")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Gender as a Moderator of Spirituality and Spiritual Care in ICU Nurses During COVID-19 Pandemic
Authors Zeilani RS , Al-Qunneh AMR, Arabiat DH , Hamdan-Mansour A
Received 24 November 2022
Accepted for publication 27 March 2023
Published 5 May 2023 Volume 2023:16 Pages 1271—1281
DOI https://doi.org/10.2147/JMDH.S396858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ruqayya S Zeilani,1 Ahmad M R Al-Qunneh,2 Diana H Arabiat,1,3 Ayman Hamdan-Mansour1
1School of Nursing, The University of Jordan, Amman, Jordan; 2Critical Care Nursing, Prince Faisal Bin Al Hussein Hospital, Zarqa, Jordan; 3School of Nursing and Midwifery, Edith Cowan University, Perth, WA, Australia
Correspondence: Ruqayya S Zeilani, School of Nursing, The University of Jordan, Amman, Jordan, Email [email protected]
Background: Earlier research has found that female healthcare providers often report greater spirituality and spiritual care than males. This would evoke attention toward factors contributing to such differences, particularly gender.
Aim: To examine the moderating effects of gender on the relationships between demographic characteristics of ICU nurses and their perceived spirituality and spiritual care.
Methods: A cross-sectional correlational design was used to recruit a national sample of 865 nurses working in ICUs in Jordan and providing care to patients diagnosed with COVID-19. Data were collected using a self-report bilingual version of Spirituality and Spiritual Care Rating Scale (SSC) and analysed using the SPSS software package.
Results: Social status, monthly income, and receiving previous courses or lecture training on spirituality and spiritual care were predictors of higher SSCRS scores. Working with COVID-19 patients was a positive predictor (B = 0.074, p = 0.023), suggesting that working with COVID-19 patients is more likely to have a higher level of SSC. Gender was a negative predictor (B = − 0.066, p = 0.046), suggesting that female participants are likelier to have a lower SSC score.
Conclusion: Working with patients during the COVID-19 pandemic positively impacted nurses’ perception of SCC, but female nurses had lower score than male nurses indicating the need for more emphasis on training female nurses and exploring further the areas in which they need more training and to be able to provide an effective SSC. A sustainable up-to-date training and in-service education programs responding to nurses’ needs and emerged emergencies crisis need to be integrated into nursing quality of care policy development.
Keywords: spirituality, spiritual care, gender, nurses, COVID-19 pandemic, intensive care unit
Introduction and Background
Nursing philosophy is based on holistic care that includes physical, psychological, social, and spiritual dimensions.1 Following the challenges facing the healthcare system due to the COVID-19 pandemic, it is essential to understand how the quality of spiritual care should be provided and if nurses’ perceptions of spirituality interfere with their quality of care. Alsyouf et al2 suggested that the quality of nursing care is influenced by healthcare providers’ socio-demographic characteristics, including gender. This infers that male and female nurses might have different perceptions of certain significant care concepts, such as spirituality and spiritual care. However, such perception might be affected by their psychological and social well-being. It has been reported that female nurses experience higher levels of anxiety, stress, and depression while providing care to patients during the COVID-19 pandemic than their male counterparts.3,4
The literature asserts that nurses’ high workload during the pandemic brought new challenges to nurses, in particular, those working in intensive care units (ICU), where a lack of awareness of the spiritual needs of COVID-19 patients has been identified as one of those main challenges.5 Spirituality is defined as the general human need to develop a sense of meaning, purpose, and morality and this is not necessarily related to faith and religion.6 Such definition would assume that nurses should consider patients’ sense of the meaning of their sickness and their experiences with their illness journey. Therefore, it is assumed that female nurses in ICUs who suffer higher levels of psychological disturbances, and their personal and socio-demographic characteristics and experiences are not positively enabling them to function well and not be able to integrate spirituality and spiritual care into their daily practice. The results will be the inability to adhere to a holistic care approach.
Spiritual care is one of the most important dimension to attending the spiritual needs of ICU patients. Spiritual care is defined as “a non-discipline-specific healthcare function analogous to emotional or physical care”.7 This concept is fundamental in providing quality care for patients with the aim of promoting patients’ spiritual wellbeing, enhancing comfort, decreasing stress, and helping patients to cope with their illness.8 Studies suggested that providing spiritual care can be achieved through attending patients’ wishes, accepting and respecting their feelings, values, religious and cultural beliefs, in addition to helping the patients to perform religious rituals and referring them to spiritual advisor when experiencing distress.8–10 During COVID-19 pandemic, infected patients died in the ICU were suffering not only from unexpected serious signs and symptoms of the disease but also were feelings isolated and lonely. Consequently, patients’ values and beliefs were challenged due to the conditions of the pandemic crisis. This may result in experiencing existential crises and the loss of meaning of life and hope that is worsen by the lack of family support.10–12 A recent review of literature emphasised that there is an advantage in implementing intervention programs of spiritual care to increase patients’ awareness and managing spiritual distress; the studies stress the importance of conducting training and education programs for nurses to increase their knowledge, attitudes, and practices in providing spiritual care.13
Care of patients during crises such as the COVID-19 pandemic is perceived as a challenging experience for nurses, healthcare decision-makers, and public health policymakers.
