Back to Journals » Journal of Pain Research » Volume 18
Fu’s Subcutaneous Needling for Pain: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Gong X ![]() , Wu F, Guo Z, Li N
, Wu F, Guo Z, Li N ![]() , Wang Z, Liu D
, Wang Z, Liu D
Received 20 June 2025
Accepted for publication 18 October 2025
Published 31 October 2025 Volume 2025:18 Pages 5739—5752
DOI https://doi.org/10.2147/JPR.S544998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Xiaogang Gong,1 Fengzhi Wu,2 Zhenyu Guo,2 Na Li,3 Zhiyong Wang,4 Dongming Liu1
1Department of Medicine, College of Special Education, Beijing Union University, Beijing, People’s Republic of China; 2School of Traditional Chinese Medicine, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3School of Acupuncture, Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 4Department of Human Anatomy and Histoembryology, School of Basic Medical Sciences, Peking University, Beijing, People’s Republic of China
Correspondence: Dongming Liu, Department of Medicine, College of Special Education, Beijing Union University, Beijing, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy and safety of Fu’s subcutaneous needling (FSN) for pain management using randomized controlled trials (RCTs), to provide evidence-based guidance for clinical practice and future research.
Methods: A systematic literature search was conducted of PubMed, Embase, Scopus, Cochrane Library, Clinical Trials.gov, and Web of Science databases for RCTs published from inception to May 15, 2025. To be included, studies were required to compare FSN with control interventions for treating pain in adults. Study quality was assessed using the Cochrane Risk of Bias tool, and meta-analysis was performed using RevMan 5.4. Outcomes included pain intensity, and pain-related and functional outcomes.
Results: Eight RCTs (n = 519 participants) were included. Compared with controls, FSN was more effective at reducing pain, with a pooled mean difference (MD) of − 1.14 (95% confidence interval [CI]: − 1.34 to − 0.95; P < 0.001) on the visual analog scale. Subgroup analyses confirmed sustained benefits at the 15-day follow-up (MD = − 1.79; P < 0.001) and 1-month follow-up (MD = − 1.08; P < 0.001) time-points. Secondary outcomes included significant improvements in the Oswestry Disability Index (MD = − 6.10; P < 0.001), range of motion (MD = 9.11; P < 0.001), Lysholm score (standardized MD [SMD] = 0.66; P < 0.001), and 36-Item Short-Form Survey (SMD = 0.78; P < 0.001). Adverse events were mild and transient, with no serious adverse effects reported.
Conclusion: FSN is an effective and safe intervention for pain management, and results in greater pain reduction and functional improvement than other non-pharmacological interventions. Future studies should prioritize multicenter RCTs with standardized protocols, extended follow-up, and diverse populations to confirm the long-term efficacy of FSN for pain management.
Keywords: Fu’s subcutaneous needling, pain management, meta-analysis, systematic review, randomized controlled trial
Introduction
Pain, defined by the International Association for the Study of Pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”,1,2 is an important health problem worldwide. Epidemiological studies suggest that 20–30% of adults worldwide suffer from chronic pain,3 contributing to disability and insomnia, and triggering psychological issues such as anxiety and depression, impairing quality of life and increasing healthcare expenditure.4,5 Addressing the problem of chronic pain necessitates developing safer and more effective pain management strategies, given the limitations of conventional pharmacotherapy including the risk of opioid dependency and inadequate long-term pain relief.3,6 Therefore, clinicians have turned to complementary and alternative medicine as alternative approaches to pain management.7 Traditional acupuncture,8 massage therapy,9,10 and cupping,11,12 have gained increasing support in contemporary pain practice.
Fu’s subcutaneous needling (FSN), developed by Dr Zhonghua Fu in 1996, is a modern acupuncture derivative characterized by its unique mechanical action on subcutaneous connective tissue.13,14 The technique uses a specialized disposable needle housed within a flexible tube, which is inserted horizontally into the subcutaneous layer and manipulated via unidirectional rotations to achieve sustained “sweeping” motions. Distinct from traditional acupuncture, FSN does not use classic meridian points but instead targets myofascial trigger points (MTrPs) within the affected functional units.15 Its proposed mechanism centers on mechanical traction-induced modulation of fascial tension, enhanced local microcirculation, and interruption of nociceptive signaling pathways. Currently, FSN is used in clinical practice for the treatment of various types of musculoskeletal pain, including frozen shoulder, lumbar and dorsal myofascial pain syndrome, knee osteoarthritis, and ankle sprains.16 This focus on musculoskeletal disorders arises from FSN’s therapeutic rationale of targeting pain originating from dysfunction of superficial soft tissues, such as muscles and fascia. As with other acupuncture-based modalities, the therapeutic effects of FSN are likely mediated by a combination of specific physiological mechanisms and non-specific contextual effects. These contextual effects include the treatment ritual, patient-practitioner interaction, and patient expectations, which have been demonstrated to significantly influence outcomes in pain trials.17–19 Therefore, when interpreting the results of randomized controlled trials (RCTs) of FSN, the potential contribution of these factors should be considered in addition to its proposed biomechanical mechanisms.
Despite increasing clinical use and a growing number of RCTs, the evidence base remains fragmented due to methodological heterogeneity, inconsistent outcome reporting, and inadequate reporting of adverse effects. To our knowledge, no comprehensive systematic review or meta-analysis has been conducted to evaluate the efficacy and safety of FSN for treating pain. To provide a methodologically sound assessment of the effectiveness of FSN and minimize bias, this review focused exclusively on synthesizing evidence from RCTs, the gold standard study design for evaluating therapeutic interventions. This systematic review and meta-analysis of RCTs is designed to synthesize the available evidence on the efficacy and safety of FSN for pain management. It aims to provide an evidence base to guide clinical practice, explore the therapeutic benefits of FSN, and identify directions for future research.
Materials and Methods
Study Registration
The design, implementation, and reporting of this study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.20 A completed PRISMA checklist is provided in Supplementary File 1. The review was pre-registered on the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) (registration number: INPLASY202550068).The review was conducted in accordance with the pre-registered protocol without any major deviations.
Search Strategy
We conducted a comprehensive search of six databases, namely PubMed, Embase, Scopus, Cochrane Library, Clinical Trials.gov, and the Web of Science, for articles published from the database inception up to May 15, 2025. The search strategy combined Medical Subject Headings (MeSH) terms with free-text keywords. For example, the PubMed search terms were: “Fu’s subcutaneous needling” [Title/Abstract] OR “Fu’s acupuncture” [Title/Abstract] OR “floating needle” [Title/Abstract] OR “Fu needling” [Title/Abstract] OR “floating-acupuncture” [Title/Abstract] OR “FSN” [Title/Abstract]. The search strategies for each database are provided in Supplementary File 2. Additionally, manual searches were performed to supplement the electronic searches, and the reference lists of all the included articles were screened to identify additional potentially eligible studies.
