Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Gamification-Based Interventions for Treatment Adherence and Self-Management in Pediatric Chronic Diseases: A Scoping Review with Implications for Thalassemia
Authors Rhamelani P ![]() , Wijayanti R, Febrian N, Widiawati A
, Wijayanti R, Febrian N, Widiawati A ![]() , Mediani HS
, Mediani HS ![]()
Received 19 April 2026
Accepted for publication 23 June 2026
Published 1 July 2026 Volume 2026:19 618146
DOI https://doi.org/10.2147/JMDH.S618146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Putri Rhamelani,1,* Restu Wijayanti,1,* Nurul Febrian,1,* Aninda Widiawati,1,* Henny Suzana Mediani2,*
1Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Henny Suzana Mediani, Email [email protected]
Abstract: Chronic diseases in children require long-term management and affect physical, psychological, and social well-being. Treatment adherence and self-management skills in children remain a challenge, particularly in conditions such as thalassemia, which require lifelong treatment. Innovative approaches such as gamification are being developed to improve children’s engagement and health behaviors, but their application in thalassemia remains limited. This study aimed to map gamification-based interventions addressing treatment adherence and self-management in children with chronic diseases and identify their implications for thalassemia. This scoping review followed the Joanna Briggs Institute (JBI) methodology and PRISMA-ScR guidelines. A literature search was conducted in five databases (PubMed, Scopus, ScienceDirect, Sage Journals, and MEDLINE) covering the years 2016– 2026. Article selection followed the PCC framework (Population: children with chronic diseases; Concept: gamification-based interventions for treatment adherence and self-management; Context: pediatric chronic disease management). A total of 16 studies involving children with various chronic diseases were included. Interventions included gamified mobile applications, serious games, augmented reality (AR), virtual reality (VR), and digital therapeutic platforms. Across the included studies, treatment adherence and self-management were the most frequently reported outcomes, followed by improvements in disease-related knowledge, technical skills, engagement, and health literacy. Several studies also reported improvements in selected clinical indicators. However, substantial heterogeneity in intervention design, outcomes, and follow-up duration limited comparisons across studies. Evidence specific to thalassemia was limited to one study, which reported improvements in health literacy, self-management, and decision-making. The mapped evidence suggests that gamification-based interventions may support treatment adherence and self-management in children with chronic diseases. Thalassemia appears to be a promising target for future digital health intervention development. However, further theory-based studies with robust designs and longer follow-up are needed.
Keywords: gamification, pediatric chronic disease, self-management, thalassemia, treatment adherence
Introduction
Chronic diseases in children are long-term conditions that require ongoing care and impact physical, psychological, and social functioning. These conditions include various diseases such as diabetes, asthma, and thalassemia, which require long-term management and the active involvement of the child and family. Management in children is more complex due to limitations in cognitive and emotional development and dependence on parents for health-related decision-making.1 The prevalence of chronic diseases in children continues to rise globally. Asthma is one of the most common chronic diseases in children,2 while type 1 diabetes also shows an increasing incidence.3 Among these conditions, thalassemia carries a high global burden, with approximately 60,000 new births annually and about 1.5% of the world’s population as carriers.4 These high figures underscore that thalassemia is a significant health issue, particularly in developing countries.
The impact of chronic diseases on children, particularly thalassemia, is multidimensional. This condition causes chronic anemia that requires lifelong blood transfusions and carries a risk of complications due to iron overload in vital organs.5 Children also experience impaired quality of life, including activity limitations, emotional issues, school-related difficulties, and social stigma.4 These impacts demonstrate that thalassemia affects not only biological aspects but also children’s psychosocial development. This underscores the critical role of treatment adherence and self-management in thalassemia care. Therapies such as blood transfusions and iron chelation require high adherence to prevent complications and improve quality of life.6 Self- management involves the child’s and family’s ability to manage treatment, monitor the condition, and make decisions regarding daily care. In reality, treatment adherence among children with chronic diseases remains low. Long-term adherence rates among children and adolescents are reported to be around 58%.7 In thalassemia, non-adherence to iron chelation therapy is common and contributes to complications and a reduced quality of life.5 This indicates a gap between therapeutic needs and real-world practice.
In such circumstances, parents play a crucial role in supporting their children’s adherence to treatment and self-management, particularly during school-age years, when children remain heavily reliant on their parents for disease management- including monitoring medication intake, scheduling follow-up appointments, and providing emotional support. Parental involvement also helps children gradually understand their health condition. Family support has been shown to improve adherence and health outcomes in children with chronic illnesses.8,9 During the school-age stage, children begin to develop independence, logical thinking skills, and an interest in interactive activities. Children are increasingly involved in their health management, though they still require guidance. Limitations in understanding the long-term consequences of therapy often lead to difficulties in maintaining adherence.1 This situation creates a gap between the demands for independence and the child’s capabilities. This gap is exacerbated by various barriers, such as low motivation, medication side effects, stigma, and a lack of social support.7 The complexity of long-term therapy also makes self-management difficult for children and their families. This situation calls for an approach that is better suited to the child’s developmental needs.10
Beyond treatment-related challenges, children with chronic diseases often experience psychosocial burdens such as anxiety related to lifelong treatment, fatigue, low motivation, and concerns about social participation. These challenges may negatively affect engagement with treatment and self-management activities. Recent discussions in digital health have emphasized the importance of designing interventions that can sustain long-term user engagement, provide meaningful outcome evaluation, and address privacy and safety concerns, particularly among vulnerable populations.11 Although much of this discussion has emerged from the mental health field, the underlying challenges are highly relevant to pediatric chronic disease management. Consequently, digital interventions for children with chronic illnesses should not only address adherence and self-management needs but also consider user engagement, acceptability, accessibility, and ethical aspects related to data privacy and protection. Gamification-based interventions may be particularly relevant in this context because they are specifically designed to enhance engagement and motivation while supporting health-related behaviors through interactive digital experiences.
Technological advancements have spurred the emergence of innovative approaches such as gamification to improve adherence and self-management. Gamification integrates game elements into health interventions to boost motivation and engagement, making it well-suited to children’s characteristics.12 Several studies have reported positive outcomes associated with gamification in the management of chronic childhood conditions. The use of virtual reality-based serious games for diabetes has been associated with improved self-management and engagement among children.1 Mobile game interventions for asthma have been reported to support medication adherence and quality of life.2 Furthermore, gamification has been proposed as a strategy to support adherence through enhanced motivation and engagement.13 Most of these studies still focus on diabetes and asthma, while research on thalassemia remains very limited. This situation highlights a research gap, even though thalassemia requires lifelong therapy with a high level of adherence.
These characteristics underscore the importance of a sustainable, innovative approach. Gamification has been proposed as a promising approach because it incorporates motivational elements, interactive learning experiences, and behavior-support strategies that may facilitate engagement in health-related activities. The limited evidence regarding thalassemia and the potential of gamification highlights the need for a more comprehensive study. A scoping review is needed to identify and map gamification interventions for pediatric chronic diseases and to explore their potential implications for school-aged children with thalassemia. Thus, the objective of this study is to explore and map gamification-based interventions addressing treatment adherence and self-management in pediatric chronic diseases, as well as to identify their implications for the development of interventions for school-aged children with thalassemia.
The remainder of this paper is organized as follows. The Methods section describes the scoping review design, search strategy, eligibility criteria, and data analysis procedures. The Results section presents the characteristics of the included studies and the mapped evidence on gamification-based interventions across pediatric chronic diseases. The Discussion section interprets the mapped findings, discusses their implications for the development of gamification-based interventions in thalassemia, and outlines directions for future research.
Materials and Methods
Study Design
This study uses a scoping review research design that maps various relevant research findings.14 This review was conducted based on the Joanna Briggs Institute (JBI) methodology and using the writing guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR).15 The article review process is carried out through various stages including identifying research questions, formulating keywords for the article search process, determining inclusion and exclusion criteria, identifying various sources of information, selecting relevant literature that meets the criteria, extracting and mapping results from selected articles, and compiling a report on the results of the article analysis.
