilongguan Hospital in Beijing, China. Still black and white pictures of faces expressing one of the seven basic emotions (anger, calm, disgust, fear, happiness, sadness, surprise) were selected from a pre-developed Chinese facial expressions picture library.38 Participants viewed six pictures of each emotion, 3 of females and 3 of males (42 in total), determines the category of the emotion. The partial half reliability of this test is 0.72 and the total retest reliability is 0.81.39
Study Procedure
All participants were informed of the purpose and significance of the study prior to enrolment. The sociodemographic questions and self-assessment scale items were read out by the researcher and then completed independently by the patients. For the Facial Emotion Recognition Task, participants were assessed individually in a quiet room while seated on an adjustable chair 60 to 80 cm from a 30-inch display screen. The participants were given practice items until they fully understood the task and response method. The test is conducted in the mode of automatic computer evaluation, with pictures of faces randomly presented on the computer screen. Briefly, pictures of faces were presented randomly on the computer screen, and the participant was required to determine the emotion, with one point given for a correct response and no points for an incorrect response. Each image was presented only once for an unlimited period of time until the response, and the next image was shown automatically after the response. Data were collected in the following order: participants first answered sociodemographic questions, followed by 2 self-assessment questionnaires, then finally a facial emotion recognition task.
Statistical Analysis
All results were analysed using SPSS 21.0. Adolescent depression scale and Facial Emotion Recognition Task results were stratified by gender to examine differences in self-harm, depressive status, and facial emotion recognition between males and females. Demographic data were compared between genders by independent sample t-test or chi-square test as indicated. The FASM and PHQ-9 scale scores were also compared by independent samples t-test. For the emotion recognition task, it was tested that the data did not conform to a normal distribution, thus the statistical analysis was performed using a non-parametric test (Mann–Whitney U-test). Associations of facial emotion recognition and self-injury were examined separately by gender using Spearman correlation. Furthermore, determining Independent Factors Influencing Self-Injurious Behavior in Adolescent Depression Using Multiple Linear Regression.
Results
Gender Differences in Self-Injury and Depression Severity
Adolescents with depression and NSSI were divided into two groups by gender and compared for depression and self-injurious behaviour severity. While neither age nor level of education differed between genders, females reported both more severe self-injury according to FASM score (t = 3.279, p < 0.01) and depression according to the PHQ-9 (t = 2.676, p < 0.01) compared to males (Table 2).
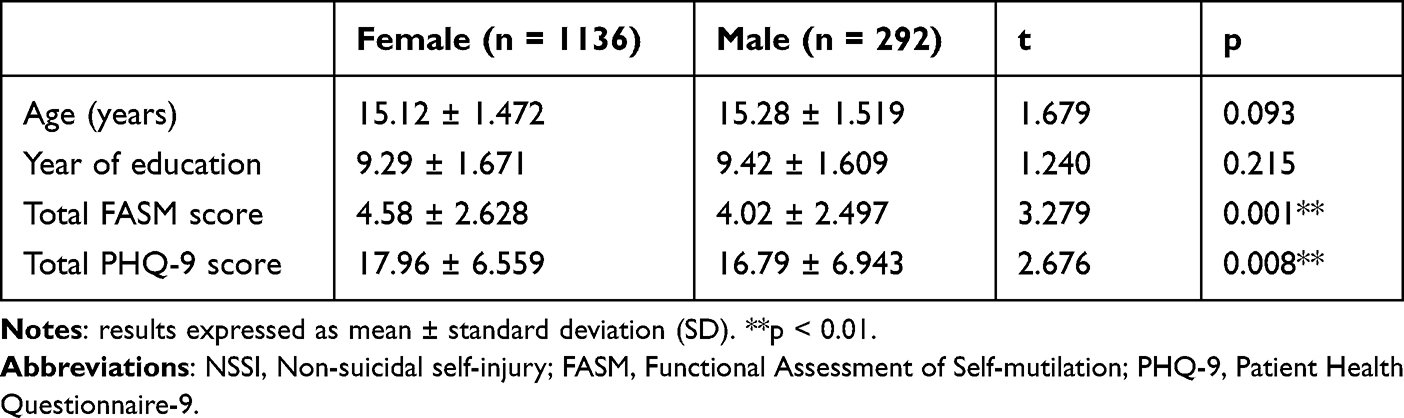 |
Table 2 Demographic and Clinical Characteristics of Male and Female Adolescents with Depression and NSSI |
Gender Differences in Facial Emotion Recognition
The results of the facial expression recognition test showed that females were more accurate at identifying facial expressions of disgust (z = −3.325, p = 0.001), fear (z = −2.541, p = 0.011), and surprise (z = −4.123, p < 0.001) than males, but were less accurate than males in identifying anger (z = −2.658, p = 0.008), while there were no gender differences in the identification of happy (z = −1.713, p = 0.121), sad (z = −1.271, p = 0.204), and calm (z = −1.045, p = 0.296) (Table 3). Overall, females exhibited greater accuracy in identifying facial emotions than males (z = −2.853, p = 0.004).