Inclusion Criteria
The inclusion criteria were defined using the Participants, Interventions, Comparisons, Outcomes, and Study design (PICOS) framework as follows: (1) Participants: aged ≥18 years, clinically diagnosed with pain symptoms, with no restrictions on sex, disease duration, or pain source; (2) Interventions: FSN was the sole or primary intervention; (3) Comparisons: sham FSN therapy, conventional treatment, or other therapeutic approaches; and (4) Outcomes: direct quantitative pain assessments (eg, visual analog scale [VAS], numerical rating scale [NRS]) and/or pain-related outcome measures, such as functional improvement, quality of life (eg, 36-Item Short-Form Survey [SF-36]), safety measurements, and adverse events; and (5) Study design: RCTs.
Exclusion Criteria
The exclusion criteria were: (1) study designs other than RCTs, including non-randomized controlled trials (non-RCTs), review articles, observational studies, case reports, and qualitative research; (2) RCTs evaluating FSN in combination with other therapies, precluding the assessment of the efficacy of FSN alone; and (3) studies with incomplete outcome measures or missing data, preventing valid analysis.
Study Selection and Data Extraction
Two researchers (X.G. and F.W.) independently conducted an initial screening of the articles identified by the literature search based on titles and abstracts, followed by assessing the full text of potentially relevant studies that passed the initial screening according to the predefined inclusion/exclusion criteria. Any disagreements between the two researchers were resolved through discussion or consultation with a third researcher (D.L).
Another two researchers (Z.G. and N.L.) performed data extraction independently using standardized templates. The information extracted included basic study details (first author, publication year, sample size, and participant age range), intervention protocols (FSN therapy specifics such as treatment frequency, duration, and comparative details for the control group), outcome metrics (pain assessment scales, functional improvement, quality-of-life measures), and follow-up data (duration and reported adverse events). For studies with incomplete data, the corresponding author was contacted via Email to request supplementary information. Any discrepancies between the two assessment were resolved through discussion or by consulting a third researcher.
Quality Assessment for Each Eligible Study
Two researchers (X.G. and F.W.) independently assessed the methodological rigor of each of the included studies using the Cochrane Risk of Bias assessment tool. The evaluation focused on seven domains: randomization procedures (selection bias), allocation concealment (selection bias), participant/personnel blinding (performance bias), outcome assessor blinding (detection bias), completeness of outcome data (attrition bias), selective reporting (reporting bias), and other sources of bias. Studies were classified as having low, unclear, or high risk of bias for each criterion. Any discrepancies between the two assessments were resolved through discussion or by consulting a third researcher.
Assessment of the Overall Certainty of the Evidence
The overall certainty of evidence for critical outcomes was assessed using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach. RCTs generally provide high-certainty evidence, but the certainty can be lowered based on five considerations: risk of bias, inconsistency, indirectness, imprecision, and other considerations. Two researchers (X.G. and F.W.) independently rated the certainty for each outcome as high, moderate, low, or very low. Any discrepancies between the two assessments were resolved through discussion or by consulting a third researcher.
Data Synthesis
All statistical analyses were conducted using RevMan 5.4 software,21 and RevMan 5.4 was also used to generate forest plots. For continuous outcomes such as the VAS, range of motion (ROM), and SF-36, either the mean difference (MD) or standardized MD (SMD) and their 95% confidence intervals (CIs) were calculated, depending on the measurement scale. Heterogeneity was assessed using Cochran’s Q statistic and the I² statistic. For the meta-analysis, a fixed-effects model was used if P > 0.05 and I² < 50%, and a random-effects model was used if P < 0.05 and I² > 50%. Subgroup analyses were performed to explore potential sources of heterogeneity if significant heterogeneity was identified.
