Back to Journals » Orthopedic Research and Reviews » Volume 15
Functional Outcomes of Neglected Elbow Dislocation Treated with Double Approach Surgery
Authors Sumarwoto T ![]() , Hadinoto SA, Aprilya D
, Hadinoto SA, Aprilya D ![]() , Bayudono S, Siswanto T
, Bayudono S, Siswanto T
Received 1 May 2023
Accepted for publication 9 August 2023
Published 21 September 2023 Volume 2023:15 Pages 175—181
DOI https://doi.org/10.2147/ORR.S419508
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Tito Sumarwoto,1 Seti Aji Hadinoto,1 Dina Aprilya,2 Sigit Bayudono,3 Totok Siswanto3
1Orthopaedic Upper Limb and Microsurgery Division, Orthopaedic & Traumatology Departement, Prof. DR. R. Soeharso Hospital, Surakarta - Faculty of Medicine Sebelas Maret University, Surakarta, Indonesia; 2Orthopaedic & Traumatology Department, Fatmawati General Hospital, Jakarta, Indonesia; 3Orthopaedic & Traumatology Department, Faculty of Medicine Sebelas Maret University, Surakarta, Indonesia
Correspondence: Tito Sumarwoto, Prof. Dr. R. Soeharso Orthopedic Hospital, Central Java, Indonesia, Email [email protected]
Background: Neglected elbow dislocation is common in developing countries. The chronic nature of the disease results in a level of complexity that makes treatments and outcomes contradictory. Several treatment methods have been described for neglected elbow dislocations. The goal of this study was to evaluate the results of neglected elbow dislocations treated using the double approach of reduction and K-wire fixation.
Methods: This series included patients with neglected elbow dislocations who were treated with open reduction using double approaches (medial and lateral incisions) between November 2020 and March 2021. Patients were evaluated for a minimum of 6 months to ascertain functional recovery in accordance with the Mayo Elbow Performance Index (MEPI) and Disability of Arm, Shoulder, and Hand (DASH) score.
Results: Nine patients with neglected elbow dislocations were included in the study, with an average delay of 3.44 months. Four patients had an excellent MEPI and five had a good score at the final follow-up, with a mean MEPI score of 86.67. The average DASH score was 36 (31– 59). Five patients (55.56%) experienced no pain, but four patients (44.44%) had mild pain, with a range of pain points of 30– 45. The motion arc improvement was 60°– 100°, with a mean of 74.44°. Almost all of the patients (eight patients, 88.89%) had elbow stability, but one patient had ulnar nerve paresthesia postoperatively. Heterotopic ossificans was associated in 1 patient, and triceps lengthening was needed in 1 patient; both came 5 months later.
Conclusion: Open reduction surgery with a double approach offers a good chance of a good result with few side effects and should be considered for all patients who have this condition.
Keywords: elbow, neglected dislocation, open reduction, surgical approach, functional outcome
Introduction
Elbow dislocation is a common orthopedic injury, with an incidence of approximately 20% of all articular dislocations. It is the second most common dislocated large joint in adults after the shoulder. A simple or isolated elbow dislocation was defined as a dislocation without concomitant fracture. Most (80%) elbow dislocations are posterior or posterolateral, resulting from a fall on the outstretched hand with the forearm pronated.1
If the dislocation remained unreduced for over three weeks, the term neglected was preferred. Neglected dislocation of the elbow is quite common, particularly in developing countries, where most cases are first treated by bonesetters.1 In neglected elbow dislocation, elbows are fixed in extension or flexion with only several degrees of flexion, supination, and pronation and have a non-functional range of motion for activities of daily living. Hence, the treatment goal is to restore elbow stability while regaining a satisfactory arc of motion, which is challenging.1,2
In neglected cases, closed reduction hardly achieves concentric and anatomical joint reduction. Open reduction, with or without triceps lengthening and medial-lateral collateral ligament release, is usually done using a single posterior approach, double medial-lateral approaches, or other modified approaches. The methods of joint stabilization vary from the external support of a splint and a hinged external fixator to the invention of an intra-articular “cruciate” ligament. Salvaging procedures may include interpositional arthroplasty before the terminal treatment of arthrodesis or total elbow arthroplasty.1–4 The purpose of this study is to evaluate the outcome following surgical treatment with a double approach for neglected elbow dislocation without concomitant fractures.
