Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Gamification Strategies in Digital Health Interventions for Attention Rehabilitation in Stroke Survivors: A Systematic Review
Authors Nugraha A ![]() , Kosasih CE
, Kosasih CE ![]() , Pramukti I
, Pramukti I ![]() , Biben V
, Biben V ![]()
Received 14 September 2025
Accepted for publication 8 December 2025
Published 22 December 2025 Volume 2025:18 Pages 8169—8184
DOI https://doi.org/10.2147/JMDH.S566115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Andri Nugraha,1,2 Cecep Eli Kosasih,3 Iqbal Pramukti,4 Vitriana Biben5
1Doctoral Program in Medical Sciences, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Nursing, STIKes Karsa Husada Garut, Garut, West Java, Indonesia; 3Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 5Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Cecep Eli Kosasih, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Fax +62 02287793411, Email [email protected]
Background: Stroke is a leading cause of long-term disability, with attentional deficits affecting most survivors and limiting independence, activities of daily living (ADL), and quality of life. Conventional rehabilitation often lacks engagement and accessibility, which underscores the need for innovative strategies. Digital health interventions incorporating gamification may enhance attentional rehabilitation. However, the evidence remains limited.
Objective: This review systematically evaluated the effectiveness, safety, and gamification strategies of digital health interventions for attentional rehabilitation after stroke, including their impact on ADL.
Methods: A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. The Scopus, PubMed, and EBSCO-host databases were searched for randomized controlled trials (RCTs) published from January 2015 to February 2025. Eligible studies included adult patients with stroke undergoing gamified digital interventions. Methodological quality was assessed using the Joanna Briggs Institute (JBI) checklist, and risk of bias was evaluated using the Cochrane RoB-2 tool.
Results: Twelve RCTs with 544 participants were included. The interventions employed computer-based programs, virtual reality systems, and mobile applications. The most common gamification elements were progression, feedback, levels, challenges, and points. Seven trials reported significant improvements in attentional performance, whereas five showed no measurable benefits. Only two studies demonstrated significant improvements in ADL. Safety outcomes were favorable, with mild adverse events (transient dizziness and ocular fatigue) reported in one trial.
Conclusion: Gamification-based digital health interventions are safe, feasible, and show promise in enhancing attention after stroke. However, heterogeneity, small sample sizes, and short intervention durations limit generalizability. Large-scale multicenter RCTs with standardized protocols and long-term follow-up are needed to establish clinical value.
Keywords: activities of daily living, attentional rehabilitation, digital health, gamification, stroke
Introduction
Stroke is a major cause of mortality and long-term disability worldwide, with approximately 12.2 million new cases occurring annually, and many survivors enduring ongoing functional impairments.1 Cognitive dysfunction, especially attentional deficits, is highly prevalent and affects up to 92% of stroke.2 These impairments hinder functional recovery, reduce independence, limit the ability to perform activities of daily living (ADL), diminish quality of life, and place a considerable burden on caregivers and the healthcare systems.3,4 Although targeted attention rehabilitation interventions have shown clinical efficacy, access to both physical and cognitive rehabilitation services is severely limited in many regions, particularly in resource-constrained settings, exacerbating disparities in after stroke recovery.5
Despite the use of conventional rehabilitation methods, individuals with after stroke attentional deficits face challenges. Paper-and-pencil tasks, occupational therapy, and patient education have shown improvements in attention and activities of daily living (ADL).6 However, Common barriers such as reduced motivation, limited engagement, and restricted access often hinder consistent participation.3 The repetitive and monotonous nature of conventional rehabilitation frequently leads to patient disengagement and high dropout rates.7 These approaches lack personalization, fail to address individual needs, and thus limit overall effectiveness.8 In-person attendance poses difficulties for patients with mobility limitations and those in remote areas.9 Consequently, Digital health innovations have emerged as alternatives for enhancing accessibility, engagement, and personalization in after stroke cognitive rehabilitation.
In recent years, digital health interventions have emerged as promising tools for cognitive rehabilitation in stroke patients.10 Platforms such as mobile applications, virtual reality systems, and computer-based programs enable structured, repetitive, and personalized training that can be delivered remotely in clinical settings.11 These interventions offer several advantages over conventional rehabilitation. Including improved accessibility, flexible scheduling, and real-time performance monitoring.12 Despite these technological advances, maintaining user engagement and adherence remains a major challenge in digital rehabilitation programs.10 To address this limitation gamification has been increasingly integrated as a motivational design strategy within digital health platforms.13 By incorporating elements such as point, feedback, and reward, gamified interventions enhance participation and motivation transforming repetitive exercises into more meaningful activities. These mechanisms may foster neuroplasticity processes supporting attentional recovery in both clinical and home-based settings.
Previous systematic reviews have primarily focused on digital or gamified interventions for motor recovery and general cognitive outcomes, with limited emphasis on attentional rehabilitation.14,15 Moreover, attentional improvements reported in these studies do not always translate into functional gains in activities of daily living (ADL), likely due to the low ecological validity of most digital tasks that fail to replicate real-world functional contexts.4,16 Based on the results of the literature search, no systematic review has specifically synthesized evidence from randomized controlled trials (RCTs) concerning digital health and gamified interventions for stroke rehabilitation, particularly in relation to attentional rehabilitation.14 Given that attention is essential for daily functioning and independence, its rehabilitation is crucial for improving post-stroke quality of life.2 This lack of focused synthesis highlights a critical knowledge gap and underscores the need for rigorous appraisal of gamification-based digital strategies targeting attentional recovery after stroke.
This systematic review aimed to synthesize and appraise the effectiveness of gamification strategies in digital interventions targeting attentional rehabilitation in stroke patients. Specifically, this review aimed to identify gamification strategies, evaluate the range of digital platforms implemented, and assess outcomes related to attentional function and activities of daily living. In addition, the safety profile of gamification-based digital therapies was evaluated. This synthesis is expected to provide healthcare professionals with valuable insights into the potential role of gamified digital technologies in optimizing attentional rehabilitation in individuals recovering from strokes.
Patients and Methods
Study Design
This systematic review was conducted in accordance with guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).17 The review protocol was not registered in any of the database.