Results
Literature Search
A total of 459 studies were retrieved from the six databases using the predefined search strategies. After removing duplicates, 146 studies remained. After screening the titles and abstracts, 110 studies were excluded because they did not meet the inclusion criteria. A full-text review was conducted of each of the remaining 36 studies, of which 28 were excluded: 10 non-RCTs, 5 studies with multicomponent interventions, 2 studies lacking objective diagnostic criteria, 3 studies with inappropriate control group interventions, and 8 studies with incomplete data. A detailed list of the 28 excluded studies and the specific reasons for the exclusion of each study is provided in Supplementary File 3. Finally, eight eligible RCTs22–29 were included in the meta-analysis. The study selection process is shown in the PRISMA flowchart (Figure 1).
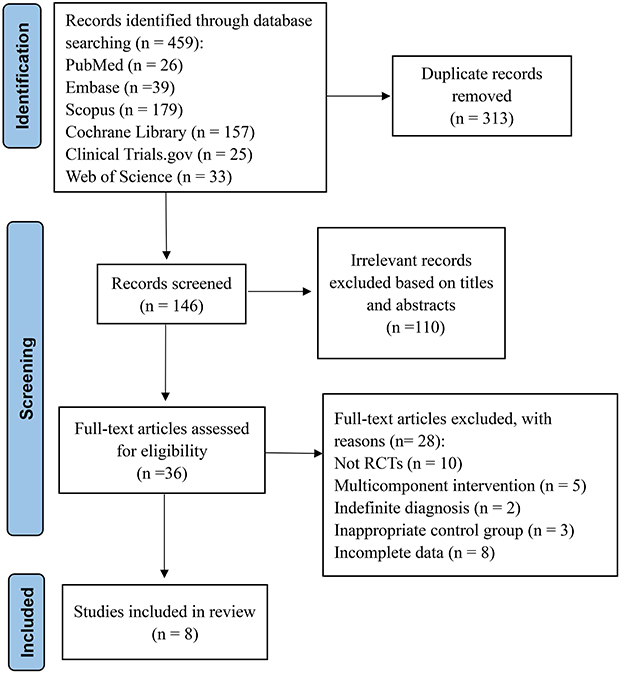 |
Figure 1 Flow chart of study selection. |
Study Characteristics
The studies included in the review and the basic characteristics of the participants are summarized in Table 1. The 8 studies included in the review were published between 2020 and 2025, and all studies were conducted in China. The 8 studies included a total of 519 participants, with 260 in the intervention group and 259 in the control group. The sample size per individual study ranged from 36 to 90. The experimental group received FSN treatment in all studies, with the treatment frequency ranging from 1 to 7 times per week, and a total of 3 to 6 treatment sessions administered over a 2- to 14-day period. The interventions received by the control group included conventional acupuncture (3 studies),24,25,29 electroacupuncture (1 study),27 transcutaneous electrical nerve stimulation (TENS) (2 studies),22,23 Tuina massage (1 study),27 and sham FSN (1 study).28 The outcome indicators included the VAS, Brief Pain Inventory-Total (BPI-T), the Oswestry Disability Index (ODI), ROM, and SF-36. Follow-up data were reported in 7 of the 8 studies,22–24,26–29 with the duration of follow-up ranging from 8 days to 12 months. Adverse events were reported in 5 of the 8 studies.24,26–29
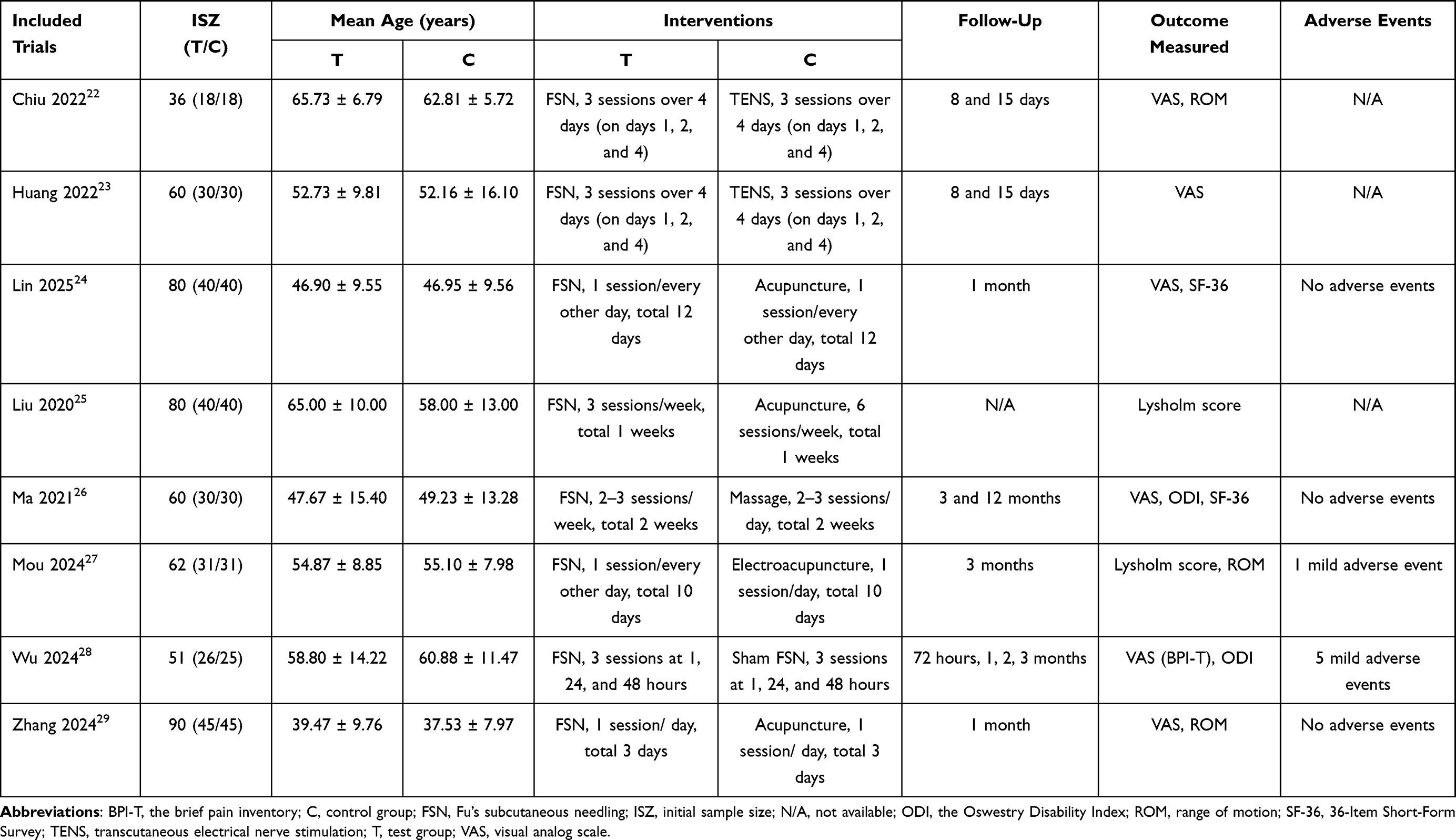 |
Table 1 Characteristics of the Studies Included in the Review |
Methodological Quality
The risk of bias assessment for each study is shown in Figure 2. All 8 studies22–29 used appropriate methods for randomization (eg, random number tables, computer-generated random numbers, stratified randomization). Five of the 8 studies24,26–29 provided detailed methods on randomization concealment (eg, computer-generated random numbers and allocation concealment using opaque sealed envelopes), effectively reducing the risk of bias. The allocation concealment methods in the remaining 3 studies22,23,25 were unclear, potentially introducing a risk of selection bias. Six of the 8 studies22–24,27–29 were reported to use blinding, 1 study26 reported that blinding of clinicians and participants to the intervention assignment was not possible due to the nature of the intervention; and the remaining study25 did not report on whether blinding was used. Six of the 8 studies22,24,26–29 reported blinding of outcome assessors, and the other 2 studies23,25 did not. All 8 studies19–26 reported dropout/attrition rates and handled missing data appropriately and were thus classified as having a low risk of bias for this criterion. All 8 studies22–29 were registered prospectively and reported pre-specified outcomes, with no evidence of selective reporting, and were assessed as having a low risk of reporting bias. None of the studies provided sufficient information to assess other potential sources of bias and were therefore judged to have an “unclear risk of bias.”
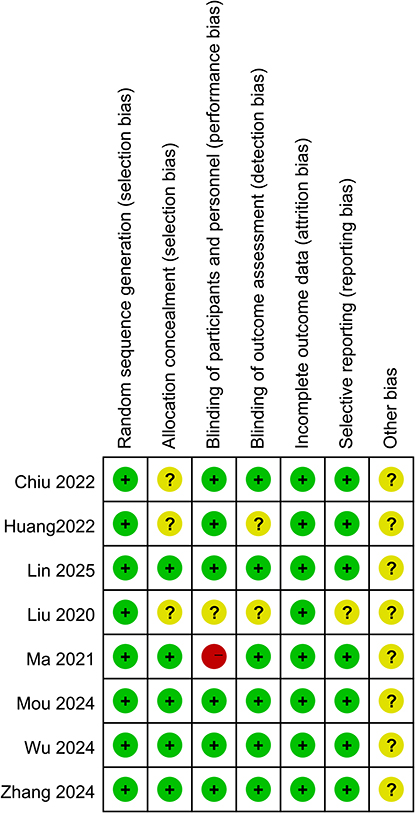 |
Figure 2 Risk of bias summary for the studies included in the review. Symbols: +, low risk of bias; −, high risk of bias;?, unknown risk of bias. |
Meta-Analysis Outcomes
Primary Outcomes (Pain Intensity)
VAS Score
Overall Pain Intensity (VAS)
Six studies22–24,26,28,29 with a total of 362 participants (181 in the experimental group and 181 in the control group), assessed pain using the VAS. The pooled analysis showed that the FSN group had significantly lower VAS pain scores than the control group (MD = −1.14, 95% CI: −1.34 to −0.95; P < 0.001), with no significant heterogeneity (I² = 0%, P = 0.43) (Figure 3).