Patients and Methods
We reviewed all neglected elbow dislocation patients who underwent surgery using a double approach (lateral-medial approach) between November 2020 and March 2021. Surgical indications included pain, reduced functional range of motion, and stiffness. Cases involving fractures, conservative treatment, or single posterior approach surgery were excluded. Furthermore, patients with acute dislocations, those lost to follow-up, and those who refused surgery or participation were excluded from the study. Informed consent was obtained from the study participants prior to the commencement of the study.
Open reduction under general anesthesia was performed through the lateral and medial approaches of the elbow (Figure 1). A tourniquet cuff was placed proximally on the arm and inflated before the incision. The medial approach was performed by using the humeral medial epicondyle as a landmark. The internervous plane developed proximally between the brachial and triceps muscles and distally between the brachial muscle and pronator teres muscle. The ulnar nerve was then identified and protected. The lateral (posterolateral) approach was performed as described by Kocher, with the lateral humeral condyle as a landmark and the internervous plane lying between the anconeus and extensor carpi ulnaris muscles.5
 |
Figure 1 (A) Medial Approach. The ulnar nerve was tagged. (B) Posterolateral Approach. The blue asterisk indicates the radial head. |
Lateral-medial and posterior capsulotomies were performed, the shortened medial and lateral collateral ligaments were released, and the contracted capsules were opened to access the articular surfaces. All dense fibrous tissue in the olecranon fossa, coronoid fossa, radial head, distal humerus-proximal radius, and ulna should be carefully removed, followed by circumferential capsular release. Joint surfaces were preserved in all patients. The elbow was then reduced, and reduction of the ulnotrochlear and radiocapitellar joints was achieved by manipulation with slow, gentle, progressive maneuvers to avoid sudden movements that could damage the cartilage and nerve. The elbow was flexed maximally to stretch the triceps. Further triceps lengthening by V-Y myoplasty was performed to achieve intraoperative elbow flexion > 100° if the functional flexion range was not achieved merely by joint reduction. V-Y lengthening of the triceps muscle may be performed using the posterolateral approach, as described by Speed.4
Then, a 2.0 mm Kirschner wire was put through the olecranon to the distal humerus with the elbow bent more than 90 degrees. A patient with a diverse dislocation had a radiocapitellar wire put in to prevent the radial head from moving to the side. Hemostasis was ascertained after the removal of the tourniquet. A 3 mm drain was inserted and the wounds were closed in layers. The posterior above-elbow plaster of Paris was adjusted as a back slab for a period of two–three weeks, following which rehabilitation under the observation of the occupational therapist was initiated.
The drain was removed after 48 hours, and the stitches were removed 10–14 days after surgery. Kirschner wires were maintained for 2–3 weeks after surgery and were removed when the elbow’s active range of movement was started. The active ranges of flexion, extension, pronation, and supination were quantified using a goniometer. Postoperative radiographs were obtained to evaluate the surgery.
Patients were assessed for follow-up for at least six months postoperatively in the outpatient clinic and contacted by phone to ascertain functional recovery. Ethical approval was obtained from the institutional ethics committee before beginning the study. Patients were evaluated according to the DASH and MEPI score. This index was used to appraise the subjective, objective, and functional features before and after surgery. This scoring system included four parameters: pain, motion, stability, and function.6 Forty-five points were given for a pain-free elbow, 20 points for normal elbow movement, 10 points for a stable elbow, and 25 points for five activities of daily living. Elbow stability was assessed as stable (no apparent varus/valgus), moderate instability (<10° varus or valgus), or gross instability (10° varus or valgus). Depending on the score, results were assessed as excellent (90–100), good (75–89), fair (60–74), or poor (< 60).7 A follow-up radiograph was also taken at the latest follow-up to evaluate any arthritic changes, heterotrophic ossificans, or non-concentric alignment of the elbow joint.
