")
Back to Journals » International Journal of Women's Health » Volume 14
Fructosamine as an Index of Short-Term Glycemic Control in Pregnant Women with Diabetes: Before, During and After Ramadan
Authors Ekhzaimy A , Alkatari S, AlMaatouq M, Alotaibi D, Aljasser S, Aseeri A, Jammah A , Mujammami M, Fouda M, Alfadda AA , Sulaimani R
Received 29 November 2021
Accepted for publication 3 March 2022
Published 30 March 2022 Volume 2022:14 Pages 435—444
DOI https://doi.org/10.2147/IJWH.S351654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Aishah Ekhzaimy,1 Shadin Alkatari,1 Mohamed AlMaatouq,1 Daad Alotaibi,1 Sarah Aljasser,1 Amal Aseeri,1 Anwar Jammah,1 Muhammad Mujammami,1– 3 Mona Fouda,1 Assim A Alfadda,1,2,4 Riad Sulaimani1
1Division of Endocrinology, Department of Medicine, College of Medicine, King Saud University Medical City, King Saud University, Riyadh, Kingdom of Saudi Arabia; 2Strategic Center for Diabetes Research, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia; 3University Diabetes Center, King Saud University Medical City, King Saud University, Riyadh, Kingdom of Saudi Arabia; 4Obesity Research Center, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Aishah Ekhzaimy, Division of Endocrinology, Department of Medicine, College of Medicine, King Saud University Medical City, King Saud University, Riyadh, Kingdom of Saudi Arabia, Email [email protected]
Purpose: Impact of ramadan fasting on healthy and women with diabetes is already known. However, there is a scarcity of data on impact of fasting on pregnant women with diabetes. Moreover, religious and medical recommendations advise pregnant women against fasting as it is unsafe. Despite being exempted, many pregnant Muslim women with diabetes still choose to fast during ramadan. This study investigated different glycemic marker as an indicator for diabetes control in fasting pregnant women.
Patients and Methods: This is a prospective observational study. A total of 89 pregnant diabetes women were recruited. Blood glucose was self-monitored in all the pregnant women using glucose monitoring device at home. We measure the fructosamine, HbA1c levels before, during and after ramadan.
Results: Pregnant women with type 1 diabetes were 14 (25%), type 2 diabetes were 21 (37.5%), and gestational diabetes were 21 (37.5%). The mean fructosamine level decreased during and after ramadan in gestation diabetes pregnant women compared to type 2 diabetes and type 1 diabetes pregnant women subjects (p = 0.009).
Conclusion: The present study indicates that pregnant women with diabetes were able to fast during ramadan and there fructosamine level reduced during fasting. Utilization of fructosamine for short-term monitoring of glycemic control in addition to home glucose monitoring in pregnant women with diabetes will provide a good index of glycemic control.
Recommendation: Religious and medical recommendations advise pregnant women against fasting as it is unsafe, and they are under high risk. However, if they insist to do fast, they must do under strict medical supervision and fructosamine can be used as a glycemic control marker.
Keywords: ramadan fasting, gestational diabetes, type 2 diabetes, type 1 diabetes, pregnant women, fructosamine
Introduction
Ramadan is a holy month for 1.5–1.9 billion Muslims and is one of the five pillar of Islam fasting during this times is mandatory for all adult Muslims.1,2 It is estimated that globally more than 50 million people with diabetes mellitus will observe fasting during ramadan annually.3 Seasonal and geographical location will influence daily fasting duration range from 11 to 18 hours per day.4 Pregnant (diabetic or healthy) women who are concerned about their health and about fetus wellbeing are exempted from fasting. Moreover, religious recommendations and medical recommendations also advise pregnant women against fasting and it is unsafe.5,6 Despite being exempted, many pregnant women with type 1 diabetes, type 2 diabetes and gestational diabetes still choose to fast during ramadan.7,8 Nevertheless, many patients wish to honor their tradition, beliefs and insist on fasting, thereby creating a medical challenges for themselves and their health care providers.9 Earlier, there were no established guidelines or recommendations, but recently few guidelines have advised pregnant women against fasting as they are under high risk.1,10 The major risk factor associated with fasting in patients with diabetes are hypoglycemia, hyperglycemia, diabetes ketoacidosis, dehydration, and thrombosis.10 Frequencies of severe hypoglycemic episodes occurring before and during ramadan in both type 1 diabetes and type 2 diabetes was significantly higher during ramadan compared to other months.11 The effect of ramadan fasting during pregnancy on the perinatal outcomes has been investigated in the systematic review and meta-analysis.12 More recently, perinatal registry of the Netherlands (Perined) study, found no effect of maternal exposure to ramadan on perinatal outcomes.13 Although, few studies explored the effects of ramadan fasting in insulin treated pregnant women.7,14
This study aims to investigate the glycemic control by measuring fructosamine as an index of short-term diabetic control than that represented by hemoglobin A1c% as an index of long-term diabetic control in diabetic pregnant women before, during and after ramadan.