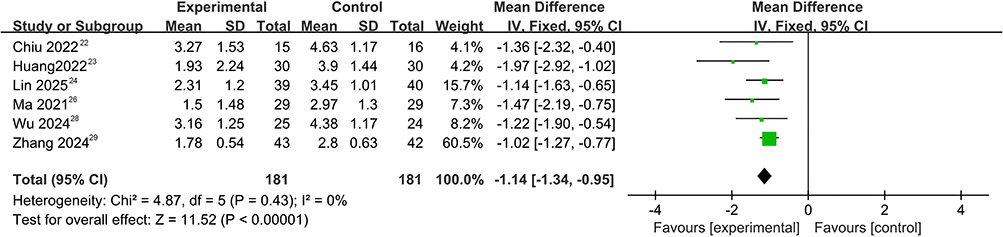 |
Figure 3 Forest plot of the meta-analysis of the effect of Fu’s subcutaneous needling (FSN) on overall pain intensity, measured using the visual analog scale (VAS). |
Pain Intensity (VAS) at Different Time-Points
Pain intensity (VAS) was significantly lower in the FSN group than in the control group at all time-points assessed (Figure 4). Four studies22,23,28,29 with a total of 225 participants assessed the immediate post-intervention effects. The results were pooled using a random-effects model (Figure 4A). The pooled analysis showed substantial reduction in pain intensity in the FSN group (MD = −1.14, 95% CI: −1.68 to −0.60, P < 0.001), with moderate heterogeneity (I² = 56%, P = 0.08). Two studies22,23 with a total of 91 participants assessed the durability of FSN 15 days after completing the intervention. The results were pooled using a fixed-effects model (Figure 4B). The pooled analysis showed substantial reduction in pain intensity in the FSN group (MD = −1.79, 95% CI: −2.37 to −1.20, P <0.001) with no heterogeneity (I² = 0%, P = 0.45). Two studies25,29 with a total of 164 participants assessed the durability of FSN 1 month after completing the intervention. The results were pooled using a fixed-effects model (Figure 4C). The pooled analysis showed a sustained reduction in pain intensity in the FSN group (MD = −1.08, 95% CI: −1.41 to −0.75, P < 0.001) with no heterogeneity (I² = 0%, P > 0.99).
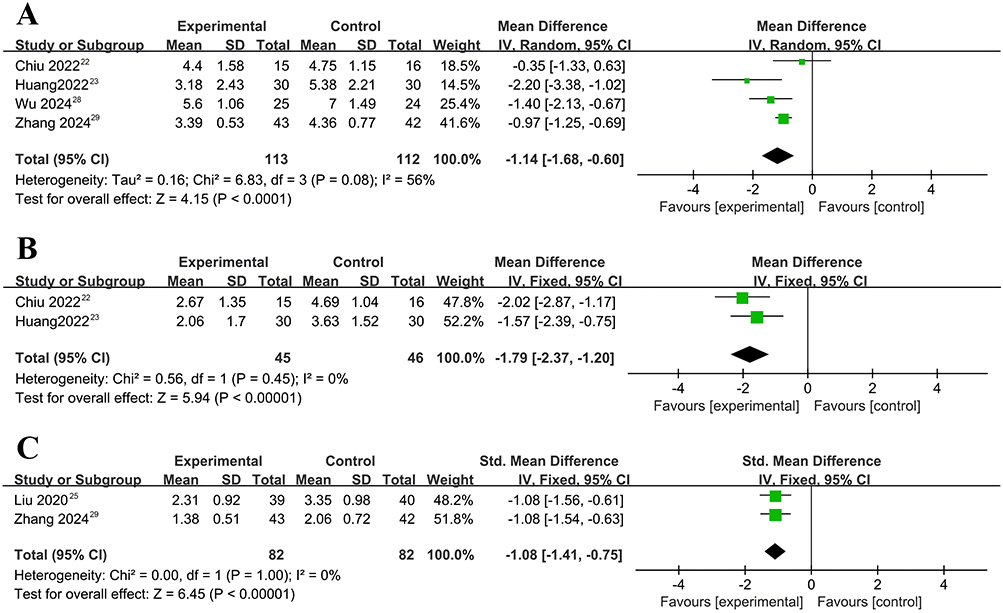 |
Figure 4 Forest plot of the meta-analysis of the effect of Fu’s subcutaneous needling (FSN) on overall pain intensity at different time-points, measured using the visual analog scale (VAS). (A) Effect of FSN on pain intensity immediately after a single session; (B) Effect of FSN on pain intensity 15 days after completing the intervention; (C) Effect of FSN on pain intensity 1 month after completing the intervention. |
Secondary Outcomes (Pain-Related and Functional Outcomes)
Meta-analysis of the effects of FSN on pain-related and functional outcomes revealed significant improvements in multiple measures (Figure 5).