Result
Nine patients with isolated, neglected elbow dislocations were included in the study. From the data obtained, 5 patients (55.56%) were men and 4 (44.44%) were women, with a mean age of 38 years (range 10–63 years). Two patients (22.22%) had elbow dislocations due to motor vehicle accidents (MVA), and seven patients (77.78%) had dislocations caused by falls. For the affected limb, 6 (66.67%) were right and 3 (33.33%) were left, and the average delay in presentation was 3.44 months. Demographic data are presented in Table 1. Moreover, one patient with a 5-month onset, presented with heterotopic ossificans, as shown in Figure 2.
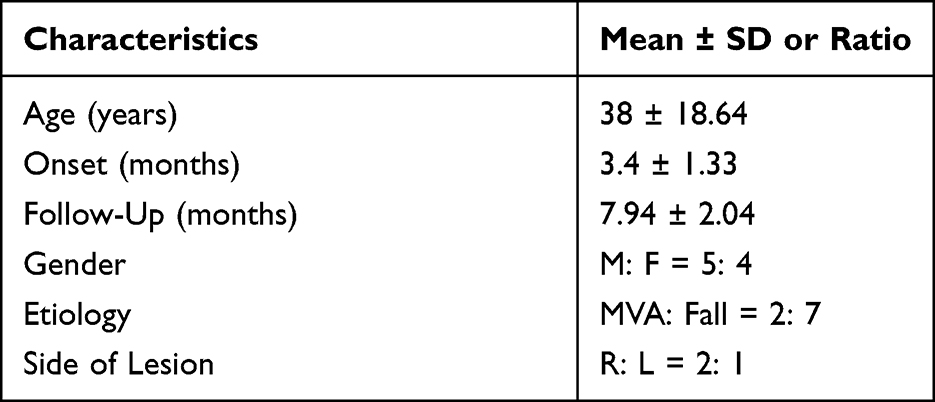 |
Table 1 Patient Characteristics |
 |
Figure 2 (A) Preoperative limited elbow range of motion of a 27-year-old male with 5 months onset of neglected posterior dislocation of the right elbow (B) Anteroposterior and lateral radiographs showed heterotopic ossificans. (C) Improvement arc of the elbow following the surgery by open reduction and V-Y triceps muscle-plasty (D). The A/P and lateral radiographs at the final follow-up. |
Patients were followed up for a minimum of 6 months (range: 6–12 months). The mean drain volume was 40 cc 24 hours after surgery. In six patients (66.67%), the drain was removed on the second postoperative day. The remaining 2 and 1 patients had drain removal on the third and fourth postoperative days, respectively. At the latest follow-up, four patients had an excellent MEPI score, and the rest had a good MEPI score, with an average of 86.67. The average of postoperative DASH score was 36 (31–59). There was no pain in five patients (55.56%), but four patients (44.44%) had mild pain when doing the repetitive motion of the elbow and lifting heavy weight, and the range of pain points was 30–45 (the mean pain score was 38.33). The arc of motion is 70°–110° postoperatively, with a mean of 90°. The motion arc improvement was 70°-100°, with a mean of 76.67°. Almost all of the patients (8 patients/88.89%) had elbow stability, and only 1 patient (11.11%) had moderate instability, even though all of the patients achieved concentric reduction and anatomic alignment of the ulnohumeral and radiocapitellar joints. The patient refused another surgical procedure and was advised to wear the brace for a long time with muscle-strengthening exercises. A summary of functional outcomes is shown in Table 2 and Table 3.