Eligibility Criteria
The study’s research question and eligibility criteria were based on the PICOT approach (population/intervention/comparators/outcomes/type of study). The inclusion criterion for the articles analyzed in this review was experimental studies published in full text in English from January 2015 to February 2025. In addition, studies must discuss the effectiveness of digital interventions incorporating gamification elements, such as points, levels, feedback, and avatars, to improve attentional function in adult post-stroke patients. In this review, the authors excluded study protocols, non-English-language publications, and inaccessible full-text articles. The following is an explanation of the PICOT applied in this review.
Population: Adult patients with stroke
Intervention: Digital health interventions with gamification elements
Comparator: Usual care or Standard care
Outcomes:
- Primary outcome: Attentional function
- Secondary outcomes: Activities of daily living (ADL), if available in the included studies
Type of Study: Randomized controlled trial
Data Collection and Analysis
Search Strategy
A systematic search was conducted based on research questions aligned with Medical Subject Headings (MeSH) terms, as well as combinations of synonyms and relevant topics, including Scopus, PubMed, and EBSCO-host. Boolean operators (“AND” and “OR”) were applied to broaden the scope and improve the accuracy of search results in each database. The search was performed using the following keyword combinations.
Pubmed: (“stroke”[Mesh] OR “post-stroke” OR “cerebrovascular accident” OR “brain ischemia” OR “cerebral infarction”) AND (“digital health” OR “mobile health” OR “mHealth” OR “telehealth” OR “telemedicine” OR “eHealth” OR “mobile application*” OR “smartphone app*” OR “virtual reality” OR “exergame*” OR “serious game*” OR “gamification” OR “game-based” OR “videogame*” OR “computer game*”) AND (“attention”[Mesh] OR “attentional function” OR “attention deficit” OR “cognitive attention” OR “attention training” OR “activities of daily living”[Mesh] OR “ADL” OR “functional independence”)
Scopus: (TITLE-ABS-KEY (“stroke” OR “post-stroke” OR “cerebrovascular accident” OR “brain ischemia” OR “cerebral infarction”)) AND (TITLE-ABS-KEY (“digital health” OR “mobile health” OR “mHealth” OR “telehealth” OR “telemedicine” OR “eHealth” OR “mobile application*” OR “smartphone app*” OR “virtual reality” OR “exergame*” OR “serious game*” OR “gamification” OR “game-based” OR “video game*” OR “computer game*”)) AND (TITLE-ABS-KEY (“attention” OR “attentional function” OR “attention deficit” OR “cognitive attention” OR “attention training” OR “activities of daily living” OR “ADL” OR “functional independence”))
EBSCO-host (Medline Ultimate): ((MH “Stroke+” OR “post-stroke” OR “cerebrovascular accident” OR “brain ischemia” OR “cerebral infarction”)) AND ((“digital health” OR “mobile health” OR “mHealth” OR “telehealth” OR “telemedicine” OR “eHealth” OR “mobile application*” OR “smartphone app*” OR “virtual reality” OR “exergame*” OR “serious game*” OR “gamification” OR “game-based” OR “video game*” OR “computer game*”) OR (MH “Mobile Applications+” OR MH “Videogames+” OR MH “Telemedicine+” OR MH “Virtual Reality+”)) AND ((MH “Attention+” OR “attentional function” OR “attention deficit” OR “cognitive attention” OR “attention training” OR MH “Activities of Daily Living+” OR “ADL” OR “functional independence”))
Study Selection and Quality Appraisal
The initial screening was conducted by one reviewer (A.N), who compiled all search results from the databases and imported them into the Mendeley’s reference manager. All studies were arranged chronologically, and duplicates were removed. Eligibility screening was performed by two reviewers (C.E and A.N) by assessing the titles and abstracts according to predefined inclusion and exclusion criteria. In the final stage, all authors (A.N, C.E, I.P, and V.B) independently assessed each full-text article using the Joanna Briggs Institute (JBI) critical appraisal checklist and the JBI assessment results were subsequently compared.18 There were 13 statements pertaining to articles that employed randomized controlled trial designs.
The critical appraisal score was calculated by dividing the number of “yes” responses by the total number of “yes”, “no”, and “unclear” responses, excluding any “no information” responses. Studies with JBI scores of < 70% were excluded from further analysis. Any discrepancies identified during the appraisal process were discussed and resolved by consensus among the authors. Ultimately, all the authors agreed on the final selection and eligibility of the studies included in this review.
Assessment of Risk of Bias in Included Studies
Risk of bias assessment of the selected clinical trials was conducted using the Cochrane Risk of Bias 2 (RoB-2) tool, with evaluations independently performed by two reviewers (A.N. and I. P). The RoB-2 framework systematically addresses five key domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias resulting from missing outcome data; (4) bias in the measurement of the outcomes; and (5) bias in the selection of the reported result.19 RoB is defined as “high”, “low”, or “some concern”, or “no information”. For each domain, any discrepancies between the reviewers were resolved through a thorough discussion until a consensus was reached.
Data Extraction and Analysis
Data from studies that met the criteria were extracted, including author, year of publication, country, sample size, study design, participant characteristics (age years median/mean ± SD; sex; type of stroke), technology utilized, comparison, and adverse events. Information about the details of the digital intervention and gamification elements (eg, type of game or application, points, levels, feedback, avatars), as well as exercise prescriptions (frequency, duration, intensity) and outcomes (attention function and ADL) were recorded. All extracted data were independently reviewed by one reviewer (A.N), and checked by other reviewers (I.P and V.B).
The data were analyzed using qualitative, exploratory, descriptive, and thematic approaches. The data analysis process began with the identification and tabulation of the data extracted from the reviewed articles. Subsequently, all authors analyzed and synthesized the results of each study, with a particular focus on how gamification strategies in digital health interventions can contribute to improving attentional rehabilitation in stroke patients.
Results
Study Selection
The study selection process was conducted through several systematic stages to ensure that only relevant and high-quality articles were included in the analysis (see Figure 1). During the identification phase, 1803 articles were retrieved from three databases: Scopus (n = 1101), PubMed (n = 301), and EBSCO-host (n = 401). After removing 623 duplicate records, 1180 articles were screened for titles and abstracts. At this stage, 1150 articles were excluded for irrelevance, leaving 30 studies for the full-text eligibility assessment. Following an assessment against predefined inclusion criteria (population, intervention, and language), 18 studies were excluded because the research design was not appropriate (n = 15), the interventions were not relevant (n = 2), or they were protocol studies (n = 1). The remaining 12 articles were then critically appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Tool, and all met the required methodological quality for inclusion in the final analysis.