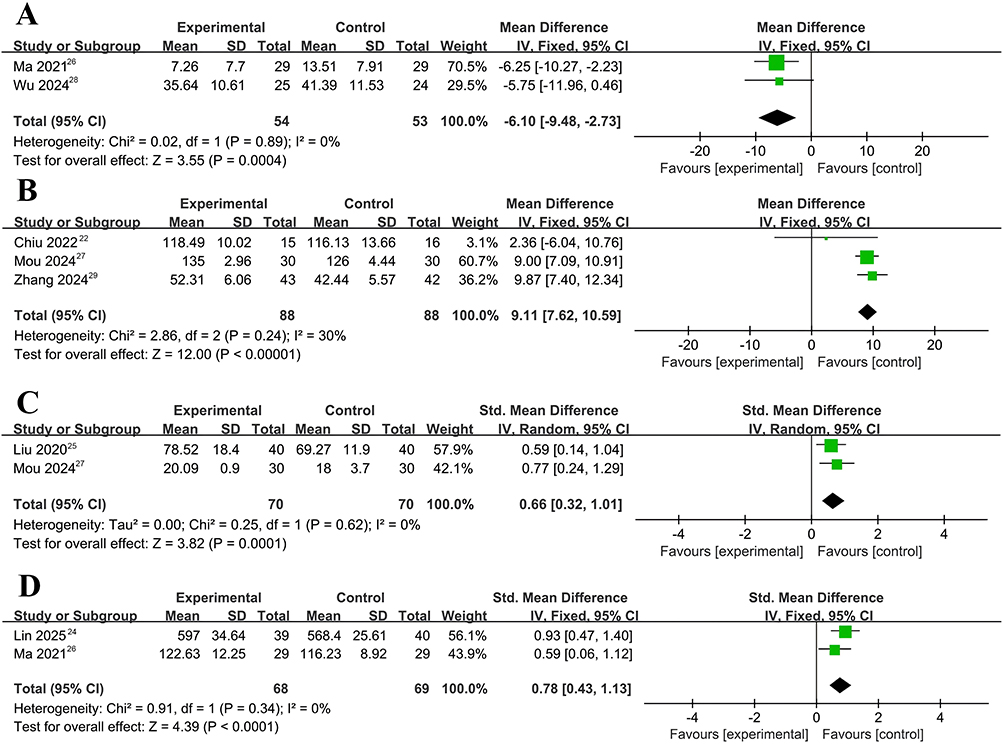 |
Figure 5 Forest plot of the meta-analysis of the effect of Fu’s subcutaneous needling (FSN) on pain-related and functional outcomes. (A) Oswestry Disability Index (ODI); (B) range of motion (ROM); (C) Lysholm score; (D) 36-Item Short-Form Survey (SF-36). |
ODI
Two studies,26,28 with a total of 107 participants, reported on the ODI (Figure 5A). The pooled analysis revealed significantly greater improvement in joint mobility in the FSN group than in the control group (MD = −6.10, 95% CI: −9.48 to −2.73, P < 0.001), with no significant heterogeneity between studies (I² = 0%, P = 0.89).
ROM
Three studies,21,27,29 with a total of 176 participants, reported on the ROM (Figure 5B). The pooled analysis revealed significantly greater improvement in the FSN group than in the control group (MD = 9.11, 95% CI: 7.62 to 10.59; P < 0.001), with no significant heterogeneity between studies (I² = 30%, P = 0.24).
Lysholm Score
Two studies,25,27 with a total of 140 participants, reported Lysholm scores (Figure 5C). The pooled analysis revealed significantly better Lysholm scores (improved knee function and symptoms) in the FSN group than in the control group (SMD = 0.66, 95% CI: 0.32 to 1.01; P < 0.001), with no significant heterogeneity between studies (I² = 0%, P = 0.62).
SF-36
Two studies,24,26 with a total of 137 participants, reported on the SF-36 (Figure 5D). The pooled analysis revealed significantly greater improvement in the quality of life in the FSN group than in the control group (SMD = 0.78, 95% CI: 0.43 to 1.13; P < 0.001), with no significant heterogeneity between studies (I² = 0%, P = 0.34).
Adverse Events
Five of the 8 studies24,26–29 reported adverse events, of which 3 studies24,26,29 reported no adverse events during FSN treatment, and 2 studies27,28 reported minor events: 5 cases of mild subcutaneous hematoma28 (which resolved completely with simple compression during the trial period), and 1 case of pain at the needle site.27 No participants withdrew due to adverse events.
Overall Certainty of the Evidence
The certainty of the evidence for critical outcomes, assessed using the GRADE approach, is summarized in Table 2. The overall certainty of the evidence was moderate for pain reduction and adverse events, and low for the secondary functional outcomes, including ODI, ROM, Lysholm score, and SF-36.
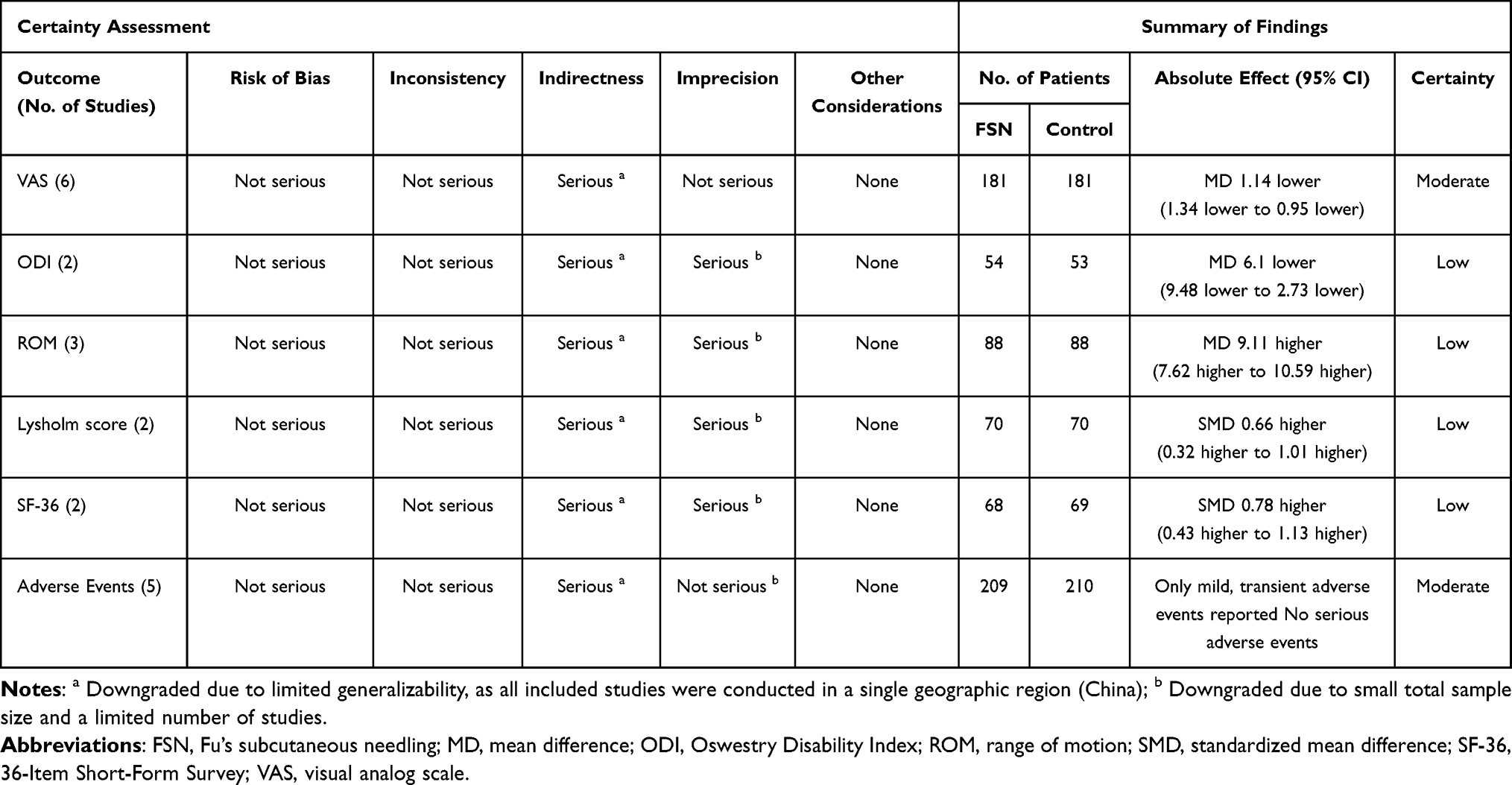 |
Table 2 GRADE Evidence Quality Evaluation Results |
Discussion
Summary of the Main Findings
This systematic review and meta-analysis synthesized data from 8 RCTs with a total of 519 participants to evaluate the comparative efficacy of FSN compared with established therapies, including conventional acupuncture, electroacupuncture, TENS, and massage therapy. The pooled results demonstrate that FSN was more effective at relieving pain than the control interventions. Specifically, FSN significantly reduced pain intensity (VAS) and led to marked improvements in pain-related functional outcomes, including ODI, ROM, knee function and symptoms (Lysholm score), and quality of life (SF-36). Furthermore, the reduction in pain intensity in the FSN group was greater than that in the control group not only immediately after completing treatment but also at the 15-day and 1-month follow-up assessments. According to the GRADE assessment, the certainty of the evidence was moderate for the effect of FSN on pain intensity and adverse events, but low for its effect on the secondary functional outcomes. These findings suggest that FSN is a viable non-pharmacological intervention for pain management and merits consideration for integration into clinical practice.