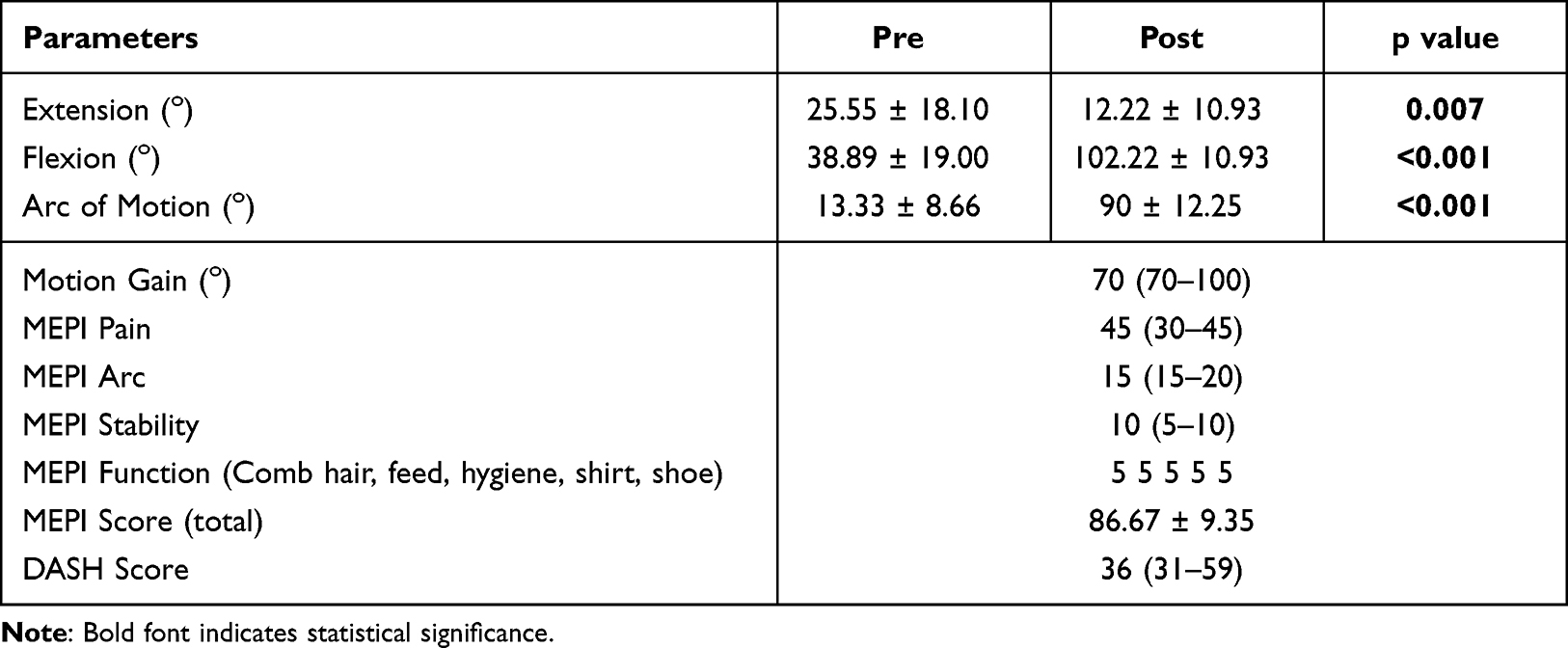 |
Table 2 Functional Outcome of Neglected Elbow Dislocation After Double Approach – Open Reduction |
 |
Table 3 The Correlation of Pre-Operative Conditions with the MEPI Score |
None of the patients had any neurovascular disturbances when they first came to the hospital, but postoperatively, one patient with a 5-month onset had transient ulnar nerve paresthesia, which fully recovered by 10 weeks. This patient underwent triceps V-Y lengthening, in addition to open reduction and capsular release, to achieve better elbow flexion.
