Back to Journals » Journal of Inflammation Research » Volume 16
Future Biomarkers for Infection and Inflammation in Rheumatoid Arthritis
Received 22 March 2023
Accepted for publication 2 June 2023
Published 29 June 2023 Volume 2023:16 Pages 2719—2726
DOI https://doi.org/10.2147/JIR.S413579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Shuang Cui, Jie Qian
Department of Rheumatology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, 226001, People’s Republic of China
Correspondence: Jie Qian, Department of Rheumatology, Affiliated Hospital of Nantong University, 20 Xisi Road, Nantong, Jiangsu, 226001, People’s Republic of China, Email [email protected]
Abstract: Rheumatoid arthritis (RA) increases the susceptibility to a variety of infections that are often difficult to diagnose and can be asymptomatic or symptoms are atypical. Usually, this is a great challenge for rheumatologists, because it is difficult to distinguish infection and aseptic inflammation at an early stage. Prompt diagnosis and treatment of bacterial infections in immunosuppressed individuals is critical for clinicians, and early exclusion of infection allows for specific treatment of inflammatory diseases and avoids the unnecessary use of antibiotics. However, for patients with clinically suspected infection, traditional laboratory markers are not specific for bacterial infection and cannot be used to distinguish outbreaks from infections. Therefore, new infection markers that can distinguish infection from underlying disease are urgently needed for clinical practice. Here, we review the novel biomarkers in RA patients with infection. These biomarkers include presepsin, serology and haematology, as well as neutrophils, T cells, and natural killer cells. Meanwhile, we discuss meaningful biomarkers that distinguish infection from inflammation and develop novel biomarkers for clinical applications, allowing clinicians to make better decisions when diagnosing and treating RA.
Keywords: rheumatoid arthritis, infection, biomarker, inflammation, T cell
Introduction
Rheumatoid arthritis (RA) is a systemic immune-related disease caused by the interaction of genetic and environmental factors and is characterized by chronic and progressive joint erosion.1 To date, infection remains a major problem in RA.2 Infections have long been one of the causes of death in RA patients.3 Altered immune function in RA patients may lead to frequent infections. RA-related immune dysfunction may be a direct factor leading to the increased risk of infection in RA patients.4 In addition, the inflammatory markers C-reactive protein (CRP), the erythrocyte sedimentation rate (ESR) and white blood cell (WBC) counts are also elevated in the acute phase of RA.5 It is difficult to distinguish between infection, inflammation and autoimmunity in patients with RA because infection and inflammation can appear very similar. Moreover, it is critical to diagnose and treat bacterial infections in a timely fashion, but this can be a daunting task.6 Microbiological culture is frequently used as the gold standard for diagnosing bacterial infections, but it usually takes 3–7 days to obtain the results, which is time-consuming and has a low positive result. Biomarkers can help doctors consider appropriate diagnosis and treatment in combination with the patient’s symptoms.7 The pathogenesis of RA involves complex interactions between B cells, T cells, antigen-presenting cells, and endothelial cells. Cytokines are also thought to play an important role in causing inflammation, joint destruction, and extra-articular manifestations associated with RA.8 If biomarkers of infection in RA patients can be identified early and applied to clinical guidance and treatment, the abuse of antibiotics may be reduced, and long-term efficacy may be facilitated. Therefore, the role of biomarkers in clinical diagnosis and decision-making is crucial. However, traditional biomarkers have low specificity and sensitivity in diagnosing infection in patients with RA, and specific infection markers are urgently needed. In this review, we discuss these future biomarkers and their potential clinical applications.
Existing Biomarkers in RA with Infection
Procalcitonin (PCT) and CRP
PCT, which is the peptide precursor of the calcitonin hormone, is normally secreted by the C cells in the thyroid and has been described as a useful and reliable marker of systemic bacterial infection in patients with autoimmune disease.9 Infection is the main factor that triggers PCT synthesis. When the body is infected with severe bacterial and fungal infections, the level of PCT in serum starts increasing quickly. The more serious the bacterial infection, the higher the level of PCT.10 However, these increases are not observed in viral infections. PCT production is stimulated by two mechanisms, directly by lipopolysaccharides and bacterial endotoxins, and it can be activated by microbial toxins, tumour necrosis factor (TNF)-α, interleukin (IL)-1, and IL-6.11
CRP is an acute-phase inflammatory protein and a member of the pentraxin protein family. CRP is a short pentraxin that is mostly synthesized in the liver and can be detected in large amounts at sites of infection or inflammation.12 CRP has multiple functions, such as activating complement through the classic pathway and regulating the function of phagocytes.13 CRP is one of the most commonly used markers of infection worldwide and is routinely evaluated as a marker of systemic inflammation in RA.14 CRP binds to immunoglobulin Fc γ receptors (FcgRs) and promotes the production of proinflammatory cytokines, leading to an inflammatory response.15 CRP specificity is low, and it is preferably used in combination with another serum biomarker.
