")
Back to Journals » Infection and Drug Resistance » Volume 16
Fungal Spectrum and Susceptibility Against Nine Antifungal Agents in 525 Deep Fungal Infected Cases
Authors Cai W, Ruan Q, Li J, Lin L, Xi L, Sun J, Lu S
Received 30 January 2023
Accepted for publication 30 June 2023
Published 18 July 2023 Volume 2023:16 Pages 4687—4696
DOI https://doi.org/10.2147/IDR.S403863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wenying Cai,1,* Qianqian Ruan,2– 4,* Jiahao Li,1 Li Lin,1 Liyan Xi,1,5 Jiufeng Sun,2,3 Sha Lu1
1Department of Dermatology and Venereology, Sun Yat-sen Memorial Hospital of Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Guangdong Provincial Institute of Public Health, Guangzhou, People’s Republic of China; 3Guangdong Provincial Center for Disease Control and Prevention, Guangzhou, People’s Republic of China; 4School of Public Health, Sun Yat-sen University, Guangzhou, People’s Republic of China; 5Dermatology Hospital, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Sha Lu, Department of Dermatology and Venereology, Sun Yat-sen Memorial Hospital of Sun Yat-Sen University, 107 West Yanjiang Road, Guangzhou, People’s Republic of China, Email [email protected] Jiufeng Sun, Guangdong Provincial Center for Disease Control and Prevention, 160 Qunxian Road, Guangzhou, People’s Republic of China, Email [email protected]
Background: Deep fungal infection has become an important cause of infection and death in hospitalized patients, and this has worsened with increasing antifungal drug resistance.
Objective: A 3-year retrospective study was conducted to investigate the clinical characteristics, pathogen spectrum, and drug resistance of deep fungal infection in a regional hospital of Guangzhou, China.
Methods: Non-duplicate fungi isolates recovered from blood and other sterile body fluids of in-patients of the clinical department were identified using biochemical tests of pure culture with the API20C AUX and CHROMagar medium. Antifungal susceptibilities were determined by Sensititre YeastOne® panel trays.
Results: In this study, 525 patients (283 female, 242 male) with deep fungal infection were included, half of them were elderly patients (≥ 60 years) (54.67%, n=286). A total of 605 non-repetitive fungi were finally isolated from sterile samples, of which urine specimens accounted for 66.12% (n=400). Surgery, ICU, and internal medicine were the top three departments that fungi were frequently detected. The mainly isolated fungal species were Candida albicans (43.97%, n=266), Candida glabrata (20.00%, n=121), and Candida tropicalis (17.02%, n=103), which contributed to over 80% of fungal infection. The susceptibility of the Candida spp. to echinocandins, 5-fluorocytosine, and amphotericin B remained above 95%, while C. glabrata and C. tropicalis to itraconazole were about 95%, and the dose-dependent susceptibility of C. glabrata to fluconazole was more than 90%. The echinocandins had no antifungal activity against Trichosporon asahi in vitro (MIC90> 8 μg/mL), but azole drugs were good, especially voriconazole and itraconazole (MIC90 = 0.25 μg/mL).
Conclusion: The main causative agents of fungal infection were still the genus of Candida. Echinocandins were the first choice for clinical therapy of Candida infection, followed with 5-fluorocytosine and amphotericin B. Azole antifungal agents should be used with caution in Candida glabrata and Candida tropicalis infections.
Keywords: fungal infection, species distribution, antifungal drugs, drug susceptibility, drug resistance
Introduction
Deep fungal infection has become a serious burden of mortality and mobility in clinic with increasing broad-spectrum antifungal drugs (antibiotics, corticosteroids), immunocompromised individuals, and interventional treatment operations.1,2 The diagnosis of invasive fungal infection is based on recovery of fungi by culture of a sample obtained by a sterile procedure from a normally sterile site showing a clinical or radiological abnormality consistent with an infectious disease process.3 The estimated 1.4 million deaths of infectious disease were caused by invasive fungal infection worldwide per year,4,5 including Candida, Aspergillus, Pneumocystis, and Cryptococcus. Among them, Candida species were the most frequent fungal pathogens in clinic, and were ranked fourth among the most common agents of bloodstream infections,6 followed by other common bacterial pathogens. Aspergillus species are the most common microbial infections in hematopoietic stem cell transplant recipients.7 The mortality rate ranged from 30~50% in invasive aspergillosis patients and was ~50% in candidemia.4 Clinical therapy of mycoses lies on the current antifungal interventions, but are often limited due to the emerging resistant clinical isolates.8,9 Poorantifungal activity and universal side effects of antifungal drugs affect the efficacy on clinical therapy of mycoses, thus concerns are growing regarding the increasing antifungal resistance in clinic.