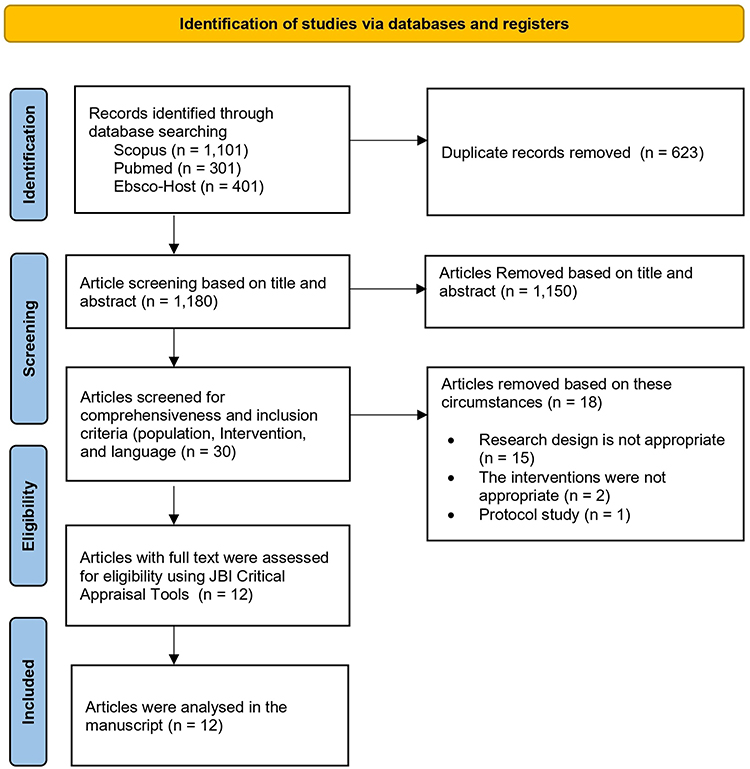 |
Figure 1 PRISMA Flowchart of Study Selection Process. Adapted from the study by Page et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews.17 |
Characteristics of the Included Studies
Table 1 describes the characteristics of the studies included in the systematic review, highlighting variations in the country of origin, sample size, study design, participant characteristics, technology utilized, and comparison. The cumulative sample of the analyzed studies included 544 patients from 12 studies. All studies analyzed were RCT-based studies with stroke patients from various countries, including the Netherlands (n=2) and Italy (n=2). Other countries, such as Denmark, Portugal, Spain, Iran, South Korea, Taiwan, China, and India, were each included in one study. This shows that the studies have diverse geographical coverage, with the majority originating from European countries and evidence from Asia and the Middle East.
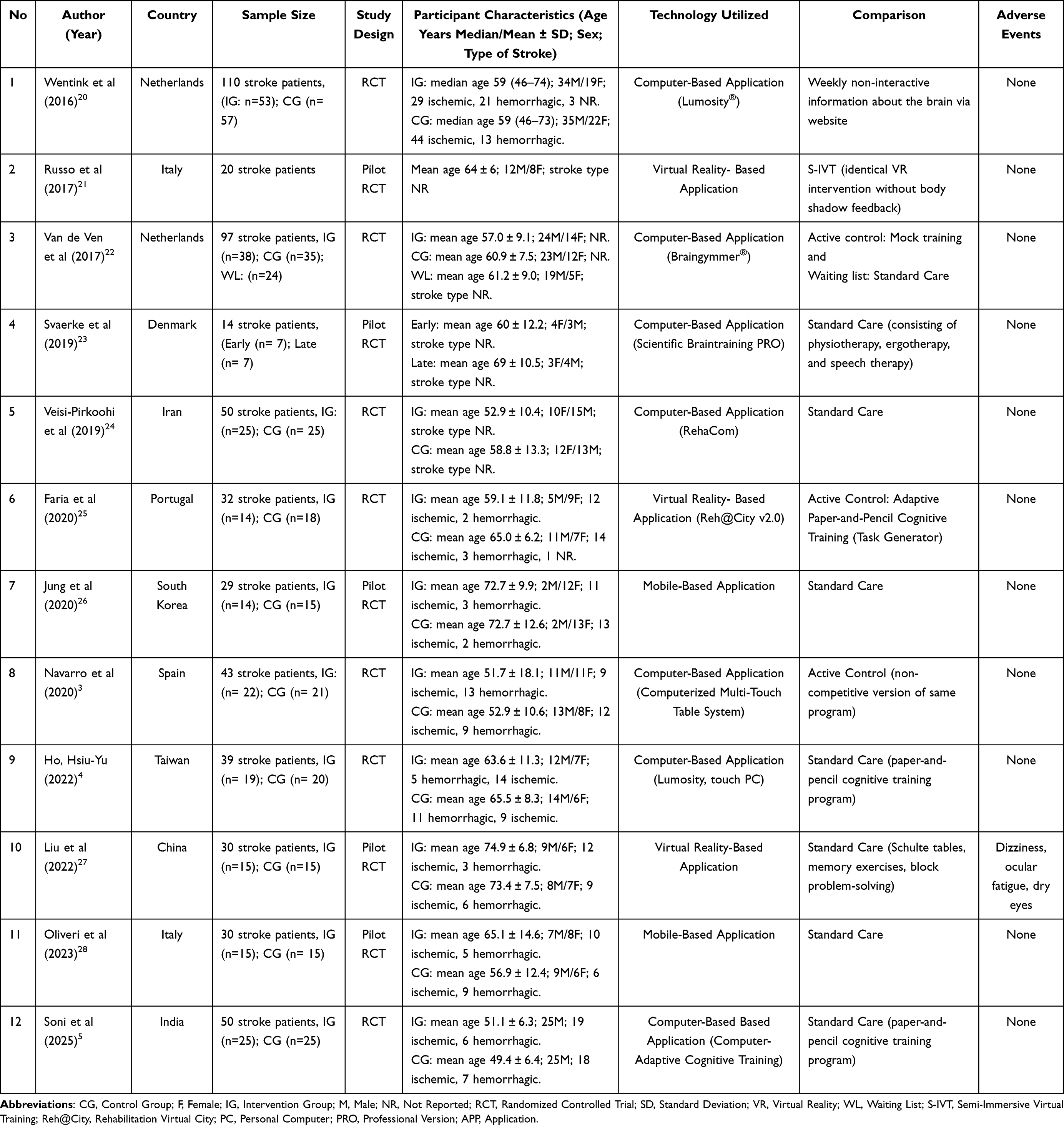 |
Table 1 General Characteristics of Studies |
Quality Appraisal and Risk of Bias of Included Studies
The JBI critical appraisal demonstrated that all the included RCTs achieved scores above 70 (see Table 2). Randomization was consistently reported across trials. However, allocation concealment was inconsistently documented, with several studies being rated as unclear. Baseline comparability and between-group treatment uniformity were generally adequate, although three trials reported imbalances and two studies did not ensure identical treatment aside from the intervention. Participant and provider blinding was rarely feasible, whereas outcome assessors were consistently blinded. Overall, the methodological quality of the included studies was acceptable, with recurring weaknesses in allocation concealment, baseline comparability, and blinding.