Eligibility Criteria
The research questions and eligibility criteria in this review use the PCC (Population, Concept, Context) approach as follows:
P (Population): children with chronic disease
C (Concept): gamification-based interventions for treatment adherence and self-management
C (Context): pediatric chronic disease management
In the article search process, the author applied selection criteria consisting of inclusion and exclusion criteria. Inclusion criteria for the population included articles with subjects of children with chronic diseases; for the concept included articles that focused on gamification-based or game-based interventions addressing treatment adherence and self-management; for the context included articles related to chronic disease management in pediatric populations; and for the source type included articles in English, original research, and publication years 2016–2026. This review focused on English-language articles to minimize the risk of translation inaccuracies that could impact the analysis and interpretation of the articles. Exclusion criteria included articles with review studies and research protocols.
Data Collection
Search Strategy
Based on the JBI methodology, there are three stages of the search strategy. In the first stage, researchers conducted an initial search limited to three databases (PubMed, Scopus, and ScienceDirect). In the second stage, researchers conducted a keyword search across all available databases. Each keyword was expanded using MeSH (Medical Subject Headings) terms and synonyms to find potentially all relevant articles using the Boolean operators “AND” and “OR” on each syllable. Full search strategies for all databases are provided in Table 1. The literature used in this review was obtained from five primary databases: PubMed, Scopus, ScienceDirect, MEDLINE, and Sage Journals. Searches were conducted between April 9 and April 11, 2026. The search dates and retrieval results for each database are presented in Table 1.
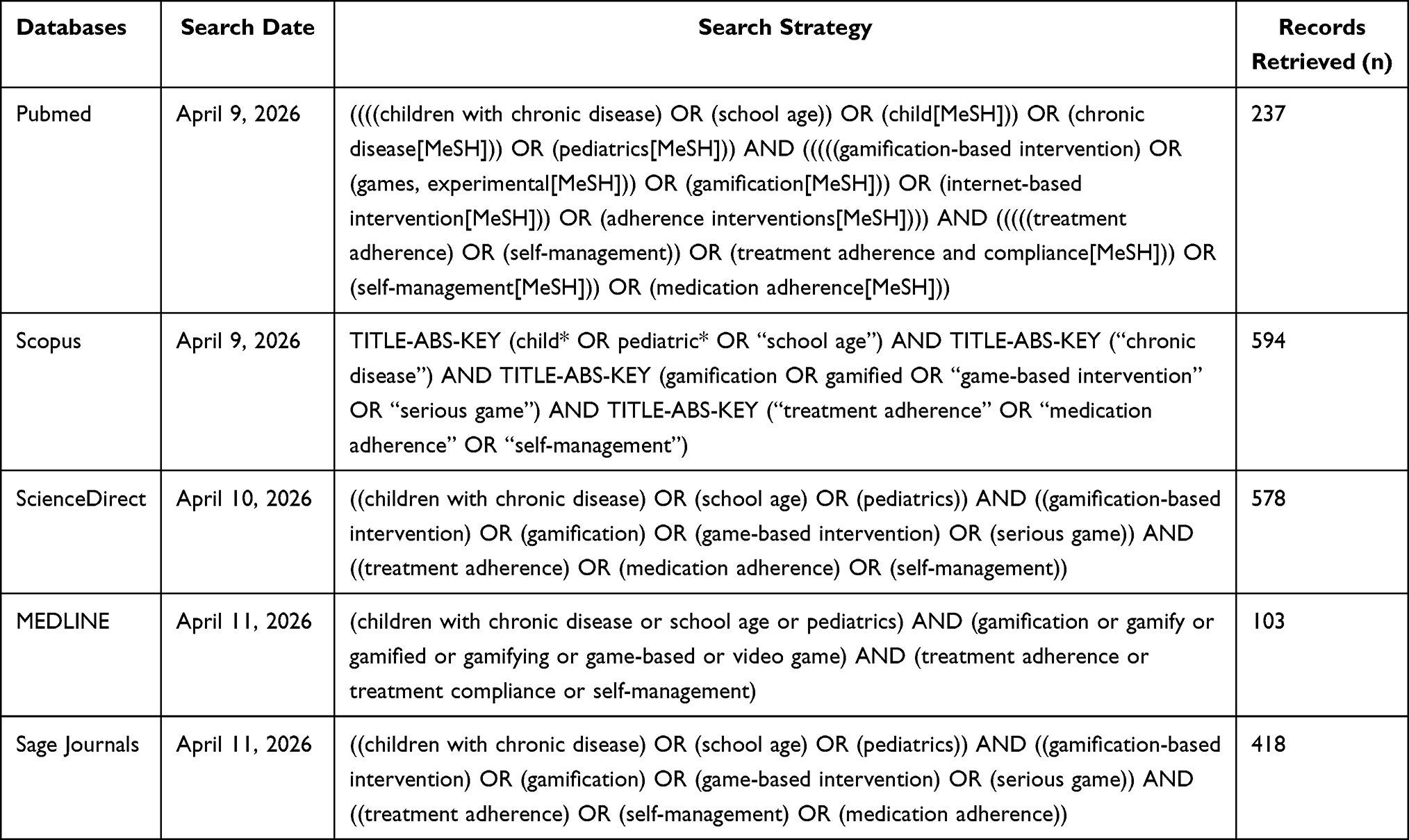 |
Table 1 Detailed Search Strategies, Search Dates, and Records Retrieved Across Databases |
The resulting inclusion and exclusion criteria were applied to the article search process. The authors used structured queries and specific search parameters to search literature databases such as Scopus, PubMed, and MEDLINE as well as publisher platforms such as Sage Journals dan ScienceDirect. All found articles were analyzed and their titles and abstracts screened for relevance to the research objectives. In the third stage, researchers conducted a bibliography search of the found articles for additional references.
Study Selection and Quality Appraisal
After the literature search was completed, all articles found were selected based on the established inclusion and exclusion criteria. The literature selection and screening process in this review is presented in the PRISMA-ScR flowchart (Figure 1). The literature selection process was carried out by eliminating duplicate articles and articles that did not meet the inclusion criteria for this review. All articles obtained from the various databases were independently screened by two reviewers (P.R. and R.W.) at the title and abstract stages using the predefined eligibility criteria. Studies considered potentially relevant were subsequently assessed through independent full-text review by the same reviewers to ensure their suitability to the focus and objectives of this review. Any discrepancies regarding study eligibility were resolved through discussion and consensus, with additional verification provided by N.F. and A.W. Articles that were irrelevant and did not meet the inclusion criteria were excluded from further analysis.