Polyenes, pyrimidine analogs, echinocandins, and triazoles were mainly used to treat invasive fungal infections.10 Triazoles were the most used antifungals. Fluconazole is the major triazole in clinical settings due to its high oral availability and tolerability by patients. In this case, the frequent use of azoles in clinical treatment increased the fungal resistance, making the incidence of emerging antifungal resistance in clinical isolates more and more serious. The trend of infection spectrum may also shift accordingly, eg, the agents of candidemia were changed from Candida albicans to non-C. albicans in clinic.11 These phenomena also occurred in other invasive aspergillosis patients, as well as superficial dermatophytic infections. Therefore, to track the fungal spectrum and the susceptibility against frontline antifungal agents will be the key to understanding the trends of shifts and guide for clinical antifungal therapy.
Clinical sentinel hospital-based surveillance was normally employed to monitor regional trends of fungal infection, and could obtain the antifungal susceptibility data as well. In China, the causative agents of both deep fungal infection and superficial fungal infections vary among geographical areas. The archived survey reported the shifts tendency.12–15 However, in Southern China where a moist and warm environment is sustained for almost 8 months (March to October), fungal infection occurred more frequently than the other regions of China. Indeed, regional mycoses Talaromyces marneffei16 and chromoblastomycosis17 were rarely encountered in the north part of China. Therefore, there are great needs to understand the fungal spectrum and the susceptibility of invasive fungal strains to antifungal drugs. In this study, we addressed the deep fungal infection and drug susceptibility against nine antifungal agents in 605 mycoses through a retrospective study in a sentinel hospital in Guangzhou, China.
Materials and Methods
Clinical Data of Cases
These retrospective data were obtained from clinical records in the mycology laboratory of Sun Yat-sen Memorial Hospital, a general hospital of Sun Yat-sen University in Guangdong, China, from September 2018 to February 2021. Variety specimens were from in-patients of the clinical department in our hospital. Repetitive strains isolated from the same patient were eliminated. This study was approved by the ethics review board of Sun Yat-sen Memorial Hospital, Sun Yat-sen University (SYSKY-2022-496-01) and was conducted in compliance with the Declaration of Helsinki. Informed consent was obtained from all participants. For patients under 18 years of age, informed consent was provided by a parent or legal guardian.
Sampling, Fungi Isolation, and Identification
All isolates were from sterile clinical samples submitted by inpatients in our hospital, including urine, drainage fluid, blood, catheter, bile, hepatic tissue, cerebrospinal fluid, and articular fluid. Urine, cerebrospinal fluid, dialysate, and drainage samples were centrifuged first at 5,000 rpm for 10 min. The precipitated substances were suspended with 0.5 mL saline and transferred onto Sabouraud Dextrose Agar (chloramphenicol included) (BD, MD, USA) with or without cycloheximide, and CHROMagar medium (CHROMagar Technology, Paris, France). Cultures were incubated at 25°C for 2 weeks and examined twice a week. Blood samples were pre-cultured directly with commercial blood culture medium (Bio-engineering, Sichuan, China) at 37°C for 1 week, and transferred onto the same culture medium and cultured under the same conditions. The same fungi isolated from the same type of samples of the same patient during one hospitalization were excluded.
Characterization of fungal pathogens can be done based on morphological, biochemical, and physiological features for most clinical laboratories.18–20 The identification of suspected fungi isolates was based on its macroscopic appearance and the color of the colonies, pigmentation of the medium, and the microscopic morphology, which were mainly used for Aspergillus and Cryptococcus species. Biochemical tests of pure culture using the API20C AUX (bioMerieux Vitek, Hazelwood, MO) and CHROMagar medium (CHROMagar Technology, Paris, France) were used to identify Candida species.
Some of the isolates have also been verified by molecular sequencing using primers targeting the internal transcribed spacer (ITS) regions, ITS4 and ITS5. The result of molecular identification is shown in Supplementary Table 1.
Antifungal Susceptibility Testing
Antifungal susceptibility of nine antifungal drugs was determined by using the Sensititre YeastOne panels trays, which contained serial two-fold dilutions of anidulafungin (0.015–8 μg/mL), micafungin (0.008–8 μg/mL), caspofungin (0.008–8 μg/mL), 5-flucytosine (0.06–64 μg/mL), posaconazole (0.008–8 μg/mL), voriconazole (0.008–8 μg/mL), itraconazole (0.015–16 μg/mL), fluconazole (0.12–256 μg/mL), and amphotericin B (0.12–8 μg/mL) (Thermo Fisher Company, Shanghai, China). A working conidium suspension of approximately 1×104 cells/mL was prepared in YeastOne broth. Each well of the dried YeastOne panels was rehydrated with 100 μL of the working conidium suspension delivered by a multichannel pipetting device, and then incubated at 35°C for 5 days in a non-CO2 incubator. Minimum inhibitory concentration (MIC) values for yeast isolates were determined by the Sensititre YeastOne method and interpreted by species-specific clinical breakpoints (CBPs), as recommended by the CLSI M6021 method. The colorimetric MIC endpoints were determined by visual reading. Fungal growth was evident as a color change from blue (no growth) to red (growth). Colorimetric MIC results for all the testing drugs were defined as the lowest concentration of antifungal agent that prevented the development of a red color from firstly blue or purple. In the light of CBPs, species can be classified as sensitive (S), intermediate (I), or dose-dependent sensitive (SDD), and drug resistant (R). With regard to species for which no CBPs were available from the CLSI we used epidemiological cutoff values (ECVs) to differentiate wild-type (WT) from non-WT (NWT) isolates according to CLSI M5922 method. The quality control strains Candida parapsilosis ATCC 22019 and Candida krusei ATCC 6258 were operated in parallel with the test strains.