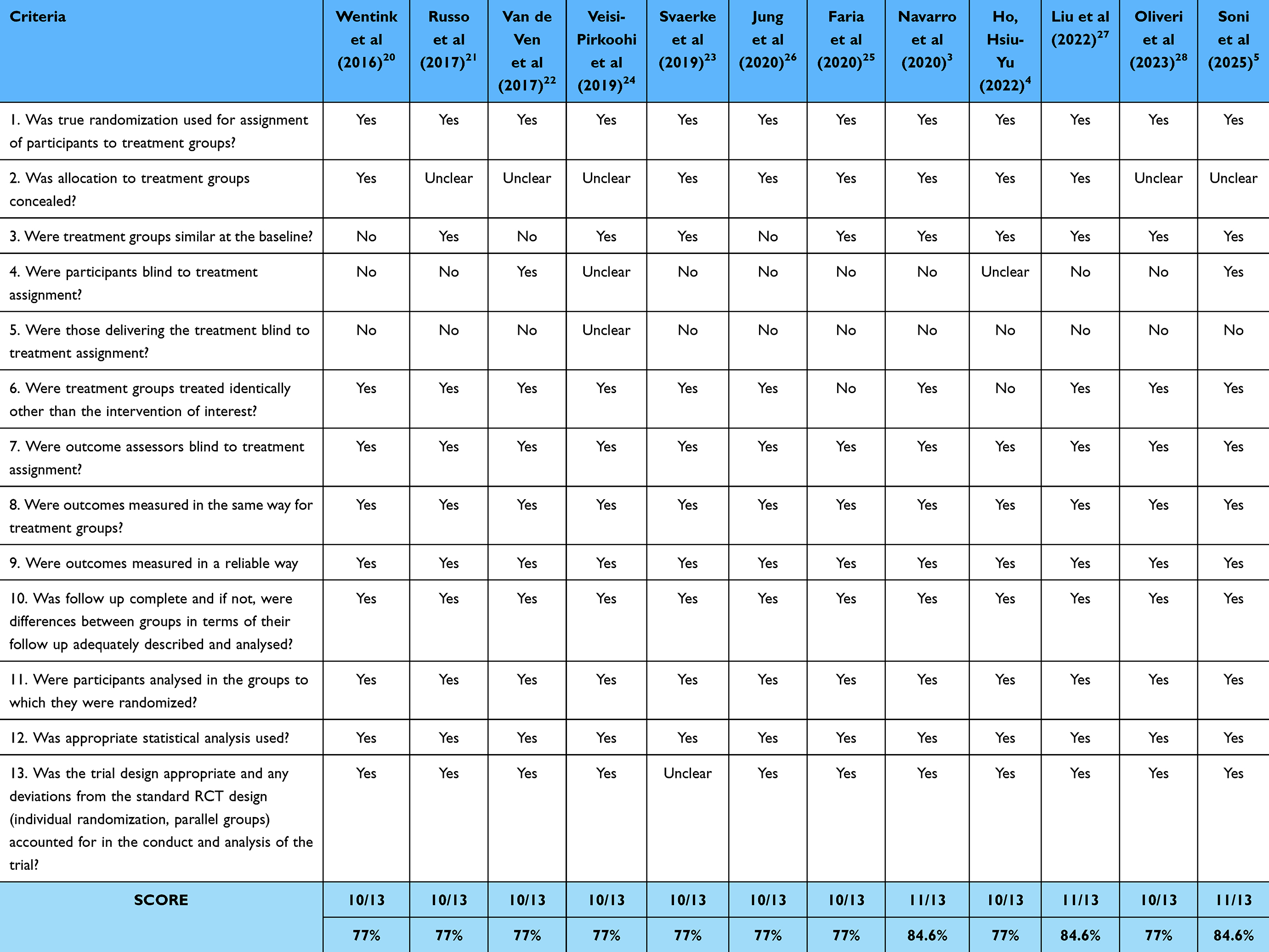 |
Table 2 Critical Appraisal Articles RCT with JBI |
In this assessment of bias risk, the majority of studies were assigned an overall rating of “some concerns”, predominantly due to deviations from intended interventions (D2) (refer to Figures 2 and 3). The randomization process (D1) was generally deemed adequate, with most trials rated as low-risk in this domain. More significant concerns were identified in the selection of the reported results (D5), which substantially impacted the overall evaluations. Most trials were assessed as having low to moderate risk concerning missing outcome data (D3) and outcome measurements (D4), although isolated instances of high risk were noted. Overall, only one trial was evaluated as having a low overall risk of bias, two trials were rated as having a high risk, and the remainder were judged as having some concerns. These findings suggest that the methodological quality was acceptable in several domains; however, further efforts are necessary to reduce deviations from the intended interventions and enhance transparency in outcome reporting.