Both PCT and CRP can be used as biomarkers to distinguish inflammation from infection. A serum PCT level ≥ 0.5 ng/mL strongly suggests bacterial infection in patients with RA, and immediate antibiotic therapy is recommended for these patients who show any signs of infection. However, physicians should be aware that even a PCT level < 0.2 ng/mL does not rule out the presence of bacterial infection.16
IL-6
Serum IL-6 levels have moderate diagnostic value in critically ill patients suspected of infection and have potential clinical application value in identifying infection. IL-6 is an important proinflammatory factor in the initial stage of inflammation and induces a variety of cells to synthesize and secrete acute phase proteins. IL-6 promotes the production and activation of neutrophils during infection, B-cell proliferation and differentiation, immunoglobulin production, and T-cell proliferation and differentiation.17 IL-6 plays an important role in the early stages of inflammation and the transition from acute to chronic inflammation. IL-6 is more sensitive and specific than PCT in detecting bacterial infection. In addition, IL-6 and IL-10 have been reported to be biomarkers for systemic infection and sepsis.18 And IL-6 and IL-10 are better than PCT in identifying patients with septic shock during fever. Serum IL-6 levels have been described as a potential biomarker that reflects disease activity in RA, and parvovirus B19 (B19V) infection can also increase blood IL-6 concentrations. Serum IL-6 levels could reflect RA disease activity as a biomarker.19 Elevated IL-6 mRNA levels or elevated serum IL-6 levels can be detected during acute B19V infection, but no follow-up was found. Plasma IL-6 concentrations were significantly increased in B19V-infected RA patients.20 Normal IL-6 levels are low, mononuclear macrophages are activated and the levels of IL-6 increase abnormally when different bacterial infections occur.21 IL-6 has been considered as a marker for different types of severe bacterial infections (SBI), including early-onset neonatal sepsis, febrile neutropenia, and septic shock bacteremia.22 Early elevation of IL-6 in the presence of SBI, is an important advantage of this cytokine compared with other biomarkers.23 IL-6 plays a significant role in inducing CRP and fibrinogen synthesis in the liver during bacterial infection.
Bacterially infected RA patients had significantly elevated levels of Th1/Th2 cytokines, especially IL-6, and IL-10. The study found that the serum levels of IL-6 were significantly higher in patients of the infection group than those in patients of the RA flare without infection group. IL-6 is more sensitive and specific than PCT in detecting bacterial infection. IL-6 had independent predictive value to differentiate bacterial infection from RA inflammation.18
TNF-α
TNF-α plays an important role in the pathophysiology of RA. The expression of serum TNF-α may enhance the inflammatory activity of early RA.23 Therefore, RA patients must be screened for this cytokine to monitor disease activity, which may be useful in patients receiving anti-TNF therapy. TNF-α itself is a potent inducer of other proinflammatory cytokines and chemokines, further enhancing the inflammatory response.24 Disease activity can be monitored by measuring rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP), which are diagnostic markers of RA. However, the levels of these biomarkers lack specificity. There is a growing need to identify new biomarkers to monitor inflammatory activity in RA, and cytokines have potential applications. TNF-α, a host inflammatory marker, is one of the most commonly used biomarkers for assessing tuberculosis treatment response. Compared with traditional sputum microscopy and sputum culture, they provide an advantage. Because these host inflammatory markers are usually acquired from plasma, serum, and/or blood.25 We should further explore the treatment monitoring of tuberculosis through these biomarkers. When a large number of pathogenic bacteria invade, TNF-α, IL-1b, IL-6 will be released excessively. These could be worsening the severity of sepsis. TNF-α has been confirmed as key pro-inflammatory cytokines in sepsis.26
In the RA flare group, the level of TNF-α in the high activity subgroup was much more higher than in the moderate activity subgroup, which may be related to RA disease activity. TNF-α was also increased in the infection group compared with those in the RA flare group, however, the difference did not reach statistical significance. Therefore, it cannot specifically distinguish between inflammation and infection.18
Krebs von den Lungen-6 (KL-6)
Interstitial lung disease (ILD) is a severe fibrotic disease of the lung parenchyma and one of the most common causes of death in patients with RA. Serum KL-6 is a glycoprotein that is mainly present on type II pneumocytes and alveolar macrophages and is frequently elevated in the serum of patients with interstitial pneumonia. In the past decade, KL-6 has been considered a sensitive biomarker for the detection of connective tissue disease-associated interstitial lung disease (CTD-ILD).27 There is increasing evidence that several circulating serological and alveolar biomarkers can reflect the pathological process from early alveolar epithelial cell damage to advanced fibrosis. Mycobacterium avium complex (MAC) infection appears to increase serum KL-6 levels, after treatment of MAC infection, KL-6 levels decrease. It suggests that KL-6 increases due to active MAC infection, rather than by a relapse of RA-ILD.28
Therefore, existing biomarkers, such as PCT, CRP, IL-6, TNF-α, and KL-6, could recognize infection and inflammation in RA. Early identification of infection contributes to early intervention and better prognosis (Table 1).