Statistical Analysis
All statistical analyses were performed using SPSS software version 24.0 (SPSS Inc., Chicago, IL). The percentage, median of demographical data, distribution of bacteria, and antifungal susceptibility data were calculated, and the counting data were expressed in cases or percentages.
Results
Demographic Information of Cases
From September 2018 to February 2021, a total of 605 sterile clinical samples from 525 in-hospital deep fungal infected cases were collected in Sun Yat-sen Memorial Hospital, including 242 male (46.10%) and 283 female patients (53.90%). Among them, age ranged from 6 to 98 years old, and the median age was 61 years old. In particular, 287 cases were elderly (over 60 years old), accounting for 54.67% of total cases.
Sampling and Fungal Isolation
A total of 3,956 samples of 1,808 deep fungal infected inpatients were sent for examination during the 3 years. There were 605 non-repetitive fungi finally isolated from sterile samples. Of the various types of specimens, over 50% of fungal isolates were recovered from urine (400, 66.12%), followed by drainage fluid (131, 21.65%), blood (40, 6.61%), and catheter (16, 2.64%). In particular, the urine sample is from patients who have not had an indwelling urinary catheter within 7 days before the first positive culture and patients have had at least two positive urine cultures.23 Only two strains were isolated from cerebrospinal fluid and one strain from articular fluid (Figure 1). Regarding the different clinical departments, 605 specimens of 525 cases came from 10 clinical departments, of which the most frequently isolated fungi was from surgery with a total of 236 strains from 226 cases (39.01%), followed by Intensive Care Unit (ICU) with 203 strains from 155 cases (33.55%) and internal medicine with 103 strains from 97 cases (17.02%) (Figure 2).
 |
Figure 1 Distribution of isolated strains in sterile samples. |
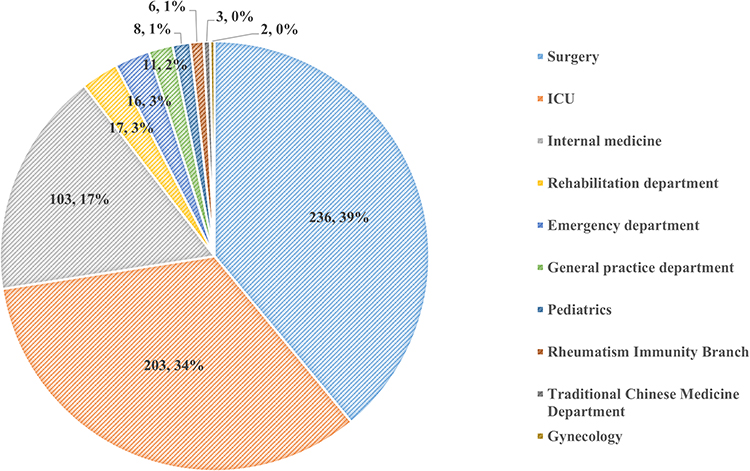 |
Figure 2 Distribution of isolated strains by clinical department. |
Fungal Spectrum Tendency in Variety Clinical Samples and Departments
Among 605 clinical isolates, Candida was the predominant genus (98.18%, n=594) in a variety of clinical samples, followed by Trichosporon asahi (1.65%, n=10), and unique Cryptococcus neoformans isolate. Within the genus of Candida, C. albicans, C. glabrata, and C. tropicalis accounted for 43.97%, 20.00%, and 17.02%, respectively. These three Candida species were ranked on the top three causative agents in 605 deep fungal infection cases (Table 1).