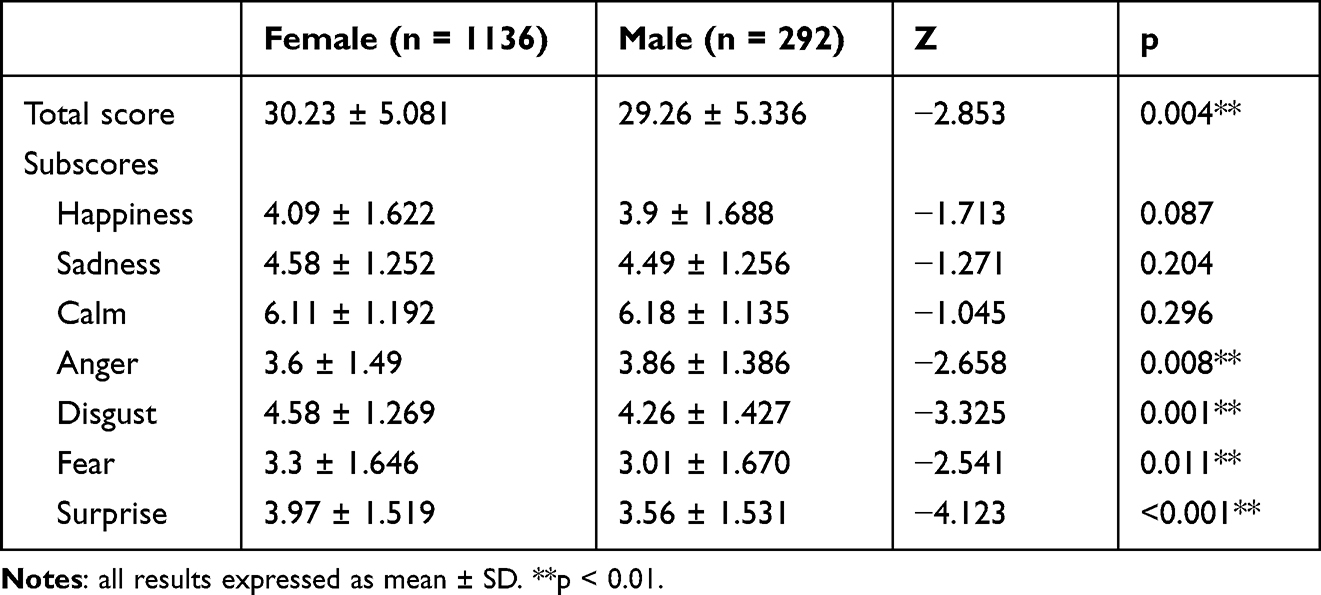 |
Table 3 Comparison of Facial Emotional Recognition Task Total Score and Subscores Between Male and Female Adolescents with Depression and NSSI |
Correlations Between NSSI, Depression and Emotional Recognition
In males, depression severity as measured by the PHQ-9 was positively associated with self-injurious behaviour (r = 0.247, p < 0.01), but total Facial Emotion Recognition Task score was not associated with the severity of either depression (r = −0.076, p > 0.05) or self-injurious behaviour (r = −0.031, p > 0.05) (Table 4). In females, depression was also positively associated with self-injurious behaviour (r = 0.363, p < 0.01), but in addition, total Facial Emotion Recognition Task score was positively associated with the severity of depression (r = 0.124, p < 0.01) and the severity of self-injurious behaviour (r = 0.120, p < 0.01) (Table 5).