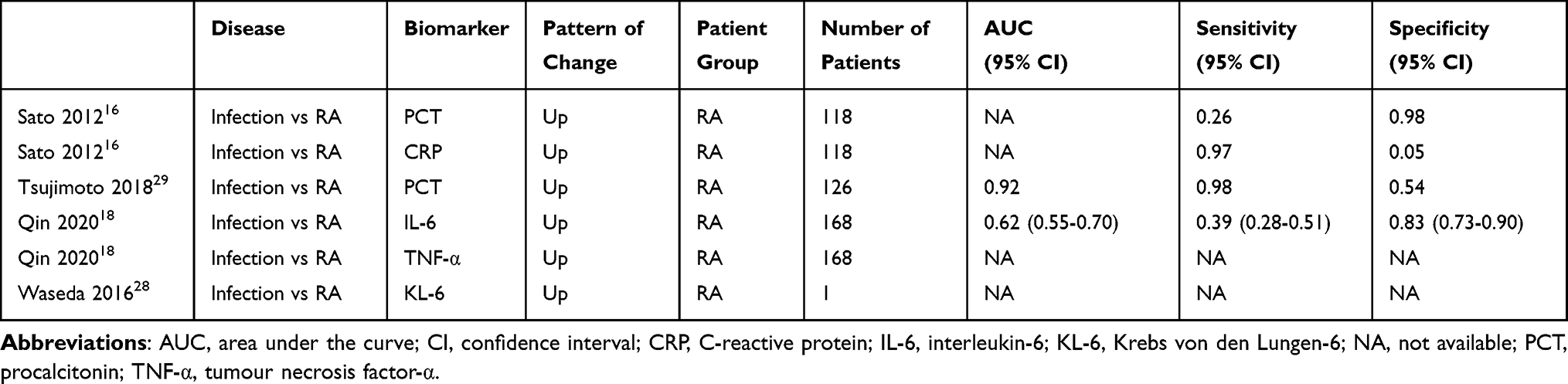 |
Table 1 Characteristics of Existing Diagnostic Biomarkers in RA with Infection |
Novel Biomarkers in RA with Infection
Presepsin
Presepsin is a protein that is particularly elevated in the blood of patients with sepsis. Presepsin is considered a diagnostic and prognostic indicator to assess the severity of sepsis and has been identified as a biomarker for bacterial infections in recent studies.30 Presepsin is the subtype of soluble CD14 (sCD14) and is linked to activation of the immune system. It is released into the bloodstream by monocytes and macrophages to fight bacterial invasion.31 CD14 belongs to the family of Toll-like receptors (TLR), that can identify several Gram-positive and Gram-negative bacterial ligands.32 The bacterial lipopolysaccharide (LPS), requires the association of the lipoprotein binding protein (LBP). The binding between CD14 and LPS-LBP complex leads to the release of cytokines, such as TNF-α, interferon (IFN)-γ, IL-1β, IL-6, and IL-8.33 Serum sCD14 levels are also elevated under inflammatory conditions in RA patients.
Presepsin concentrations have been used to monitor clinical response to treatment. Classifying patients with RA into infected group and noninfected group, the study found that plasma concentrations of presepsin in the infected group were significantly higher than in the noninfected group. Presepsin can be used to distinguish disease activity from infection in patients with RA, even if patients have high RA disease activity. Additionally, PCT and presepsin levels appear to have greater sensitivity in diagnosing bacterial infections than CRP levels or WBC counts. In severe infections, presepsin may be a better indicator of the severity of infection than PCT.29
Serum Amyloid A (SAA) and S100
SAA and S100 (S100A8, S100A9 and S100A12) proteins have previously been highlighted as potential biomarkers of interest in RA. The SAA family consists of 4 subtypes, 2 of which (SAA1 and SAA2) are associated with the acute phase of inflammation. SAA concentrations in RA patients are higher than those in healthy individuals. The level of SAA in synovial fluid was significantly higher than that in the corresponding serum, suggesting local production in the joint.34 SAA1 interacts with Mycobacterium tuberculosis (Mtb), causing up-or down-regulation of Mtb transcriptional response. During infection, Mtb-SAA1 binding can modulate the functional response of the pathogen. Mtb-SAA1 stimulates the infection of host macrophages by Mtb. SAA1 can also bind concentration-dependently to different Gram-negative bacteria such as Escherichia coli, Pseudomonas aeruginosa, Salmonella typhimurium, Vibrio cholerae, Shigella flexneri, and Klebsiella pneumoniae.35 Compared to studies of disease candidate genes, studies of biomarkers have been more successful in identifying and explaining changes in pharmacological responses.36
SAA and S100 are other biomarkers for the diagnosis and monitoring of recurrence of non-infectious febrile disease. SAA plays a pro-inflammatory role in RA and can induce the release of other pro-inflammatory cytokines. Elevated levels of SAA are significantly associated with the degree of RA disease activity. Inflammation and infection cannot be distinguished well.37
Hematologic Abnormalities
Haematologic abnormalities in patients with RA are associated with increased risks of infection, anaemia and lymphopenia, but neutropenia does not increase the risk of common infections in individuals with RA.38 In recent years, the neutrophil to lymphocyte ratio (NLR) has been used as a useful parameter for monitoring disease activity or as a surrogate marker of infection in systemic inflammatory diseases and is recognized as a sensitive inflammatory marker. The NLR and post-NLR/pre-NLR ratios were significantly increased in RA patients who received tocilizumab (TCZ) and developed a bacterial infection, indicating that the post-NLR/pre-NLR ratio may serve as a surrogate predictor of bacterial infection.39 NLR has significantly increased during infection.40 Compared with traditional inflammatory markers, the NLR may be a less expensive and effective marker of inflammation in RA. Its efficacy is comparable to that of CRP, and it is not affected by cytokines that affect CRP and ESR.41
Neutrophil CD64
Neutrophil CD64 is a high affinity receptor for the Fc portion of IgG. Neutrophil CD64 is a member of the immunoglobulin superfamily and is mainly present on the surface of antigen-presenting cells, such as monocytes, macrophages and dendritic cells. During infection or when there is a large amount of bacterial endotoxin, neutrophils are exposed to factors such as LPS, complement molecules, IL-8, IL-12, IFN-γ, TNF-α, and granulocyte colony stimulating factor. These molecules stimulate the expression of CD64 and keep it stable over time.42 The upregulation of neutrophil CD64 is a useful diagnostic marker of infection. Systemic infection and the flare of autoimmune diseases can be distinguished by quantitative measurement of CD64 expression on neutrophils. Quantitative measurements of CD64 can be more easily and rapidly, compared to microbial culture or specimen polymerase chain reaction detection.43 When bacterial infection occurs, neutrophil CD64 can be up-regulated by pro-inflammatory cytokines such as bacterial cell wall lipopolysaccharide, granulocyte-colony stimulating factor, IL-12, and IFN-γ within 4–6 