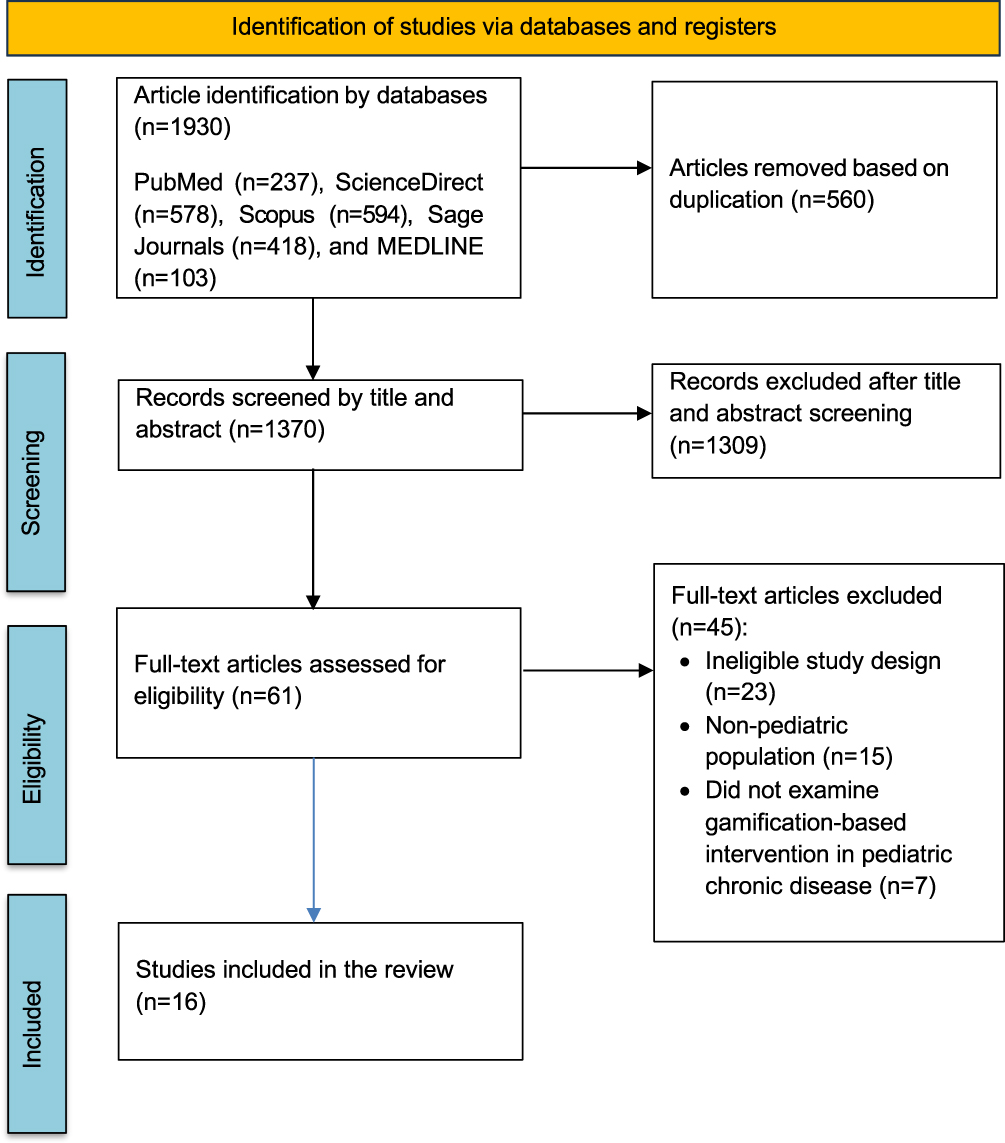 |
Figure 1 PRISMA Flowchart. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PMet al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. Creative Commons.16. |
After the literature selection process was completed, the authors conducted a thorough analysis of the articles that passed the screening stage. Although a scoping review does not require a critical assessment of the included studies, such assessments are included in this review to provide additional context regarding the methodological rigor and credibility of the reviewed studies. The authors used the JBI critical appraisal checklist to provide additional information regarding the methodological characteristics and rigor of the included studies. Consistent with JBI guidance for scoping reviews, the critical appraisal results were used to describe the quality of the evidence and inform interpretation of findings, rather than as a basis for excluding studies from the review.
The assessment based on the JBI critical assessment checklist consists of 13 items was used for experimental studies, while the checklist for quasi-experimental studies (9 items) was applied to non-randomized interventional studies. For analytical cross-sectional and observational studies, the JBI checklist with 8 items was used. In addition, qualitative and mixed-methods components were appraised using the JBI qualitative checklist consisting of 10 items, where applicable. Each item in the checklist was rated as “yes”, “no”, “unclear”, or “not applicable”. The overall quality score for each study was calculated by dividing the number of “yes” responses by the total number of applicable items (excluding “not applicable”). Any discrepancies in the assessment process were resolved through discussion among the authors until consensus was reached. No disagreements remained regarding the final inclusion of studies.
Data Extraction and Analysis
In this review, the authors analyzed 16 articles that met the established criteria. The extraction and analysis of articles in this review were conducted using a matrix table that included information on the author’s name, year of article, country, research purposes, sample and types of chronic disease research, methods, gamification-based interventions (type of gamification intervention, description, outcomes), and results. Data charting was initially performed by one reviewer (P.R.) using a standardized extraction matrix. The extracted data were independently reviewed and verified by a second reviewer (R.W.) to ensure completeness, consistency, and accuracy. Additional checks were conducted by N.F. and A.W., and any discrepancies were resolved through discussion and consensus among the authors. All articles reviewed were original research, observational or exploratory studies, and development studies.
This review ensured that all research articles reviewed were relevant and supported the review’s objective, which was to map gamification-based interventions addressing treatment adherence and self-management in pediatric chronic diseases. The author conducted data analysis through a process of identifying findings, which were then presented in a matrix table Afterward, the author organized the findings on gamification-based interventions for pediatric chronic diseases for analysis and interpretation.
Results
Study Selection
The initial literature search process was conducted by identifying articles from several databases, resulting in a total of 1930 articles. All articles were then screened based on duplicate articles, titles, and abstracts, leaving 61 articles. Further selection was carried out using the predefined inclusion and exclusion criteria, resulting in 16 articles eligible for inclusion in this review. The JBI critical appraisal checklist was subsequently applied to characterize the methodological rigor of the included studies and to support interpretation of the mapped findings. The JBI critical appraisal results for the included studies are presented in Table 2. The article selection process is explained visually using a PRISMA flow diagram (Figure 1), which details the number of records identified, screened, excluded, and included, together with the reasons for exclusion at the full-text review stage. Of the 61 full-text articles assessed for eligibility, 45 were excluded because of ineligible study designs (n=23), non-pediatric populations (n=15), or lack of relevance to gamification-based interventions in pediatric chronic disease management (n=7), resulting in 16 studies included in the review.