Materials and Methods
Design and Subjects
This is a prospective cohort study. It was conducted at King Saud University Medical City, Riyadh, Saudi Arabia from April- to July 2019. This study was approved by Institution review board ethics committee (Approval No: E-18-3074), College of medicine, King Saud University, Riyadh, Saudi Arabia. Informed consent was obtained from all the pregnant women patients before participating in the study.
A total of 89 diabetic pregnant women patients who attended diabetes and pregnancy clinic were interviewed by Research physician, nutritionist, and diabetes educators before ramadan (Figure 1). They agreed to participate in the study. All the diabetic pregnant women patient’s follow-up during ramadan and after ramadan. Inclusion criteria were pregnant women patients with type 1 diabetes, type 2 diabetes, and gestational diabetes. Age was between 22–46 years, and on medication such as insulin, diet with or without oral hypoglycemic agents. All pregnant women patients were under well glycemic control before ramadan and insist to fast during the month of ramadan. All the participants received strict glucose monitoring, and standard diabetes management before ramadan, during ramadan and after ramadan.
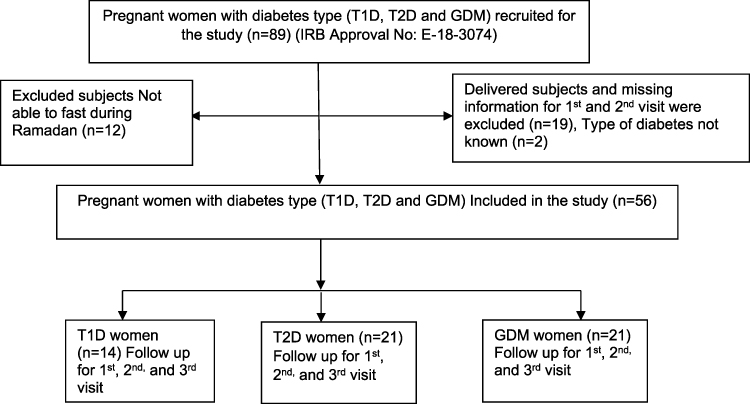 |
Figure 1 Patient selection. |
All the participants who did not fit the inclusion criteria or having eclampsia/preeclampsia, chromosomal abnormalities, cardiac abnormalities, placental abnormalities, or other risk factors (intrauterine growth restriction) were initially excluded from the study. A total of twelve diabetic pregnant women patients were excluded as they were unable to fast during ramadan. Moreover, two diabetic pregnant women patients were also excluded as the type of diabetes was unknown. The manuscript was written based on the “Strengthening the reporting of observational studies in epidemiology (STROBE)” established guideline.15
Data Collection
A total of 56 pregnant women with diabetes (Type 1 diabetes (n= 14); Type 2 diabetes (n=21) and Gestational diabetes (n=21) were instructed by research physician to check, monitor, and keep records of their blood glucose reading using glucose meters with a minimum of three-six times daily. Blood glucose readings were monitor by patients at pre and/post 2 hour after breakfast, pre and/post 2-hour meals at lunch, and pre and/post 2-hour meals at dinner for one month before ramadan. During ramadan glucose readings were monitor by patients at pre and/post-2 hour after sohour, noon, and pre and/post 2-hour after Iftar. Moreover, blood glucose readings were monitored at pre and/post 2-hour after breakfast, pre and/post 2-hour meals at lunch, pre and/post 2-hour meals at dinner for one month after Ramadan.
All pregnant women with diabetes were counseled by the members of research team during clinic visits, for discussing their readings and recommending the appropriate adjustments. Severe hyperglycemia was defined as blood glucose level more than >300 mg/dl (> 16.7 mmol/L). Hyperglycemia was defined as blood glucose level more than >140 mg/dl (>7.8 mmol/L), hypoglycemia was defined as glucose level below <70 mg/dl (<3.9 mmol/L). The fast should be stop if glucose reaches <70 mg/dl (3.9 mmol/l) and blood glucose >300 mg/dl (16.7 mmol/l).16 All diabetic pregnant women patients documented hypoglycemic episodes during the study period after educating them about the signs and symptoms. Demographic data were collected from all diabetic pregnant women patients, including age, parity, gestational age, and type of diabetes.