During the COVID-19 pandemic, several studies reported that hospitals were lagging in training and lacked sufficient training to provide spiritual care to their staff.14–16 This was intensified by the dramatic increase in death reports due to the COVID infection among different countries. In addition, nurses needed clarification about how to incorporate spiritual care into their patients’ care during the pandemic, crises, and emergencies.14 Lessons learned from the COVID-19 pandemic enlightened nurses and healthcare decision-makers about the significant need for nurses to incorporate spirituality and spiritual care in emergencies and crises comparable to COVID-19. Furthermore, earlier studies reported that nurses’ demographical characteristics tend to impact nurses’ provision of spiritual care and their perception of spirituality.16 Overall, studies on gender differences in spirituality have found that female nurses reported a higher level of spirituality than male nurses.13 Factors associated with a higher level of spirituality and spiritual care included attending education courses in spiritual care,17–21 providing care for a terminally ill patient, and being married.18
It is important to point out that, since 1996, the Jordanian government has initiated policies that focus on gender equity and empowerment of women to have equal chances in labour force as men.22 Along the same line, the government posed many policies to enhance safety and ensure high quality of patients’ care.23 However, all these decisions and procedures mainly focused on the physical dimension of care rather than the psychological and the spiritual aspects. This led to assume that spirituality and spiritual care may not be associated with quality care outcomes and supported the notion that nurses, and other healthcare providers may tend to underestimate the impact of spiritual care as a major core component of healthcare services. This study attempted to assess nurses’ perceptions of their spirituality and spiritual care provided for their patients at critical care units during COIVID-19 pandemic. This study aimed to examine the potential moderating effects of gender on the relationships between demographic characteristics of ICU nurses and their perceived spirituality and spiritual care. The specific aims were:
- To assess nurses’ perception of their spirituality and spiritual care at critical care units and caring for patients diagnosed with COVID-19.
- To examine the moderating effect of gender on the relationships between demographic characteristics of ICU nurses and their perceived spirituality and spiritual care.
Methods
Study Design and Settings
This study utilized a correlational, cross-sectional study design. The study was conducted in eight randomly selected hospitals in Jordan. There are four healthcare sectors in Jordan: (a) The governmental sector (mainly affiliated with the Ministry of Health), (b) the university educational sector, (c) the private sector, and (d) the military sector (hospitals affiliated to Royal Medical Services). The researchers randomly selected two hospitals from each of the four health sectors providing intensive care for patients with COVID-19 in Jordan. During COVID-19 pandemic, the decision was made by the government that all the admitted patients had PCR test positive and were diagnosed with COVID-19 delta infection are to receive care in the selected hospitals which included eight ICUs.
Participants
Nurses who matched the inclusion criteria were recruited as participants in this study. This was when COVID-19 in Jordan reached its peak with the highest death reports, and the cases of active COVID-19 escalated from some hundred to numerous thousand cases a day. During this time, the number of admitted cases to the ICU increased dramatically, and all ICUs had a full capacity of all beds. In addition, the sample size was calculated using a medium effect size of 0.25 as used in previous similar literature, using G*Power 3.1.9.4 software program.18 A significance level of a=0.05 is set to control the risk for type I error, and a power of 95% is selected to reduce the risk of a type II error using one-way analysis of variance (ANOVA). Accordingly, the estimated sample size was calculated to be 305 and more. However, during the data collection period, the number of nurses involved in COVID-19 pandemics were increased as the number of patients dramatically increased. Therefore, the researcher decided to invite all nurses who met the inclusion criteria and agreed to participate in this study. The inclusion criteria were to be a registered nurse, working in the ICU in the selected hospitals, have a minimum experience of 1 year, and worked as full-time nurse at the time of COVID-19 pandemic. Thus, the total number of nurses who agreed to participate and met the inclusion criteria was 896.
Recruitment and Data Collection
The recruitment process started immediately after gaining access permission to the hospitals. First, the principal investigator (PI) and second researcher (KH) took a list of all eligible nurses who worked in the ICU from the nursing office. Next, an invitation letter was handed to the nurses in the ICU in the selected hospitals. Those who agreed to participate called the researcher back via telephone, the researcher had further contact to discuss the information sheet, and the nurse signed the consent form.
The SSCRS was translated into the Arabic language (the formal language in Jordan) following the WHO format of translation24 to overcome any language barrier with the study participants. The process of translation started by forward translation of the tool by a translator who was professional translator in medical terminology. Then a panel of three experts who were familiar with health-related terminology had bilingual English and Arabic languages checked the translated tool for face validity and to identify and resolve the poor terminologies of the translation, as well as any incongruities between the English and Arabic translation. Then, back translation was performed by a health professional (a clinical nurse specialist), familiar with health-related terminology. The panel decided that there are no changes in translation, except for one word “the Chaplin” that was replaced by the word “spiritual advisor”. A pilot study was conducted on a group of 40 nurses working in the ICUs; these nurses were excluded from the main study. Because of some items were unclear to the nurses, it was decided to use a tool bilingually (Arabic and English). The Cronbach’s alpha reliability coefficient was calculated and showed 0.849 which providing evidence of reliability of the translated tool.
The Instruments
The spirituality and spiritual care rating scale (SSC) is a commonly used measure to assess spirituality and spiritual care that was developed by McSherry et al25 and widely used by many researchers around the world.18,19,26–29 The SSC consists of 17 statements categorized under two parts: spirituality (11 items) and spiritual care (6 items).25 In order to prevent response bias, the original authors organized the questions in the scale randomly. Five-point Likert type scale was used for rating each statement with scores of 1 (strongly disagree), 2 (disagree), 3 (uncertain), 4 (agree) and 5 (strongly agree). The researchers used bilingual versions of the SSC. which was originally formed by McSherry et al.25 The acceptable values of alpha for the internal consistency reliability of the items range from of 0.64 to 0.95.25,29, The tools were applied in many settings for nurses and revealed good validity and reliability; Cronbach’s alpha values for SSCRS were 0.86, 0.90, and 0.87, respectively.18,30,31 For this study, Cronbach’s alpha value was 0.849.