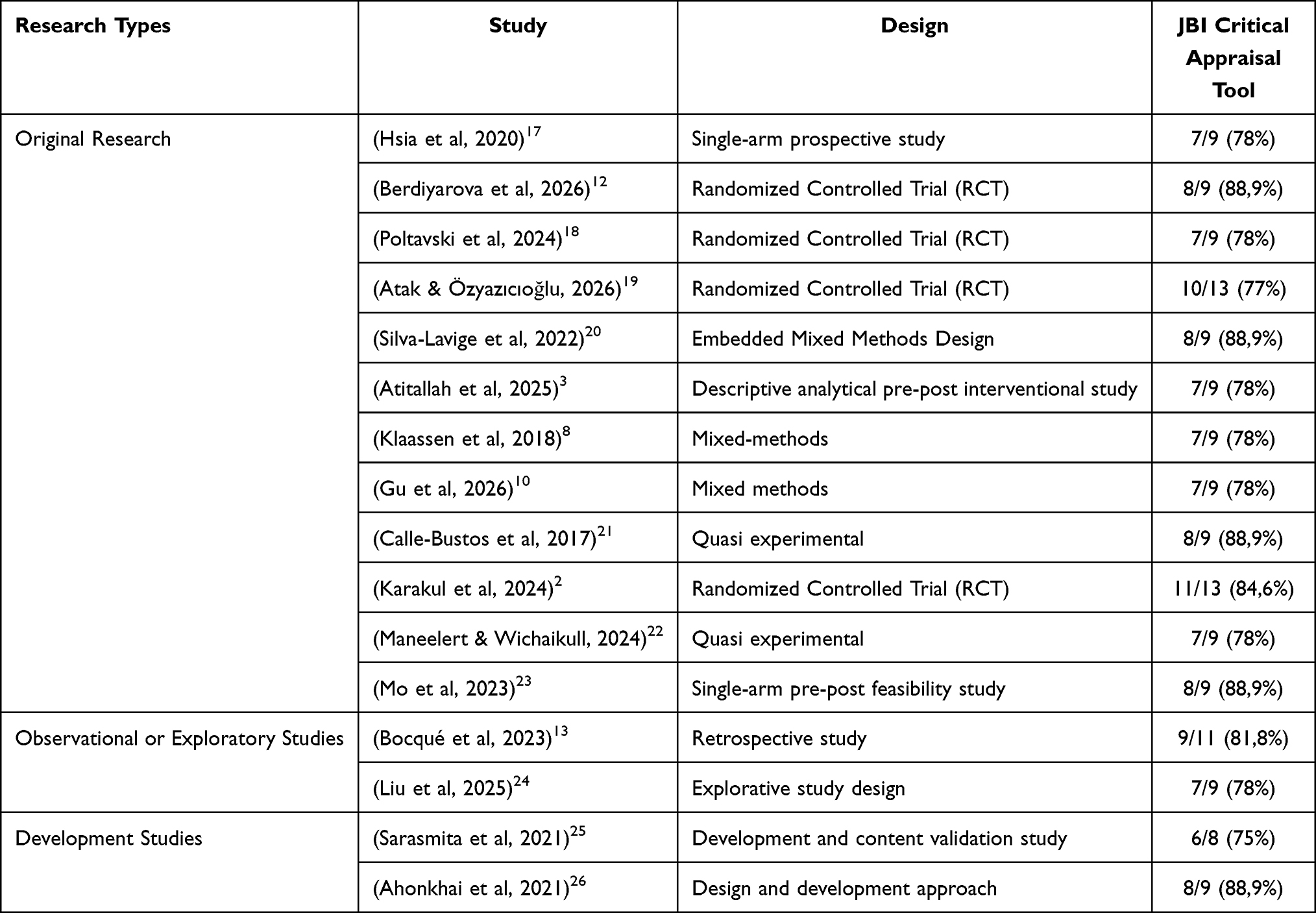 |
Table 2 JBI Critical Appraisal Results |
Study Characteristic
From the 16 articles analyzed, there were 12 articles of original research including Randomized Controlled Trial (RCT), quasi experimental, prospective study, mixed methods, feasibility study, and interventional study; 2 articles of observational or exploratory studies including retrospective study and explorative study; and 2 articles of development studies including development and content validation, design and development approach (Table 2). All involving a population of children in various childhood stages. These articles came from various countries, including United States (n=2), Uzbekistan (n=1), Germany (n=1), Nigeria (n=1), Turkey (n=2), Canada (n=1), China (n=3), Tunisia (n=1), Netherlands (n=1), Spain (n=1), Thailand (n=1), and one article was from a multi-country study (Indonesia and Taiwan). The total number of participants in this review was 857 children with chronic disease. In this review, the article with the largest sample size was 267 children,13 and the smallest sample size only involved 5 children.20
Gamification-Based Interventions for Pediatric Chronic Diseases
Sixteen studies examined the use of gamification-based interventions across various pediatric chronic diseases and developmental stages. The majority of interventions targeted school-age children (6–12 years), particularly in respiratory conditions such as asthma, where diverse gamification approaches were identified, including mobile health applications, serious games, computer-based interactive programs, and mobile game-based training. These interventions primarily focused on improving self-management and clinical outcomes, with some studies also addressing treatment adherence and user engagement.
In addition to asthma, gamification was widely applied in type 1 diabetes, mainly through serious games, augmented reality (AR), and virtual reality (VR)-based interventions. These approaches predominantly targeted knowledge improvement and self-management behaviors, often accompanied by measures of usability, satisfaction, and user experience. Similarly, in amblyopia, gamified interventions such as mobile applications and therapeutic video games focused on treatment adherence and clinical outcomes, including visual acuity and stereopsis, with engagement as a supporting component. Other chronic conditions were less frequently represented. A single study addressed chronic functional constipation, emphasizing lifestyle-related self-management behaviors such as diet, fluid intake, and physical activity. Likewise, only one study was identified for thalassemia, which focused on enhancing knowledge, decision-making, and self-management through an online gamified learning program.
Among adolescents, gamification interventions were applied to diabetes, HIV, and hypertension, with a stronger emphasis on self-management, behavioral engagement, and adherence-related outcomes. Notably, some interventions directly measured medication adherence, while others targeted psychological determinants such as self-efficacy and self-regulation. Studies involving mixed age groups were primarily conducted in amblyopia, where gamified therapeutic platforms consistently targeted treatment adherence and clinical improvements, supported by engagement and feasibility outcomes. Overall, the included studies reported a broad range of gamification-based interventions across pediatric chronic diseases, with a predominant focus on self-management and adherence-related outcomes, while also incorporating engagement and usability as commonly reported supporting components (Tables 3 and 4).
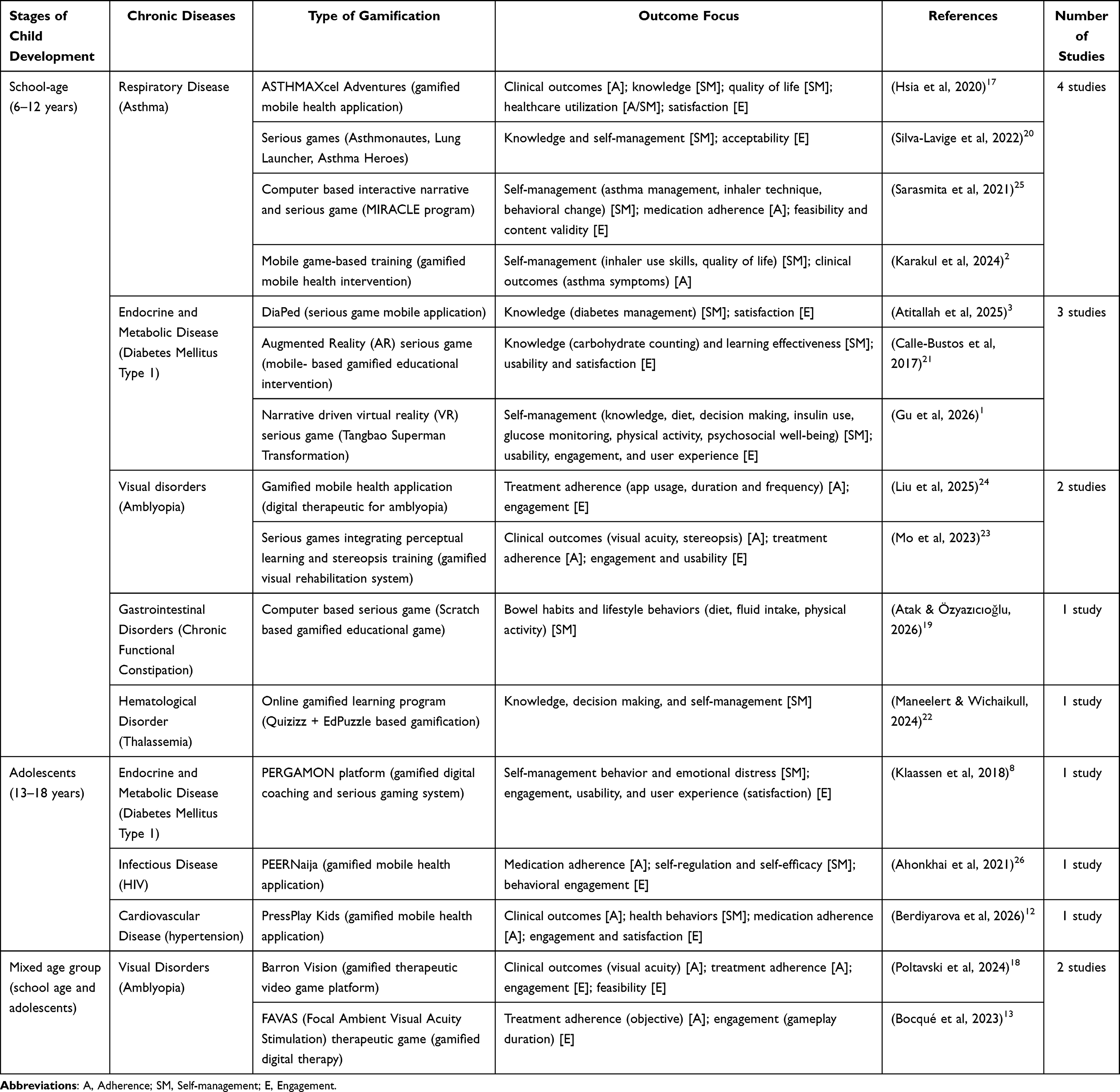 |
Table 3 Mapping of Gamification-Based Interventions for Pediatric Chronic Diseases |
 |
Table 4 Results of Article Analysis |
Discussion
Gamification-based interventions in pediatric chronic diseases have emerged as a promising digital health strategy, bridging the gap between clinical adherence requirements and the motivational needs of children and adolescents. The included studies suggest that gamification-based interventions are associated with engagement, usability, self-management, and treatment adherence outcomes across various pediatric chronic diseases. However, as this review was designed to map existing evidence rather than evaluate intervention effectiveness, these findings should be interpreted cautiously. These findings resonate with broader literature emphasizing the role of interactive, reward-based systems in sustaining behavioral change among pediatric populations. However, the diversity of technological formats, disease contexts, and age groups necessitates a critical discussion of both the strengths and limitations of gamification, as well as its implications for long-term sustainability and equity in healthcare delivery.