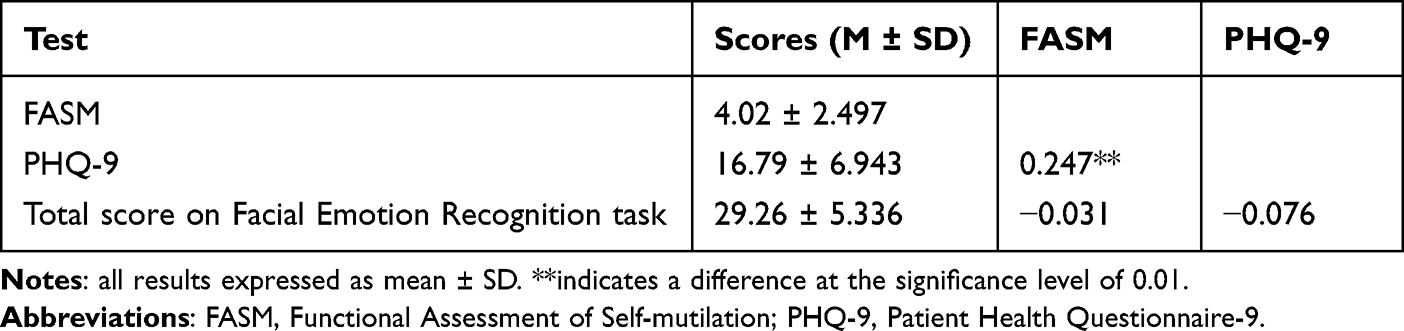 |
Table 4 Correlations of FASM and PHQ-9 Scores with Facial Emotion Recognition Task Performance in Males |
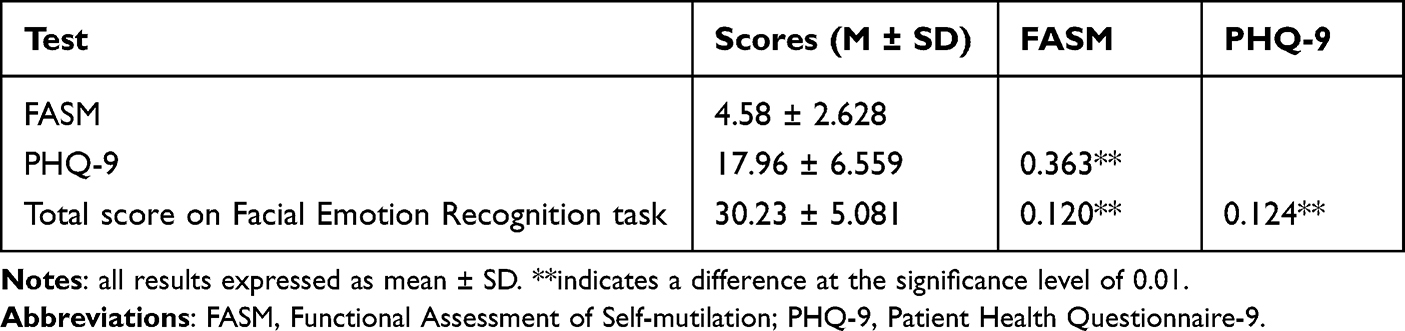 |
Table 5 Correlations of FASM and PHQ-9 Scores with Facial Emotion Recognition Task Performance in Females |
Multiple Linear Regression Analysis Among PHQ-9 Scores, Gender, and Total Facial Emotion Recognition Task Score
Multivariable linear regression analysis was conducted with the PHQ-9 scores, gender, and total Facial Emotion Recognition Task score as independent variables and the scores of FASM as dependent variables. Depression (Beta = 0.125, p <0.001), gender (Beta = 0.454, p =0.005), and emotion recognition (Beta = 0.042, p =0.001) were all findings to be independent factors influencing non-suicidal self-injury in depressed adolescents (Table 6).