The second researcher-adapted measure included participants’ sociodemographic characteristics, including age, gender, marital status, religion, educational level, monthly income, years of clinical experience in ICU, ICU type, health sector type of the hospital, and whether receiving previous training in spiritual care. The sociodemographic characteristics of the sample were chosen based on previous study conducted in Jordan.18 The researchers added more variables from other studies used the same tool.19,22,28,30
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was obtained from the Institutional Review Board (IRB) committee at the School of Nursing at The University of Jordan (IRB# 2020/50-20). In addition, the IRB committee’s ethical approval in all hospitals was obtained before the data collection. Participation in the study was voluntary and based on signing a consent form. The anonymity and confidentiality of participants were assured. Before data collection, researchers explained that participants had the right to withdraw from the study without any negative impact or consequences. All soft copy of entered questionnaires and demographics was kept secret in the PI’s personal and password-protected computer. The hardcopy materials were stored in a locked cabinet.
Statistical Analyses
Statistical Package for Social Science (IBM, SPSS Statistics, Version 25) was used to enter and analyze the data. All data were checked for missing outliers, and assumptions of normality were applied. We found less than 1% missing data, mainly related to demographic characteristics. There were no outliers. Preliminary analyses were carried out to assure no violations of the assumptions of normality, linearity, multicollinearity, and homoscedasticity. A p-value less than 0.05 was considered statistically significant. We used descriptive statistics, including frequencies (n), percentages (%), means, and standard deviations (SDs), to present our findings. A series of analyses of variance (ANOVAs) was performed to examine the differences of SCC and demographic variables (age, marital status, income level, level of education, length of clinical experience, type of ICU, and type of sector). An independent sample two-tailed t-test has been used for the dichotomous variables (gender, religion, receiving previous courses or lecture training in spiritual care).
The researchers performed three-step multiple hierarchical regression analysis. In model 1, a selected sociodemographic (age, social status, monthly income, level of education, experience, and receiving previous courses or lecture training in spiritual care) were entered, in model 2 adding working with COVID-19 patients, and in model 3 adding gender as moderating factor in order to test the moderation effect of gender on the perceived level of spirituality and spiritual care and nurses socio demographic characteristics.
Results
Participants’ Demographic Characteristics
The response rate of distribution was 96%; most of the non-responding nurses were busy and felt no mood for filling out any questionnaire. The participants’ sociodemographic characteristics are presented in (Table 1). Approximately 50.2% of the participants were women; most participants were aged below 29 years (56.9%) and married (56.9%). Almost all participants were Muslims (98.9%), held a baccalaureate degree (89.2%), and provided direct care to patients. Over 42.1% of the participants had over 7 years of clinical experience. Questions regarding the COVID-19 Pandemic revealed that all participants provided direct care for patients who had tested positive for COVID-19. However, only 34.6% of the participants worked in a specialized ICU unit for advanced COVID-19 cases.