Types of Gamification-Based Interventions in Pediatric Chronic Diseases
The included studies indicate that gamification-based interventions in pediatric chronic diseases encompass a diverse range of technological formats, delivery platforms, and interaction designs, reflecting an evolution from simple educational tools to complex, behavior-oriented digital health interventions. Broadly, these interventions can be categorized into gamified mobile health (mHealth) applications, serious games, immersive technologies such as augmented reality (AR) and virtual reality (VR), gamified therapeutic video games, and hybrid gamified platforms integrating coaching and social features.
Gamified mobile health applications represent the most dominant intervention type across disease categories. These applications integrate core game mechanics such as rewards, points, levels, and progress tracking into self-management tools that are accessible via smartphones. Interventions such as ASTHMAXcel Adventures and PressPlay Kids illustrate how mobile-based gamification has been applied to support behavioral modification, adherence-related outcomes, and clinical indicators through real-time monitoring and personalized feedback.12,17 This finding is consistent with previous literature, which emphasizes that gamified eHealth interventions leveraging feedback systems and reward mechanisms have been associated with improved self-management behaviors in youth with chronic conditions.27 The accessibility and seamless integration of these applications into daily routines make them particularly suitable for sustaining long-term engagement.
Serious games constitute another major category, designed specifically for educational and behavioral change purposes. These interventions employ interactive scenarios, simulation-based learning, and narrative elements to enhance knowledge acquisition and self-management skills. For example, programs such as MIRACLE and DiaPed utilize structured, level-based learning and interactive gameplay to improve disease-related knowledge and behavioral competence.3,25 Findings from these approaches are consistent with the broader literature, which suggests that gamification may enhance intrinsic motivation by transforming health-related tasks into engaging and meaningful experiences.28 This is particularly relevant in pediatric populations, where engagement and enjoyment are critical determinants of intervention success.
More advanced forms of gamification are represented by immersive technologies, including AR and VR-based interventions. These approaches provide interactive and experiential learning environments, allowing children to practice disease management skills in simulated real-life contexts. For instance, AR-based carbohydrate counting games and VR-based narrative interventions such as “Tangbao Superman Transformation” reported improvements in knowledge, decision-making, and self-management behaviors.1,21 These findings are supported by prior evidence suggesting that immersive and interactive environments enhance engagement and facilitate experiential learning, thereby strengthening behavioral outcomes.28 However, despite their promising potential, such technologies may face limitations in scalability and accessibility, particularly in low-resource settings.
Gamified therapeutic video games and digital therapeutics represent another important category, particularly for conditions requiring sustained adherence to repetitive treatments. Interventions such as Barron Vision and FAVAS transform therapeutic exercises into engaging gameplay experiences, integrating adaptive difficulty, real-time feedback, and structured sessions to improve both clinical outcomes and adherence.13,18 These findings suggest that gamification may serve as a strategy to reduce perceived treatment burden and support motivation, particularly in long-term therapies.
In addition, hybrid gamification platforms that combine gaming elements with coaching systems, wearable sensors, and social interaction features are emerging as comprehensive solutions for chronic disease management. The PERGAMON platform exemplifies this approach by integrating serious gaming with personalized coaching and self-monitoring, although challenges related to usability and sustained engagement remain.8 Similarly, gamified learning platforms using tools such as Quizizz and EdPuzzle have been reported to support knowledge acquisition and decision-making through interactive, multimedia-based learning.22 These hybrid approaches reflect a shift toward ecosystem-based interventions that address multiple dimensions of self-management simultaneously.
Despite these strengths, several limitations must be considered. First, there is substantial heterogeneity in intervention design, game mechanics, and outcome measures across studies, making it difficult to identify which gamification components may be most relevant across different contexts. This limitation has also been highlighted in prior systematic reviews, which report variability in theoretical frameworks and evaluation methods.27 Second, while short-term positive outcomes related to engagement, knowledge, and adherence are frequently reported, evidence regarding long-term outcomes remains limited.28 Many studies included in this review employ short follow-up periods or pilot designs, restricting conclusions about sustained behavioral change.
Furthermore, issues related to accessibility and digital inequality present important challenges for implementation. Although mobile-based interventions offer relatively high scalability, more advanced technologies such as AR and VR may not be widely accessible in all settings, particularly in low- and middle-income countries. This raises concerns regarding equity and the potential for disparities in access to digital health innovations.28 Finally, methodological limitations, including small sample sizes and limited use of randomized controlled designs in some studies, may affect the robustness of the evidence base.27
Recent evidence from a systematic review of policy-driven digital health interventions suggests that the effectiveness and sustainability of digital health programs depend not only on technological design but also on supportive policy and health-system environments.29 Such interventions have been recognized as important mechanisms for promoting equitable access, scalability, integration into routine healthcare services, and long-term population health impact. From this perspective, future gamification-based interventions for pediatric chronic diseases should be considered not as standalone applications but as components of broader digital health ecosystems that incorporate clinical workflows, caregiver involvement, health education, data governance, and supportive health policies. Such integration may facilitate sustainable implementation while addressing important considerations related to equity, accessibility, privacy, and clinical effectiveness. This policy-level perspective also highlights important future research opportunities, including the evaluation of implementation outcomes, health-system integration, and the long-term public health impact of gamification-based interventions.29
Overall, the typology of gamification-based interventions in pediatric chronic diseases reflects a continuum from simple educational tools to sophisticated, multi-component digital health ecosystems. While gamified mobile applications and serious games dominate due to their feasibility and scalability, emerging technologies and hybrid platforms offer promising opportunities for enhancing personalization, engagement, and clinical impact. However, future research should focus on standardizing intervention components, strengthening methodological rigor, and evaluating long-term outcomes to better understand the long-term impact and sustainability of gamification in pediatric chronic disease management.
Gamification-Based Intervention Across Diseases and Age Groups
The synthesis of the included studies highlights that gamification-based interventions have been widely implemented across a broad spectrum of pediatric chronic diseases and developmental stages, demonstrating considerable adaptability and relevance in pediatric healthcare. These interventions are not confined to a single disease domain but span respiratory, endocrine, visual, gastrointestinal, hematological, infectious, and cardiovascular conditions, reflecting the versatility of gamification as a behavior-oriented digital health strategy.