Discussion
In our series, falls on the outstretched hand predominated as the mode of injury in the initial trauma. In this position, the elbow was imperfectly extended, and the forearm was naturally pronated to absorb the shock. Hence, force is transmitted to the posterior capsule, causing posterior or posterolateral dislocation of the elbow.1
Neglected dislocation was defined as a dislocation that persisted for more than three weeks after the injury. A delayed presentation of elbow dislocation is common in developing countries. In our series, the patients came after a delay of approximately 3 months. This delay in presentation was caused by initial treatment of the bone setter, poor access to healthcare, or insufficient early management of acute dislocations. Bone setter treatments usually include massage, forcible manipulations, and immobilization in extension, which not only delay the diagnosis and treatment but also create complications such as heterotopic ossificans, ulnar nerve entrapment, and compartment syndrome, along with their sequelae. One patient with a 5-month delay developed heterotrophic ossification. However, none of the patients presented with Volkmann’s ischemic contracture or nerve entrapment syndrome.1,2,6
How does the patient tolerate the associated elbow stiffness and the onset of dislocation as basic indications for surgery?2,6,8–11 Martini et al proposed that elbow flexion of 80°- 90° correlates with functional stiffness. In such cases, surgery should not be performed. In cases where the patient has the ability to achieve a maximum flexion of 80°, despite using the shoulder and hand for compensation, the stiffness makes the arm nonfunctional. Almost all authors recommend surgery only for this group of patients.2,12 In our series, all patients had preoperative elbow flexion less than 80°, which is an indication for surgery.
Surgery has not been recommended in many years. However, following many published studies reporting good outcomes after open reduction, many surgical management procedures are currently being performed. When the dislocation is less than six months old, surgery is more convenient as the tissues (triceps and ligaments) are minimally shortened.12 The average time of neglected dislocation in this study was less than 6 months, so the reduction could still be achieved. However, in one patient with a 5-month onset, additional VY muscle plasty was performed because of the shortened triceps that impeded the functional arch of reduction.
The posterior and lateral approaches are utilized most frequently for open reduction. Surgical treatment for neglected elbow dislocation was first reported by Speed13 who utilized a posterior approach that provides excellent exposure and accommodates adequate release of all contracted tissues. This approach has been in use worldwide for several decades. However, its efficacy has been reported to decline if performed in cases with more than three months of chronicity because of extensive soft tissue fibrosis, degeneration of articular cartilage, and regional osteoporosis.14
The lateral approach proposed by Krishnamoorty15 has the benefit of providing great exposure of the humeroradial joint and the anterior structures, mainly the coronoid fossa. Nevertheless, the posteromedial capsule may not be entrained, and the ulnar nerve may not be observed. The lateral approach is frequently paired with the medial approach. This double approach causes another scar but promotes medial and lateral flaps that permit sufficient debridement and a low possibility of postoperative hematoma while allowing early motion and not infringing the extensor complex. The retracted medial and lateral collateral ligaments were removed, and fibrous tissue was located between the distal humerus and ulna. This approach can also facilitate V-Y triceps plasty and ulnar nerve transposition if necessary.2,4,16
In the management of neglected elbow dislocations, the seemingly contradictory purposes of recovering elbow stability and retrieving an adequate arc of motion are a challenge for senior upper extremity orthopedic surgeons. Some recent procedures have announced great outcomes, such as hinged external fixators.4 However, open reduction and V-Y muscle triceps plasty, as reported by Speed when needed, are still beneficial procedures to obtain a functional elbow.
In this study, all patients showed a significant improvement in elbow range after surgery. These patients retrieve beneficial range of flexion-extension of the elbow following open reduction, regardless of the preoperative conditions, including age, duration of the unreduced dislocation, and preoperative range of motion. Our results for elbow motion at the final follow-up were comparable to those of previous series.