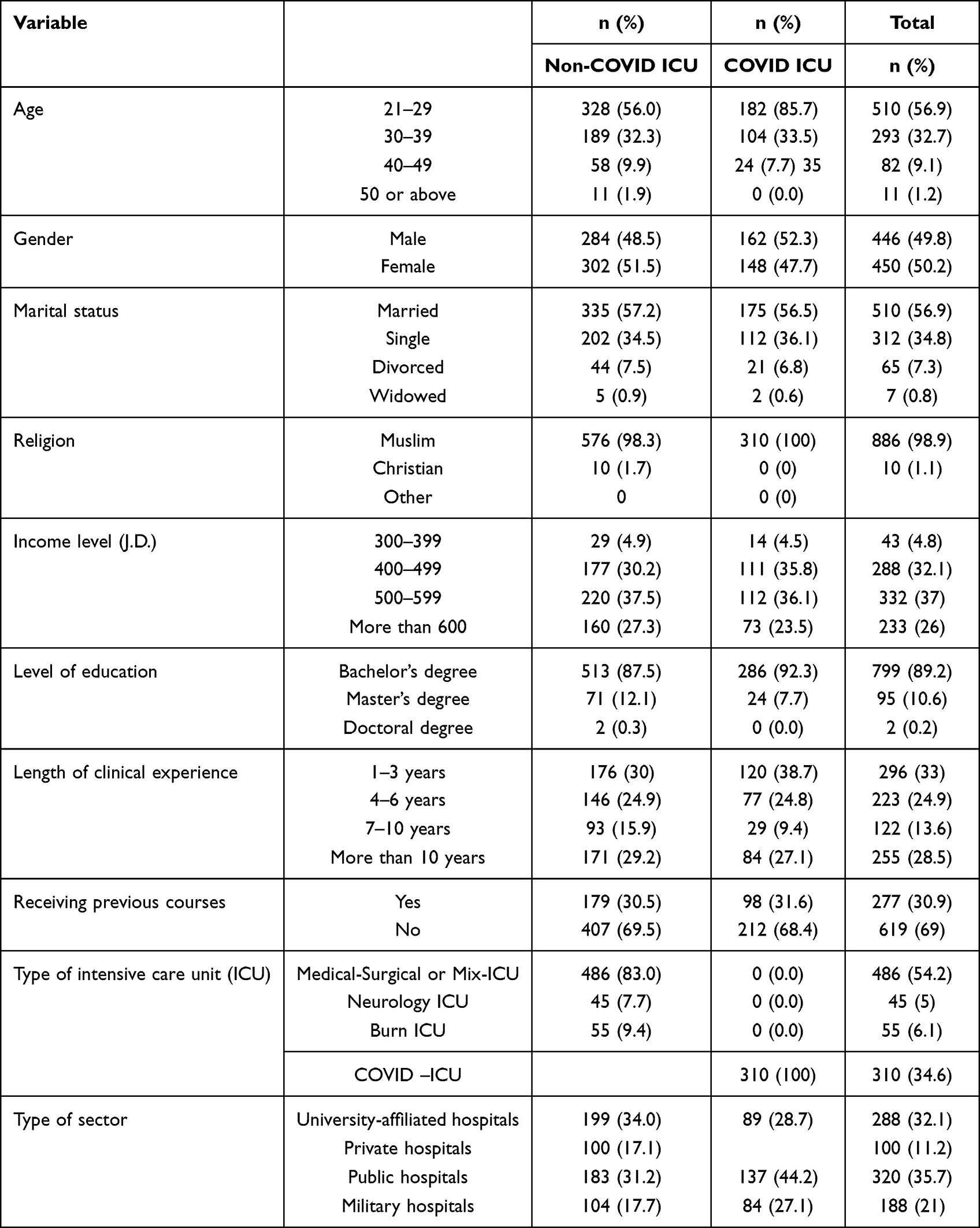 |
Table 1 Participants’ Sociodemographic Characteristics |
Nurses’ Perception of Their Spirituality and Spiritual Care and Caring of Patients Diagnosed with COVID-19 in the ICU
All nurses who worked with patients diagnosed with COVID-19 and admitted to the ICU were included in the analyses. A series of an independent sample two-tailed t-test has been used for the dichotomous variables (gender, religion, receiving previous courses or lecture training in spiritual care). In addition, one-way analysis of variance (ANOVA) has been used to compare means of SSCRS of independent variables (age, marital status, income level, level of education, length of clinical experience, type of ICU, and type of sector). No significant differences between males and females were found. Then, the Pearson correlation coefficient was conducted and showed that social status, monthly income, and receiving previous courses or lecture training in spiritual care and working with COVID-19 patients have a significant positive correlation with SSC (r = 0.104, p = 0.001; r = 0.056, p = 0.047; r = 0.207, p < 0.001; r = 0.096, p = 0.020; respectively). This is followed by applying the Pearson correlation coefficient on the relationship between gender and SSC; this showed a significant negative correlation with SSC (r = 0.058, p = 0.043). On the other hand, age, level of education, and experience were not significantly correlated (p > 0.05). In Table 2, the researchers described the differences in spirituality and spiritual care by general characteristics.
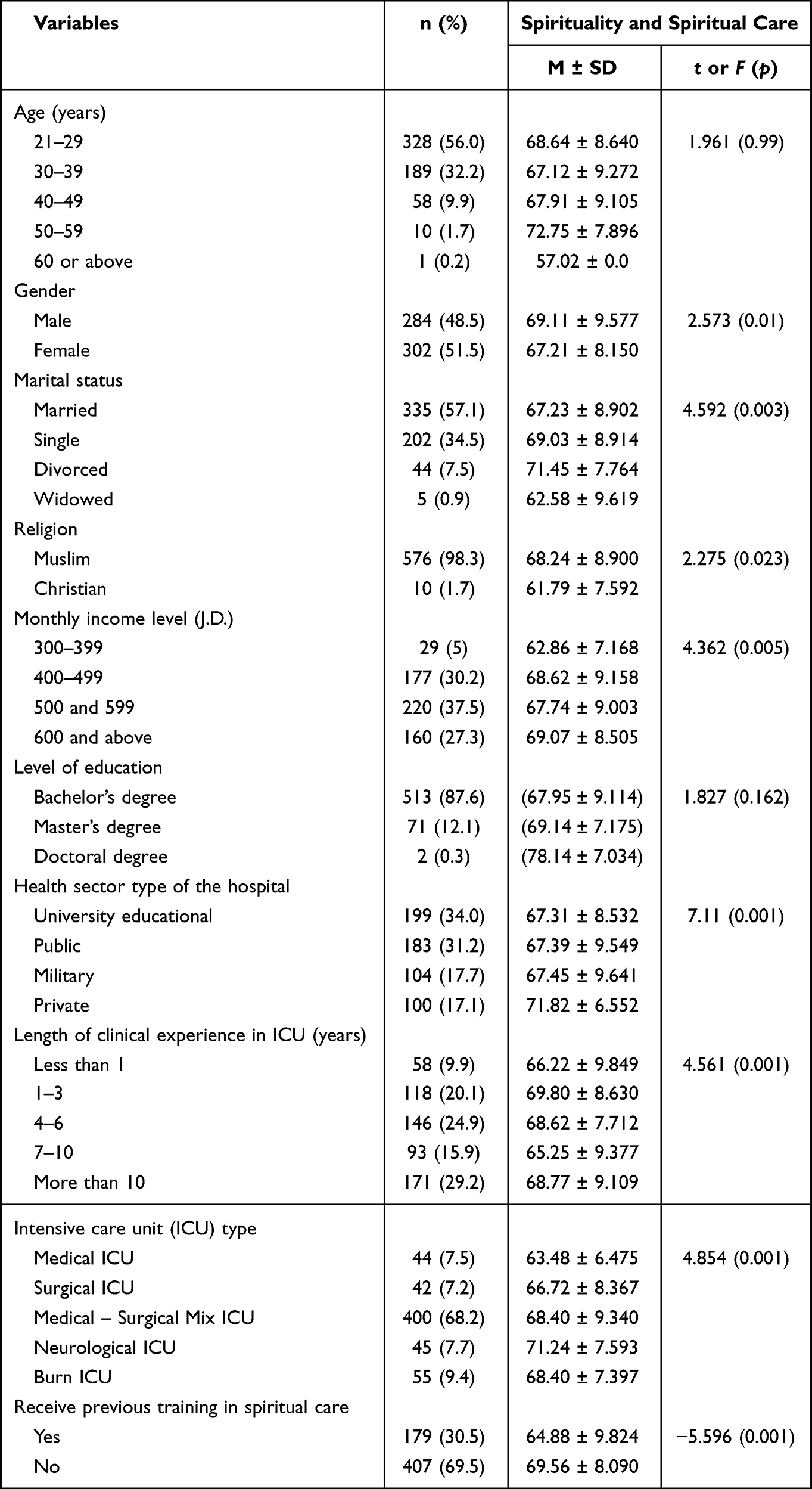 |
Table 2 Differences in Spirituality and Spiritual Care by General Characteristics (N = 865) |
The Moderating Effect of Gender on the Relationships Between Demographic Characteristics of ICU Nurses and SSC
The researchers examined the moderating effect of gender on the relationships between demographic characteristics of ICU nurses and SSC and used a three-step multiple hierarchical linear regression analysis conducted to assess the prediction power of whether working with COVID-19 patients and selected sociodemographic (age, social status, monthly income, level of education, experience, and receiving previous courses or lecture training in spiritual care) and consider gender as moderating factor. In model 1, a selected sociodemographic (age, social status, monthly income, level of education, experience, and receiving previous courses or lecture training in spiritual care) was significant (F6, 895 = 9.645, p < 0.001) with R2 = 0.061 (6.1%). Each expectancy score was standardized when interaction terms were computed to eliminate nonessential multicollinearity.32
