Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Functional capacity as a predictor of postoperative delirium in transurethral resection of prostate patients in Northeast Brazil
Authors Braga ILS ![]() , Castelo-Filho J
, Castelo-Filho J ![]() , Pinheiro RSB, de Azevedo RB, Ponte AT
, Pinheiro RSB, de Azevedo RB, Ponte AT ![]() , da Silveira RA
, da Silveira RA ![]() , Braga-Neto P
, Braga-Neto P ![]() , Campos AR
, Campos AR ![]()
Received 20 March 2019
Accepted for publication 16 July 2019
Published 22 August 2019 Volume 2019:15 Pages 2395—2401
DOI https://doi.org/10.2147/NDT.S209379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Ianna Lacerda Sampaio Braga,1–3 João Castelo-Filho,2 Rafael de Sousa Bezerra Pinheiro,3 Rodrigo Barbosa de Azevedo,3 Antônio Talys Ponte,4 Romulo Augusto da Silveira,4 Pedro Braga-Neto,5,6 Adriana Rolim Campos1,2
1Northeast Biotechnology Network, Universidade de Fortaleza (UNIFOR), Fortaleza, Ceará, Brazil; 2Medical School Graduate Program, Health Sciences Center, Universidade de Fortaleza, Fortaleza, Ceará, Brazil; 3Internal Medicine Service, Hospital Geral Dr. César Carls, Fortaleza, Ceará, Brazil; 4Urology Service, Hospital Geral Dr. César Cals, Fortaleza, Ceará, Brazil; 5Division of Neurology, Department of Clinical Medicine, Universidade Federal do Ceará, Fortaleza, Brazil; 6Center of Health Sciences, Universidade Estadual do Ceará, Fortaleza, Brazil
Correspondence: Ianna Lacerda Sampaio Braga
Medical School Graduate Program, Health Sciences Center, Universidade de Fortaleza (UNIFOR), Av. Washington Soares, 1321 - Edson Queiroz, Fortaleza, Ceará, Brazil
Email [email protected]
Pedro Braga-Neto
Department of Clinical Medicine, Universidade Federal do Ceará, Rua Prof. Costa Mendes, 1608 - 4 andar - Rodolfo Teófilo
, Fortaleza, Ceará, Brazil
Tel +55 859 998 5616
Email [email protected]
Introduction: Postoperative delirium (POD) is a common disorder and its frequency varies from 15% to 25% after major elective surgery. There are few data on the incidence of POD in Brazil. Here, we sought to assess the incidence of POD following transurethral resection of the prostate (TURP) and to examine precipitating and predisposing factors associated.
Method: We performed a prospective observational study of elderly male patients undergoing TURP (N=55) in Northeast Brazil. Information on demographic, medical, cognitive and functional characteristics were collected. The participants were followed until hospital discharge. POD was diagnosed by the Confusion Assessment Method.
Results: A total of three participants (5.45%) were identified with POD. Episodes of delirium lasted 3±1 days. The study sample consisted of a healthy population. Patients with POD had longer hospital stay and more precipitating factors. The POD group showed statistically significant lower Barthel index score (p<0.001) and higher Pfeffer’s Functional Activities Questionnaire scores (p<0.01).
Conclusion: Loss of functional capacity was associated with POD in a healthy population of elderly patients undergoing TURP.
Keywords: delirium, transurethral resection of prostate, neurocognitive disorders, risk factors, activities of daily living
Introduction
Postoperative delirium (POD) is associated with a significant increase in morbidity and mortality, institutionalization, longer hospital stay and higher health care costs.1 There are scarce data on the incidence of delirium in Brazil.2 A study conducted in Brazil found a frequency of POD of 18.8% in 680 multimorbid patients undergoing emergency and high-risk surgery, excluding cardiac and neurological surgical procedures.3
The occurrence of delirium depends on the type of surgical procedure and patient health characteristics. Few studies have investigated POD after minor surgery. The risk of POD after transurethral resection of the prostate (TURP) ranged from 4.6% to 21.23% in different studies from China.4,5
This study aimed to assess the incidence of POD following TURP and to examine precipitating and predisposing factors associated with elderly patients admitted to a general hospital in a Northeast city of Brazil.