Comparison with Existing Evidence
FSN is primarily used for treating musculoskeletal disorders, and is used primarily for pain management.13,30 Consequently, both clinical application and research on FSN for pain-related conditions has expanded rapidly, covering over twenty conditions including cervical spondylosis, tennis elbow, frozen shoulder, herpes zoster, lumbar disk herniation (LDH), osteoarthritis (OA), rheumatoid arthritis, gout, headache, primary dysmenorrhea, chronic gastralgia, localized cancer pain, and ankylosing spondylitis.16,31,32 Notably, a case report33 demonstrated significant improvement in phantom limb pain following FSN treatment for a patient with symptoms 10 years after above-the-knee amputation. However, our comprehensive search of major English databases revealed no published systematic reviews and meta-analyses on the efficacy of FSN for pain management covering a diverse range of conditions. One previous meta-analysis34 focused specifically on FSN for LDH. The meta-analysis found that FSN led to greater improvement of the VAS pain score, ODI, SF-36, and Japanese Orthopaedic Association (JOA) scores than those in the control group, consistent with the findings of this study.
Previous research has examined various non-pharmacological interventions for pain, including acupuncture,8 dry needling,35 and physical therapy7,36 and have reported beneficial effects of these interventions. FSN uniquely combines acupuncture and subcutaneous needling,15 and could potentially provide greater immediate and sustained pain relief than alternative non-pharmacological interventions.
Mechanisms of FSN for Pain
Current evidence indicates that the therapeutic mechanism by which FSN reduces pain primarily involves MTrPs.37,38 These points are defined as palpable, hyperirritable nodules within skeletal muscle taut bands, characteristically observed in chronic pain disorders including LDH and OA.39,40 FSN primarily targets muscular regions harboring MTrPs,38 aiming to break the pathological cycle of “aseptic inflammation leading to muscle spasm, which in turn produces pain.” Its core mechanism lies in restoring local blood perfusion.41 By eliminating the abnormal muscle contraction associated with MTrPs, FSN can alleviate compression of blood vessels and nerves, thereby reducing ischemia, hypoxia, and the accumulation of metabolic waste products. This reperfusion effect improves circulation and nutrient supply, promotes tissue repair, and achieves immediate and significant analgesic results at the MTrPs.38
The therapeutic effects of FSN extend beyond vascular changes. Its unique subcutaneous sweeping manipulation provides a mechanical stimulus to connective tissue.42 The needle body compresses and stretches the subcutaneous loose connective tissue at the affected area.30 This may alter the spatial configuration of the loose connective tissue in its liquid crystal state, producing bioelectrical signals by means of a piezoelectric effect. These signals can be efficiently conducted to the lesion site owing to the semiconductor properties of the tissue, triggering an inverse piezoelectric effect.31 This effect modulates ion channels and functions in cell membranes, ultimately improving the local pathological state of the affected muscles and alleviating pain. This manipulation can also stimulate subcutaneous nerve endings, triggering a local neurogenic anti-inflammatory response.43 This manifests as the release of neuropeptides and neurotransmitters, and the recruitment of immune cells, thereby reducing the inflammatory response and diminishing mechanical sensitivity in the affected joints. Furthermore, the results of an animal study44 suggest that FSN may restore mitochondrial function in dysfunctional muscles by enhancing citrate synthase, Complex II, and cytochrome c oxidase (COX-I) expression, improving cellular energy metabolism to support analgesia. Additionally, FSN treatment may also affect the body’s immune system through subcutaneous connective tissue.45
Although existing evidence suggests that FSN has effects on connective tissue, neural modulation, and immune responses, further research is required to determine the biochemical pathways and its long-term effects on inflammation and tissue repair.
Implications for Clinical Practice and Research
The findings of this review suggest that FSN is a viable non-pharmacological option for managing musculoskeletal pain in clinical settings. It may be particularly useful if resources for other interventions are limited and for patients seeking a minimally invasive approach. Future research should address the limitations identified in this study. Additional large-scale multicenter RCTs using standard FSN protocols are required to enhance statistical power and reduce the risk of bias associated with small sample sizes. An international multi-regional collaborative trial network should be established to implement studies in a range of different geographical regions (eg, representative areas such as Europe, North America, and Southeast Asia) to confirm the efficacy of FSN in different populations and expand its global use. Furthermore, long-term follow-up assessments are required to determine the durability of the effects of FSN. Future RCTs should prioritize the use of well-designed placebo control groups (eg, sham FSN devices) to distinguish the specific effects of FSN from its non-specific contextual effects.46 In addition, further in-depth research is needed to determine its mechanisms of action, including the molecular mechanisms through which FSN modulates pain pathways, thus providing a scientific basis for its clinical application.