Laboratory Investigation
We obtained 4 mL of fasting venous blood from each pregnant women during clinic visit. Fasting blood samples were evaluated for HbA1c% and fructosamine. HbA1c and fructosamine level were measured before ramadan, during ramadan and after ramadan during the clinic visit. The normal HbA1c level is between 4–5.6%. High performance liquid chromatography (HPLC) by TOSOH was used for the determination of HbA1c% in the blood. Serum fructosamine was measured by colorimetric method Labcorp (Test No: 100800) to evaluate short-term glycemic control index (fructosamine; one to three weeks) of pregnant women than of long-term glycemic control index (HbA1c; 3 months average). The normal fructosamine level was 205–285 μmol/l.
Statistical Analysis
The data obtained from all diabetes pregnant women patients collected and saved in an excel sheet then transferred into SPSS V.21 program for analysis. Normal distribution of continuous variable was done by Kolmogorov–Smirnov test. Mean and standard deviations were used to express quantitative variables, whereas numbers and percentages were used for qualitative variables. T-test and Chi-square were used for comparison between the two groups based on the type of variables. ANOVA test was used for comparison between the three groups. P-value was considered significant at < 0.05.
Results
Table 1 shows the demographic characteristics of the all the diabetes pregnant women. Total 56 diabetes pregnant women participated in the study. Pregnant women with type 1 diabetes were 14 (25%), pregnant women with type 2 diabetes were 21 (37.5%), pregnant women with gestational diabetes were 21 (37.5%). Most of the diabetes pregnant women were in age group 30–40 years (71.4%), multigravida (80.4%), gestational