Methods
Study design and population
We conducted a prospective observational study in a single medical center from November 2016 to November 2017. The study was carried out at Hospital Geral Dr. César Cals, a tertiary academic hospital in Northeast Brazil, which is one of the poorest regions in the country. The inclusion criteria included patients 60 years of age or older who were admitted to the hospital for TURP surgery. The exclusion criteria were preoperative delirium and history of acute neurological disorder (stroke, traumatic brain injury) in the past 3 months.
Study protocol
We carried out a careful clinical evaluation of patients with administration of preoperative assessment scales. We evaluated the participants using a guided interview for geriatric assessment as part of the anamnesis and a simplified physical examination. We administered a standardized questionnaire to collect information on demographic and clinical variables (age, marital status, years of schooling, Charlson Comorbidity Index (CCI),6 number of medications used and smoking and alcohol consumption), and collected information regarding length of hospital stay, anthropometric measurements and laboratory test results (blood counts, creatinine and sodium).
To delirium diagnosis,7 we applied the Diagnostic and Statistical Manual of Mental Disorders criteria8 and the Confusion Assessment Method (CAM).7 The Mini-Mental State Examination (MMSE)9 and the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE)10 were used for cognitive evaluation. Functional capacity was assessed using the Barthel index (BI)11 for activities of daily living (ADL) and Pfeffer’s Functional Activities Questionnaire (FAQ)12 for instrumental activities of daily living (IADL). The American Society of Anesthesiologists (ASA) classification was used for risk assessment of preoperative patients.
Surgical and postsurgical assessment
We collected intraoperative information including type of anesthesia and hemodynamic status of the patient during the surgical procedure and results of laboratory tests performed during the surgery, when requested by the surgeon, including hemoglobin, creatinine and sodium. After surgery, we administered the CAM on a daily basis to identify POD. The participants were asked to record their levels of pain at rest preoperatively and postoperatively. We measured pain intensity using a Likert scale (0–10) and assessed precipitating factors of delirium up to hospital discharge.
Statistical analyses
All statistical analyses were performed using the statistical package SPSS 22® for Windows (Version 22, SPSS, Chicago, IL, USA). The presence of a normal distribution of data was determined by the Kolmogorov–Smirnov test. For normally distributed variables with homogeneity of variance, a two-tailed Student’s t-test was performed. For variables that did not meet the homogeneity of variance requirement, the nonparametric Mann–Whitney U-test was used. Categorical variables were analyzed by Fisher’s exact test. The null hypothesis was rejected in every statistical testing when p<0.05 for type I error.
Ethical issues
The institution of Universidade de Fortaleza – UNIFOR ethics committee approved the study (approval number 1,562,383). All participants signed an informed consent. All procedures performed in studies involving human participants were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Results
A total of 55 elderly participants (71.80±5.78 years) were included in the study. They had on average 3.06±3.06 years of schooling and 30% were illiterate. CCI scores ranged between 0 (64.80%) and 4 (1.90%). The patients were clinically stable at admission in both groups. There were no significant differences in demographic characteristics and clinical and laboratory parameters between POD and non-POD groups (Table 1). Though not statistically significant, participants in the POD group were older and showed higher CCI scores compared to the non-POD group.