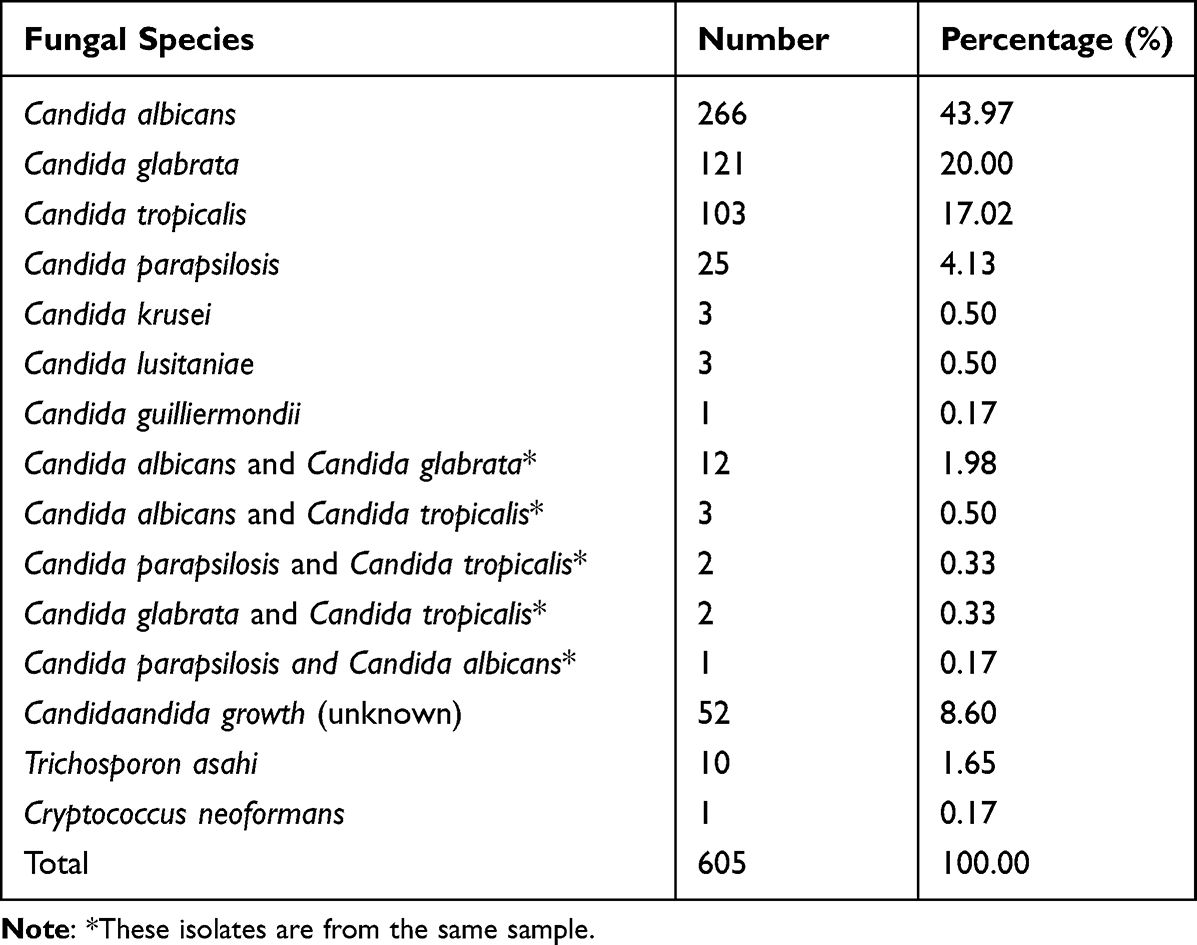 |
Table 1 Fungal Species Distribution of Fungal Isolates |
The fungi isolated from urine were mainly C. albicans (41.50%, n=166), followed by C. glabrata (24.25%, n=97) and C. tropicalis (18.25%, n=73). The distribution of fungi species isolated from drainage fluid (including from the abdominal cavity, pelvic cavity, thoracic cavity, or kidney) was C. albicans (49.62%, n=65), C. tropicalis (17.56%, n=23), and C. glabrata (11.45%, n=15). Moreover, C. albicans was also the major agent of blood samples (n=18, 45%), followed by C. parapsilosis (25%, n=10), C. tropicalis (12.5%, n=5), and C. glabrata (12.5%, n=5) (Table 2).
 |
Table 2 Distribution of Fungal Species According to Clinical Samples |
Regarding the clinical department distribution of fungal isolates, C. albicans accounted for 51.72% of fungal isolates in the ICU, 43.69% in internal medicine, and 37.29% in surgical wards, respectively. We should note that C. glabrata became a more frequent isolated species than C. tropicalis in medical departments (20.39%, n=21 vs 15.53%, n=16) and surgical medicine (29.24%, n=69 vs 15.68%, n=37), while it was the converse in ICU Wards, with C. tropicalis (17.24%, n=35) vs C. glabrata (11.33%, n=23) (Figure 3).