 |
Figure 2 RoB of Included Studies. |
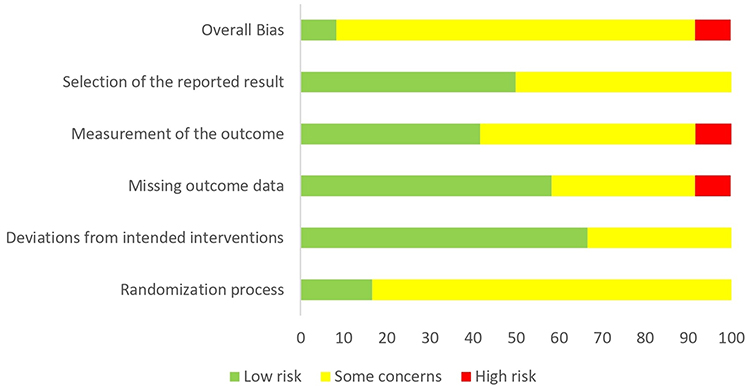 |
Figure 3 Summary of RoB. |
Digital Health Technologies Utilized for Attentional Rehabilitation in Stroke
The included studies, summarized in Table 1, demonstrated diverse applications of digital health technologies in post-stroke attentional rehabilitation. Computer-based interventions were the most frequently reported modality, identified in seven trials, encompassing both commercially available platforms such as Lumosity®,4,20 Braingymmer®,22 RehaCom,24 and Scientific Braintraining PRO,23 as well as custom-built solutions, including multi-touch table systems3 and purpose-built cognitive software.5
Other modalities include virtual reality (VR)- and mobile-based applications, each offering distinct advantages for rehabilitation delivery. VR-based interventions have been reported in three studies ranging from semi-immersive systems to fully immersive platforms, such as [email protected].21,25,27 Mobile-based applications were examined in two pilot RCTs that offered portable and flexible training options accessible beyond clinical environments.26,28 Comparators most commonly comprised paper-and-pencil cognitive training, although some studies employed active control conditions such as mock training.22
Gamification Strategies Were Identified
All 12 interventions incorporated at least one gamification element, with progression present in all studies (n = 12).3–5,20–28 Feedback (n = 10),3–5,20–22,25–28 levels (n =7),4,20–23,26,27 challenges (n = 6),3–5,21,26,28 and points (n = 5),3,20,22,25,28 were the most frequently reported features, whereas constraints (n = 3),20–22 choices (n = 2),20,22 single instances of content unlocking,22 rewards,25 competition, leaderboards, avatars,3 and chance20 occurred less often.
Progression was typically operationalised through structured levels or incremental increases in task complexity, ensuring gradual cognitive improvement.3–5,20–28 Feedback was implemented as immediate performance updates or progress tracking to enhance engagement.3–5,20–22,25–28 Challenges were used to dynamically adjust task difficulty,3–5,21,26,28 while points functioned either as indicators of performance or as virtual currency for unlocking additional content.3,20,22,25,28 Collectively, these features were often combined to form a core engagement loop centred on progression, feedback, and challenge.3–5,20–28
Although most interventions employed a fundamental cycle of progression, feedback, and challenge, significant variations were evident across studies. Certain interventions combined progression with points and levels to maintain motivation22,25,28 whereas others integrated less conventional elements such as competition, leaderboards, and avatars.3 Social and reward-based mechanisms, including rewards and content unlocking, were infrequently observed,22,25 suggesting that most interventions prioritized structured skill development and performance feedback over social or competitive reinforcement. Notably, only one study incorporated competition, leaderboards, and avatars.3 Additional details can be seen in Table 3.
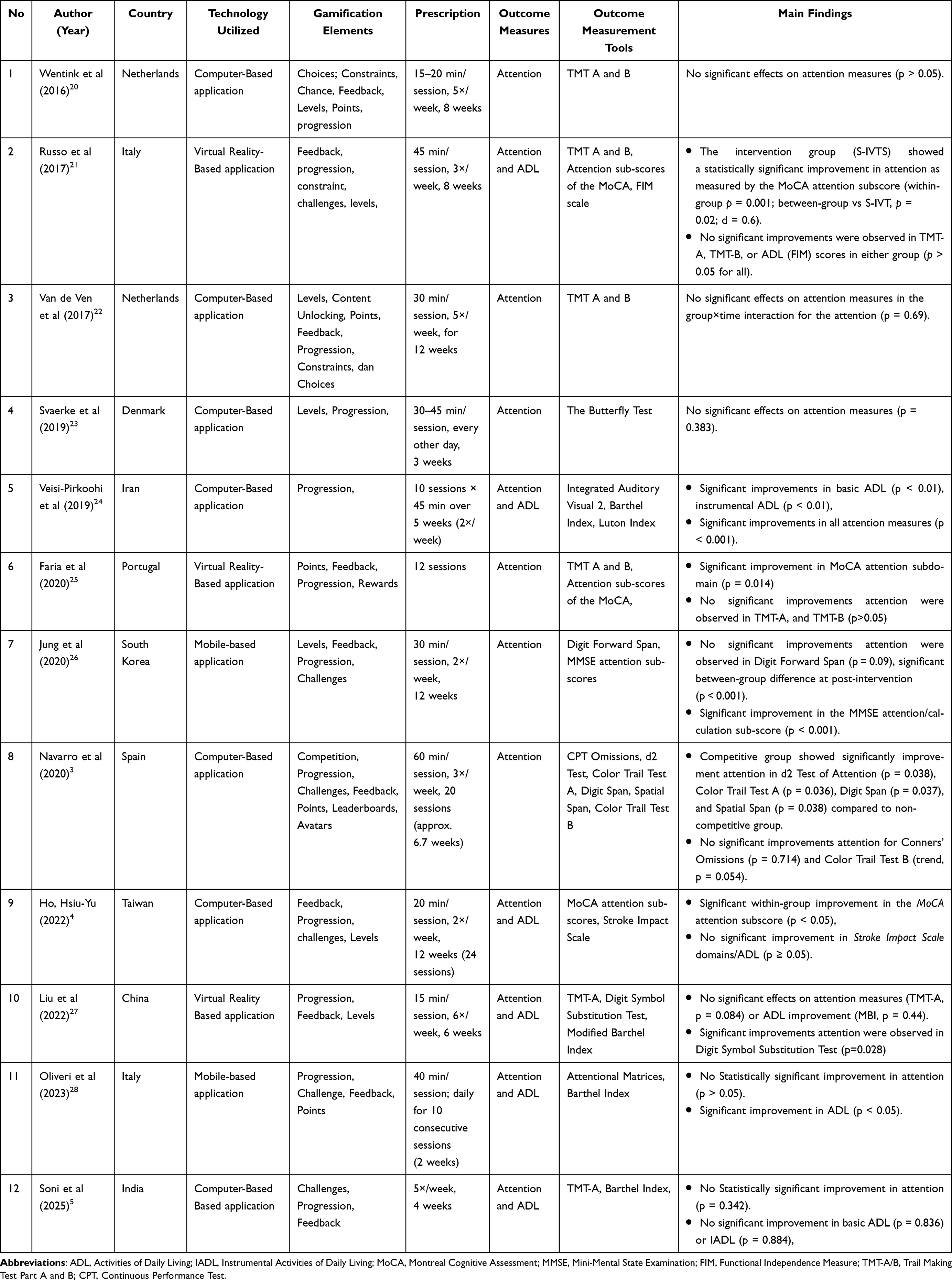 |
Table 3 Main Findings of the Included Studies |
Outcome of Intervention
Across the 12 included studies, gamification-based digital health interventions demonstrated mixed effects on poststroke attention (Table 3). Significant attentional gains were reported in seven studies, particularly in MoCA attention subscores4,21,25 and specific cognitive tests such as computerized training or neuropsychological assessments.3,24,26,27 In contrast, five studies reported no significant improvements in attentional function.5,20,22,23,28 For ADL, only two studies demonstrated significant improvements,24,28 whereas four studies reported no significant effects.4,5,21,27 Collectively, these findings suggest that gamification-based interventions may hold promise for enhancing attentional outcomes after stroke. However, their effects on functional independence and ADL were less consistent.
Safety of Digital Health Technology Interventions
One study reported mild, self-limiting adverse events, including dizziness, ocular fatigue, and dry eyes, which occurred during immersive virtual reality training.27 Other studies did not report any safety data.
Discussion