Then in model 2, adding working with COVID-19 patients, the model retrieved to be significant (F7, 895 = 9.103, p < 0.001) with R2 = 0.067 (6.7%). The R2 change from model 1 to 2 was 0.006 (0.06%). Then in model 3, adding gender as the moderating factor, the model retrieved to be significant (F8, 895 = 8.489, p < 0.001) with R2 = 0.071 (7.1%). The R2 change from model 1 to 3 was 0.010 (1%) and from model 2 to 3 was 0.004 (0.04%). The results indicate that 7.1% of the variation in spirituality and spiritual care is explained by model 3, which contains working with COVID-19 controlling for selected demographic characteristics and moderated by gender. Also, 6.7% of the variation in spirituality and spiritual care is explained by model 2, which contains selected demographic characteristics. Also, 6.1% of the variance in spirituality and spiritual care is explained by model 2, which contains working with COVID-19.
In model 3, social status was a positive predictor (B = 0.115, p = 0.001). The result suggests that widowed participants are more likely to have higher SSC scores, then divorced participants, then single participants, and finally, married participants. Additionally, monthly income was a positive predictor (B = 0.116, p = 0.007). The results indicate that participants with higher monthly incomes are likelier to have a higher SSC score. In addition, receiving previous courses or lecture training in SSC was a positive predictor (B = 0.203, p < 0.001). This indicates that the participants who did not receive any training in SSC are more likely to have a higher level of SSC. Also, working with COVID-19 patients was a positive predictor (B = 0.074, p = 0.023), which implies that the participants working with COVID-19 patients are more likely to have a higher level of SSC. Gender was a negative predictor (B = −0.066, p = 0.046), suggesting that female participants are likelier to have a lower SSC score. Please see details description predictors of spirituality and spiritual care the regression models in Table 3.
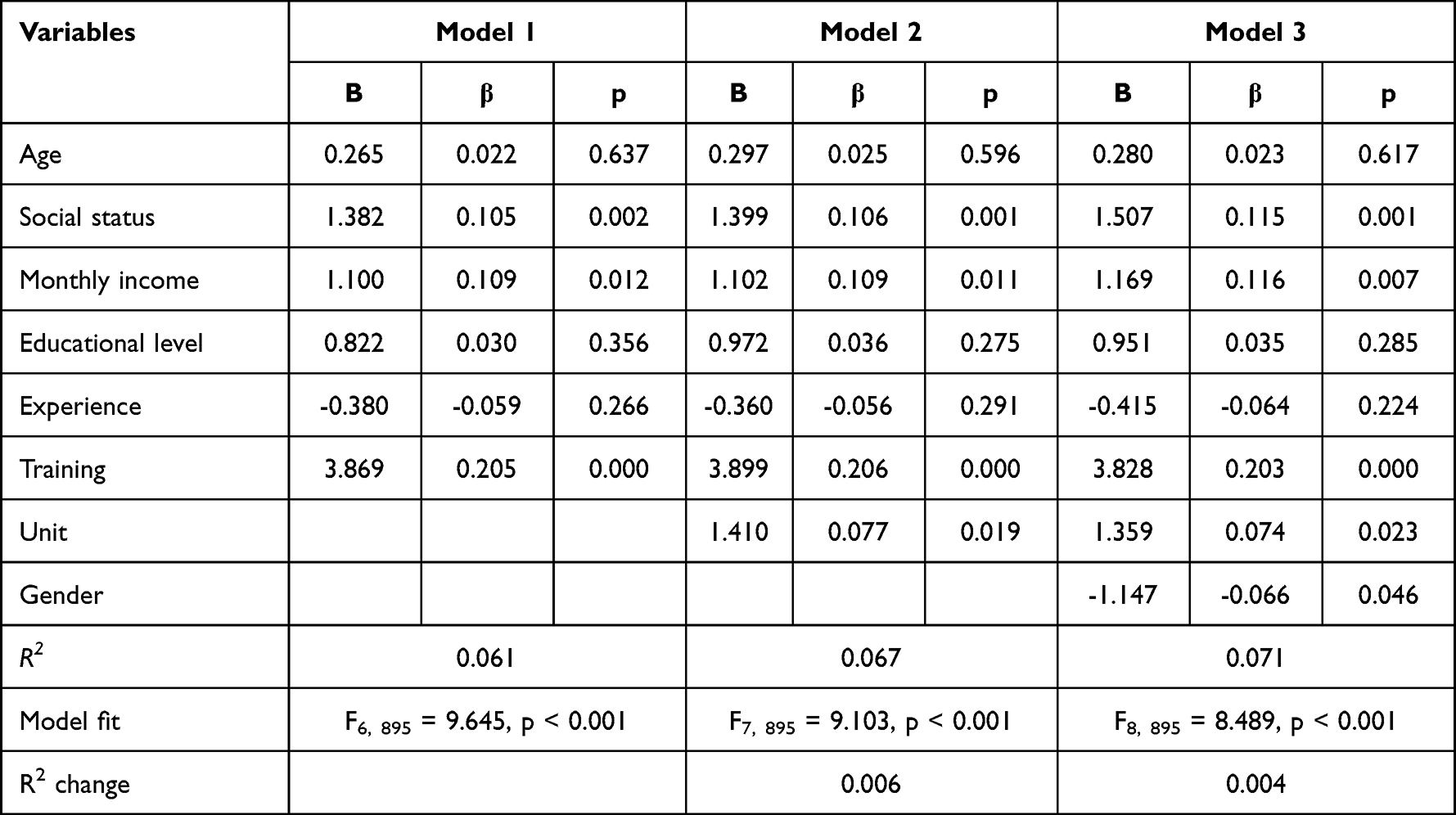 |
Table 3 Predictors of Spirituality and Spiritual Care |
Discussion
Spirituality and spiritual care are essential components of holistic nursing care; more important in critical care units. Although ICU nurses recognized that SSC are essential for their quality care outcomes, they seem in need for training and enhancement for their knowledge and skills to effectively provide SSC.21 This study found that gender has a significant moderation effect on the relationship between sociodemographic and personal factors and SSC. Such an effect found to be positive. The results indicate that female and male nurse do differ in terms of their perception of SSC and such perception in influenced by their other sociodemographic and personal factors. The findings of the present study are consistent with previous studies included nurses assuming different spiritual beliefs and religions where male and female nurses found to be different in their SSC perception13–15,28,33 This indicates that nurses whether Muslims, as in this study, or not are sharing perceptions that SSC is a significant component of their work as nurses and their perception is mainly influenced by their gender rather than their spiritual beliefs or religious background. The results of this study add the body of knowledge that SSC although attributed to religiosity, the variations in religiosity have not contributed to SSC as much as the gender of the nurse. Female nurses seem to be influence largely by their attributes as females enhancing the principle of feminist approach of thinking that is integrated with professional knowledge and skills. Such an explanation is supported by studies conducted across cultures that perception of spirituality and spiritual care among female nurses is much apparent and significant than male nurses regardless of their religious background.12,28–31