hours.44 Quantitative detection of neutrophil CD64 is effective for detecting different types of infections in RA and can distinguish infection from autoinflammation.45 In recent years, an increasing number of studies on neutrophil CD64 expression have been reported with high sensitivity and specificity, which can be used as a useful early biomarker for the detection of infection and sepsis and can be used as an early indicator to distinguish infected from noninfected patients.46 Although serum CD64 has been shown to have good sensitivity for the diagnosis of systemic infection, the diagnostic value of serum CD64 for local joint infection is limited.47 Systemic infection and the flare of autoimmune diseases can be distinguished by quantitative measurement of CD64 expression on neutrophils. With the simplification and expanded availability of flow cytometry, the neutrophil CD64 index assay may be a useful tool in the clinic.48
In RA patients with infection, CD64 expression is significantly associated with CRP. On the other hand, in RA patients without infection, CD64 expression did not increase even though CRP was elevated due to the high disease activity of RA. Therefore, these results suggest that CD64 expression is not affected by the disease activity of RA. Neutrophils CD64 can distinguish between infection and inflammation. Using CD64 as a marker will allow us to start using effective antibiotics early.45,49
CD4+CD28− T Cells
RA is a systemic autoimmune disease in which CD28null CD4 T cells were first described and extensively studied. The presence of CD28null CD4 T cells positively correlated with the degree of extra-articular manifestations, suggesting that these cells mediate some systemic effects of RA, and CD28null and CD4 T cells are closely related to cytomegalovirus (CMV) infection.50 Over the years, CD4+CD28− T cells have been shown to be associated with various inflammatory conditions, and CD4+CD28− T cells are associated with increased infection and mortality. Furthermore, CD4+CD28− T cells are significantly increased in RA and other autoimmune diseases. Interestingly, the expansion of this subset by more than 1–2% occurred only in CMV-infected individuals. CMV infection alone is known to increase the severity of autoimmune disease, especially RA, and is also associated with increased vascular pathology.51
CD81 T Cells
CD81 T cells in CMV-positive RA patients, which exhibit proinflammatory, cytolytic and antiviral features, are functionally suppressed due to the upregulated expression of leukocyte immunoglobulin-like receptor 1 (LIR-1). Increased LIR-1 expression on CD81 T cells may represent a CMV-induced chronic infection phenotype and is associated with latent CMV infection in healthy individuals.52 Compared with controls, CD19+ lymphocytes had significantly increased CD81 expression associated with human immunodeficiency virus (HIV) or hepatitis C virus (HCV) infection. CD81 upregulation increases the risk of HCV infection, especially in HIV-infected individuals. Furthermore, cytokines released by activated lymphocytes at sites of inflammation may play a role in upregulating CD81 expression.53
The absolute number of CD19+ B cells and CD4+ T cells in the infection group was significantly lower than in patients with the RA flare group. It suggests that a reduced number of CD19+ B cells and CD4+ T cells may make RA patients more susceptible to bacterial infections.18
Natural Killer (NK) Cells
Growing evidence indicates the importance of NK cells, which are lymphocytes of the innate immune system, in autoimmune disease. The best-known role of NK cells is to eliminate virally infected and transformed cells by secreting proinflammatory cytokines. NK cells are present in the synovial fluid of RA patients and are thought to play an important role in bone destruction. Identifying these markers will identify patients with the potential to develop severe disease with irreversible structural damage and allow for appropriate treatment.54
Compared with healthy volunteers, RA patients have a higher percentage of NK cells in peripheral blood. The expression of NK cells could be used as a marker of RA severity. Therefore, elevated NK cells in RA patients may favour inflammation rather than infection.55
Soluble Markers of Antibody-Secreting Cells (ASCs) Functions
Antibodies against infection are produced by ASCs, including plasma cells.56 Abnormal autoantibodies and immunoglobulins suggest B cell and ASC dysfunction. In RA, ASC deficiency may play dual roles in pathogenic autoantibody production and defective responses to infection. Soluble factors associated with B cell and ASC activity are decreased in RA patients, which may be associated with altered antibody production and increase risk of infection.57
Soluble Interleukin-2 Receptor (sIL-2R)
sIL-2R is a marker of T cell activation, and serum sIL-2R levels are elevated in patients with RA and Pneumocystis jirovecii pneumonia (PJP). Serum sIL-2R can be used as a biomarker for the diagnosis of PJP in RA patients treated with methotrexate.58
In general, novel biomarkers, such as presepsin, SAA, haematologic abnormalities, neutrophil CD64, CD4+ T cells, CD81 T cells, NK cells and sIL-2R, could better distinguish systemic infection and inflammation in RA patients. We summarized the characteristics of the novel biomarkers to help early recognition and intervention of infection to improve better prognosis (Table 2).