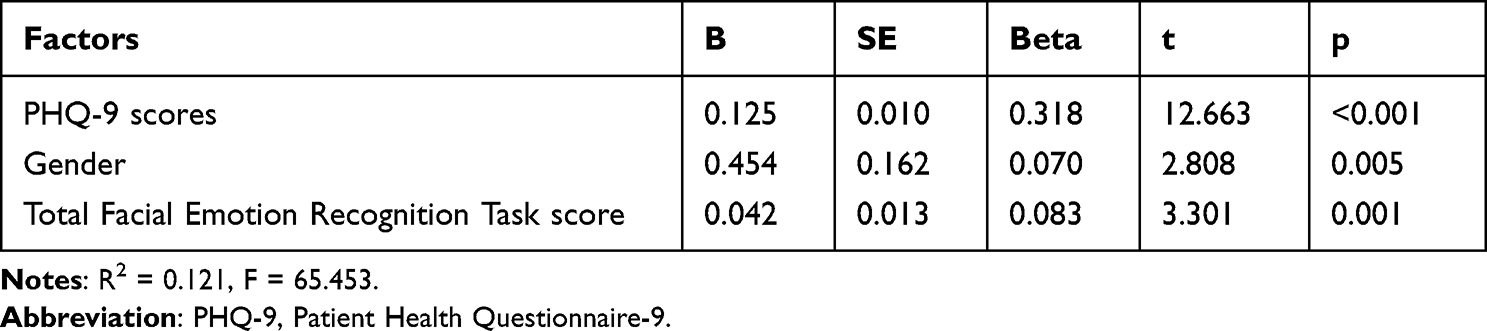 |
Table 6 Multivariate Logistic Regression Analysis of Factors Influencing NSSI Among Adolescents with Depression |
Discussion
The current findings suggest that depressed adolescent females exhibiting non-suicidal self-injury possess superior facial emotion recognition abilities as well as significantly more severe depression and self-injury compared to males with these same symptoms. Further, the level of self-injury in females but not males was positively associated with general facial emotion recognition capacity.
Previous studies have found that females are more accurate than males at identifying positive and negative emotions in faces27,40 due to greater inherent emotionality, which biases attention towards emotional stimuli.41 The present results are partially consistent with these findings in that depressed females with NSSI demonstrated significantly better overall facial emotion recognition than males. Unlike previous studies,27,40 however, we report significant gender differences in the identification of negative emotions but no differences in the identification of positive emotions. Possibly that’s since females with depressive symptoms and NSSI appear to show lower responsiveness to positive stimuli (consistent with the positive attenuation theory) and increased responsiveness to negative stimuli (consistent with the negative enhancement theory).42 Moreover, a few studies have reported mood-specific negative biases in judging facial expressions among individuals with depression,43,44 Major depressive disorder patients manifest an attentional bias to negative face stimuli,45 and females were proven to be at higher risk for major depression. Females with depression show a higher sensitivity to negative emotions, which enables them to more accurately identify negative emotions.46 Thus, Our findings provide further evidence that adolescent females with depression exhibiting greater recognition of negative emotions than males, presumably due to greater emotional sensitivity and susceptibility to the negative emotions of others.
Females in the present study identified facial expressions of fear, disgust, and surprise more accurately than males, but identified expressions of anger less accurately. A possible explanation is that anger is an emotional response to misfortune or an existential threat47 and is strongly associated with interpersonal conflict and aggressive behavior,48 which is a more dominant trait in males. Consistent with this notion, males have been found to be more aggressive and better at recognizing angry facial expressions than females.49,50 These findings in turn suggest that males are better able to interpret the aggressive messages of others (angry facial expressions) and respond with outwardly aggressive behaviour. Alternatively, that depressed adolescent females were less likely to correctly identify angry faces than males is consistent with a previous study reporting that depressed females were less sensitive to angry emotional faces.51 In contrast to these gender differences, we found no significant disparities in the accuracy of sad face recognition, possibly because sadness is a less physiologically and psychologically intense negative emotion than fear or anger. Thus, it appears that only highly stimulating negative emotional information can reveal gender differences in facial emotion recognition among adolescents with depression and NSSI.
Plenner and colleagues reported correlations among depression, self-injury, and emotion recognition, and suggested that the psychopathology of depression may evolve into self-injury due to a deficit in emotional processing.52 Further, several other studies have found that symptoms of depression are associated with a widespread deficit in facial emotion recognition.53,54 Individuals who engage in self-injurious behaviour frequently exhibit poor social communication and language skills as well as narrative impairment55,56 and deficits in emotional facial recognition.9 Furthermore, the development of depressive symptoms42 and the relationships among depression, NSSI, and emotion recognition in adolescents may differ by gender. The present study thus supports and extends previous research by demonstrating that these associations are indeed significantly stronger in females or exclusive to females. We suggest that females experience more severe depressive symptoms and exhibit more frequent self-injurious behaviour due to superior recognition and greater sensitivity to the negative cues (especially fear, disgust and disgust) conveyed by others.