Given that female nurses had lower scores of SSC, working with patients with COVID-19 could be more stressful for female nurses than for male nurses. This can be due to several reasons. For example, Rachel et al21 identified that SSC among nurses is affected by nurses’ preparation, training experiences, actual practices of spiritual care, and the environment where nurses practice and provide care. Such factors could explain the lower score for female nurses working at Jordanian healthcare settings where SSC is a neglected topic in education, training g and in nursing practices.18,34 Therefore, nurses rely primarily on their personal accumulated knowledge and experience to provide spiritual care for their patient rather than formal education or training. Moreover, female nurses are more fragile practitioners in crisis management where they were found to have higher levels of anxiety, stress, and depression during and due to the care of patients with COVID-19.3,4 This infers that female nurses although believe in SSC, their willingness to provide spiritual care for their patients is much more compromised by their psychological and wellbeing during crisis such as COVID-19 pandemic than male nurses.
The literature emphasized several components that interfere with the quality of nursing care in general, including the influence of sociodemographic characteristics.2 However, spiritual care is assumed to be more affected by nurses’ personal and sociodemographic characteristics. In a very recent study, moral distress was found to be high among nurses due to the effect of religiosity and the personal belief system of nurses.35 In this study, widowed and divorced nurses and those with higher incomes were found to have a higher level of spirituality and spiritual care. Initially, this might confuse readers as it is assumed that being a divorced or widowed female nurse is associated with stress and anxiety that might negatively affect their SSC. Nevertheless, widow and divorced female nurses had higher SSC levels, indicating that nurses might have used their negative life experiences to energize and positively use their learned experiences to provide SSC. The results are not inconsistent with previous international studies that did not find significant differences in SSC concerning sociodemographic factors of nurses.13 It is worth mentioning that there is an inconsistent report related to the role of sociodemographic characteristics on spirituality and spiritual care among nurses due to several factors, including the method of measurement used (qualitative versus quantitative), working areas (special care unit versus general), and role of and effect of religiosity on the spirituality of nurses themselves.35
One interesting findings in this study was related to the number of nurse’s response; male nurses in ICU were almost equal to female nurses in this study. This might be related to the high number of male nurse graduates in Jordan comparing to other countries globally, in which male nurses represent approximately half percentage of the total Jordanian nurses.36 However, the number of male nurses had no influence on the nurses’ perception of SSC.