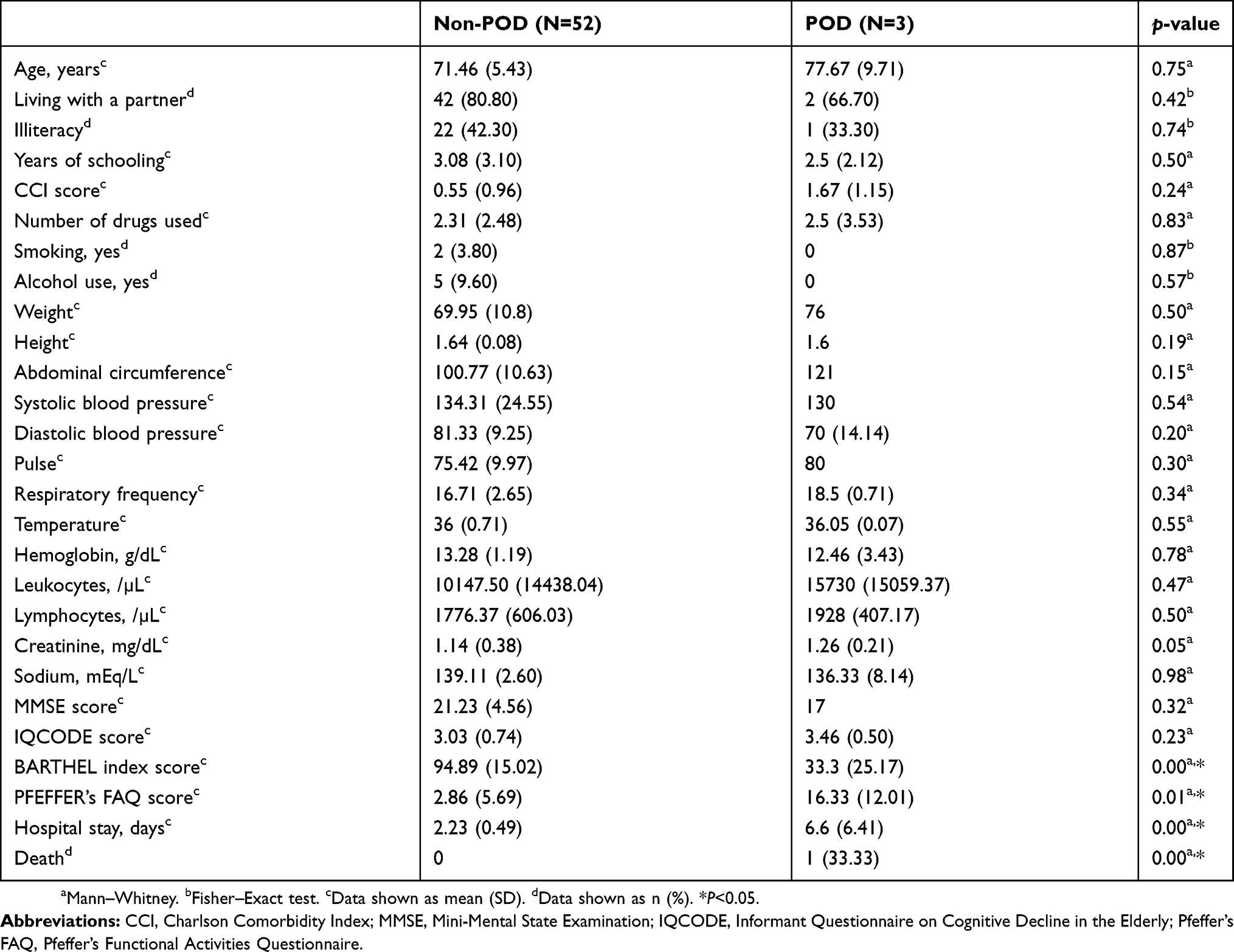 |
Table 1 Sociodemographic, clinical, cognitive and functional characteristics and laboratory test results of patients experiencing postoperative delirium (POD) and not experiencing postoperative delirium (non-POD) |
Pain at admission was similar in both groups. The participants used 2.31±2.48 medications. Compared to the POD group, participants in the non-POD group used more psychoactive drugs and more inappropriate medications for the elderly (benzodiazepines, antiparkinsonians and anticholinergics), though this difference was not statistically significant.
All participants underwent spinal anesthesia; 93.50% of them were ASA 2 and only one patient was ASA 3. One patient developed hypotension during surgery and was admitted to the intensive care unit (ICU) and subsequently died.