 |
Table 2 Characteristics of Novel Diagnostic Biomarkers in RA with Infection |
Conclusion
In this review, we summarized future biomarkers, including presepsin, serology and haematology, as well as neutrophils, T cells, and NK cells, which could help us to differentiate between infection and inflammation. It is worth emphasizing that various serious infections are major causes of death in patients with RA. These novel biomarkers have good sensitivity and specificity in differentiating patients with acute autoimmune disease and patients with systemic bacterial infections compared with traditional markers. It can help clinicians identify the different stages of the disease and achieve early intervention. Only through early detection of infection and proper treatment can a better prognosis be achieved.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was funded by grants from China International Medical Foundation (Z-2018-40), Nantong Science and Technology Bureau Project (MSZ18108, JCZ20058 and JCZ2022026) and Special Clinical Basic Research Key Project of Nantong University (2019JZ001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alivernini S, Firestein GS, McInnes IB. The pathogenesis of rheumatoid arthritis. Immunity. 2022;55:2255–2270. doi:10.1016/j.immuni.2022.11.009
2. Avouac J, Amrouche F, Meune C, Rey G, Kahan A, Allanore Y. Mortality profile of patients with rheumatoid arthritis in France and its change in 10 years. Semin Arthritis Rheum. 2017;46:537–543. doi:10.1016/j.semarthrit.2016.10.007
3. Rothe K, Quandt D, Schubert K, et al. Latent cytomegalovirus infection in rheumatoid arthritis and increased frequencies of cytolytic LIR-1+CD8+ T cells. Arthritis Rheumatol. 2016;68:337–346. doi:10.1002/art.39331
4. Atzeni F, Masala IF, Di Franco M, Sarzi-Puttini P. Infections in rheumatoid arthritis. Curr Opin Rheumatol. 2017;29:323–330. doi:10.1097/BOR.0000000000000389
5. Hussein OA, El-Toukhy MA, El-Rahman HS. Neutrophil CD64 expression in inflammatory autoimmune diseases: its value in distinguishing infection from disease flare. Immunol Invest. 2010;39:699–712. doi:10.3109/08820139.2010.491520
6. Ng KJ, Yu HC, Huang Tseng HY, Hsu CW, Lu MC. Modestly elevated serum procalcitonin levels in patients with rheumatoid arthritis free of active infection. Medicina. 2020;56. doi:10.3390/medicina56100545
7. Zandstra J, Jongerius I, Kuijpers TW. Future biomarkers for infection and inflammation in febrile children. Front Immunol. 2021;12:631308. doi:10.3389/fimmu.2021.631308
8. Zaky DS, El-Nahrery EM. Role of interleukin-23 as a biomarker in rheumatoid arthritis patients and its correlation with disease activity. Int Immunopharmacol. 2016;31:105–108. doi:10.1016/j.intimp.2015.12.011
9. Chen Y, Shen J, Yang H, Xu S, Ma Y, Pan F. Serum procalcitonin and C-reactive protein levels as diagnostic markers for distinguishing bacterial infections from lupus flares in systemic lupus erythematosus: a systematic review and meta‑analysis. Int Immunopharmacol. 2021;101:108304. doi:10.1016/j.intimp.2021.108304
10. Li Y, Min L, Zhang X. Usefulness of procalcitonin (PCT), C-reactive protein (CRP), and white blood cell (WBC) levels in the differential diagnosis of acute bacterial, viral, and mycoplasmal respiratory tract infections in children. BMC Pulm Med. 2021;21:386. doi:10.1186/s12890-021-01756-4
11. Yang M, Choi SJ, Lee J, et al. Serum procalcitonin as an independent diagnostic markers of bacteremia in febrile patients with hematologic malignancies. PLoS One. 2019;14:e0225765. doi:10.1371/journal.pone.0225765
12. Stol K, Nijman RG, van Herk W, van Rossum AMC. Biomarkers for infection in children: current clinical practice and future perspectives. Pediatr Infect Dis J. 2019;38:S7–S13. doi:10.1097/INF.0000000000002318