age 2nd (48.2%) and 3rd trimester (41.1%) and majority of them were taking short (62.5%) and long acting (51.8%) insulin. Most of the of them were taking insulin (39.3%) and oral hypoglycemic agents (OHA) with insulin (30.4%). All the diabetes pregnant women were fasted during the month of ramadan.
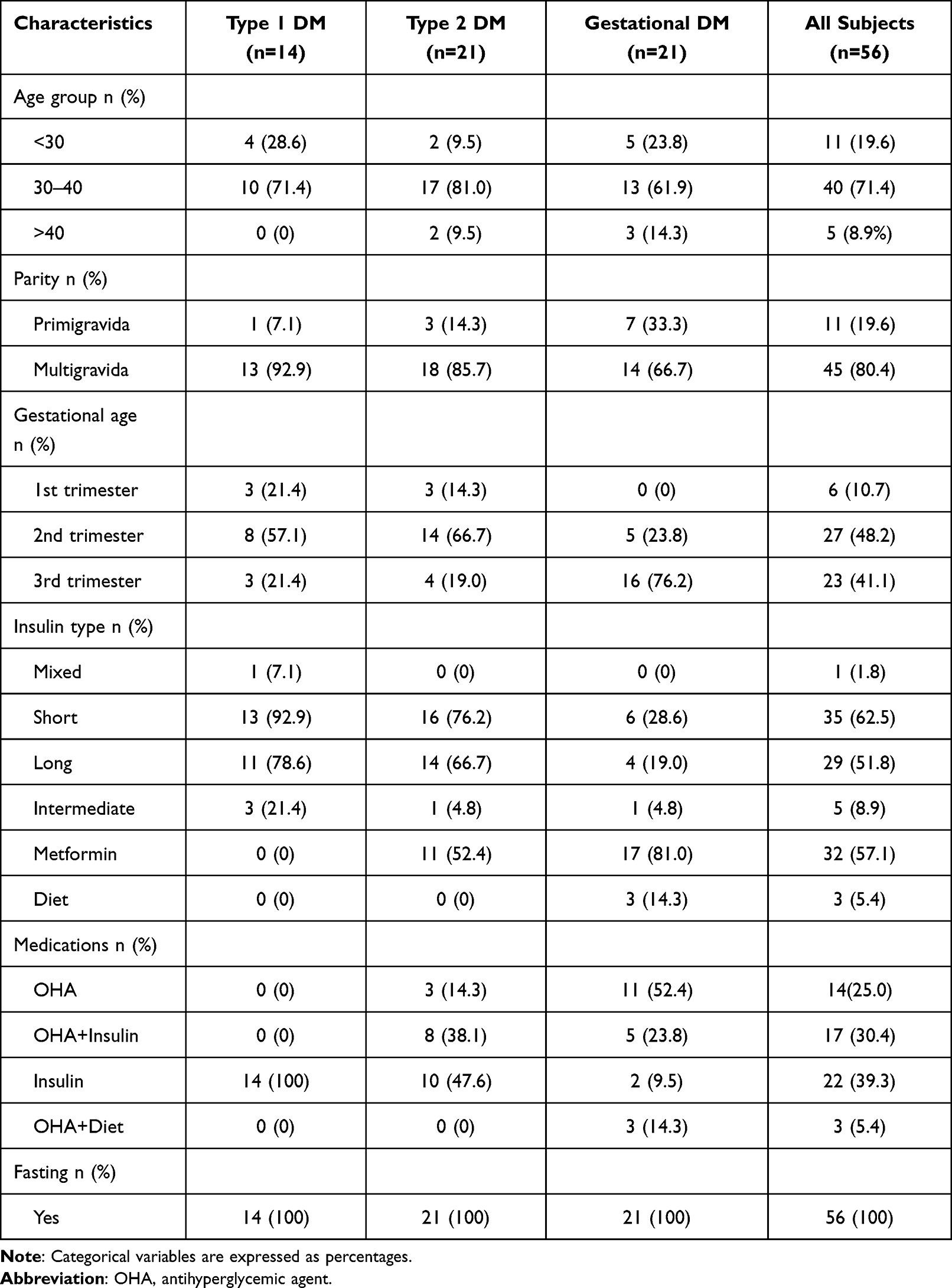 |
Table 1 Patients Demographic Characteristics |
Table 2 showing the glycemic parameters between Type 1 diabetes, Type 2 diabetes, and gestational diabetes pregnant women. Before ramadan, the mean HbA1c% was 6.0±0.8 for gestational diabetes pregnant women compared to type 1 diabetes and type 2 diabetes pregnant women. The mean HbA1c% was improved during and after ramadan in gestational diabetes pregnant women compared to type 2 diabetes and type 1 diabetes pregnant women Moreover, before ramadan the mean fructosamine concentration was 208.1±21.5 μmol/L for gestational diabetes pregnant women compared to type 1 diabetes and type 2 diabetes pregnant women. The mean fructosamine concentration improved during and after ramadan in gestational diabetes pregnant women compared to type 2 diabetes and type 1 diabetes pregnant women Demonstrating the short-term glycemic control than blood glucose levels, especially in gestational diabetes pregnant women when compared to type 1 diabetes and type 2 diabetes pregnant women before ramadan, during ramadan and after ramadan.
 |
Table 2 Glycemic Parameters Between the Diabetes Types |
Table 3 shows the hypoglycemia frequencies among type 1, type 2, and gestational diabetes pregnant women subjects. Type 1, Type 2 diabetes pregnant women had the highest incidence of hypoglycemic episodes, whereas the gestational diabetes pregnant women had highest rate of normoglycemia.