Three patients were identified with POD using the CAM. POD started on day 1 postoperatively in two patients and day 3 postoperatively in one patient. It lasted 3±1 days. One of them died. Table 1 shows cognitive and functional scores for all patients. The POD group showed statistically significant lower BI (p<0.00) and higher FAQ scores (p<0.01) when compared with the non-POD group. Tables 2 and 3 compare predisposing and precipitating factors for both groups. In the immediate postoperative period, all participants in the POD group were restricted to bed (p<0.001). There were no other differences between both groups.
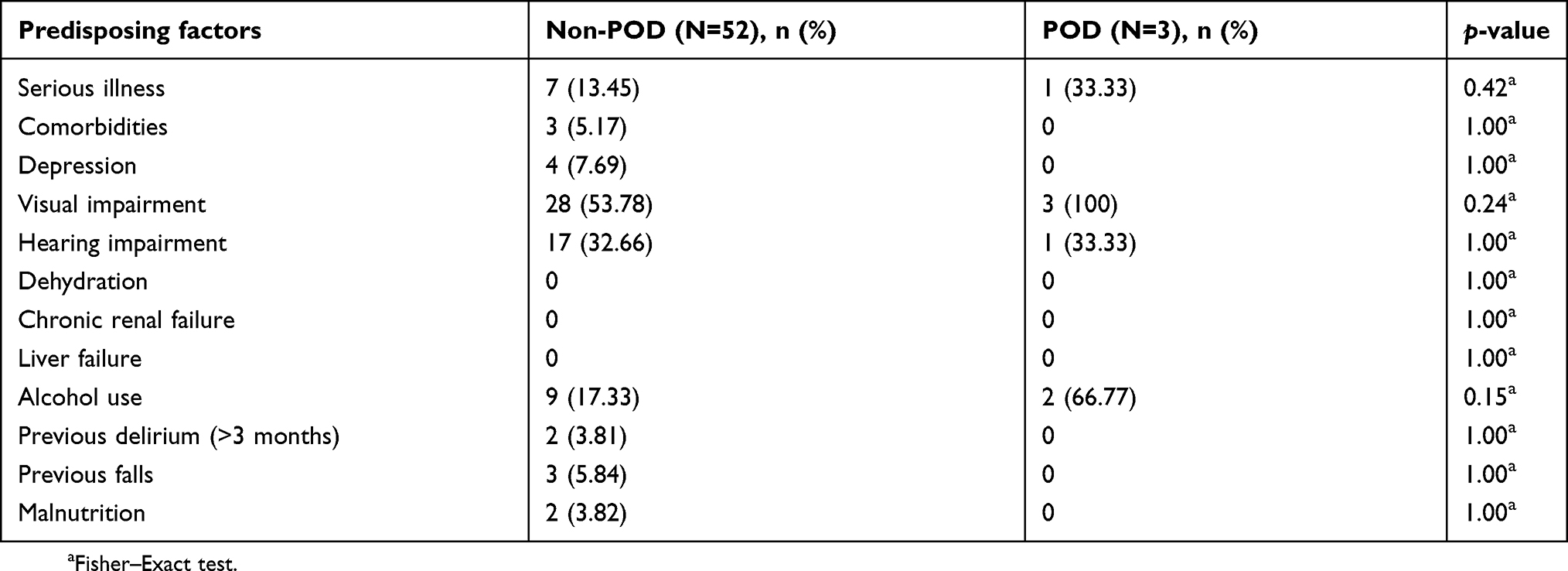 |
Table 2 Predisposing factors in postoperative delirium (POD) and non-postoperative delirium (non-POD) groups |