13. Escadafal C, Incardona S, Fernandez-Carballo BL, Dittrich S. The good and the bad: using C reactive protein to distinguish bacterial from non-bacterial infection among febrile patients in low-resource settings. BMJ Global Health. 2020;5. doi:10.1136/bmjgh-2020-002396
14. Marnell L, Mold C, Du Clos TW. C-reactive protein: ligands, receptors and role in inflammation. Clin Immunol. 2005;117:104–111. doi:10.1016/j.clim.2005.08.004
15. Newling M, Sritharan L, van der Ham AJ, et al. C-Reactive protein promotes inflammation through fcgammar-induced glycolytic reprogramming of human macrophages. J Immunol. 2019;203:225–235. doi:10.4049/jimmunol.1900172
16. Sato H, Tanabe N, Murasawa A, et al. Procalcitonin is a specific marker for detecting bacterial infection in patients with rheumatoid arthritis. J Rheumatol. 2012;39:1517–1523. doi:10.3899/jrheum.111601
17. Iwase S, Nakada TA, Hattori N, et al. Interleukin-6 as a diagnostic marker for infection in critically ill patients: a systematic review and meta-analysis. Am J Emerg Med. 2019;37:260–265. doi:10.1016/j.ajem.2018.05.040
18. Qin Y, Feng M, Wu Y, et al. Comprehensive analysis of multiple cytokines and blood parameters for the diagnosis of bacterial infections in rheumatoid arthritis. Cytokine. 2020;136:155251. doi:10.1016/j.cyto.2020.155251
19. Shimamoto K, Ito T, Ozaki Y, et al. Serum interleukin 6 before and after therapy with tocilizumab is a principal biomarker in patients with rheumatoid arthritis. J Rheumatol. 2013;40:1074–1081. doi:10.3899/jrheum.121389
20. Naciute M, Mieliauskaite D, Rugiene R, et al. Frequency and significance of parvovirus B19 infection in patients with rheumatoid arthritis. J Gen Virol. 2016;97:3302–3312. doi:10.1099/jgv.0.000621
21. Gao L, Liu X, Zhang D, et al. Early diagnosis of bacterial infection in patients with septicopyemia by laboratory analysis of PCT, CRP and IL-6. Exp Ther Med. 2017;13:3479–3483. doi:10.3892/etm.2017.4417
22. Slaats J, Ten Oever J, van de Veerdonk FL, Netea MG. IL-1beta/IL-6/CRP and IL-18/ferritin: distinct inflammatory programs in infections. PLoS Pathog. 2016;12:e1005973. doi:10.1371/journal.ppat.1005973
23. Rincon-Lopez EM, Navarro Gomez ML, Hernandez-Sampelayo Matos T, et al. Interleukin 6 as a marker of severe bacterial infection in children with sickle cell disease and fever: a case-control study. BMC Infect Dis. 2021;21:741. doi:10.1186/s12879-021-06470-4
24. Inam Illahi M, Amjad S, Alam SM, Ahmed ST, Fatima M, Shahid MA. Serum tumor necrosis factor-alpha as a competent biomarker for evaluation of disease activity in early rheumatoid arthritis. Cureus. 2021;13:e15314. doi:10.7759/cureus.15314
25. Zimmer A, Lainati F, Aguilera Vasquez N, et al. Biomarkers that correlate with active pulmonary tuberculosis treatment response: a systematic review and meta-analysis. J Clin Microbiol. 2022;60:e0185921. doi:10.1128/jcm.01859-21
26. Li X, Yuan X, Wang C. The clinical value of IL-3, IL-4, IL-12p70, IL17A, IFN-gamma, MIP-1beta, NLR, P-selectin, and TNF-alpha in differentiating bloodstream infections caused by gram-negative, gram-positive bacteria and fungi in hospitalized patients: an observational study. Medicine. 2019;98:e17315. doi:10.1097/MD.0000000000017315
27. Wang Y, Chen S, Zheng S, et al. The role of lung ultrasound B-lines and serum KL-6 in the screening and follow-up of rheumatoid arthritis patients for an identification of interstitial lung disease: review of the literature, proposal for a preliminary algorithm, and clinical application to cases. Arthritis Res Ther. 2021;23:212. doi:10.1186/s13075-021-02586-9
28. Waseda K, Ocho K, Hasegawa K, et al. Increased serum KL-6 levels induced by pulmonary mycobacterium avium complex infection in a patient with RA-associated lung disease. Acta Med Okayama. 2016;70:217–221. doi:10.18926/amo/54422