Training and education in SSC have also been tested and found to be significant. This is consistent and supports previous reports that nurses exposed to educational packages to improve their attitudes, knowledge, and skills to provide spiritual care have been significant and positive1,5,14 Unfortunately, spirituality and spiritual care are not integrated into nursing curricula where nurses acquire knowledge and skills at their clinical site and await employment agencies and staff development programs to improve their knowledge and skills. This has been noted with higher scores of those who have received training and those who have not.
Limitations of the Study
One limitation of this study is related to the prediction power of the variables included in this study that was low which might require a cautious interpretation of the clinical implication of the results. Therefore, the study recommends conducting a qualitative research approach to elucidate the nurses’ perception of spirituality and their experiences in delivering spiritual care to Muslim patients.
Implementation and Recommendations
This study recommends further research, especially in middle-income countries, to understand nurses’ experiences and recognize the main needs that can be incorporated into interventions designed to improve the services provided to ICU nurses in the ICU during crises or disasters and recognize the main needs that can be incorporated into interventions designed to improve the services provided to ICU nurses in the ICU. The study recommends to conduct further research on female nurses’ experiences during COVID-19 pandemic.
Moreover, the study highlighted the importance of organizational support by providing counseling sessions, stress management courses, and group therapy for female nurses working in the ICU mainly during pandemics and disasters. Further research related to the experiences of female nurses during COVID-19 pandemic is recommended.
Conclusion
This study reported that demographic characteristics including gender, social status, income, and being trained in spiritual care are significant predictors of SSC among nurses working with COVID-19 patients. Female nurses had lower score than male nurses indicating the need for more emphasis on training female nurses and exploring further the areas in which they need more training and to be able to provide an effective SSC. Similarly, in spite of scoring higher, male nurses need to have their SSC emphasized and enhanced further to improve the quality of care in general and promote holistic approach as an effective model of care. A sustainable up-to-date training and in-service education programs responding to nurses’ needs and emerged emergencies crisis need to be integrated into nursing quality of care policy development.
Consent
Informed consent was obtained from all nurses who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by the Deanship of Scientific Research at The University of Jordan.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors have no relevant financial or non-financial interests to disclose.
References
1. Booth L, Kaylor S. Teaching spiritual care within nursing education: a holistic approach. Holist Nurs Pract. 2018;32(4):177–181. doi:10.1097/HNP.0000000000000271
2. Alsyouf WS, Hamdan-Mansour AM, Hamaideh SH, Alnadi KM. Nurses’ and patients’ perceptions of the quality of psychiatric nursing care in Jordan. Res Theory Nurs Pract. 2018;32(2):226–238. doi:10.1891/1541-6577.32.2.226
3. Hamaideh SH, Al‐Modallal H, Tanash MA, Hamdan‐Mansour A. Depression, anxiety and stress among undergraduate students during COVID‐19 outbreak and” home‐quarantine”. Nurs Open. 2022;9(2):1423–1431. doi:10.1002/nop2.918
4. Li R, Chen Y, Lv J, et al. Anxiety and related factors in frontline clinical nurses fighting COVID-19 in Wuhan. Medicine. 2020;99:30.
5. Bahramnezhad F, Asgari P. Spiritual care for COVID-19 patients: a neglected necessity. Infect Dis Clin Pract. 2021;29(1):e63. doi:10.1097/IPC.0000000000000955
6. Al‐Fayyadh S, Diener E, Wright V. Spirituality as a core concept in the theoretical literature of nursing: a comparative overview between Watson & Lovering’s perspectives. Nurs Forum. 2022;57(4):717–723. doi:10.1111/nuf.12722
7. Gao J, Wang Q, Wu Q, Weng Y, Lu H, Xu J. Spiritual care for the management of Parkinson’s disease: where we are and how far can we go. Psychogeriatrics. 2022;22(4):521–529. doi:10.1111/psyg.12834
8. Zakaria Kiaei M, Salehi A, Moosazadeh Nasrabadi A, et al. Spirituality and spiritual care in Iran: nurses’ perceptions and barriers. Int Nurs Rev. 2015;62(4):584–592. doi:10.1111/inr.12222
9. Ramezani M, Ahmadi F, Mohammadi E, Kazemnejad A. Spiritual care in nursing: a concept analysis. Int Nurs Rev. 2014;61(2):211–219. doi:10.1111/inr.12099
10. Seid K, Eneyew M. Nurse’s spiritual care perception in Ethiopia: a multicenter cross-sectional study. SAGE Open Med. 2022;10:20503121221104436. doi:10.1177/20503121221104436
11. O’Brien MR, Kinloch K, Groves KE, Jack BA. Meeting patients’ spiritual needs during end-of-life care: a qualitative study of nurses’ and healthcare professionals’ perceptions of spiritual care training. J Clin Nurs. 2019;28:182–189. doi:10.1111/jocn.14648
12. Gurdogan E, Kurt D, Aksoy B, Kınıcı E, Şen A. Nurses’ perceptions of spiritual care and attitudes toward the principles of dying with dignity: a sample from Turkey. Death Stud. 2017;41(3):180–187. doi:10.1080/07481187.2016.1231242
13. Abusafia A, Mamat Z, Rasudin NS, Bakar M, Ismail R. Spiritual care competence among Malaysian staff nurses. Nurse Media J Nurs. 2021;11(1):1–9. doi:10.14710/nmjn.v11i1.34757
14. de Diego-Cordero R, López-Gómez L, Lucchetti G, Badanta B. Spiritual care in critically ill patients during COVID-19 pandemic. Nurs Outlook. 2022;70(1):64–77. doi:10.1016/j.outlook.2021.06.017
15. Timmins F, Connolly M, Palmisano S, et al. Providing spiritual care to in-hospital patients during COVID-19: a preliminary European fact-finding study. J Relig Health. 2022;61(3):2212–2232. doi:10.1007/s10943-022-01553-1
16. Tan M, Ozdelıkara A, Polat H. An exploratory study of spirituality and spiritual care among Turkey nurses. Int J Caring Sci. 2018;11(2):1311–1318.