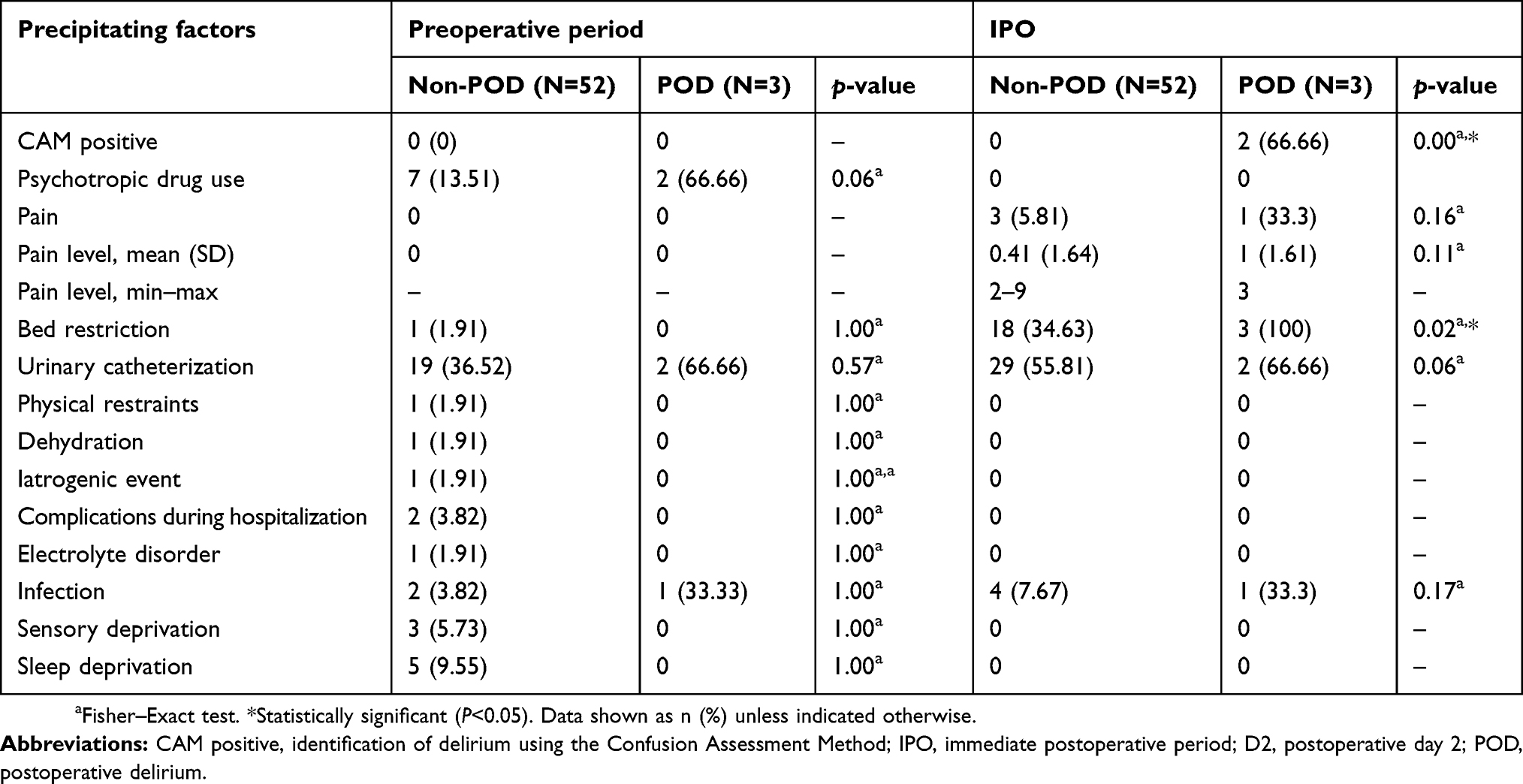 |
Table 3 Precipitating factors of delirium in the preoperative period and immediate postoperative period in postoperative delirium (POD) and non-postoperative delirium (non-POD) groups |
In the following is a detailed description of the patients experiencing POD.
Patient 1 was an 87-year-old male, retired farmer, widowed and illiterate. He had Parkinson’s disease (CCI score of 1) and showed an IQCODE score of 4/5, BI of 30/100 and Pfeffer’s FAQ score of 17/30. He had low visual acuity and did not use any prior medications, but required a catheter because of urinary retention. He was on a psychoactive drug while in hospital. The patient developed hypotension during surgery and was admitted to the ICU after the surgical procedure and died 2 weeks later.