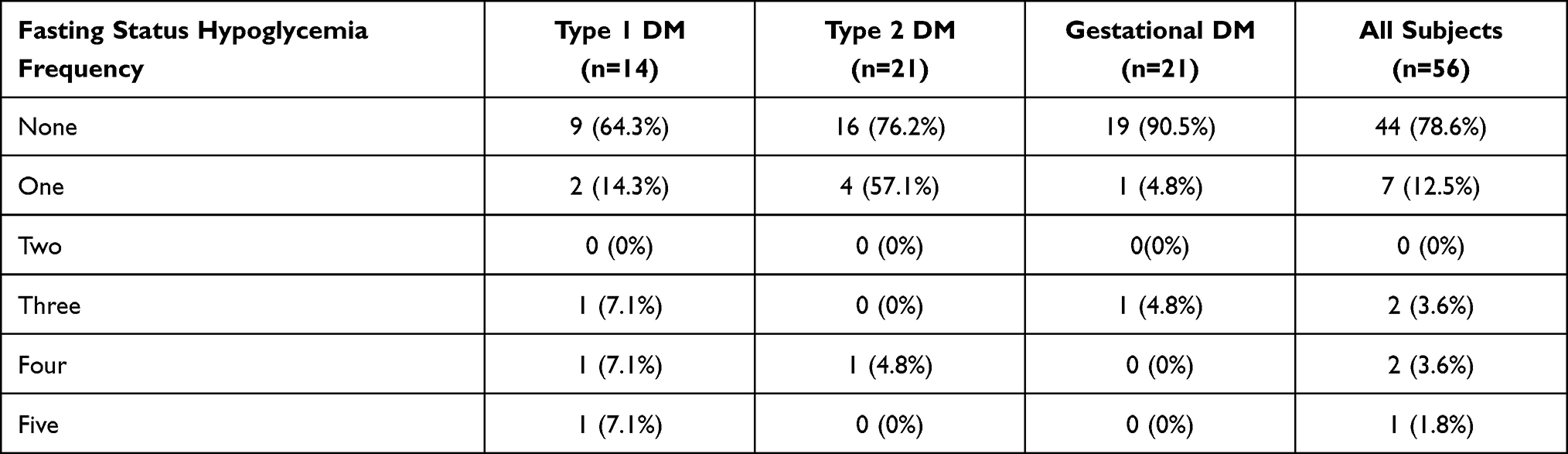 |
Table 3 Frequencies of Hypoglycemia Between the DM Groups During Ramadan |
Table 4 shows the level of fructosamine and HbA1c in type 1, type 2, and gestational diabetes pregnant women. In type 1 and type 2 diabetes pregnant women fructosamine level improved during ramadan and it demonstrate the favorable short-term glycemic control compared to HbA1c which did not improve long-term glycemic control.
 |
Table 4 Show Fructosamine and HbA1c Within Type 1 Diabetes, Type 2 Diabetes, and Gestational Diabetes (1st Visit, 2nd Visit and 3rd Visit) |
Figure 2A shows the fructosamine level in type 1 diabetes pregnant women. The fructosamine level improve during ramadan fasting in type 1 diabetes pregnant women but did not attend statistical significance.
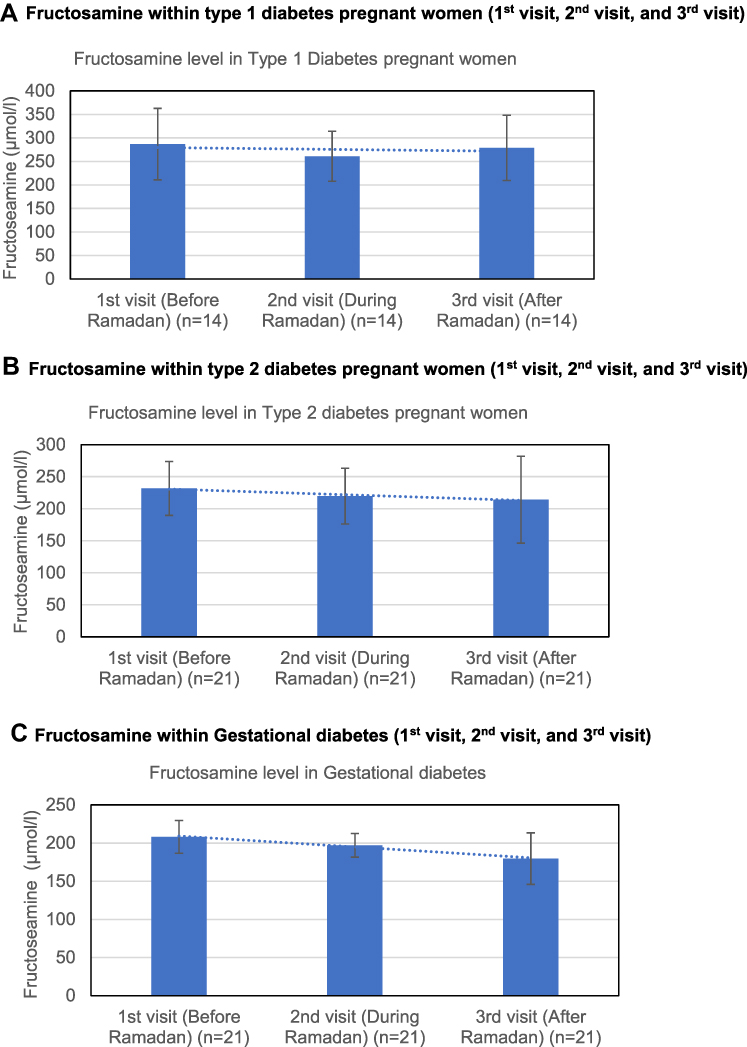 |
Figure 2 (A) Fructosamine within type 1 diabetes pregnant women (1st visit, 2nd visit, and 3rd visit). (B) Fructosamine within type 2 diabetes pregnant women (1st visit, 2nd visit, and 3rd visit). (C) Fructosamine within Gestational diabetes (1st visit, 2nd visit, and 3rd visit). |
Figure 2B shows the fructosamine level in type 2 diabetes pregnant women subjects. The fructosamine level improve during ramadan, and after ramadan in type 2 diabetes pregnant women but did not attend statistical significance.