This systematic review found that gamified digital interventions after stroke attentional rehabilitation were implemented through computer-based programs, virtual reality systems, and mobile applications. Common gamification elements included progression, feedback, levels, challenges, and points. While several studies demonstrated improvements in attentional and functional outcomes, others reported minimal or inconsistent effects. Overall, these interventions were safe and well tolerated, with only mild adverse events such as dizziness or visual fatigue, although methodological heterogeneity and small sample sizes limit generalizability and highlight the need for more standardized research.
The diversity of delivery models highlights both the opportunities and limitations of digital rehabilitation after stroke. Computer-based applications remain confined to clinical settings, limiting their integration into daily routines.3–5,20,22–24 In contrast, Mobile-based interventions show greater potential for engagement and scalability, though evidence is limited.26,28 Virtual reality systems offer ecological validity through real-world environment replication but require specialized equipment and expertise.21,25,27 These contrasts highlight the need to align delivery models with patient needs and the healthcare infrastructure. Mobile formats may offer the most feasible pathway for widespread adoption, while VR and computer-based programs suit targeted rehabilitation in specialized centers. Nevertheless, differences in sensory immersion and feedback mechanisms between VR and mobile formats may yield distinct neurocognitive responses, suggesting that modality-specific mechanisms could partly account for the heterogeneous attentional outcomes.13
Several studies identified specific gamification elements that were particularly effective in enhancing attentional rehabilitation after stroke. Feedback3–5,20–22,25–28 and progression3–5,20–28 were the most consistently implemented and associated with improved attentional outcomes.4,20–23,26,27 Other common elements, included levels,4,20–23,26,27 challenges,3–5,21,26,28 and points, served to reinforce user motivation.3,20,22,25,28 Notably, Only one trial used competitive elements such as leaderboards and avatars, which enhanced attentional outcomes through social comparison.3 These findings aligns with Self-Determination Theory, suggesting that digital interventions fostering autonomy, competence, and relatedness are more likely to sustain engagement.29 However, optimal gamification configuration remains uncertain due to heterogeneity in study design, dosage, and outcome measures across trials. These inconsistencies indicate that attentional gains depend on matching task complexity, user capability, and feedback timing, which remain insufficiently standardized.
Specific gamification components may contribute differently to cognitive functional outcomes. For instance, for feedback mechanisms reinforce attentional learning through real-time correction, enhancing users’ awareness of performance and error adjustment.3 Meanwhile, progression systems sustain engagement by providing visible mastery levels and rewarding incremental improvement, consistent with motivational design principles and self-determination theory framework.29 Gamified feedback and progression systems may enhance the integration of attentional and sensorimotor networks and increase cortical recruitment to optimize neuroplasticity, thereby supporting sustained cognitive recovery.13 In addition, activities-of-daily-living (ADL)-simulating challenges enhance ecological validity and facilitate functional transfer, bridging the gap between digital task performance and real-world independence.25,28 Therefore, future gamified systems should integrate adaptive feedback loops and task scenarios that mirror daily life complexity to strengthen generalization to functional independence.14
Gamification-based digital interventions have shown measurable benefits in terms of attentional performance and daily functioning in stroke rehabilitation. Several Structured digital programs improved MoCA attention subscores and other attention domains, with comparable improvements reported across varied durations, delivery formats, and short-term protocols.3,4,21,24–28 Functional enhancements in basic and instrumental ADL were also observed, including in studies focused primarily on cognitive outcomes.4,21,24,27,28 These outcomes align with previous reviews that targeted, repetitive cognitive training fosters neuroplasticity, reinforces task-specific skills, and indirectly supports functional independence.14 However, heterogeneity in design, intensity, and outcome measures underscores the need for standardized protocols and large-scale, multicenter trials to optimize clinical application. This suggests that gamification may function best as an adjunct to conventional therapy, rather than as a standalone modality.