Patient 2 was an 80-year-old male, farmer, illiterate (1 year of schooling). He had prostate cancer (CCI score of 1) and did not use any prior medications. He had visual impairment, an IQCODE score of 3/5, BI of 60/100 and Pfeffer’s FAQ score of 4/30. The episode of delirium started on day 3 postoperatively. He was discharged from the hospital on day 4 after surgery.
Patient 3 was a 78-year-old male, lifeguard and literate (4 years of schooling). He had a CCI score of 3 (stroke, dementia and diabetes). He was on several medications (levodopa/benserazide, promethazine, amlodipine, gliclazide and calcium) and used an inappropriate medication for the elderly (promethazine). He had used a Foley’s catheter for 6 months and was restricted to bed. He had several predisposing risk factors including dementia, vision and hearing impairment, activity limitation and history of alcohol use. He experienced pain in the immediate postoperative period (pain intensity of 3). The episode of delirium lasted until postoperative day 3, and he was discharged on postoperative day 4. Tables 2 and 3 show a detailed description of his predisposing and precipitating factors.
Although not statically significant, the POD group had a longer hospital stay and more precipitating factors (psychoactive drug and urinary catheter use).
Discussion
The present study evaluated a healthy population undergoing a low-to-medium complexity endoscopic procedure.13 The prevalence of POD was 5.45% and the episodes of POD lasted 3±1 days. These findings are in accordance with previous reports.4,5,14
There are few studies on POD incidence following low-to-medium complexity surgical procedures. This study demonstrated that POD is not an uncommon complication of minor surgical procedures and may be associated with in-hospital mortality.15 Patients experiencing POD following transcatheter aortic valve replacement are at increased risk for in-hospital mortality,16 suggesting that surgery complexity, patient frailty and precipitating and predisposing factors are associated with this condition.
One participant in our study died (1.81%), though the immediate cause of death is not known. We also found a higher 30-day in-hospital mortality rate than that reported in Austria (0.10%)17 and the United States (0.66%).18 The patient who died developed intraoperative hypotension, which is a risk factor associated with POD6 after TURP.19 Brain hypoperfusion may explain this finding.20
Regarding precipitating and predisposing factors for POD, age19,21,22 and preoperative use of benzodiazepines21 were factors associated with POD in elderly patients undergoing various types of low-complexity surgical procedures. The participants who received psychoactive drugs while in the hospital were more likely to have POD, which was shown to be independent of preoperative cognitive impairment in another study of patients admitted for hip fracture surgery.23 However, there were other reports of no differences in demographic characteristics, number of medications used (including anticholinergics and benzodiazepines) and number of comorbidities as predictors of delirium.24 Moreover, a recent meta-analysis from the United Kingdom25 concluded that there is low-quality evidence associating POD with medication use in patients undergoing hip fracture surgery.
In our study, only one participant reported a pain level of 5 (0–10 scale) in the POD group. Therefore, it was not possible to determine whether pain is a precipitating factor, which is in contrast with a study from China that found that patients who developed POD following TURP referred more pain postoperatively than non-POD patients.5 Regarding morbidity, CCI score was not a predictor of POD. However, this same study from China reported a significant association of a comorbidity level of two with POD.5 In Northeast Brazil, patients often do not know their health conditions and do not inform them to health providers. For instance, Patient 3 was taking levodopa but he did not mention he had Parkinson’s disease.
Interestingly, a significant number of participants in our study refused to answer MMSE scale questions and thus this tool could not be used as a predictor of POD. One explanation for this finding is that less-educated patients may find it difficult to take this test. It also may suggest that MMSE scale is not a good assessment tool for a population undergoing surgery. However, a study from China found that MMSE is an essential predictor of POD.4 We also used the IQCODE scale in our study. Although it is easily administered, it did not allow to predict POD, probably because of the small number of participants experiencing POD and the scale’s narrow numerical range (0–5).