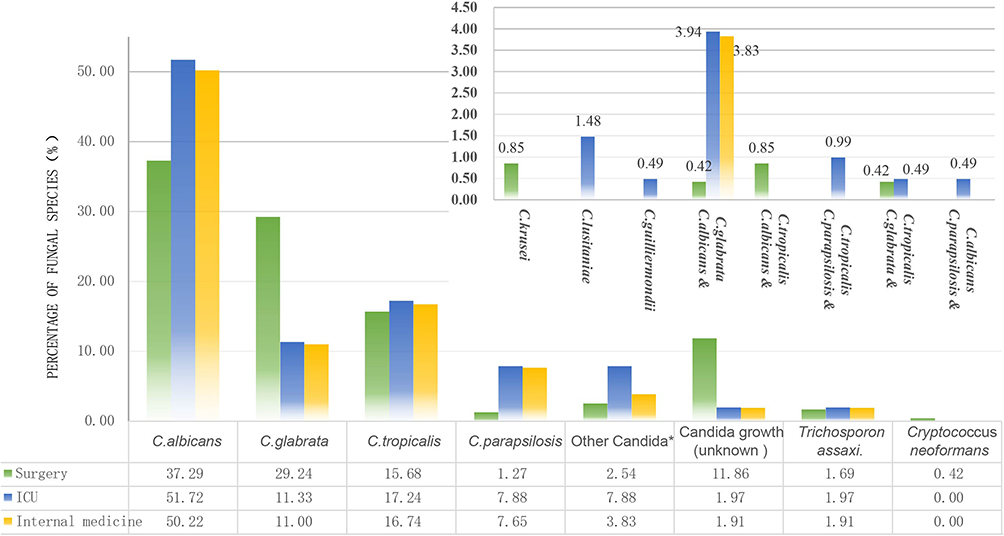 |
Figure 3 Distribution of fungal species according to different wards. The asterisk (*) indicates the species and distribution of other Candida on the top right panel. |
Antifungal Susceptibility
The results of susceptibility testing in vitro of the main Candida isolates against nine frontline antifungal agents are summarized in Table 3. C. albicans, C. glabrata, C. tropicalis, and C. parapsilosis all showed high susceptibility to echinocandin (anidulafungin, micafungin, and caspofungin) and 5-flucytosine (S>95%), while T. asahi was completely resistant to echinocandin drugs. Candida showed variable resistance to azole drugs (voriconazole, itraconazole, fluconazole, posaconazole). C. albicans showed slight resistance to voriconazole and fluconazole (R<5%), followed by posaconazole (R=9.02%), and higher resistance to itraconazole (R=17.67%). On the contrary, C. glabrata and C. tropicalis were more sensitive to itraconazole (S=99.17%/94.17%), among which C. glabrata was highly sensitive to fluconazole in a dose-dependent manner (SDD=90.91%). It is worth noting that the resistance of C. tropicalis to posaconazole was close to 50%. C. parapsilosis was completely sensitive to itraconazole, voriconazole, and posaconazole, but resistant to fluconazole (R=16%). As there is no recommended CBPs of T. asahi for reference presently, the sensitivity and drug resistance cannot be clearly determined. The results showed that echinocandins had no antifungal activity against T. asahi in vitro (MIC90>8 μg/mL). Unlike echinocandins, the antifungal activity of azole drugs was good: MIC90 of voriconazole, itraconazole, fluconazole, and posaconazole were 0.25 μg/mL, 0.25 μg/mL, 8 μg/mL, and 0.25 μg/mL, respectively. MIC90 of amphotericin B and 5-fluorocytosine is 1 μg/mL and 16 μg/mL, respectively (Supplementary Table 2).
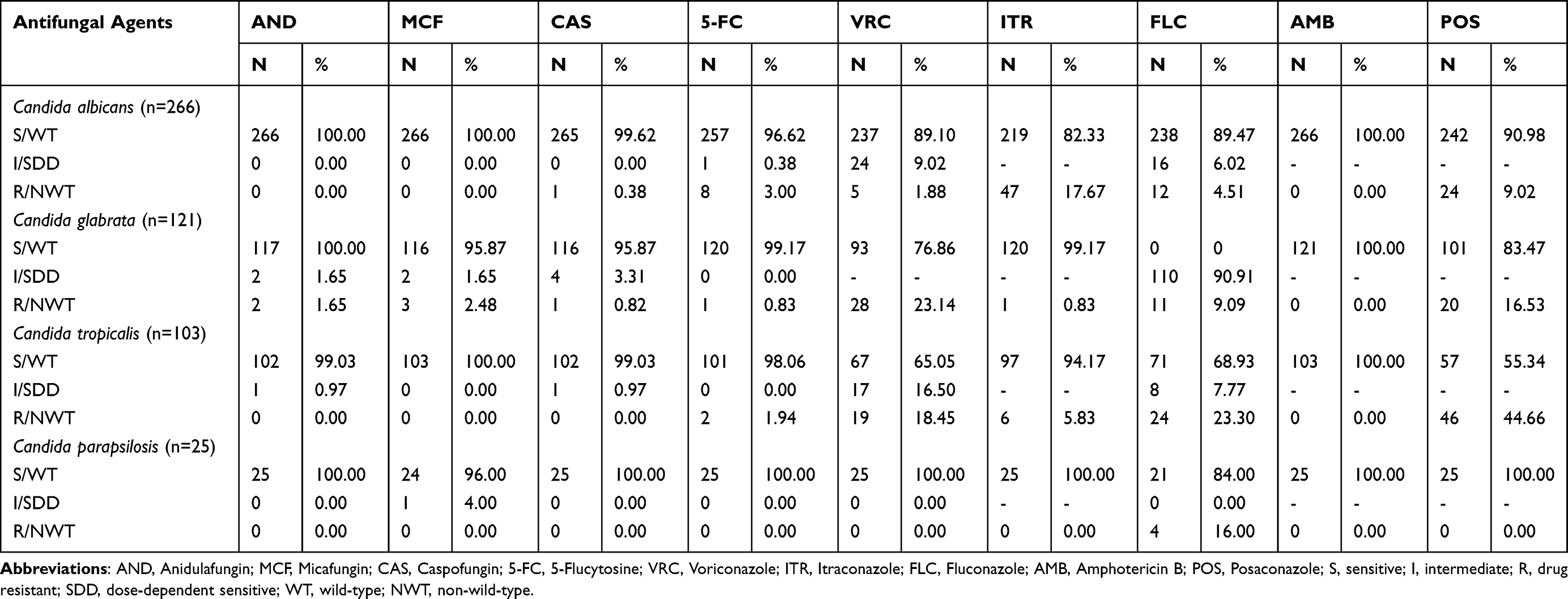 |
Table 3 In vitro Susceptibilities of Fungal Isolates to Eight Antifungal Agents |
Discussion
Isolation of pathogenic fungi from sterile sites is the key for the diagnosis of invasive fungal infections.24 In this study, we determined the fungal spectrum and characteristic resistance to antifungal drugs used in the clinic. Causative agents of fungi were isolated from sterile samples of hospitalized deep fungal infection patients in a general hospital in Guangzhou, China, where a moist and warm environment suits fungal survival and transmission. The results showed that patients mainly came from surgical, ICU, and internal medicine wards, and more than half of them were over 60 years old (54.48%). The high isolation rate of fungi was in surgical and ICU patients, which may link to invasive surgery, long-term hospitalization, and the use of broad-spectrum antibiotics for infection.25 In addition, the large amount of elderly infected patients may be due to the aging of organ function and the decline of immune function, which make them more vulnerable to fungal infection.26,27
Despite the global trend toward decreased frequency of C. albicans and increased frequency of non-C. albicans species,28 the epidemiological survey of fungi in China shows that the genus Candida were still the dominant fungal pathogens, in which the proportion of non-C. albicans and some uncommon Candida were increasing and Aspergillus and Cryptococcus neoformans were also on the rise.29 In our study, C. albicans was the main pathogen of fungal infection, accounting for 43.97% of all Candida species, which is close to the archived data reported by CHIF-NET (44.9%),30 but lower than that in Europe (52.5%).11 In reports in Russia (42.86%),31 France (55.8%),32 Belgium (50.4%),33 and Spain (45.6%),34 C. albicans is also