Gamification-based interventions were generally well-tolerated, with no serious adverse events reported across the studies. Only one trial of a VR-based application documented Minor and transient effects such as eye strain, mild headache, and cognitive fatigue were observed primarily in VR-based applications, while rare instances of cybersickness resolved after brief rest periods.27 These results align with previous digital rehabilitation studies reporting low-risk profiles in stroke patients.16
Despite the promising outcomes of digital cognitive rehabilitation for after stroke attentional recovery, persistent challenges continue to hinder optimal implementation, particularly in community-based and resource-limited settings.3,26,28 Sustaining long-term engagement and adherence remains a major barrier, especially among older adults with limited digital literacy or insufficient caregiver support, where inconsistent participation can compromise therapeutic gains and impede neuroplasticity-driven recovery.20,26,27 Moreover, the limited transfer of cognitive training benefits to daily functioning suggests that a lack of contextual relevance and intrinsic motivation may reduce real-world impact.22 We hypothesize that this limited generalization occurs because many digital cognitive exercises emphasize isolated attentional processes rather than ecologically meaningful, goal-directed activities encountered in everyday life.4 The absence of such contextualized challenges may constrain cross-domain neuroplasticity and neural reorganization, thereby limiting the generalization of functional gains to real-life performance.24,30 Future gamified interventions should therefore integrate ADL-simulating tasks within immersive environments to enhance the ecological validity and facilitate the translation of cognitive gains into functional independence.
Beyond individual-level factors, system-related barriers further constrain scalability, including restricted access to compatible devices, unstable internet connectivity, and technical malfunctions that disrupt training continuity.3,28 Cultural perceptions that undervalue gamified therapy compared with conventional rehabilitation may also erode user trust and widen disparities in access.20 Addressing these challenges requires tailored, low-barrier delivery models, culturally relevant content, and robust technical support frameworks to sustain engagement and maximize therapeutic outcomes.4,25
Implication for Practice
Gamification-based digital interventions can enhance post-stroke attentional rehabilitation by increasing engagement, extending therapeutic reach, and enabling personalized care. Their successful integration requires tailoring to patient needs, addressing access and connectivity barriers, and ensuring providers’ competence in adaptive delivery. Embedding these interventions into multidisciplinary care pathways, supported by clear guidelines and robust technical infrastructure, can promote scalability without compromising individualized quality. Strategic collaboration among clinicians, researchers, developers, and policymakers, combined with sustainable funding and evaluation frameworks, can transition gamified rehabilitation from a promising concept to a standard patient-centered component of stroke recovery. Importantly, careful patient selection is required, as individuals with severe cognitive impairment, low digital literacy, or comorbid conditions may have a limited tolerance for digital engagement. Safety considerations should also be prioritized, including monitoring for adverse effects, such as visual fatigue, dizziness, or overexertion, and ensuring that interventions are accessible, inclusive, and adaptable to patients’ functional and cognitive capacities. Integrating ecologically valid ADL-like gamified tasks within these interventions may further strengthen real-life applicability and functional independence, ensuring that attentional improvements translate into meaningful participation in everyday activities.
Limitation
This review was limited by the substantial heterogeneity in intervention designs, gamification elements, and outcome measures, which reduced comparability across studies and precluded meta-analyses. Most trials were small-scale, single-center, and of short duration, with limited or absent follow-up, restricting conclusions regarding long-term efficacy. The inconsistent reporting of intervention fidelity and variability in study protocols further hinders cross-trial synthesis. Although studies have been conducted in diverse regions, the lack of standardized approaches highlights the need for large, multicenter, randomized trials with harmonized frameworks and rigorous reporting to establish definitive evidence. Moreover, patient characteristics such as age, cognitive status, and chronic comorbidities may also influence rehabilitation outcomes.31 Access barriers in low-resource settings or regions with limited digital infrastructure may further restrict the feasibility and scalability of such interventions.
Conclusion
Gamification-based digital health interventions represent a promising strategy to support attentional rehabilitation after stroke, with some evidence indicating benefits for activities of daily living. Among gamification elements progression, feedback, levels, challenges, and points were associated with enhanced engagement and improved attentional outcomes. These interventions have demonstrated favorable safety profiles, with only minor and transient adverse effects reported in one study. However, inconsistencies in study design, small sample sizes, short intervention durations, and varied outcome measures limit the strength of the conclusions and preclude meta-analyses. To advance the field, future research should employ standardized protocols, including long-term follow-up, and conduct large-scale, multicenter trials. Such efforts will be critical in determining the true clinical value of gamification-based digital rehabilitation and its potential role as an adjunct to conventional stroke care.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025) and the authors would also like to express their sincere gratitude to STIKes Karsa Husada Garut for their institutional support during the study. The authors also acknowledge the use of Paperpal (2025 version) for language editing. All the scientific content, analyses, interpretations, and conclusions are the sole responsibility of the authors.
Funding
This research is financially supported by the Indonesian Education Scholarship, the Center for Higher Education Funding and Assessment, and the Indonesian Endowment Fund for Education, under grant number: 00565/BPPT/BPI.06/9/2024.
Disclosure
The authors (s) report no conflicts of interest.