Most activities in daily living may be carried out within a 100° of flexion arc; the condition of this elbow is termed as “useful”.1 Most of the patients in this study achieved a useful elbow and may return to normal daily activities. Only three patients had to modify their activities to perform normal activities, especially the activities that led to the head and center of the body, such as combing, feeding, hygiene, shirting, and wearing a shoe. This overall upper limb function was assessed with a DASH score. Our result is somewhat comparable with the posterior approach only arthrolysis as studied in 14 patients by Nejad et al17 (36 vs 33.7). Another study conducted by Ayadi et al18 also gave similar postoperative DASH result (31.6) regardless of the open surgical approaches used.
The Mayo Clinic Elbow Performance Index (MEPI) is one of the most commonly utilized physician-based elbow rating systems and a beneficial scoring system for these injuries.7,19 This study reported that three patients were excellent and six patients were good in this series of nine patients. This result is similar to other series conducted by Anderson et al8 (mean MEPI of 93 and good or excellent outcomes in 97% of patients), Mehta et al20 (mean MEPI of 89 with 80% of patients having excellent and good results), and Coulibaly et al12 (mean MEPI of 86 with 82% of patients having excellent and good results).
In the correlation analysis, preoperative conditions did not correlate with postoperative stability. However, one patient with a 5-month onset and heterotopic ossificans developed moderate instability after surgery. In this patient, we performed VY tricepsplasty, as advised in previous literature, for the neglected case after 3 months.20 This procedure allowed reduction while decompressing the compromised articular cartilage. The elbow is usually unstable and requires stabilization following triceps splasty with either a transfixing wire or hinged external fixator. In a series, a valgus-varus instability of 33° was reported in patients who underwent tricepsplasty.14,20 In our patient, temporary fixation was performed by using a transfixing wire. Although some instability may persist after the wire removal, this method is relatively low-cost and has potential to be used in situations where articulated external fixators are not available.
No infections, recurrent dislocations, stiffness, or heterotopic ossificans were observed at the latest follow-up. One patient with a 5-month-old dislocation developed postoperative transient ulnar nerve palsy. While performing ulnar nerve transposition has been a subject of debate, careful dissection and protection of the nerve to avoid impingement during reduction maneuvers are essential. In our patient, although the ulnar nerve was protected, the mechanism of ulnar neuropraxia was likely caused by chronic shortening and fibrosis around the nerve resulting from chronic dislocation that was stretched after reduction and temporary fixation in flexion.
The limitations of our study include its small sample size and short-term follow-up. A larger sample with different onsets may reflect other possible problems that can happen during reduction in an older dislocation, such as degenerative articular changes or spontaneous bony ankylosing, which necessitates a more advanced strategy.
Conclusion
Surgical treatment using a double approach for neglected elbow dislocations provides good results with minimal complications and should be considered for all patients presenting with this condition.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Dr. Soeharso Orthopedic Hospital. The privacy and personal identity of all participants were protected and written informed consent was obtained from all participants. This study is complied with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Islam S, Jahangir J, Manzur RM, Chowdury AAA, Tripura N, das A. Management of neglected elbow dislocations in a setting with low clinical resources. Orthop Surg. 2012;4(3):177–181. doi:10.1111/j.1757-7861.2012.00190.x
2. Kodde IF, van Rijn J, van den Bekerom MPJ, Eygendaal D. Surgical treatment of post-traumatic elbow stiffness: a systematic review. J Shoulder Elb Surg. 2013;22(4):574–580. doi:10.1016/j.jse.2012.11.010
3. Nicola L, Birhanu A, Aselefech G, Giovanni M. Outcome of open reduction for the neglected posterior dislocation of the elbow in a low-to-middle income country. Trop Doct. 2016;46(2):96–100. doi:10.1177/0049475515598465
4. Crenshaw JRA. Elbow - Old Unreduced Dislocations. In: Azar FM, Beaty JH, editors. Campbell’s Operative Orthopaedic. Elsevier; 2021:3246–3270