the main pathogen of fungal infections. C. tropicalis and C. glabrata were ranked as the top two non-C. albicans species, of which the tropical region accounts for 17.34% of the total number of Candida, higher than that in the Asia Pacific region (11.7%).35 That is in line with the concept of regional differences in the distribution of C. tropicalis proposed by research of ARTEMI. These results also concur with the prevalence of Candida species causing candidemia in Asia, which recorded C. albicans as the leading (41.3%) isolate causing candidemia.36 However, the prevalence rate of non-C. albicans varies considerably given that they found C. tropicalis (25.4%) and C. glabrata (13.9%) as the main species.37
Echinocandin showed good antifungal activity against Candida, and was recommended as the first choice for the treatment of candidemia in the clinic.38 In our study, all four candida species showed high susceptibility to echinocinoid reagents (anidulafungin, micafungin, and caspofungin). C. albicans and C. parapsilosis were relatively sensitive to azole drugs, which is consistent with the statistical results of domestic CHIF-NET30 and global SENTRY monitoring.39 At present, CLSI has no standard document specifically for the in vitro drug sensitivity test of Trichosporon. The existing operations refer to Candida, and there is no reference standard for the sensitivity judgment break point, so it is unable to calculate the sensitivity rate and other indicators. From the distribution of MIC values in this study, echinocandin has no antifungal activity against T. asahi in vitro, which is consistent with domestic and foreign reports.40,41 The azole drugs showed good antifungal activity in vitro, especially voriconazole and itraconazole. Azole drug plays an important role in the treatment of Trichosporon infection, which was confirmed by Suzuki et al.40
Our research has some limitations. The clinical incidence rate of invasive aspergillosis is increasing yearly.42 We did not observe invasive aspergillosis, thus antifungal drug sensitivity tests of Aspergillus were not determined. As a retrospective study, our data may be affected by the integrity of demographic and laboratory data. In addition, the clinical diagnosis of deep fungal infection was referred to the clinical symptoms and laboratory data (microscopy detection, API20C AUX, and CHROMagar medium), while molecular detection was not carried out.43–45
In conclusion, we addressed the fungal spectrum and characteristics of the resistance to nine antifungal drugs through 525 hospitalized deep fungal infection patients in Guangzhou, China, a hyperepidemic region of fungal infection. The genus Candida was ranked the top deep fungal infection, while Aspergillus and Penicillium were rarely encountered. Instead, we detected appreciable T. asahi infected cases. Echinocandins were the first choice for clinical therapy of Candida infection, followed with 5-fluorocytosine and amphotericin B. Besides, azole antifungal agents should be used with caution in Candida glabrata and Candida tropicalis infections. The data presented in this study may help in the clinical diagnosis and therapy in similar endemic regions of fungal infection in China, as well as neighboring southeast Asia countries, eg, Thailand and Vietnam, which share a similar climate to Guangdong, China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science foundation of China (82172289).
Disclosure
The authors declare no competing interest in this work.
References
1. Bo L. 临床患者深部真菌感染菌群分布情况及耐药性分析 [Bacterial flora distribution and antibiotic resistance analysis for deep fungal infections of clinical patients]. China Modern Med. 2017;24(3):135–137. Chinese.