29. Tsujimoto K, Hata A, Fujita M, Hatachi S, Yagita M. Presepsin and procalcitonin as biomarkers of systemic bacterial infection in patients with rheumatoid arthritis. Int J Rheum Dis. 2018;21:1406–1413. doi:10.1111/1756-185x.12899
30. Bassetti M, Russo A, Righi E, et al. Role of procalcitonin in bacteremic patients and its potential use in predicting infection etiology. Expert Rev Anti Infect Ther. 2019;17:99–105. doi:10.1080/14787210.2019.1562335
31. Maddaloni C, De Rose DU, Santisi A, et al. The emerging role of presepsin (P-SEP) in the diagnosis of sepsis in the critically ill infant: a literature review. Int J Mol Sci. 2021;23:22. doi:10.3390/ijms222212154
32. Memar MY, Baghi HB. Presepsin: a promising biomarker for the detection of bacterial infections. Biomed Pharmacother. 2019;111:649–656. doi:10.1016/j.biopha.2018.12.124
33. Hincu MA, Zonda GI, Stanciu GD, Nemescu D, Paduraru L. Relevance of biomarkers currently in use or research for practical diagnosis approach of neonatal early-onset sepsis. Children. 2020;7. doi:10.3390/children7120309
34. Nys G, Cobraiville G, Servais AC, Malaise MG, de Seny D, Fillet M. Targeted proteomics reveals serum amyloid A variants and alarmins S100A8-S100A9 as key plasma biomarkers of rheumatoid arthritis. Talanta. 2019;204:507–517. doi:10.1016/j.talanta.2019.06.044
35. Kawka M, Brzostek A, Dzitko K, et al. Mycobacterium tuberculosis binds human serum amyloid A, and the interaction modulates the colonization of human macrophages and the transcriptional response of the pathogen. Cells. 2021;11:10. doi:10.3390/cells10051264
36. Puentes-Osorio Y, Amariles P, Calleja MA, Merino V, Diaz-Coronado JC, Taborda D. Potential clinical biomarkers in rheumatoid arthritis with an omic approach. Auto Immun Highlights. 2021;12:9. doi:10.1186/s13317-021-00152-6
37. Zhang Y, Zhang J, Sheng H, Li H, Wang R. Acute phase reactant serum amyloid A in inflammation and other diseases. Adv Clin Chem. 2019;90:25–80. doi:10.1016/bs.acc.2019.01.002
38. Nikiphorou E, de Lusignan S, Mallen C, et al. Haematological abnormalities in new-onset rheumatoid arthritis and risk of common infections: a population-based study. Rheumatology. 2020;59:997–1005. doi:10.1093/rheumatology/kez344
39. Nagai Y, Yokogawa N, Shimada K, Sugii S. Utility of the neutrophil-to-lymphocyte ratio for predicting bacterial infection in patients with rheumatoid arthritis receiving Tocilizumab. Rheumatol Int. 2020;40:2039–2046. doi:10.1007/s00296-020-04705-2
40. Li D, Li J, Zhao C, et al. Diagnostic value of procalcitonin, hypersensitive C-reactive protein and neutrophil-to-lymphocyte ratio for bloodstream infections in pediatric tumor patients. Clin Chem Lab Med. 2023;61:366–376. doi:10.1515/cclm-2022-0801
41. Chandrashekara S, Mukhtar Ahmad M, Renuka P, Anupama KR, Renuka K. Characterization of neutrophil-to-lymphocyte ratio as a measure of inflammation in rheumatoid arthritis. Int J Rheum Dis. 2017;20:1457–1467. doi:10.1111/1756-185x.13157
42. Cong S, Ma T, Di X, Tian C, Zhao M, Wang K. Diagnostic value of neutrophil CD64, procalcitonin, and interleukin-6 in sepsis: a meta-analysis. BMC Infect Dis. 2021;21:384. doi:10.1186/s12879-021-06064-0
43. Hu BQ, Yang Y, Zhao CJ, et al. Accuracy of neutrophil CD64 expression in diagnosing infection in patients with autoimmune diseases: a meta-analysis. Clin Rheumatol. 2019;38:1319–1328. doi:10.1007/s10067-019-04518-0
44. Feng M, Zhang SL, Liang ZJ, et al. Peripheral neutrophil CD64 index combined with complement, CRP, WBC count and B cells improves the ability of diagnosing bacterial infection in SLE. Lupus. 2019;28:304–316. doi:10.1177/0961203319827646
45. Matsui T, Ohsumi K, Ozawa N, et al. CD64 on neutrophils is a sensitive and specific marker for detection of infection in patients with rheumatoid arthritis. J Rheumatol. 2006;33:2416–2424.