In our study, we found that ADL and IADL dependency was associated with POD following TURP. Impairment in IADL has been described as a risk factor for POD in patients undergoing urological procedures.4,19 Additionally, to the best of our knowledge, this is the first study reporting an association of ADL dependency with POD following TURP. Indeed, it seems important to assess functional capacity in patients undergoing other surgical procedures. Loss of functional capacity resulting in ADL and IADL dependency was a factor associated with POD in patients undergoing hip fracture surgery.23 BI and MMSE and IADL results were reported as independent factors associated with POD after gastrointestinal surgery.26 Also, a recent meta-analysis identified functional dependence as a predictor of postoperative complications in patients with gastric cancer.27
Our study has some limitations. The sample size was small because participants had to enter the study and undergo careful evaluation before the surgical procedure, but most of them were admitted to the hospital on the same day of surgery. In addition, the number of participants experiencing POD was small, making it difficult the interpretation of the results of the statistical analyses, though the incidence of POD was similar to that reported in the literature.
Yet, our study has some strengths. Although the results are not new in other populations, to the best of our knowledge, this is the first study to assess POD incidence in elderly patients undergoing TURP in Northeast Brazil. The participants underwent thorough evaluation for delirium by a skilled medical team trained to identify POD. This multidisciplinary team comprised a geriatrician, an internist, urologists and anesthesiologists. Cognitive and functional tests were administered, which allows comparisons with other patient populations. For improving care for the elderly, functional capacity should be assessed in all patients undergoing TURP. Surgeons will be able to identify patients at risk of POD and establish delirium prevention measures to prevent in-hospital complications such as death, prolonged hospital stay and increased costs.
As a conclusion, we found that functional dependence is associated with POD even in patients undergoing low-complexity urological procedures (TURP). Studies with POD patients are important to be conducted in patients of all ethnicities and socioeconomic backgrounds.
Disclosure
PBN and ARC were supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). JCR received a scholarship from Universidade de Fortaleza. The authors report no other conflicts of interest in this work.
References
1. Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in older persons: advances in diagnosis and treatment. Jama. 2017;318(12):1161–1174. doi:10.1001/jama.2017.12067
2. Malik AT, Quatman CE, Phieffer LS, Ly TV, Khan SN. Incidence, risk factors and clinical impact of postoperative delirium following open reduction and internal fixation (ORIF) for hip fractures: an analysis of 7859 patients from the ACS-NSQIP hip fracture procedure targeted database. Eur J Orthop Surg Traumatol. 2019;29:435–446.
3. Veiga D, Luis C, Parente D, et al. Delirium pós-operatório em pacientes críticos: fatores de risco e resultados. Rev Bras Anestesiol. 2012;62:476–483.
4. Tai S, Xu L, Zhang L, Fan S, Liang C. Preoperative risk factors of postoperative delirium after transurethral prostatectomy for benign prostatic hyperplasia. Int J Clin Exp Med. 2015;8(3):4569–4574.
5. Xue P, Wu Z, Wang K, Tu C, Wang X. Incidence and risk factors of postoperative delirium in elderly patients undergoing transurethral resection of prostate: a prospective cohort study. Neuropsychiatr Dis Treat. 2016;12:137–142. doi:10.2147/NDT.S97249
6. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
7. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157–1165. doi:10.1056/NEJMra052321
8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
9. Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3B). doi:10.1590/S0004-282X2003000500014
10. Sanchez M, Lourenço RA. Informant questionnaire on cognitive decline in the elderly (IQCODE): adaptação transcultural para uso no Brasil. Cad Saude Publica. 2009;25:1455–1465.