2. Jenks JD, Cornely OA, Chen SC, Thompson GR, Hoenigl M. Breakthrough invasive fungal infections: who is at risk? Mycoses. 2020;63(10):1021–1032. doi:10.1111/myc.13148
3. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
4. Brown GD, Denning DW, Gow NA, Levitz SM, Netea MG, White TC. Hidden killers: human fungal infections. Sci Transl Med. 2012;4(165):165rv113. doi:10.1126/scitranslmed.3004404
5. Netea MG, Brown GD. Fungal infections: the next challenge. Curr Opin Microbiol. 2012;15(4):403–405. doi:10.1016/j.mib.2012.07.002
6. Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers. 2018;4:18026. doi:10.1038/nrdp.2018.26
7. Rahi MS, Jindal V, Pednekar P, et al. Fungal infections in hematopoietic stem-cell transplant patients: a review of epidemiology, diagnosis, and management. Therap Adv Infect Dis. 2021;8:20499361211039050. doi:10.1177/20499361211039050
8. Perlin DS, Rautemaa-Richardson R, Alastruey-Izquierdo A. The global problem of antifungal resistance: prevalence, mechanisms, and management. Lancet Infect Dis. 2017;17(12):e383–e392. doi:10.1016/S1473-3099(17)30316-X
9. Revie NM, Iyer KR, Robbins N, Cowen LE. Antifungal drug resistance: evolution, mechanisms and impact. Curr Opin Microbiol. 2018;45:70–76. doi:10.1016/j.mib.2018.02.005
10. Mercer DK, O’Neil DA. Innate inspiration: antifungal peptides and other immunotherapeutics from the host immune response. Front Immunol. 2020;11:2177. doi:10.3389/fimmu.2020.02177
11. Pfaller MA, Diekema DJ, Turnidge JD, Castanheira M, Jones RN. Twenty years of the SENTRY antifungal surveillance program: results for candida species from 1997–2016. Open Forum Infect Dis. 2019;6(Suppl 1):S79–s94. doi:10.1093/ofid/ofy358
12. Xiao M, Chen SC, Kong F, et al. Distribution and antifungal susceptibility of candida species causing candidemia in China: an update from the CHIF-NET study. J Infect Dis. 2020;221(Suppl 2):S139–s147. doi:10.1093/infdis/jiz573
13. Bilal H, Shafiq M, Hou B, et al. Distribution and antifungal susceptibility pattern of Candida species from mainland China: a systematic analysis. Virulence. 2022;13(1):1573–1589. doi:10.1080/21505594.2022.2123325
14. Cai W, Lu C, Li X, et al. Epidemiology of superficial fungal infections in Guangdong, Southern China: a retrospective study from 2004 to 2014. Mycopathologia. 2016;181(5–6):387–395. doi:10.1007/s11046-016-9986-6
15. Wang X, Ding C, Xu Y, Yu H, Zhang S, Yang C. Analysis on the pathogenic fungi in patients with superficial mycosis in the Northeastern China during 10 years. Exp Ther Med. 2020;20(6):281. doi:10.3892/etm.2020.9411
16. Hu Y, Zhang J, Li X, et al. Penicillium marneffei infection: an emerging disease in mainland China. Mycopathologia. 2013;175(1–2):57–67. doi:10.1007/s11046-012-9577-0
17. You Z, Yang X, Yu J, Zhang J, Ran Y. Chromoblastomycosis caused by Fonsecaea nubica: first report in Northern China and literature review. Mycopathologia. 2019;184(1):97–105. doi:10.1007/s11046-018-0307-0
18. Cuenca-Estrella M, Bassetti M, Lass-Flörl C, Rácil Z, Richardson M, Rogers TR. Detection and investigation of invasive mould disease. J Antimicrob Chemother. 2011;66(Suppl 1):i15–24. doi:10.1093/jac/dkq438
19. Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA. Manual of Clinical Microbiology. ASM Press; 2015.
20. Larone DH. Medically Important Fungi: A Guide to Identification. ASM Press; 2002.
21. Institute CaLS. Performance Standards for Antifungal Susceptibility Testing of Yeasts. Institute CaLS; 2020.
22. Clinical and Laboratory Standards Institute. Epidemiological Cutoff Values for Antifungal Susceptibility Testing. Clinical and Laboratory Standards Institute; 2020.
23. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
24. Hao-min GD. Distribution and antimicrobial susceptibilities of invasive fungi isolated from sterile sites of inpatients in a hospital of Harbin. J Harbin Med Univ. 2017;24:187.