46. Gao Y, Lin L, Zhao J, Peng X, Li L. Neutrophil CD64 index as a superior indicator for diagnosing, monitoring bacterial infection, and evaluating antibiotic therapy: a case control study. BMC Infect Dis. 2022;22:892. doi:10.1186/s12879-022-07725-4
47. Qin L, Hu N, Li X, Chen Y, Wang J, Huang W. Evaluation of synovial fluid neutrophil CD64 index as a screening biomarker of prosthetic joint infection. Bone Joint J. 2020;102-B:463–469. doi:10.1302/0301-620x.102b4.Bjj-2019-1271.R1
48. Xiong SD, Pu LF, Wang HP, et al. Neutrophil CD64 Index as a superior biomarker for early diagnosis of infection in febrile patients in the hematology department. Clin Chem Lab Med. 2017;55:82–90. doi:10.1515/cclm-2016-0118
49. Nishino J, Tanaka S, Kadono Y, et al. The usefulness of neutrophil CD64 expression in the diagnosis of local infection in patients with rheumatoid arthritis in daily practice. J Orthop Sci. 2010;15:547–552. doi:10.1007/s00776-010-1498-5
50. Bano A, Pera A, Almoukayed A, et al. CD28 (null) CD4 T-cell expansions in autoimmune disease suggest a link with cytomegalovirus infection. F1000Res. 2019;8:327. doi:10.12688/f1000research.17119.1
51. Broadley I, Pera A, Morrow G, Davies KA, Kern F. Expansions of Cytotoxic CD4(+)CD28(-) T cells drive excess cardiovascular mortality in rheumatoid arthritis and other chronic inflammatory conditions and are triggered by CMV infection. Front Immunol. 2017;8:195. doi:10.3389/fimmu.2017.00195
52. Minichiello E, Semerano L, Boissier MC. Time trends in the incidence, prevalence, and severity of rheumatoid arthritis: a systematic literature review. Joint Bone Spine. 2016;83:625–630. doi:10.1016/j.jbspin.2016.07.007
53. D’Agosto G, Trento E, Nosotti L, et al. CD81 expression on CD19+ peripheral blood lymphocytes is associated with chronic HCV disease and increased risk for HCV infection: a putative role for inflammatory cytokines. J Biol Regul Homeost Agents. 2009;23:155–164.
54. Yamin R, Berhani O, Peleg H, et al. High percentages and activity of synovial fluid NK cells present in patients with advanced stage active rheumatoid arthritis. Sci Rep. 2019;9:9. doi:10.1038/s41598-018-37448-z
55. Lin SJ, Hsu CY, Kuo ML, Lee PT, Hsiao HS, Chen JY. Phenotypic and functional characterization of natural killer cells in rheumatoid arthritis-regulation with interleukin-15. Sci Rep. 2020;10:5858. doi:10.1038/s41598-020-62654-z
56. Nutt SL, Hodgkin PD, Tarlinton DM, Corcoran LM. The generation of antibody-secreting plasma cells. Nat Rev Immunol. 2015;15:160–171. doi:10.1038/nri3795
57. Gutierrez MJ, Desiderio SV, Wang NY, et al. Soluble markers of antibody secreting cell function as predictors of infection risk in rheumatoid arthritis. J Immunol Res. 2019;2019:3658215. doi:10.1155/2019/3658215
58. Sakamoto N, Hara S, Ishimoto H, et al. Serum soluble interleukin-2 receptor is a biomarker for pneumocystis jirovecii pneumonia among patients with rheumatoid arthritis under methotrexate therapy. Tohoku J Exp Med. 2019;248:209–216. doi:10.1620/tjem.248.209
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
AMPK/SIRT1 Deficiency Drives Adjuvant-Induced Arthritis in Rats by Promoting Glycolysis-Mediated Monocytes Inflammatory Polarization
Wang DD, He CY, Wu YJ, Xu L, Shi C, Olatunji OJ, Zuo J, Ji CL
Journal of Inflammation Research 2022, 15:4663-4675
Published Date: 15 August 2022
Theaflavin-3,3’-Digallate Ameliorates Collagen-Induced Arthritis Through Regulation of Autophagy and Macrophage Polarization

Zhang L, Li W, Hou Z, Wang Z, Zhang W, Liang X, Wu Z, Wang T, Liu X, Peng X, Yang X, Yang H, Geng D
Journal of Inflammation Research 2023, 16:109-126
Published Date: 10 January 2023
α-Mangostin Inhibited M1 Polarization of Macrophages/Monocytes in Antigen-Induced Arthritis Mice by Up-Regulating Silent Information Regulator 1 and Peroxisome Proliferators-Activated Receptor γ Simultaneously

Wu YJ, Zhang SS, Yin Q, Lei M, Wang QH, Chen WG, Luo TT, Zhou P, Ji CL
Drug Design, Development and Therapy 2023, 17:563-577
Published Date: 23 February 2023
The Involvement of Glucose and Lipid Metabolism Alteration in Rheumatoid Arthritis and Its Clinical Implication
Luo TT, Wu YJ, Yin Q, Chen WG, Zuo J
Journal of Inflammation Research 2023, 16:1837-1852
Published Date: 26 April 2023
Vitamin K: Infection, Inflammation, and Auto-Immunity
Xie Y, Li S, Wu D, Wang Y, Chen J, Duan L, Li S, Li Y
Journal of Inflammation Research 2024, 17:1147-1160
Published Date: 20 February 2024