The current study has several limitations. First, the cross-sectional study design does not allow for a causal interpretation of the results. Longitudinal studies are required to establish if emotion recognition disorder directly contributes to self-injurious behaviour among female adolescents with depression and NSSI. Second, there were many fewer males in the study cohort, so it is possible that other significant gender differences were missed due to insufficient statistical power. As male adolescents display a lower frequency of depression, a matched-sample study may be necessary to reveal additional gender differences in facial emotion recognition, NSSI, and depressive symptom patterns. Nonetheless, this is the first study with sufficient sample size to identify critical gender disparities in emotional recognition that may help explain the observed gender differences in prevalence, symptom severity, and self-injury pattern between adolescent males and females.
In conclusion, this study suggests that female adolescents with depression are more able to recognize negative emotions, are more sensitive to negative emotions of others, and this trait is associated with their NSSI behavior. These findings may have important implications for further research into NSSI pathomechanisms and gender-specific treatments.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Medical Ethics Committee of Hefei Fourth People’s Hospital. All individual-level data were anonymous. All patients gave their written informed consent.
Funding
This study was supported by National Natural Science Foundation of China (31970979), Key Projects of Applied Medical Research of Hefei Health Care Commission (Hwk2021zd013) and Fund project of Anhui Medical University (2022xkj118, 2022xkj116).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Plener PL, Kaess M, Schmahl C, Pollak S, Fegert JM, Brown RC. Nonsuicidal self-injury in adolescents. Dtsch Arztebl Int. 2018;115(3):23–30.
2. Hu Z, Yu H, Zou J, Zhang Y, Lu Z, Hu M. Relationship among self-injury, experiential avoidance, cognitive fusion, anxiety, and depression in Chinese adolescent patients with nonsuicidal self-injury. Brain Behav. 2021;11(12):e2419.
3. Muehlenkamp JJ. An investigation of differences between self-injurious behavior and suicide attempts in a sample of adolescents. Suicide Life Threat Behav. 2004;34(1):12–23.
4. Klonsky ED, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003;160(8):1501–1508.
5. Whitlock J, Eckenrode J, Silverman D. Self-injurious behaviors in a college population. Pediatrics. 2006;117(6):1939–1948.
6. Daukantaite D, Lundh LG, Wangby-Lundh M, et al. What happens to young adults who have engaged in self-injurious behavior as adolescents? A 10-year follow-up. Eur Child Adolesc Psychiatry. 2021;30(3):475–492.
7. Wilkinson PO, Qiu T, Jesmont C, et al. Age and gender effects on non-suicidal self-injury, and their interplay with psychological distress. J Affect Disord. 2022;306:240–245.
8. Nock MK, Joiner TE Jr, Gordon KH, Lloyd-Richardson E, Prinstein MJ. Non-suicidal self-injury among adolescents: diagnostic correlates and relation to suicide attempts. Psychiatry Res. 2006;144(1):65–72.
9. Seymour KE, Jones RN, Cushman GK, et al. Emotional face recognition in adolescent suicide attempters and adolescents engaging in non-suicidal self-injury. Eur Child Adolesc Psychiatry. 2016;25(3):247–259.
10. In-Albon T, Ruf C, Schmid M. Facial emotion recognition in adolescents with nonsuicidal self-injury. Psychiatry Res. 2015;228(3):332–339.
11. Krompinger JW, Simons RF. Electrophysiological indicators of emotion processing biases in depressed undergraduates. Biol Psychol. 2009;81(3):153–163.
12. Andersson H, Aspeqvist E, Dahlstrom O, et al. Emotional dysregulation and trauma symptoms mediate the relationship between childhood abuse and nonsuicidal self-injury in adolescents. Front Psychiatry. 2022;13:897081.
13. B K. Five indices of emotion regulation in participants with a history of nonsuicidal self-injury: a daily diary study. Behav Ther. 2013;45(1):56–66.