25. Yang SP, Chen YY, Hsu HS, Wang FD, Chen LY, Fung CP. A risk factor analysis of healthcare-associated fungal infections in an intensive care unit: a retrospective cohort study. BMC Infect Dis. 2013;13:10. doi:10.1186/1471-2334-13-10
26. Scott LJ, Simpson D. Voriconazole: a review of its use in the management of invasive fungal infections. Drugs. 2007;67(2):269–298. doi:10.2165/00003495-200767020-00009
27. Ruiz-Ruigómez M, Dueñas C, Hernandez C, et al. Clinical predictors of candidemia in medical non-neutropenic, non-ICU patients. The CaMed score. Int J Clin Pract. 2018;72(12):e13275. doi:10.1111/ijcp.13275
28. Lamoth F, Lockhart SR, Berkow EL, Calandra T. Changes in the epidemiological landscape of invasive candidiasis. J Antimicrob Chemother. 2018;73(suppl_1):i4–i13. doi:10.1093/jac/dkx444
29. Chen M, Xu Y, Hong N, et al. Epidemiology of fungal infections in China. Front Med. 2018;12(1):58–75. doi:10.1007/s11684-017-0601-0
30. Xiao M, Sun ZY, Kang M, et al. Five-year national surveillance of invasive candidiasis: species distribution and azole susceptibility from the China Hospital Invasive Fungal Surveillance Net (CHIF-NET) study. J Clin Microbiol. 2018;56(7). doi:10.1128/JCM.00577-18
31. Vasilyeva NV, Raush ER, Rudneva MV, et al. Etiology of invasive candidosis agents in Russia: a multicenter epidemiological survey. Front Med. 2018;12(1):84–91. doi:10.1007/s11684-017-0612-x
32. Sasso M, Roger C, Sasso M, et al. Changes in the distribution of colonising and infecting Candida spp. isolates, antifungal drug consumption and susceptibility in a French intensive care unit: a 10-year study. Mycoses. 2017;60(12):770–780. doi:10.1111/myc.12661
33. Trouvé C, Blot S, Hayette MP, et al. Epidemiology and reporting of candidaemia in Belgium: a multi-centre study. Eur J Clin Microbiol Infect Dis. 2017;36(4):649–655. doi:10.1007/s10096-016-2841-3
34. Puig-Asensio M, Padilla B, Garnacho-Montero J, et al. Epidemiology and predictive factors for early and late mortality in Candida bloodstream infections: a population-based surveillance in Spain. Clin Microbiol Infect. 2014;20(4):O245–O254. doi:10.1111/1469-0691.12380
35. Pfaller MA, Diekema DJ, Gibbs DL, et al. Results from the ARTEMIS DISK global antifungal surveillance study, 1997 to 2007: a 10.5-year analysis of susceptibilities of candida species to fluconazole and voriconazole as determined by CLSI standardized disk diffusion. J Clin Microbiol. 2010;48(4):1366–1377. doi:10.1128/JCM.02117-09
36. Tan BH, Chakrabarti A, Li RY, et al. Incidence and species distribution of candidaemia in Asia: a laboratory-based surveillance study. Clin Microbiol Infect. 2015;21(10):946–953. doi:10.1016/j.cmi.2015.06.010
37. Eggimann P, Bille J, Marchetti O. Diagnosis of invasive candidiasis in the ICU. Ann Intensive Care. 2011;1:37. doi:10.1186/2110-5820-1-37
38. Zeng B, Li J, Wang Y, et al. In vitro and in vivo effects of suloctidil on growth and biofilm formation of the opportunistic fungus Candida albicans. Oncotarget. 2017;8(41):69972–69982. doi:10.18632/oncotarget.19542
39. Castanheira M, Messer SA, Rhomberg PR, Pfaller MA. Antifungal susceptibility patterns of a global collection of fungal isolates: results of the SENTRY Antifungal Surveillance Program (2013). Diagn Microbiol Infect Dis. 2016;85(2):200–204. doi:10.1016/j.diagmicrobio.2016.02.009
40. Suzuki K, Nakase K, Kyo T, et al. Fatal Trichosporon fungemia in patients with hematologic malignancies. Eur J Haematol. 2010;84(5):441–447. doi:10.1111/j.1600-0609.2010.01410.x
41. Li-na GU, Shu-ying YU, He WA, Ying-chun XU. Comparative evaluation of Sensititre YeastOne colorimetric panel with broth microdilution methods for antifungal susceptibility testing of Trichosporon asahii isolates. Chin J Mycol. 2017;12:198.
42. Ying LI, Ying-chun XU. Evaluation of ITS, BenA and CaM in identification of clinical aspergillus. Chin J Mycol. 2017;12:74.
43. Ala-Houhala M, Koukila-Kähkölä P, Antikainen J, Valve J, Kirveskari J, Anttila VJ. Clinical use of fungal PCR from deep tissue samples in the diagnosis of invasive fungal diseases: a retrospective observational study. Clin Microbiol Infect. 2018;24(3):301–305. doi:10.1016/j.cmi.2017.08.017
44. García-Salazar E, Acosta-Altamirano G, Betancourt-Cisneros P, et al. Detection and molecular identification of eight candida species in clinical samples by simplex PCR. Microorganisms. 2022;10(2):374. doi:10.3390/microorganisms10020374
45. Liu W, Li M, Xu Y, et al. Evaluation of the performance of a multiplex real-time PCR assay for the identification of aspergillus, Cryptococcus neoformans, and Pneumocystis jirovecii simultaneously from sputum in multicenter. Infect Drug Resist. 2022;15:6009–6017. doi:10.2147/IDR.S379043
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.