Across disease categories, gamification has been most extensively applied in asthma and type 1 diabetes, likely due to the high demand for continuous self-management, adherence to medication, and behavioral regulation in these conditions. In asthma, gamified interventions such as mobile applications and serious games consistently target symptom recognition, trigger avoidance, and inhaler technique, with reported outcomes related to self-management and clinical indicators.2,17 Similarly, in type 1 diabetes, interventions range from educational serious games to immersive VR platforms that address complex self-management behaviors, including insulin administration, carbohydrate counting, and glucose monitoring.1,3 These findings are consistent with prior literature, which indicates that gamification may be particularly relevant in chronic conditions requiring daily decision-making and sustained behavioral engagement.30
Beyond these common conditions, gamification has also been applied in less frequently studied diseases, with several studies reporting favorable outcomes. For example, in amblyopia, gamified therapeutic video games and digital applications have been associated with treatment adherence and clinical outcomes reported in the included studies by transforming repetitive visual training into engaging gameplay.24 In gastrointestinal disorders such as chronic functional constipation, gamified educational games promote healthy lifestyle behaviors, including diet and fluid intake.19 Additionally, gamification has been applied in conditions such as thalassemia, HIV, and pediatric hypertension, where interventions focus on supporting knowledge acquisition, adherence-related outcomes, and behavioral outcomes through interactive and reward-based systems.12,22,26 This wide applicability underscores the flexibility of gamification in addressing diverse clinical and behavioral needs.
From a developmental perspective, the design and implementation of gamified interventions vary significantly across age groups, reflecting differences in cognitive, emotional, and behavioral characteristics. In school-aged children (6–12 years), interventions tend to emphasize visual engagement, simple game mechanics, and short, interactive sessions. Features such as avatars, animations, rewards, and mini-games are commonly used to enhance motivation and facilitate learning through play. In contrast, adolescents (13–18 years) are more responsive to complex systems that incorporate autonomy, social interaction, and self-regulation. Interventions targeting this age group often include goal-setting, peer interaction, leaderboards, and personalized feedback, as seen in platforms such as PEERNaija and PERGAMON.8,26
This age-sensitive design aligns with developmental and behavioral theories, which suggest that motivation and engagement strategies must be tailored to the user’s developmental stage. Supporting this, DeSmet et al (2016) highlight that gamification interventions may be more beneficial when they incorporate age-appropriate behavior change techniques and align with users’ cognitive abilities and motivational drivers30 Younger children benefit more from extrinsic motivators and playful interaction, whereas adolescents are more influenced by intrinsic motivation, autonomy, and social dynamics.
Despite these strengths, several challenges emerge when examining gamification across diseases and age groups. One key limitation is the variability in effectiveness across different conditions. While a larger body of evidence exists for asthma and diabetes, the evidence base for other conditions remains limited and often relies on small-scale or exploratory studies. This concern is echoed in a systematic review by Johnson et al (2017), which found that although gamification shows promise in improving health behaviors, the strength of evidence varies widely depending on the target population and condition, with inconsistent effects across studies.31
Another limitation relates to developmental disparities in engagement. While younger children may initially respond well to gamified elements, maintaining long-term engagement can be challenging as novelty effects diminish. Conversely, adolescents may experience reduced engagement if interventions are perceived as overly simplistic or not aligned with their need for autonomy and social relevance. Previous research further emphasizes that poorly designed gamification, especially when it relies too heavily on extrinsic rewards, may fail to sustain motivation over time, highlighting the importance of incorporating meaningful and intrinsically motivating elements.31
Additionally, the diversity of diseases and age groups introduces complexity in intervention design and evaluation. Standardizing gamification strategies across heterogeneous populations is inherently challenging, as interventions must balance disease-specific requirements with age-appropriate engagement strategies. This complexity may contribute to inconsistencies in outcomes and limit the generalizability of findings.
Overall, gamification-based interventions appear applicable across a wide range of pediatric chronic diseases and developmental stages. Their adaptability allows for tailored approaches that address both disease-specific needs and age-related characteristics. However, future research should focus on strengthening the evidence base in underrepresented conditions, optimizing age-specific design strategies, and evaluating long-term effectiveness to ensure sustainable impact across diverse pediatric populations.
Gamification Outcome: Adherence and Self-Management
Adherence is one of the primary outcomes of gamification in health contexts. Included studies reported increases in medication adherence associated with reward and reminder systems among children and adolescents with hypertension.12 In addition, the development of adherence tracking systems has helped adolescents with HIV monitor their treatment progress more effectively.26 Previous study reported higher adherence to physical and visual therapy interventions, with adherence rates reaching 85.7% in the video game group, which proved non-inferior compared to standard eye-patching therapy.18 The latest FAVAS technology further increased mean objective adherence from 55% to 68.5%.13 However, evidence from systematic reviews indicates that results are not always consistent; Johnson et al (2016) reported that while 59% of studies demonstrated positive effects, 41% showed mixed or neutral findings, suggesting that the effectiveness of gamification should be interpreted with caution.31
Duration and consistency of therapy use are also important indicators of adherence. Children using FAVAS technology spent significantly more time engaged in visual therapy, with a total duration of 2651.2 minutes, reflecting greater involvement compared to earlier versions.13 Mobile health applications also contributed by increasing exercise frequency and app usage duration compared to baseline.24 This suggests that gamification may support adherence-related behaviors and sustained engagement in therapy. Nevertheless, previous study highlighted methodological and population heterogeneity in gamification studies on medication adherence, limiting the generalizability of findings.32 Moreover, some patients reported that gamification features felt repetitive or irrelevant, which could reduce long-term motivation.
Self-management was a commonly reported outcome across the included studies. Previous study reported improvements in diabetes-related knowledge following serious game interventions, with mean scores rising from 29.8 to 68.6.3 Augmented reality (AR) technology also enhanced carbohydrate counting skills, with median scores increasing from 2 to 6–7.21 Understanding of asthma improved from 20% to 60% correct responses after interactive scenario use.20 Among thalassemia patients, health literacy increased significantly (p =0.001).22 Yet Brown et al (2016) found that most web-based interventions with gamification features employed only one simple game element (such as story/theme), and no study explicitly examined the impact of gamification on adherence33 This suggests that while gamification may enhance literacy and technical skills, empirical evidence on its specific mechanisms remains limited.
Beyond knowledge outcomes, several studies reported improvements in technical skills associated with gamification-based interventions. Mobile game interventions were associated with improvements in inhaler use skills among children with asthma.2 Interactive simulations helped children master disinfection and insulin injection techniques independently.3 Behavioral changes in diet and lifestyle were also observed; for example, children with constipation showed significant improvements in defecation frequency and fiber and fluid intake.19 Hypertensive patients successfully reduced sodium intake and increased physical activity by 2000 steps per day.12 However, the Triumf study by Tark et al (2019) revealed that although children with cancer rated the gamified application positively and easy to use, some declined participation due to lack of interest in digital games34 This highlights limitations in gamification acceptance among certain populations.
Self-efficacy and decision-making were also improved through gamification. The use of VR superhero games increased children’s confidence and reduced resistance to medical procedures such as injections.1 Thalassemia patients also demonstrated improved clinical decision-making skills related to daily self-care management.22 These findings emphasize that gamification not only targets adherence but also empowers patients to manage their chronic conditions. Nonetheless, several critical reviews have noted that gamification effects are often short-term and may even cause anxiety when rewards are not achieved.31,32 Therefore, intervention design must carefully consider psychosocial factors to avoid unintended negative consequences.
Clinical outcomes were also reported in several studies examining adherence and self-management interventions. The proportion of well-controlled asthma patients increased from 30.8% to 59.0% after gamified interventions.17 Among hypertensive patients, systolic blood pressure decreased by −8.2 mmHg.12 Thalassemia patients experienced a reduction in serum ferritin levels from 2454.93 to 1975.64.22 Visual function also improved significantly in terms of visual acuity (logMAR) and stereopsis.23 However, Brown et al (2016) stressed that adherence data in web-based interventions were often reported inconsistently, making it difficult to draw strong conclusions about the clinical impact of gamification33 Thus, although preliminary findings suggest potential benefits, further research with stronger methodological designs remains necessary.