Figure 2C shows the fructosamine levels in gestational diabetes pregnant women who had significant improvement in their fructosamine levels during ramadan, and after ramadan (p = 0.009).
Discussion
Our study demonstrates that measurement of fructosamine will provide a good short-term glycemic tool to monitor glycemic control especially in pregnant women with gestational diabetes. Our study also demonstrates fructosamine variability in type 1, type 2, and gestational diabetes differ significantly between before ramadan, and during ramadan. Other glycemic parameters such as mean glucose and HbA1c% levels were comparable. Measurement of fructosamine can be considered as a potential alternative for monitoring of short-term diabetes control in type 1, type 2, and gestational diabetes pregnant women. Ramadan fasting is associated with changes in eating, physical activity, sleeping patterns, and medication.17 Although the various effects of fasting including the metabolic and physiological adaptations to early starvation as reflected by glucose intake restriction have been extensively studied,18 little is known about the effects of fasting on diabetes in pregnant women. Unfortunately, only limited studies examine glucose variability in type 1, type 2 and gestational diabetes pregnant women who fast in ramadan.
Previously, Afandi B et al, demonstrated that continuous glucose monitoring (CGM) is needed in women with gestational diabetes who are treated with diet alone or with diet and metformin and are categorized as high risk for adverse events. Ramadan fasting increases the risk of hypoglycemia in GDM treated with diet alone or with both diet and metformin.8 Recently, Harbuwono et al, evaluated glucose variability in subjects with type 2 diabetes on oral antidiabetic agents using continuous glucose monitoring system (CGMS) during and after ramadan fasting.19 In our study, it is noted that glucose monitoring and home readings were lower and were under normal range during ramadan when compared to the readings before ramadan in all pregnant women with diabetes. This may be due to the short-term improvement in the glycemic control. On the other hand, there was no change in HbA1c levels before and after ramadan for type 1 and type 2 diabetes in pregnant women. Hassanein M et al, assessed the biochemical and biometric changes in patients with diabetes during ramadan in comparison to the pre-ramadan and post-ramadan and suggest low risk patient to fast as fasting is not associated with an increased risk.20 Nor Azlin et al, in prospective cohort study also demonstrated the safety and tolerability of once or twice daily neutral protamine Hagedorn (NPH) insulin for pregnant women who wish to fast during ramadan, while there was a reducing trend in home readings with overall readings noted to be within acceptable limits.21
In our study none of the pregnant women with type 1 diabetes, type 2 diabetes and gestational diabetes patients had experienced severe hypoglycemia. Our results are in line with Afandi B et al, report that glycemic control before ramadan will reduce the potential risks associated with ramadan fasting and minimize glucose fluctuation in diabetes patients.22 The hypoglycemic and hyperglycemic episode were higher in pregnant women with uncontrolled glycemia (HbA1c%; 9.1+0.9) respectively.21,22 Although, in our study all the diabetes pregnant women were under glycemic control (HbA1c%; 7.4±1.3) and experience less hypoglycemic and hyperglycemic episode. In an observational retrospective case-control study in high-risk diabetes patients who insisted on ramadan fasting against healthcare professional and medical advice were more likely to break their fast due to severe hypoglycemia.23
In fact, population-based, epidemiology of diabetes and ramadan (EPIDIAER) study in 2001 also evaluated the safety of ramadan fasting among pregnant women with diabetes while exploring the status of glycemic control during ramadan. It also raised concerns over the high risk of dehydration, diabetes ketoacidosis (DKA), and thrombosis during ramadan fasting. Although, reported a fivefold increase in hyperglycemia in type 2 diabetes and threefold increase in Type 1 diabetes.11 Recently, Multi‐Country Retrospective Observational Study of the Management and Outcomes of Patients with Diabetes during ramadan (CREED study) found 64% of Type 2 diabetes patients fasted every day during ramadan and 94.2% fasted for at least 15 days of ramadan.24 Likewise, many pregnant women with diabetes insisted on fasting ramadan despite being advised against doing so.7,8
In our study all the pregnant women with diabetes appear to have impact of fasting on the short-term glycemic control. Therefore, we have evaluated glycemic control condition as reflected by the improvement of fructosamine levels after ramadan when compared to before ramadan levels. Earlier, it was reported that the paired values of fructosamine with blood glucose for screening high-risk pregnant women with gestational diabetes will be benefited in their management plan.25,26 On the other hand, there was no change in HbA1c between levels before and after ramadan. Fructosamine, unlike HbA1c, results from binding of glucose to serum proteins and, therefore, could have reflected this short-term improvement of glycemic control during the fasting periods.27 In pregnant women with diabetes, strict glycemic control is needed to reduce the incidence of perinatal, maternal, and infant complications. So, we have demonstrated that measurement of fructosamine reflects glycemic control during pregnancy and might be a better indicator of glycemic control in pregnant women. However, large-population studies are needed to assess glycemic control and safety of fasting ramadan during pregnancy.