11. Minosso JSM, Amendola F, Alvarenga MRM, Oliveira M. Validação, no Brasil, do Índice de Barthel em idosos atendidos em ambulatórios. Acta Paulista De Enfermagem. 2010;23:218–223. doi:10.1590/S0103-21002010000200011
12. Dutra MC, Ribeiro R, Pinheiro SB, GFd M, Carvalho G. Accuracy and reliability of the Pfeffer questionnaire for the Brazilian elderly population. Dement Neuropsychol. 2015;9:176–183. doi:10.1590/1980-57642015DN92000012
13. Sociedade_Brasileira_de_Urologia. Programa de Residência Médica em Urologia; Published 2018. Available from: http://portaldaurologia.org.br/wp-content/uploads/2015/09/programa-residencia.pdf.
14. Brodak M, Tomasek J, Pacovsky J, Holub L, Husek P. Urological surgery in elderly patients: results and complications. Clin Interv Aging. 2015;10:379–384. doi:10.2147/CIA.S73381
15. Stachon P, Kaier K, Zirlik A, et al. Risk factors and outcome of postoperative delirium after transcatheter aortic valve replacement. Clin Res Cardiol. 2018;107(9):756–762. doi:10.1007/s00392-018-1241-3
16. Abawi M, Nijhoff F, Agostoni P, et al. Incidence, predictive factors, and effect of delirium after transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2016;9(2):160–168. doi:10.1016/j.jcin.2015.09.037
17. Eredics K, Wachabauer D, Rothlin F, Madersbacher S, Schauer I. Reoperation rates and mortality after transurethral and open prostatectomy in a long-term nationwide analysis: have we improved over a decade? Urology. 2018;118:152–157. doi:10.1016/j.urology.2018.04.032
18. Wallace B, Breau RH, Cnossen S, et al. Age-stratified perioperative mortality after urological surgeries. Can Urol Assoc J. 2018;12(8):256–259. doi:10.5489/cuaj.5022
19. Tognoni P, Simonato A, Robutti N, et al. Preoperative risk factors for postoperative delirium (POD) after urological surgery in the elderly. Arch Gerontol Geriatr. 2011;52(3):e166–e169. doi:10.1016/j.archger.2010.10.021
20. Tobar E, Abedrapo MA, Godoy JA, et al. [Impact of hypotension and global hypoperfusion in postoperative delirium: a pilot study in older adults undergoing open colon surgery]. Rev Bras Anestesiol. 2018;68(2):135–141. doi:10.1016/j.bjan.2017.10.002
21. Milstein A, Pollack A, Kleinman G, Barak Y. Confusion/delirium following cataract surgery: an incidence study of 1-year duration. Int Psychogeriatr. 2002;14(3):301–306.
22. Rohan D, Buggy DJ, Crowley S, et al. Increased incidence of postoperative cognitive dysfunction 24 hr after minor surgery in the elderly. Can J Anaesth. 2005;52(2):137–142. doi:10.1007/BF03027718
23. Levinoff E, Try A, Chabot J, Lee L, Zukor D, Beauchet O. Precipitants of delirium in older inpatients admitted in surgery for post-fall hip fracture: an observational study. J Frailty Aging. 2018;7(1):34–39.
24. Zietlow K, McDonald SR, Sloane R, Browndyke J, Lagoo-Deenadayalan S, Heflin MT. Preoperative cognitive impairment as a predictor of postoperative outcomes in a collaborative care model. J Am Geriatr Soc. 2018;66(3):584–589. doi:10.1111/jgs.15261
25. Smith TO, Cooper A, Peryer G, Griffiths R, Fox C, Cross J. Factors predicting incidence of post-operative delirium in older people following hip fracture surgery: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2017;32(4):386–396. doi:10.1002/gps.4655
26. Maekawa Y, Sugimoto K, Yamasaki M, et al. Comprehensive geriatric assessment is a useful predictive tool for postoperative delirium after gastrointestinal surgery in old-old adults. Geriatr Gerontol Int. 2016;16(9):1036–1042. doi:10.1111/ggi.12587
27. Xue DD, Cheng Y, Wu M, Zhang Y. Comprehensive geriatric assessment prediction of postoperative complications in gastrointestinal cancer patients: a meta-analysis. Clin Interv Aging. 2018;13:723–736. doi:10.2147/CIA.S155409
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.