Implication for Gamification-Based Intervention in Thalassemia
Thalassemia represents a particularly suitable target for gamification-based interventions due to the lifelong, multi-component nature of its management. Patients must adhere to regular transfusions, iron chelation therapy, clinic attendance, and lifestyle monitoring, all of which require sustained behavioral commitment. The chronicity of the disease and the need for continuous engagement align well with the strengths of gamification, including habit formation, motivation reinforcement, and skill rehearsal. Early evidence, such as the online Quizizz/EdPuzzle program, demonstrated promising improvements in knowledge, decision-making, and self-management among school-age children.22 These findings suggest that gamification can serve as a complementary tool to traditional education and clinical care, particularly in pediatric populations where interactive and engaging formats may facilitate learning and participation.
To maximize impact, gamification interventions in thalassemia should be designed with clear outcome targets and robust evaluation metrics. Primary outcomes should include objective measures of chelation adherence (eg, electronic pillboxes, pharmacy refill rates), transfusion appointment attendance, and clinically relevant biomarkers such as serum ferritin trends. Secondary outcomes may encompass disease knowledge, decision-making in iron overload scenarios, self-efficacy for home care, and quality of life. The rationale for prioritizing biomarkers is that they provide direct evidence of how behavioral changes translate into tangible health benefits.
Core intervention components should address the unique demands of thalassemia care. A medication module could incorporate daily reminders, micro-learning on chelation administration, and streak/reward systems to reinforce consecutive adherence. Appointment and transfusion trackers may gamify attendance with rewards for punctuality and preparatory tasks. Scenario-based mini-games could simulate recognition of iron overload symptoms and management of chelation side effects, thereby strengthening patient readiness. Caregiver integration is essential, with weekly summaries, shared goals, and caregiver badges to align family support particularly critical for younger children. Clinician dashboards and secure data-sharing mechanisms would ensure timely intervention when adherence declines or ferritin levels worsen.
Theoretical grounding and co-design are vital for ensuring relevance and sustainability. Self-Determination Theory emphasizes autonomy, competence, and relatedness, while Social Cognitive Theory highlights modeling and reinforcement.35 Embedding these frameworks into gamification design can enhance intrinsic motivation and behavioral change. Co-design with children, parents, and hematology teams will further ensure cultural acceptability, usability, and clinical relevance.
Implementation should follow a phased pathway. Phase 1 involves formative co-design and usability testing, including cultural adaptation and content validity. Phase 2 should pilot feasibility trials to measure engagement, acceptability, and short-term adherence proxies. Phase 3 requires adequately powered randomized controlled trials with objective adherence measures and clinical endpoints (eg, ferritin levels, transfusion intervals) and at least 12 months of follow-up to assess maintenance. Process evaluations should explore mediators such as motivation and self-efficacy, as well as moderators including age, family support, and socioeconomic status.
Equity, access, and safety considerations must also be addressed. Interventions should include low-bandwidth and offline functionality for resource-limited settings, ensure privacy and data security for minors, and provide transparent consent and data-use policies. Designing for low literacy and multiple languages, alongside caregiver-facing content, will broaden accessibility and relevance. In summary, thalassemia care demands sustained adherence and behavioral engagement, making it an ideal candidate for gamification-based interventions. While early evidence is promising, future work must prioritize rigorous evaluation, contextual adaptation, and equitable access to fully realize the potential of gamification in improving long-term outcomes for thalassemia patients.
Given that several included studies reported positive outcomes related to knowledge, engagement, and adherence in other pediatric chronic diseases, a theory‑driven, co‑designed gamified intervention tailored to the specific adherence tasks of thalassemia (chelation, transfusion attendance, symptom monitoring) is a promising next step. Early development should emphasize objective adherence measurement and clinical biomarkers to demonstrate meaningful health impact before broad implementation.
Strengths and Limitations
This study employed a scoping review approach based on the Joanna Briggs Institute (JBI) methodology and the PRISMA-ScR guidelines, thereby ensuring a systematic and transparent process for identifying and mapping evidence related to gamification interventions for chronic childhood diseases. A comprehensive literature search was conducted across several major databases, enabling a broad scope of studies and enhancing the representativeness of the results. The analysis not only focused on the type of intervention but also encompassed variations in approaches based on disease type, age group, and key outcomes such as treatment adherence and self-management, thereby providing a more comprehensive overview. The review mapped evidence from various research designs, including randomized controlled trials, quasi-experimental studies, mixed-methods studies, and development studies, enabling a broad overview of the current landscape of gamification-based interventions in pediatric chronic diseases. This approach allows for a broader understanding of the characteristics, reported outcomes, feasibility, and acceptance of gamification interventions across different contexts.
As a scoping review, this study was intended to map and characterize the existing evidence rather than determine the effectiveness of gamification-based interventions. Therefore, the findings should be interpreted as an overview of intervention characteristics, reported outcomes, and research trends rather than definitive evidence of intervention effectiveness. Although a JBI critical appraisal was conducted, the appraisal results were used to provide contextual information regarding methodological rigor and were not used as criteria for study inclusion or exclusion.
The JBI critical appraisal was conducted to provide contextual information regarding the methodological rigor of the included studies and to support interpretation of the mapped evidence. The focus on implications for thalassemia provides an additional contribution by highlighting areas that were under-explored in previous research. On the other hand, the high variability in intervention designs, gamification elements, and outcome indicators across studies limits the ability to make direct comparisons and determine which intervention components may be most relevant across different settings and populations. Differences in disease type, participant characteristics, and intervention duration also affect the consistency of findings. The relatively short follow-up duration and the predominance of small-scale or early-stage studies limit understanding of long-term outcomes and the sustainability of behavioral changes. The number of studies specifically addressing thalassemia remains very limited, so the implications drawn are largely conceptual and require further empirical validation. The restriction to English-language articles has the potential to introduce publication bias, while some studies with small sample sizes and methodological limitations may affect the strength of the synthesized evidence.
Conclusion
This scoping review mapped the existing evidence on gamification-based interventions addressing treatment adherence and self-management in children with chronic illnesses. The included studies suggest that gamification-based interventions may support these outcomes across various pediatric chronic diseases. Various forms of intervention, ranging from gamification-based mobile apps to immersive technologies such as AR and VR, were reported to target engagement, knowledge, and health-related behaviors among children. Several included studies also reported outcomes related to clinical indicators in certain conditions. The mapped evidence indicates that gamification-based interventions have been applied across various disease types and developmental stages. These interventions commonly incorporate motivational elements and interactive learning experiences that are designed to align with children’s developmental characteristics. Reported outcomes may vary according to intervention design, alignment with user needs, and the context of the targeted disease.
The findings of this review suggest that thalassemia represents a relevant area for the future development of gamification-based interventions, given the need for long-term therapy and the importance of active patient and family involvement. The lack of direct evidence regarding thalassemia highlights the need for further, more targeted, and evidence-based research. Future intervention development should emphasize theory-based approaches, involve children and families through co-design, and be tailored to the specific adherence demands of thalassemia care. Evaluation of objective adherence outcomes and clinically relevant biomarkers is crucial to demonstrate meaningful health impacts before broader implementation. Gamification may represent a promising component of future digital health innovations aimed at supporting the management of chronic diseases in children, particularly thalassemia. However, further rigorous research is needed, particularly in underrepresented chronic conditions, to evaluate long-term outcomes, optimize age-specific intervention designs, and assess implementation across diverse healthcare and sociocultural contexts.
Acknowledgments
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gu H, Mohd Muhaiyuddin NDB, Shaari NB. Narrative-driven virtual reality serious game to support type 1 diabetes self-management in children. Sci Rep. 2025;2025:1.