Study Limitations
There was no comparison made with women who did not fast. The outcome of the pregnancies was not studied. Nevertheless, this is a prospective study on the effects of fasting ramadan on insulin treated diabetes pregnant women with relatively good number of patients. A comparison was made between the effects of fasting on fructosamine and HbA1c levels.
Conclusion
In conclusion, religious and medical recommendations advise pregnant women against fasting as it is unsafe, and they are under high risk. However, if they insist to do fast, they must do under strict medical supervision. Pregnant woman with gestational diabetes tends to tolerate fasting better with less propensity for hypoglycemia. Utilization of fructosamine for short term monitoring of glycemic control in addition to home glucose readings in pregnant women with diabetes will provide a good index of glycemic control.
Data Sharing Statement
The study data are available from the corresponding author upon reasonable request.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee at College of Medicine, King Saud University (Approval No: E-18-3074).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
This project was funded by Dallah HealthCare, Kingdom of Saudi Arabia and grant number(CMRC-DHG 2/008) and research is carried out at King Saud University Medical City (KSUMC) and College of Medicine, King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors declare no conflict of interest in this work.
References
1. Hassanein M, Al-Arouj M, Hamdy O, et al. Diabetes and Ramadan: practical guidelines. Diabetes Res Clin Pract. 2017;126:303–316. doi:10.1016/j.diabres.2017.03.003
2. Muslim Majority Countries 2021. Available from: https://worldpopulationreview.com/country-rankings/muslim-majority-countries.
3. Almalki MH, Alshahrani F. Options for controlling type 2 diabetes during Ramadan. Front Endocrinol (Lausanne). 2016;7:32. doi:10.3389/fendo.2016.00032
4. Azizi F. Research in Islamic fasting and health. Ann Saudi Med. 2002;22(3–4):186–191. doi:10.5144/0256-4947.2002.186
5. Hui E, Reddy M, Bravis V, Rahman M, Darko D, Hassanein M. Fasting among pregnant women with diabetes during Ramadan. Int J Clin Pract. 2012;66(9):910–911. doi:10.1111/j.1742-1241.2012.02983.x
6. Safari K, Piro TJ, Ahmad HM. Perspectives and pregnancy outcomes of maternal Ramadan fasting in the second trimester of pregnancy. BMC Pregnancy Childbirth. 2019;19(1):1–10. doi:10.1186/s12884-018-2145-y
7. Ismail NAM, Raji HO, Abd Wahab N, Mustafa N, Kamaruddin NA, Jamil MA. Glycemic control among pregnant diabetic women on insulin who fasted during Ramadan. Iran J Med Sci. 2011;36(4):254.