14. Nyquist AC, Luebbe AM. An emotion recognition-awareness vulnerability hypothesis for depression in adolescence: a systematic review. Clin Child Fam Psychol Rev. 2020;23(1):27–53.
15. Andric Petrovic S, Jerotic S, Mihaljevic M, et al. Sex differences in facial emotion recognition in health and psychotic disorders. Cogn Neuropsychiatry. 2019;24(2):108–122.
16. Kapitanovic A, Tokic A, Simic N. Differences in the recognition of sadness, anger, and fear in facial expressions: the role of the observer and model gender. Arh Hig Rada Toksikol. 2022;73(4):308–313.
17. Campbell-Sills L, Barlow DH, Brown TA, Hofmann SG. Acceptability and suppression of negative emotion in anxiety and mood disorders. Emotion. 2006;6(4):587–595.
18. Winer ES, Jordan DG, Collins AC. Conceptualizing anhedonias and implications for depression treatments. Psychol Res Behav Manag. 2019;12:325–335.
19. Ahmed SP, Bittencourt-Hewitt A, Sebastian CL. Neurocognitive bases of emotion regulation development in adolescence. Dev Cogn Neurosci. 2015;15:11–25.
20. Muris P, Ollendick TH. Current challenges in the diagnosis and management of selective mutism in children. Psychol Res Behav Manag. 2021;14:159–167.
21. Jenness JL, Hankin BL, Young JF, Gibb BE. Misclassification and identification of emotional facial expressions in depressed youth: a preliminary study. J Clin Child Adolesc Psychol. 2015;44(4):559–565.
22. Lopez-Duran NL, Kuhlman KR, George C, Kovacs M. Facial emotion expression recognition by children at familial risk for depression: high-risk boys are oversensitive to sadness. J Child Psychol Psychiatry. 2013;54(5):565–574.
23. Giuliani C. The Flavonoid Quercetin Induces AP-1 Activation in FRTL-5 Thyroid Cells. Antioxidants. 2019;8(5):67.
24. Schepman K, Taylor E, Collishaw S, Fombonne E. Face emotion processing in depressed children and adolescents with and without comorbid conduct disorder. J Abnorm Child Psychol. 2012;40(4):583–593.
25. Sfarlea A, Greimel E, Platt B, Dieler AC, Schulte-Korne G. Recognition of emotional facial expressions in adolescents with anorexia nervosa and adolescents with major depression. Psychiatry Res. 2018;262:586–594.
26. McClure EB. A meta-analytic review of sex differences in facial expression processing and their development in infants, children, and adolescents. Psychol Bull. 2000;126(3):424–453.
27. Collignon O, Girard S, Gosselin F, Saint-Amour D, Lepore F, Lassonde M. Women process multisensory emotion expressions more efficiently than men. Neuropsychologia. 2010;48(1):220–225.
28. Codispoti M, Surcinelli P, Baldaro B. Watching emotional movies: affective reactions and gender differences. Int J Psychophysiol. 2008;69(2):90–95.
29. Wild B, Bartels M. Are emotions contagious? Evoked emotions while viewing emotionally expressive faces: quality, quantity, time course and gender differences. Psychiatry Res. 2001;102(2):109–124.
30. Nichols TR, Bryant K, Botvin GJ. Examining anger as a predictor of drug use among multiethnic middle school students. J Sch Health. 2008;78(9):480–486.
31. Bomfim AJL, Ribeiro R, Chagas MHN. Recognition of dynamic and static facial expressions of emotion among older adults with major depression. Trends Psychiatry Psychother. 2019;41(2):159–166.
32. Liedtke C, Kohl W, Kret ME, Koelkebeck K. Emotion recognition from faces with in- and out-group features in patients with depression. J Affect Disord. 2018;227:817–823.
33. McIvor L, Sui J, Malhotra T, Drury D, Kumar S. Self-referential processing and emotion context insensitivity in major depressive disorder. Eur J Neurosci. 2021;53(1):311–329.
34. Qu D, Wang Y, Zhang Z, et al. Psychometric Properties of the Chinese Version of the Functional Assessment of Self-Mutilation (FASM) in Chinese Clinical Adolescents. Front Psychiatry. 2022;12:755857.