2. Karakul A, Düzkaya DS, Bozkul G, Çapanoğlu M. The effect of mobile game training designed for asthmatic children on asthma management and quality of life. J Pediatr Nurs. 2024;76:e149–23. doi:10.1016/j.pedn.2024.02.025
3. Atitallah S, Neffati A, Boukeri MA, et al. A serious game “DiaPed”: impact on therapeutic education for children with type 1 diabetes in Tunisia. Sage Open Pediatrics. 2025;12:10. doi:10.1177/30502225251357044
4. Erkul M, Öztürk Z. Lived experiences of adolescents with thalassemia major: a phenomenological study/lived experiences in tm adolescents. J Pediatr Nurs. 2026;87:118–125. doi:10.1016/j.pedn.2026.01.009
5. Wang LE, Muttar S, Badawy SM. The challenges of iron chelation therapy in thalassemia: how do we overcome them? Expert Rev Hematol. 2025;18:351–357. doi:10.1080/17474086.2025.2489562
6. Reddy PS, Locke M, Badawy SM. A systematic review of adherence to iron chelation therapy among children and adolescents with thalassemia. Ann Med. 2022;54:326–342. doi:10.1080/07853890.2022.2028894
7. Mohamed YA, Bashir M, Khanan A, Hakro DN. The feasibility and acceptability of ai-based eguide for healthcare centers in Oman. Information. 2025;16(12):1093. doi:10.3390/info16121093
8. Klaassen R, Bul KCM, den Akker R, van der Burg GJ, Kato PM, Di Bitonto P. Design and evaluation of a pervasive coaching and gamification platform for young diabetes patients. Sensors. 2018;18(2):402. doi:10.3390/s18020402
9. Rhamelani P, Rakhmawati W, Fitri SYR, Mujar NMM. Factors associated with parental involvement in efforts to prevent drug-resistant tuberculosis in children: a scoping review. Infect Drug Resist. 2026;Volume 19:1–21. doi:10.2147/IDR.S573094
10. Rhamelani P, Rakhmawati W. Implementation and strategy in developmental care practice in infants with congenital heart disease in intensive care unit: scoping review. J Multidiscip Healthc. 2025;18:2901–2919. doi:10.2147/JMDH.S516216
11. Ali M, Ali S, Abbas Q, Abbas Z, Lee SW. Artificial intelligence for mental health: a narrative review of applications, challenges, and future directions in digital health. Digit Health. 2025;11:20552076251395548
12. Berdiyarova S, Rakhmatova M, Uzbekova N, et al. Digital therapeutics and gamified mobile applications for behavioral modification in pediatric hypertension. Revista Latinoamericana de Hipertension. 2026;21:66–72.
13. Bocqué C, Wang J, Rickmann A, Julich-Haertel H, Kaempf U, Januschowski K. Gamification to support adherence to a therapeutic ambylopia treatment for children: retrospective study using a focal ambient visual acuity stimulation game. JMIR Pediatr Parent. 2023;6:e32282. doi:10.2196/32282
14. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29:12–16. doi:10.1002/2327-6924.12380
15. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–473. doi:10.7326/M18-0850
16. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
17. Hsia BC, Singh AK, Njeze O, et al. Developing and evaluating ASTHMAXcel adventures: a novel gamified mobile application for pediatric patients with asthma. Ann Allergy Asthma Immunol. 2020;125:581–588. doi:10.1016/j.anai.2020.07.018
18. Poltavski D, Adams RJ, Biberdorf D, Patrie JT. Effectiveness of a novel video game platform in the treatment of pediatric amblyopia. J Pediatr Ophthalmol Strabismus. 2023;61:20–29. doi:10.3928/01913913-20230324-01
19. Atak M, Özyazıcıoğlu N. Effect of computer-based gaming on constipation management in children: a randomized controlled trial. J Pediatr Nurs. 2026;86:223–230. doi:10.1016/j.pedn.2025.11.023
20. Silva-Lavigne N, Valderrama A, Pelaez S, et al. Acceptability of serious games in pediatric asthma education and self-management: pilot study. JMIR Pediatr Parent. 2022;5:e33389. doi:10.2196/33389
21. Calle-Bustos A-M, Juan M-C, García-García I, Abad F. An augmented reality game to support therapeutic education for children with diabetes. PLoS One. 2017;12:e0184645. doi:10.1371/journal.pone.0184645
22. Maneelert O, Wichaikull S. The effects of gamification on health literacy in school-aged children with thalassemia. J Royal Thai Army Nurses. 2024;25:311–318.
23. Mo Y, Chen P, Hou M, et al. Serious games integrating perceptual learning and stereopsis training in children with amblyopia: single-arm pre-post feasibility study. JMIR Serious Games. 2025;13:e77402–e77402. doi:10.2196/77402
24. Liu B, Fan Y, Xu M, Chang F, Shi Y, Liu Z. Effectiveness of a gamified mobile app in enhancing treatment adherence for children with amblyopia: explorative study. JMIR Serious Games. 2025;13:e60309–e60309. doi:10.2196/60309
25. Sarasmita MA, Larasanty LPF, Kuo L-N, Cheng K-J, Chen H-Y. A computer-based interactive narrative and a serious game for children with asthma: development and content validity analysis. J Med Internet Res. 2021;23:e28796. doi:10.2196/28796
26. Ahonkhai AA, Pierce LJ, Mbugua S, et al. PEERNaija: a gamified mhealth behavioral intervention to improve adherence to antiretroviral treatment among adolescents and young adults in Nigeria. Front Reproduct Health. 2021;3. doi:10.3389/frph.2021.656507
27. Stutvoet MD, Levelt L, Hrehovcsik MM, et al. Gamification in eHealth for chronic disease self-management in youth: a systematic review. Games Health J. 2024;13:314–331. doi:10.1089/g4h.2023.0111
28. Gkintoni E, Vantaraki F, Skoulidi C, Anastassopoulos P, Vantarakis A. Promoting physical and mental health among children and adolescents via gamification—A conceptual systematic review. Behav Sci. 2024;14:102. doi:10.3390/bs14020102
29. Faizan M, Han C, Lee SW. Policy-driven digital health interventions for health promotion and disease prevention: a systematic review of clinical and environmental outcomes. Healthcare. 2025;13(18):2319. doi:10.3390/healthcare13182319
30. DeSmet A, Thompson D, Baranowski T, Palmeira A, Verloigne M, De Bourdeaudhuij I. Is participatory design associated with the effectiveness of serious digital games for healthy lifestyle promotion? A meta-analysis. J Med Internet Res. 2016;18(4):e94. doi:10.2196/jmir.4444
31. Johnson D, Horton E, Mulcahy R, Foth M. Gamification and serious games within the domain of domestic energy consumption: a systematic review. Renewable Sustainable Energy Rev. 2017;73:249–264. doi:10.1016/j.rser.2017.01.134
32. Tran S, Smith L, El-Den S, Carter S. The use of gamification and incentives in mobile health apps to improve medication adherence: scoping review. JMIR mHealth uHealth. 2022;10(2):e30671. doi:10.2196/30671
33. Brown M, O’Neill N, van Woerden H, Eslambolchilar P, Jones M, John A. Gamification and Adherence to Web-Based Mental Health Interventions: A Systematic Review. JMIR Ment Health; 2016; doi:10.2196/mental.5710
34. Tark R, Metelitsa M, Akkermann K, Saks K, Mikkel S, Haljas K. Usability, Acceptability, Feasibility, and Effectiveness of a Gamified Mobile Health Intervention (Triumf) for Pediatric Patients: Qualitative Study. JMIR Serious Games; 2019; doi:10.2196/13776
35. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psycholog. 2000;55:68. doi:10.1037/0003-066X.55.1.68
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Let Us Talk Treatment: Using a Digital Body Map Tool to Examine Treatment Burden and Coping Strategies Among Young People with a Chronic Condition
van Schelven F, van der Meulen E, Wessels E, Boeije HR
Patient Preference and Adherence 2023, 17:517-529
Published Date: 2 March 2023