8. Afandi BO, Hassanein MM, Majd LM, Nagelkerke NJ. Impact of Ramadan fasting on glucose levels in women with gestational diabetes mellitus treated with diet alone or diet plus metformin: a continuous glucose monitoring study. BMJ Open Diabetes Res Care. 2017;5(1):e000470. doi:10.1136/bmjdrc-2017-000470
9. Al-Arouj M, Assaad-Khalil S, Buse J, et al. Recommendations for management of diabetes during Ramadan: update 2010. Diabetes Care. 2010;33(8):1895–1902. doi:10.2337/dc10-0896
10. Ibrahim M, Davies MJ, Ahmad E, et al. Recommendations for management of diabetes during Ramadan: update 2020, applying the principles of the ADA/EASD consensus. BMJ Open Diabetes Res Care. 2020;8(1):e001248. doi:10.1136/bmjdrc-2020-001248
11. Salti I, Bénard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27(10):2306–2311. doi:10.2337/diacare.27.10.2306
12. Glazier JD, Hayes DJ, Hussain S, et al. The effect of Ramadan fasting during pregnancy on perinatal outcomes: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2018;18(1):1–11. doi:10.1186/s12884-018-2048-y
13. Savitri AI, Painter RC, Lindeboom M, Roseboom TJ, Van Ewijk RJ. Ramadan exposure and birth outcomes: a population-based study from the Netherlands. J Dev Orig Health Dis. 2020;11(6):664–671. doi:10.1017/S2040174419000837
14. Deeb A, Al Qahtani N, Attia S, Al Suwaidi H, Nagelkerke N. Does reducing basal insulin during Ramadan fasting by children and adolescents with type 1 diabetes decrease the risk of symptomatic hypoglycemia? Diabetes Technol Ther. 2016;18(9):539–542. doi:10.1089/dia.2016.0197
15. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Bull World Health Organ. 2007;85:867–872. doi:10.2471/BLT.07.045120
16. Ahmad J, Pathan MF, Jaleel MA, et al. Diabetic emergencies including hypoglycemia during Ramadan. Indian J Endocrinol Metab. 2012;16(4):512–515. doi:10.4103/2230-8210.97996
17. Alghamdi AS, Alghamdi KA, Jenkins RO, Alghamdi MN, Haris PI. Impact of Ramadan on physical activity and sleeping patterns in individuals with type 2 diabetes: the first study using Fitbit device. Diabetes Therapy. 2020;11(6):1331–1346. doi:10.1007/s13300-020-00825-x
18. Sanvictores T, Casale J, Huecker MR. Physiology, Fasting. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534877/.
19. Harbuwono DS, Kurniawan F, Sudarsono NC, Tahapary DL. The impact of Ramadan fasting on glucose variability in type 2 diabetes mellitus patients on oral anti diabetic agents. PLoS One. 2020;15(6):e0234443. doi:10.1371/journal.pone.0234443
20. Hassanein M, Abdelgadir E, Obaid HA, et al. Biometric and metabolic changes in patients with diabetes prior, during and after the holy month of Ramadan (ABCD Study). Diabetes Res Clin Pract. 2021;173:108678. doi:10.1016/j.diabres.2021.108678
21. Nor Azlin MI, Adam R, Sufian SS, et al. Safety and tolerability of once or twice daily neutral protamine hagedorn insulin in fasting pregnant women with diabetes during Ramadan. J Obstetrics Gynaecol Res. 2011;37(2):132–137. doi:10.1111/j.1447-0756.2010.01330.x
22. Afandi B, Kaplan W, Al Hassani N, Hadi S, Mohamed A. Correlation between pre-ramadan glycemic control and subsequent glucose fluctuation during fasting in adolescents with Type 1 diabetes. J Endocrinol Invest. 2017;40(7):741–744. doi:10.1007/s40618-017-0633-y
23. Afandi B, Kaplan W, Al Kuwaiti F, Al Dahmani K, Nagelkerke N. Ramadan challenges: fasting against medical advice. J Nutrition Fasting Health. 2017;5(3):133–137.
24. Babineaux SM, Toaima D, Boye KS, et al. Multi‐country retrospective observational study of the management and outcomes of patients with Type 2 diabetes during Ramadan in 2010 (CREED). Diabetic Medicine. 2015;32(6):819–828. doi:10.1111/dme.12685
25. Khan HA, Sobki SH, Alhomida AS, Khan SA. Paired values of serum fructosamine and blood glucose for the screening of gestational diabetes mellitus: a retrospective study of 165 Saudi pregnant women. Indian J Clin Biochem. 2007;22(1):65–70. doi:10.1007/BF02912884
26. Ayyappan S, Philips S, Kumar CK, Vaithiyanandane V, Sasikala C. Serum fructosamine a better indicator than glycated hemoglobin for monitoring gestational diabetes mellitus. J Pharm Bioallied Sci. 2015;7(Suppl 1):S32. doi:10.4103/0975-7406.155786
27. Hashimoto K, Koga M. Indicators of glycemic control in patients with gestational diabetes mellitus and pregnant women with diabetes mellitus. World J Diabetes. 2015;6(8):1045. doi:10.4239/wjd.v6.i8.1045
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.