References
1. Theppan K, Suphunnakul P. Factors influencing limb movements in post-stroke patients. Bull Faculty Phys Ther. 2024;29(1):32. doi:10.1186/s43161-024-00190-x
2. Spaccavento S, Marinelli CV, Nardulli R, et al. Attention deficits in stroke patients: the role of lesion characteristics, time from stroke, and concomitant neuropsychological deficits. Behav Neurol. 2019;2019:1–12. doi:10.1155/2019/7835710
3. Navarro MD, Llorens R, Borrego A, Alcañiz M, Noé E, Ferri J. Competition enhances the effectiveness and motivation of attention rehabilitation after stroke. A randomized controlled trial. Front Hum Neurosci. 2020;14. doi:10.3389/fnhum.2020.575403
4. Ho HY, Chen MD, Tsai CC, Chen HM. Effects of computerized cognitive training on cognitive function, activity, and participation in individuals with stroke: a randomized controlled trial. NeuroRehabilitation. 2022;51(1):79–89. doi:10.3233/NRE-210271
5. Soni AK, Kumar M, Kothari S. Efficacy of home based computerized adaptive cognitive training in patients with post stroke cognitive impairment: a randomized controlled trial. Sci Rep. 2025;15(1):1072. doi:10.1038/s41598-025-85511-3
6. Gibson E, Koh CL, Eames S, Bennett S, Scott AM, Hoffmann TC. Occupational therapy for cognitive impairment in stroke patients. Cochrane Database Syst Rev. 2022;2022(3). doi:10.1002/14651858.CD006430.pub3
7. Wojciechowski A, Korjonen-Kuusipuro K. Rehabilitation in digital environments – biophysiologically motivated gamification. Human Technol. 2022;18(3):209–212. doi:10.14254/1795-6889.2022.18-3.1
8. Erdoğan MŞ, Arpak ES, Keles CSK, et al. Biochemical, biomechanical and imaging biomarkers of ischemic stroke: time for integrative thinking. Eur J Neurosci. 2024;59(7):1789–1818. doi:10.1111/ejn.16245
9. Ghozali MT. The Effectiveness of Virtual Reality (VR)-Assisted Physical and Cognitive Rehabilitation on Stroke Recovery: a Mini Systematic Review. In:
10. Kheirollahzadeh M, Sarvghadi P, Bani Hani J, Azizkhani S, Monnin C, Choukou MA. Digital health technologies to support at-home recovery of people with stroke: a scoping review. Appl Sci. 2025;15(10):5335. doi:10.3390/app15105335
11. Ciortea VM, Motoașcă I, Ungur RA, Borda IM, Ciubean AD, Irsay L. Telerehabilitation—A viable option for the recovery of post-stroke patients. Appl Sci. 2021;11(21):10116. doi:10.3390/app112110116
12. Xing Y, Xiao J, Zeng B, Wang Q. ICTs and interventions in telerehabilitation and their effects on stroke recovery. Front Neurol. 2023;14. doi:10.3389/fneur.2023.1234003
13. Tosto-Mancuso J, Tabacof L, Herrera JE, et al. Gamified neurorehabilitation strategies for post-stroke motor recovery: challenges and advantages. Curr Neurol Neurosci Rep. 2022;22(3):183–195. doi:10.1007/s11910-022-01181-y
14. Sánchez-Gil JJ, Sáez-Manzano A, López-Luque R, Ochoa-Sepúlveda JJ, Cañete-Carmona E. Gamified devices for stroke rehabilitation: a systematic review. Comput Methods Programs Biomed. 2025;258:108476. doi:10.1016/j.cmpb.2024.108476
15. Tuah NM, Goh DL, Nasirin S, Ahmedy F, Hossin M. Mapping data mining technique and gamification approach for studying post-stroke rehabilitation training: a systematic literature review. IEEE Access. 2023;11:31323–31340. doi:10.1109/ACCESS.2023.3262260
16. Hestetun-Mandrup AM, Toh ZA, Oh HX, He HG, Martinsen ACT, Pikkarainen M. Effectiveness of digital home rehabilitation and supervision for stroke survivors: a systematic review and meta-analysis. Digit Health. 2024;10. doi:10.1177/20552076241256861
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:n71. doi:10.1136/bmj.n71
18. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. Joanna Briggs Institute. 2022. Available from: https://jbi.global/critical-appraisal-tools.
19. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019:l4898. doi:10.1136/bmj.l4898
20. Wentink MM, Berger MAM, de Kloet AJ, et al. The effects of an 8-week computer-based brain training programme on cognitive functioning, QoL and self-efficacy after stroke. Neuropsychol Rehabil. 2016;26(5–6):847–865. doi:10.1080/09602011.2016.1162175
21. Russo M, De Luca R, Naro A, et al. Does body shadow improve the efficacy of virtual reality-based training with BTS NIRVANA? Medicine. 2017;96(38):e8096. doi:10.1097/MD.0000000000008096
22. van de Ven RM, V BJI, Schmand B, et al. Brain training improves recovery after stroke but waiting list improves equally: a multicenter randomized controlled trial of a computer-based cognitive flexibility training. PLoS One. 2017;12(3):e0172993. doi:10.1371/journal.pone.0172993
23. Svaerke KW, Omkvist KV, Havsteen IB, Christensen HK. Computer-based cognitive rehabilitation in patients with visuospatial neglect or homonymous hemianopia after stroke. J Stroke Cerebrovascular Dis. 2019;28(11):104356. doi:10.1016/j.jstrokecerebrovasdis.2019.104356
24. Veisi-Pirkoohi S, Hassani-Abharian P, Kazemi R, Vaseghi S, Zarrindast MR, Nasehi M. Efficacy of RehaCom cognitive rehabilitation software in activities of daily living, attention and response control in chronic stroke patients. J Clin Neurosci. 2020;71:101–107. doi:10.1016/j.jocn.2019.08.114
25. Faria AL, Pinho MS, Bermúdez I Badia S. A comparison of two personalization and adaptive cognitive rehabilitation approaches: a randomized controlled trial with chronic stroke patients. J Neuroeng Rehabil. 2020;17(1):78. doi:10.1186/s12984-020-00691-5
26. Jung HT, Daneault JF, Nanglo T, et al. Effectiveness of a serious game for cognitive training in chronic stroke survivors with mild-to-moderate cognitive impairment: a pilot randomized controlled trial. Appl Sci. 2020;10(19):6703. doi:10.3390/app10196703
27. Liu Z, He Z, Yuan J, et al. Application of immersive virtual-reality-based puzzle games in elderly patients with post-stroke cognitive impairment: a pilot study. Brain Sci. 2022;13(1):79. doi:10.3390/brainsci13010079
28. Oliveri M, Bagnato S, Rizzo S, et al. A novel digital approach for post-stroke cognitive deficits: a pilot study. Restor Neurol Neurosci. 2023;41(3–4):103–113. doi:10.3233/RNN-231305
29. Gao F. Advancing gamification research and practice with three underexplored ideas in self-determination theory. TechTrends. 2024;68(4):661–671. doi:10.1007/s11528-024-00968-9
30. Nan MY, Karako K, Song P, Hu X, Xia Y. Integrative neurorehabilitation using brain-computer interface: from motor function to mental health after stroke. Biosci Trends. 2025;19(3):
31. Dedijer Dujović S, Djordjević O, Vidaković A, et al. Inequities in stroke recovery: examining sociodemographic predictors of rehabilitation success. Healthcare. 2025;13(14):1739. doi:10.3390/healthcare13141739
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.