17. Galek K, Flannelly KJ, Jacobs MR, Barone JD. Spiritual needs: gender differences among professional spiritual care providers. J Pastoral Care Counsel. 2008;62(1–2):29–35. doi:10.1177/154230500806200104
18. Melhem GAB, Zeilani RS, Zaqqout OA, Aljwad AI, Shawagfeh MQ, Abd Al-Rahim M. Nurses’ perceptions of spirituality and spiritual care giving: a comparison study among all health care sectors in Jordan. Indian J Palliat Care. 2016;22(1):42. doi:10.4103/0973-1075.173949
19. Akgün Şahin Z, Kardaş Özdemir F. Spirituality and spiritual care: a descriptive survey of nursing practices in Turkey. Contemp Nurse. 2016;52(4):454–461. doi:10.1080/10376178.2016.1221324
20. Gonçalves A, Santos M, Volpato R, Furtado EF, Barroso T, Pillon S. Attitudes of nursing students towards substance users and perceptions about religious/spiritual care. Revista da Escola de Enfermagem da USP. 2018;52(20). doi:10.1590/s1980-220x2017027903425
21. Rachel H, Chiara C, Robert K, Francesco S. Spiritual care in nursing: an overview of the measures used to assess spiritual care provision and related factors amongst nurses. Acta Bio Med. 2019;90(Suppl 4):44.
22. Edres N. Gendered representations in Jordanian textbooks: a combined quantitative and qualitative analysis based on UNESCO guidelines for the promotion of gender equality. Cogent Educ. 2022;9(1). doi:10.1080/2331186X.2022.2059826
23. Diab SM. The effect of primary health accreditation standards on the primary health care quality and employees satisfaction in the Jordanian Health Care Centers. Int J Acad Res Bus Soc Sci. 2015;5(4):204–220. doi:10.6007/IJARBSS/v5-i4/1568
24. World Health Organization (WHO). Process of translation and adaptation of instruments; 2010. Available from: http://www.who.int/substance_abuse/research_tools/translation/en.
25. McSherry W, Gretton M, Draper P, Watson R. The ethical basis of teaching spirituality and spiritual care: a survey of student nurses’ perceptions. Nurse Educ Today. 2008;28(8):1002–1008. doi:10.1016/j.nedt.2008.05.013
26. Babamohamadi H, Ahmadpanah MS, Ghorbani R. Attitudes toward spirituality and spiritual care among Iranian nurses and nursing students: a cross-sectional study. J Relig Health. 2018;57(4):1304–1314. doi:10.1007/s10943-017-0485-y
27. Yildirim JG, Ertem M. Professional quality of life and perceptions of spirituality and spiritual care among nurses: relationship and affecting factors. Perspect Psychiatr Care. 2022;58(2):438–447. doi:10.1111/ppc.12794
28. Herlianita R, Yen M, Chen CH, Fetzer SJ, Lin EC. Perception of spirituality and spiritual care among Muslim nurses in Indonesia. J Relig Health. 2018;57(2):762–773. doi:10.1007/s109436-0437-017
29. Ozbasaran F, Ergul S, Temel AB, Aslan GG, Coban A. Turkish nurses’ perceptions of spirituality and spiritual care. J Clin Nurs. 2011;20(21–22):3102–3110. doi:10.1111/j.1365-2702.2011.03778.x
30. Atarhim MA, Lee S, Copnell B. An exploratory study of spirituality and spiritual care among Malaysian nurses. J Relig Health. 2019;58(1):180–194. doi:10.1007/s10943-018-0624-0
31. Kaddourah B, Abu-Shaheen A, Al-Tannir M. Nurses’ perceptions of spirituality and spiritual care at five tertiary care hospitals in Riyadh, Saudi Arabia: a crosssectional study. Oman Med J. 2018;33(2):154–158. doi:10.5001/omj.2018.28
32. Aiken LS, West SG, Reno RR. Multiple Regression: Testing and Interpreting Interactions. Sage; 1991.
33. Bakir E, Samancioglu S, Kilic SP. Spiritual experiences of Muslim critical care nurses. J Relig Health. 2017;56(6):2118–2128. doi:10.1007/s10943-017-0382-4
34. Musa AS, Al Qadire MI, Aljezawi M, Tawalbeh LI, Aloush S, Albanian FZ. Barriers to the provision of spiritual care by nurses for hospitalized patients in Jordan. Res Theory Nurs Pract. 2019;33(4):392–409. doi:10.1891/1541-6577.33.4.392
35. Shehadeh J, Almaraira O, Hamdan-Mansour A. Determinants of moral distress among mental health professionals. Open Nurs J. 2022;16(1). doi:10.2174/18744346-v16-e2203030
36. Rababa M, Hayajneh AA, Bani-Iss W. Association of death anxiety with spiritual well-being and religious coping in older adults during the COVID-19 pandemic. J Relig Health. 2021;60(1):50–63. doi:10.1007/s10943-020-01129-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.