Strengths and Limitations
To our knowledge, this is the first meta-analysis specifically evaluating the efficacy of FSN in pain management. These findings based on RCTs provide reliable evidence supporting the clinical application of FSN for pain management. Strengths of this study include the use of a comprehensive search strategy, adherence to the PRISMA guidelines, pre-registration of the protocol, and the use of the GRADE approach to assess the certainty of the evidence.
However, this study has several limitations. First, the relatively small sample size limits the strength of the clinical evidence. Although clinical research on FSN has increased in recent years, the number of studies meeting our inclusion criteria was limited. Consequently, only 8 RCTs, with a combined total of 519 participants, were included in the analysis. Second, the comprehensiveness of the data may have been affected by our search strategy, which focused solely on major English-language databases, resulting in the selective inclusion of studies published in English. Third, all included trials were conducted in China. As the evidence is drawn from a single geographic region, the findings may not adequately represent the efficacy of FSN in wider clinical practice or in populations in other settings, thereby restricting the generalizability of the findings. Fourth, significant heterogeneity was observed between studies, despite their overall reasonable quality. This heterogeneity likely arises from differences in methodological quality, diverse underlying pain conditions, variable pain severity levels, differences in FSN treatment parameters (site, frequency, and duration), and differences in the control intervention, all of which may have had an effect on the results. Finally, the duration of follow-up was limited. Of the 8 studies included in the review, only one reported long-term follow-up for a period of 12 months. The remaining 7 studies had follow-up periods ranging from 15 days to 3 months. Based on the available data, we were only able to pool analyses for 15 days and 1 month, and were unable to assess the long-term effects of FSN.
Conclusion
This meta-analysis of RCTs provides a comprehensive assessment of the efficacy and safety of FSN for pain management. The findings demonstrate that FSN is more effective than the control interventions at reducing pain intensity, and that these effects are sustained for at least 1 month. In addition, FSN significantly improves pain-related functional outcomes, including ODI, ROM, the Lysholm score (knee symptoms and function), and SF-36 (quality of life). Only a few mild side effects of FSN were reported, with no serious adverse events. These findings provide evidence that FSN is a safe and effective non-pharmacological option for pain management. However, owing to the small sample sizes and short follow-up periods, the results should be interpreted with caution. Further large-scale, multicenter RCTs are required to investigate the long-term effects of FSN, assess the efficacy of FSN for treating different pain conditions, and standardize the operating procedures to reduce bias.
Abbreviations
BPI-T, Brief Pain Inventory-Total; CI, confidence interval; COX-I, cytochrome c oxidase; FSN, Fu’s subcutaneous needling; GRADE, Grading of Recommendations, Assessment, Development, and Evaluations; INPLASY, International Platform of Registered Systematic Review and Meta-analysis Protocols; LDH, lumbar disk herniation; MD, mean difference; MTrP, myofascial trigger point; NRS, numerical rating scale; OA, osteoarthritis; ODI, Oswestry Disability Index; PICOS, Participants, Interventions, Comparisons, Outcomes, Study design; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial; ROM, range of motion; SF-36, 36-Item Short-Form Survey; SMD, standardized mean difference; TENS, transcutaneous electrical nerve stimulation; VAS, visual analog scale.
Data Sharing Statement
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, including contributing to one or more of the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on its submission to the Journal of Pain Research; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
2. Treede RD. The international association for the study of pain definition of pain: as valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018;3(2):e643. doi:10.1097/PR9.0000000000000643
3. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
4. Aaron RV, Ravyts SG, Carnahan ND, et al. Prevalence of depression and anxiety among adults with chronic pain: a systematic review and meta-analysis. JAMA Network Open. 2025;8(3):e250268. doi:10.1001/jamanetworkopen.2025.0268
5. Rice ASC, Smith BH, Blyth FM. Pain and the global burden of disease. Pain. 2016;157(4):791–796. doi:10.1097/j.pain.0000000000000454
6. Goldberg DS, Mcgee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. doi:10.1186/1471-2458-11-770
7. Wang Y, Aaron R, Attal N, Colloca L. An update on non-pharmacological interventions for pain relief. Cell Rep Med. 2025;6(2):101940. doi:10.1016/j.xcrm.2025.101940
8. Qin C, Ma H, Ni H, et al. Efficacy and safety of acupuncture for pain relief: a systematic review and meta-analysis. Support Care Cancer. 2024;32(12):780. doi:10.1007/s00520-024-08971-9
9. Miake-Lye IM, Mak S, Lee J, et al. Massage for pain: an evidence map. J Altern Complement Med. 2019;25(5):475–502. doi:10.1089/acm.2018.0282
10. Mak S, Allen J, Begashaw M, et al. Use of massage therapy for pain, 2018-2023: a systematic review. JAMA Network Open. 2024;7(7):e2422259. doi:10.1001/jamanetworkopen.2024.22259
11. Choi TY, Ang L, Ku B, Jun JH, Lee MS. Evidence map of cupping therapy. J Clin Med. 2021;10(8):1750. doi:10.3390/jcm10081750
12. Yiying W, Shuai D, Bo LI, Mei H, Huijuan C. Update evidence of effectiveness on pain relieving of cupping therapy: a systematic review and Meta-analysis of randomized controlled trials. J Tradit Chin Med. 2025;45(2):234–253. doi:10.19852/j.cnki.jtcm.2025.02.002
13. Fu ZH. The Foundation of Fu’s Subcutaneous Needling. Beijing: People’s Medical Publishing House; 2016.
14. Fu ZH, Xu JG. A brief introduction to Fu’s subcutaneous needling. Pain Clin. 2005;17(3):343–348. doi:10.1163/1568569054729599
15. Fu ZH, Wu XD, Mearns AB. Under the Skin: A Manual of Fu’s Subcutaneous Needling (FSN) Acupuncture. Beijing: People’s Medical Publishing House; 2021.
16. Fu ZH. The Manual of Fu’s Subcutaneous Needing for Painful Problems. Beijing: People’s Medical Publishing House; 2024.