35. Chagas MH, Tumas V, Rodrigues GR, et al. Validation and internal consistency of Patient Health Questionnaire-9 for major depression in Parkinson’s disease. Age Ageing. 2013;42(5):645–649.
36. Beard C, Hsu KJ, Rifkin LS, Busch AB, Bjorgvinsson T. Validation of the PHQ-9 in a psychiatric sample. J Affect Disord. 2016;193:267–273.
37. Ruihua M, Hua G, Meng Z, et al. The relationship between facial expression and cognitive function in patients with depression. Front Psychol. 2021;12:648346.
38. Liu Jing RY, Wei Q, Nan C, et al. The establishment of Graded image bank of Chinese facial expression intensity. Chine J Mental Health. 2019;02:120–125.
39. Du Xia FH, Yunhui W, Jie Z, Xiaolin Z, Yanli Z, Shuping T. Differences in facial emotion recognition between bipolar disorder and schizophrenia. Chine J Neuropsychiatric Disorders. 2021;404–408.
40. Kret ME, De Gelder B. A review on sex differences in processing emotional signals. Neuropsychologia. 2012;50(7):1211–1221.
41. Schoofs D, Pabst S, Brand M, Wolf OT. Working memory is differentially affected by stress in men and women. Behav Brain Res. 2013;241:144–153.
42. Somers JA, Borelli JL, Depressive Symptoms HLM. Rumination, and emotion reactivity among youth: moderation by gender. J Clin Child Adolesc Psychol. 2020;49(1):106–117.
43. Lee TM, Ng EH, Tang SW, Chan CC. Effects of sad mood on facial emotion recognition in Chinese people. Psychiatry Res. 2008;159(1–2):37–43.
44. Bouhuys AL, Groothuis TG. Induction of depressed and elated mood by music influences the perception of facial emotional expressions in healthy subjects. J Affect Disord. 1995;33(4):215–226.
45. Nowacki J, Wingenfeld K, Kaczmarczyk M, et al. Selective attention to emotional stimuli and emotion recognition in patients with major depression: the role of mineralocorticoid and glutamatergic NMDA receptors. J Psychopharmacol. 2021;35(8):1017–1023.
46. Gotlib IH, Krasnoperova E, Yue DN, Joormann J. Attentional biases for negative interpersonal stimuli in clinical depression. J Abnorm Psychol. 2004;113(1):121–135.
47. Fink G. Stress: concepts, cognition, emotion, and behavior. Handbook Stress. 2016;1:67.
48. Fernandez E, Johnson SL. Anger in psychological disorders: prevalence, presentation, etiology and prognostic implications. Clin Psychol Rev. 2016;46:124–135.
49. Mandal MK. Perceptual skill in decoding facial affect. Percept Mot Skills. 1985;60(1):96–98.
50. Fahlgren MK, Cheung JC, Ciesinski NK, McCloskey MS, Coccaro EF. Gender differences in the relationship between anger and aggressive behavior. J Interpers Violence. 2022;37(13–14):NP12661–NP12670.
51. Porter-Vignola E, Booij L, Bosse-Chartier G, Garel P, Herba CM. Emotional facial expression recognition and depression in adolescent girls: associations with clinical features. Psychiatry Res. 2021;298:113777.
52. Plener PL, Bubalo N, Fladung AK, Ludolph AG, Lule D. Prone to excitement: adolescent females with Non-suicidal self-injury (NSSI) show altered cortical pattern to emotional and NSS-related material. Psychiatry Res. 2012;203(2–3):146–152.
53. Csukly G, Czobor P, Szily E, Takacs B, Simon L. Facial expression recognition in depressed subjects: the impact of intensity level and arousal dimension. J Nerv Ment Dis. 2009;197(2):98–103.
54. Langenecker SA, Bieliauskas LA, Rapport LJ, Zubieta JK, Wilde EA, Berent S. Face emotion perception and executive functioning deficits in depression. J Clin Exp Neuropsychol. 2005;27(3):320–333.
55. Nock MK, Mendes WB. Physiological arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. J Consult Clin Psychol. 2008;76(1):28–38.
56. Nock MK. Actions speak louder than words: an elaborated theoretical model of the social functions of self-injury and other harmful behaviors. Appl Prev Psychol. 2008;12(4):159–168.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.