5. Hoppenfeld S, de Boer P, Buckley R. The Elbow. In: Surgical Exposures in Orthopaedics the Anatomic Approach.
6. Morrey B, Adams R. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Jt Surg Am. 1992;74-A(4):479–490. doi:10.2106/00004623-199274040-00003
7. Longo UG, Franceschi F, Loppini M, Maffulli N, Denaro V. Rating systems for evaluation of the elbow. Br Med Bull. 2008;87(1):131–161. doi:10.1093/bmb/ldn023
8. Fahsi M, Benameur H, Hiba O, et al. Neglected dislocation of the elbow: about 8 cases and review of literature. OALib. 2015;02(11):1–5. doi:10.4236/oalib.1102066
9. Anderson DR, Haller JM, Anderson LA, Hailu S, Chala A, O’Driscoll SW. Surgical treatment of chronic elbow dislocation allowing for early range of motion: operative technique and clinical results. J Orthop Trauma. 2018;32(4):196–203. doi:10.1097/BOT.0000000000001097
10. Karakoyun Ö, Erol MF, Küçükkaya M. Treatment of neglected elbow dislocations with the help of hinged external fixator: report of two cases. J Clin Exp Investig. 2015;5(2):307–312. doi:10.5799/ahinjs.01.2014.02.0409
11. Kachnerkar DNI, Lakde DN, Salokhe DS. Neglected old posterior dislocation of elbow: treatment and results of open reduction. Int J Orthop Sci. 2017;3(3o):1062–1066. doi:10.22271/ortho.2017.v3.i3o.154
12. Essi FA, Najeb Y, Latifi M. Transtricipital dorsal approach in neglected elbow dislocation. Chir Main. 2010;29(5):321–325. doi:10.1016/j.main.2010.03.009
13. Coulibaly NF, Tiemdjo H, Sane AD, Sarr YF, Ndiaye A, Seye S. Posterior approach for surgical treatment of neglected elbow dislocation. Orthop Traumatol Surg Res. 2012;98(5):552–558. doi:10.1016/j.otsr.2012.03.006
14. Speed J. An operation for unreduced posterior dislocation of the elbow. South Med J. 1925;18(1):193–198. doi:10.1097/00007611-192503000-00007
15. Pal CP, Mittal V, Dinkar KS, Kapoor R, Gupta M. Neglected posterior dislocation of elbow: a review. J Clin Orthop Trauma. 2021;18:100–104. doi:10.1016/j.jcot.2021.04.016
16. Krishnamoorthy S, Bose K, Wong K. Treatment of old unreduced dislocation of the elbow. Injury. 1976;8:39e42. doi:10.1016/0020-1383(76)90008-5
17. Pundkar GN, Sonar SB, Kulkarni OP. A Case of 3-month-old Neglected Elbow Dislocation Managed by Open Reduction and Cruciate Ligament Reconstruction Using Tendon Graft. J Orthop Case Rep. 2017;7(4):58–60. doi:10.13107/jocr.2250-0685.852
18. Birjandi Nejad A, Ebrahimzadeh MH, Moradi A. Clinical outcomes after posterior open elbow arthrolysis for posttraumatic elbow stiffness. Arch Trauma Res. 2014;3(3):0–4. doi:10.5812/atr.21742
19. Mehta S, Sud A, Tiwari A, Kapoor SK. Open reduction for late-presenting posterior dislocation of the elbow. J Orthop Surg. 2007;15(1):15–21. doi:10.1177/230949900701500105
20. Ayadi D, Etienne P, Burny F, Schuind F. Results of open arthrolysis for elbow stiffness. A series of 22 cases. Acta Orthop Belg. 2011;77(4):453–457.
21. Kapukaya A, Ucar BY, Gem M. Open reduction and Kirschner wire fixation with triceps lengthening for neglected elbow dislocations. J Orthop Surg. 2013;21(2):178–181. doi:10.1177/230949901302100212
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.