17. Rossettini G, Campaci F, Bialosky J, Huysmans E, Vase L, Carlino E. The biology of placebo and nocebo effects on experimental and chronic pain: state of the art. J Clin Med. 2023;12(12):4113. doi:10.3390/jcm12124113
18. Rossettini G, Emadi Andani M, Dalla Negra F, Testa M, Tinazzi M, Fiorio M. The placebo effect in the motor domain is differently modulated by the external and internal focus of attention. Sci Rep. 2018;8(1):12296. doi:10.1038/s41598-018-30228-9
19. Ezzatvar Y, Duenas L, Balasch-Bernat M, Lluch-Girbes E, Rossettini G. Which portion of physiotherapy treatments’ effect is not attributable to the specific effects in people with musculoskeletal pain? A meta-analysis of randomized placebo-controlled trials. J Orthop Sports Phys Ther. 2024;54(6):391–399. doi:10.2519/jospt.2024.12126
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(n71). doi:10.1136/bmj.n71
21. Sterne JA, Sutton AJ, Ioannidis JP, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343(d4002):d4002–d4002. doi:10.1136/bmj.d4002
22. Chiu PE, Fu Z, Sun J, Jian GW, Li TM, Chou LW. Efficacy of Fu’s subcutaneous needling in treating soft tissue pain of knee osteoarthritis: a randomized clinical trial. J Clin Med. 2022;11(23):7184. doi:10.3390/jcm11237184
23. Huang CH, Tsai LH, Sun MF, Fu Z, Sun J, Chou LW. Rapid improvement in neck disability, mobility, and sleep quality with chronic neck pain treated by Fu’s subcutaneous needling: a randomized control study. Pain Res Manag. 2022;2022:7592873. doi:10.1155/2022/7592873
24. Lin Y, Hong W, Sui L, et al. Fu’s subcutaneous needling combined with kinematic acupuncture versus electroacupuncture in the treatment of cervical spondylotic radiculopathy: a randomized controlled trial. J Pain Res. 2025;18:1191–1204. doi:10.2147/JPR.S498728
25. Liu Z, Ma L, Bi H. Clinical effect on knee osteoarthritis treated with Fu’s subcutaneous needling therapy. World J Acupunct Moxibustion. 2020;30(1):29–32. doi:10.1016/j.wjam.2020.02.001
26. Ma KL, Zhao P, Cao CF, et al. Fu’s subcutaneous needling versus massage for chronic non-specific low-back pain: a randomized controlled clinical trial. Ann Palliat Med. 2021;10(11):11785–11797. doi:10.21037/apm-21-2986
27. Mou J, Wang Q, Wu J, et al. The effect of Fu’s subcutaneous needling in treating knee osteoarthritis patients: a randomized controlled trial. Explore. 2024;20(4):562–571. doi:10.1016/j.explore.2023.12.015
28. Wu CY, Chou LW, Huang SW, et al. Effects of Fu’s subcutaneous needling on postoperative pain in patients receiving surgery for degenerative lumbar spinal disorders: a single-blind, randomized controlled trial. J Pain Res. 2024;17:2325–2339. doi:10.2147/JPR.S465417
29. Zhang DQ, Fu ZH, Sun J, Song YJ, Chiu PE, Chou LW. Effects of Fu’s subcutaneous needling on clinical efficacy and psychological cognitive characteristics in patients with chronic non-specific low back pain: a randomized controlled trial. Complement Ther Med. 2024;85:103080. doi:10.1016/j.ctim.2024.103080
30. Fu ZH. Essentials of Myology. Beijing: People’s Medical Publishing House; 2023.
31. Xiao AJ, Xia YB, Fu ZH, Guo J, Liang S. Review on the role of Fu’s subcutaneous needling (FSN) in pain relieving. Zhongguo Zhen Jiu. 2013;33(12):1143–1146. doi:10.13703/j.0255-2930.2013.12.030
32. Jia W, Luo L, He LY, et al. Systematic review and analysis on the appropriate diseases in clinical treatment with Fu’s subcutaneous needling therapy. Zhongguo Zhen Jiu. 2019;39(1):111–114. doi:10.13703/j.0255-2930.2019.01.029
33. Huang H, Yu Y, Peng Y, Fu Z. Ten-year phantom limb pain with only four sessions of Fu’s subcutaneous needling: a case report and systematic review. Explore. 2024;20(4):513–519. doi:10.1016/j.explore.2023.11.011
34. Liang J, Zhang J, Zhou J, Yang K, Xiong Q. Study on the safety and efficacy of Fu’s subcutaneous needling for the treatment of lumbar disc herniation: a systematic review and meta analysis of randomized controlled trials. Front Neurol. 2025;16:1509291. doi:10.3389/fneur.2025.1509291
35. Chys M, De Meulemeester K, De Greef I, et al. Clinical effectiveness of dry needling in patients with musculoskeletal Pain-An umbrella review. J Clin Med. 2023;12(3):1205. doi:10.3390/jcm12031205
36. Minor MA, Sanford MK. The role of physical therapy and physical modalities in pain management. Rheum Dis Clin North Am. 1999;25(1):233–248. doi:10.1016/s0889-857x(05)70062-4
37. Li HP, Zhang D, Liu ZX, et al. Effects of Fu’s subcutaneous needling at myofascial trigger points on pain and lumbar mobility in patients with lumbar disc herniation: a randomized controlled trial. Zhen Ci Yan Jiu. 2024;49(5):512–518. doi:10.13702/j.1000-0607.20230167
38. Fu ZH, Wang JH, Sun JH, Chen XY, Xu JG. Fu’s subcutaneous needling: possible clinical evidence of the subcutaneous connective tissue in acupuncture. J Altern Complement Med. 2007;13(1):47–51. doi:10.1089/acm.2006.6125
39. Travell J, Rinzler S, Herman M. Pain and disability of the shoulder and arm: treatment by intramuscular infiltration with procaine hydrochloride. JAMA. 1942;120(6):417–422. doi:10.1001/jama.1942.02830410005002
40. Wheeler AH. Myofascial pain disorders: theory to therapy. Drugs. 2004;64(1):45–62. doi:10.2165/00003495-200464010-00004
41. Fu ZH, Gan XL. New Theory on Qi and Blood. Beijing: People’s Medical Publishing House; 2021.
42. Tao JZ, Fu ZH, Zhang HR. The analysis with mechanism of Fu’s subcutaneous needling. Lishizhen Medicine and Materia Medica Res. 2014;12:3006–3008.
43. Chiu PE, Fu Z, Tsai YC, et al. Fu’s subcutaneous needling promotes axonal regeneration and remyelination by inhibiting inflammation and endoplasmic reticulum stress. Transl Res. 2024;273:46–57. doi:10.1016/j.trsl.2024.06.005
44. Li Y, Gao X, Huang H, Zhou X, Zang Y, Chou LW. Effects of Fu’s subcutaneous needling on mitochondrial structure and function in rats with sciatica. Mol Pain. 2022;18:17448069221108717. doi:10.1177/17448069221108717
45. Xu W, Wu J, Xu P. An immunological hypothesis of Fu’s subcutaneous needling acupuncture. J Acupunct Meridian Stud. 2021;14(3):110–115. doi:10.51507/j.jams.2021.14.3.110
46. Rossettini G, Testa M. Manual therapy RCTs: should we control placebo in placebo control? Eur J Phys Rehabil Med. 2018;54(3):500–501. doi:10.23736/S1973-9087.17.05024-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.